Embed Size (px)
Citation preview
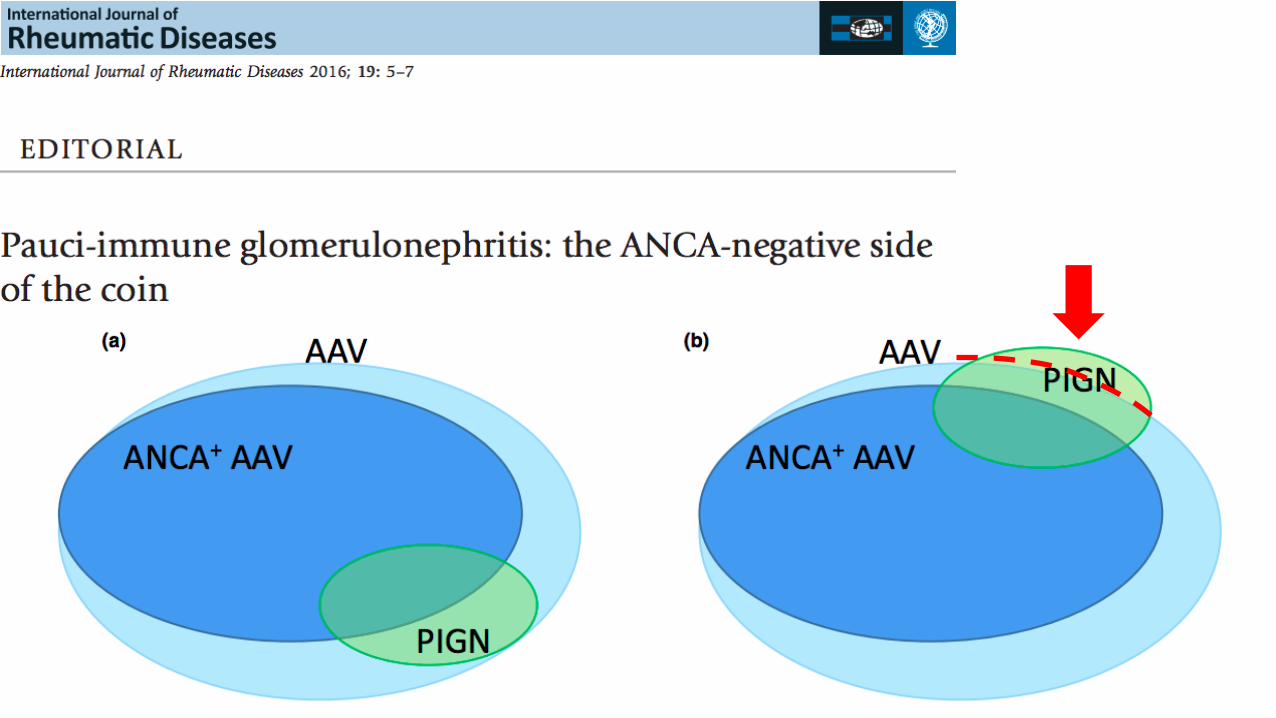
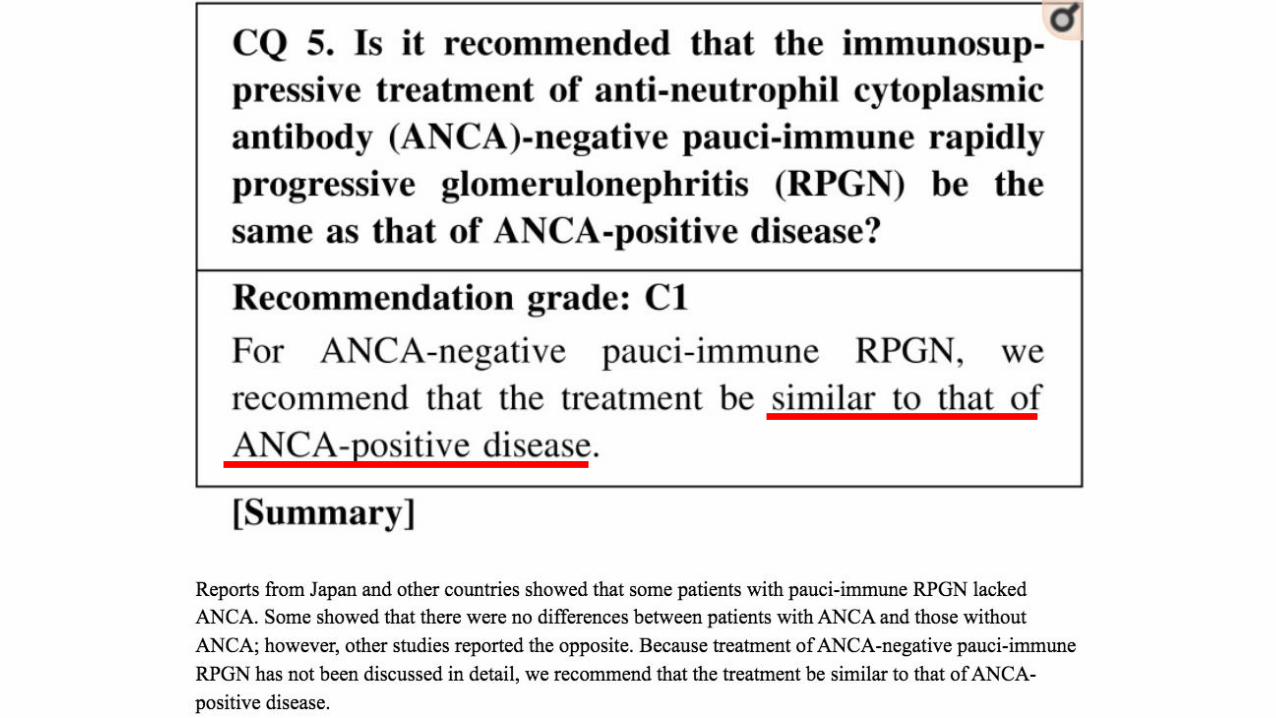
ANCA-negative Pauci-Immune Glomerulonephritis
Supervisor: VS 楊松昇
Speaker: PGY 陳恩揆
Clerk 陳昱臻

Clinical manifestations of GN
• Hematuria
• Proteinuria
• Renal insufficiency
• Hypertension
• Edema
• Hypercoagulability
• Systemic findings
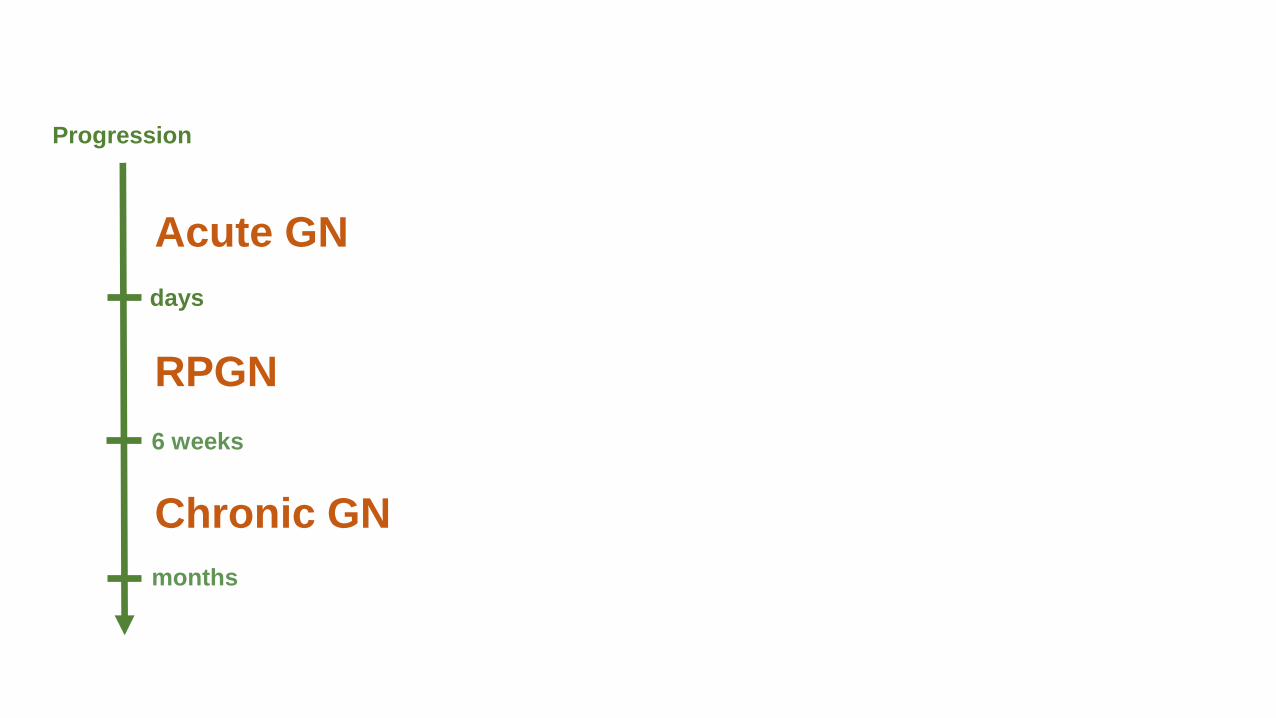
months
6 weeks
days
Acute GN
RPGN
Chronic GN
Progression

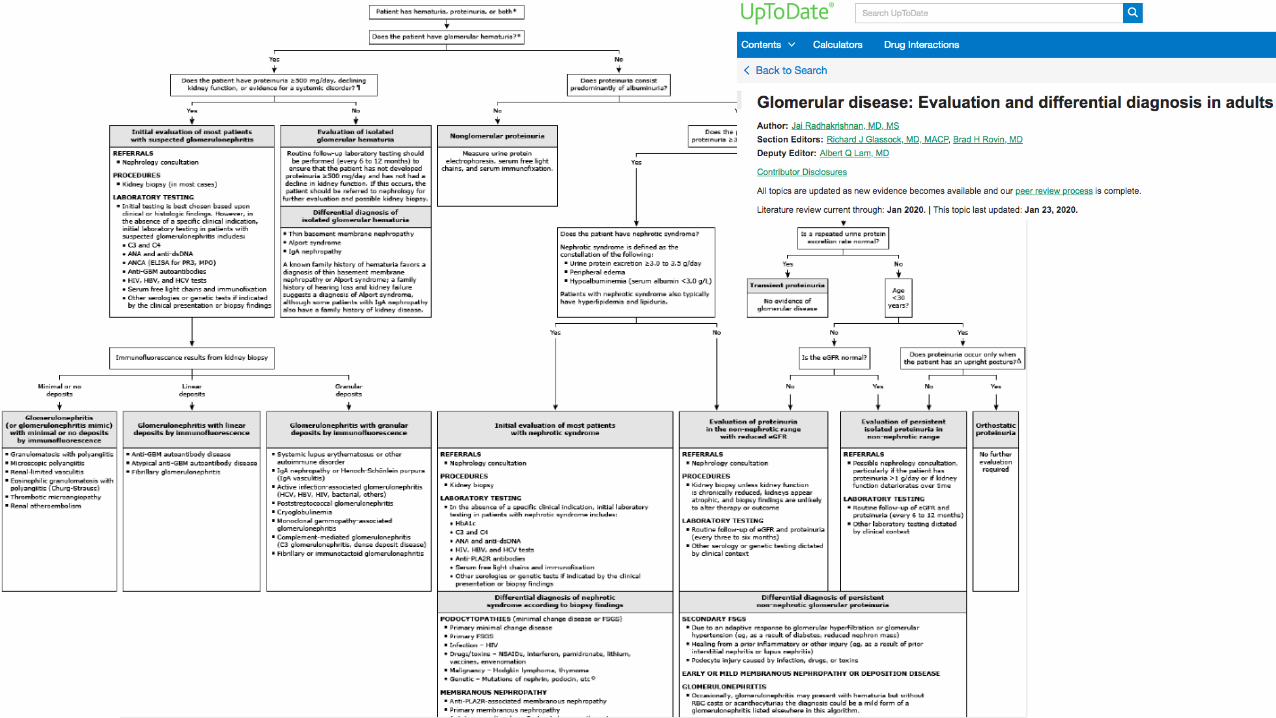
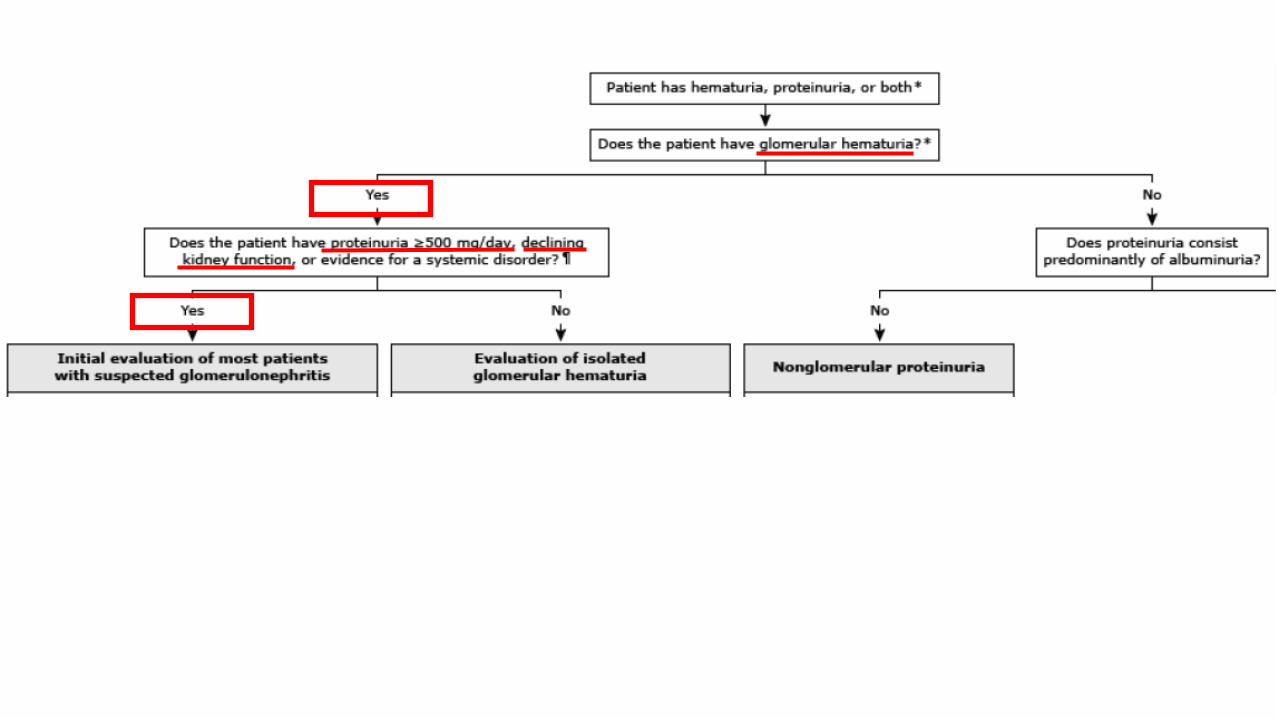
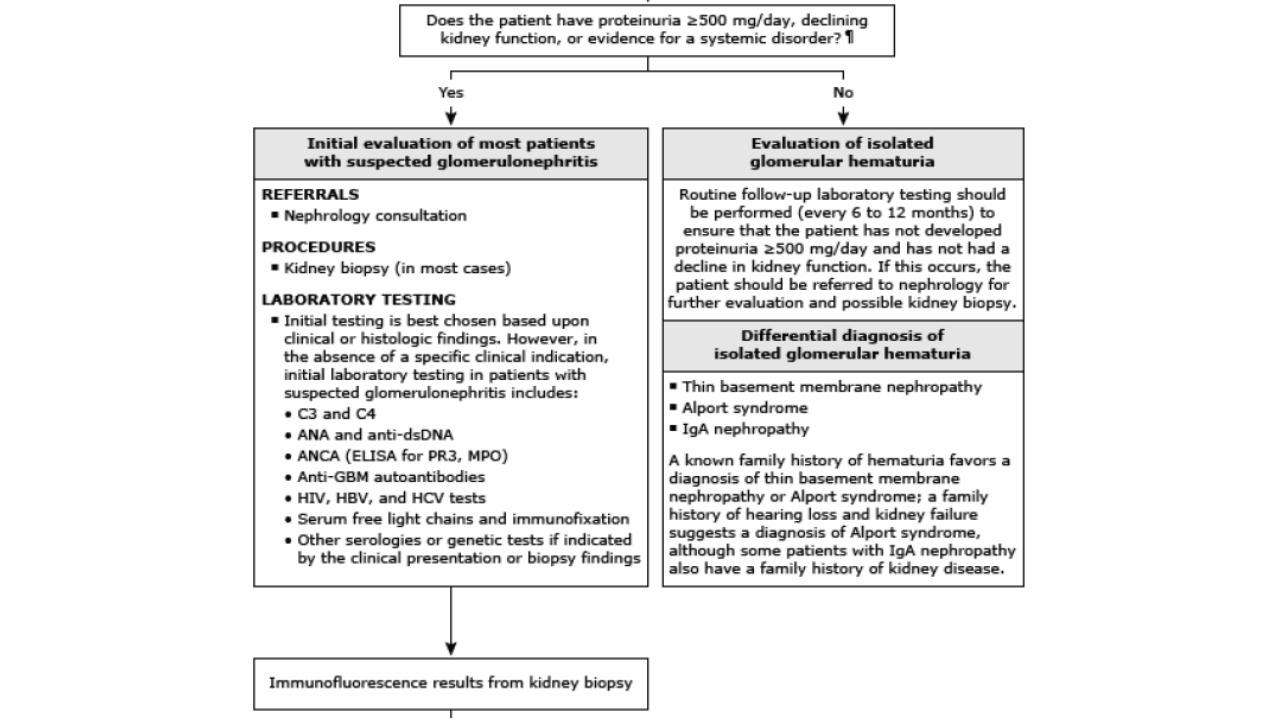
Evaluation of glomerulonephritis
• modest proteinuria (1-4 g/d)
• microscopic hematuria
• RBC and WBC casts.
• Serum C3 and C4
• ANCA(proteinase-3 and myeloperoxidase)
• Anti-GBM Ab
• ANA
• Anti-dsDNA Ab
• HBV, HCV and HIV
• Serum free light chains

Hematuria Proteinuria
• RBC casts or dysmorphic red blood cells
• exclude anatomic lesions, such as BPH or malignancy of the urinary tract, particularly in older men.
• Sustained proteinuria >1–2 g/24 h
• Exclude functional or transient proteinuria(nonsustained, generally <1 g/24 h).
• Fever, exercise, obesity, sleep apnea, emotional stress, and congestive heart failure
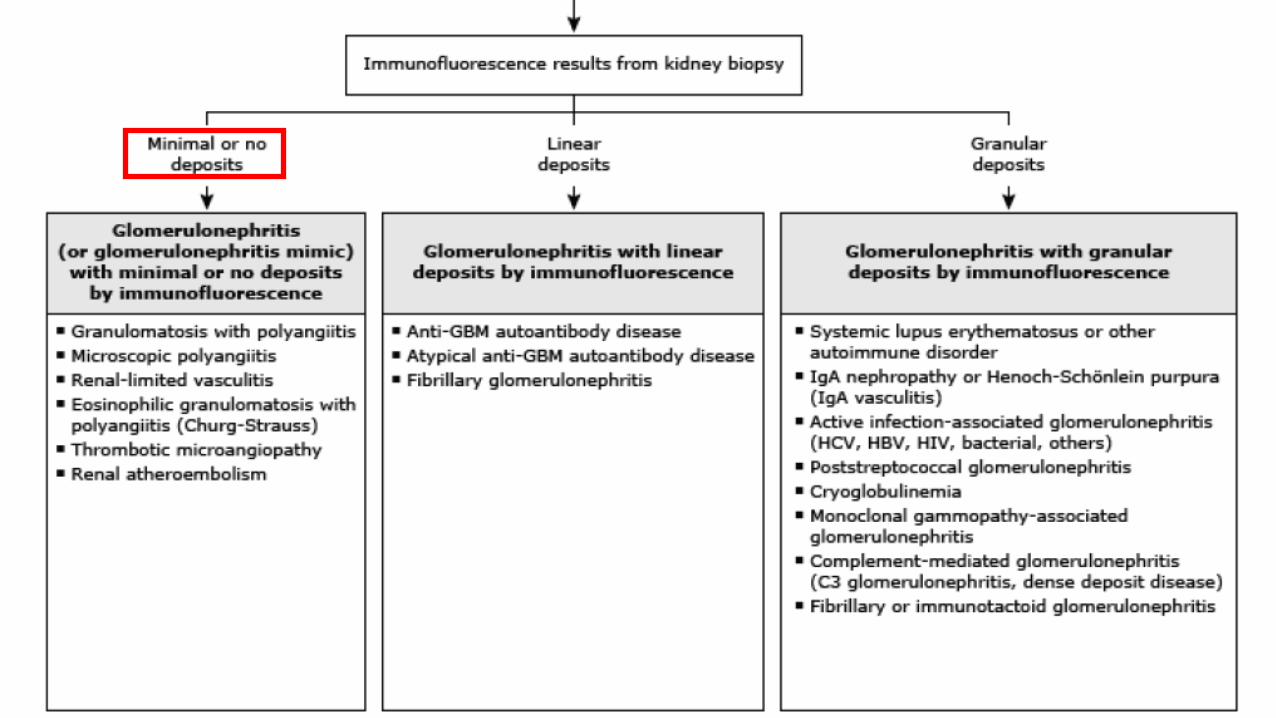

Primary/Idiopathic RPGN
• Type 1 (anti-glomerular basement membrane disease)
• Type 2 (immune-complex mediated)
• Type 3 (pauci-immune)
• Type 4 (combinations of types 1 and 3)
• Type 5 (ANCA-negative, pauci-immune renal vasculitis)
Secondary RPGN
• Infectious process
• Secondary to systemic illness
• Drugs use
• Antithyroid agents
• Superimposed on another primary glomerular disease
14

The role of neutrophils
• Immunohistochemical staining for neutrophil markers(CD15, myeloperoxidase) was much more prominent in active lesions than in inactive lesions
• the degree of neutrophil infiltration in the glomeruli and interstitium: ANCA(-) > ANCA(+)
• Neutrophil-gelatinase-associated lipocalin and lactoferrin.
• Lipocalin: a specific marker of neutrophil degranulation
• Lactoferrin: a biomarker of neutrophil activation and degranulation
• serum levels of neutrophil-gelatinase-associated lipocalin and lactoferrin: ANCA-negative > ANCA-positive
Neutrophil activation
• Anti-endothelial cell antibodies (AECA) are presented in over 50% of patients (10 of 19) with ANCA-negative pauci-immune crescenti glomerulonephritis. AECA bind to endothelial cells, which could facilitate the interaction of neutrophils with these cells via Fc and C3b receptors on neutrophils.
• Autoantibodies to human lysosomal membrane protein 2 (LAMP2) are present in over 90% of individuals with active pauci-immune focal necrotizing glomerulonephritis. These antibodies can activate neutrophils and cause apoptosis of endothelial cells in vitro.
http://www.ijpmonline.org/article.asp?issn=0377-4929;year=2012;volume=55;issue=1;spage=28;epage=32;aulast=Minz#ref8

https://jasn.asnjournals.org/content/21/10/1628.long

19

20
• Clinical and pathologic characteristics were compared between patients with and without ANCA.
https://jasn.asnjournals.org/content/18/2/599#T3
Compared with ANCA(+) PIGN:
• The level of urinary protein and the prevalence of nephrotic syndrome were significantly higher
• the prevalence of extrarenal involvement was significantly lower in ANCA-negative patients.
• Among all the ANCA(-) PIGN, all of them had hematuria and proteinuria. The level of urinary protein was 5.47 ± 3.32 g/24 h.
Compared with ANCA(+) PIGN:
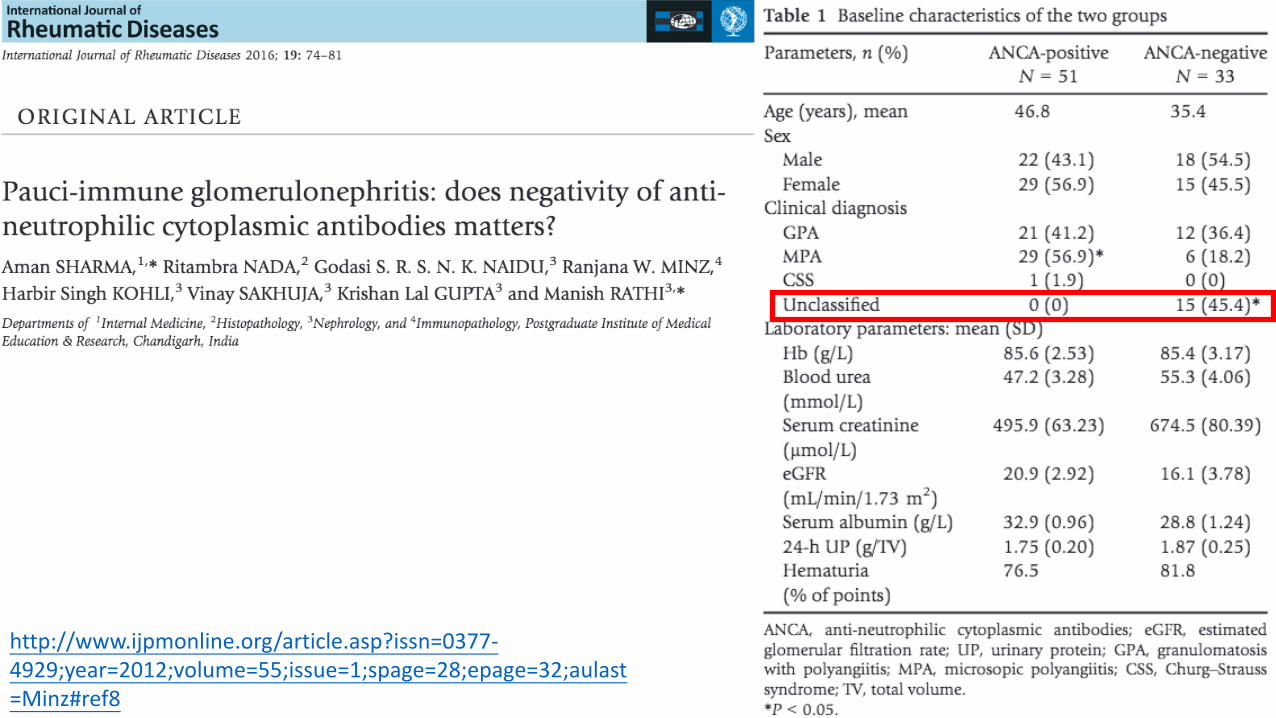
• the ANCA-negative patients were much younger
• Patients with negative ANCA had a significantly lower percentage of normal glomeruli.
• Among glomeruli with crescent formation, the percentage of cellular crescent tended to be higher in patients with negative ANCA than that in patients with positive ANCA
Treatment
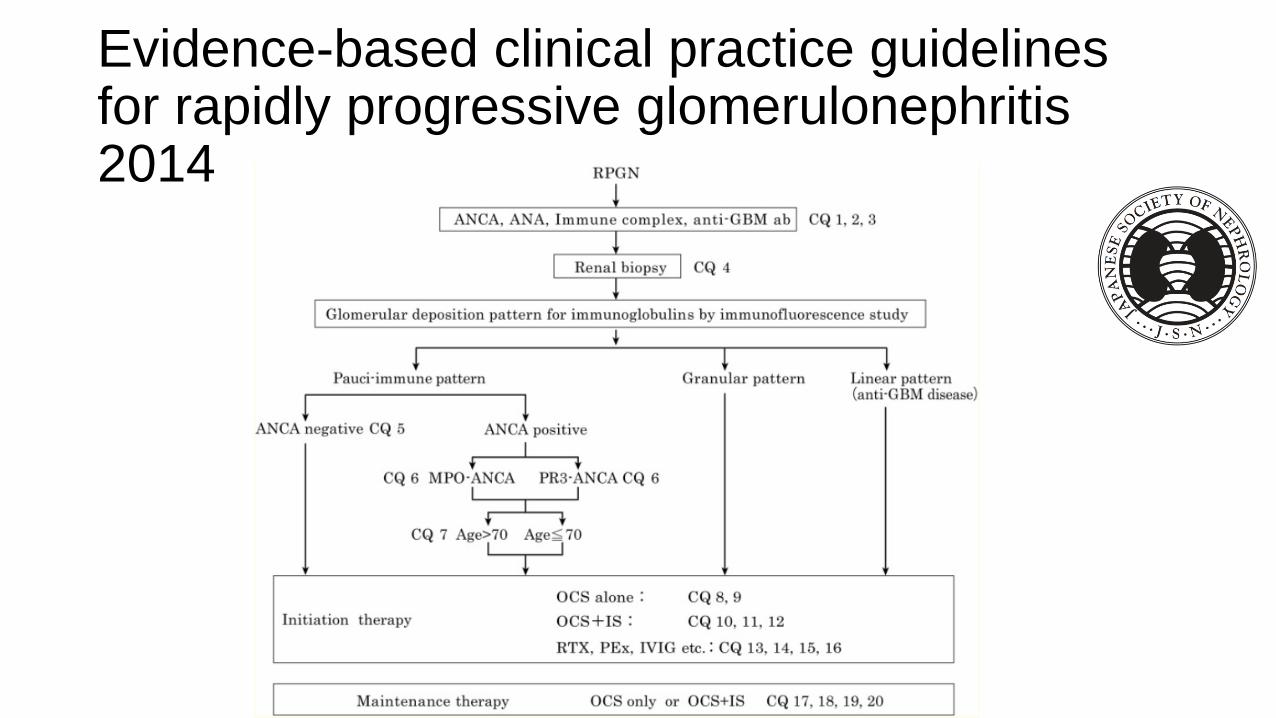
Evidence-based clinical practice guidelines for rapidly progressive glomerulonephritis 2014
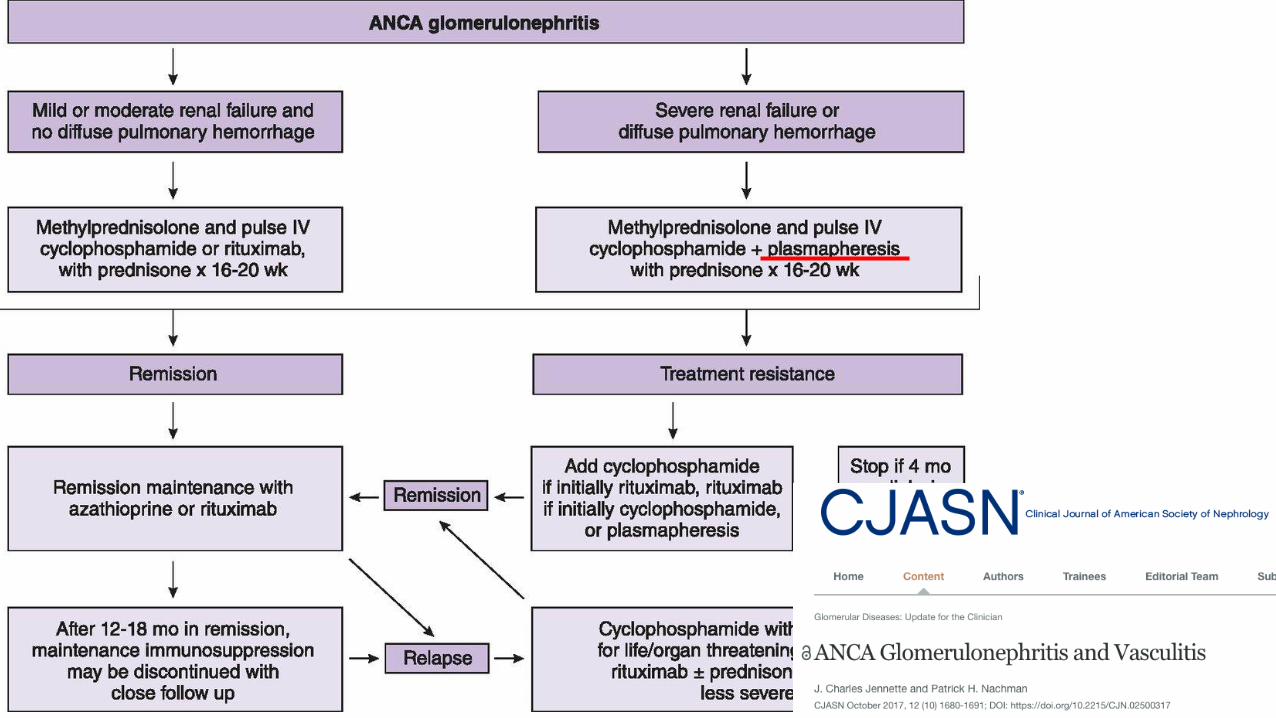
Induction therapy
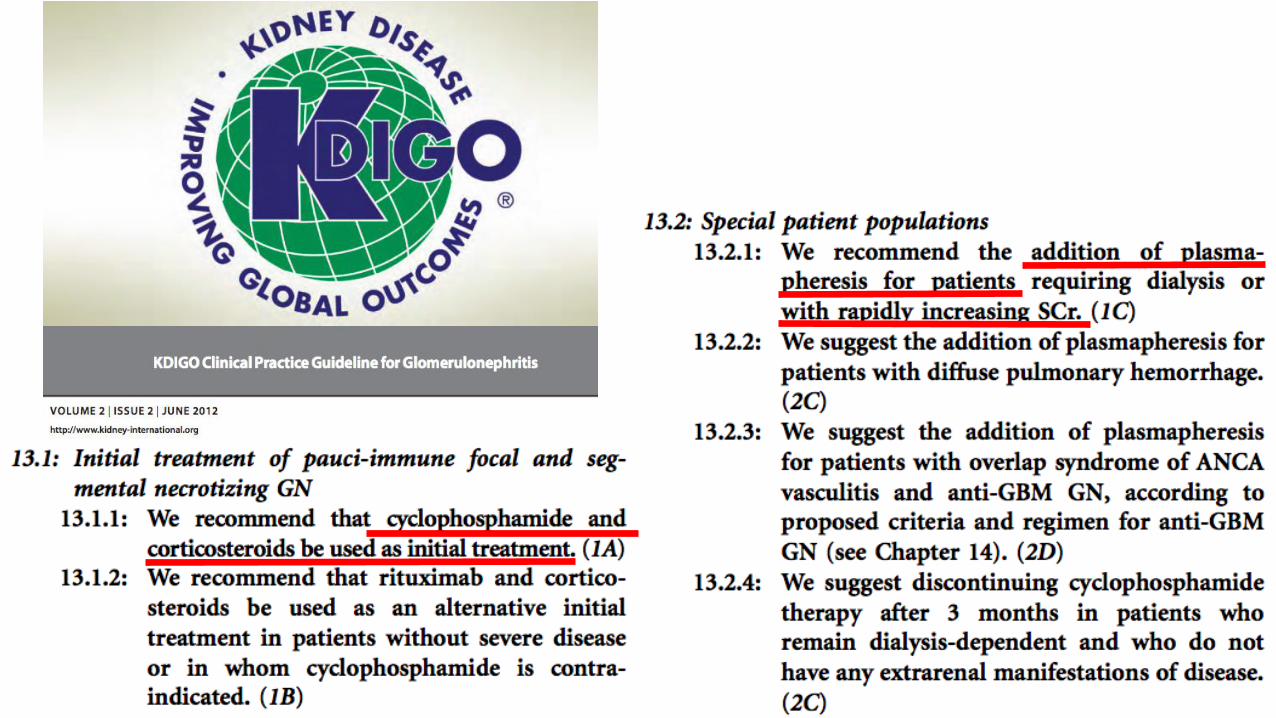
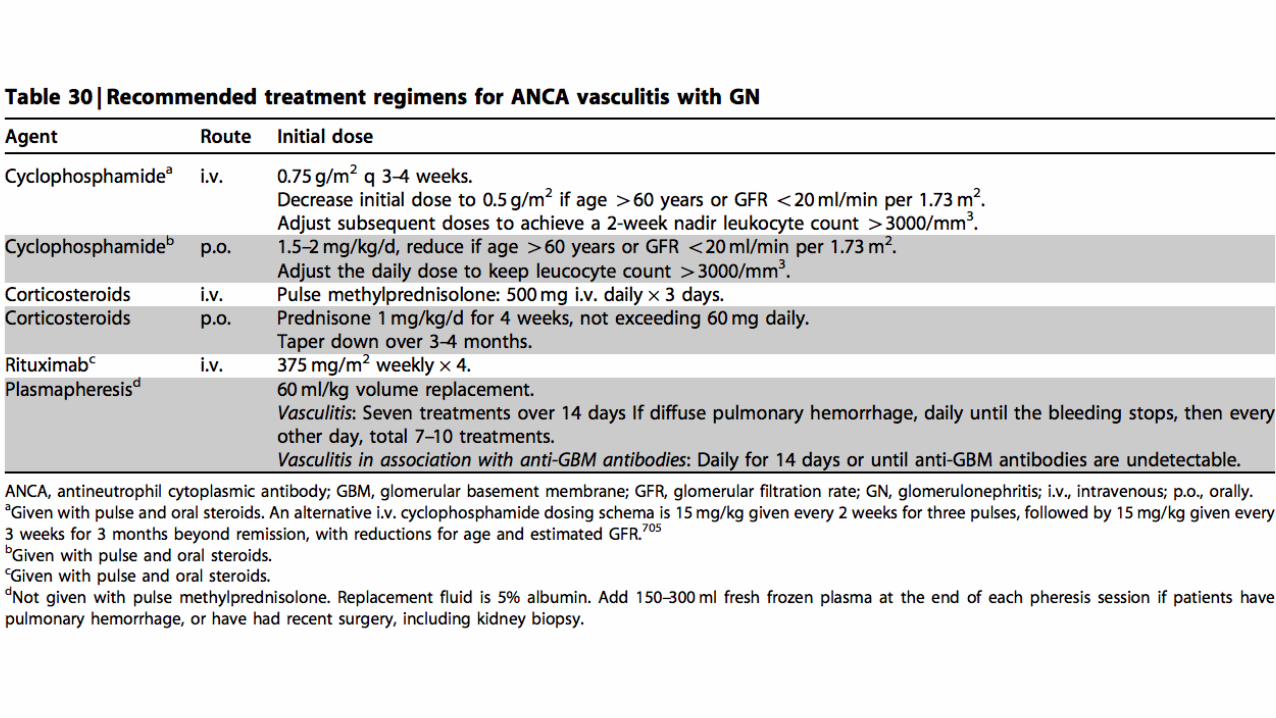
• Gold standard: corticosteroids + cyclophosphamide
• Corticosteroids: 1. IV pulse of methylprednisolone(7mg/kg BW/day) for 3 consecutive
days, followed by oral prednisone(1mg/kg BW/day) for the first 4 weeks
2. reduced gradually over the next 3-5 months.
• Cyclophosphamide: 1. Monthly, IV with starting dose of 0.5g/m2 of BSA
2. Oral with initial dose of 2mg/kg BW/day
3. The duration of cyclophosphamide therapy is usually 6-12 months
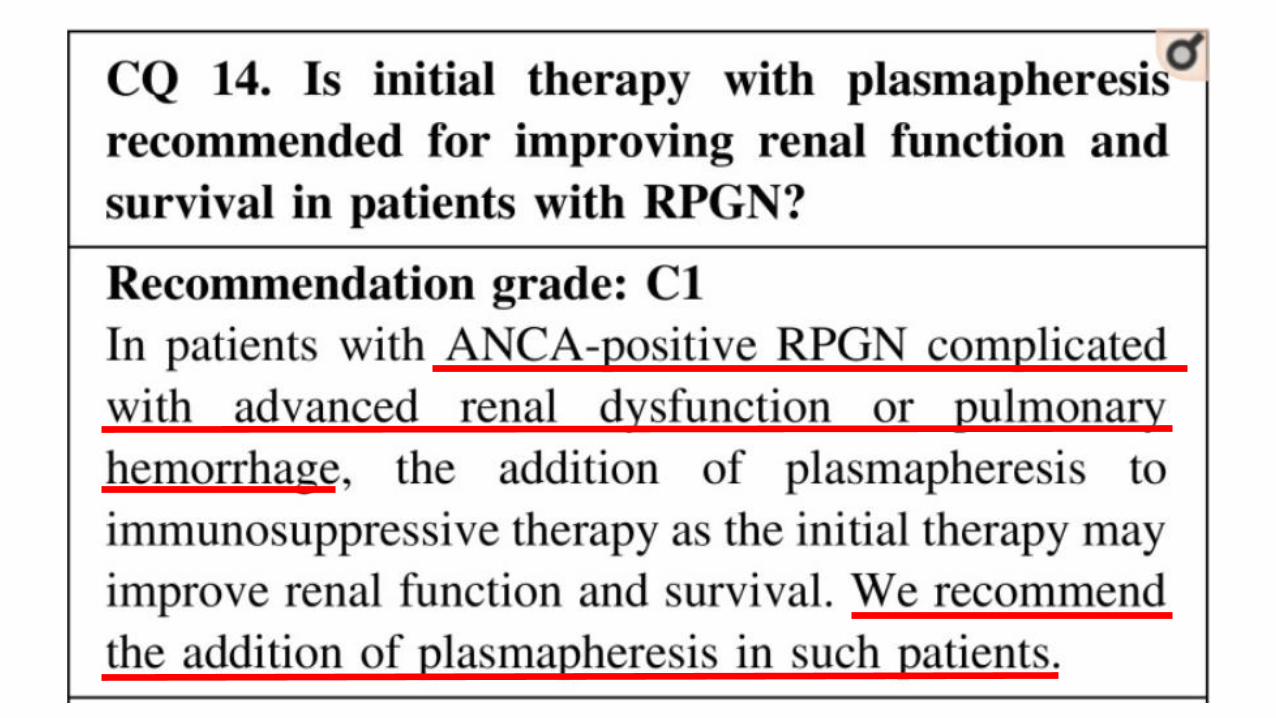
Indications of plasma exchange
• Pulmonary hemorrhage
• Severe renal dysfunction(serum Cr > 5.66mg/dL or >500 umol/L)

Maintenance therapy
• Azathioprine at a dose of 2 mg/kg of body weight/day
• More patients with AAV had sustained remission at 28 months with rituximab than with azathioprine while the frequencies of severe adverse events were similar in the two groups
Reference
• Clinical journal of American Society: ANCA Glomerulonephritis and Vasculitis
• Nature: ANCA-negative pauci-immune crescentic glomerulonephritis
• Clinical and experimental Nephrology: Evidence-based clinical practice guidelines for rapidly progressive glomerulonephritis 2014
• KDIGO Clinical Practice Guideline for Glomerulonephritis(2012)
• Evidence-based clinical practice guidelines for rapidly progressive glomerulonephritis 2014
• Kidney diseases: The Prevalence and Management of Pauci-Immune Glomerulonephritis and Vasculitis in Western Countries
• International journal of Rheumatic disease: Pauci-immune glomerulonephritis: does negativity of anti-neutrophilic cytoplasmic antibodies matters?
• International journal of Rheumatic disease: Pauci-immune glomerulonephritis: the ANCA-negative side of the coin
• Journal of the American Society of Nephrology: Histopathologic Classification of ANCA-Associated Glomerulonephritis
• StatPearls: Crescentric Glomerulonephritis
• UptoDate: Overview of the classification and treatment of rapidly progressive (crescentic) glomerulonephritis
• UptoDate: Glomerular disease: Evaluation and differential diagnosis in adults

Thank you









![ANCA-associated pauci-immune glomerulonephritis in a ... · [8], pauci-immune GN requires immunosup-pression, posing a therapeutic challenge in the setting of bacterial sepsis. We](https://img.pdfslide.net/doc/110x75/5ed359f3080258622969b69d/anca-associated-pauci-immune-glomerulonephritis-in-a-8-pauci-immune-gn-requires.jpg)



















