Embed Size (px)
Citation preview

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
1
Anesthesia Clinical Tutor and Calculator Version 3.0/4.0
Tutorial
PPC/PALM/iPhone
Please refer to the website for iPhone information
All screens have “Help” buttons that explain in detail the screens details and science
behind the screen.
GASSHEAD LLC PO Box 172
Rollins, MT 59931

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
2
ACKNOWLEDGEMENTS ......................................................................................................................... 5 INSTALLATION AND ACTIVATION OF ACTC .................................................................................. 7 ANESTHESIA CLINICAL TUTOR AND CALCULATOR (ACTC)..................................................... 9
Quick Start ...................................................................................................................... 9 PATIENT DATA SCREEN....................................................................................................................... 10 SNAP SHOT ............................................................................................................................................... 14 AIRWAY..................................................................................................................................................... 15 ON AIRWAY SCREEN............................................................................................................................. 15
ETT Chart ..................................................................................................................... 15 LMA Chart – (courtesy of LMA North America, Inc)[6] ............................................ 16 Mallampati screen......................................................................................................... 18 LEMON screen ............................................................................................................. 18 Cuff vs. Uncuffed.......................................................................................................... 20 Axes screen ................................................................................................................... 20 Difficult Mask............................................................................................................... 21
FLUID SCREEN ........................................................................................................................................ 22 TOTAL FLUID BREAKDOWN............................................................................................................... 22
Intraoperative variability and fluids.............................................................................. 23 Fluid Calculations in ACTc .......................................................................................... 24
BLOOD SCREEN ...................................................................................................................................... 25 COAGULATION AND RESUSCITATION........................................................................................... 31 INHALATIONAL SCREEN ..................................................................................................................... 32
Understanding AGE Adjustments in MAC requirements. ........................................... 33 Common Terms ............................................................................................................ 34 Gasshead’s findings on CSDT...................................................................................... 36
50% CSDT................................................................................................................ 37 80% CSDT................................................................................................................ 38 90 & 95% CSDT....................................................................................................... 39
General Notes................................................................................................................ 40 Contraindications .......................................................................................................... 40 Nitrous Oxide................................................................................................................ 40 Isoflurane ...................................................................................................................... 41 Sevoflurane ................................................................................................................... 42 Desflurane ..................................................................................................................... 43 Enflurane....................................................................................................................... 43 Halothane ...................................................................................................................... 44 Factors Affecting MAC ................................................................................................ 44

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
3
ACTc Application of MAC ......................................................................................... 46 AGE MAC CAL ........................................................................................................... 47 AGE ET CAL ............................................................................................................... 49
3D ANATOMICAL FIGURES ................................................................................................................. 50 SPINAL ....................................................................................................................................................... 50
Tetracaine...................................................................................................................... 51 Bupivacaine................................................................................................................... 52 Lidocaine 5% in 7.5 Glucose ........................................................................................ 52 Procaine 10% ................................................................................................................ 53 Ropivacaine................................................................................................................... 53
SPINAL OPIATES..................................................................................................................................... 54 Fentanyl......................................................................................................................... 55 Sufentanil ...................................................................................................................... 55 Morphine....................................................................................................................... 55 Meperidine .................................................................................................................... 55
EPIDURAL ................................................................................................................................................. 55 Determination of Dose and Spread ............................................................................... 56 Redosing ....................................................................................................................... 56 Chloroprocaine.............................................................................................................. 57 Lidocaine....................................................................................................................... 57 Bupivicaine ................................................................................................................... 57 Etidocaine ..................................................................................................................... 58 Mepivacaine.................................................................................................................. 58 Ropivacaine................................................................................................................... 59 Prilocaine ...................................................................................................................... 59
EPIDURAL OPIATES............................................................................................................................... 60 DRUG SCREEN ......................................................................................................................................... 60 MALIGNANT HYPERTHERMIA SCREEN ......................................................................................... 64
Dose calculations .......................................................................................................... 64 VITAL STATISTICS................................................................................................................................. 65
Pediatric outpatient considerations: .............................................................................. 66 LABORATORY VALUES ........................................................................................................................ 67
PH/ETCO2/K calculator ............................................................................................... 68 SETTINGS SCREEN................................................................................................................................. 70 TROUBLE SHOOTING AND QUESTIONS .......................................................................................... 71
Q: On a PALM installation, I do not see the ACTc icon only the GASSHEAD icon.. 71 Q: I did not receive an email confirmation of my purchase ......................................... 71

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
4
Q: (PPC) When changing some screens, sometimes I have a portion of a previous screen still present or see portions of graphics. Or Program exits unexpectedly. ........ 71 Q: How can I see my account information?.................................................................. 72 Q: The program will not install all the files (PALM) ................................................... 72 Q: How do I see more of the cell in the Snap-Shot and Drug Screen?......................... 72 Q: I have a Palm Device and cannot read all the words in the drug detail box or lab detail Box...................................................................................................................... 72 Q. (PPC) I have a prior installation of ACTc and have errors after install version 3.0. What should I do? ......................................................................................................... 72 Q: I have the old ACTc icon in my program list – How can I get rid of it (usually seen in Windows Mobile 2003)? .......................................................................................... 74 Q: I have the old ACTc icon in my program list – How can I get rid of it (usually seen in Windows Mobile 2002)? .......................................................................................... 74 Q: I noticed that all your Help screens indicate specific references in your Readings Section, is there a main document that this originated or is there a help document available? ...................................................................................................................... 75 Q: What if I change my PDA how do I re-register? ..................................................... 75
READINGS AND REFERENCES............................................................................................................ 76

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
5
Acknowledgements The development of Anesthesia Clinical Tutor and Calculator represents an amalgam of a sincere desire to combine my experience and understanding of anesthesia science, a passion for education, and a bit of an obsession with computers and small technological devices. Deepest thanks to my family, especially my wife Cindy, whose patient encouragement was priceless and has kept my focus keen. Many thanks to my friends and colleagues at Sacred Heart Medical Center, Spokane WA, who greatly contributed by reviewing/editing my supporting data and providing some very thoughtful insight. Special recognition and thanks to these who took there valuable time to provide written feedback or consultation:
• Jeffrey Burgan, MD, staff anesthesiologist • Mehran Khosravi, CRNA, MAE • George Momany, MD, staff anesthesiologist specializing in pain medicine • John G. Weisbrod, CRNA, MAE – Clinical Director – School of Anesthesia,
Gonzaga University Thanks also to all of our worldwide field testers (US, Middle East, and Europe) Special recognition to Dr. Dan Clark, CA-2, University of Arkansas. iPhone
• Justin Aden, MD • Nicholas Bancroft, SRNA • Micheal Bentley, PhD, CRNA • Hun-Chi Kwok, MD • Francois Hoang, PharmD • Tracie Loscalzo, CRNA • Mike MacKinnon, CRNA • Ray Howard, CRNA • John Weisbrod, CRNA
Thanks also to my development team at Endeavour Software Technologies. Avinash, Jayandra, Nidhi, Jesus, Youvraj, and Madhan (PALM/PPC team); Lakshmi, Narayana & Alok (iPhone Team)…All of you are miracle workers. It was a pleasure working with such talented individuals.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
6
Finally, thanks to all the researchers and educators in anesthesia whose endeavors keep enhancing our understanding to this wonderful and challenging field. It sharpens our practice, tempers our vision, and ultimately improves the daily care of our patients. Anthony T Young

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
7
Installation and Activation of ACTc Iphone: Please refer to the website for detailed information. The iphone version is only available via the iTunes store. PALM/PPC Uninstall all previous versions from both your hand held and Desktop PPC users must install via their Active sync window Goto -> Tools-> Add/Remove->Highlight Gasshead/ACTc->Click remove
Confirm uninstallation on your PDA Goto settings-> Systems-> Remove Programs Remove Any Gasshead or ACTc programs
PALM Delete 2 files – ACTc and Gasshead
1. Download and install from http://www.gasshead.com PPC Users (Windows) http://www.gasshead.com/Installers/Trial_versions/ACTc_TrialVersionPPC.exe Palm Users (Windows) http://www.gasshead.com/Installers/Trial_versions/ACTc_TrialVersion.exe PPC Users (MAC) http://www.gasshead.com/Installers/Trial_versions/ACTcPPCApplication.tar Palm Users (MAC) http://www.gasshead.com/Installers/Trial_versions/ACTcPalmApplication.tar 2. Trial the program to your satisfaction 3. Purchase ACTc at this page: https://www.gasshead.com/purchase.aspx
Complete the payment form completely – at a point you will be asked for the Product ID
A. Start your PDA - Start the ACTc program - Click on the “Purchase button” to obtain the Product ID and type it in Exactly on the on-line form - Click OK on your PDA Once the process has been confirmed and completed you will be given an Activation Code.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
8
To Activate: - Click on the “Activate” button on your ACTc start up screen and type in the activation code exactly as provided
If you have a promotion code, goto to this page: https://www.gasshead.com/frmPurchaseViaPromo_Key.aspx
- Input the promo code provided on your gift certificate (case sensitive) - Complete the form completely – at a point you will be asked for the Product ID A. Start your PDA
- Start the ACTc program - Click on the “Purchase button” to obtain the Product ID and type it in - Exactly on the online form - Click OK on your PDA Once the process has been confirmed and completed you will be given an Activation Code.
To Activate: - Click on the “Activate” button on your ACTc start up screen and type in the activation code exactly as provided

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
9
Anesthesia Clinical Tutor and Calculator (ACTc)
ACTC is a collection of tools and is not meant to be all inclusive or comprehensive. It is meant to as a adjunct to existing anesthesia references. For all good practitioners in training will utilize a number of sources – both in written form (references, research publications, scholarly articles, etc…) and by clinical guides (attendings, clinical faculty, and peers). ACTc is built to mimic clinical thought flow and provide an interactive feedback on data each anesthesia provider inputs. Each patient has specific presentation that must be accounted, Hence after a thorough focused anesthesia patient assessment each clinician mentally “sets up” by determining the anesthetic plan and operative needs to ensure the safest course. This encompasses accounting for patient variables and perioperative needs:
• Pathologic considerations and anesthetic implications • Fluid and Blood requirements • Specific operative demands on patient stability
o Possible contingent actions for issues related to operation and or anesthetic technique
• Pharmacologic intervention • Monitoring requirement • Positioning implications • And post operative needs / concerns
Quick Start Starting at the Patient data screen On the Patient data screen, intuitive flow helps one understand “setting up.” 1) Selecting the appropriate “Patient type” plays a large part in a multitude of calculations: estimating blood requirements, fluid volumes, drug calculations, airway needs, etc…hence select the appropriate patient type: Newborn (<30 days) infant (1 – 12 months), Child, Adult Male or Female, and Geriatric Male or Female.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
10
2) For Every Anesthetist the following inputs are natural and establishes the base for many calculations and helps anticipate needs 3) The Snap Shot screen pre-selects common values and drug selections for a multitude of cases. Most importantly, it allows each user to customize each screen for their individual practice styles 4) Finally, based on patient type, airway (ETT or LMA) selections/guides are generated at the bottom 5) For Pediatrics categories, the 50% percentile Vital signs are also shown, separated into age groups and genders 6) Now, in appropriate sections – weight and patient type considerations are now inputted to generate specific calculations as you navigate to these other screens 7) Note – an adult patient type must be selected to review spinal and epidural data.
Patient Data Screen The surgical schedule dictates every anesthetist day. The ability to process and plan the course of that day hinges upon ones ability to properly plan and anticipate surgical demands balanced upon patient presentation and needs. Naturally, one looks at the procedures (which may or may not hint at the patient population you can expect to encounter) and then at the age of your patients. Many times, without meeting the patients, one can delineate some basic core requirements (potential fluid needs, airway needs &
equipment, and minimum drug requirements). This is preemptive to a patient focused assessment.
Figure 1

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
11
On the Patient data screen, it allows you to start intuitively “setting up.” In the following areas. 1) Patient type plays a large part in a multitude of calculations: estimating blood requirements, fluid volumes, drug calculations, airway needs, etc…hence select the appropriate patient type: Newborn (<30 days) infant (1 – 12 months), Child, Adult Male or Female, and Geriatric Male or Female. 2) The default value of Hours NPO is 12 (which can be changed). This number is used to help determine NPO deficits on the are determined by the hours NPO multiplied by the 4-2-1 rule
• 4 cc/kg/hr per first 10 kg • 2 cc/kg/hr for each kg between 10 – 20 • 1 cc/kg/hr for each kg 21 and greater[1, 2]
Note: that in pediatric patients with dehydration who cannot tolerate oral re-hydration:
• 40 cc/kg of LR over 1 – 2 hours should be administered (moderate dehydration).
• For severe dehydration, LR or NS made be used. o If skin turgor, alertness, or pulse do not return to normal with the above
dose, an additional dose of 20-40 mL/kg may be given - over 1-2 hours.[3] In Adults with severe dehydration, presenting with hypovolemia
• Rehydration with sufficient fluid to restore mean arterial pressure, heart rate and filling pressure (preload or CVP) prior to induction is advisable.
• If time allows, establishing normal urine output is also advisable.[4] 3) Evaporative Constants are based on degree of exposed or manipulated tissue(s). This hourly estimation varies from source to source but is ultimately up to each provider to determine. A rough guideline that can be used is:
• Minimal trauma (0 – 4 cc/kg/hr Arthroscopic , Laparoscopic, Small incision) • Moderate trauma (4 – 6 cc/kg/hr Hystectomies, Thorocotomy) • Severe trauma ( 6 + cc/kg/hr Bowels, Large Abdominal Cases, Burns, Aortas,
Open Chests, Trauma)[2, 5]
Figure 2
Figure 3

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
12
Based on this, you can select Evaporative ranges from 1 – 15 ml/ kg/hr in ACTc
4) The bottom of the screen provides the user with either LMA or ETT selection information for the specific patient type they have selected. These selection is based on the following criteria:
• LMA (courtesy of LMA North America, Inc)[6]
o Figure 5
ETT selection for Adults & Geriatric are selected based on the following table
Figure 6
• For Pediatric ETT selection is based on a combination of several guidelines. The appropriate selection is automated values are based on the following criteria:
• PALS recommended guidelines up to age 2
ETT Wt or Age ETT Average Dist
Adult Female 6.5 - 7.5 19 - 24 cm Adult Male 7.0 - 9.0 20 - 24 cm Geriatric Female 6.5 - 7.5 19 - 24 cm Geriatric Male 7.0 - 9.0 20 - 24 cm
Figure 4

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
13
Wt or Age ETT Av Dist Laryngoscope Comments Preterm <1.5 GM
2.5 - 3.0 ncuf
8 cm Miller 0 Alt Calculation for MidTrac. Distance, IF < 44 weeks Gest. Age: 6 / KG
Term 3.0 - 3.5 ncuf
9 - 10 cm
Miller 0 - 1, Wis-Hipple 1, Robert Shaw 0
Alt Calculation for MidTrac. Distance, IF > 44 weeks Gest. Age then: 3 x ETT Size
Up to 6 Months
3.5 - 4.0 ncuf
10.5 - 12 cm
Miller 0 - 1, Wis-Hipple 1, Robert Shaw 0
Alt Calculation for MidTrac. Distance, IF > 44 weeks Gest. Age then: 3 x ETT Size
Up to 1 Year
4.0 - 4.5
12 - 13.5 cm
Miller 1, Wis-Hipple 1.5, Robert Shaw 1
Alt Calculation for MidTrac. Distance, IF > 44 weeks Gest. Age then: 3 x ETT Size
2 Years 4.0 - 4.5
13.5 cm
Miller 2, Macintosh 2 Alt Calculation for MidTrac. Distance, IF>44 weeks Gest. Age then: 3 x ETT Size
Table 1[7]
For patients under 2 -3 years of age • FT Infant can take 3 - 3.5 ETT. • Infants 1.5 - 3.5 gm = 3.0 ETT • <1.5 gm a 2.5 mm tube is recommended[8]
o Most NB have an appropriate leak w/ 3.o ETT and can use a 3.5 ETT at a few months of age
o Incorrect selection occurs frequently prior to actual leak tests and is recommended to have one half size below and above accessible & available.
o Leaks less than 10 might compromise adequate ventilation and not protect against aspiration.
o Leaks greater than 30 increases the risk of post-extubation stridor and potential for ischemic damage to the mucosa[9]
• • For children above 2 years of age the following calculation is used: Tube
size for children = 4 + Age (years) /4)[7, 10] •
Other alternatives for pediatric tube selection:
Penlington indicated that for children less than 6 years:
o Age (years)/3 + 3.75 o 6 and greater : Age(years)/4+ 4.5[10, 11]
• The easiest technique but is often unreliable is the use of the little finger to determine internal diameter of which ETT to be used. [12]
• Pediatric Depth determination

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
14
• If > then 44 weeks gestational age use the following calculation • 3 x ETT size • If <44 weeks gestational age: 6 / KG[7] • An alternative to this is : 12 + Age (years)/2[2, 7, 11, 12]
Snap Shot
All clinician have specific preferences for specific cases.
ACTc allows for each user to build their own “Snap Shot”
New Profiles are entered using the drop down arrow new to “Standard”
Then desired data is selected and positioned on the screen using the “Up,” “Down,” and “Remove” buttons.
If a change is desired in a specific Profile – Select the Profile and click on “Customize This Screen”
o Add the desired data by selecting the “Add” button and its position on the screen is controlled by highlighting it and clicking up or down.
o Click “back when done

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
15
Airway Above all, anticipate and be prepared. A notable quote from Morgan and Mikhail is “It must be stress that because no examination technique is fool-proof and the signs of a difficult airway may be subtle…always be prepared for unanticipated difficulties”[1] Airway concerns are central to any anesthetic. Primary assessment and history assists the clinician to proactively plan for airway concerns. ACTc provides core understanding in airway management and assessment.
On Airway Screen Two Menu selections are available. Scrolling the buttons at the bottom right and the “EVAL” button allows you to review the following data:
ETT Chart ETT
Wt or Age ETT AvDist 1 kg 2.5 ncuf 7 cm 1.5 kg 3.0 ncuf 7.5 cm 2 kg 3.0 ncuf 8 cm 3 kg (preterm) 3.0 ncuf 9 cm 3 kg (term) 3.0 ncuf 10 cm 6 -12 mon 3.0 ncuf 11 cm 12 - 18 mon 3.5 ncuf 12 cm 18 -36 mo 4.0 ncuf 13 cm 3 - 5 yr 4.5 ncuf 14 cm 5 - 6 yr 5.0 cuf 15 cm 6 - 8 yr 5.5 cuf 16 cm
Figure 7

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
16
ETT Wt or Age ETT AvDist
8 - 10 yr 6.0 cuf 18 cm 11 - 12 yr 6.5 cuf 18 cm Adult Female 6.5 - 7.5 19 - 24 cmAdult Male 7.0 - 9.0 20 - 24 cmGeriatric Female 6.5 - 7.5 19 - 24 cmGeriatric Male 7.0 - 9.0 20 - 24 cm
o
LMA Chart – (courtesy of LMA North America, Inc)[6]
o • Difficult Mask considerations • Cuffed vs. Uncuffed • Axis Alignment Diagrams • LEMON Assessment Guide • Mallampati Diagrams
The following table is also added to the Pediatric Vital Signs table
Variable NB 1 yo 3 yo 5 yo 12 yo Resp. Rate 40 - 60 20 - 30 18 - 25 18 - 25 20 TV (cc/kg) 10 - 12 10 - 12 10 - 12 10 - 12 10 - 12
Table 2[1]
If the “?” next to the airway is clicked then the following is shown:

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
17
Pediatric ETT selection is as follows: PALS recommended guidelines up to age 2 (AHA) Tube size for children = 4 + Age (years) /4 (AHA)[7, 10]
Another Alternative by Penlington for children less than 6 years[10, 11]: Age (years)/3 + 3.75 6 and greater : Age(years)/4+ 4.5
The easiest technique but is often unreliable is the use of the little finger to determine internal diameter of which ETT to be used.
Pediatric Depth determination
If > then 44 weeks gestational age use the following calculation 3 x ETT size
If <44 weeks gestational age: 6 / KG[7]
An alternative to this is : 12 + Age (years)/2[2, 7, 10, 11] Another alternative:
• ETT tip should be advanced until the tip is positioned at least 2 cm
below vocal cords o Basic Rules:
1 kg = 7 at lips 2 kg = 8 at lips 3 kg = 9 at lips 4 kg 10 cm at gums for mid tracheal placement
• Or try a main-stem approach where tip is advanced until BS can only be heard only in right lung fields (diminished on the Left) and then pull ETT back 2 - 3 cm until equal breath sounds are heard
• Optional: CXR • Generally: distance = 30 times internal diameter of ETT should be
distance at the teeth[9]
For nasal distances, Add 2 - 3 cm for nasal depth[1]
If the “?” next to the LMA section is clicked then the data from fig 6 is shown

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
18
Mallampati screen Based on Mallampati et determination of visualization of specific structures and modified by Samsoon and Young[13]. Refer to figures below for graphical guide.
The patient sits upright with the head in the neutral position.
The patient is asked to open the mouth as widely as possible and to protrude the tongue to the maximum.
The observer sits opposite at eye level and with a light source inspects the pharyngeal structures.
Limited Neck Mobility <35 degrees Obesity Anatomical deformities secondary to congenital issues, trauma, disease, or
surgical history Small oral opening[13-15]
LEMON screen The L.E.M.O.N method, as described by Ron Walls, is another method for assessing potential airway issues but can be difficult to use in certain patient presenting for resuscitation. [16-18]
Look externally Evaluate the 3-3-2 rule
Figure 8 L.E.M.O.N. by Walls[17]/Images by Gasshead

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
19
Mallampati Positioning First
o Figure 9 Images by Gasshead Instructions by Mallampati[15]
Figure 10 Images by Gasshead Instructions by Mallampati[15]
Obstruction Neck mobility
Figure 11 L.E.M.O.N. by Walls[17]/Images by Gasshead

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
20
Cuff vs. Uncuffed
Pediatric Peak Pressures and use of Cuffed vs. Uncuffed ETT:
Avoiding tracheal damage by proper selection of ETT and monitoring peak airway pressures in children is paramount. Though no source in complete agreement, a small air leak at peak inflation pressure (PIP) of 20–30 cm H2O should be acceptable (which can vary based on provider, pulmonary compliance, and procedure). Also in flux is the issue of cuffed vs. uncuffed ETT. [12, 19, 20] Traditionally, it has been the norm to recommend the use of cuffed ETT for children older than 8 years old.. But even this is being challenged. Gavin et al. is quoted “…this advantage (referring to un-cuffed tubes) does not hold for ventilated patients, for whom ventilator settings can be adjusted to provide optimal airflow. Longer duration of intubation and a poorly fitted ETT are risk factors for mucosal damage, whether the ETT is cuffed or uncuffed.” [21]
Axes screen “?” brings up the following text The concept of aligning the “Three Axes” via the sniff position has been institutionalized in all practitioners thinking. Yet recent studies have brought to question it’s true ability to align themselves on a single plane and or improve actual glottic view. At minimum, direct laryngoscopy requires force, manipulation (active position changes to head/neck), and or varying degrees of the Sellick manoeuvre (cricoid pressure). Regardless, an appreciation of the applied geometry helps in visualizing what we are attempting by direct manipulation. Proper positioning is a vital part of a dynamic process. In practice, it is extremely helpful to appreciate and visualize anatomical changes that can help us achieve efficient airway placement that minimizes its impact on our patients.[16, 22-24]
Figure 12 Drop Down List

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
21
Figure 13 Axis Reference[25]
Difficult Mask Langeron O. et al in 2000 was able to identify 5 independent variables that help identify potential difficult mask ventilation.
1. Presence of a beard 2. Body-mass index greater than 26 kg/m2 3. History of regular snoring 4. Edentulousness 5. Age older than 55
Interestingly, subjective evaluation identified only 17% of the aforementioned variables. Langeron found that if a patient was difficult to mask, there was also a 4 – 12 time potential for a difficult / impossible intubation, respectively.[26] Magboul condensed the finding with the word OBESE
Obese Bearded Elderly Snorers Edentulous[16]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
22
Kheterpal, S. et al found similar findings adding Mallampati classification III or IV, age of 57 yr or older, severely limited jaw protrusion, abnormal neck anatomy, & sleep apnea also contributed.[27]
Fluid Screen Important considerations of perioperative fluid replacement guidelines as automated in ACTc are as follows. The fluid screen provides a break down of the different values consisting of the hourly totals for fluid administration. It does not however account for blood loss. The screen layout is self explanatory with an hourly total running left to right at the middle/bottom of the screen. Scroll down for an explanation on the hourly totals.
Total Fluid Breakdown Total fluids required for the anesthetic are as
follows:
• NPO deficit replacement
• Maintenance Fluid
• Evaporative Losses
• and Blood Replacement. (* not account for in this screen) [1]
The Hourly Maintenance Fluid will calculate the values using the formula.
Calculated using WT in KG
For KG 1 – 10 kg add 4cc for each kg
For KG 11 – 20 kg add 2cc for each kg
For KG > 21 kg add 1cc for each kg[5]
Figure 14 PPC Fluid Screen

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
23
The Hourly Evaporative Rate will be calculated as
Calculated by KG x User Defined Evaporative Constants
Evaporative Constants are based on degree of exposed or manipulated tissue(s).
This hourly estimation varies from source to source but is ultimately up to each
provider to determine. A rough guideline to use is:
• Minimal trauma (0 – 4 cc/kg/hr Arthroscopic , Laparoscopic, Small incision)
• Moderate trauma (4 – 6 cc/kg/hr Hystectomies, Thorocotomy) • Severe trauma ( 6 + cc/kg/hr Bowels, Large Abdominal Cases, Burns,
Aortas, Open Chests, Trauma)[2, 5, 28]
The NPO Deficit is calculated by Hours NPO multiplied by Hourly Maintenance
Fluid.
Note: that in pediatric patients with dehydration who cannot tolerate oral re-hydration: • 40 cc/kg of LR over 1 – 2 hours should be administered (moderate dehydration). • For severe dehydration, LR or NS made be used.
o If skin turgor, alertness, or pulse do not return to normal with the above dose, an additional dose of 20-40 mL/kg may be given - over 1-2 hours.[3]
In Adults with severe dehydration, presenting with hypovolemia
• Rehydration with sufficient fluid to restore mean arterial pressure, heart rate and filling pressure (preload or CVP) prior to induction is advisable.
• If time allows, establishing normal urine output is also advisable.[4]
The Total Hourly Fluids is calculated by adding the Hourly Fluids and Hourly
Evaporative Rate
Intraoperative variability and fluids Several preoperative predictors have been identified for intraoperative hemodynamic variability/instability.
• Preoperative mean arterial pressure (MAP) greater than or equal to 110 • Ability of walking distance of less than 400 m (poor exercise tolerance) • Plasma volume less than 3000 cc [29]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
24
• The presence of HTN and use of combined spinal epidural techniques[30] • Pre-existing HTN
o Severe decreases in BP post induction secondary to volume contracted state[28]
• Elderly o Responds to anesthetics with greater degree (compared to younger
patients) of hypotension and blood pressure variations during anesthesia. o Have a higher sympathetic tone resulting in greater degrees of
hypotension. o Anesthesia decreases in vascular resistance, contractility, and heart
rate.[31] Due to the volume contracted state that HTN can have on normal fluid status and the
resulting rapid decrease in BP after an induction of general anesthesia, appropriate fluid
loading can mitigate a very exciting (but unnecessary post induction time) but this must
be balanced with the potential issues of fluid loading in patients with limited cardiac
functioning and renal reserve.
To offset the potential drop in BP post-induction, ¾ o the preoperative deficits compared
to ½ of preoperative deficits should be given to induction.
Fluid Calculations in ACTc In ACTc - there is an option of adjusting for preloading for patients with and without
HTN.
If the Box is checked:
The “Pre Op” Box value is equal to .75 of the NPO Deficit (3/4 of the NPO deficit
should be given prior to induction and the remainder of the deficit given over the next 2
hours in addition to hourly maintenance and evaporative rates
In the “1st Hour” box value is equal to the Value from the “Pre Op Box” + Hourly
Fluid Maintenance + Hourly Evaporative Rate + .125 * the NPO deficit
The “2nd Hour” box value is equal to the Value from the “1st Hour” + Hourly
Fluid Maintenance + Hourly Evaporative Rate + .125 * the NPO deficit

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
25
The “3rd Hour” box value is equal to the Value from the “2nd Hour” + Hourly
Fluid Maintenance + Hourly Evaporative Rate
And in the same way up to 24 hours
And if the user did not checked it than the ongoing picture is
The “Pre Op” Box value is equal to .5 of the NPO Deficit
The “1st Hour” box value is equal to the Value from the “Pre Op Box” + Hourly
Fluid Maintenance + Hourly Evaporative Rate + .25 * the NPO deficit
The “2nd Hour” box value is equal to the Value from the “1st Hour” + Hourly
Fluid Maintenance + Hourly Evaporative Rate + .25 * the NPO deficit
The “3rd Hour” box value is equal to the Value from the “2nd Hour” + Hourly
Fluid Maintenance + Hourly Evaporative Rate
And in the same way up to 24 hours
Blood Screen Virtually every surgical procedure has a potential for blood loss. Hence each clinician
must be aware of lower thresholds limits and the variables that can impact them, which if
met, will require action. Additionally, open communication about blood replacement
strategies with the surgeon will help clarify perioperative needs and postoperative
management / follow-up.
Steps for preparation:
1. If high risk or probability for transfusion – order blood ahead of time (anticipate )
a. The amount is based on starting lab values and anticipated intraoperative
loss
b. Should include an appreciation/assessment of current anticoagulant state.
2. Determine Estimated Blood volume (EBV - see below)

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
26
3. Determine starting and ending points (HCT) for your patient (based on recent lab
values if possible)
o Trigger Points for transfusions are controversial and a universal point is
generally not recommended.[5]
o General recommendations and Observations[5, 28, 32]:
In healthy patients, a HCT of 21 – 30% (Hemoglobin 7 –
10 g/dl) can be tolerated
Transfusions for hemoglobin greater then 10 g/dl are rarely
indicate
The risk for allowing low hemoglobin of between 6 – 10
g/dl must be weighted against potential complications of
inadequate oxygenation
For HCT Under 21% - Cardiac output increases to maintain
oxygen delivery.
• This can be detrimental to elderly patients hence
patients with cardiopulmonary alterations have
higher minimums
• Generally, a minimal HCT of 30% is acceptable
o Some useful guidelines for potential “trigger points” for
transfusion[5]:
If Blood loss greater than 20% of blood volume
If Hemoglobin is less than 8 g/dl
If Hemoglobin is less than 10 g/dl with major disease
(cardiopulmonary)
If Hemoglobin is less than 12 g/dl in a ventilator dependent
patient
4. Calculate Allowable Blood Loss (ABL- see below)
5. As blood loss occurs, replace by crystalloids or colloids (based on surgical
evolution / needs, patient response to loss, & availability)

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
27
o 3cc crystalloids per 1 cc Blood loss
o 1 cc colloid per 1 cc Blood loss
o Predetermine (patient and case specific) at which loss threshold you will:
o replace with strictly crystalloids
o move on to colloids
o order/set up blood/ order confirming lab studies
o transfuse blood
o send coag studies
Points to ponder
There is an ongoing controversy on set guidelines for the use of colloids
vs. crystalloids with supporting evidence with both and wet vs. dry
strategies with issues surrounding[33-48]:
o Cardiopulmonary functioning
o Hormonal Cardiac responses
o Postoperative symptomatology
o Time to discharge
o Wound healing
o GI functioning
o Acidosis (Hyperchloremic)
Hence, review of current literature is
highly recommended.
A suggested strategy would be to
transfuse to a 20% loss with a
combination of crystalloid (LR) and
colloids
• Exception in Bowel
Surgery where limiting Figure 15 Blood Screen

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
28
fluids is advisable[28, 49]
• See above for possible trigger point strategy.
On the Blood Screen, a number of blood volume calculations are found using the
following:
The value of Starting HCT will be by Default of 40 (changeable).
The value of Ending HCT will be by Default 30 (changeable).
EBV (Estimated Blood Volume). Is determined by patient category * by the
Patient’s weight (in KG). Categories as follows:
• If Newborn then KG multiplied by 90
• If Infant then KG multiplied by 85
• If Child then KG multiplied by 80
• If Adult Male then KG multiplied by 75
• If Adult Female then KG multiplied by 70
• If Geriatric Male then KG multiplied by 70
• If Geriatric Female then KG multiplied by 65
Estimating Blood loss, as accurately as possible, helps guide many clinicians. This
does not replace confirming loss with lab tests and constant discussions with the
surgeon about his/her anticipated ongoing surgical losses. In addition to loss in the
suction canisters remember that if saturated:
Dry sponges (4 x4) holds @ 10 cc of blood
Dry Ray techs @ 10 – 20 cc of blood
Dry Lap sponges @ 100 cc of blood[28]
ABL (Allowable blood loss) will be calculated using the formula: ABL= EBV x
(Starting HCT- Ending HCT) / Starting HCT

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
29
Figure 16
Possible Current HCT will be calculated using the formula • Possible HCT = Starting HCT – (starting HCT x (Current Blood Loss / EBV))
Figure 17[2]
Incremental Loss
• Based on the above calculation but when subtracted from the starting HCT
it shows the increment of HCT decrease for that Current Blood Loss at a
starting HCT compared to the EBV
• Equation = Starting HCT – Possible Current HCT
• Most Clinicians track EBL in increments (i.e. for Adults: 50, 100, 200,
300 ml – for it is hard to account for every ml of blood loss)
• Try 50, 100, 200, or 300 as values in “Current blood loss “ in the
equation above to see what HCT change would occur at the
different ml of blood loss
• Pediatric values are significantly less and allowances must be
made in light of their smaller volumes
• Tracking at 100 plus increments for blood loss would not
be recommended
Whole Blood CC is calculated by the formula:
Whole Blood CC = EBV x ((Transfuse to HCT – Current HCT) / 35)[50]
• Where 35 is the average HCT of the Whole blood
• Where Transfuse to HCT is always greater than Current HCT

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
30
Whole Blood Units needed = Whole Blood in cc divided by 500
• Where 500 = average volume in one unit of whole Blood
PRBC cc needed will be calculated by the formula
PRBC cc = EBV x ((Transfuse to HCT – Current HCT)/70)[50]
• Where 70 is the average HCT of the Whole blood
• Where Transfuse to HCT is always greater than Current HCT
PRBC Units = PRBC in cc divided by 300.
• Where 300 = average volume in one unit of whole Blood
• The usual 250-300 ml unit of red blood cells (RBCs) has a
hematocrit of 55-80%, with some platelets and/or white cells
removed during processing.
Total Loss Calculations
• Hypothetical needs based on necessary amount of blood products needed
to maintain a patient at a specific HCT
• Transfusion must be guided by patient needs/safety, operative
demands/evolution, & current/verified lab results – all to treat and
or prevent alterations in 02 delivery and the issues that arise.
• PRBC in cc
• EBV x ((Desired maintenance HCT)/70)
• where Desired maintenance HCT =
minimum HCT you want to maintain in an
active loss situation
• 70 is the average HCT concentration of
PRBC
• In ACTc Type in Your Desired HCT and then Type
in “0” in the Current HCT
• PRBC in units
• (EBV x ((Desired maintenance HCT)/70))/300

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
31
• Where 300 is the average volume of a unit
of PRBC
• Whole blood uses the same calculations but the maximum
HCT is limited to the maximum HCT available in the WB
– where the average is 35%
Figure 18 Transfusion
Coagulation and Resuscitation It is vital to understand the processes of possible coagulation issues that can arise with large transfusions (6 – 10 units of PRBCs) in combination with the duration of hypotension or hypoperfusion[5]. Hence, ACTc has provided some general guides and information about the calculations for Platelets, FFP, and Cryoprecipitate. Platelets[5, 32, 51]
Rarely indicated for Platelet counts greater then 100 x 109/L
Usually indicated for levels less than 50 x 109/L Can be indicated regardless of normal count values
Figure 19 Resuscitation Screen

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
32
in the presence of known platelet dysfunction and microvascular bleeding Dosed at One unit per 10 kg of body weight to see an increase 40 - 50 k
FFP[5, 32]
Used in reversal of warfarin therapy Correction of known coagulation deficiencies - in presence of increased (>1.5) PT
or PTT Used in correction of microvascular bleeding in presence of increased (>1.5) PT
or PTT For correction of microvascular bleeding secondary to coagulation factor
deficiency in patients transfused with more than one blood volume and when PT and PTT cannot be obtained in a timely fashion
Massive blood transfusions – rarely and only when factors V and VIII are less than 25% of normal and increased (>1.5) PT or PTT
Dosed to achieve a minimum of 10% increase in plasma factor concentration o 10 – 15 cc/kg
One CC/kg increases factors by 1% o 5 – 8 cc/kg for coumadin reversal
Contradicted for augmentation of plasma volume or albumin concentration Also used In cases of ATIII deficiencies in which heparinization is need for
coronary pulmonary bypass Cryoprecipitate[52]
Contains concentrated factor VIII, XIII, von Willebrand, fibrinogen, and fibronectin
Indicated in o Hypofibrinogenemia - < 100 mg/dl o von Willebrands disease o Hemophilia A – when factor VIII is not available
Dose o One unit per 7 – 10 kg
will increase fibrinogen 60 -70 mg/dl Furthermore, ACTc has provided coagulation issue tables where the use of the Coagulation deficiencies and DIC tables granted by Elsevier publication.
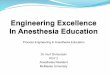
Inhalational Screen “Anesthetic solubility is a prime determinant of recovery from anesthesia” – Eger EI II Apart from TIVA (total intravenous anesthesia) techniques, General Anesthesia is generally maintained via the use of inhalational agents. Detailed knowledge regarding

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
33
Using Age MAC and CSDT’s
Age calculations upon MAC multiples, secondary gases, and temperature, allows the clinician to appreciate the age specific MAC ranges where
amnesia may occurs, movement may be affected, and hemodynamic impacts may be seen. By
applying age considerations, ET agent numbers are fluid and change over the MAC continuum as
secondary gases are added/removed or temperature decreases. Each individual
practitioner needs to determine what ET is best suited for their patients needs.
CSDT’s help the clinician understand the impact of operative time, individual lambda, and specific decrements on the elimination of specific agents.
Example: The case is coming to completion.
Isoflurane is being used with a intraoperative ET of 0.91 for a 3 hour case, and the clinicians goal
is to be below MAC awake for extubation (which for a 40 y.o. pt. is less then 0.4)
The decrement required to go from .91 to less then .4 is 65% - which is takes approximately 5
minutes for this to occur.*
*Using computer stimulations with fixed CO, high flows, flushing the circuit, and turning off
the agent dial.
the pharmacokinetics/dynamics is vital for every practitioner to properly administer these agents. [28, 53-60]
• A Limited summary follows & it is advisable that all practitioners to be well versed in all aspects of the following agents.
• MAC values listed for adults 30 – 55 years of age (40 average) at 1 atm.
Understanding AGE Adjustments in MAC requirements. In understanding the nuances of MAC, ACTc assists in showing the clinician the calculated range of the effects of age on the MAC continuum – from MACawake, MAC, and MACBAR. Based on age calculations of Nickalls, Mapleson [58, 61], Eger’s Temperature variations [56, 62-65], and Eger’s and Baileys Context Sensitive Decrement Time Considerations[53, 66-69]. It is also worth noting that Age adjustments are considerations, and not definitive in determining proper intra-operative end tidal concentrations. Each patient presents differently - Age plays a significant part but in no way does it completely describe or define an absolute intraoperative end tidal level. The MAC continuum shows the implications of specific ET concentrations and the physiologic effects – specifically amnesia, movement, and blocking of adrenergic responses. Using current published research, ACTc interactively shows the effects of increasing age on the continuum. Additionally, the clinician can also see the effects of decreasing temperature on MAC requirements. The inhalation screens show these interactions instantaneously to enforce fundamental MAC teaching. Addition to age adjustments but the addition of MAC multiples can also be seen. The addition of the Context Sensitive Decrement Times – utilizes the principles of solubility and time in circuit described by Eger and Bailey[53, 66, 67]. ACTc allows the practitioner to compare various agents (with various solubility) and select duration of the anesthetic vs the amount of decrement desired. This action alone helps the user

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
34
anticipate inhalation elimination. ACTc highly recommends recreating Eger’s research using GASMAN software to completely appreciate CSDTs[66, 70]
Common Terms o At the lower end of the MAC continuum, MACAwake: the average
concentration permitting voluntary response to commands Memory is usually lost at this point MACAwake is approximately 0.34 MAC for Desflurane, Isoflurane,
and Sevoflurane[56, 71] MACAwake for N20 and Halothane it is 0.5[56] MACAwake /MAC ratio is maintained with advancing age[56] 0.1 MAC is the point where cognition is affected (slight)[54] In reviewing the literature, BIS monitoring has helped validate this
point. • In a study by Wong[72], where intraoperative ET% of
isoflurane (in combination with Fentanyl) was adjusted to BIS values of 50 -60, the average ET% was .39 =/- .05 with no evidence of recall
• If adjusted for age of the participants, the MAC Awake ET value for isoflurane is .33% (if used in combination with Fentanyl)
• Furthermore, In a study of fast tracking with Desflurane vs Propofol using BIS, Song provided the following data
o ET% of Desflurane of 2.7% (with N20 at 65% & Fentanyl)[73]
o If adjusted for age of the participants, MAC awake in this study = 2.43%
• Worbel looked at Desflurane concentrations below 1 MAC and found similar results
o Where BIS 64-50 corresponded to 2.9 +/-1.3 % when used with remifentanil[74]
• In reference to the definition that memory is lost at this point,, the available BIS studies help validate this very important point.
o MAC: Minimum Alveolar Concentration of an anesthetic that produces immobility in 50% of patients exposed to a painful stimuli
o MACbar: the anesthetic concentration that blocks autonomic/ adrenergic response to incision
Usually resides at the higher end of the MAC Continuum Since MACAwake /MAC ratio is maintained with age, the author
also applies Eger’s assumption to the MACbar /MAC ratio.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
35
o MAC40 : The MAC values at age 40 as expressed by Mapleson Age Adjusted calculation (resulted from meta-analysis of available MAC data)[61]
Halothane: 0.75% Isoflurane: 1.17% Enflurane: 1.63% Sevoflurane: 1.8% Desflurane: 6.6% N20: 104%
o Context-sensitive decrement time (CSDT). CSDT are directly influenced by anesthetic duration and
individual gas solubility; and expressed as time to reach x% reduction once an anesthetic gas is discontinued
• Example o A 50% decrement time is the time required to
obtain a 50% reduction in the ET% Important in considering agent selection and operative
management Using CSDT can help a clinician plan on emergence times (using
80% CSDT) • If starting point upon cessation of inhalational agent is @ 1
MAC or below • Targeting MACawake at emergence in reference to 80%
CSDT has assisted the author in wakeups • Useful since the general goal is responsiveness for
extubation • If cases under 120 minutes, most agents allow the level to
obtained in a short period of time[66] o The authors data shows @ < 12 minutes o This does not include Halothane or Enflurane
95% CSDT is significant for it possibly represent complete clinical recovery.[66]
CSDT are influenced significantly by: percentage of desire reduction, duration of inhalational exposure, and solubility of the inhalational agent.
• Generally, the impact of low solubility is greatest (faster elimination) in higher decrement times (>90%) in cases longer then 60 – 90 minutes.
• The major differences in the rates at which desflurane, sevoflurane, isoflurane, and enflurane are eliminated occur in the final 20% of the elimination process.[53]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
36
• Higher required CSDT (greater then 90%) is dependent on gas solubility
o The lower the solubility the shorter the time required to obtain a specific CSDT
Studies by Both Eger and Bailey show that regardless of duration show little difference in 50% decrement times for all agents[53, 66]
• Bailey used mathematical calculations vs. Eger’s use of Gas Man software
Eger and Bailey differ in some points of their findings • Bailey indicates that at 60 minutes the 80% decrement
times for Sevoflurane and Desflurane are similar; while Enflurane and Isoflurane start diverging significantly – reflecting those agents solubility
• Eger states that for Isoflurane, Sevoflurane, and Desflurane, the 80% decrement time would be clinically indistinguishable up to 90 – 120 minutes.
• For the difference of divergence between Sevoflurane and Desflurane for a 90% decrement time
o Eger indicates this occurs at 120 min o Bailey indicates this occurs at 90 min
Gasshead’s findings on CSDT Understanding CSDTs is central in understanding inhalational elimination
• Using the study by Eger as a guide for methodology[66], the author obtained the following data (*note – all references as described below reference the Egers primary article unless otherwise stated)
o Using Gas Man v3.1.6[70] Accepting default lambda values and volumes for all gases and
compartments • Desflurane 0.42, Sevoflurane 0.65, Isoflurane 1.3, Nitrous
Oxide 0.46, Enflurane 1.9, Halothane 2.5 70 kg, Open circuit, FGF 10 L/m, VA 4L/m, CO 6 L/m Noted CSDT at 50%, 80% , 90% CSDT for all agents at 30
minutes, 1 hour, 90 minutes, 2 Hour, 3 Hour, 4 Hour, 6 Hour, and 12 hours.
95% CSDT for only Isoflurane, Sevoflurane, Desflurane, & Nitrous Oxide at 15 minutes, 30 minutes, 1 – 4 hours, 6 hours, & 12 Hours
80%, 90%, and 95% were chosen due to clinical experience of decreases required at emergence for extubation.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
37
Time ranges selected were based on the broad range of case times.
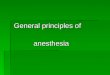
50% CSDT
0:00:00
0:01:26
0:02:53
0:04:19
0:05:46
0:07:12
0:08:38
30 min 1 hr 90 min 2 hr 3 hr 4 hr 6 hr 12 hr
n20DesfluraneSevofluraneIsofluraneEnfluraneHalothane
Figure 20 50% CSDT
o The 50% CDST was < 5 minutes for all agents except Halothane, regardless of duration
o This is in line with the findings for both Eger and Bailey

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
38
80% CSDT
0:00:00
0:28:48
0:57:36
1:26:24
1:55:12
2:24:00
2:52:48
30 min 1 hr 90 min 2 hr 3 hr 4 hr 6 hr 12 hr
n20DesfluraneSevofluraneIsofluraneEnfluraneHalothane
Figure 21 80% CSDT
In terms of of the 80% CSDT, Bailey indicated that after 45 – 60 minutes both Isoflurane and Enflurane started diverging from Desflurane and Sevoflurane trend line
Eger indicated that for the 80% CSDT o Is short for desflurane, isoflurane, and sevoflurane particularly for
anesthesia in the range of up to 120 min duration. In the authors data above, this does not apply to higher solubility
agents (Enflurane & Halothane) For these agents, anesthetic durations beyond 60 minutes show
considerable CSDT. The above findings agrees with Eger’s findings that “For anesthesia shorter than
90 min, the times to an 80% decrement would likely be clinically indistinguishable among the three drugs.”
Eger also states, “For anesthesia longer than 90 min, accumulation of isoflurane in tissue increasingly delays the time to an 80% decrement. These delays might be clinically appreciable.”
o This does impact on cases where the clinician doesn’t anticipate the time required for emergence
At 3 Hours, the time for Isoflurane to reach the 80% CSDT is @ 16 minutes vs 5 minutes for Sevoflurane and 3 minutes for Desflurane
o Eger further states that “accumulation of drug in tissue does not appreciably influence 80% decrement times for anesthesia of less than 240 min duration” between Sevoflurane and Desflurane.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
39
The results above do not reveal this. At 12 hours, the lowest soluble agents times are: 3 – 4 minutes for N20 and
Desflurane, 8 minutes for sevoflurane, and 47 minutes for Isoflurane Main points
o Duration and solubility have the greatest effect on CSDT o Important for planning for emergence, but complete recovery as
represented by CSDT>90% have more impact on discharge criteria as shown below for the 90 and 95% CSDT
90 & 95% CSDT
0:00:00
1:12:00
2:24:00
3:36:00
4:48:00
6:00:00
7:12:00
30 min 1 hr 90 min 2 hr 3 hr 4 hr 6 hr 12 hr
HR:
M:S
n20DesfluraneSevofluraneIsofluraneEnfluraneHalothane
Figure 22 90% CSDT

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
40
0:00:00
1:12:00
2:24:00
3:36:00
4:48:00
6:00:00
15 min 30 min 1 hr 2 hr 3 hr 4 hr 6 hr 12 hr
Hr:M
:S
N20DesfluraneSevofluraneIsoflurane
Figure 23 95% CSDT
General Notes
Contraindications Finally, Inhalation anesthesia is contraindicated in patients with hypersensitivity to halogenated anesthetics& with known or genetic susceptibility to malignant hyperthermia, & severe hypotension.
Nitrous Oxide [28, 71, 75-77]:
• MAC: 104 ET % • MAC Awake: 0.55 • Blood Gas Partition Coefficient : 0.47 • 50% decrement time: possibly < 5minutes
o S/S abate within 5 minutes[78] o Author assigned related to solubility resembling Desflurane but lacking
potency • 80% Decrement Time: 9 minutes[69]
o It is important to note that Context-sensitive Decrement times do not take into account what fraction of MAC a patient is starting at prior to the

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
41
cessation of inspired agent. Hence the impact of MAC additives, readiness for emergence, or end points of recovery are not taken into account.
• Most commonly used anesthetic gas • Symptoms occur in a dose-related fashion with increases in visual analog scale
ratings of "anxious", "stimulated", "coasting (spaced out)", "lightheaded", "confused", and "high"[78]
• Only inorganic anesthetic gas • Anesthetic effects can occur when mixed at 80% with 20% O2
o Potential for hypoxia if O2 inappropriately mixed OR if high concentration is maintained and abruptly discontinued without increasing delivered O2 concentration to 100% for 5 – 10 minutes (resulting in Diffusional Hypoxia.)
• Due to it’s potentially high inspired concentration it provides a concentration gradient effect and hence affects the increase of the rate of rise in a second gas (Concentration effect and Second gas effect) occurring both on induction and elimination.
• Due to stimulation of catecholamines vs. its depression of myocardial contractility – little change in hemodynamics occur.
o Unless catecholamine depletion is present • Diffusion to closed spaces d/t high inspired concentration – resulting in
potentially detrimental side effects o For example, caution should be used in cases of bowel obstructions,
pneumothorax, air embolism, middle ear procedures, uses with sulfur hexafluoride (retinal tears repairs), & pneumocephalus.
Isoflurane [28, 53, 57, 66, 69, 71, 79-83]
• MAC Awake: 0.25 - 0.38 • MAC 1.15 ET % • MACbar: 1.3 • Blood Gas Partition Coefficient = 1.4 • 50% decrement time: < 5 – 8 minutes (w/o significant change with increased
duration of anesthesia) • 65% decrement time: 5 – 8 minutes ( op. durations of 30 – 360 minutes)[53] • 80% Decrement Time: 17 minutes (for cases < 60 minutes) or up to < 20 - 30
minutes for case great then 60 – 120 minutes[53, 66]; a plateau of 30 minutes occurs @ 200 – 250 minutes and greater[53]
• For decrements >80% - significant time is required for reduction[53, 66] o Example: . case with ET ISO at 1.0 o Need 17 minutes in order to reach ET ISO of 0.2 (80% decrement)

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
42
o Eger and Shafer indicate that in cases less than 90 minutes, there would be little clinical differences between Isoflurane vs. Sevoflurane vs. Desflurane to obtain a 80% decrement
o 90% decrement can require up to 60 minutes o It is important to note that context-sensitive decrement times do not take
into account what fraction of MAC a patient is starting at prior to the cessation of inspired agent. Hence the impact of MAC additives, readiness for emergence, or end points of recovery are not taken into account.
• Pungent – limiting its use for inhalational inductions • Though known to dilate coronary arteries, there is conflicting data showing
potential coronary steal can occur with increase heart rates or decreases in pressure
• Bronchodilates • Decreases SVR with reflective increases in heart rate, yet causes little myocardial
depression • Non-convulsant • Increases cerebral blood flow and ICP • Decreases cerebral metabolic requirements • Due to it’s blood gas partition coefficient, surgical duration greater than 60
minutes can result in 30 minutes to obtain an 80% Context-sensitive Decrement time
Sevoflurane [28, 66, 71, 76, 83-87]
• MAC Awake: 0.34 • MAC : 2.0 ET % • MACbar: 2.2 - 3.5 • Blood Gas Partition Coefficient = .63 - .69 • 50% decrement time: < 5 – 8 minutes (w/o significant change with increased
duration of anesthesia) • 65% decrement time: 4 – 7 (op. durations 30 – 360 minutes) • 80% decrement time: 5 minutes (duration no effect) • 90% decrement time : < 10 minutes if duration is less then 90 min[53]
o Due to low blood gas coefficient, context sensitive decrement times similar to Desflurane
o It is important to note that context-sensitive decrement times do not take into account what fraction of MAC a patient is starting at prior to the cessation of inspired agent. Hence the impact of MAC additives, readiness for emergence, or end points of recovery are not taken into account.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
43
• Nonpungent – easily tolerated for inhalational inductions • Bronchodilates • Compound A exposure in patients also has been shown to rise with increased
Sevoflurane concentrations and duration of anesthesia. o Compound A end product increases significantly with prolonged
dehydration of Baralyme. Hence, Sevoflurane degradation to Compound A is decreased by lowering the concentration of monovalent bases in the carbon dioxide absorbent
o Renal effects of low-flow sevoflurane are similar to those of isoflurane in patients with stable renal insufficiency.
• Dose related cardiac depressant without increase in heart rates less than 2 MAC • Increases cerebral blood flow and ICP • Decreases cerebral metabolic requirements
Desflurane [28, 53, 57, 66, 71, 83]
• MAC Awake: 0.34 • MAC : 6.0% ET • MACbar: 1.3 • Blood Gas Partition Coefficient = .42 • 50% decrement time: < 5 – 8 minutes (w/o significant change with increased
duration of anesthesia) • 65% decrement time: 3 minutes ( op. durations of 30 – 360 minutes) • 80% decrement time: 5 minutes • 90% decrement time: < 10 minutes[53]
o It is important to note that context-sensitive decrement times do not take into account what fraction of MAC a patient is starting at prior to the cessation of inspired agent. Hence the impact of MAC additives, readiness for emergence, or end points of recovery are not taken into account.
• Rapid increases in concentration is associated with tachycardia and hypertension • Pungent – limiting its use for inhalational inductions • Increases cerebral blood flow and ICP • Decreases cerebral metabolic requirements
Enflurane [28, 53, 69, 82, 88]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
44
• MAC Awake: 0.27 • MAC : 1.7% ET • MACbar: 1.6 • Blood Gas Partition Coefficient = 1.9 • 50% decrement time: < 5minutes (w/o significant change with increased duration
of anesthesia) • 80% Decrement Time: 35 minutes (for cases >60 minutes)
o It is important to note that context-sensitive decrement times do not take into account what fraction of MAC a patient is starting at prior to the cessation of inspired agent. Hence the impact of MAC additives, readiness for emergence, or end points of recovery are not taken into account.
• For decrements >80% - significant time is required for reduction[53, 66] • • Has a mild sweet odor • Myocardial depressant and decreases SVR • Seizures have been seen with high concentrations and hypocapnia • Avoid in patients with preexisting renal dysfunction d/t fluoride byproduct
Halothane [1, 28, 71, 88]
• MAC : 0.75 ET % • MAC Awake: 0.55 • MACbar: 1.45 • Blood Gas Partition Coefficient = 2.4 • Dose dependent myocardial depressant • Dilates coronary arteries • Decreases myocardial oxygen demands • Blunts baroreceptors in aortic arch – decreasing vagal stimulation • Bronchodilates • Pungent • Increases cerebral blood flow and ICP • Hepatitis occurs in 1: 35,000
o At risk are Exposure to multiple halothane anesthetics in a short period, Obese and middle age women, and familial history to halothane toxicity.
Factors Affecting MAC
• Age[56, 58, 61] o >1 years of age – MAC requirements are reduced @ 6% per decade of life

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
45
o Age adjusted MAC values can be obtained by using the following calculation by Mapleson:
MACage = MAC40 * 10 -.00269 (Age-40) Using the above formula,
• the specific change per decade is 5.422% which is close to Eger’s quote of 6%
o Furthermore one can also obtain MAC Multiples by the following: MAC Multiple * MACage * 10 -.00269 (Age-40)
o If N20 is used – the following calculation can be used to find the total MAC value
(Fraction of Expired Agentagent/ MACage/agent ) + (Fraction of Expired AgentN20/ MACage/N20)
• Temperature[56, 62-65] o MAC requirements decrease 4 – 5% per centigrade o <20 degrees centigrade – no anesthesia is required o Calculated 1-(.05)(37-t)
Where t = core temperature o N20 is not affected by Temperature changes
• Pregnancy[89, 90] o MAC requirement decrease by 30%
• Other factors: o Alpha 2 agonists o Lidocaine o Pa02 < 38mmHG o BP < 40 mmHg o Preoperative medications o ETOH

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
46
ACTc Application of MAC
The inhalational screen condenses the aforementioned research data onto easily navigated screens.
1. All Inhalational agents are represented by the drop down list
a. 2. Age input box along with temperature
adjustment a. Age calculations are as follows
Age adjusted MAC calculations are as follows with inputted age applied within calculation from Mapleson
• MACage = MAC40 * 10 -.00269 (Age-40) Hence MACage=
• If Isoflurane is selected then o 1.17 * 10 -.00269 (Age-40)
• If Sevoflurane is selected then o 1.8 * 10 -.00269 (Age-40)
• If Desflurane is selected then o 6.6 * 10 -.00269 (Age-40)

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
47
• If Halothane is selected then o Where X = .75 * 10 -.00269 (Age-40)
• If Enflurane is selected then o 1.68 * 10 -.00269 (Age-40)
• If N20 is selected then a. 104 * 10 -.00269 (Age-40)
Temperature adjustment Calculation uses Eger temperature adjustment and then utilizes the Mapleson age calculation
• Works only for temp below 37 • Calculation
o Z = (1-.05)(37-t) • Applied to Age Adjustment
o Z * MACage = MAC40 * 10 -.00269 (Age-40)
The screen will show the following: • MAC awake value from data
& ET calculation = MAC Awake * Age Adj. MAC % (see above for equation)
• MAC BAR = MAC BAR * Age Adj. MAC %
• 50% and 80 % Decrement values from data
AGE MAC CAL
The AGE MAC CAL screen allows the user to see the impact of age on ET requirements with the use of nitrous as the secondary gas. Based on research from
Nickalls, R.W. and W.W. Mapleson, Age-related iso-MAC charts for isoflurane, sevoflurane and desflurane in man. Br J Anaesth, 2003. 91(2): p. 170-4.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
48
i. 1. First: User inputs values in all top three boxes and
a. MAY NOT input an age LESS than 1 b. May only enter a value of ET N20 between 0 – 70%
2. User will then select an Agent from the following list: a. Isoflurane b. Sevoflurane c. Desflurane d. Halothane e. Enflurane
On this screen, Current MAC is then calculated by the following formula 1. If Isoflurane is selected then
o Current MAC = (ET Agent/X) + (ET N20/Y) o Where X = 1.17 * 10 -.00269 (Age-40)
o Where Y = 104 * 10 -.00269 (Age-40) 2. If Sevoflurane is selected then
o Current MAC = (ET Agent/X) + (ET N20/Y) o Where X = 1.8 * 10 -.00269 (Age-40)
o Where Y = 104 * 10 -.00269 (Age-40) 3. If Desflurane is selected then
o Current MAC = (ET Agent/X) + (ET N20/Y) o Where X = 6.6 * 10 -.00269 (Age-40)
o Where Y = 104 * 10 -.00269 (Age-40) 4. If Halothane is selected then
o Current MAC = (ET Agent/X) + (ET N20/Y) o Where X = .75 * 10 -.00269 (Age-40)

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
49
o Where Y = 104 * 10 -.00269 (Age-40) 5. If Enflurane is selected then
o Current MAC = (ET Agent/X) + (ET N20/Y) o Where X = 1.68 * 10 -.00269 (Age-40)
o Where Y = 104 * 10 -.00269 (Age-40)
AGE ET CAL
• This screen allows the user to input a desired MAC level along with the optional use of nitrous – the difference with the above screen is that the user already knows the ET reading of his primary anesthetic gas
1. If Isoflurane is selected then
o AGENT ET% should = (Desired Combined MAC Level – Z) * X
o Where Z = Desired ET N20/Y
o Where Y = 104 * 10 -.00269 (Age-40) o Where X = 1.17 * 10 -.00269 (Age-40)
2. If Sevoflurane is selected then o AGENT ET% should = (Desired
Combined MAC Level – Z) * X o Where Z = Desired ET N20/Y
o Where Y = 104 * 10 -.00269 (Age-40) o Where X = 1.8 * 10 -.00269 (Age-40)
3. If Desflurane is selected then
o AGENT ET% should = (Desired Combined MAC Level – Z) * X
o Where Z = Desired ET N20/Y
o Where Y = 104 * 10 -.00269 (Age-40) o Where X = 6.6 * 10 -.00269 (Age-40)
4. If Halothane is selected then o AGENT ET% should = (Desired Combined MAC Level – Z) * X o Where Z = Desired ET N20/Y
o Where Y = 104 * 10 -.00269 (Age-40) o Where X = .75 * 10 -.00269 (Age-40)
5. If Enflurane is selected then o AGENT ET% should = (Desired Combined MAC Level – Z) * X o Where Z = Desired ET N20/Y
o Where Y = 104 * 10 -.00269 (Age-40)

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
50
o Where X = 1.68 * 10 -.00269 (Age-40)
3D Anatomical Figures • Using clinical and educational expertise, the author
generated the anatomical figures used in Anesthesia Clinical Tutor and Calculator Produced using a combination of the following programs[1, 2, 91-95]:
o PoserTM by Curious Labs v 6.0 efrontier
5615 Scotts Valley Drive Suite 210 Scotts Valley, CA 95066, USA http://www.e-frontier.com
o Adobe Photoshop CS2TM Adobe Systems Incorporated
345 Park Avenue San Jose, CA 95110-2704 USA www.adobe.com
o Jasc Paint Shop Pro v 9.1TM Corel Minneapolis
7905 Fuller Road Eden Prairie, MN 55344 USA http://www.corel.com
Spinal ACTc provides visual cues on dosing guides for both spinal and epidural cases. Dosing suggestions were derived from product inserts then cross referenced with anesthesia textbooks, research, and references.[1, 2, 92, 93, 96-102] Understanding of pharmacodynamics /kinetics, anatomical, proper technique (s), readiness for emergencies, patient selection, and equipment requirements is critical for any safe and successful spinal anesthetic. Complete and detailed appreciation is required prior to any patient care. Additionally, direct communication with the surgeon for case specific need(s) and duration will assist each clinician in determination of the appropriate regional anesthetic agent. Factors Affecting SAB[103, 104]
• Baricity – affecting spread post-injection o Patient positioning after injection, esp. for hypobaric and hyperbaric
solutions

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
51
Hypobaric - rising Hyperbaric – descending Isobaric – little or minimal spread
• Increase intrabdominal pressure will diminish dose requirements o Pregnancy o Ascities o Tumors
• Age • Additives
o Epinephrine o Opiates o Clonidine
• Height/Weight o Chandrasekhar suggestion was “Doses are based on a 66 - inch [167.64
cm] patient. An additional 2 mg tetracaine, 10 mg of lidocaine, or 1.5 mg bupivicaine should be added or subtracted for each 6 inches [15.24 cm] in height above or below 66 inches” [104] (conversions - authors addition)
• Gender • Site of Injection • Direct of bevel at time of injection • Diffusion • Characteristics of the spinal fluid • Amount and Volume of the anesthetic
Below is a general guide using drug inserts cross referenced with several published anesthesia resources (see below for details). Published dosing recommendations for spinal anesthetics – unless indicated all doses are for hyperbaric solutions in adult patients. An interesting note, many drug inserts defer to “standard textbooks” for more detailed dosing. Tetracaine: Drug manufacture (Taylor Pharmaceuticals& Abbott) recommending using 1% solution for:
o Perineum: 5 mg (0.5 cc + 0.5 cc spinal fluid) – injected at 4th lumbar interspace o Perineum & lower extremities: 10 mg ( 1 cc + 1 cc spinal fluid) - injected at 3rd
or 4th lumbar interspace. o Costal Margins (T5- T7)* : 15 mg ( 1.5 to 2 cc + 1.5 – 2 cc spinal fluid) – injected
at the 2nd, 3rd, or 4th lumbar interspace.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
52
o These recommendations fall midline with Tezlaff Suggestions (shown below) and corresponds with what the author has experienced clinically.
o Duration is noted between 2 – 3 hours o Maximum spinal dose: 20 mg
[76, 98, 105] *author’s interpretation Bupivacaine: Drug manufacture (Hospira) recommends using 0.75%
o 7.5 mg or 1.0 mL lower extremity and perineal procedures including TURP and vaginal hysterectomy. Twelve mg (12 mg or 1.6 mL) has been used for lower abdominal procedures such as abdominal hysterectomy, tubal ligation, and appendectomy.
o No recommendations are listed for levels higher level procedures. [106] o These recommendations are listed in the table below with a recommendation for
blocks up to T6 (which the author has used and agrees with the recommended dose)
o Duration of sensory blockade (time to return of complete sensation in the operative site or regression of two dermatomes) following a 12 mg dose averages 2 hours with or without 0.2 mg epinephrine.
o 12 mg Spinal averages 3 1/2 hours without epinephrine and 4½ hours with the addition of 0.2 mg epinephrine.
o In comparison with to equal milligram doses of hyperbaric Tetracaine, the duration of sensory blockade was the same but the time to complete motor recovery was significantly longer for Tetracaine.
o The addition of 0.2 mg epinephrine significantly prolongs the motor blockade and time to first postoperative narcotic.
o Maximum Doses o Maximum single dose 225 mg with Epinephrine (1:200K) – maybe
repeated once every 3 hours o Maximum single dose spinal dose 175 without Epinephrine - maybe
repeated once every 3 hours o Maximum spinal dose 20 mg [76, 98, 106]
Lidocaine 5% in 7.5 Glucose Previously, widely used in the United States - recently concerns over the post-operative occurrences of transient neurologic syndrome (TNS) have made this anesthetic fall out of general favor for SAB. The 5% solution had been withdrawn from the market during 2003.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
53
Drug manufacture (Hospira) recommends using 5% Lidocaine Hydrochloride and 7.5% Dextrose Injection
o The dosage recommended for normal vaginal delivery is approximately 1 mL (50 mg).
o For Caesarean section and those deliveries requiring intrauterine manipulations, 1.5 mL (75 mg) is usually adequate.
o Surgical anesthesia: o The dosage recommended for abdominal anesthesia is 1.5 to 2 mL (75 to
100 mg). No specific dose for dermatomal level. Hospira recommends that standard textbooks should be consulted for specific techniques and precautions for various spinal anesthetic procedures.
o Duration for a 50 mg dose is @ 100 min. – with an additionally 40 minutes if an analgesic is added
o Duration for doses between 75 – 100 mg is @ 120 min. o Maximum Doses
o Spinal dose: 100 mg o Maximum individual dose 7 mg/kg with Epinephrine o Maximum individual dose 4.5 mg/kg without Epinephrine[76, 98, 107]
Procaine 10% Standard textbooks should be consulted for specific techniques and precautions for various spinal anesthetic procedures. Drug manufacture (Hospira) recommends using 10% Procaine
o For Perineum: 50 mg (0 .5 cc + 0.5 cc of dilutent) – if injected at the 4th Lumbar Interspace
o Perineum lower extremities: 100 mg (1.0 cc + 1.0 cc of dilutent) – if injected at the 3rd or 4th Lumbar Interspace
o Up to Costal Margins (T5 – T7)* 200 mg ( 2.0 cc + 1 cc of dilutent) – if injected at the 3rd or 4th Lumbar Interspace
o Maximum spinal dose: 1000 mg [76, 96, 108] *author’s interpretation
Ropivacaine The author contacted AstraZeneca (1/2/2007) for US prescribing information – currently Ropivicaine is not approved for Intrathecal use in the United States nor does the package insert provide and direction for spinal anesthetic use.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
54
Numerous studies have been done, but no formal recognition has been received as of the present. AstraZeneca does provide dosing information on their website (http://www.anesthesia-az.com/article/509875.aspx) under the banner “Global prescribing information,” of which spinal doses can be found. General Intrathecal dosing recommendations from AstraZeneca
• Using 5.0 mg/ml using, a volume of 3 – 4 cc. o = 15 – 20 mg o Onset occurs within 1 – 5 minutes o Duration of 2 – 6 hours[109]
Spinal Doses
Medication T10 T8 T6 Duration Plain
Duration with Epinephrine
Tetracaine 1% 4 - 7.5 mg
8 -12 mg
10 - 16 mg
1.5 - 2 hrs 2 - 4 hrs
Bupivacaine 0.75% 4 - 10 mg
12 mg 14 -18 mg
1.5 - 2 hrs 2 hrs
Lidocaine 5% in 7.5 Glucose (Caution w/ TNS)
50 mg 60 - 70 mg
70 - 100 mg
1 hr 1 - 1.5 hrs
Procaine 10% 75 mg 125 mg 200 mg 45 min 1 hr Ropivicaine 0.5% * 8 - 12
mg 13 - 16 mg
16 - 18 mg
1.5 - 2 hrs 1.5 - 2 hrs
[98, 100, 104] *Check for FDA approval – not approved for SAB in U.S.
Spinal Opiates Dosing suggestions were derived from product inserts then cross referenced with anesthesia textbooks, research, and references. [28, 76, 102, 104] Use of Intrathecal opiates injected, as an adjunct to intraoperative anesthesia techniques and to mitigate postoperative pain. Understanding of pharmacodynamics /kinetics, anatomical, proper technique (s), readiness for emergencies, patient selection, and equipment requirements is critical for any safe and successful anesthetic. Complete and detailed appreciation is required prior to any patient care. Additionally, direct communication with the surgeon for case specific need(s) and duration will assist each clinician in determination of the appropriate regional anesthetic agent.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
55
Fentanyl Dose: 5 – 25 mcg Onset 5 – 10 min Duration 2 – 4 hours If respiratory depress occurs, it can occur earlier (< 6 hours) vs later
Sufentanil Dose: 2 – 10 mcg Onset 5 – 10 min Duration 2 – 4 hours If respiratory depress occurs, it can occur earlier (< 6 hours) vs later
Morphine Dose:
• 0.1 – 0.3 mg • 0.5 – 1 mg
Onset 30 – 60 min Duration 6 – 24 hours If respiratory depress occurs, it can occur earlier (< 6 hours) and later >6hr [93]
Meperidine Dose: 10 – 20 mg
Epidural . Understanding of pharmacodynamics /kinetics, anatomical, proper technique (s), readiness for emergencies, patient selection, and equipment requirements is critical for any safe and successful spinal anesthetic. Complete and detailed appreciation is required prior to any patient care. Additionally, direct communication with the surgeon for case specific need(s) and duration will assist each clinician in determination of the appropriate regional anesthetic agent. Accessed via similar techniques as a spinal but has an added benefit of placement of an indwelling catheter. Hence, the ability of continuous access to the epidural space, allows

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
56
anesthesia providers another route to provide perioperative and postoperative pain control.
Determination of Dose and Spread Dosing suggestions were derived from product inserts then cross referenced with anesthesia textbooks, research, and references [99, 101, 104, 110, 111]
• Volume o Generally 1.6 cc of anesthetic per segment to be block is required.
• Age o Multiple studies have found a spread of dose requirements based on age
and segments blocked Ranging from 0.25% - 1% per year reduction per year after 20
years of age[101, 110, 111] o Generally, a 50% reduction in dose is required in the elderly and neonate o Using Bromage suggestion is the most conservative at 1% per year
reduction on dose • Pregnancy
o A 30% reduction in dose is required • Vasoconstrictors
o Epinephrine 5 mcg/ml or 1:200 K, will generally increase the duration of the block
• pH o Adding 1 mEq of NaHCO3 to each 10 cc of local anesthetic produces a
faster onset, spread, and completeness of block Redosing [193, 23] Redosing for epidural anesthetics allows for proper planning for prolongation of block if required. Identical agent concentration of initial bolus for a surgical block is assumed in the following 2 segment regression. Medication Time to 2 segment regression Choroprocaine 45 – 70 min Prilocaine 90 – 130 min Lidocaine 60 – 150 min Mepivacaine 60 – 160 min Etidocaine 120 – 240 min Bupivacaine 120 – 260 min

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
57
Chloroprocaine Drug manufacture (Bedford Labs) recommends 2 to 2.5 mL per segment of a 2% or 3% solution can be used.
• The usual total volume of chloroprocaine hydrochloride injection is from 15 to 25 mL.
• Repeated doses 2 to 6 mL less than the original dose may be given at 40 to 50 minute intervals.
• The maximum single recommended doses of chloroprocaine in adults are: o Without epinephrine, 11 mg/kg, not to exceed a maximum total dose of
800 mg o With epinephrine (1:200,000), 14 mg/kg, not to exceed a maximum total
dose of 1000 mg. • Fast Onset: 10 – 15 minutes • Duration: 30 min. – 1 hour (Plain), 60 – 90 Min ( with epinephrine)[76, 98, 99,
112]
Lidocaine
• Drug manufacture (Hospira) recommends using 1% - 2% Lidocaine Hydrochloride solutions
• 2−3 mL of the indicated concentration per dermatome • In Normal Healthy Adults Maximum Doses
o With epinephrine should not exceed 7 mg/kg (3.5 mg/lb) of body weight and in general it is recommended that the maximum total dose not exceed 500 mg.
o When used without epinephrine, the maximum individual dose should not exceed 4.5 mg/kg (2 mg/lb) of body weight and in general it is recommended that the maximum total dose does not exceed 300 mg.
o For continuous epidural or caudal anesthesia, the maximum recommended dosage should not be administered at intervals of less than 90 minutes.
• Onset 15 min • Duration
o 80 – 120 min (plain) o 120 – 180 min (with epinephrine)[76, 98, 99, 113]
Bupivicaine • Drug manufacture (Hospira) statements for epidural:
o 0.25%─ incomplete motor block.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
58
• “For operations in which muscle relaxation is not important, or when another means of providing muscle relaxation is used”
• “Onset may be slower than with the 0.5% or 0.75%.” o 0.5% ─ Provides motor blockade but muscle relaxation may be
inadequate for operations in which complete relaxation is required o 0.75% ─ Produces complete motor block.
• Most useful for epidural block in procedures requiring complete muscle relaxation.
• Not for obstetrical anesthesia. • In Normal Healthy Adults Maximum Doses
o “Maximum dosage limit must be individualized in each case after evaluating the size and physical status of the patient, as well as the usual rate of systemic absorption from a particular injection site.”
o Up to 225 mg with epinephrine 1:200,000 o Up to 175 mg without epinephrine. o 24 hour dose should not exceed 400 mg. [114]
• Onset: 10 – 20 Min • Duration: 180 – 300 min ( with epinephrine)[98, 99]
Etidocaine • Not FDA approved for pregnancy, labor, delivery or lactation.
Local anesthetics rapidly cross the placenta and when used for epidural, paracervical, pudendal or caudal block anesthesia, can cause varying degrees of maternal, fetal, and neonatal toxicity.
• For Epidural use 1% and1.5%, concentrations are recommended • Maximum single does
o 300 mg without Epinephrine o 400 mg with Epinephrine
• Usual volume 15 – 30 cc • Onset 5 – 15 min • Duration 2 – 4 hours[98, 99]
Mepivacaine
• Drug manufacture (Hospira) recommends that standard textbooks should be consulted to determine the accepted procedures and techniques for the administration.
• For Epidural use 1%, 1.5%, and 2% concentrations are recommended

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
59
• Dosing • The recommended single adult dose for un-sedated, healthy, normal-sized
individuals should not usually exceed 400 mg. o This should be reduced in elderly or debilitated patients.
• Maximum doses of 7 mg/kg (550 mg) + epinephrine o Not recommended, except in exceptional circumstances o Cannot be repeated at intervals of less than 1 1/2 hours. o The total dose for any 24-hour period should not exceed 1,000 mg
• Onset: Fast – 5 – 15 min • Duration: 1 – 3 hours[97-99, 115]
Ropivacaine • Epidural infusions can be used up to 24 hours • Surgical concentrations: 0.5%, 0.75%, 1% • C-Section & Thoracic Epidural concentration: 0.5% & 0.75% • Labor: 2% concentration • Duration
o 0.5% : 2 – 4 hours o 0.75%: 3 – 5 hours o 1% - 4 – 6 hours o 2% (labor) : 0.5 – 1.5 hour
• Onset o 0.5% :15 – 30 min o 0.75%: 10 – 20 min o 1%: 10 – 20 min o 2% (labor) : 10 – 15 min[76, 109]
Prilocaine • Metabolism leads to formation of methaemoglobin
o More than 600 mg prilocaine is needed to cause a clinically apparent methaemoglobinemia in the normal adult
• Concentrations: 1 – 3% • Dosing
• The recommended single adult dose for un-sedated, healthy, normal-sized individuals should not usually exceed 600 mg.
• Onset: Fast – 5 – 15 min • Duration: 1 – 3 hr [98, 99]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
60
Epidural Opiates
Opiates used in conjunction with local anesthetics can reduce intraoperative an postoperative pain requirements. Selection of individual agents are determined by perioperative and postoperative pain needs.
o Side effects[102, 116] o Puritis (1– 100%),15 – 18%, Nausea Vomiting ( 20 – 50%), Urinary
retention ( 15 – 25%), Respiratory Depression (0.1 – 2% )
Drug Screen The medication dosages complied in the drug section were obtained first from the package insert, then cross referenced using multiple current pharmacology and anesthesiology text books.[1, 2, 5, 7, 76, 93, 120-123] Highlighting any drug will bring up its Name, dose and concentration up for review. Clicking “GO” will bring the user to the modifying screen where the user can change, modify, add notes, or delete their drug data. American Heart Association (2000). Handbook of Emergency Cardiovascular Care for healthcare providers, American Heart Association.
Epidural Opiates[102, 116-119] Name Dose Onset Duration
Alfentanil 15 mcg/kg 15 min 1 - 2 hr Fentanyl 25 -150 mcg 5 - 10 min 4 - 6 hr Hydromorphone .75 - 1.5 mg 5 - 10 min 3 - 18 hr Meperidine 12.5 - 100 mg 5 - 30 min 4 - 20 hr Methadone 1 - 5 mg 10 -15 min 3 - 11 hr PF Morphine 1- 5 mg 30 - 60 min 12 - 24 hrSufentanil 10 - 50 mcg 5 - 15 min 4 - 7 hr

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
61
American Heart Association (2002). PALS Provider Manual, American Heart Association.
Barash, P. G., B. F. Cullen, et al. (2001). Clinical anesthesia. Philadelphia, Lippincott Williams & Wilkins.
Dunn, P. F., T. A. Alston, et al. (2002). Clinical anesthesia procedures of the Massachusetts General Hospital. Philadelphia, Lippincott Williams & Wilkins.
Facts and Comparisons (Firm) (2004). Drug facts and comparisons 2004. St. Louis, MI., Facts and Comparisons.
Gahart, B. L., Nazareno, Adrienne R. (2006). 2006 Intravenous medications. St Louis, Elsevier Mosby.
Katzung, B. G. (2001). Basic & Clinical Pharmacology. New York, Lange Medical Books/McGraw-Hill, Medical Pub. Division.
Miller, R. D. (2005). Miller's Anesthesia. Philadelphia, Pa., Elsevier Churchill Livingstone.
Morgan, G. E. and M. S. Mikhail (2002). Clinical anesthesiology. Stamford, Conn., Appleton & Lange.
PDR (2007). 2007 Physicians' Desk Reference. Montvale, NJ, Thomson PDR The following drug inserts were also referred to for direction:
Company Drug Abbott Halothane Abbott Isoflurane Abbott METOCURINE IV Abbott Remifentanil Abbott Sevoflurane AHA Aspirin PO ACLS AHA Captopril PO ACLS AHA Flumazenil IV ACLS AHA Lidocaine IV ACLS AHA Lisinopril PO ACLS AHA Metoprolol IV ACLS AHA Procainamide IV ACLS
Akorn Labetalol American Regent Atropine IV ACLS
American Regent Atropine for Edrophonium IV
Reversal
American Regent Atropine for Neostigmine IV
Reversal American Regent CaCl 10% IV ACLS American Regent Dopamine American Regent Droperidol IV American Regent Epinephrine IV 1:10K ACLS

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
62
American Regent Furosemide IV ACLS
American Regent Glycopyrolate IV for
Pyridostigmine Reversal
American Regent Glycopyrrolate IV for
Neostigmine Reversal American Regent Magnesium IV ACLS American Regent Mannitol IV ACLS American Regent Neostigmine IV American Regent Nitroglycerin American Regent Phenylephrine
American Regent Sodium Bicarbonate IV
ACLS American Regent Vasopressin IV ACLS American Regent Verapamil IV ACLS
AstraZeneca Atenolol IV ACLS AstraZeneca Propofol IV
Baxter Desflurane Baxter Diazepam IV IM Baxter Diazepam PO Baxter Doxapram Baxter Esmolol Baxter Fentanyl IV Baxter Flumazenil IV
Baxter Glycopyrrolate (for Drying)
IV Baxter Lorazepam IM Baxter Lorazepam IV Baxter Meperidine IV, IM Baxter Midazolam IV Baxter Promethazine IV Baxter Propofol Infusion Baxter Propranolol IV ACLS
Bedford Laboratories Amrinone IV ACLS Bedford Laboratories Enalapril IV ACLS Bedford Laboratories Fenoldopam Bedford Laboratories Inamrinone Bedford Laboratories Ketamine IM Bedford Laboratories Ketamine IV Bedford Laboratories Romazicon IV
Ben Venue Laboratories, Inc. Etomidate IV
Bio Vail Diltiazem IV ACLS BristolMyers Stadol IV
Eli Lilly Glucagon IV ACLS Endo Pharmaceuticals Inc. Narcan IV
Fujisawa Adenosine IV ACLS

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
63
GlaxcoSmithKline CISATRACURIUM IV GlaxoSmithKline Digoxin IV ACLS GlaxoSmithKline MIVACURIUM IV GlaxoSmithKline Ondasetron IV GlaxoSmithKline Remifentanil IV
Hospira Alfentanil Hospira Aminophylline Hospira ATRACURIUM IV Hospira Atropine IV/IM Drying Hospira Diltiazem Hospira Fentanyl Hospira Lidocaine Hospira Magnesium Hospira Midazolam IV Hospira Milrinone Hospira MSO4 IV, IM Hospira Nalbuphine IV, IM Hospira Nitroprusside Hospira Procainamide - Adult Hospira Procainamide - Child
Janssen-Ortho Sufentanil IV lCN Pharmaceuticals, Edrophonium IV lCN Pharmaceuticals, Pyridostigmine IV
Mayne pharma Hydromorphone IV Merck Dexamethasone IV
Monarch Pharmaceuticals Methohexital IV Nicholas Piramal Dobutamine
Novartis Scopolamine TD Organon ROCURONIUM IV Organon SUCCINYLCHOLINE IV
Pfizer Ibutilide Roche Ketorolac
Sanofi-Aventis Dolasetron IV Sicor Metoclopramide IV Sicor Norepinephrine Sicor PANCURONIUM IV Sicor VERCURONIUM IV
Watson Labs Lorazepam PO Wyeth Amiodarone
Xanodyne Pharmaceuticals Amicar
Xanodyne Pharmaceuticals Methadone IV

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
64
The Propofol + Ketamne drip included in the program is a commonly used combination in our practice – refer to your institutional guidelines prior to use. Furthermore, the drip range for Vasopressin is provided by research currently in multiple trauma & shock states. [124-128] Dose ranges publish varies:
From 0.04 units/min[128] To 0.00002 units/kg/min up to 0.0003 U/kg/min[127] And 0.067 IU/min[126]
Malignant Hyperthermia Screen Information obtained [129, 130] & reprint permission provided by: MALIGNANT HYPERTHERMIA ASSOCIATION of the United States (MHAUS), 11 East State St. PO Box 1069 Sherburne, NY 13460
MH Hotline: 1-800- MH-HYPER (1-800-644-9737) or 1-315-464-7079 if outside the U.S.
http://www.mhreg.org/ AND
Malignant Hyperthermia Investigation Unit ES11-423, Toronto General Hospital 200 Elizabeth St. Toronto, ON M5G 2C4 416-340-3128 (Phone) 416-340-4960 (FAX)
Dose calculations
1. Calculate dose from calculated KG using 2 -3 mg per kg

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
65
• Example: If the Patient is 100 kg, then 200 mg – 300 mg is shown in the box
2. Calculate “Volume” by dividing the above range by .33 • This is due to if reconstituted as per directions 60 cc per vial – there is
only .33 mg per cc. • Example: If the dose range is 200 mg – 300 mg, then
• 200 / .33 = 606 cc • 300/ .33 = 909 cc • SO “606 – 909 cc” is shown in the box
3. Calculate “Number of Vials” by dividing Volume range by 60 • Example: If the dose range is 606 cc – 909 cc, then
• 606 / 60 = 10.1 • 909 / .33 = 15.15 • SO “10.1 – 15.15 ” is shown in the box
Vital statistics These tables are viewable when pediatric patients are selected, accessed on the “Patient Data” screen by clicking on “VS” Adult Values[131] Normal Range of Resting Values
Variable Adult Resp. Rate / min 12 - 20 TV (cc/kg) 10 - 12 HR / min 60 - 80 Syst. 110 – 135 Diast. 80 – 89
• Systolic and Diastolic range from 5th to 95th Height percentile • 50th percentile BP values (representing normal ranges) are shown • Normal Range of Resting Values for RR/min, and HR /min are shown • Alternative lowest blood pressure: 70 = 2*age[131, 132]
Male BP
Variable NB 1 yo 3 yo 5 yo 10 yo 12 yo Resp. Rate / min 30 - 60 22 - 30 22 - 30 20 - 24 16 - 22 16 - 22 TV (cc/kg) 10 - 12 10 - 12 10 - 12 10 - 12 10 - 12 10 - 12
HR / min 100 - 160
90 - 150 80 - 125 70 - 115 70 - 110 60 - 100

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
66
Syst. 60 - 96 80 - 89 86 - 95 90 - 98 97 - 106 101 - 110 Diast. 30 - 62 34 - 39 44 - 48 50 - 55 58 - 63 59 - 64
Female BP
Variable NB 1 yo 3 yo 5 yo 10 yo 12 yo Resp. Rate 30 - 60 22 - 30 22 - 30 20 - 24 16 - 22 16 - 22 TV (cc/kg) 10 - 12 10 - 12 10 - 12 10 - 12 10 - 12 10 - 12
HR 100 - 160 90 - 150 80 - 125 70 - 115 70 - 110 60 - 100
Syst. 60 - 96 83 - 90 86 - 93 89 - 96 98 - 105 102 - 109
Diast. 30 - 62 38 - 42 50 - 54 52 - 56 59 - 62 61 - 64
Pediatric outpatient considerations: Pediatric Patients at risk:
• Low hemoglobin or hematocrit • A history of respiratory distress syndrome • Aspiration • Prematurity • History of apnea or with feeding is also at risk. • Ex-premature should not be operated on as an outpatient until they are at least 46
weeks post conceptual age (gestational age plus postnatal age). • The ex-premature less than 46 weeks post conceptual age must be apnea
monitored for 24 hours post operatively as an inpatient.[133] o Patients with a history of prematurity can potentially develop significant
periods of apnea in the postoperative period. There are multiple studies that address this issue, all of which are a topic of great controversy. Ages ranging 44 weeks post –conceptual age (PCA: gestational age at birth + chronological age) to 60 weeks PCA (to potentially achieve < 1% incidence) at cited for guidelines as admittance guidelines for overnight monitoring for apnea.[10, 134-136]
Many facilities choose cutoff between 46 and 60 weeks postconceptual ages. Regardless of age, if patient continues to have apnea at home, inpatient overnight monitored is required.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
67
Laboratory Values Various references were used to build the base of the lab values in ACTc.[137-139] Item ACT Albumin Alk Phos ALT Ammonia Amylase Anion Gap Arterial Blood Gas Base Excess Arterial Blood Gas HCO3 Arterial Blood Gas O2 Sats Arterial Blood Gas P02 (@21%) Arterial Blood Gas PCO2 Arterial Blood Gas pH Antithrombin III AST Bilirubin (Direct) Bilirubin (Indirect) Bilirubin (Total) Bleeding Time (BT) BUN Calcium (CA)
Cardiac Enzymes: CK - MB subforms
Cardiac Enzymes: Creatine Phosphokinase Cardiac Enzymes: Creatine Phosphokinase Isoenzymes
Cardiac Enzymes: MB fraction
Cardiac Enzymes: Myoglobin
Cardiac Enzymes: Troponins T and I
Cardiac Enzymes: Troponin Chloride (CL) Cholesterol (Total) CO2 Creatinine Fibrin Split Products or Degradation Products Glucose HDL Hematocrit (HCT) Hemoglobin (HEM) INR Ionized CA LDH LDL Magnesium (MG) Osmolarity Phosphate Platelet (Plat) Potassium (K) PT PTT RBC Sodium (NA) Toxicology Screen Acetaminophen Toxicology Screen Amocarbital Toxicology Screen Butabarbital Toxicology Screen Carbonmonoxide Toxicology Screen Digoxin

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
68
Toxicology Screen Dilantin
Toxicology Screen ETOH
Toxicology Screen Glutethimide Toxicology Screen Lead Toxicology Screen Lithium Toxicology Screen Phenobarbital Toxicology Screen Salicylate Toxicology Screen Theophylline Triglycerides Uric Acid Venous Blood Gas O2 Sats
Venous Blood Gas pH Venous Blood HCO3 Venous Blood PCO2 Venous Blood PO2 VLDL WBC: WBC:Basophils WBC:Eosinophils WBC:Lymphocytes WBC:Monocytes WBC:Neutrophils
PH/ETCO2/K calculator Using the following general premise that Changes in ETCO2 will affect blood pH hence can impact serum potassium:
• Respiratory Driven pH Changes: o Acute Acidosis/Alkalosis: pH change = 0.008 units per 1 mm Hg Paco2
change o Chronic Acidosis: pH change = 0.003 units per 1 mm Hg Paco2 change o Chronic Alkalosis: pH change = 0.0017 units per 1 mm Hg Paco2 change
[140] o The equation means that a change of 0.1 in the pH can be caused by either:
A respiratory change (PCO2 change) of 12mmHg – 12.5 (10 mmHg change in PCO2 = 0.8 change in pH), or[140, 141]
A metabolic change (Base Excess change) of 6 mEq/L. A mixture of the two.[141]
• Potassium o In evaluating serum potassium, the consideration must include the possible
acute changes in serum pH. o Having an inverse relationship
When serum pH falls, serum potassium rises because potassium
shifts from the cellular to the vascular space. Conversely, when serum pH rises, serum potassium falls because
potassium shifts intracellularly.[142] o For any pH change the effect of acidaemia is greater than alkalaemia. o In general, serum K+ decreases by approximately 0.3 mEq/L – 0.6 mEq/L
for every 0.1 U increase in pH above normal. [142, 143] o During hyperventilation for each 0.1 pH unit, the serum K+ will decrease
rapidly by about 0.2 mmol/L[144]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
69
o There are conflicting studies Acute respiratory acidosis does not affect plasma potassium
concentration. [145, 146] Another study showed Respiratory and metabolic alkalosis and
respiratory acidosis result in similar small shift of potassium into and out of cell respectively (0.1-0.4 mmol/l on average). [143]
o Non-organic results in a shift of 0.24-1.7 mmol/l per 0.1 unit pH change. o In chronic acid-base disorders, the final potassium levels are affected
primarily on renal function and to lesser degree to transcellular shifting. [143]
The actual tool is shown below where the user input the initial values and selecting the pathologic state, the possible outcomes will be then calculated
Figure 24 PH Calculator Input Screen
Calculated values:
Figure 25 PH Calculated values

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
70
Settings Screen ACTc settings section allows for modification of all listed databases within ACTc
“New” starts a new input dialog to add to your database
o Ensure you are in the correct category “Edit” allows for modifying the highlighted entry “Delete allows for complete removal of the item form you database

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
71
Trouble Shooting and Questions
Q: On a PALM installation, I do not see the ACTc icon only the GASSHEAD icon. A: - Please install your program on the device & use the uncompressed installation files in the ACTcMAC folder in the zip file from gasshead. -If you are using a MAC, please uncompress the files to your desktop and install the files (not the folder) to your palm device. -Also if you have Epocrates installed - you "might" have to uninstall Epocrates first then install ACTc, then you may reinstall Epocrates. - Finally, if you do not have enough storage on the device, ACTc will not install. DO NOT install on a storage card.
Q: I did not receive an email confirmation of my purchase A: Please adjust your junk mail settings and goto our Login Page where you can view your information and resend your information to your email in question Click here to GOTO the Login PAGE
Q: (PPC) When changing some screens, sometimes I have a portion of a previous screen still present or see portions of graphics. Or Program exits unexpectedly. A: ACTc requires a current processor with spare RAM available. Hence, stopping all unrequired programs will allow ACTc to function correctly.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
72
Please close all running programs and re-attempt using ACTc. For PPC users: GOTO Settings>Systems>Memory>Running Programs>Select (Highlight the program(s) and click "Stop"
Q: How can I see my account information? A: Sign in to your account using your email provided at time of purchase and your password you made. If you have forgotten your password, enter your password in the “Forgot Password” page and it will be sent to you.
Q: The program will not install all the files (PALM) A: Please check to ensure you have adequate memory on the device to install ACTc. Additionally, issues have been identified with the drug program Epocrates, where Epocrates will prevent ACTc from installing. Severe cases have required a full un-installation of Epocrates then an installation of ACTc, then a re-installation of Epocrates.
Q: How do I see more of the cell in the Snap-Shot and Drug Screen? A: Click on the Right Edge of the cell with your stylus and hold and drag open the cell
Q: I have a Palm Device and cannot read all the words in the drug detail box or lab detail Box A: Use your toggle button (the large round or square button on the front of your PALM device) – click on the right side of the button to read more text
Q. (PPC) I have a prior installation of ACTc and have errors after install version 3.0. What should I do? A:
6. Please uninstall both versions

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
73
7. Click on Programs
8. Click on File Explorer
9. Click on My Documents
10. A drop down list will appear
11. Click on My Device
12. Click on Program files
13. Delete any ACTc folders or Gasshead folders If you still have a ACTc icon in the program list (usually occurs with Windows mobile 2003 – if you have Windows mobile 2002 see the next Q & A for deleting details)
1. Connect your PDA to ActiveSync and allow it device to synchronize
2. In the Microsoft ActiveSync box
3. Click on File
4. Click on Explore
5. In the new Window that appears, Double click on “My Windows Mobile-Based Device”
6. Click on Windows
7. Click on Start Up
8. Click on Programs
9. Click on ACTc and delete
10. Reinstall ACTc version 3

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
74
Q: I have the old ACTc icon in my program list – How can I get rid of it (usually seen in Windows Mobile 2003)? A:
1. Connect your PDA to ActiveSync and allow it device to synchronize
2. In the Microsoft ActiveSync box
3. Click on File
4. Click on Explore
5. In the new Window that appears, Double click on “My Windows Mobile-Based Device”
6. Click on Windows
7. Click on Start Menu
8. Click on Programs
9. Click on ACTc and delete
Q: I have the old ACTc icon in my program list – How can I get rid of it (usually seen in Windows Mobile 2002)? A:
1. Connect your PDA to ActiveSync and allow it device to synchronize
2. In the Microsoft ActiveSync box
3. Click on File
4. Click on Explore

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
75
5. In the new Window that appears, Double click on “My Windows Mobile-Based
Device”
6. Click on Windows
7. Click on Start Menu
8. Click on ACTc and delete
Q: I noticed that all your Help screens indicate specific references in your Readings Section, is there a main document that this originated or is there a help document available? A: All sections of ACTc have been well researched and reviewed, all supporting documents have been listed and full credit has been given to all researchers, software, development team members, pharmaceuticals, publication permission sources, and educators. You are reading the document.
Q: What if I change my PDA how do I re-register? A: The device key is unique to each device and the unlock codes only work for that device with that unique code. Gasshead recognizes that PDAs are upgraded (usually once every 3 – 5 years), and offers one free transfer to a new device in that time period. Please email support for guidance at: [email protected] mailto:[email protected]

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
76
Readings and References ACTc readings and Calculations allow the user to review or modify all anesthesia calculations and review the references and readings list [1-7, 10, 11, 13-27, 29-49, 51-69, 71, 75-77, 79-107, 109-132, 147-191] 1. Morgan, G.E. and M.S. Mikhail, Clinical anesthesiology. 3rd ed. 2002, Stamford,
Conn.: Appleton & Lange. 2. Barash, P.G., B.F. Cullen, and R.K. Stoelting, Clinical anesthesia. 4th ed. 2001,
Philadelphia: Lippincott Williams & Wilkins. 3. Friedman, A.L., Pediatric hydration therapy: historical review and a new
approach. Kidney Int, 2005. 67(1): p. 380-8. 4. Pandey, C.K., Singh, R. B. , Fluid and Electrolyte Disorders. Indian J. Anaesth.,
2003. 45(5): p. 380 - 387. 5. Miller, R.D., Miller's Anesthesia. 6th ed. 2005, Philadelphia, Pa.: Elsevier
Churchill Livingstone. 6. LMA, N.A., LMA AIRWAY INSTRUCTION MANUAL. 2005, San Diego: LMA
North America. 7. American Heart Association, PALS Provider Manual, ed. M.F. Hazinski. 2002:
American Heart Association. . 8. Fisher, D.M., Anesthesia equipment for Pediatrics, in Pediatric Anesthesia, G.A.
Gregory, Editor. 2002, Churchill Livingstone: New York. p. 206 - 207. 9. Cauldwell, C.B., Induction, Maintenance, and Emergence, in Pediatric
Anesthesia, G.A. Gregory, Editor. 2002, Churchill Livingstone: New York. p. 218, 224 - 225.
10. Gregory, G.A., Pediatric anesthesia. 3rd ed. 2002, New York: Churchill Livingstone.
11. Penlington, G.N., Letter: Endotracheal tube sizes for children. Anaesthesia, 1974. 29(4): p. 494-5.
12. Gregory, G.A., Pediatric anesthesia. 3rd ed. 1994, New York: Churchill Livingstone.
13. Samsoon, G.L. and J.R. Young, Difficult tracheal intubation: a retrospective study. Anaesthesia, 1987. 42(5): p. 487-90.
14. Mallampati, S.R., Clinical sign to predict difficult tracheal intubation (hypothesis). Can Anaesth Soc J, 1983. 30(3 Pt 1): p. 316-7.
15. Mallampati, S.R., et al., A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J, 1985. 32(4): p. 429-34.
16. Magboul, M.A., The Dilemma of Airway Assessment and Evaluation. The Internet Journal of Anesthesiology, 2005. 10(1).
17. Walls, R.M., Manual of emergency airway management. 2nd ed. 2004, Philadelphia: Lippincott Williams & Wilkins.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
77
18. Braude, D., Difficult airways are "LEMONS": updating the LEMON mneumonic to account for time and oxygen reserve. Ann Emerg Med, 2006. 47(6): p. 581.
19. Cote, C.J., Pediatric anesthesia, in Anesthesia, R.D. Miller, Editor. 2000, Churchill Livingstone: Philadelphia. p. 2088–117.
20. Haskell, G.H., PALS review. 2nd ed. Pearls of wisdom. 2006, New York: McGraw-Hill.
21. Fine, G.F. and L.M. Borland, The future of the cuffed endotracheal tube. Paediatr Anaesth, 2004. 14(1): p. 38-42.
22. Chou, H.C. and T.L. Wu, Rethinking the three axes alignment theory for direct laryngoscopy. Acta Anaesthesiol Scand, 2001. 45(2): p. 261-2.
23. Cooper, R.M., Laryngoscopy — its past and future. Canadian Journal of Anesthesia, 2004. 51(R6).
24. Landsman, I., Cricoid pressure: indications and complications. Paediatr Anaesth, 2004. 14(1): p. 43-7.
25. Rosenblatt, W., Airway Management, in Clinical Anesthesia, P.G. Barash, Editor. 2001, Lippincott Williams & Wilkins: New York. p. 608.
26. Langeron, O., et al., Prediction of difficult mask ventilation. Anesthesiology, 2000. 92(5): p. 1229-36.
27. Kheterpal, S., et al., Incidence and Predictors of Difficult and Impossible Mask Ventilation. Anesthesiology, 2006. 105(5): p. 885-891.
28. Morgan, G.E., et al., Clinical anesthesiology. 3rd ed. 2002, New York: Langae Medical Books/McGraw-Hill, Medical Pub. Division. xi, 1042 p.
29. Charlson, M.E., et al., Preoperative characteristics predicting intraoperative hypotension and hypertension among hypertensives and diabetics undergoing noncardiac surgery. Ann Surg, 1990. 212(1): p. 66-81.
30. Klasen, J., et al., Differing incidences of relevant hypotension with combined spinal-epidural anesthesia and spinal anesthesia. Anesth Analg, 2003. 96(5): p. 1491-5, table of contents.
31. Juneja, R., Anaesthesia for the Elderly Cardiac Patient. Annals of Cardiac Anaesthesia, 2006. 9: p. 67 - 77.
32. American Society, A., Practice Guidelines for Perioperative Blood Transfusion and Adjuvant Therapies. 1995.
33. Boldt, J., et al., The value of an albumin-based intravascular volume replacement strategy in elderly patients undergoing major abdominal surgery. Anesth Analg, 2006. 103(1): p. 191-9, table of contents.
34. Christ, F., et al., Hyperosmotic-hyperoncotic solutions during abdominal aortic aneurysm (AAA) resection. Acta Anaesthesiol Scand, 1997. 41(1 Pt 1): p. 62-70.
35. Finfer, S., et al., A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med, 2004. 350(22): p. 2247-56.
36. Gold, M.S., Perioperative fluid management. Crit Care Clin, 1992. 8(2): p. 409-21.
37. Grocott, M.P. and M.A. Hamilton, Resuscitation fluids. Vox Sang, 2002. 82(1): p. 1-8.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
78
38. Grocott, M.P., M.G. Mythen, and T.J. Gan, Perioperative fluid management and clinical outcomes in adults. Anesth Analg, 2005. 100(4): p. 1093-106.
39. Hai, S.A., Permissive hypotensive resuscitation--an evolving concept in trauma. J Pak Med Assoc, 2004. 54(8): p. 434-6.
40. Holte, K., P. Jensen, and H. Kehlet, Physiologic effects of intravenous fluid administration in healthy volunteers. Anesth Analg, 2003. 96(5): p. 1504-9, table of contents.
41. Joshi, G.P., Intraoperative fluid restriction improves outcome after major elective gastrointestinal surgery. Anesth Analg, 2005. 101(2): p. 601-5.
42. Shoemaker, W.C., et al., Resuscitation from severe hemorrhage. Crit Care Med, 1996. 24(2 Suppl): p. S12-23.
43. Sigurdsson, G.H., Perioperative fluid management in microvascular surgery. J Reconstr Microsurg, 1995. 11(1): p. 57-65.
44. Sinclair, S., S. James, and M. Singer, Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. BMJ, 1997. 315(7113): p. 909-12.
45. Stephens, R. and M. Mythen, Optimizing intraoperative fluid therapy. Curr Opin Anaesthesiol, 2003. 16(4): p. 385-92.
46. Holte, K., N.E. Sharrock, and H. Kehlet, Pathophysiology and clinical implications of perioperative fluid excess. Br J Anaesth, 2002. 89(4): p. 622-32.
47. Rehm, M. and U. Finsterer, Treating intraoperative hyperchloremic acidosis with sodium bicarbonate or tris-hydroxymethyl aminomethane: a randomized prospective study. Anesth Analg, 2003. 96(4): p. 1201-8, table of contents.
48. Rehm, M., et al., Acid-base changes caused by 5% albumin versus 6% hydroxyethyl starch solution in patients undergoing acute normovolemic hemodilution: a randomized prospective study. Anesthesiology, 2000. 93(5): p. 1174-83.
49. Brandstrup, B., Tønnesen, H., Beier-Holgersen, R., Hjortsø, E., Ørding, H., Lindorff-Larsen, K., Rasmussen, M.S., Lanng,C.,Wallin, L.,Iversen, L.H.,Gramkow,C.S., Okholm,M., Blemmer, T., Svendsen, P., Rottensten, H., Thage,B. ,Riis,J. ,Jeppesen,I.S. , Teilum, D., Christensen, A.M., Graungaard,B. ,Pott, F., Effects of Intravenous Fluid Restriction on Postoperative Complications: Comparison of Two Perioperative Fluid Regimens. Annals of Surgery, 2003. 238(5): p. 641 - 648.
50. Dunn, P.F., T.A. Alston, and Massachusetts General Hospital. Dept. of Anesthesia and Critical Care., Clinical anesthesia procedures of the Massachusetts General Hospital. 7th ed. 2007, Philadelphia: Lippincott Williams & Wilkins.
51. Ferrera, P.C., Trauma management : an emergency medicine approach. 2001, St. Louis, Mo.: Mosby.
52. Gernsheimer, T., Blood Component Therapy, in Puget Sound Blood Center and Program. 2005: Seattle

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
79
53. Bailey, J.M., Context-sensitive half-times and other decrement times of inhaled anesthetics. Anesth Analg, 1997. 85(3): p. 681-6.
54. Cook, T.L., et al., Behavioral effects of trace and subanesthetic halothane and nitrous oxide in man. Anesthesiology, 1978. 49(6): p. 419-24.
55. Cook, T.L., et al., Effect of subanesthetic concentration of enflurane and halothane on human behavior. Anesth Analg, 1978. 57(4): p. 434-40.
56. Eger, E.I., 2nd, Age, minimum alveolar anesthetic concentration, and minimum alveolar anesthetic concentration-awake. Anesth Analg, 2001. 93(4): p. 947-53.
57. Daniel, M., et al., Fentanyl augments the blockade of the sympathetic response to incision (MAC-BAR) produced by desflurane and isoflurane: desflurane and isoflurane MAC-BAR without and with fentanyl. Anesthesiology, 1998. 88(1): p. 43-9.
58. Mapleson, W.W., Effect of age on MAC in humans: a meta-analysis. Br J Anaesth, 1996. 76(2): p. 179-85.
59. Dwyer, R., et al., Effects of isoflurane and nitrous oxide in subanesthetic concentrations on memory and responsiveness in volunteers. Anesthesiology, 1992. 77(5): p. 888-98.
60. Katoh, T., et al., Influence of age on awakening concentrations of sevoflurane and isoflurane. Anesth Analg, 1993. 76(2): p. 348-52.
61. Nickalls, R.W. and W.W. Mapleson, Age-related iso-MAC charts for isoflurane, sevoflurane and desflurane in man. Br J Anaesth, 2003. 91(2): p. 170-4.
62. Eger, E.I., 2nd and B.H. Johnson, MAC of I-653 in rats, including a test of the effect of body temperature and anesthetic duration. Anesth Analg, 1987. 66(10): p. 974-6.
63. Eger, E.I., 2nd, L.J. Saidman, and B. Brandstater, Temperature dependence of halothane and cyclopropane anesthesia in dogs: correlation with some theories of anesthetic action. Anesthesiology, 1965. 26(6): p. 764-70.
64. Satas, S., et al., MAC for halothane and isoflurane during normothermia and hypothermia in the newborn piglet. Acta Anaesthesiol Scand, 1996. 40(4): p. 452-6.
65. Antognini, J.F., Hypothermia eliminates isoflurane requirements at 20 degrees C. Anesthesiology, 1993. 78(6): p. 1152-6.
66. Eger, E.I., 2nd and S.L. Shafer, Tutorial: context-sensitive decrement times for inhaled anesthetics. Anesth Analg, 2005. 101(3): p. 688-96, table of contents.
67. Bailey, J.M., Technique for quantifying the duration of intravenous anesthetic effect. Anesthesiology, 1995. 83(5): p. 1095-103.
68. Schraag, S., et al., Recovery from opioid anesthesia: the clinical implication of context-sensitive half-times. Anesth Analg, 1998. 86(1): p. 184-90.
69. Thompson, C., Context Sensitive Decrement Times. 2000: Royal Prince Alfred Hospital, Sydney, Australia.
70. Philip, J.H., Gas Man: Understanding Anenesthesia Uptake and Dstribution. 1997, H.M Franklin Associates: Chestnut Hill MA.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
80
71. Eger II, E., Weiskopt, R.B., Eisenkraft J.B., The Pharmacology of Inhaled Anesthetics. 2002, Chicago: HealthCare Press.
72. Wong, J., et al., Titration of isoflurane using BIS index improves early recovery of elderly patients undergoing orthopedic surgeries. Can J Anaesth, 2002. 49(1): p. 13-8.
73. Song, D., J. van Vlymen, and P.F. White, Is the bispectral index useful in predicting fast-track eligibility after ambulatory anesthesia with propofol and desflurane? Anesth Analg, 1998. 87(6): p. 1245-8.
74. Wrobel, M., S. Kreuer, and W. Wilhelm, [Bispectral index and desflurane concentration below 1 MAC]. Anaesthesist, 2004. 53(1): p. 36-40.
75. Birch, W.A., Nitrous Oxide, in Anesthesiology Review, R.J. Faust, Editor. 1994, Churchhill Livingstone: NewYork. p. 104 - 105.
76. Facts and Comparisons (Firm), Drug facts and comparisons 2004. 2004, Facts and Comparisons: St. Louis, MI.
77. Masuda, T. and K. Ikeda, Elimination of nitrous oxide accelerates elimination of halothane: reversed second gas effect. Anesthesiology, 1984. 60(6): p. 567-8.
78. James, P.Z., J. Lance Lichtor, Dennis W. Coalson, Jeffrey L. Apfelbaum, David Flemming, Vanessa Foster Time course of effects of brief inhalations of nitrous oxide in normal volunteers Addiction, 1994. 89(7): p. 831 - 839.
79. Eger, E.I., 2nd, The pharmacology of isoflurane. Br J Anaesth, 1984. 56 (Suppl 1): p. 71S-99S.
80. Rhodia New Zealand Limited, Isoflurane Drug Insert. 1999: Manukau City, Auckland New Zeland.
81. Alkire, M.T. and L.A. Gorski, Relative amnesic potency of five inhalational anesthetics follows the Meyer-Overton rule. Anesthesiology, 2004. 101(2): p. 417-29.
82. Gaumann, D.M., J.P. Mustaki, and E. Tassonyi, MAC-awake of isoflurane, enflurane and halothane evaluated by slow and fast alveolar washout. Br J Anaesth, 1992. 68(1): p. 81-4.
83. White, D., Uses of MAC. Br J Anaesth, 2003. 91(2): p. 167-9. 84. Abbott Laboratories, Ultane (sevoflurane) - drug insert. 2005: North Chicago, IL
60064, USA. 85. Higuchi, H., et al., Compound A concentrations during low-flow sevoflurane
anesthesia correlate directly with the concentration of monovalent bases in carbon dioxide absorbents. Anesth Analg, 2000. 91(2): p. 434-9.
86. Higuchi, H., et al., The effects of low-flow sevoflurane and isoflurane anesthesia on renal function in patients with stable moderate renal insufficiency. Anesth Analg, 2001. 92(3): p. 650-5.
87. Ura, T., et al., Minimum alveolar concentration of sevoflurane that blocks the adrenergic response to surgical incision in women: MACBAR. Eur J Anaesthesiol, 1999. 16(3): p. 176-81.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
81
88. Roizen, M.F., R.W. Horrigan, and B.M. Frazer, Anesthetic doses blocking adrenergic (stress) and cardiovascular responses to incision--MAC BAR. Anesthesiology, 1981. 54(5): p. 390-8.
89. Chan, M.T., P. Mainland, and T. Gin, Minimum alveolar concentration of halothane and enflurane are decreased in early pregnancy. Anesthesiology, 1996. 85(4): p. 782-6.
90. Palahniuk, R.J., S.M. Shnider, and E.I. Eger, 2nd, Pregnancy decreases the requirement for inhaled anesthetic agents. Anesthesiology, 1974. 41(1): p. 82-3.
91. Brown, D.L., Atlas of regional anesthesia. 2nd ed. 1999, Philadelphia: Saunders. 92. Chelly, J.E., Peripheral nerve blocks : a color atlas. 1999, Philadelphia:
Lippincott Williams & Wilkins. 93. Dunn, P.F., T.A. Alston, and Massachusetts General Hospital. Dept. of
Anesthesia and Critical Care., Clinical anesthesia procedures of the Massachusetts General Hospital. 6th ed. 2002, Philadelphia: Lippincott Williams & Wilkins.
94. Gray, H., Gray's Anatomy: The Classic Collector's Edition 15th ed. 1988, New York: Gramercy.
95. Netter, F.H. and A.F. Dalley, Atlas of human anatomy / Frank H. Netter ; Arthur F. Dalley II, consulting editor. 2nd ed. 1997, East Hanover, N.J.: Novartis.
96. Bridenbaugh, P.G., Nicholas, Spinal (Subarachnoid) Neural Blockade, in Neural Blockade - In Clinical Anesthesia and Management of Pain, M. Cousins, Editor. 1988, JB Lippincott Company: Philadelphia. p. 213 - 224.
97. Kleinman, W., Spinal, Epidural, & Caudal Blocks, in Clinical anesthesiology, G.E. Morgan, Editor. 2002, Lange Medical Books/McGraw-Hill, Medical Pub. Division: New York. p. 253 - 282.
98. Liu, S.S., Hodgson, Peter, Local Anesthetics, in Clinical Anesthesia, P.G. Barash, Editor. 2001, Lippincott Williams & Wilkins: Philadelphia. p. 458.
99. Strichartz, G.R., Berde, Charles B., Local Anesthetics, in Miller's Anesthesia, R.D. Miller, Editor. 2005, Churchill Livingstone: New York. p. 573 - 603.
100. Tetzlaff, J., Spinal, Epidural, and Caudal Blocks, in Clinical Anesthesiology, G.E. Morgan, Editor. 2002, Lange: Stamford.
101. Veering, B.T., et al., Epidural anesthesia with bupivacaine: effects of age on neural blockade and pharmacokinetics. Anesth Analg, 1987. 66(7): p. 589-93.
102. Wu, C., Acute Postoperative Pain, in Miller's Anesthesia, R.D. Miller, Editor. 2005, Churchill Livingstone: New York. p. 2737 - 2741.
103. Greene, N.M., Distribution of local anesthetic solutions within the subarachnoid space. Anesth Analg, 1985. 64(7): p. 715-30.
104. Chandrasekhar, S., Pian-Smith, May, Spinal, Epidural, and Caudal Anesthesia, in Clinical Anesthesia Procedures of the Massachusetts General Hospital, W. Hurford, Editor. 2002, Lippincott Williams & Wilkins: New York. p. 231 - 252.
105. Taylor, P., Tetracaine Drug insert, Taylor Pharmaceuticals Decatur, IL 62522. 106. Hospira, Bupivacaine (Bupivacaine and Dextrose) Drug Insert. 2004, HOSPIRA,
INC.: Lake Forest, IL 60045 USA.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
82
107. Hospira, Lidocaine Hydrochloride and Dextrose - Drug Insert. 2004, HOSPIRA, INC.: Lake Forest, IL 60045 USA.
108. Hospira, Novocaine (Procaine Hydrochloride) Injection- Drug Insert. 2004, HOSPIRA, INC.: Lake Forest, IL 60045 USA.
109. AstraZeneca, Naropin (ropivacaine HCl) Injection - package insert. 2006: Wilmington, DE 19850.
110. Bromage, P.R., Spread of analgesic solutions in the epidural space and their site of action: a statistical study. Br J Anaesth, 1962. 34: p. 161-78.
111. Park, W.Y., et al., Age and the spread of local anesthetic solutions in the epidural space. Anesth Analg, 1980. 59(10): p. 768-71.
112. BedfordLabs, Chloroprocaine - package insert. 2005, Bedford Labs: Bedford, OH 44146.
113. Hospira, Lidocaine hydrochloride (Lidocaine Hydrochloride) injection FOR INFILTRATION AND NERVE BLOCK. 2004, HOSPIRA, INC.: Lake Forest, IL 60045 USA.
114. Hospira, bupivacaine hydrochloride (Bupivacaine Hydrochloride) injection Drug Insert. 2004, HOSPIRA, INC.: Lake Forest, IL 60045 USA.
115. Hospira, Carbocaine (Mepivacaine Hydrochloride) injection, solution package insert. 2004, HOSPIRA, INC.: Lake Forest, IL 60045 USA.
116. Lubenow, T., R., Ivankovich, Anthony D., Mccarthy, Robert J., Management of Acute Postoperative Pain, in Clinical anesthesia, P.G. Barash, Editor. 2001, Lippincott Williams & Wilkins: Philadelphia. p. 1403 - 1434.
117. Baxter, Duramorph - package insert. 2004, Baxter Healthcare Corporation: Deerfield, IL 60015 USA.
118. Pasero, C., Portenoy, R., McCaffery, M. , Opioid Analgesics, in Pain: Clinical Manual, P.C. McCaffery M., Editor. 1999, Mosby: St. Louis. p. 161-299.
119. Sinatra, R.S., Acute Pain Management and Acute Pain Services, in Clinical Anesthesia and Management of Pain, M. Cousins, Editor. 1998. p. 808.
120. American Heart Association, Handbook of Emergency Cardiovascular Care for healthcare providers, ed. M.F. Hazinski. 2000: American Heart Association. .
121. Katzung, B.G., Basic & Clinical Pharmacology. 9th ed. 2001, New York: Lange Medical Books/McGraw-Hill, Medical Pub. Division.
122. PDR, 2007 Physicians' Desk Reference. 2007, Thomson PDR: Montvale, NJ. 123. Gahart, B.L., Nazareno, Adrienne R., 2006 Intravenous medications. 22nd ed.
2006, St Louis: Elsevier Mosby. 124. Tsuneyoshi, I., et al., Low-dose vasopressin infusion in patients with severe
vasodilatory hypotension after prolonged hemorrhage during general anesthesia. J Anesth, 2005. 19(2): p. 170-3.
125. Treschan, T.A. and J. Peters, The vasopressin system: physiology and clinical strategies. Anesthesiology, 2006. 105(3): p. 599-612; quiz 639-40.
126. Krismer, A.C., et al., Vasopressin during cardiopulmonary resuscitation and different shock states: a review of the literature. Am J Cardiovasc Drugs, 2006. 6(1): p. 51-68.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
83
127. Lechner, E., et al., Vasodilatory shock after surgery for aortic valve endocarditis: use of low-dose vasopressin. Pediatr Cardiol, 2004. 25(5): p. 558-61.
128. Tsuneyoshi, I., et al., Hemodynamic and metabolic effects of low-dose vasopressin infusions in vasodilatory septic shock. Crit Care Med, 2001. 29(3): p. 487-93.
129. Malignant_Hyperthermia_Investigation_Unit, MALIGNANT HYPERTHERMIA. 2000: Toronto, ON M5G 2C4
130. MHAUS, MALIGNANT HYPERTHERMIA. 2000: Sherburne, NY. 131. Seidel, H.M., Mosby's physical examination handbook. 2nd ed. 1999, St. Louis,
MO: Mosby. 132. National High Blood Pressure Education Program Working Group on High Blood
Pressure in Children and Adolescents, The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics 2004. 114: p. 555-576.
133. Eichhorn, J.H., ASA Adopts Basic Monitoring Standards. Anesthesia Patient Safety Foundation Newletter, 1987. 2(1): p. 1 - 8.
134. Allen, G.S., et al., Postoperative respiratory complications in ex-premature infants after inguinal herniorrhaphy. J Pediatr Surg, 1998. 33(7): p. 1095-8.
135. Bryson, G.L., et al., Patient selection in ambulatory anesthesia - an evidence-based review: part II. Can J Anaesth, 2004. 51(8): p. 782-94.
136. Cote, C.J., et al., Postoperative apnea in former preterm infants after inguinal herniorrhaphy. A combined analysis. Anesthesiology, 1995. 82(4): p. 809-22.
137. Pagana, K.D. and T.J. Pagana, Mosby's manual of diagnostic and laboratory tests. 2nd ed. 2002, St. Louis: Mosby.
138. Hopkins, T.B., Lab Notes: Guide to Lab & Diagnostic Tests. 2005, Philadelphia: F.A. Davis Company.
139. Fischbach, F.T. and M.B. Dunning, A manual of laboratory and diagnostic tests. 7th ed. 2004, Philadelphia: Lippincott Williams & Wilkins.
140. Mathews, P., Predicting Arterial Blood-Gas Results. RT The Journal for Respiratory Care Practitioners, 2000.
141. Grogono, A.W., Acid-Base Tutorial. 2006, www.acid-base.com. 142. Americain Heart Association, Guidelines 2000 for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Part 8: Advanced Challenges in Resuscitation. Circulation, 2000. 102(I - 217).
143. Rastegar, A. and M. Soleimani, Hypokalaemia and hyperkalaemia. Postgrad Med J, 2001. 77(914): p. 759-64.
144. Brown, R.S., Potassium homeostasis and clinical implications. Am J Med, 1984. 77(5A): p. 3-10.
145. Natalini, G., et al., Acute respiratory acidosis does not increase plasma potassium in normokalaemic anaesthetized patients. A controlled randomized trial. Eur J Anaesthesiol, 2001. 18(6): p. 394-400.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
84
146. Wiederseiner, J.M., et al., Acute metabolic acidosis: characterization and diagnosis of the disorder and the plasma potassium response. J Am Soc Nephrol, 2004. 15(6): p. 1589-96.
147. Bailey, J.M., Context-sensitive half-times: what are they and how valuable are they in anaesthesiology? Clin Pharmacokinet, 2002. 41(11): p. 793-9.
148. Brambrink, A.M., R.R. Meyer, and F.J. Kretz, [Management of pediatric airway--anatomy, physiology and new developments in clinical practice]. Anaesthesiol Reanim, 2003. 28(6): p. 144-51.
149. Butler, K.H. and B. Clyne, Management of the difficult airway: alternative airway techniques and adjuncts. Emerg Med Clin North Am, 2003. 21(2): p. 259-89.
150. Cannesson, M., et al., Relation between respiratory variations in pulse oximetry plethysmographic waveform amplitude and arterial pulse pressure in ventilated patients. Crit Care, 2005. 9(5): p. R562-8.
151. Cannesson, M., et al., Respiratory variations in pulse oximeter waveform amplitude are influenced by venous return in mechanically ventilated patients under general anaesthesia. Eur J Anaesthesiol, 2006: p. 1-7.
152. Cherng, C.H., et al., Airway length in adults: estimation of the optimal endotracheal tube length for orotracheal intubation. J Clin Anesth, 2002. 14(4): p. 271-4.
153. Cote, C.J., et al., Ionized hypocalcemia after fresh frozen plasma administration to thermally injured children: effects of infusion rate, duration, and treatment with calcium chloride. Anesth Analg, 1988. 67(2): p. 152-60.
154. Culpepper, T.L., AANA Journal course: update for nurse anesthetists--intraoperative fluid management for the pediatric surgical patient. Aana J, 2000. 68(6): p. 531-8.
155. De Backer, D., Stroke volume variations. Minerva Anestesiol, 2003. 69(4): p. 285-8.
156. Eger, E.I., 2nd, A brief history of the origin of minimum alveolar concentration (MAC). Anesthesiology, 2002. 96(1): p. 238-9.
157. Eger, E.I., 2nd, Characteristics of anesthetic agents used for induction and maintenance of general anesthesia. Am J Health Syst Pharm, 2004. 61 Suppl 4: p. S3-10.
158. Eger, E.I., 2nd, et al., Women appear to have the same minimum alveolar concentration as men: a retrospective study. Anesthesiology, 2003. 99(5): p. 1059-61.
159. Eger, E.I., 2nd and L.J. Saidman, Illustrations of inhaled anesthetic uptake, including intertissue diffusion to and from fat. Anesth Analg, 2005. 100(4): p. 1020-33.
160. Eger, E.I., 2nd and S. Shafer, The complexity of recovery from anesthesia. J Clin Anesth, 2005. 17(6): p. 411-2.
161. Eger, E.I., 2nd and J.M. Sonner, Anaesthesia defined (gentlemen, this is no humbug). Best Pract Res Clin Anaesthesiol, 2006. 20(1): p. 23-9.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
85
162. Eger, E.I., 2nd and J.M. Sonner, How likely is awareness during anesthesia? Anesth Analg, 2005. 100(5): p. 1544; author reply 1545.
163. Gepts, E., New concepts in pharmacokinetics and pharmacodynamics. Acta Anaesthesiol Belg, 1997. 48(4): p. 199-204.
164. Hofer, C.K., et al., Stroke volume and pulse pressure variation for prediction of fluid responsiveness in patients undergoing off-pump coronary artery bypass grafting. Chest, 2005. 128(2): p. 848-54.
165. Hughes, M.A., P.S. Glass, and J.R. Jacobs, Context-sensitive half-time in multicompartment pharmacokinetic models for intravenous anesthetic drugs. Anesthesiology, 1992. 76(3): p. 334-41.
166. Kapila, A., et al., Measured context-sensitive half-times of remifentanil and alfentanil. Anesthesiology, 1995. 83(5): p. 968-75.
167. Karason, S., et al., Direct tracheal airway pressure measurements are essential for safe and accurate dynamic monitoring of respiratory mechanics. A laboratory study. Acta Anaesthesiol Scand, 2001. 45(2): p. 173-9.
168. Kee, W.D., K.S. Khaw, and F.F. Ng, Prevention of hypotension during spinal anesthesia for cesarean delivery: an effective technique using combination phenylephrine infusion and crystalloid cohydration. Anesthesiology, 2005. 103(4): p. 744-50.
169. Kennedy, R.R. and A.B. Baker, The effect of cardiac output changes on end-expired volatile anaesthetic concentrations--a theoretical study. Anaesthesia, 2001. 56(11): p. 1034-40.
170. Kessler, V., J. Guttmann, and C.J. Newth, Dynamic respiratory system mechanics in infants during pressure and volume controlled ventilation. Eur Respir J, 2001. 17(1): p. 115-21.
171. Lu, C.C., et al., Pharmacokinetics of sevoflurane uptake into the brain and body. Anaesthesia, 2003. 58(10): p. 951-6.
172. Masters, I.B., et al., Airway sizes and proportions in children quantified by a video-bronchoscopic technique. BMC Pulm Med, 2006. 6: p. 5.
173. McFarlan, C.S., B.J. Anderson, and T.G. Short, The use of propofol infusions in paediatric anaesthesia: a practical guide. Paediatr Anaesth, 1999. 9(3): p. 209-16.
174. Michard, F., Changes in arterial pressure during mechanical ventilation. Anesthesiology, 2005. 103(2): p. 419-28; quiz 449-5.
175. Min, J., Haddad, Tanina., Anesthesia for Obstetrics and Gynecology, in Clinical anesthesia procedures of the Massachusetts General Hospital. 2007, Lippincott Williams & Wilkins: Philadelphia. p. 500.
176. Nakayama, M., et al., Hemodynamic and bispectral index responses to tracheal intubation during isoflurane or sevoflurane anesthesia. J Anesth, 2003. 17(4): p. 223-6.
177. Nyssen, A.S., et al., A comparison of the training value of two types of anesthesia simulators: computer screen-based and mannequin-based simulators. Anesth Analg, 2002. 94(6): p. 1560-5, table of contents.

ACTc Version 3.0 tutorial Reproduction and Distribution prohibited unless authorized by Gasshead LLC
Copyright 2004, 2005, 2006, 2007 US Patent Pending
86
178. Pal, S.K., G.G. Lockwood, and D.C. White, Uptake of isoflurane during prolonged clinical anaesthesia. Br J Anaesth, 2001. 86(5): p. 645-9.
179. Paul, M., et al., A randomized, controlled study of fluid management in infants and toddlers during surgery: hydroxyethyl starch 6% (HES 70/0.5) vs lactated Ringer's solution. Paediatr Anaesth, 2003. 13(7): p. 603-8.
180. Price, J.D., J.W. Sear, and R.M. Venn, Perioperative fluid volume optimization following proximal femoral fracture. Cochrane Database Syst Rev, 2004(1): p. CD003004.
181. Reed, M.J., M.J. Dunn, and D.W. McKeown, Can an airway assessment score predict difficulty at intubation in the emergency department? Emerg Med J, 2005. 22(2): p. 99-102.
182. Reed, M.J., et al., Is the 'LEMON' method an easily applied emergency airway assessment tool? Eur J Emerg Med, 2004. 11(3): p. 154-7.
183. Rodriguez, R.A., et al., The bispectral index does not correlate with clinical signs of inhalational anesthesia during sevoflurane induction and arousal in children. Can J Anaesth, 2004. 51(5): p. 472-80.
184. Runciman, W.B., et al., Crisis management during anaesthesia: cardiac arrest. Qual Saf Health Care, 2005. 14(3): p. e14.
185. Tavernier, B., et al., Systolic pressure variation as a guide to fluid therapy in patients with sepsis-induced hypotension. Anesthesiology, 1998. 89(6): p. 1313-21.
186. van den Berg, A.A. and T. Mphanza, Choice of tracheal tube size for children: finger size or age-related formula? Anaesthesia, 1997. 52(7): p. 701-3.
187. Venn, R., et al., Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Br J Anaesth, 2002. 88(1): p. 65-71.
188. Waikar, S.S. and G.M. Chertow, Crystalloids versus colloids for resuscitation in shock. Curr Opin Nephrol Hypertens, 2000. 9(5): p. 501-4.
189. Wiesenack, C., et al., Assessment of fluid responsiveness in mechanically ventilated cardiac surgical patients. Eur J Anaesthesiol, 2005. 22(9): p. 658-65.
190. Yemen, T., Pediatric anesthesia handbook. 2002, New York: McGraw-Hill, Medical Pub. Division.
191. Zausig, Y.A., M.A. Weigand, and B.M. Graf, [Perioperative fluid management : An analysis of the present situation.]. Anaesthesist, 2006. 55(4): p. 371-90.