Embed Size (px)
Citation preview
Anesthesia in Laser Surgery
R1 Minghui Hung
Department of Anesthesiology, NTUH
“Never are cooperation and communication between surgeon and anesthesiologist more important than during head and neck surgery.”
Morgan, Clinical Anesthesiology
Physics of Laser light (I)
Light Amplification by Stimulated Emission of Radiation
Electromagnetic radiation Einstein:
all electromagnetic radiation consisted of wavelike quanta called photons
→E (J) = h v
Wavelength for visible light ranges from 385nm to 760 nm
Physics of Laser light (II)
Characteristics: Monochromatic (one wavelength)Coherent (oscillates in the same phase)Collimated (exists as a narrow, parallel beam)
Intense light beams, intense energy to small target sites
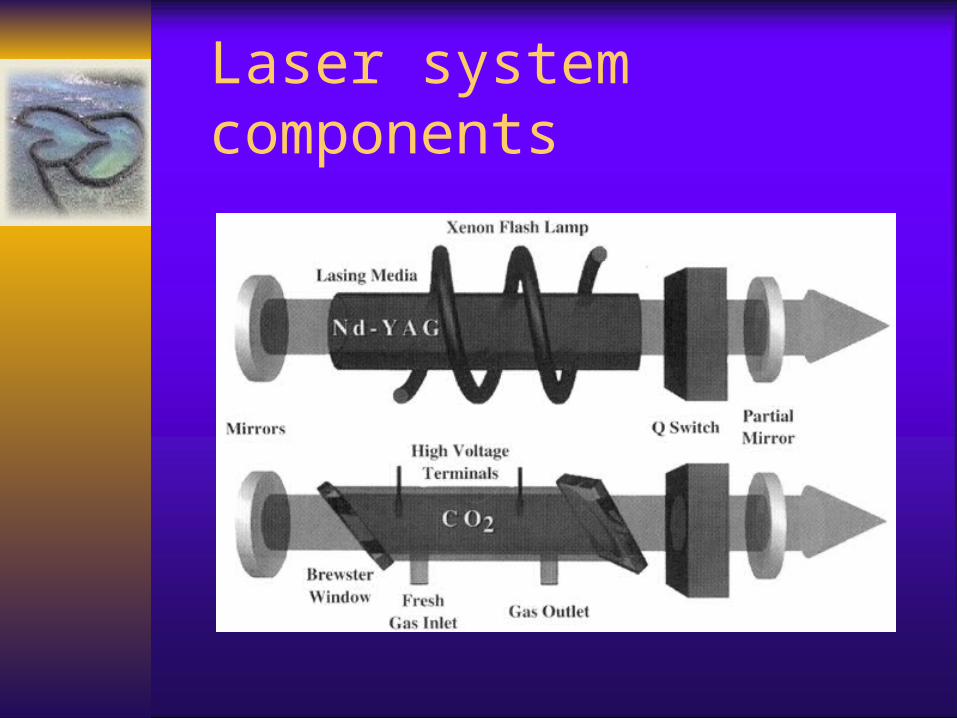
Laser system components
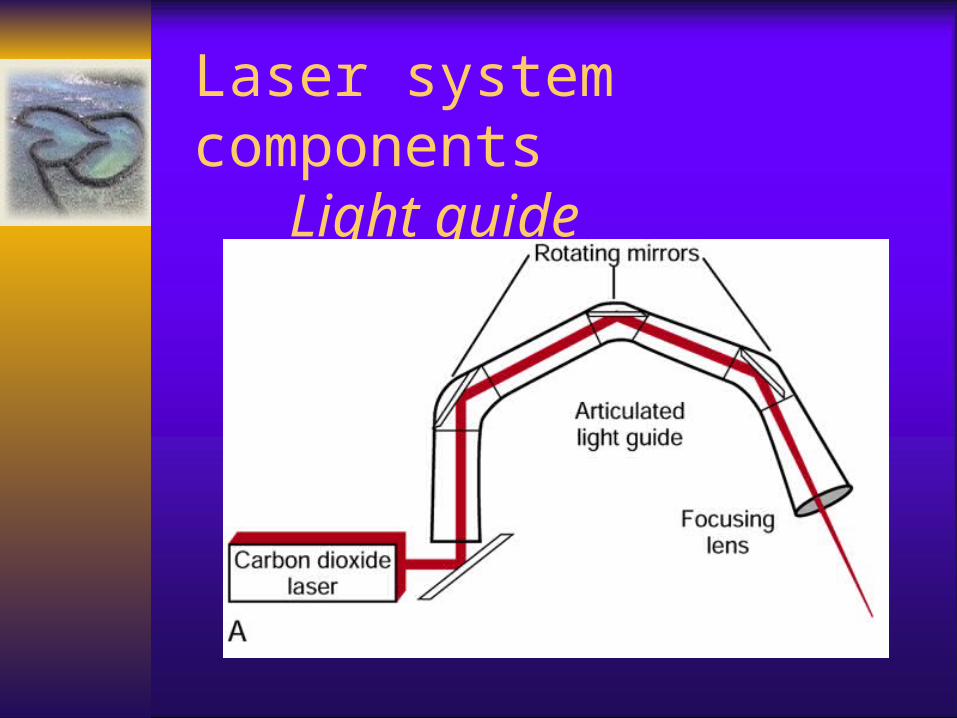
Laser system componentsLight guide
Used as scalpels and electrocoagulators
Dermatology, thoracic surgery, ophthalmology, gynaecology, plastics, ENT, urology and neurosurgery
Clinical applications
Laser interaction with tissue
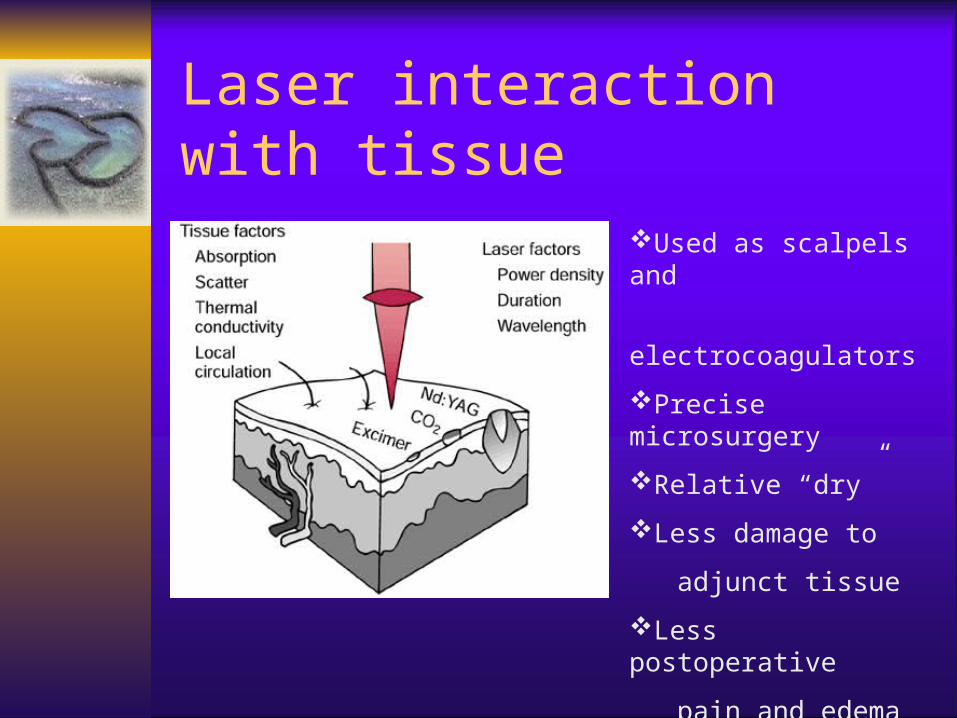
Used as scalpels and
electrocoagulators
Precise microsurgery
Relative “dry”
Less damage to
adjunct tissue
Less postoperative
pain and edema
Common used Laser lights
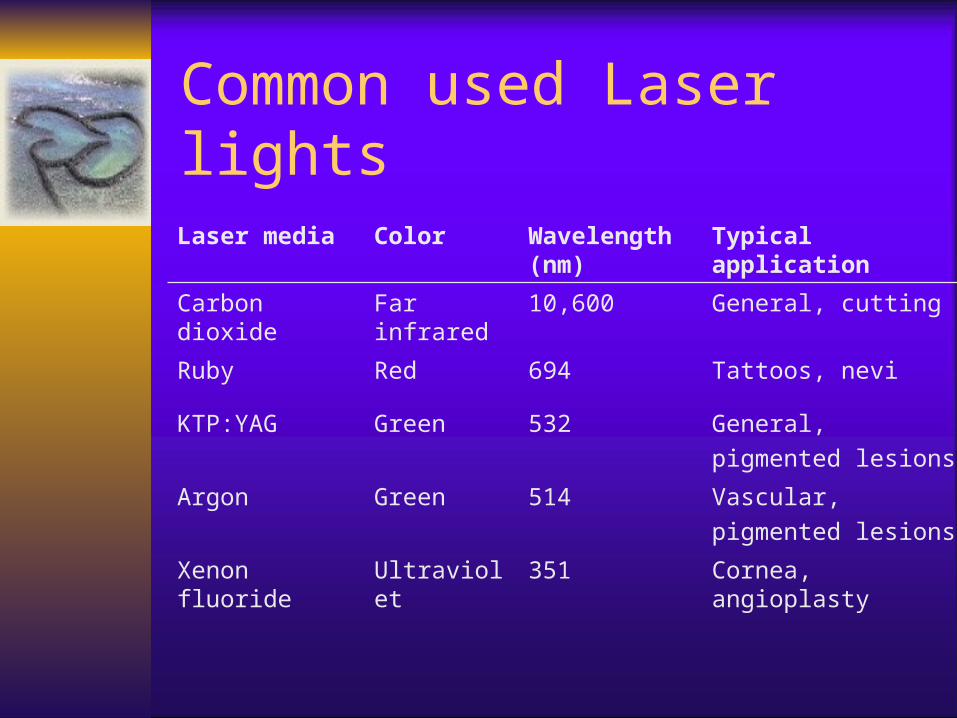
Laser media Color Wavelength (nm)
Typical application
Carbon dioxide Far infrared 10,600 General, cutting
Ruby Red 694 Tattoos, nevi
KTP:YAG Green 532 General,
pigmented lesions
Argon Green 514 Vascular,
pigmented lesions
Xenon fluoride Ultraviolet 351 Cornea, angioplasty
Atmospheric contamination Perforation of a vessels or structure Embolism Inappropriate energy transfer
Laser Hazards
Plume of smoke and fine particulates (mean size 0.31um)
Efficiently transported and deposited in the alveoli Sensitive individuals: headaches, tearing, and
nausea after inhalation Animal study: interstitial pneumonia, bronchiolitis,
reduced mucociliary clearance, inflammation, emphysema
Prevention → smoke evacuator → high-efficiency masks
Atmospheric contamination
Misdirected laser energy may perforate a viscus or a large blood vessel
Laser-induced pneumothorax Perforation may occur several days later
when edema and necrosis are maximal
Perforation
Venous gas embolism when laparoscopic or hysteroscopic laser surgery
At hysteroscopy, liquid (saline) coolant is the only safe option
If coolant gas must be used, CO2 should be considered
→ Continuous airway CO2 monitoring
Venous gas embolism
Incidentally pressing the laser control trigger
Tissue damage outside of surgical site Drape fire Eye (patient or other medical staff) Endotracheal tube fires
Inappropriate energy transfer
Incidence: 0.5 – 1.5 % Source:
– direct laser illumination– reflected laser light– incandescent particles of tissue blown from
the surgical site
Endotracheal tube fires
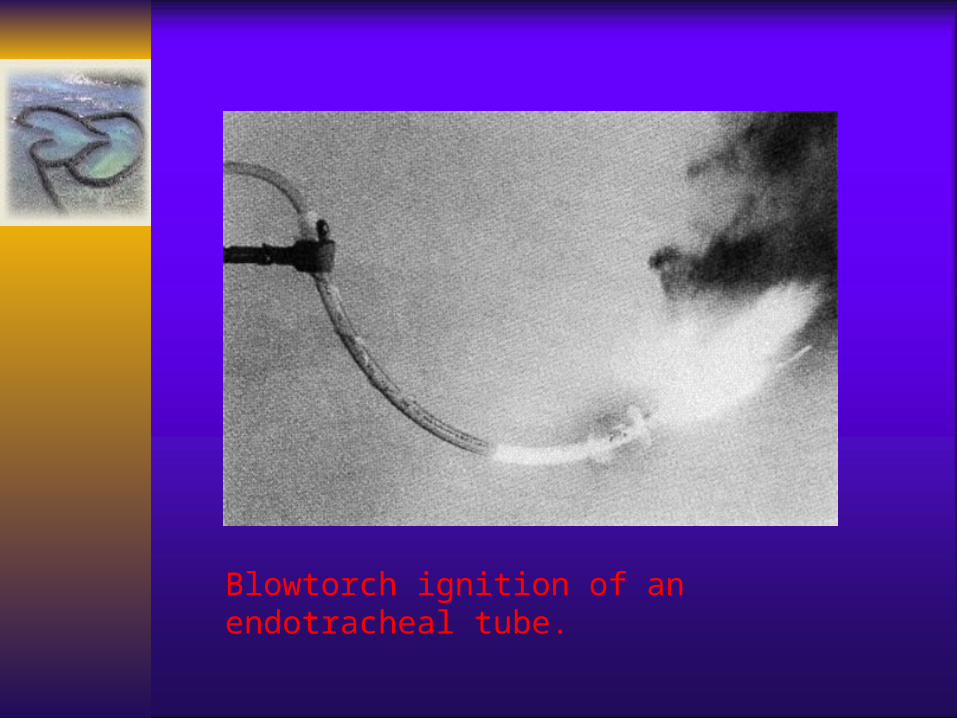
Blowtorch ignition of an endotracheal tube.
Approaches to reduce the incidence of airway fire
Reduce the flammability of the endotracheal tube
Use Venturi ventilation Use intermittent apnea technique
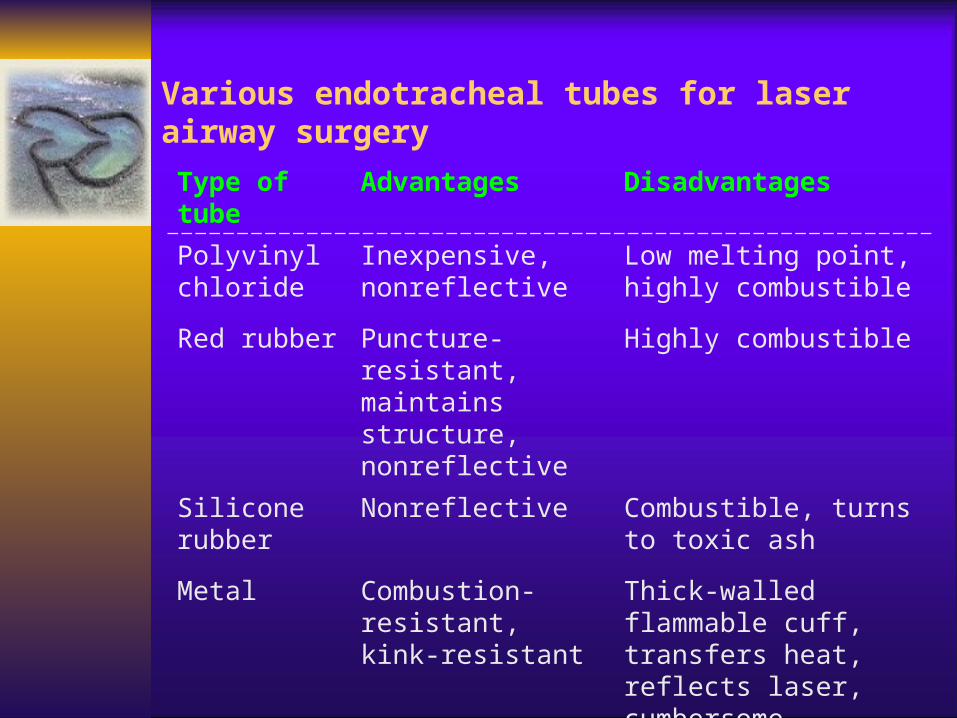
Various endotracheal tubes for laser airway surgery
Type of tube Advantages Disadvantages
Polyvinyl chloride
Inexpensive, nonreflective
Low melting point, highly combustible
Red rubber Puncture-resistant, maintains structure, nonreflective
Highly combustible
Silicone rubber
Nonreflective Combustible, turns to toxic ash
Metal Combustion-resistant, kink-resistant
Thick-walled flammable cuff, transfers heat, reflects laser, cumbersome
wrapping with moistened muslin coating with dental acrylic wrapping with metallized foil tape
→ most popular approach aluminum foil copper foil plastic tape thinly coated with metal
Protection of the endotracheal tubes

Cuff wrapping technique
methylene blue
stained saline
instead of air
No cuff protection Adds thickness to tube Not an FDA-approved device Protection varies with type of metal foil Adhesive backing may ignite May reflect laser onto non-targeted tissue Rough edges may damage mucosal surfacess
Disadvantages of wrapping
Oxygen and nitrous oxide are powerful oxidizers
Reduce FiO2 to minimum concentration
Helium may benefit as a diluent gas Volatile anesthetics currently used are
nonflammable and nonexplosive Pyrolized toxic compounds
Effect of high oxygen and nitrous oxide gas mixture
Norton. spiral wound stainless steel ETT Bivona Fome-Cuff. aluminium spiral tube with
a silicone polyurethane foam cuff Xomed Laser-Shield. silicone elastomer tube
containing metallic powder Mallinckrodt Laser-Flex. airtight stainless
steel spiral wound tube with two PVC cuffs
Metal endotracheal tubes
Barotrauma Pneumothorax Restriction to only intravenous agents Gastric distention Relative requirement for compliant lungs
Jet ventilation
Intermittent apnea technique Hypoventilation Pulmonary aspiration
Remove source of fire (the laser!). Stop ventilating, disconnect circuit, extubate. Extinguish fire in bucket of water (MUST have
one ready!). Mask ventilate with 100% O2, continue
anaesthesia i.v. Direct laryngoscopy & rigid bronchoscopy for
damage and debris.
Airway fires protocol (I)
Reintubate if damage. Blowtorch fire may need distal fibreoptic
bronchoscopy and lavage. Severe damage may need low
tracheostomy. Assess oropharynx and face. CXR. Steroids.
Airway fires protocol (II)

I am a sheep.
SHEEP me 2.
We wish you…
羊 羊 得 意