Embed Size (px)
Citation preview
Bleeding Disorders Magazine
A P U B L I C A T I O N O F
M A R C H 2 0 1 4 — I S S U E N O. 3 1
WOMEN AND BLEEDING DISORDERS

Quest StaffLaura Persons, Managing EditorValerie Hansen, Contributing WriterDan Lorch, Graphic Design
Quest magazine is provided free of charge to the bleeding disorders community. Opinions expressed by contributing authors and sources are not necessarily those of the publisher. Information contained in this newsletter is for educational purposes only and is not intended to substitute for medical or billing advice. Do not use this information to diagnose or treat a health problem or disease without consulting a qualified physician. Consult a physician or appropriate clinical professional before starting or modifying any course of supplementation or treatment. Never disregard medical advice or delay in seeking it because of something you have read in this magazine.
We welcome your comments, stories and suggestions. All correspondence, reprint requests, changes of address and subscription inquiries should be sent to:
Quest Magazine Coram Specialty Infusion Services 555 17th Street, Suite 1500 Denver, CO 80202
Email [email protected]
© 2014 Coram LLC. All rights reserved. No part of this publication may be distributed, reprinted or photocopied without prior written permission of copyright owner. All service marks, trademarks and trade names presented or referred to in this newsletter are the property of their respective owners.
CONTENTS
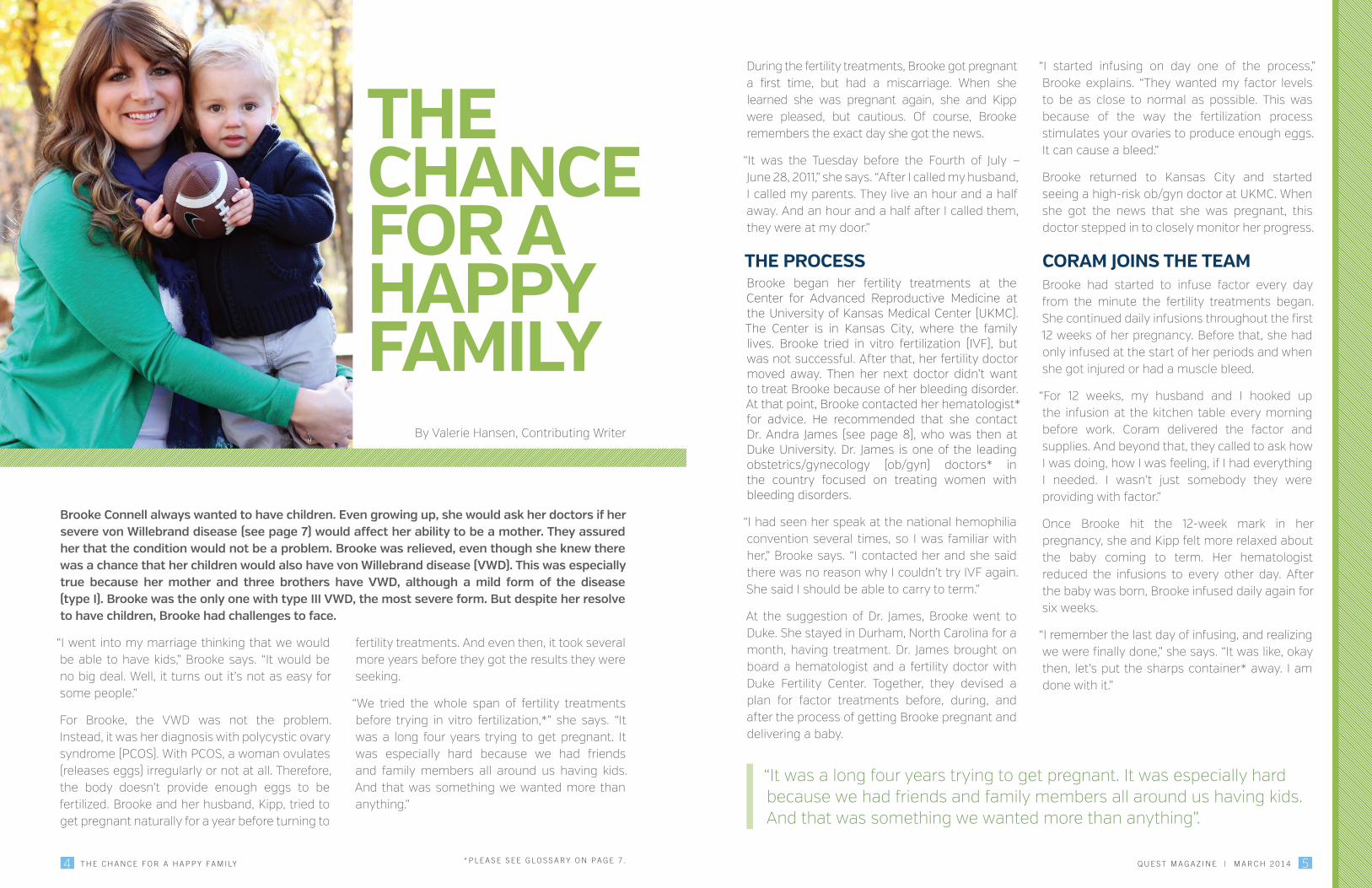
THE CHANCE FOR A HAPPY FAMILYBrooke Connell always wanted to have children. And her doctors always assured her that her severe von Willebrand disease would not stand in her way. But another health condition proved to be a challenge in Brooke's quest to have a child. Learn how Brooke worked with fertility and bleeding disorder specialists to make her lifelong dream come true.
Bleeding Disorders Magazine
4
HOW BLEEDING DISORDERS AFFECT WOMEN THROUGHOUT THEIR LIVESFor women, the impact of bleeding disorders on their lives is quite different than it is for men. To learn more, we spoke with Dr. Andra James, who holds the John M. Nokes Chair as Professor of Obstetrics and Gynecology at the University of Virginia. Read about how women are uniquely impacted by bleeding disorders because of the effects of these conditions on women's reproductive lives.
8
WOMEN CAN HAVE HEMOPHILIA!In the past, many have considered hemophilia to be a disease that only affects males. Women with low levels of clotting factor VIII or factor IX — signs of hemophilia — have instead been called “symptomatic carriers.” In the last few years, however, there has been a shift in the bleeding disorder community. Learn about how more people are now starting to identify these women as having mild hemophilia.
12
MAR. 2014 | ISSUE NO. 31
COR07002-0214
4 5Q U E S T M A G A Z I N E | M A R C H 2 0 1 4T H E C H A N C E F O R A H A P P Y FA M I LY
Brooke Connell always wanted to have children. Even growing up, she would ask her doctors if her severe von Willebrand disease (see page 7) would affect her ability to be a mother. They assured her that the condition would not be a problem. Brooke was relieved, even though she knew there was a chance that her children would also have von Willebrand disease (VWD). This was especially true because her mother and three brothers have VWD, although a mild form of the disease (type I). Brooke was the only one with type III VWD, the most severe form. But despite her resolve to have children, Brooke had challenges to face.
“I went into my marriage thinking that we would be able to have kids,” Brooke says. “It would be no big deal. Well, it turns out it’s not as easy for some people.”
For Brooke, the VWD was not the problem. Instead, it was her diagnosis with polycystic ovary syndrome (PCOS). With PCOS, a woman ovulates (releases eggs) irregularly or not at all. Therefore, the body doesn’t provide enough eggs to be fertilized. Brooke and her husband, Kipp, tried to get pregnant naturally for a year before turning to
fertility treatments. And even then, it took several more years before they got the results they were seeking.
“We tried the whole span of fertility treatments before trying in vitro fertilization,*” she says. “It was a long four years trying to get pregnant. It was especially hard because we had friends and family members all around us having kids. And that was something we wanted more than anything.”
During the fertility treatments, Brooke got pregnant a first time, but had a miscarriage. When she learned she was pregnant again, she and Kipp were pleased, but cautious. Of course, Brooke remembers the exact day she got the news.
“It was the Tuesday before the Fourth of July — June 28, 2011,” she says. “After I called my husband, I called my parents. They live an hour and a half away. And an hour and a half after I called them, they were at my door.”
THE PROCESSBrooke began her fertility treatments at the Center for Advanced Reproductive Medicine at the University of Kansas Medical Center (UKMC). The Center is in Kansas City, where the family lives. Brooke tried in vitro fertilization (IVF), but was not successful. After that, her fertility doctor moved away. Then her next doctor didn’t want to treat Brooke because of her bleeding disorder. At that point, Brooke contacted her hematologist* for advice. He recommended that she contact Dr. Andra James (see page 8), who was then at Duke University. Dr. James is one of the leading obstetrics/gynecology (ob/gyn) doctors* in the country focused on treating women with bleeding disorders.
“I had seen her speak at the national hemophilia convention several times, so I was familiar with her,” Brooke says. “I contacted her and she said there was no reason why I couldn’t try IVF again. She said I should be able to carry to term.”
At the suggestion of Dr. James, Brooke went to Duke. She stayed in Durham, North Carolina for a month, having treatment. Dr. James brought on board a hematologist and a fertility doctor with Duke Fertility Center. Together, they devised a plan for factor treatments before, during, and after the process of getting Brooke pregnant and delivering a baby.
“I started infusing on day one of the process,” Brooke explains. “They wanted my factor levels to be as close to normal as possible. This was because of the way the fertilization process stimulates your ovaries to produce enough eggs. It can cause a bleed.”
Brooke returned to Kansas City and started seeing a high-risk ob/gyn doctor at UKMC. When she got the news that she was pregnant, this doctor stepped in to closely monitor her progress.
CORAM JOINS THE TEAMBrooke had started to infuse factor every day from the minute the fertility treatments began. She continued daily infusions throughout the first 12 weeks of her pregnancy. Before that, she had only infused at the start of her periods and when she got injured or had a muscle bleed.
“For 12 weeks, my husband and I hooked up the infusion at the kitchen table every morning before work. Coram delivered the factor and supplies. And beyond that, they called to ask how I was doing, how I was feeling, if I had everything I needed. I wasn’t just somebody they were providing with factor.”
Once Brooke hit the 12-week mark in her pregnancy, she and Kipp felt more relaxed about the baby coming to term. Her hematologist reduced the infusions to every other day. After the baby was born, Brooke infused daily again for six weeks.
“I remember the last day of infusing, and realizing we were finally done,” she says. “It was like, okay then, let’s put the sharps container* away. I am done with it.”
THE CHANCE FOR A HAPPY FAMILY
By Valerie Hansen, Contributing Writer
“It was a long four years trying to get pregnant. It was especially hard because we had friends and family members all around us having kids. And that was something we wanted more than anything”.
* P L E A S E S E E G L O S S A RY O N PA G E 7 .

7Q U E S T M A G A Z I N E | M A R C H 2 0 1 46 T H E C H A N C E F O R A H A P P Y FA M I LY
THE DELIVERYBrooke had a hard delivery. The baby was big at 8 pounds, 10 ounces. And the doctors had ruled out an epidural* for fear it might cause bleeding into the spinal column.
“That was definitely not my choice,” Brooke says. “I wanted that epidural.”
Her preference is no surprise, as she checked into the hospital at 4:00 am on February 29, 2012 and didn’t have the baby until the next day at 6:00 am. Brooke required five pints of blood and platelets. And three days after delivery, she had a postpartum hemorrhage.* After a week in the hospital, she and Kipp took their baby boy home.
“We named him Chance because he was our chance to be parents,” Brooke says. “If it had been a girl, we were going to name her Andra, after Dr. James.”
THE CENTER OF THEIR UNIVERSEChance is a toddler now, with all that entails. He has mild VWD, but that doesn’t slow him down at all. He is doted on by two sets of grandparents, his parents, and his dog, Lucky.
“You can tell he is a little spoiled,” Brooke says with a smile, “but he is very sweet. He will just look at you and say, ‘Hi,’ very softly. He is into sports and watches football with his dad, which makes his dad very happy. He doesn’t have many limitations. He has bruises like any other little boy, but it’s nothing like what I went through growing up.”
It’s pretty certain that Chance will be involved in sports. He is a big boy, and his father played college football. That’s fine with Brooke.
“His hematologist wants Chance to do whatever he wants. He just has to keep in mind that he might have to get factor before he does it. And I agree. The more active, the better.”
At the present, however, Chance is more into dancing at weddings. The young family has attended quite a few recently, and Chance gets out on the dance floor as soon as the music starts.
“People have actually asked at the weddings if Chance is going to dance,” Brooke says. “He’s pretty proud of himself when he does.”
THE FUTUREAs hard as the process was for Brooke to get pregnant, carry to term, and undergo 26 hours of labor, she is ready to have another child.
“A month after we were home, I told my husband I was ready to do it again,” Brooke says.
They tried a frozen embryo transfer* last summer, but Brooke miscarried eight weeks into the pregnancy. Despite that setback, it’s clear that Brooke and Kipp would like to give Chance a little brother or sister sooner rather than later. Maybe he will teach him or her some of his dance moves.
*Glossary
» Epidural: A form of anesthesia used to partly numb the lower body. It is injected into the area around the spinal cord. This area is called the epidural space.
» Frozen embryo transfer: A procedure during which an embryo is fertilized outside of the body and frozen. It is then thawed and placed in a woman’s uterus.
» Hematologist: A doctor who treats blood diseases.
» In vitro fertilization (IVF): A type of fertility treatment. With IVF, sperm is placed with an egg in a laboratory. After fertilization occurs, the embryo is placed into the woman’s uterus. Or it may be frozen for future use.
» Ob/gyn doctor: A doctor who works in obstetrics and gynecology. Obstetrics is the care of women during pregnancy and childbirth. Gynecology is the treatment of female reproductive organs.
» Postpartum hemorrhage: Abnormal bleeding that occurs two to four weeks after birth.
» Sharps container: A container used to safely dispose of used needles (sharps).
ABOUT VON WILLEBRAND DISEASE
The most common bleeding disorder in women is von Willebrand disease (VWD).
VWD is an inherited bleeding disorder. This means it is passed down from parent to child through the genes. With VWD, there
are low levels of a certain protein in the blood, or the protein doesn't work the way it should.
The protein is called von Willebrand factor (VWF). It helps the blood to clot.
• VWD is the most common of all the inherited bleeding disorders. In the U.S., it occurs in about
1 out of every 100 people.
• VWD affects both males and females equally.
• Common signs of VWD in women include frequent bruising and heavy menstrual periods.
There are three types of VWD: types I, II, and III.
• With type I, there is a low level of VWF, and there may be lower levels of factor VIII than normal. (Factor
VIII is another type of blood-clotting protein.) This is the mildest form of VWD. It is also the most common form.
About 75% of people who have VWD have type I.
• With type II, the VWF doesn’t work the way it's supposed to. Type II is divided into subtypes: 2A, 2B, 2M, and 2N.
Changes in different genes cause each type. Each type is treated differently. For this reason, it is important to know
the exact type of VWD a person has.
• With type III, there is usually no VWF, and low levels of factor VIII. Type III is the most serious form of VWD and is very rare.
Although there is no cure for VWD, treatment is available. It can help to control symptoms. It can also help people with VWD avoid
complications, and help improve their quality of life.
Sources:Facts about von willebrand disease. The Centers for Disease Control and Prevention. www.cdc.gov/ncbddd/vwd/facts.html. Accessed 1.17.14.
What is von Willebrand disease? The National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health/health-topics/topics/vwd/. Accessed 1.17.14.

9Q U E S T M A G A Z I N E | M A R C H 2 0 1 4
Dr. Andra James holds the John M. Nokes Chair as Professor of Obstetrics and Gynecology at the University of Virginia. She is considered one of the top obstetrics and gynecology (ob/gyn) and high-risk pregnancy doctors in the country. She is also one of the founders of the Foundation for Women and Girls with Blood Disorders (see page 11). In addition, she is the doctor who led Brooke Connell through her fertility treatments and pregnancy two years ago (see page 4). We spoke with Dr. James recently to learn more about how bleeding disorders affect women.
For women, the impact of bleeding disorders on their lives is quite different than it is for men. “Women are uniquely affected by bleeding disorders because of reproduction issues. These are mainly menstruation and childbirth,” Dr. James says.
DIAGNOSIS FOR WOMENMany women with bleeding disorders are not diagnosed until they start menstruating. They may have frequent bruising as children, but that does not raise a red flag like a long and heavy period. This delayed diagnosis often occurs for women with no family history of bleeding disorders.
According to Dr. James, period symptoms that can signal a bleeding disorder include:
� Periods lasting more than seven days
� Soaking through a tampon or pad every hour or two
� Passing clots more than an inch in diameter
� Soaking through nightclothes despite the use of a pad or tampon
� A diagnosis of anemia* caused by heavy periods
Fortunately, heavy periods in many women with bleeding disorders can be treated. Clotting factor may be an option. Another option may be hormones (birth control pills).
How Bleeding Disorders Affect Women Throughout Their LivesBy Valerie Hansen, Contributing Writer
SUPPORT THROUGHOUT THEIR LIVESDuring certain phases of their reproductive lives, women with von Willebrand disease (VWD)* or mild hemophilia often require support. This support can come from a hematologist* and an ob/gyn doctor. After the start of menstruation, these women may need support during:
� Pre-conception
� Pregnancy
� Childbirth
� Postpartum
� Perimenopause
PRE-CONCEPTIONPrior to conception (getting pregnant), women with bleeding disorders may want to have genetic counseling.* This can help them gain knowledge about the chances of their child having a bleeding disorder and how severe it could be.
“For a woman who has mild hemophilia or is a carrier,* we are interested in the family’s genetics,” Dr. James says. “This can tell us how likely it is that her child will have hemophilia.”
The next issues to be addressed before pregnancy include the risks to the mother of a pregnancy and childbirth. They also include the risks to the unborn baby. Once these risks are assessed, planning can begin for a safe pregnancy and delivery.
PREGNANCYAccording to Dr. James, after a woman conceives, a special medical team is assembled. This group of experts plans the steps to be taken for a successful pregnancy and delivery.
“It takes a team every time,” Dr. James says. “It takes a specialist who understands the issues the mother might have. It also requires a specialist who knows the issues the unborn baby might have. A genetic counselor may be involved. And the hospital should have access to experts in
hemostasis* [such as the professionals in a hemophilia treatment center]. Also, the team should include a pediatric hematologist.”
Throughout her pregnancy, the mother’s factor levels and platelet count* are checked. Her treatment is adjusted in response to the results.
CHILDBIRTHBefore delivery, Dr. James's team of specialists decides if a cesarean section* or vaginal delivery is best. They also make choices to help ensure the safest delivery. For instance, some choices are made to try to prevent bleeding.
“If we cannot ensure that the mother’s lowest factor level [her “trough” level] is above 50%, we will not give an epidural,*” says Dr. James. “This is because of concern about bleeding.”
POSTPARTUM (AFTER BIRTH)Bleeding is also a concern after delivery for women with bleeding disorders.
“With childbirth, there are several chances for blood loss,” Dr. James explains. “Women’s von Willebrand and factor VIII levels* rise by about 50% in the time before delivery. And they remain raised for a short time afterward. But a woman with a bleeding disorder is at greater risk of bleeding because she will have lower factor levels to begin with.”
If a woman with a bleeding disorder does have bleeding, she will be treated with factor, says Dr. James. But despite the bleeding risk, many such women do not need factor during or after pregnancy. This is because either their condition is mild, or their natural increase in factor levels is enough to protect them.
* P L E A S E S E E G L O S S A RY O N PA G E 1 0 .
The Foundation for Women and Girls with Blood Disorders (FWGBD) was formed in July 2010. It was created by three powerful women in the world of blood disorders. They are Dr. Andra James, Dr. Barbara Konkle, and Dr. Roshni Kulkarni (see right). The goal of these women was to improve understanding in the medical field about women and blood disorders.
“We were started by three of the top experts in the world on women with blood disorders,” says Executive Director Ann-Marie Nazzaro. She says they recognized a problem in the medical community regarding women and these conditions. “Their sense was that providers were not resistant to knowing more about women with blood disorders. They just weren’t well-trained in that area.”
“We have found that hematologists don’t always understand reproductive issues,” says Dr. James. “We have also found that reproductive specialists don’t always understand bleeding disorder issues. We wanted the Foundation to be a bridge between those two medical professions.”
The Foundation addresses a range of blood disorders. However, hemophilia and von Willebrand disease are a large part of their focus. The group’s goal is to build a bridge of knowledge between the key healthcare providers that treat girls and women through each phase of their lives. These providers range from pediatric hematologists and adolescent gynecologists to nurses and social workers.
FWGBD created four core tactics to help achieve their educational goals:
1. Presenting workshops at the major medical society meetings.
2. Building a state-of-the-art website as a resource for healthcare providers.
3. Creating educational webinars and working with Duke University to grant continuing education credits for these and other programs.
4. Improving the teaching tools for medical professionals who might care for female patients with blood disorders.
FWGBD works with numerous other groups concerned with blood disorders in women. These include the National Hemophilia Foundation, the Hemophilia Federation of America, and the World Federation of Hemophilia. The FWGBD is an exciting new force in the world of blood disorders. And it is one that may have a real impact on the way that women’s blood disorder issues are treated by the medical field in the future.
For more information about FWGBD, visit www.fwgbd.org.
FWGBD Founders
Dr. Dr. Andra James
• The John M. Nokes Professor of Obstetrics and Gynecology at the University of Virginia
• An obstetrics and gynecology doctor and high-risk pregnancy expert
Dr. Barbara Konkle
• Director of Clinical and Translational Research at the Puget Sound Blood Center
• Professor of Medicine, Division of Hematology, at University of Washington
• Co-chair of the National Heart, Lung and Blood Institute’s Research Committee on Women’s Bleeding Disorders
Dr. Roshni Kulkarni
• Director of Pediatric Hematology/Oncology at Michigan State University
• Former Director of the Centers for Disease Control’s Division of Blood Disorders
• Recipient of the Food and Drug Administration’s Distinguished Service Award
The vision for FWGBD is to “ensure that all women and adolescent girls with blood disorders are correctly diagnosed and optimally treated and managed at every life stage.”
FWGBD: Exciting New Support for Women with Bleeding Disorders
10 11Q U E S T M A G A Z I N E | M A R C H 2 0 1 4H O W B L E E D I N G D I S O R D E R S A F F E C T W O M E N T H R O U G H O U T T H E I R L I V E S
PERIMENOPAUSE*As women move into menopause, they begin to have irregular periods. If this causes their cycle to be delayed, the lining of the uterus may become thicker than normal. This can result in heavy bleeding during their period. Heavy bleeding can be an even bigger concern for women with bleeding disorders.
“These women need to have their periods regulated,” Dr. James explains. “They may not be candidates for birth control pills [which can help manage periods] at that point in their life. But there are other treatments that can help. Again, this is an issue that needs to be addressed by the hematologist along with the gynecologist.“
As they grow older, women with bleeding disorders need to be aware that they may be more likely to have some health issues than those with normal factor levels. For instance, they may develop heavy bleeding if they have certain gynecologic problems. These include uterine fibroids,* cervical polyps,* and endometrial hyperplasia.*
CARE THROUGHOUT THEIR LIVESThroughout their reproductive lives, women with bleeding disorders have special concerns. Therefore, it is essential that they be properly diagnosed and treated. A diagnosis and a care team working together can help these women understand their unique health needs. This can help them plan for the care that's right for them throughout their lives.
*Glossary
» Anemia: A condition in which there are not enough red blood cells to carry oxygen throughout the body.
» Carrier: A person who has genes for a certain condition, but does not have symptoms of the condition.
» Cesarian section: Also called a C-section. Surgery in which a baby is delivered through an incision (cut) in the mother’s abdomen.
» Cervical polyp: A tissue mass inside the cervix.
» Genetic counseling: Educational counseling regarding conditions that are passed down in families through their genes. This counseling addresses the impacts these conditions can have on the children’s health.
» Endometrial hyperplasia: Overgrowth of the lining of the uterus.
» Epidural: A form of anesthesia used to partly numb the lower body. It is injected into the area around the spinal cord. This area is called the epidural space.
» Factor — von Willebrand factor and factor VIII: Proteins in the blood that help with clotting. Missing or low levels of von Willebrand factor cause von Willebrand disease (see below). Missing or low levels of factor VIII cause hemophilia A.
» Hematologist: A doctor who treats blood diseases.
» Hemostasis: The process of stopping bleeding.
» Perimenopause: The time when a woman’s body transitions to menopause.
» Platelet count: The number of platelets in the blood. Platelets are tiny cells that clump together to form a blood clot.
» Uterine fibroids: Benign (not cancerous) tumors that can form in the uterus.
» von Willebrand disease (VWD): An inherited bleeding disorder. VWD occurs when the blood does not have enough von Willebrand factor, or when that factor doesn’t work right. (See page 7.)
12 13Q U E S T M A G A Z I N E | M A R C H 2 0 1 4
In the past, many have considered hemophilia* to be a disease that only affects males. Women with low levels of clotting factor VIII or factor IX — signs of hemophilia — have instead been called “symptomatic carriers.” This means that they carry the hemophilia gene and have symptoms of the bleeding disorder. But they have not been considered to have hemophilia.
In the last few years, however, there has been a shift in the bleeding disorder community. People are now starting to identify these women as having mild hemophilia. In truth, both descriptions apply. This is because one is a genetic description and the other is a clinical diagnosis. This is explained by Dr. Marion Koerper (pictured above), Medical Advisor for the National Hemophilia Foundation (NHF). Dr. Koerper is also Director Emerita of the Hemophilia Treatment Center (HTC)* at the University of California, San Francisco.
“Symptomatic carrier is a term that relates to genetics. All it does is tell a woman what her chances are of having a child with hemophilia. It has nothing to do with treatment,” Dr. Koerper explains. “Mild hemophilia is a clinical diagnosis. This diagnosis is what impacts treatment. And
treatment is the important part when someone has a bleeding disorder.”
Dr. Koerper has been ahead of the curve in changing how women with mild hemophilia are viewed. For 30 years, she has been telling her diagnosed female patients that they have mild hemophilia and need to get treatment through an HTC.
“If your factor level is low,” Dr. Koerper says, “it makes no difference if you are male or female. The result is the same. You have mild or moderate hemophilia.”
Fortunately, her view is growing within the hemophilia community. This shift is important because it affects how medical professionals — even hematologists* — treat a woman’s bleeding disorder. “Hemophilia” is considered to be more of a medical condition that needs treatment than “symptomatic carrier” is. And more aggressive treatment can mean healthier women. In the past, there have been many cases when a woman’s claim to have hemophilia was dismissed by healthcare professionals. This approach led to serious bleeds after surgery or other procedures.†
EXPLAINING FACTOR LEVELSTo understand what mild hemophilia means, it helps to understand the ranges of the condition. Normal factor VIII and IX* levels — these are the amounts of clotting factors in a person’s blood
— range between 50% and 150%. People in that range do not have a bleeding disorder, Dr. Koerper explains. At the other end of the spectrum are people with a factor level of 1% or below. These people have severe hemophilia.
People with factor levels of 1% to 5% have moderate hemophilia. “People with moderate hemophilia will bleed once or twice a month, and will certainly bleed with surgery,” Dr. Koerper says. “They may not bleed often enough to require prophylaxis,* as those with severe hemophilia do. But in some cases, they will.”
People with a factor level that ranges between 6% and 49% have mild hemophilia.
HORMONES AND FACTOR VIII LEVELSOne important aspect of factor VIII levels, in contrast to factor IX levels, is how greatly they can change. For example, a woman’s factor VIII level drops before her period starts, and rises afterward.
“Hormones cause changes in factor VIII levels,” Dr. Koerper explains. “A woman’s lowered estrogen level before her period causes her factor VIII level to drop. Then, the increase in her estrogen level after the start of her period causes this level to rise. If you test her factor VIII level on the first day or two of her period, you might get a level of 35%. However, that reading might be 55% shortly before her period starts again.
“What counts is the lower level. That is the level that needs to be treated. With women, the treatment isn’t always factor. If the problem is heavy periods, we can sometimes put them on a birth control pill that contains estrogen.”
For all women, factor VIII levels go up a good deal during pregnancy due to changes in hormone levels. If a woman normally has a 100% factor level, it might rise to 200% by the ninth month of her pregnancy, says Dr. Koerper. If her usual factor VIII level is 30%, it might rise to 130% by the end of the pregnancy. This change helps keep the mother from bleeding when she delivers her infant.
Dr. Koerper points out that estrogen is not the only hormone that affects factor VIII levels. Another is adrenaline* (epinephrine). If a woman is frightened because of surgery, for instance, that will cause her adrenaline level to increase. As a result, her factor VIII level will go up. However, in a few days the level can go down again. And then she may need treatment for her low factor level.
A third hormone that can affect factor levels is desmopressin (DDAVP). In fact, this hormone can be used as a treatment for women who have problem periods due to a bleeding disorder.
THE GENETICSTo explain the genetic connection of hemophilia, Dr. Koerper gives an example. If identical twin girls have a father with severe hemophilia A, one of the girls could have mild hemophilia, while the other could be normal. The first girl could have a factor level of 25%, while the other girl could have a normal factor level of 84%.
“The reason this could happen is called ‘lyonization.’ The process is named for the scientist who first discovered it, Mary Lyons,” Dr. Koerper says.
“In every cell of her body, a female has two X chromosomes* — one from her mother and one from her father. A male, on the other hand, has only one X chromosome in each cell, from his mother. As the female fetus develops, one of the X chromosomes in each cell goes inactive. It’s random whether it is the normal X chromosome or the defective X chromosome that goes inactive.
“In this example, both of these girls would get from their father the same X chromosome that
Women Can Have Hemophilia!
By Valerie Hansen, Contributing Writer
* P L E A S E S E E G L O S S A RY O N PA G E 1 4 .

14 15Q U E S T M A G A Z I N E | M A R C H 2 0 1 4
lacks the instructions for making factor VIII. In one twin, more of the defective X chromosomes would remain active. This would result in a low factor VIII level. But in the other twin, more of the normal X chromosomes would remain active. This would produce a higher factor VIII level. Both girls would be carriers, but only one would have a bleeding disorder.
“That is why it is important to distinguish between genetic designation and clinical diagnosis,” Dr. Koerper says. “The twin with the low factor level would need treatment. Her sister would not.”
THE BOTTOM LINEThe sooner girls get tested for a bleeding disorder, the more normal their lives can be. For females born into a family with a history of a bleeding disorder, early testing is advised by experts such as Dr. Koerper. For others, it might not be as simple. For instance, many women with bleeding disorders don’t show any signs of bleeding problems until they start having periods. (Women with untreated bleeding disorders can have periods lasting 10 to 14 days.) Therefore, they may not have any reason to get tested before they start menstruation.
In addition to heavy periods, another possible sign of a problem is frequent bruising. Dr. Koerper encourages females with either of these symptoms to get tested. For any females who decide to get tested, timing is important.
“It is important to be tested at the right time. This means during day one or two of the woman's period," Dr. Koerper says. "It also means at a time when the woman is not stressed or pregnant. This is because in both of these situations, a woman's factor VIII level will be higher due to the effect of hormones. This is especially important for females with a family history of hemophilia A.”
Testing at the right time is important for two main reasons. First, an incorrect diagnosis can put the woman’s health at risk. Second, it can affect whether an insurance company will pay for factor concentrate.* If a bleeding disorder is
not diagnosed because the woman is tested at a time when her factor level is higher, the insurance company may not cover factor concentrate.
The earlier a woman or girl is tested, the better she and her family will be able to manage her bleeding disorder. If a female suspects she has a bleeding disorder, she should seek out an HTC. Hematologists at HTCs have experience diagnosing bleeding disorders. Other hematologists may not accept the fact that women can have hemophilia. (To find an HTC, visit the website for the Centers for Disease Control and Prevention at: www.cdc.gov/ncbddd/hemophilia.)
A CHANGING FUTUREFortunately, experts such as Dr. Koerper and others in the bleeding disorder community are changing how women with hemophilia are viewed. With their help, treatment of these women may soon be as accepted as it has always been for males. In the meantime, women need to be aware of possible symptoms. They also need to be advocates, for themselves as well as for other females in their family.
† Aldridge, S. The carrier barrier. HemAware magazine, National Hemophilia Foundation. www.hemaware.org/story/carrier-barrier. Published 7.12. Accessed 1.16.14.
*Glossary
» Adrenaline (epinephrine): A hormone in the body that is secreted in times of stress. It can cause the factor VIII level to rise.
» Factor VIII and factor IX: Proteins in the blood that help with clotting. Missing or low levels of factor VIII cause hemophilia type A. Missing or low levels of factor IX cause type B. (Most people with hemophilia have type A.)
» Factor concentrate: A commercially prepared factor product that is used to treat bleeding disorders.
» Hematologist: A doctor who treats blood diseases.
» Hemophilia: A hereditary disease in which one of the clotting factors in a person’s blood is lower than normal. This makes the blood less able to form a clot.
» Hemophilia treatment center (HTC): A healthcare center for people with bleeding disorders. HTCs are funded by the federal government. They are located throughout the country. HTCs have specialists who are trained in the diagnosis and treatment of people with bleeding disorders. These specialists include hematologists, nurses, social workers, and physical therapists.
» Prophylaxis: Treatment to prevent bleeds in people with a bleeding disorder. Prophylaxis often consists of factor treatments on two or three days of the week. This starts at an early age, before frequent bleeds have occurred. Prophylaxis helps prevent sudden joint bleeds. It can also help prevent joint disease.
» X chromosome: A structure within cells that carries genes. X and Y chromosomes determine a person’s gender. Women have two X chromosomes, and men have one X chromosome and one Y chromosome. In hemophilia A and B, the damaged chromosome is always the X chromosome.
Today, there are increasing numbers of resources for women with bleeding disorders. Below are several websites that provide information you may find helpful. Also included are links to articles in HemAware, the magazine of the National Hemophilia Foundation.
• Victory for Women with Blood Disorders (National Hemophilia Foundation) www.victoryforwomen.org
• Foundation for Women & Girls with Blood Disorders www.fwgbd.org
• The Hemophilia Federation of America (HFA) www.hemophiliafed.org
• Centers for Disease Control and Prevention — Blood Disorders in Women www.cdc.gov/ncbddd/blooddisorders/women
• The American Thrombosis & Hemostasis Network www.athn.org
HemAware Magazine (National Hemophilia Foundation)www.hemaware.org/women
• “The Carrier Barrier: Women Push for Mild Hemophilia Diagnosis” www.hemaware.org/story/carrier-barrier
• “Mild Hemophilia: Symptoms Don’t Often Surface Until Major Surgery or Trauma” www.hemaware.org/story/mild-hemophilia
• “Pregnancy Planning for Carriers: Steps to Take for a Safe Pregnancy and Delivery” www.hemaware.org/story/pregnancy-planning-carriers
With this listing, we do not endorse these organizations or information they may offer. We strongly suggest that you discuss any information you receive from these organizations with a qualified professional. Please do so before making any changes in your healthcare, insurance, coverage, or home care provider.
RESOURCESWEB
W O M E N C A N H AV E H E M O P H I L I A !
16
Bleeding Disorders Magazine
© 2014 Coram LLC | Quest is a publication of Coram
A P U B L I C A T I O N O F
twitter.com/coramhc youtube.com/coramhealthcare facebook/coramhemophilia
Follow us online!