Embed Size (px)
Citation preview

R
C
A
E
a
b
c
RA
I
Wrndoof
0h
ev Bras Anestesiol. 2014;64(2):128---130
REVISTABRASILEIRA DEANESTESIOLOGIA Official Publication of the Brazilian Society of Anesthesiology
www.sba.com.br
LINICAL INFORMATION
nesthesia for a child with Walker---Warburg syndrome
mine Arzu Kosea,∗, Bulent Bakarb, Gokay Atesa, Didem Aliefendiogluc, Alpaslan Apana
Department of Anesthesiology and Reanimation, School of Medicine, Kirikkale University, Kirikkale, TurkeyDepartment of Neurosurgery, School of Medicine, Kirikkale University, Kirikkale, TurkeyDepartment of Neonatology, School of Medicine, Kirikkale University, Kirikkale, Turkey
eceived 30 October 2012; accepted 19 December 2012vailable online 11 October 2013
KEYWORDSWalker---WarburgSyndrome;Congenital musculardystrophy;General anesthesia
AbstractBackground and objectives: Walker---Warburg Syndrome is a rare, autosomal recessive con-genital muscular dystrophy manifested by central nervous system, eye malformations andpossible multisystem involvement. The diagnosis is established by the presence of four crite-ria: congenital muscular dystrophy, type II lissencephaly, cerebellar malformation, and retinalmalformation. Most of the syndromic children die in the first three years of life because ofrespiratory failure, pneumonia, seizures, hyperthermia and ventricular fibrillation.Case report: The anesthetic management of a two-months-old male child listed for electiveventriculo-peritoneal shunt operation was discussed.Conclusions: A careful anesthetic management is necessary due to the multisysteminvolvement. We reported anesthetic management of a two-months-old male child with
Walker---Warburg Syndrome who was listed for elective ventriculo-peritoneal shunt operation.© 2013 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. All rightsreserved.owomcl
ntroduction
alker---Warburg Syndrome (WWS) is a rare, autosomalecessive congenital muscular dystrophy (CMD).1 The diag-osis is generally depends on clinical manifestations, geneticiagnosis has been made by DNA analysis only in 10---20%
f the cases. The diagnosis is established by the presencef four criteria: CMD, type II lissencephaly, cerebellar mal-ormation, and retinal malformation.2 The other frequently∗ Corresponding author.E-mail: [email protected] (E.A. Kose).
medrbdr
104-0014/$ – see front matter © 2013 Sociedade Brasileira de Anestesiottp://dx.doi.org/10.1016/j.bjane.2012.12.002
bserved abnormalities are ventricular dilatation with orithout hydrocephalus, anterior chamber malformationf eye, congenital macrocephaly, Dandy---Walker malfor-ation. Congenital microcephaly, microphthalmia, ocular
oloboma, congenital cataract, urogenital anomalies, cleftip and cleft palate are the less frequently observed abnor-alities. Differential diagnosis with Fukuyama CMD, muscle-
ye-brain disease, cerebro-ocular-cerebral syndrome isepend on the severity of the clinical manifestations and
adiological findings.2,3 Clinical manifestation are present atirth or or appears after in a short period. Most of the syn-romic children dies in the first three years of life because ofespiratory failure, pneumonia, seizures, hyperthermia andlogia. Published by Elsevier Editora Ltda. All rights reserved.

Anesthesia in Walker---Warburg syndrome 129
abnesis (
emoheDr
pbtpsi
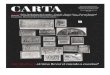
Figure 1 FLAIR MR scan images demonstrating Dandy---WalkerT2 WI MR scan image demonstrating septum pellucidum dysgen
ventricular fibrillation. Prenatal diagnosis is possible and therisk of having another child with this syndrome is 25% in thefamilies with one affected child.4
Case report
A two-months-old male child weighing 3.3 kg was listedfor elective ventriculo-peritoneal shunt operation. Deliveryhad been by cesarean section at the 38th weeks of gesta-tion. The mother’s previous gestation had been ended bymedical abortus due to determined hydrocephalus by ultra-sonographic evaluations and the parents were relative. Thepatient was admitted to intensive care unit of newborn
because of hydrocephalus and respiratory distress. Macro-cephalia, low nasal bridge, frontal bulging of the forehead,micrognathia, receding mandible, moderate hypotonia, andbilateral retinal detachment were determined by physicalgTle
ormality (A and D); and lissencephaly with hydrocephalus (B).C).
xamination. Creatine phosphokinase (CPK) levels wereeasured as 4226 u L−1 (normal 24---195 u L−1). Magnetic res-
nance imaging (MRI) was revealed type II lissencephaly,ypomyelination of white matter, dilated ventricles, bilat-ral cerebellar hypoplasia, agesis of septum pellucidum,andy---Walker malformation, bilateral hyperplasia of vit-eus and buphthalmus (Fig. 1).
After obtaining written informed parental consent, theatient was fasted for 3 h. The probability of difficult entu-ation was thought and equipment was prepared. Followinghe monitorization of pulse oxymetry, noninvasive bloodressure, electrocardiography, body temperature, anesthe-ia induction was made with sevoflurane and nitrous oxiden oxygen. An intravenous cannula was inserted and laryn-
oscopy was performed during spontaneous ventilation.he intubation attempts performed using traditional mid-ine approach with anterior cervical pressure and increasedxtension of head were failed, view was evaluated as grade

1
4arbbeceproomsdseaui
D
Amkicwsssnfdtetgwgbtpocm
hdipdtppns
ncrubd
sptpwaqsd
ai
C
T
R
1
2
3
30
. Therefore, the patient’s head was slightly turned to leftnd Miller size zero straight blade was introduced extremeight side of the mouth. The tip of the epiglottis visualizedy the aid of the external manipulation of the larynx andlind intubation was performed by using a 3.5 mm uncuffedndotracheal tube. The endotracheal tube placement wasonfirmed with capnography and auscultation of lungs. Thendotracheal tube was fixed and an oropharyngeal throatack was inserted. Anesthesia was maintained with sevoflu-ane 2% with oxygen and nitrous oxide mixture in the ratiof 50:50. Neither neuromuscular blocker agents nor opi-ids were used during the surgery. Fluid management wasade intravenous administration of balanced electrolyte
olution regarding the calculation of the perioperative fluideficits and basal requirement of the child. At the end of theurgery, the throat pack was removed, and the trachea wasxtubated when the patient was full-awake. Postoperativenalgesia was provided with paracetamol 25 mg kg---1. After aneventful recovery period, the patient was taken into thentensive care unit.
iscussion
careful anesthetic management is necessary due to theultisystem involvement. Difficult airway should always
eep in mind because of short neck, micrognathia, reced-ng mandible and sometimes accompanied cleft lip and/orleft palate. After the difficult intubation preparation,e preferred inhalation induction with sevorane without
uppression of spontan ventilation. Due to the intrusion pos-ibility of a curved blade into the view line, Miller size zerotraight blade was used but visualization of larynx couldot be provided by the traditional midline approach. There-ore, paraglossal straight blade laryngoscopy described inifficult tracheal intubation was used and blind intuba-ion was performed after visualization of the tip of thepiglottis.5 Lateral approach was provided to bypass theongue and maxillary structures and improved view of thelottis. In case of unsuccessful intubation, our back-up planas to perform fiber-optic laryngoscopy. The use of laryn-eal mask airway was discussed but was not preferredecause to provide a safe airway could be impossible dueo the movements of head during the operation and the
robability of the aspiration of the oropharyngeal secreti-ns. To use the succinylcholine was avoided because it canause exaggerated potassium release, fatal cardiac dysrhyt-ias and malign hyperthermia. Because of the increased4
5
E.A. Kose et al.
yperthermia risk in WWS, body temperature was monitoreduring the surgery and postoperative period.2,3 Nondepolar-zing muscle relaxants and opioids were not used due to theossibility of delayed recovery and postoperative respiratoryepression resulting from the chronic weakness of respira-ory muscles.2,3 Postoperative analgesia was provided witharacetamol, heavy sedation was avoided. Postoperativeulmonary dysfunction and consequent aspiration pneumo-ia was kept in the mind and oropharyngeal secretions wereuctioned regularly.
Although, our patient had not any cardiac or genitouri-ary abnormality, renal dysfunction and involvement ofardiac muscles can observe in WWS and it is important toecognize the increased perioperative cardiac and renal fail-re risk.2 Maintenance of adequate fluid management shoulde provide to avoid the renal dysfunction and cardiovascularepression.
Children with WWS may have increased intracranial pres-ure (ICP), so anesthetic management should include therecautions to provide adequate cerebral circulation such aso avoid the excessive decrease or increase in mean arterialressure.3 It is also important to recognize that the patientsith WWS are prone to develop seizures, episodes of centralnd obstructive apnea, difficulty in swallowing and conse-uent cardiorespiratory failure, aspiration pneumonia andepsis.2,3 It should be avoid the use of the epileptogenicrugs and hypoxic episodes which can lead to seizures.
In summary, for an unevenful anesthetic managementnd postoperative care it should be keep in mind that WWSs a severe CMD with multisystemic involvement.
onflicts of interest
he authors declare no conflicts of interest.
eferences
. Walker AE. Lissencephaly. Arch Neurol Psychiatry.1942;48:13---29.
. Dobyns WB, Pagon RA, Armstrong D, et al. Diagnostic criteria forWalker---Warburg syndrome. Am J Med Genet. 1989;32:195---210.
. Sahajanda H, Meneges J. Anaesthesia for a child withWalker---Warburg syndrome. Pediatr Anesth. 2003;13:624---8.
. Crowe C, Jassani M, Dickerman L. The perinatal diagnosis of theWalker---Warburg syndrome. Diagnosis. 1986;6:177---85.
. Henderson J. The use of paraglossal straight blade laryngoscopyin difficult tracheal intubation. Anaesthesia. 1997;52:522---6.