Embed Size (px)
DESCRIPTION
hjjg
Citation preview

ANESTHESIA:Principles and Practice

And last, not least, in each perplexing case,Learn the sweet magic of a cheerful face;Not always smiling, but at least serene,
When grief and anguish cloud the anxious scene.Each look, each movement, every word and tone,Should tell your patient you are all his own.
-DR. OLIVER WENDELL HOLMuE



ANESTHESIA:
Principles and Practice
A PRESENTATION FOR THE NURSING
PROFESSION BY Alice M. Hunt
FOUNDED 838
GIP
G. P. PUTNAM'S SONS: NEW YORK

COPYRIGHT, 1949, BY G. P. PUTNAM'S SONS
All rights reserved. This book, or parts thereof, mustnot be reproduced in any form without permission.
Manufactured in the United States of America

FOREWORD
IT is a pleasure to have the opportunity ofacknowledging the great obligation which the SurgicalDepartment of the Yale University School of Medi-cine and the surgeons operating in the New HavenHospital these past twenty-five years have owed MissHunt for her skill and her devotion to the welfare ofthe patient in the performance of her duties as ateacher and a practitioner in the field of anesthesia.It is indeed fortunate that she has had the oppor-tunity and the desire to summarize her experience inthis manner.
Whether or not the nurse will continue to have asimportant a role in the field of anesthesia as she hashad in the recent past, it will always remain true thatshe, whatever her activities may be, will need to havean intelligent understanding of anesthesia, and it isto this end that this book has been written. The pro-fessional anesthetist will of course seek elsewhere formore detailed and technical information, but nowherewill the intimate concern for the welfare of thepatient, which is or should be the primary motivationof physician and nurse alike, be found better ex-pressed.
SAMUEL C, HARVEY, M.D.


CONTENTS
Foreword by Samuel C. Harvey, M.D. v
Introduction ix
I. Brief Historical Outline of SurgicalAnesthesia 3
II. Physiology of Anesthesia 13
III. Methods of Introducing SurgicalAnesthesia 19
IV. Premedication 23
V. General Immediate Preoperative andPostoperative Care of Patient 32
VI. Volatile Liquid Anesthetic Drugs: Ether,Chloroform, Ethyl Chloride, Vinethene 43
VII. Gaseous Anesthetics: Nitrous Oxide,Ethylene, Cyclopropane 63
VIII. Avertin 86
IX. Intravenous Anesthesia 93
X. Local Anesthesia 99
XI. Regional Anesthesia 104
XII. Spinal Anesthesia 107
vii

viii
XIII. Obstetrical Anesthesia
XIV. Endotracheal Anesthesia
XV. Curare
XVI. Dangerous Potentialities
XVII. Oxygen Therapy
Bibliography
Index
CONTENTS
113
121
124
129
134
139
143

ILLUSTRATIONS
FACING
PAGE
Fig. 1. Operating Table 34
Fig. 2. Wrist Straps 36
Fig. 3. Desirable Position for UnconsciousPatient 38
Fig. 4. Pharyngeal Airways 40
Fig. 5. Avertin Dosage Scale 88
Fig. 6. DuBois Body Surface Chart 90
Fig. 7. Endotracheal Apparatus 122


INTRODUCTION
THE preparation of this book was under-taken with the primary object of presenting to nursesin general a clear and practical concept of the subjectof controllable anesthesia, which has played so vital arole in the evolution of surgery from the stage of"choice of last resort" of a century ago, and all preced-ing time, to the almost limitless possibilities of thismomentous branch of medicine today.
It is the intention of the author that focus be con-centrated on the patient, not the surgeon, as rightlybeing in the center of the picture-without the patientnone of us would be necessary, surgeon, anesthetist,nurse, or hospital. In consequence, emphasis is given todetails of procedure and nursing care to enhance thecomfort and well-being of the patient, the importanceof which, unfortunately, is not in general sufficientlyappreciated as being a necessary adjunct to the per-fection of anesthesia iri each individual case. And onlywhen the course of anesthesia is smooth and undergood control can the surgeon's work proceed withcomplete accuracy and safety. Such efforts of livingup to the ideal of the Golden Rule will also be foundto pay us high dividends in personal satisfaction andthe lasting gratitude of many patients to whom thefear of "taking ether" is a very real, though perhapsnowadays an irrational, dread.
xi

Simplicity in administration of the various anes-thetic drugs, and safeguards against special dangers,are detailed for the guidance of the nurse who may atsome time of emergency find herself having to extem-porize as anesthetist. It is hoped also that a fund ofexperience, gained over many years devoted to thepractice and teaching of the art of anesthesia, mayprove helpful to those beginning their career in thisspecialty.
I have had the good fortune of participating to thefull in the modern evolution of surgical anesthesia.This I have found very stimulating and enjoyable. Iappreciate the fact that success in the enterprise wasmade possible, largely, by the trust and co-operationafforded me by the many surgeons with whom I havebeen associated over the years. I feel especially in-debted to Dr. Samuel C. Harvey, my "chief" for thelast twenty-five years, under whose sympathetic andinspiring leadership I was enabled to keep our depart-ment of anesthesia up to date.
I am grateful also to Dr. Edna H. Tompkins formuch valuable assistance in the compilation of thisbook and to Mrs. Marguerite DuMortier for her un-failing interest and encouragement in the project.
ALICE M. HUNTNew Haven, Connecticut
Xii INTRODUCTION

ANESTHESIA:Principles and Practice


Chapter
BRIEF HISTORICAL OUTLINEOF SURGICAL ANESTHESIA
IN keeping with our reactions to many mod-ern inventions that have added so much to the easeand well-being of normal daily life, we tend to lookupon controllable surgical anesthesia as so much amatter of course and necessity that we fail to appreci-ate its infinite boon and the fact that this has beenavailable to the civilized world for only one century.
At the Massachusetts General Hospital, Boston,Massachusets, on October 16, 1846, for the first timein history a group of reputable physicians were givenconvincing proof that, by inhaling ether vapor, apatient could safely be made insensible to the pain ofa surgical operation.
Over the ages, seemingly, pain had been consideredso inevitably a part of life that had to be endured thatattempts to alleviate it were sporadic and unconvinc-ing. Primitive man resented pain as an invisibledemon that could, in some unexplainable way, takepossession of his body. Charms of weird variety wereworn as guard against the demon's entrance or, once
3

enthroned, he might be exorcised by fright or magicalincantations.1
However, from time immemorial, mankind hassought palliatives to heal or soothe his pain. Probablyin his search for food he early learned that manyvegetable substances have hypnotic and analgesiceffects when chewed, or burnt and the fumes inhaled.That this knowledge was used for the relief of painas civilization progressed is evidenced by many refer-ences found in the literature of ancient Greece andRome, of China, Assyria, and Egypt, and throughoutthe early Christian era. Notable among the substancesused were henbane and the root of the mandrake-hyoscin; seed of the white poppy-opium; leaves ofthe coca tree-cocaine; and the fumes of burninghemp-Oriental hashish. There are many recipes forthe preparation of elaborate combinations of these andother vegetable substances, which are to be imbibedor inhaled by patients prior to imperative surgicaloperations, such as amputation of diseased or injuredlimbs, trephination, removal o'f bladder stone, etc.
Alcoholic beverages of sorts seem to have antedatedrecorded history, and their hypnotic effects were notedand used for the relief of pain. But crude drugs ofall kinds have many side actions, often harmful anddangerous; their general effect is unpredictable andspecific effect definitely beyond control. Not until theactive principle of opium-morphine-was discoveredby the German chemist, Friederich W. Sertiirner,2 in1806, could this most valuable narcotic drug be usedwith reasonable safety. He named the alkaloid mor-phium, after the Greek god of dreams, Morpheus. Byhis invention of the hollow needle in 1853, Dr. Alex-
1Ren6 Fiil5p-Miller, Triumph Over Pain, p. 11.
2 Thomas E. Keys, The History of Surgical Anesthesia, p. 88.
4 ANESTHESIA

BRIEF HISTORICAL OUTLINE
ander Wood of Edinburgh blazed the trail for themodern hypodermic injection of this drug.
Descriptions of surgical operations in preanestheticdays are most harrowing. For the patient to survivethe agony involved, the procedure had to be com-pleted hastily. Haste is usually the antithesis of gentle-ness, and probably surgeons became more or less cal-loused to causing pain. But the more sensitive sur-geons, doubtless, suffered with the patient and under-standingly sought means for controlling the pain.Among such, in the sixteenth century, was the famousGerman physician, Paracelsus, who, it is recorded, bycombining and distilling sulphuric acid and alcoholdiscovered ether and named it "sweet vitriol." Hemost remarkably anticipated modern medical researchby testing its effect on chickens, noting that it putthem to sleep and they subsequently awakened un-harmed. 3 He recommended that the drug be used asan anodyne, and there is evidence that it was soprescribed, more or less, through succeeding centuries,to be used in liquid form dropped on sugar or inwine.
Ether vapor seems to have been first used thera-peutically about the mid eighteenth century, when aLiverpool surgeon advised it "be snuft up the nose"repeatedly for relief of persistent headache. 4 Evi-dently it was not intended that this be continued tothe point of loss of consciousness, such being con-sidered too hazardous a procedure.
The foundation of modern surgical anesthesia hasbeen ascribed to the painstaking study of gases by theEnglish chemist, Joseph Priestley. In the late eight-eenth century he succeeded in isolating carbon
SIbid., p. 9.4 John F. Fulton and Madeline E. Stanton, The Centennial ofSurgical Anesthesia: An Annotated Catalogue, p. 22.
5

dioxide, oxygen, and nitrous oxide and stimulatedinterest in the experimental use of gases in the treat-ment of disease. 5
A "pneumatic institute" was established in Bristol,England, by a Dr. Beddoes and rapidly gained popu-larity. The famous chemist, Sir Humphrey Davy, wasemployed there as a very young man and became es-pecially interested in the study of nitrous oxide.About 1800, on inhaling the gas one day he noted asa remarkable fact that the pain of an aching tooth wasgreatly relieved, which prompted him to make theprophetic suggestion that nitrous oxide might provevaluable for the relief of pain during surgical opera-tions. But this prophecy was not fulfilled for nearlyhalf a century, despite the devoted efforts of anotheryoung Englishman, Dr. Henry H. Hickman, who hadscientifically confirmed Davy's hypothesis in 1820 butfailed to impress the bigoted medical world of Eng-land and France. It has been well said "the time wasnot ripe" for the acceptance of so startling an inno-vation.6
Nitrous oxide, when inhaled diluted with sufficientair to prevent asphyxial symptoms developing, fre-quently initiates a state of exhilaration and intoxica-tion, interesting and amusing to the subject and toobservers. Ether vapor has a similar effect. This factsoon was noted and the practice later exploited, es-pecially in America, by pseudo chemists as a lucrativeshow business, volunteers from the audience beingused for subjects. Inhaling the vapors also became apopular means of entertainment among groups ofmedical students. During these so-called "etherfrolics" subjects frequently became boisterous andactive, to the added merriment of the audience. Occa-
a Keys, op. cit., p. 14.6
Fill6p-Miller, op. cit., p. 85.
6 ANESTHESIA

BRIEF HISTORICAL OUTLINE
sionally minor injuries resulted, and it was noted in-dependently by at least two observing young men, Dr.Crawford Long of Athens, Georgia, and Dr. HoraceWells, a dentist of Hartford, Connecticut, that whileunder the influence of the gases the subject was quiteunconscious of pain at the site of injury.7
These men were sufficiently impressed to experi-ment further with the pain-control effect of the drugs,hoping to benefit their own patients thereby. Dr.Long's results with ether were so satisfactory that heaccomplished several minor surgical operations pain-lessly in the year 1842. But his practice was limited,and Athens, Georgia, so small a community that littlepublicity was given to this surprising achievement.Two years later, in 1844, the Hartford dentist, Dr.Wells, extracted teeth painlessly from patients ren-dered unconscious by the inhalation of nitrous oxide.Prematurely, he undertook to demonstrate this won-der to a group of students at Harvard Medical School.Unfortunately the patient, a young man, struggledand cried out during the extraction, and though laterhe reiterated that he had been unconscious of pain,the skeptical audience would not believe the state-ment and jeered Dr. Wells as an impostor. Thisexperience was too shocking for Dr. Wells and prac-tically finished his career.
Dr. William T. G. Morton, a dentist of Boston,Massachusetts, had been an associate of Dr. Wells andprobably was familiar with his limited use of nitrousoxide. In his efforts to find a means of relieving painfor his dental treatments, Dr. Morton, at the sugges-tion of a well-known Boston chemist, Dr. CharlesJackson, tried local application of sulphuric ether.He was prompted to experiment further with thisdrug on the family goldfish and pet dog. While so
7 Keys, op. cit., p. 24.

doing, he accidently put himself to sleep one day byinhaling the ether fumes, happily confirming his ob-servations of the relative safety of the drug as ahypnotic.
After devoting much time and effort to those stud-ies, he succeeded in persuading an outstanding sur-geon of the Massachusetts General Hospital, Dr.John C. Warren, to allow him to prove his discoveryof the efficiency of ether vapor in preventing painduring a surgical operation. The patient chosen wasa young man and he slept quietly under the influenceof ether while a small tumor was excised from hisneck by Dr. Warren, to the amazement of all theobservers.
And so, convincingly, took place the historic eventof the first public demonstration of surgical anes-thesia. The endorsement of the highly reputablemedical staff of the Massachusetts General Hospitalassured the rapid spread throughout America andEurope of the knowledge and practice of this dis-covery.
The terms "anaesthesia" and "anaesthetic," twowords of Greek origin defining the condition pro-duced and the drug employed to produce it respec-tively, were suggested to Dr. Morton by the notedauthor and physician, Dr. Oliver Wendell Holmes.With the suggestion came a warning of the need forlearned pondering in choosing a name "which willbe repeated by the tongue of every civilized race ofmankind." 8
Ether anesthesia for control of the pain of child-birth was first used by Sir James Y. Simpson of Edin-burgh, Scotland, in January 1847.9 This practice met
SFulton and Stanton, op. cit., p. 51. Albert H. Miller, The originof the word "Anaesthesia." New Eng. J. Med., 197:1218.
*Fulton and Stanton, op. cit., p. 72.
8 ANESTHESIA

BRIEF HISTORICAL OUTLINE
with severe criticism from adherents of the stern reli-gious belief of the period, especially members of theCalvinist clergy who taught that it was sinful to sothwart the curse pronounced on womanhood by thedisobedience of Eve in the Garden of Eden. But Dr.Simpson, a canny Scotsman with a warm heart, inrebuttal also cited the Bible, Genesis 2:21, claimingthat God set a precedent for anesthesia when, oncreating Eve, He "made a deep sleep to fall uponAdam" for the removal of his rib.10
However, the controversy continued until 1853when Queen Victoria gratefully accepted anesthesiafor the birth of her eighth child, Prince Leopold, thusgiving court sanction to a blessing the general publicwas anxious to enjoy.11
Hoping to find a more pleasing drug than ether forhis purpose, Dr. Simpson experimented on himselfand a few interested medical friends, finally demon-strating the anesthetic properties of chloroform inNovember 1847. Being more agreeable to inhale andof greater potency, for a while chloroform seriouslychallenged the supremacy of ether, but time proved itinferior from the standpoint of safety.
With the acceptance of surgical anesthesia as anestablished fact, interest in nitrous oxide revived, andthe gas became the standard anesthetic for briefdental extractions. Anesthesia for general surgery wasnecessarily limited to ether and chloroform until theFirst World War, 1914-1918, when the need for asafer anesthetic drug for patients who had to be oper-ated upon while still in a state of shock stimulatedinterest in nitrous oxide. It was found that, whennitrous oxide was combined with pure oxygen instead
10 Keys, op. cit., p. 34.n Herbert Thoms. Anesthsie 4 la Reine. Am. J. Obst. & Gynec.,
40:840.
9

of air to prevent asphyxial symptoms, results for thistype of patient were surprisingly good. Thus impetuswas provided for the designing and manufacture ofsuitable apparatus for administering "gas-oxygen."
Scientific research has remarkably enriched theworld in many different fields of endeavor during thelast few decades, and innovations in anesthesia wereto be expected. The first to be realized was the intro-duction of ethylene gas, a volatile hydrocarbon, in1923, clinical proof of its suitability as an anestheticagent having been first established at the PresbyterianHospital in Chicago.
An interesting side light on the discovery of ethyleneas an anesthetic is the fact that the research wasstarted at the request of florists who suffered heavycommercial loss in growing carnations, the well-developed flower buds failing to open. Chemists wereable to prove that the 4 per cent ethylene commonlypresent in illuminating gas used for lighting thegreenhouses was responsible for this "sleep of theflowers." 12 Considered first as a harmful poison,further research emphasized the beneficial effects ofthe gas as an anesthetic.
Another gaseous hydrocarbon, cyclopropane, ofmuch greater anesthetic potency was added to the listin 1933. It had been sponsored clinically by Dr.Ralph M. Waters of Wisconsin.13
At about the same time, a volatile liquid anesthetic,Vinethene (divinyl ether), was synthetized by agroup of California pharmacologists. After extensiveclinical studies at the medical school of the Universityof Pennsylvania, and at the Royal Victoria Hospital,
U James Tayloe Gwathmey, Anesthesia, p. 712.1a Ralph M. Waters and Erwin R. Schmidt. Cyclopropane anes-
thesia. J.A.M.A., 103:975.
10 ANESTHESIA

BRIEF HISTORICAL OUTLINE
Montreal, 14 this new drug, too, became generallyavailable.
Investigation, particularly by German chemists, ofthe anesthetic properties of nonvolatile drugs resultedin the addition of Avertin (tribromethyl alcohol) tothe list. It is given by rectal instillation and was firstused clinically in America in 1927. Following this, in1933-1934, two anesthetic drugs for intravenous usebecame available, Evipal soluble (hexobarbital sol-uble) and pentothal sodium, which are short-actingderivatives of barbituric acid. Credit for the clinicalintroduction of pentothal sodium is due Dr. John S.Lundy and collaborators of the Mayo Clinic.
Cocaine, an alkaloid of the leaves of the tropicalcoca tree, had been discovered and named by the Ger-man chemist, Albert Niemann, in 1860. Proof of itsefficacy as a local anesthetic, when applied topicallyto mucous membrane, was established by Carl Koller,a Viennese surgeon, in 1884. It was then adopted byEuropean surgeons in the specialties of ophthalmologyand otolaryngology. Dr. William Halsted of JohnsHopkins Hospital, Baltimore, Maryland, extendedthe use of cocaine to the field of general surgery by thehypodermic injection in and about nerves nowcalled "nerve block." The high toxicity of cocainecaused search for safer synthetic drugs of a similar na-ture. Several have been found over the years, notablyNovocain (procaine hydrochloride), also of Germanorigin, which since its birth in 1904 has well stood thetest of time and still holds supremacy as a local anes-thetic.
As the advent of controllable anesthesia gave im-petus to the widening of the scope of surgery, so theambitious daring of the modern surgeon in tackling
14Wesley Bourne and Douglas W. Sparling. Some aspects of vinylether (vinethene) anesthesia. Anesth. & Analg., 14:4.
11

12 ANESTHESIA
disease and malformation, even in the most remoteand vital regions of the body, spurs on the alert anes-thetist in striving for perfection in the "art of anesthe-sia." This infers not only thoroughness in knowledgeand good judgment but also skill and ingenuity inovercoming the manifold and mechanical difficultiesthat may be encountered, always, of course, with thesafety of the patient uppermost in mind.
Despite the advantages gained by the addition ofnew drugs and refinements in technique, the perfectanesthetic has not yet been found; all those of thepresent have their drawbacks, and so the search goeson. Doubtless, further valuable discoveries will bemade, but, realizing the great variation in individualtolerance for drugs or even for simple foods in vary-ing conditions of health and disease, one fears theprospect of this "perfect anesthetic" emerging mayprove to be only a chimera. However, for the averagecase, the skilled anesthetist proves it is possible nearlyto attain this goal of perfection by combining two ormore agents in careful proportion, thereby enhancingthe value and minimizing the danger inherent in theindividual drugs.
Truly we have much for which to be thankful inthe evolution of modern surgical anesthesia!

Chapter 2
PHYSIOLOGY OF ANESTHESIA
MANY drugs are known to have anestheticproperties, but few have been found to measure up tothe requirements for surgical anesthesia in regard tosafety and controllability.
It is essential that, in therapeutic dosage, the drugbe innocuous to body tissues as a whole, causing noserious interference with normal organic functions,that it be effective in controlling muscle reaction topain stimuli, and that the induction and recoverystages be reasonably brief and cause little discomfortfor the patient.
Several plausible theories have been formulated asto how drugs produce the state of general anesthesia,but so far scientific proof has not been established. Itis definitely known that nervous tissue is more sensi-tive to anesthetic drugs than are the body cells in gen-eral, that when a definite quantity of the drug isintroduced directly into the blood stream, either byintravenous injection or by absorption through thealveoli of the lungs, a state of unconsciousness super-venes, the central nervous system being affected in thereverse order of its embryonic development. Thehigher centers become paralyzed before the vital cen-
13

14 ANESTHESIA
ters of respiration and circulation are depressed; this,of course, is essential for the well-being of the patient.
One explanation for the hypersensitivity of nervoustissue to the volatile anesthetic drugs is that suchdrugs are, in general, lipoid solvents,1 i.e., readilysoluble in fats, of which nervous tissue has a high pro-portion. The drugs are distributed to the body tissuesthrough the blood stream, and the central nervoussystem has a very large blood supply. For prolongedsatisfactory anesthesia, it is requisite that a uniformtension, or degree of saturation, of the drug be estab-lished throughout the whole system, but very shortpainful procedures can be effectively completed with-out discomfort to the patient when consciousness isfirst blotted out. Oftentimes this is of great benefitbecause of the brevity of the recovery stage.
Volatile drugs and gases, when inhaled, obey thewell-recognized law of gases in establishing and main-taining equilibrium of partial pressure throughoutthe living body, by passage from the area of higherconcentration to that of lesser concentration until thepartial pressure in both areas is equalized. (Partialpressure means that in a mixture of gases at a givenpressure, the pressure of each is divided betweenthe different gases in proportion to their relative vol-umes.)
The exchange of oxygen and carbon dioxide inmaintenance of the metabolic process largely repre-sents the function of the respiration. The anestheticvapor permeates into the blood stream through thethin walls of the lung alveoli, i.e., air cells, in con-junction with these gases. There it dissolves or formsa loose chemical combination with both the bloodcorpuscles and the plasma and, in turn, is passed on
x Yandell Henderson and Howard W. Haggard, Noxious Gases andthe Principles of Respiration Influencing Their Action, p. 83-84.

PHYSIOLOGY OF ANESTHESIA
through the capillary walls into the body tissues as awhole. 2 Fatty tissue absorbs the drug most readily. Allis constantly in a state of flux, or exchange, portionsof all the gases passing on into the venous system andback to the lungs. But as inhalation of the vapor con-tinues, an increasing tension, or partial saturation, ofthe anesthetic drug is established throughout thewhole system. When the degree of anesthetic tensionsufficient for the control of pain reflexes is reached,the concentration of the vapor being inhaled must bereduced, or the anesthesia will progress to the pointof serious depression, or paralysis, of the vital centersof the medulla. The degree of saturation required foradequate surgical anesthesia varies greatly accordingto the drug, or combination of drugs, used and thedegree of pain stimuli to be controlled.
During the induction stage of anesthesia, the con-centration of the drug in the arterial blood is higherthan that in the venous blood; during the ideal surgi-cal or maintenance stage, the drug concentration isabout equal in both the arterial and venous blood;and when the administration of anesthetic vapor isstopped, the venous blood takes on the higher concen-tration and unloads the anesthetic into the lungs,through which most of the drug is eliminated.3
With the exception of chloroform, all of the drugscommonly used as surgical anesthetics are relativelyharmless to normal body tissues when given with skilland good judgment. But it must be remembered thatanesthesia is an abnormal condition and all anes-thetics are potentially poisonous to protoplasm. Whengiven in maximum dosage or in too high a concen-tration they may have fatal results. Debility and dis-
SC. Langton Hewer, Recent Advances in Anesthesia and Analgesia,p. 1.3
Henderson and Haggard, loc. cit.
15

16 ANESTHESIA
ease lower resistance to these potentially harmfuleffects, and idiosyncratic reaction to the drug mayoccasionally prove an important factor in regard tosafety. In other words, it should be understood thatevery anesthesia carries with it a potential risk to life,and under no circumstances should it be undertakenlightly.
Late in the eighteenth century, the great Frenchscientist Lavoisier demonstrated the similarity of fire,or combustion, and breathing and proved that it isoxygen combining with carbonaceous matter that lib-erates heat and energy and, in the process, formscarbon dioxide. 4 The lungs serve as the portal bywhich oxygen enters the system and from whichcarbon dioxide is excreted, and since these gases aretransported to and from the tissues and the lungsin the blood stream, the circulation of the blood mustbe considered an essential part of the respiration. Afire cannot burn without oxygen, and a prolonged de-ficiency of oxygen in the body will finally cause death.
The air we normally breathe contains approxi-mately 20 per cent oxygen. That this quantity con-stitutes the low limit of oxygen essential to thewell-being of our bodies is demonstrated by the in-creasing discomfort, rapid pulse, labored breathing,undue fatigue, and nausea that are experienced bymountain climbers as they approach high altitudes.This is explained by the fact that the atmosphericpressure is reduced as the altitude is increased, andconsequently the quantity of oxygen in the airbreathed is less. A similar deficiency will be producedin a patient breathing an anesthetic atmosphere thatis deficient in oxygen, the severity of the symptomsbeing dependent upon the degree of oxygen deficiencyand the general condition of the patient.
4 Yandell Henderson, Adventures in Respiration, p. 5.

PHYSIOLOGY OF ANESTHESIA
It is evident that some degree of oxygen deficiencywill persist during the inhalation anesthesia when at-mospheric air only is used as the means of providingoxygen, for the bulk of the anesthetic vapor auto-matically reduces the percentage of oxygen in the airbreathed. In addition to this dilution of oxygen, nar-cotics, in varying degree, depress the respiration andcirculation and thereby lessen still further the quan-tity of available oxygen in the body. They also inter-fere with the chemical processes involved in tissueoxidation.5
Normal respiration is dependent on the mainte-nance of the acid-base balance in the blood and tissues.This balance is effected by the interrelationship of anintricate system of physicochemical reactions of oxy-gen and the by-products of metabolism and by theadequate functioning of the lungs and kidneys asexcretory organs.
The determining factors for the regulation of res-piration are: the carbon dioxide of the alveolar airand of the arterial blood, which normally is kept veryconstant at a tension of 40 mm. Hg.; and the thresh-old, i.e., sensitivity, for carbon dioxide of the respira-tory center in the medulla. Increase of the tension ofcarbon dioxide or decrease of the respiratory thresh-old for carbon dioxide results in stimulation ofbreathing, and vice versa. Pain, fear, and emotionalexcitement of any kind decrease the respiratorythreshold for carbon dioxide. The consequent stimu-lation of breathing lowers the carbon dioxide tensionin the body system faster than it is being replaced, andthis condition of "overventilation" is likely to induceapnea of varying degrees of severity, which in extremeinstances may prove fatal.
5 Samson Wright, Applied Physiology, p. 417.
17

18 ANESTHESIA
With clearer understanding of the causes and ap-preciation of the dangers of the various conditionsthat may complicate anesthesia have come efforts andmeans for their prevention or control. It is now gen-erally accepted that additional oxygen increases thesafety of all anesthetics. Modern apparatus for the ad-ministration of inhalation anesthesia makes it readilypossible for the anesthetist to adjust the proportionof oxygen and carbon dioxide, as well as that of theanesthetic drug, to suit the immediate need of eachpatient.

Chapter 3
METHODS OF INDUCINGSURGICAL ANESTHESIA
THE methods commonly used for the controlof pain during surgical operations can be grouped intothree general classifications: general anesthesia, localanesthesia, and regional anesthesia. Each method maybe relied upon individually, or they may be used incombination for the more difficult and resistant typesof patients in order to reduce the possible danger ofcumulative toxic dosage when used singly, or whenthe peculiar advantages of different methods are es-pecially desired.
General anesthesia. This is, in particular, distin-guished by loss of consciousness, which is initiated byintroduction into the blood stream of an anestheticdrug readily soluble in blood and body tissues. Entryinto the blood stream may be effected in three ways:(1) Inhalation anesthesia is the inhaling of a volatileliquid or gaseous anesthetic that, on reaching thealveoli of the lungs, will readily permeate into thearterial system. This is the original and most com-monly used method, being entirely controllable. Thevolatile anesthetics are changed very little in the body
19

and are excreted almost entirely by the lungs. There-fore, to lessen the percentage of the drug in the system,it is necessary merely to stop administering the drugand to keep the patient breathing. With maintenanceof adequate respiration, the plane of anesthesia canbe delicately adjusted by increasing or decreasing thequantity of the drug inhaled. (2) In rectal anesthesiacertain solutions are absorbed readily through themucosa of the lower bowel, and anesthesia can there-fore be induced by rectal injection of the drug. Thedrugs most commonly used in this way are ether-oilmixtures in varying proportion, Avertin (tribrom-ethanol) and paraldehyde. As the solution is injecteden masse, even though it may be absorbed graduallyand evenly (as has been claimed for ether-oil mixturesby Gwathmey, 1 the originator of the method), rectalanesthesia definitely lacks flexibility of control. (3)For intravenous anesthesia the most popular drugused at the present time is sodium pentothal, a dilutesolution of which is injected slowly into any conven-ient vein. By securing the needle in the vein through-out the surgical procedure, the solution can be givenintermittently and the plane of anesthesia kept wellunder control.
As with the three general classifications for surgicalanesthesia, i.e., general, local, and regional, these threetypes of general anesthesia may be used singly or incombination.
Local anesthesia. The term implies the desensitizingof a limited, superficial area of the body without in-terference with consciousness. The two usual methodsfor producing this effect are: (1) The topical applica-tion to mucous membranes of the alkaloidal drugcocaine, or a derivative thereof. (2) Hypodermic in-jection of a dilute solution of the nonirritating sodium
1 Gwathmey, op. cit., p. 439.
20 ANESTHESIA

METHODS OF SURGICAL ANESTHESIA 21salt of a synthetic drug; Novocain (procaine hydro-chloride), derived from benzoic acid, is the mostcommonly used. These drugs have a depressing effecton the superficial nerves and interfere with conduc-tion of pain impulses. The sensory nerves are affectedfirst.
Regional anesthesia. This denotes control of pain,without interference with consciousness, in a wider,deeper area of the body than in local anesthesia. Thismay be accomplished in four ways: (1) Nerve blockis produced by the injection of a local anestheticsolution in the region of a nerve trunk, or other largenerve branches, blocking impulses throughout its, ortheir, ramifications. (2) Spinal anesthesia is the injec-tion of the solution into the subarachnoid space, pref-erably through the third or fourth lumbar interspace,thus avoiding injury to the spinal cord, which nor-mally does not descend beyond the second lumbarspace. Mixed slowly with the spinal fluid, the drugbathes the roots of the spinal nerves and desensitizesapproximately the whole lower half of the body. Caremust be taken to avoid paralysis of the muscles thataffect normal respiration. (3) Caudal or epidural anes-thesia is the injection of the solution through thesacral hiatus, the drug entering the spinal canal be-low the dural sac and reaching the nerves emergingfrom it. This procedure induces anesthesia in the lowpelvic, perineal, and anal regions, with the completeavoidance of the risk of too high an area of anesthesiaby diffusion of the drug in the spinal fluid. (4) Re-frigeration anesthesia-a limb can be amputatedpainlessly after it has been adequately packed inchopped ice, or snow, for a specified time, a tourniquetbeing applied during the refrigerating process. Thiscauses a marked slowing down, or cessation, of metab-olism in all of the cells of the chilled area-a condition

22 ANESTHESIA
that has been compared to the state of hibernationnatural to some wild animals. Its special field of use-fulness is in the amputation of a limb for advanceddiabetic or arteriosclerotic gangrene, for gas-bacillusgangrene, and for severe traumatic injuries compli-cated by acute infection. Advantages claimed for re-frigeration anesthesia in these types of cases are: (a)slowing down of bacterial growth with consequentlessened spread of toxin from the infected area; (b)elimination of the additional toxic element of an an-esthetic drug; and (c) lessening of operative shock byvirtue of the complete blocking of afferent nerve im-pulses by the gradual and thorough chilling of thewhole nerve network of the area involved.2
Many conditions may influence the selection of theanesthetic drug and of the method for its administra-tion. Except in the most well-equipped and up-to-dateclinics, the ability and experience of the anesthetistand the equipment available may necessarily be thedeciding factors. Otherwise, the age and general con-dition of the patient, the site and type of operationand its probable duration, the possibility of the use ofthe actual cautery, diathermy, etc., are to be givenstudied consideration.
There is much difference, seemingly, in individualtolerance for anesthetic drugs, and a history of idio-syncrasy should be sought for and must not be ignored.Under some conditions it may be desirable that thepatient retain consciousness, while the temperamentof the patient may make this inadvisable. Other com-plicating problems are bound to arise; fortunately itis often possible to so combine drugs and methodsthat these can be solved satisfactorily for both thepatient and the surgeon.
2 Sergel S. Yudin. Refrigeration anesthesia for amputations.Anesth. & Analg., 24:252.

Chapter 4
PREMEDICATION
THE purpose of medication preliminary toanesthesia is usually threefold: (1) to allay fear, ap-prehension, and excitement and so reduce the bodymetabolism; (2) to diminish pain and thereby reducethe muscular reflexes caused by pain; and (3) to in-hibit secretion of mucous glands and so counteractthe stimulative effects of certain anesthetics on theseglands. A fourth advantage may be added, namely, toinduce amnesia so that the unpleasant experience willnot be remembered.
Variation in tolerance, or reaction, to anestheticdrugs has been evident and commonly recognizedsince the inception of surgical anesthesia. The patientsmost difficult to anesthetize are not necessarily thelarge robust individuals. More often they are foundamong the thin, wiry, nervous, emotionally unstabletypes of people and the patients suffering from feveror acute toxicosis, such as the thyrotoxic cases. Theyare, in short, the types of patients for whom sedativemedication frequently is indicated. So it is not re-markable that such medication has been used sporad-ically, prior to inhalation anesthesia, for many decades.
The volatile liquids, ether and chloroform, proved23

sufficiently potent to anesthetize all types of patientseventually, so sedative premedication was by nomeans a routine procedure until the advent, as sur-gical anesthetics, of the far less potent gases, nitrousoxide and ethylene. It soon was found that these"weak anesthetics," which normally must be used inconcentrations of 80 per cent, are frequently incapableof inducing satisfactory anesthesia unless the oxygencombined in their clinical use is reduced gravely be-low the 20 per cent atmospheric oxygen to which thehuman body is so delicately geared to function.
In 1924, Dr. A. E. Guedel first pointed out thesignificance of the metabolic rate, and consequentdegree of reflex irritability, in relation to anesthesia.'He emphasized the fact that increase of metabolismfrom any cause necessitates increase of oxygen con-sumption. At the same time a higher concentrationof the anesthetic drug in the body tissues is requiredfor control of the increased reflex irritability. Thiscombination is impossible of achievement with asingle anesthetic drug of low potency, so it is nowgenerally recognized that preoperative sedation is notonly desirable from the standpoint of the patient'scomfort but may be essential for the safe conduct ofthe anesthesia.
Emotional excitement, pain, fever, and certaintoxemias increase metabolism, and adequate sedativepremedication is helpful in preventing or controllingthese complications. The drugs most commonly usedfor this purpose are the alkaloids of opium, especiallymorphine sulfate, Pantopon, and codeine, and themoderately short-acting barbiturates: Nembutal, Amy-tal, Seconal, etc. The alkaloids of belladonna-atropine
1 Arthur E. Guedel. Metabolism and reflex irritability in anes-thesia. J.A.M.A., 83:1786.
24 ANESTHESIA

and scopolamine-are useful in diminishing secretionof mucus.
The use of a routine form of dosage for medicationof any kind is deplorable, for there is much differencein individual tolerance for drugs under conditions ofboth normal and impaired health. For instance, thebasal metabolic rate varies considerably in differentage groups as well as under abnormal conditions ofhealth, and the rate of destruction of the opiates inthe body depends largely upon the rate of the metab-olism of the individual concerned. Again, if the pa-tient is in pain, scopolamine and the barbiturates,given without morphine, may cause delirium and rest-lessness instead of somnolence. Consequently, selectionand dosage of all medication should be carefully ad-justed to the need of the individual patient. Thisneed will vary in accordance with the age and thestate of physical and mental health of the patient andwith the anesthetic drug, method of anesthesia, andtype of surgical operation to which he is to be sub-jected.
The possibility of idiosyncrasy to these drugs has tobe given consideration. A good method for provingthe validity of a history of idiosyncrasy is to first givesmall test doses of the drug so that the effect may benoted and the originally calculated dose omittedshould this seem advisable. Some similar drug forwhich the patient shows better toleration may be sub-stituted or a change made in the choice of the anes-thetic.
It should also be clearly understood that the thera-peutic dose of a drug that might safely be given byhypodermic injection into the tissues may be criticallytoxic if it is injected directly into the blood stream.Consequently, hypodermic injection should always bepreceded by slight aspiration through the needle, after
25PREMEDICATION

it is inserted, to make certain that a blood vessel hasnot been accidentally punctured. The needle shouldthen be slightly withdrawn and the solution injectedslowly. If blood is aspirated, the needle should beentirely withdrawn and reinserted a little distancefrom the original puncture.
A hypodermic injection will be more quickly ab-sorbed and cause less local irritation if it is givensufficiently deep into the tissue so as not to cause aninflamed wheal at the site of injection.
The order in which premedication is commonlygiven is: (1) a sedative such as Nembutal (pentobar-bital) at bedtime, to insure the patient a restful night;(2) morphine, given subcutaneously, preferably three-quarters to one hour before operation, to allay appre-hension and diminish pain, and thus to reducemetabolism somewhat and increase the effectiveness ofthe anesthetic; (3) atropine or scopolamine, given sub-cutaneously with the opiate, to inhibit secretion ofmucus in the air passages and so offset the stimulatingeffect of some anesthetics, especially ether and Vine-thene, on the mucus glands. Atropine is rather themore effective for this purpose and, to a limited ex-tent, offsets the respiratory-depressant effect of mor-phine. Normally scopolamine contributes a definitesedative effect and desirable amnesia.
Preliminary medication should be given sufficientlyearly for the full effects of the drug to be apparent bythe time the anesthetic is started. This is especiallyimportant in the case of ether because of the dangerof so high a concentration of ether being establishedin the system during the induction stage that, by thetime the opiate attains its maximum effect, a condi-tion of serious apnea may develop. The primary toxiceffect of both of these drugs is depression of respira-tion. This risk is present also in regard to the barbitu-
26 ANESTHESIA

rates, though to a lesser extent. In short, preoperativesedation supplements anesthesia and reduces thequantity of the anesthetic that it is necessary or de-sirable to use in order to maintain a satisfactory planeof anesthesia.
The subcutaneous injection of morphine does notnormally attain its maximum effect in the system un-til approximately one hour has elapsed. Should thepatient be in a state of severe shock, or badly chilledfrom exposure to cold, absorption of the drug may begreatly delayed on account of the inefficient circula-tion of the blood under these conditions. Specialwarning to this effect was found to be necessary in thetreatment of casualties during the war in order toprevent overdosage from too frequent repetition ofthe injection.
Morphine may be given intravenously when it isnecessary, or desirable, to hasten absorption of thedrug, but its effect will be of shorter duration. Foruse in this way, the tablet should be dissolved in atleast 2 cc. of sterile water, or saline, and the solutioninjected very slowly (three to five minutes being al-lowed for the whole amount); the patient should bewatched carefully meanwhile for untoward reactionso that, if indicated, the injection can be stopped.Maximum narcotic effect will be obtained withintwenty minutes by the intravenous method of in-jection.
ADVANTAGES OF SEDATION
1. Morphine, a powerful narcotic, usually is help-ful in promoting a state of drowsiness with a lessen-ing of fear and anxiety in the patient who is facing asurgical ordeal.
2. The narcotized patient seems less sensitive to the
27PREMEDICATION

28 ANESTHESIA
passage of time, so unavoidable delays will be less irk-some to him.
3. The metabolic rate is somewhat reduced and thesense of pain appreciably dulled; in consequence, alesser quantity of the anesthetic drug will be requiredin order to maintain satisfactory anesthesia.
4. With relatively short operations, the discomfortof the immediate postoperative recovery period isminimized.
5. The addition of one of the barbiturates enhancesmost of the good effects of the narcotic and gives theadvantage of some degree of amnesia.
DISADVANTAGES OF SEDATION
1. Morphine depresses the rate and depth of res-piration, and this may prolong the induction of in-halation anesthesia.
2. This drug retards gastric and intestinal secretionand motility, thereby causing flatulence and consti-pation.
3. Its primary effect of stimulation of the medullamay cause nausea and vomiting, and this distressingoperative sequence not infrequently can be traced tothe morphine that has been given rather than to theanesthetic drug. (Goodman and Gilman suggest thatthis discomfort may be prevented in some cases if asmall portion of the drug is injected and the re-mainder given fifteen to twenty minutes later; thehypothesis being that the small initial dose will causea minimum of primary medullary stimulation, withthe final dose exerting the secondary, or depressant,effect only.)2 Some patients who are nauseated bymorphine seem to have more tolerance for Pantopon
2Louis Goodman and Alfred Gilman, The Pharmacological Basis
of Therapeutics, p. 204.

(Omnopon), a mixture of purified alkaloids of opiumincluding approximately 50 per cent by weight ofmorphine.
4. Occasionally, idiosyncrasy to morphine may bemanifested by restlessness and excitement, continuedcerebral stimulation rather than the usual subsequentdepression.
5. By contracting the pupil of the eye, morphinedisguises one of the valuable signs of the plane ofanesthesia in the maintenance stage.
The effects of codeine are in every way milder thanthose of morphine, and this drug is unique among thederivatives of opium in that, when the maximumtherapeutic dose of 60 mgm. is exceeded, the toxicsymptoms are those of stimulation and excitementrather than depression.3
Opium derivatives, as a whole, depress the respira-tory center and cause increase of intracranial pressure,so usually they are contraindicated prior to surgeryfor intracranial lesions. These drugs are also to beavoided in obstetrics during the last few hours oflabor, because of the danger of the narcotic seriouslydelaying the spontaneous respiration of the baby atbirth.
A new synthetic drug, Demerol (merperidine hydro-chloride), is now in process of clinical evaluation as asubstitute for morphine. This drug, it is claimed,ranks between morphine and codeine in its narcoticaction. In comparison with morphine, it does not de-press the respiration, does not constrict the pupil, isnot constipating, is less frequently followed by nausea,and drug addiction less often results from its pro-longed use. Encouraging reports have recently comefrom obstetric clinics of the analgesic effectiveness ofDemerol during labor without causing respiration
8 Ibid., p. 206.
29PREMEDICATION

difficulties in the baby.4 Demerol inhibits secretion ofsaliva and mucus, causing dryness of the mouth andthirst, so the additional use of atropine is not indi-cated.
The other two drugs commonly used in preanes-thetic medication are atropine sulfate and scopola-mine hydrobromide (hyoscine). The specific action ofthese drugs, for this purpose, is to offset the stimulat-ing effect which some anesthetics exert on the salivaryand mucus glands of the air passages, by inhibitingsecretion of these glands. Their depressing effect onthe parasympathetic nervous system also helps tocounteract respiratory difficulties, such as laryngo-spasm, occasionally met with during anesthesia andprecipitated by stimulation of that system from vari-ous causes.
Atropine and scopolamine stimulate the respiratorycenter. So, to a limited extent, they decrease or coun-teract the depressant effect of morphine on thatcenter. Being mydriatics, they also tend to combatconstriction of the pupils caused by morphine.
Comparing atropine and scopolamine, it is to benoted that atropine is somewhat more effective as anantispasmodic and in the control of excessive secretionof mucus, while scopolamine, in addition to theseattributes, contributes psychic sedation and amnesia.Idiosyncrasy is more commonly met in the use ofscopolamine than with atropine.
The need for a means of controlling the secretionof mucus will be apparent when it is realized that thefumes of the volatile liquid anesthetics, especiallywhen given in high concentration, are irritant to themucosa of the air passages, frequently causing a copi-
SGordon Gilbert and Alfred B. Dixon. Observation on demerol asan obstetric analgesic. Am. J. Obst. & Gynec., 45:320.
William R. Schumann. Demerol (S-140) and scopolamine in labor,a study of 1,000 cases. Am. J. Obst. & Gynec., 47:93.
30 ANESTHESIA

PREMEDICATION 31
ous flow of saliva and mucus. This abundance ofmucus may increase the hazard of anesthesia in severalways: (1) the fluid, saturated with ether, constantlybathing the sensitive bronchial epithelium may causeserious irritation and bronchitis; (2) plugs of mucusmay become lodged in the narrow passages of thebronchioli, giving rise to the possibility of subsequentatelectasis and pneumonia; (3) a coating of mucus onthe walls of the lung alveoli may delay absorption ofthe anesthetic vapor into the blood stream; (4) mucus,churned to a froth by the breathing, may seriouslyobstruct the airway and interfere critically with theexchange of oxygen and carbon dioxide; and (5) someof the ether-saturated fluid will be swallowed and soaggravate postoperative nausea and vomiting.
Everything considered, it is evident that successfulpremedication depends upon good judgment in evalu-ating a drug, or combination of drugs, in accordancewith the advantages and disadvantages that theyafford and in relation to the state of disability of theindividual patient.

Chapter 5
GENERAL IMMEDIATE PREOPERATIVEAND POSTOPERATIVE CARE
OF PATIENT
THE natural first reaction of the patient tothe prospect of having to submit to a surgical opera-tion, however slight from the surgeon's point of view,is one of more or less resentment and apprehensionif not profound fear. Admission to the hospital isitself disturbing and exciting, but with a little kindlyunderstanding and tact on the part of the nurses andattendants, the patient, unhurried, usually soon ad-justs to the change more easily than he anticipated.So, whenever possible, it is advisable that the patientbe admitted to the hospital at least a day before opera-tion, for adjustment and observation.
Though the need for surgical intervention may bereadily evident, a careful preoperative general physicalexamination and laboratory studies of blood and urineare indicated to determine the patient's probabletolerance for anesthesia and operation, and time isrequired for adequate arrangement for preparatoryor supportive treatment, should such become neces-
32

PREOPERATIVE AND POSTOPERATIVE CARE
sary. It is important also that the alimentary tract begiven special preparation.
Care in detail. Except when especially contraindi-cated, as prior to surgery for acute gastric disease orintestinal obstruction, an easily digested diet, rich incarbohydrates (to increase liver glycogen), may begiven with advantage up to the night before operation.Water should be allowed freely to within two to threehours of operation, since it is readily absorbed froman empty stomach. Rarely will a patient ask for adrink of water in the early morning, so it is a goodrule to include a glass of water, hot or cold accordingto the patient's preference, in the routine preoperativemorning treatment; this will do much to alleviatelater thirst and to promote normal kidney function.When possible to avoid it, forbidden food should notbe displayed in the feeding of other patients, especiallywhen the patient awaiting surgery is a child.
Proper preoperative preparation of the bowel willhelp greatly in preventing postoperative "gas pains,"and this usually includes a thorough cleansing enema.Preferably, this enema should be given in the earlyevening prior to operation. The order commonlywritten "enema till clear" carries the assumption thatthe enema will be inefficiently given-a reflection onthe nurse! Such procedure is needlessly tiring to thepatient, and some of the fluid may be retained andthe bowel continue in a state of irritability. This isespecially annoying if the enema is given within a fewhours of the surgical operation. One injection, givenslowly and carefully, should be effective in emptyingthe lower bowel.
Commonly, simple sedative medication is orderedto be given at bedtime to assure the patient a restfulnight before the surgical ordeal. A hot drink, such asmilk or malted milk, given at the same time may aid
33

in inducing sleep. It is most important that all neces-sary examinations and treatments have been completedbefore such sedation is given. Otherwise its effect isspoiled. If the cleansing bath also is given the eveningbefore operation, there will be little need for disturb-ing the patient too early in the morning.
Thorough brushing of the teeth and rinsing themouth with a mild saline or antiseptic mouth washjust before going to the operating room is refreshingand a safeguard against respiratory infection. All de-tachable dentures should be removed in the patient'sroom; the final responsibility for removal of such, ofcourse, rests with the anesthetist, but these expensivesmall things may easily be lost in a busy operatingroom. Dental bridgework especially is a source ofdanger to the unconscious patient; fatalities have re-sulted from lacerating effects of the attached metalclips when such articles have become displaced andswallowed.
Hairpins and combs may cause injury to the scalpduring unconsciousness and should be previously re-moved. Long hair should be combed and braided.
The lips and fingernail beds are valuable indices ofproper oxygenation of the blood and should be devoidof artificial coloring; this fact should be tactfully ex-plained to women patients who insist on applyingsuch cosmetics prior to general anesthesia.
The patient should be requested to empty the blad-der just before leaving for the operating room; andthe quantity of urine, time of voiding, or inability todo so should be noted on the patient's chart. Time isvaluable but the thoughtful, efficient nurse is carefulto avoid giving the patient an impression of beinghurried. By her sympathetic yet cheerful and confi-dent attitude she can greatly mitigate the patient'snatural reaction of apprehension and of repugnance
34 ANESTHESIA



PREOPERATIVE AND POSTOPERATIVE CARE
to the humiliating indignities that unfortunately arecommonly a necessary adjunct to the preparation formajor surgery.
The environment of the operating-room suite maywell prove distressing to a nervous person, and thepatient should not be kept waiting there just for theconvenience of the operating-room staff. However, thefeeling of being hurried is also unfortunate, and in abusy department these drawbacks may have to becounteracted by sedative premedication to dull thepatient's sensitivity. Every nurse should understandthe importance of not deceiving a child; such too-common practices as telling a child, "You are goingto have your picture taken," when he is en route tothe operating room are inexcusable, for the provenfalsehood naturally undermines his trust in everyoneconnected with his hospital treatment. In contrast,very commendable is the kindly effort of the headnurse of a children's ward who, with rare psychicalunderstanding in her love of children, teaches theman amusing jingle to be sung as a chorus. The jingledescribes the helmets and gowns of green, etc., wornby the doctors there, and is accompanied by a de-lightfully graphic fling of bandage scissors to thefloor by the leader of the group; all of which stimu-lates a child's interest in the coming experience,without the element of deceit. It is desirable that thepatient be taken to the operating room by a nursewith whom he is familiar and who will introduce thenurse or anesthetist to whose care he is being en-trusted.
Transfer to operating table, for general anesthesia. Asa general rule, a mattress in two sections can be usedto cover the operating table; this and a firm rollplaced under the knees when the patient is to lie inthe supine position will aid in relieving muscle strain
35

and in preventing postoperative backache. (If the pa-tient has inadequate circulation in the legs, however,it is best to omit the knee roll as a precaution againstfurther circulatory interference from pressure in thepopliteal space.) The mattress, preferably filled withhair, should be approximately three inches in thick-,ness and covered with waterproof material over whichis placed a folded sheet. A simple means for liftingthe patient from table to bed or stretcher is providedby the placing of two straight abdominal binders ontop of the mattress and sheet, under the patient'sbody. (Figure 1.) The ends of these binders can alsobe used to advantage in confining the patient's armsduring anesthesia.
Wrist straps made of heavy flannelette (Figure 2)are harmless and effective as restraints when fastenedsecurely to the sides of the table. The cuffs may beattached to the wrists when the patient is first trans-ferred to the table, but with an adult the arms shouldnever be evidently restrained while the patient re-mains conscious. Such ill-considered premature re-straint suggests great discomfort to be experienced,provoking resistance by alerting the patient to a com-bative state of mind.
A strap, suitably cushioned to prevent nerve injury,can be inconspicuously passed under the table andover the patient's knees and fastened securely at oneside of the table with the casual remark that it isdone to safeguard the patient from falling off the nar-row table. Straps and braces of all kinds need to bewell cushioned, hands straightened in normal position,etc., in order to avoid the danger of serious circulatoryinterference or nerve injury.
For the patient lying in the prone position duringanesthesia, it is necessary that the shoulders be firmlysupported by pads placed on top of the mattress at
36 ANESTHESIA

Figure 2. Wrist straps: soft, yet firm and washable.


PREOPERATIVE AND POSTOPERATIVE CARE
each side. Separate pads are used in order to preventinadequate chest expansion due to compression duringprofound muscular relaxation. The knee roll shouldthen be placed under the front of the feet, to keep thetoes suspended slightly from the mattress.
Small children may be wrapped up in a half sheetor small cotton blanket folded in half and laid on thetable so that the open end lies under the child's neck;a single layer of the sheet is then passed at each sideover an arm and under the body, the weight of whichrestrains movement of the arms; then the second layerof the sheet is passed over both arms and tucked underthe body at each side. With a little ingenuity andimagination the whole procedure can be made intoa game and then is seldom resented by the child. Thereis great satisfaction in being able to anesthetize mostchildren in such a way that they fall asleep quietlyand later have no fearful recollection of the ordealand, usually, the smoother the induction of anesthesiathe easier it will be to maintain a smooth surgicalstage also.
\Too heavy covering is to be avoided, especially inhot humid weather, because of the risk of heat ex-haustion due to a combination of concentrated heatfrom high-powered surgical lamps and heavy cover-ings. These interfere with the evaporation of sweatand with the dissipation of body heat. The heat-regulating mechanism is upset in turn and high feverresults. Such cases have been reported.1
To anyone unfamiliar with it, an operating room islikely to appear fearful and alarming, anything buta soothing place in which to "be put to sleep." So,whenever possible, a quiet side room should be chosenfor the induction of anesthesia, with only an assistant
1Mortimer B. Genauer. Post-anesthetic heat stroke. Anesthesiology,
7:302.
37

present beside the anesthetist and patient. When thisis not practicable for any reason and the anesthesiamust be started in the operating room, the roomshould be kept as quiet as possible. The sorting anddisplay of instruments must be delayed and generalconversation stopped until the patient loses conscious-ness. The anesthetist should have everything preparedin readiness so that there will be no delay in the startof the induction when the patient is brought into theroom. A properly conducted induction of anesthesiais rarely complicated by a troublesome stage of ex-citement. Absence of the excitement stage cannot besurely predicted beforehand, however, and an assist-ant who is capable of restraining an active patient, ifnecessary, should always be close at hand during theinduction stage.
At the completion of the operative procedure, allwet coverings should be replaced by warm dry onesand the patient lifted gently into bed. Though thepatient may still be unconscious, rough handling im-mediately following a major surgical operation mayprovoke a state of shock with serious fall of bloodpressure.
Unless definitely contraindicated from a surgicalstandpoint, all surgical patients, when first transferredto bed, should be turned on one side with the upperknee flexed and a pillow tucked snugly at the backin order to maintain the lateral position, (Figure 3.)Care should be taken to place the head so that theneck is in normal contour in order to facilitate normalbreathing and the expulsion of vomitus should suchoccur. A thin pillow may be helpful for this, andoften adds to the patient's comfort. With the headproperly placed in this way, the relaxed tongue of anunconscious patient will fall to the dependent side ofthe mouth thus providing a reasonably clear airway
38 ANESTHESIA

~1~
I


PREOPERATIVE AND POSTOPERATIVE CARE 39
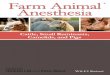
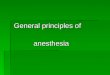
above it. Should the tongue relax against the posteriorwall of the pharynx, the airway becomes almost com-pletely blocked, a condition typified by a noisy snoreor total suppression of breathing-the misnamed stateof "swallowing the tongue." If such a condition oc-curs, it can be quickly corrected by grasping the lowerjaw on both sides at the angle posteriorly and draw-ing the jaw forward so that the lower teeth come intoline with, or slightly in front of, the upper teeth. Thetongue is thus pulled away from the posterior wall ofthe pharynx. If it is not permissible to turn the patienton one side, an adequate airway may be maintaineduntil the patient recovers consciousness by the inser-tion of a pharyngeal airway tube, either through themouth or nostril. (Figure 4.) These details of safe-guarding the patient from respiratory embarrassmentare primarily the responsibility of the anesthetist, butemergencies may later arise and the nurse should beready and able to cope with them.
For several reasons it is essential that the post-surgical patient be protected from drafts and insuffi-cient covering in cold weather and from contact withpeople suffering from acute respiratory infections.Frequently there is loss of body heat during a pro-longed surgical operation due partly to metabolicand circulatory disturbances and the sweating causedby some anesthetic drugs and partly to evaporationfrom severed tissues and serous surfaces. Also surgeryand anesthesia, especially in major operations, lowerresistance to acute respiratory infection from the germsthat are always present in a quiescent state in theupper air passage. When the weather is hot, undueoverheating of the patient by warm coverings, etc., is,of course, to be avoided, both for the comfort of thepatient and for the danger of further loss of bodyfluids by excessive sweating.

40 ANESTHESIA
To insure his safety, the anesthetized patient mustbe kept under continuous observation until the returnto a conscious state is completed. This period can beused to advantage for the initiation of parenteralfluid therapy or other postoperative orders that mightcause some discomfort during consciousness.
It may be well here to stress the fact that the com-mon practice of surgeons in leaving "P.R.N." ordersfor sedative medication for the postoperative patientputs a heavy responsibility on the nursing staff. Thisis particularly true in the case of the powerful opiatesand when the more depressant type of anesthetic hasbeen given.
As a rule, a lesser quantity of a narcotic is requiredif it is given early rather than if it is delayed whilethe severity of the pain increases or the patient'sability to tolerate the pain decreases. But the timerequired for destruction of the drug in the body, orfor its elimination, depends largely upon the rate ofthe body metabolism. Narcotic drugs lower the meta-bolic rate, and therefore the metabolism of a patientwho is recovering from a prolonged surgical anesthesiais probably reduced. This is especially so whenAvertin, pentothal, a deep plane of ether, or a com-bination of such drugs has been used. A narcotic drugfor the relief of pain or restlessness may be indicatedrelatively soon after the completion of a painful sur-gical operation, even though the patient may not havecompletely recovered consciousness. But this addi-tional medication will still further reduce the metab-olism, and repetition of the dose calls for the exerciseof experience and good judgment, with a realizationof the significance of the metabolic factors. The aver-age four-hour interval allowed for destruction ofmorphine in the system may be grossly inadequateunder such circumstances, and the destruction of vital

aaaaaaaaaaaaa~
Figure 4. Pharyngeal airways. Available in various sizes andtypes and from various firms. The instruments illustrated arefrom the Foregger Co., New York. A) nasal tube, rubber; B)oral, rubber; C) oral airway and insufflation tube, rubber;D) oral, metal.
~:::


PREOPERATIVE AND POSTOPERATIVE CARE 41body cells can be caused by anoxia due to profoundrespiratory depression resulting when the nurse fol-lows too literally the usual order for morphine "q.4 h. P.R.N." Soothing details of nursing care often-times are sufficient to prolong satisfactorily the inter-vals between doses, and these should be given a fairtrial. This danger of serious depression is less pro-nounced following the gaseous anesthetics for these arequickly eliminated, and unless a condition of surgicalshock has developed, the patient's metabolism maybe expected to return to normal as consciousness isregained. More frequent repetition of the prescribednarcotic for these cases may then be safe, and neces-sary in order to protect the patient from debilitatingand unwarranted pain.
During the first few postoperative days, adequateexpansion of the patient's lungs may be prevented byhis shallow breathing. This may be a result of his"splinting" against the pain of an abdominal or chestwound or of restriction caused by tight dressing strapsor bandages. In order to lessen the danger of develop-ment of postoperative pulmonary complications dueto this inadequate ventilation, the patient should bemoved several times a day from side to side (unless thetype of injury prohibits this), and he should be in-6tructed and encouraged to breathe deeply at intervalsand to cough up mucus and phlegm which may col-lect in the deep air passages. This procedure shouldbe followed despite the transient additional pain theseefforts may cause him.
Desirable deep breathing can also be induced me-chanically by the use of a "blow bottle"-a gallonbottle half filled with water and fitted with a piercedstopper and tubing through which the patient blowsinto the water vigorously enough to cause it to bubbleactively.

Physiological stimulation of the respiration can bebrought about by having the patient breathe a smallquantity of carbon dioxide diluted with air or oxygen;5 per cent carbon dioxide is usually sufficient. By theintelligent use of a gas-oxygen face mask and breath-ing bag, a single bagful of the carbon dioxide mixturecan be rebreathed and will suffice for each treatment.The patient must be encouraged to inhale the mixtureuntil stimulation of the respiration is evident (a fewbreaths will suffice for this), then the obturation valveis closed, to retain the gas in the bag, and the maskis removed from the patient's face. The stimulationof breathing gradually fades and, after a few momentsof rest for the patient, the treatment is resumed. Theusual order is for three such treatments at two to four-hour intervals, but the treatments are of no availunless their purpose is understood and they are givenintelligently and well. This treatment is also helpfulfor the relief of postoperative "gas pains."
Endotracheal catheter suction at intervals duringthe first few postoperative days may prove a lifesavingmeasure when other methods are ineffectual in clear-ing the deep-seated respiratory tract of accumulationsof obstructing mucus. 2 When skillfully done it is notvery disturbing to the patient.
2Cameron Haight. Intratracheal suction in the management of
postoperative pulmonary complications. Ann. Surgery, 107:218.
42 ANESTHESIA

Chapter 6
VOLATILE LIQUID ANESTHETICDRUGS: ETHER, CHLOROFORM,ETHYL CHLORIDE, VINETHENE
ALL inhalation anesthetics are chemicallyalmost unchanged in the body but are excretedthrough the lungs, loaded with the excess carbondioxide of metabolism. If the exhaled vapor can bepassed through a chamber of soda-lime (sodium andcalcium hydroxide), which is, or can be, incorporatedin all modern gas-oxygen machines, the carbon dioxidewill be removed and the anesthetic restored to itsoriginal pure state.
Ethyl ether, the herald of surgical anesthesia a cen-tury ago, still holds prominence as the fundamental,relatively safe anesthetic drug, for it has a large marginof safety (the difference between the therapeutic andlethal dose); it is a volatile liquid of high potency;and it is easily portable and can be used effectivelywith very simple apparatus. Consequently, if limitedto one drug only, most probably ether would be thefirst choice of surgeons and anesthetists in general.But from the patient's point of view, ether is the least
43

44 ANESTHESIA
agreeable, largely because prolonged postanestheticnausea and vomiting are more common than with theother anesthetic drugs. Happily, under average cir-cumstances, a wide choice of anesthetics is now avail-able.
The severity of the symptoms of nausea and vomit-ing depends largely upon the degree of saturation ofether in the body system. The small quantity of ethersometimes desirable or necessary to stabilize the effectof a less efficient, though less toxic, drug may havelittle or no disagreeable sequence.
ETHER ANESTHESIA
Ethyl, or sulfuric, ether, (C2H5)20, is a clear color-less volatile liquid with a boiling point of 36.50 C. It ishighly inflammable but, as the vapor is approximatelytwo and a half times heavier than air, the area ofdanger can be fairly well limited and kept under con-trol. Ether can be administered for anesthesia in sev-eral ways: (1) by pouring, or dropping, the liquid ona semiopen cone or face mask; (2) by intrapharyngealinsufflation of the vapor; (3) by a closed method of re-breathing, for which oxygen and a complete gas-oxygen machine are required; (4) by rectal injection ofliquid ether combined with a bland oil; and (5) as asupplement to other less potent anesthetic drugs.
The simplicity of the first method of administration,the semiopen method, makes this the most commonlyused method. It was the original way in which etherwas used, though the method has been varied, modi-fied, and improved over the years.
The second method, intrapharyngeal insuffiation, isof special value as a simple means of maintaining asmooth plane of anesthesia for surgery in the vicinityof the face, mouth, and throat when, for obvious rea-

LIQUID ANESTHETIC DRUGS
sons, a face mask could not well be used. After the.in-duction of surgical anesthesia has been brought aboutin some other way, insufflation of the vapor is madeby means of a nasal catheter, or oral tube, which isinserted so that the tip of the tube will lie in thenasopharynx. A motorized machine can be used forvaporizing the liquid ether, or a simple apparatuscomprising a bottle and hand bulb can readily beimprovised for the purpose.
The third method, the closed method, offers certainadvantages. The more important of these is the factthat an abundance of vital oxygen can be includedin the atmosphere breathed by the patient. Whenether is diluted with air only, some degree of oxygendeficiency will persist during anesthesia on account ofthe bulk of ether vapor and the latent depressanteffect of the drug on the respiration. It is generallyaccepted that some addition of oxygen increases thesafety of all anesthetics. Another advantage is the factthat the patient breathes a warm moist atmosphereinstead of the icy coldness produced by ether evapora-tion within the face mask. Still another is that con-tamination of the operating-room air with ether vaporis greatly minimized. Finally, normal respiration canmore readily be maintained. Abnormalities of respira-tion induced by the anesthetic, or emotional conditionof the patient, can seriously upset the fine adjustmentof the percentage of carbon dioxide in the bloodstream. Maintenance of the normal percentage ofcarbon dioxide is essential for proper functioning ofthe vital organs of the body.
In order to induce anesthesia by the fourth method,rectal injection of ether oil, four to six ounces of a50 per cent to 75 per cent ether-in-oil mixture areinjected into the rectum. Within a few minutes ethercan be detected on the patient's breath, for the drug
45

is excreted almost entirely through the lungs in thesame way as when ether is inhaled. Despite the oil,the solution is irritating to the mucosa, and it shouldbe injected very slowly in the hope of establishing alocal analgesia in the bowel to prevent expulsion ofthe enema. It is good practice to give the injectionwhile the patient is in bed so that an emotional upset,due to the conscious patient being removed to theoperating room, may be avoided.
The advantages of this method are: (a) the facecan remain uncovered; (b) when given in correctdosage, this form of ether anesthesia is nonirritatingto the lungs and air passages; (c) it does not seriouslyaffect the blood pressure; and (d) effective obstetricalanalgesia can be induced in this way simply and with-out injurious effects to mother or infant.
The disadvantages of this method are: (a) uncer-tainty in regard to individual patient's tolerance forthe drug over a long period of time; (b) inflexibilityof control of the depth of anesthesia, as in the case ofany drug which is given in single dose; and (c) thelikelihood of a mild delirium persisting throughoutthe period of anesthesia.
As the fifth method implies, a supplementary effect,small quantities of ether given at intervals will en-hance the anesthetic effect of less potent drugs with-out detracting greatly from their own peculiaradvantages.
Illustration of the induction of ether anesthesiawill be given in detail for the "drop method" only.
A stimulating maxim for the anesthetist to remem-ber is: "A difficult and bad anesthesia is the fault ofthe anesthetist, and not of the patient," or, it mightbe added, of the anesthetic drug employed. This say-ing is especially applicable to the ether-cone methodby which, for decades, the induction of anesthesia too
46 ANESTHESIA

LIQUID ANESTHETIC DRUGS
often resembled suffocation for lack of a little thought-ful understanding on the part of the anesthetist.
Concentrated ether vapor is irritating and difficultto breathe unless a tolerance for it is worked upgradually. This holds true even in the case of patientsalready unconscious by induction with some othermeans of anesthesia. Failure to appreciate this obviousfact for so long generated the common fear of "takingether." As a rule, the vapor was first applied in a fartoo concentrated form that was really nonrespirable;this caused the patient to obey the law of self-preservation and "fight for breath." But the more hefought the more he was restrained and forced to en-deavor to breathe the irritating vapor, and thus a"vicious circle" was set up. It is quite understandablethat a repetition of such an ordeal would be dreaded.
When properly administered, "open-drop ether" isnot at all difficult to breathe and of itself rarely causestroublesome coughing. The special disadvantage ofconfining the induction of anesthesia to ether is thatthe abnormal sensations involved in the gradual loss ofconsciousness persist for a relatively long time, andthe patient should be reassured repeatedly during thistime. A pleasing rule in the case of a child is to dis-tract his attention from the discomfort by telling hima story suitable to his age and temperament. It is agratifying compliment for the anesthetist later to besent for by the little patient "to come and tell the endof the story because I fell asleep in the middle of it."
The vapor of ether is not injurious to the eye butthe liquid drug, if accidentally dropped into the eye, isvery irritating to the mucosa, and this irritation is themore pronounced the longer evaporation of the drugis delayed. Friction of any kind on the exposed eyeballmay have serious consequences; corneal ulcers haveresulted from prolonged contact of a rubber-cushioned
47

nitrous oxide-oxygen face mask with the open eye.A wise rule for the anesthetist is to train oneself auto-matically to protect the patient's eyes at all times,both by keeping the eyelids closed and by preventingthe possibility of liquid ether getting into the eyes eitherfrom careless handling of the ether can or from seep-age from a saturated face mask. (The mask shouldnever be allowed to become saturated with the anes-thetic.) A drop or two of pure castor oil is soothingand harmless to the eye and, when applied early, isof much value in counteracting the irritant effects ofliquid ether.
Covering the eyes during anesthesia is a commonrule, but for it to be of value, precaution must betaken against the use of faulty material for the pur-pose. If the covering rule is to be followed, a soft wadof dampened absorbent cotton or a sound piece ofrubber tissue placed over the closed eyelids providesrelative safety.
Technique for drop-method ether. The face maskshould be of ample size to cover the nose and mouthof the patient and of sufficient height so that themoistened covering does not come in contact withthe skin of the face. A double thickness of closelywoven stockinette makes the best vaporizing mediumas a covering for the mask, though six to eight layersof gauze or a piece of bath toweling will answer thispurpose very well. A dropper can be provided for theether can in the form of a cork with a groove cut on twosides, in one of which a thin wick of rolled cotton isplaced; or a large safety pin can be passed throughthe soft lead cap of the can and fastened to serve asa dropper.
An effort should be made to gain the patient's con-fidence and co-operation by explaining the procedurebriefly. Describing the simplicity of the face mask
48 ANESTHESIA

LIQUID ANESTHETIC DRUGS
and letting him breathe through it for a moment be-fore any ether is applied will frequently allay anyfeeling of repugnance or claustrophobia he mighthave. Mention should be made that ether vapor ispungent but can be breathed easily in the way it willbe given. The mask is then laid lightly on the face,neatly covering the nose and mouth, and the ether isstarted, allowed to fall slowly drop by drop for sixto eight drops, then the rate of drop is increased gradu-ally to as rapid a rate as possible without causing em-barrassment of the patient's respiration. The rate ofdrop can be easily regulated by slight adjustment inthe method of holding the can. The flow should belimited to drops, slow or fast as indicated, but neveran uninterrupted stream.
Should any sign of embarrassment of respirationappear, or early efforts at struggling, the mask mustbe lifted momentarily and the rate of dropping theether slowed somewhat, the patient being reassuredmeanwhile and encouraged to relax and breathe nor-mally. Abnormally deep breathing is not helpful buttires and overventilates (reduces the carbon dioxidenecessary to maintain normal respiration). This mightprecipitate a temporary apnea and so defeat the ob-ject of hastening the induction of anesthesia.
Even after consciousness is lost, it may be necessaryto lift the mask occasionally to prevent the accumula-tion of too irritating a vapor, which, if allowed tocontinue, may cause congestion of the tongue andupper respiratory tract. A condition of stertorousbreathing, tightly clamped jaws, and increasing cya-nosis is typical of this state of congestion, which isdue to an insufficiency of oxygen. The condition canbe immediately remedied at this stage by the passageof a lubricated rubber tube or catheter through onenostril and behind the base of the tongue to the
49

pharynx. This will allow the free entrance of air andis a much simpler and safer procedure than trying toforce open a clenched jaw.
Once tolerance for a concentrated vapor of ether isestablished, it should usually be possible to completethe induction of anesthesia smoothly and quickly,with little evidence of excitement or discomfort onthe part of the patient. However, it is to be remem-bered that an early effect of the anesthetic is the un-dermining of the patient's power of self-control, andthe assistant must be alert to the possibility for needof restraint. This is commonly demonstrated by move-ment of the arms in an effort to remove the anestheticmask, for which the patient may have felt some re-sentment as he fell asleep. Grasping the elbows andpinioning them to the operating table is the best wayin which to control these movements, and with thearms under control the anesthetist should be able, tokeep the situation well in hand. This includes con-trol of movements of the patient's head and deepeningthe plane of anesthesia. It should be borne in mindthat resistance can frequently be quieted more effec-tively by lifting the mask from the face for a momentthan by increasing the concentration of the anestheticvapor.
Vomiting may occur during the induction period,especially if the stages are protracted. At the first signof retching, the head should be turned to one sideand an effort made to deepen the plane of anesthesia.Should vomiting occur, precautions must be takenfor avoidance of the possibility of aspiration of thefluid by providing for its free expulsion from thethroat and mouth. Lowering the head of the table,drainage by gravity, and the use of suctioning appara-tus may be of value in this respect.
The beginner is often surprised by the relatively
50' ANESTHESIA

LIQUID ANESTHETIC DRUGS
large quantity of ether that is required by the open-drop method to bring the patient to the surgical stageof anesthesia, but it should be evident that much ofthe ether dropped on the mask never reaches thepatient's lungs but is blown off into the surroundingatmosphere as he exhales. The induction period canbe inefficiently prolonged by a too generous flow ofether, in the evaporation of which the mask becomestoo chilled and frosty for the vapor to penetrate thecovering. The surgical "bad risk" kind of patient, be-cause of his debility and poor resistance, as a rule iseasily anesthetized but may also become criticallydepressed by the anesthetic drug, and special caremust be taken to prevent this from happening. Themost difficult patients to anesthetize are likely to bethe high-strung nervous individuals and, of course,the drug addicts and alcoholics, who have establisheda high tolerance for intoxicants. The medical opinionthat alcohol is not a stimulant applies also to thevolatile anesthetics. The "stage of excitement," whenit is evident, is ascribed to the drug's effect of releas-ing the patient's pent-up emotions by undermininghis powers of self-control, i.e., to the depressant effectof the drug on the higher mental centers.
Stages of anesthesia. These are classified as follows:(1) stage of analgesia, (2) stage of excitement or de-lirium, and (3) stage of maintenance or the surgicalstage.
Stage 1, stage of analgesia: This stage is character-ized by an increasing sense of unreality, by dizziness,ringing in the ears, lessening of the sensitivity to painand touch, tingling and numbness in the extremities.But the sense of hearing is sharpened, and noise isintensified. (It is well to remember, in regard to an-esthesia, that the sense of hearing is the last to be lostand the first to return and care should be taken to
51

avoid remarks which it is undesirable that the patientshould hear.) Control of the respiration in this stageis voluntary, and the patient should be encouragedto breathe normally; holding of the breath probablyis an indication that the ether vapor is too concen-trated, and the mask should be lifted momentarily.The flushing of the face and neck, increase of pulseand blood pressure, and active eyes with dilated pupils,which are commonly noted during the inductionstages of anesthesia, are ascribed to the primary stim-ulating effect of the anesthetic on the sympatheticnervous system.1 As the plane of anesthesia deepens,the alert, conscious expression of the eyes changes toa fixed stare, frequently with the eyeballs in an ec-centric position.
Stage 2, stage of excitement: Loss of consciousnessmay be followed by delirium and muscular activity.But there is much variation in these reactions, andoften they do not occur at all; much depends uponthe skill with which the anesthetic is administered.During this second stage, the vital signs usually con-tinue to show evidence of stimulation. The respira-tion may be irregular and become stertorous. Thelatter condition is due to some obstruction of the air-way, probably congestion of the tissues caused by toogreat concentration of the ether. Approaching thecompletion of this stage, the respiration becomesrhythmic and peripheral muscular activity ceases. Lossof the eyelid reflex, i.e., movement in response totouch, is the signal of the entrance to the third stage,during which the muscular relaxation and generalappearance of the patient should resemble the con-dition of normal sleep.
Stage 3, stage of maintenance: The surgical stage isfrequently referred to as embodying three planes. This
1Henry K. Beecher, The Physiology of Anesthesia, p. 8.
52 ANESTHESIA

LIQUID ANESTHETIC DRUGS 53classification is based upon the degree of concentra-tion of the drug which must be built up in the bodytissues in order to prevent muscular reaction to pain-ful stimuli. The degree of concentration varies inaccordance with the severity of the pain. This in turnmay vary according to the area of the body which isinvolved and the care with which sensitive tissues arebeing handled. The appearance of the eyes and thecharacter of respiration are the guiding signs for rec-ognition of these planes of anesthesia.
Generally speaking, the eye signs for the first planeare a slowly oscillating eyeball and a contracted pupil;those for the second plane, a quiet eye in normalposition and a slightly widening pupil; and for thethird plane, a still, dry eye with dilated pupil. Relax-ation of the pupil in the third plane of anesthesia isof paralytic origin. (The corneal reflex, often referredto in relation to anesthesia, is lost at the beginning ofthe second plane.) Of course, these signs are not clear-cut; they may overlap, are progressive, and may bemarkedly altered by the effects of premedication.
The wise anesthetist learns to evaluate the characterof the respiration and is guided largely by that mostvital function. Throughout the surgical stage, thebreathing should be regular with evident movementof the chest wall. The depth of respiration is of greatersignificance than is the rate, which may vary greatlyin accordance with the age and state of health of theindividual patient, and the type and quantity of pre-medication which has been given to him. Once thisrespiratory rate has been established for the case inhand, an increase in the rate is commonly the firstsign of reaction to greater stimulation at the operativefield, and this calls for deepening of the plane ofanesthesia.
The more painful the surgical procedure, either

due to the sensitivity of the tissues involved, or to themanner in which they are being handled, gently orroughly, the deeper will the plane of anesthesia haveto be in order to prevent reaction to the pain. Thereis much difference in sensitivity of the body tissues.In a general way, areas of the skin, peritoneum, muco-cutaneous borders, and joints are the most easilystimulated. The muscles, the brain, abdominal viscera,and bone are much less sensitive to surgical interfer-ence. The experienced anesthetist can adjust theplane of anesthesia to suit the need of the momentby watching the progress of the operation sufficientlyto anticipate painful stimulation. This precautionwill aid much in preventing delay and embarrassmentfrom muscular reaction to pain during the course ofthe operation. For instance, in the case of laparotomy,a deeper plane of anesthesia is necessary for the in-cision of the skin, the opening of the peritoneum, ex-ploration of the abdominal cavity for exposure of theorgan needing correction, such as lifting the uterusfrom its pelvic bed, and the "walling off" of the intes-tines with gauze sponges, than will be required forsurgery of the visceral organs alone. A long surgicalprocedure of this kind can be carried on satisfactorilyunder a plane of light anesthesia for the most part,provided the surgeon is reasonably gentle in hismanipulations and the anesthetist is understandinglyalert to the need of deepening the anesthesia in timeto prevent reaction to the greater stimulation thatthe preliminary steps for closure of the peritoneumwill involve.
The ability to adjust skillfully the degree of anes-thesia to the need of the moment largely constitutesthe "art of anesthesia," and the conscientious anes-thetist will find it most stimulating and essential tomaster this art, for danger to the patient lies much
54 ANESTHESIA

LIQUID ANESTHETIC DRUGS
more in the degree of concentration of the anestheticdrug in his body tissues than in the length of time theanesthesia is maintained.
Although, when properly given, ether is not difficultto breathe, the abnormal sensations of the first two orthree minutes before consciousness is lost may be dis-turbing to some hypersensitive people, especiallychildren. Also, if at some previous time the patienthas suffered severe nausea following ether anesthesia,the odor of ether may cause repulsive recollectionof the experience. Realizing these drawbacks, manyanesthetists nowadays start the induction with ananesthetic of more rapid action: nitrous oxide, Vin-ethene, ethyl chloride, or intravenous pentothal. Withany one of these drugs consciousness can be blottedout within one minute.
For the induction of anesthesia in a child, nitrousoxide has the advantage of being practically odorless.The procedure can be made very simple: a smallrubber tube connected to a nitrous oxide tank or gas-oxygen machine is placed under the open-methodether mask, and the child is reassured that "there willbe no smell to it." The gas flow must be very gentle,and unless oxygen is given with it, the face mask mustbe arranged so that plenty of air can circulate underit also. A few breaths of the gas dulls the sense ofsmell so well before consciousness is lost that the etherdrop can then be started carefully without unpleasantreaction from the child. For a safe, smooth induction,any degree of cyanosis must be carefully avoided, butit is necessary to continue the flow of gas until a tol-erance for a concentrated ether vapor has been gradu-ally worked up. This tolerance can be establishedmore quickly than when ether only is being used.When Vinethene or ethyl chloride are used for in-duction to ether, the drug is dropped slowly on the
55

open mask, and since the effects are very similar tothose of nitrous oxide, practically the same procedureis followed as for the gas. In either case, the procedurecalls for practice and skill and, above all, the desireof the anesthetist for its satisfactory accomplishment.
The advantages of ether, when used in therapeuticdosage, are: (1) the potency is sufficient for the controlof severe pain reflexes; (2) the planes of anesthesia areelastic and readily definable; (3) the margin of safetyis relatively large; (4) little change is effected in thepulse and blood pressure; (5) it is relatively harmlessto normal body tissues; and (6) the apparatus that isnecessary for its effective use is very simple.
The disadvantages of ether are: (1) the vapor is ir-ritating to the epithelium of the respiratory tract andcauses increased secretion of saliva and mucus; (2) itis irritating to the lungs and kidneys, especially wheninflammation is already present; (3) it causes muchincrease in blood sugar so its use is dangerous in thepresence of diabetes unless the diabetic state is undercontrol; (4) the incidence of postanesthetic nauseaand vomiting is higher than with other anestheticdrugs; and (5) ether is inflammable.
CHLOROFORM ANESTHESIA
Chloroform, CHC13, is a clear, heavy liquid ofsweetish odor with a high anesthetic potency. It has aboiling point of 61° C., much higher than that ofether, so the evaporation rate of chloroform is slower.This slow evaporation is an advantage under tropicalconditions, but normal conditions present a need forprecaution against toxic accumulation of the drug onthe face mask in the event of shallow or erratic breath-ing.
The vapor of chloroform is relatively nonirritating
56 ANESTHESIA

LIQUID ANESTHETIC DRUGS 57
to the air passages and can be breathed easily, so as arule the induction of anesthesia is comfortable andrapid with little evidence of a stage of excitement.Unfortunately chloroform does not compare favorablywith the other anesthetics in regard to safety, for it isa cardiac depressant, exerting a poisonous effect onthe heart muscle. In serious accidents under chloro-form anesthesia the heartbeat stops before, or at themoment of, cessation of respiration, and the possi-bility of resuscitating the patient is slight. Fatalitiesunder chloroform are particularly shocking usually,for they are more likely to occur in the "good risk"patient, and during the induction stage before anes-thesia is complete, rather than from an overdose ofthe drug. An explanation for this is given by Levy 2on the principle that the toxic effect of chloroformcauses pronounced cardiac irritability and hypersen-sitivity to stimulation of the sympathetic nervous sys-tem. He warns that an overflow of adrenalin fromthe adrenal glands, precipitated by excitement orfear, or by painful manipulation before the sensorynerves are paralyzed by the anesthetic, can throw theirritable heart into a state of ventricular fibrillation.Levy stresses the danger from surgical interference intoo light a plane of anesthesia, both during the in-duction and recovery stages. Adrenalin or epinephrinemedication in any form is definitely contraindicatedduring chloroform anesthesia.
Chloroform may also cause serious damage to theliver. Wesley Bourne 3 reported experimental studiesgiving proof that liver function is depressed for eight
; A. Goodman Levy, Chloroform Anaesthesia, p. 23.s Wesley Bourne, Morris Bruger, and N. B. Dreyer. Effects of
general anesthesia on function of the liver; the effects of Amytaland Avertin, separately, on the blood, its reaction, the carbon dioxidecombining power, and the concentration; on body temperature; onthe function of the liver; and on the, rate of secretion and composi-tion of the urine. Anesthesia and Analgesia, 10:85.

days by half an hour of chloroform anesthesia. Hefurther states that following a two-hour anesthesia,the liver function is not fully restored for six weeks."Delayed, or secondary, chloroform poisoning" is acondition of necrotic changes in the lobules of theliver, sometimes described as "fatty degeneration ofthe liver." The symptoms are those of acute acidosis,and the condition usually terminates fatally. As ameans of safeguarding the liver against the damagingeffects of anesthetic drugs, it is suggested that thepatient be given generous quantities of sugar or glu-cose during the day preceding operation, whenpossible, in order to promote storage of liver glycogen. 4
Technique for induction of chloroform anesthesia.Chloroform may be given by the open-drop method,by insufflation of the vapor with oxygen, or it maybe added in very small proportion to nitrous oxide-oxygen in order to increase the efficiency of the gaswhen a potentially explosive anesthetic mixture iscontraindicated. Chloroform is not inflammable. Theopen-drop method only will be described in detail.
The face mask for open-drop chloroform must bemore open and less thickly covered than the ordinaryether mask, for chloroform is approximately ten timesmore potent than ether.5 Chloroform is vesicant tothe skin if evaporation is delayed, so the face shouldbe lightly anointed with vaseline or cold cream beforethe mask is applied. The patient is reassured, andthen the drug is started, drop by drop, increasingslowly, as a tolerance for the vapor is worked up, to arate of about thirty drops per minute. As previouslynoted, special care must be taken to prevent frightand discomfort and to avoid accumulation of the
'M. D. Nosworthy, The Theory and Practice of Anaesthesia, p. 82.SArthur E. Guedel, Inhalation Anesthesia. A Fundamental Guide,
p. 10.
58 ANESTHESIA

LIQUID ANESTHETIC DRUGS 59
drug on the mask during interruption of the rhythmof breathing. The stages of anesthesia, in general, aresimilar to those of ether, but they follow each othermore quickly. The outstanding differences in effectsfrom those of ether are that the face is more likelyto be pale than flushed since there is decrease of pulseand blood pressure and the respiration is shallowand quiet rather than stimulated. Increased pallor,bradycardia, and shallow, sighing respiration aresigns of dangerous overdosage. The maintenance of apatent airway and avoidance of cyanosis are essentialfor safety.
The advantages of chloroform are: (1) the vapor isnonirritating to the epithelium of the lungs and airpassages; (2) it is noninflammable (but excessive heatwill break it down into toxic phosgene gas); (3) thehigh boiling point makes its use practical in tropicalatmospheres.
The disadvantages are: (1) the drug is a powerfulcirculatory depressant and cardiac irritant; (2) itsometimes causes serious toxic effects to the liver andother vital organs; and (3) the margin of safety issmall.
ETHYL CHLORIDE
Ethyl chloride, C2H 5Cl, with a boiling point of 12.5°C., is used both as a local and as a general anesthetic.In either of these ways its usefulness is limited to verybrief procedures, one to three minutes. It is sold as aliquid in a metal or glass ampoule, which is fitted witha metal nozzle and finger-tip control valve. The liquidcan be delivered in drops or in the form of a fine sprayof vapor. General anesthesia can be induced with ethylchloride either by the open-drop or the closed method.As the term implies, the drop method is given on a

face mask that allows for much dilution of the drugwith air. This is the more commonly used method.With the closed method, 1 to 5 cc. of the drug aresprayed as a vapor into a breathing bag immediatelybefore the attached mask is applied to the patient'sface. The pungency of the vapor will cause embarrass-ment of respiration by either method if the vapor istoo concentrated, but this can be avoided of course.The patient loses consciousness in about thirty secondson breathing the vapor. This is followed rapidly byflushing of the face, muscular rigidity, and stertor. Asa rule, recovery after the mask is removed is equallyrapid, but the margin of safety is very narrow.
Ethyl chloride may be used for a quick induction ofether anesthesia, and the early loss of consciousnessgives tolerance for a higher initial concentration ofether vapor. However, any embarrassment of respira-tion, due to too strong a vapor of either drug, willdefeat this purpose of a rapid induction.
Analgesia for dental treatment work is obtainedwith a weak ethyl chloride vapor, by means of a nasalapparatus fitted with a hand bulb of rubber that thepatient controls. Should consciousness be lost, thepower to squeeze the bulb in order to vaporizethe drug goes with it, of course, and the patientquickly recovers.
The advantages of ethyl chloride are: (1) the rapidinduction and recovery periods that the drug affords;(2) the drug and apparatus required for its effectiveuse are compact and easily portable; and (3) a periodof one to two and a half minutes of anesthesia, with-out cyanosis, after the mask is removed, allows forbrief minor surgery without causing pain to the pa-tient.
The disadvantages are: (1) the depth of anesthesiais not readily controllable; (2) the margin of safety is
60 ANESTHESIA

LIQUID ANESTHETIC DRUGS
small; (3) stertor and muscular rigidity persist, witha tendency to laryngeal spasm; (4) postanesthetic nau-sea and vomiting are common with this drug; (5) thedrug is a circulatory depressant and cardiac irritant;and (6) it is inflammable,
VINETHENE
Vinethene, or divinyl ether, (C2H 3 )20, is a colorless,volatile liquid anesthetic. The high potency of thisdrug, estimated to be seven times greater than ethylether, allows for such great dilution that its pungentodor is less disturbing to patients than is that of ether.Anesthesia is effected very rapidly, and the recoveryperiod is equally short and comfortable with thisdrug. Owing to the speed of its action, the stages ofanesthesia are not clearly defined as they are withdiethyl ether. The very low boiling point, 28.30 C.,and the high volatility of the drug increase the diffi-culties of maintaining an even plane of anesthesia.Experimental work on dogs has given evidence ofliver damage following prolonged anesthesia with thisdrug; 6 in consequence, it is generally considered ad-visable to limit the time of anesthesia by open-dropmethod to one half hour. This drug is uniquely valu-able as an agreeable anesthetic for very brief painfulprocedures, to ease and hasten induction of ether an-esthesia, and to supplement nitrous oxide. The bestguide for judging the depth of anesthesia and condi-tion of the patient is the respiration, the excursionof which must always be kept adequate to allow forgood exchange of oxygen and carbon dioxide. Muscu-lar relaxation and control of pain reflexes, sufficient
e Samuel Goldschmidt, I. B. Ravdin, Baldwin Lucke, G. P. Muller,C. G. Johnston, and W. L. Ruigh. Divinyl ether: experimental andclinical studies. J. A. M. A., 102:21.
61

for many minor operative procedures, develop withintwo to three minutes, as soon as the conscious expres-sion of the eyes is lost and before the eyelid reflex istotally abolished.
When given by the open-drop method, the facemask must be less thickly covered than is needed forether. Vinethene should be dropped slowly on themask and increased only moderately as the breathingtolerance is established. A high concentration of thevapor causes respiratory embarrassment and anexcessive flow of saliva and mucus, and dangeroussymptoms may quickly develop. Premedication withatropine to control secretions is indicated with thisdrug unless the anesthesia is to be very brief. Vin-ethene can also be given by the closed rebreathingmethod, in combination with oxygen and the gaseousanesthetics. Frequently it is used for a quick induc-tion of ether anesthesia.
The advantages of the drug are: (1) the inductionand recovery periods are brief; (2) postanesthetic nau-sea and vomiting are very rare with the use of thisdrug; (3) a minimum of apparatus is necessary foreffective results; and (4) its high potency is helpful forthe induction of ether anesthesia and to supplementnitrous oxide-oxygen.
The disadvantages are: (1) the plane of anesthesiais not readily definable; (2) some liver damage may becaused by prolonged anesthesia with this drug; and(3) in combination with air or oxygen, it is inflam-mable.
62 ANESTHESIA.

Chapter 7
GASEOUS ANESTHETICS: NITROUSOXIDE, ETHYLENE,CYCLOPROPANE
SOME knowledge, in detail, of the apparatusinvolved in the use of the gaseous anesthetics is es-sential for a general understanding of the subject asa whole.
The gases commonly used for the purpose of surgi-cal anesthesia at the present time are the anesthetics,nitrous oxide, ethylene, cyclopropane; and the adju-vants, oxygen, carbon dioxide, and helium. Thesegases are marketed, under great compression, in heavysteel cylinders that are fitted with a valve head andkey, i.e., hand wrench, for attachment of the cylinderand release of the gas to the gas-oxygen machine. Themachine provides for the accurate proportioning andmixing of the gases for administration to the patient.
The cylinders of each gas are of several sizes desig-nated by letters, A through G. The sizes D, E, andG are most commonly used on hospital apparatus.The cost per gallon of gas decreases in proportion tothe increase in the size of the cylinder; but in order to
63

use the large G cylinder, a truck of special construc-tion with a connecting metal tubing is necessary. Insome large hospitals where a great deal of "gas anes-thesia" is used, the gases are piped into the operatingroom under reduced pressure from a main supply base.
The initial pressure of each gas is uniform for allsizes of cylinders. But this pressure varies considerablyfor the different gases and depends upon the molecu-lar weight and response to compression of the individ-ual gas. The pressure range is from 75 lbs. per squareinch for cyclopropane to 2000 lbs. per square inch foroxygen.
For control of this great force, all gas machines arefitted with a finely adjusted valve at each inlet. Thiscontrol valve must be closed before the cylinder isopened; this is essential in order to prevent the dangerof personal injury as well as damage to the gas-oxygen machine. Within recent years neglect of thisseemingly small detail was responsible for the deathof an anesthetist who was critically injured by flyingglass when the machine was demolished by an oxygen-pressure explosion.
Identification of the gas content of cylinders is madereadily apparent by a uniform color system agreedupon by the anesthetic-gas distributors of Americaand approved by the United States Bureau of Stand-ards. An individual color is assigned to each gas re-gardless of the size of the cylinder. In addition, adistinctive label is pasted on each cylinder giving thename of the gas, weight of cylinder and of contents,etc. Manufacturers of the gas-oxygen machine alsohave done their best to safeguard against mistakenidentity of the gases by a similar distinct system oflabeling. Occasionally, however, tragic accidents hap-pen from one of the anesthetic gases being mistakenlyused in place of vital oxygen. Such an accident is in-
64 ANESTHESIA

excusable, for with proper precaution it is alwayspreventable.
The usual sequence of such an accident is thatcylinders of oxygen and nitrous oxide emptied on aprevious case have been replaced by full cylinders,but they have been accidentally transposed on themachine. This has remained unnoticed. Many gas-oxygen machines are fitted with duplicate cylindersof each gas, and for the next patient the anesthetist,while using the original oxygen outlet, happens to usethe duplicate outlet for the anesthetic gas. Very soonthe patient's color proclaims the pressing need foroxygen, and the anesthetist opens the emergency valveand too late realizes the patient has been asphyxiatedby a blast of nitrous oxide from the transposed cyl-inder. (The oxygen valve is equipped with an emer-gency valve in addition to the control valve, by whichoxygen can be added in large quantity should such aneed arise.) No one is wholly infallible, and too muchemphasis cannot be put on the need for constantvigilance for the avoidance of such tragic accidents.Before starting the anesthesia, a thorough checkmust be made by the anesthetist for assurance thatthe entire equipment is identified correctly. This isan essential rule for the correct dispensing of allmedication.
At the close of each case, the face mask, breathingtubes, and bag need to be thoroughly washed withliquid soap and running warm water. When this isdone thoroughly, it is sufficient cleansing of thesearticles for the routine case; but additional boiling, orsoaking in an antiseptic solution, is indicated whenthey have been used for a patient suffering from anyform of infectious respiratory disease. Boiling is theideal way to disinfect rubber articles, but rubber cuffsof all descriptions must be deflated before immersion
65GASEOUS ANESTHETICS

in boiling water to prevent expansion of the enclosedair and consequent rupture of the cuff. Celluloid at-tachments, facepiece, etc., should be sterilized in theantiseptic solution since they are ruined by boiling.The disagreeable odor left on rubber by soaking ina solution of the phenol derivatives makes this groupof antiseptics undesirable for rubber equipment.
Another advisable precaution in cleaning the ma-chine between cases is the rinsing out of pungentodors of ether and ethylene, which cling to all thetubes and passages. This can be effected by a briskflow of the practically odorless oxygen or nitrous ox-ide for a few moments. This practice is essential if theanesthetist plans to coax a patient to accept nitrousoxide-oxygen anesthesia readily with the promise"there is no smell to it."
Nitrous oxide being a "weak anesthetic," i.e., ef-fective for the average patient only when given in veryhigh concentration, presented several problems to besolved before it attained its present high status insurgical anesthesia. The danger of the complication ofanoxia, which was the most important problem, wassolved by the substitution of oxygen for air as thediluent. Another problem was the risk of overventila-tion, profound loss of carbon dioxide from the system.This is caused by the stimulation of breathing due toinefficient control of pain reflexes by an anesthetic oflow potency. This problem was solved by sedativepremedication and the inclusion of a breathing bagbetween the cylinder outlet and the face mask. Thebreathing bag allowed the patient to rebreathe aportion of his exhaled carbon dioxide and in thisway to circumvent apnea caused by overventilation.An exhaling valve provided a means of escape for ex-cess carbon dioxide. Of course, much of the anestheticgas was lost also through the exhaling valve, and a
66 ANESTHESIA

GASEOUS ANESTHETICS
continuous flow of gas from the cylinder was necessaryin order to replace this loss as well as to replace oxy-gen used in the body metabolism.
The publication in 1926 by Dr. Ralph M. Waters 1
of the encouraging results he obtained by filtering thecarbon dioxide from the exhaled gases, in order thatthey might be effectively rebreathed for prolongedperiods, led to the present-day general adoption ofthe method of closed rebreathing. In addition to greateconomy in the use of the gases, the method providesfor adequate control of the respiration by control ofits normal stimulant, carbon dioxide, as the filter canbe turned in and out of the circuit at will. It alsoaffords an excellent means of artificial respiration incase of need.
The gases are filtered by being passed through achamber filled with soda-lime (sodium and calciumhydroxide), which has an affinity only for the carbondioxide in the exhaled mixture. The carbon dioxidereacts with the hydroxide to form a carbonate.
Two types of filter chambers are available: theoriginal "Waters' to-and-fro," and the "circle" appa-ratus. With the former, as the term implies, thepatient breathes both in and out through the soda-lime. The filter chamber is inserted between the facemask and breathing bag and in direct contact withthem; no valves are involved. With the circle type ofapparatus, the filter chamber and breathing bag areattached to the gas-oxygen machine, and connectionwith the face mask is made by means of two large-caliber, corrugated-rubber tubes. Sensitive valves areinterposed so that the exhaled gas mixture can bepassed through the filter and on into the bag, fromwhich the purified gases are returned direct to the
1 Ralph M. Waters. Advantages and technic of carbon dioxidefiltration with inhalation anesthesia. Anesth. and Analg., 5:160.
67

face mask to be rebreathed by the patient, so com-pleting the circle.
The to-and-fro apparatus is simpler and less ex-pensive than the circle type, is readily portable andinterchangeable from one gas machine to another,and the "dead space" is decreased by the absence oflong breathing tubes. This last feature is of specialvalue with the shallow, rapid breathing common inyoung children and febrile patients. The special ad-vantage of the circle apparatus is that the weight ofthe canister of soda-lime is borne by the gas-oxygenmachine, so there is less drag of the face mask toimpede its leakproof adjustment to the patient's face.However, this desirable tight adjustment can usuallybe maintained with the to-and-fro apparatus if alittle ingenuity is exercised in the support of thecanister. In skilled practice, the omission of a by-passvalve seldom presents a serious problem.
Success with either method depends upon the useof a high grade of soda-lime, with granules of 4 to 8mesh. In recent years another absorbent, Baralyme(barium and calcium hydroxide), has become avail-able. The material is compressed into uniform hardpellets that have the advantage over soda-lime gran-ules of greater stability in form, thus diminishing thedanger of the patient's inhaling dust from the ab-sorbent.
The duration of absorbent efficiency of both ofthese agents depends, of course, upon the amount ofcarbon dioxide that is being excreted by the patient.This, in turn, depends upon the age, size, and me-tabolic rate of the patient. Any condition that in-creases the metabolism causes an increase in theconsumption of oxygen and the production of carbondioxide in the body system. Normally, the rate ofmetabolism is highest in extreme youth, decreasing
68 ANESTHESIA

slowly in adults. But throughout life, the rate is in-creased in varying degree by such stimulating factorsas fever, certain forms of toxicosis, pain, fear, andemotional excitement of all kinds. In the normal case,an average of five to seven hours of absorbent effi-ciency may be expected from each charge of the filter.
As the filter efficiency becomes exhausted, the clini-cal signs of accumulating carbon dioxide are clearlyevidenced by marked stimulation of breathing andincrease in systolic pressure. The pulse rate, usually,is also increased if the stimulation is prolonged. Mostof the modern gas-oxygen machines allow for rapidchange to a fresh charge of the absorbent, with littleinterference in the smoothness of the anesthesia.
There are several types of gas-oxygen apparatusbearing trade names on the market, and equally goodresults can be obtained with them all. Requisite forthis, of course, are familiarity with the machine andskill on the part of the anesthetist. Fundamental com-ponents for the machines are: a means for the ac-curate measurement and mixing of one or moreanesthetic gases and oxygen, a reservoir for ether,breathing bag, tubes, and face mask. Provision shouldbe made for duplicate cylinders of oxygen equippedwith valves for both fine and coarse control of oxygenflow so that an abundant supply of oxygen is readilyavailable in case of emergency.
NITROUS .OXIDE
Nitrous oxide gas, N20, is very soluble in the bloodand is carried by the plasma in simple solution.2 Afterpassing through the body, it is excreted in its originalgaseous form by the lungs. When the gas is breathedundiluted, consciousness is lost within twenty to
Goodman and Gilman, op. cit., p. 81.
69GASEOUS AlNESTHETICS

thirty seconds, and a state of asphyxia rapidly de-velops if breathing of the gas continues. However, ifthe gas flow is stopped, a state of analgesia persists forone to two minutes before full consciousness is re-established, a sufficient time for the rapid extractionof one or a few teeth. For many years. before nitrousoxide was accepted as an anesthetic for surgery, thefollowing simple method of gas anesthesia was widelyused in the dental office. The patient's mouth wasopened, inspected, and a prop inserted between theupper and lower teeth before the face mask was ap-plied-a necessary precaution against extreme diffi-culty in opening the mouth when the jaw musclesbecame rigid from .oxygen insufficiency. As soon asthe ,patient lost cbnsciousness, the face mask wasthrown aside and the work commenced. The numberof teeth that could be extracted without pain for thepatient depended chiefly upon the skillful speed ofthe dentist. The appearance of the patient meanwhilewas usually sufficiently alarming to discourage hisbeing subjected to a repetition of the ordeal on thesame day, even though his recovery was immediateand uncomplicated. The forced brevity of the expe-rience probably accounts for the fact that serious ac-cidents very seldom complicated this precarioustechnique of dental anesthesia.
The addition of oxygen to the anesthetic gas andthe use of a nasal inhaler have eliminated the needfor speed in dental surgery, and extensive procedurescan now be safely undertaken.
Nitrous oxide analgesia. Without loss of conscious-ness nitrous oxide analgesia is practiced for prolongeddental treatments by means of a small inhaler madeto fit over the nose only, which is held in place by astrap passed around the patient's head. The gas, muchdiluted with air or oxygen, is delivered through a con-
70 ANESTHESIA

GASEOUS ANESTHETICS
necting tube to which is attached a simple rubberbulb, or spraying valve, that the patient controls withhis hand. Should the stage of analgesia begin to de-velop into true anesthesia, the patient's pressure onthe valve relaxes, automatically shutting off the flowof gas, and the patient recovers consciousness. A sim-ilar method of analgesia can be used effectively inobstetric practice for the relief of the intermittentpain of the late first and early second stages of laborwhen an anesthetist is not immediately available.Analgesia alone can be relied upon for these caseswhen the proportion of nitrous oxide in the mixtureis not allowed to exceed 50 per cent. A £fae masklarge enough to cover the patient's nose and mouth isdesirable, but in order that it will fall off if the pa-tient goes to sleep, it must not be in any way fastenedto the face.
Nitrous oxide-oxygen surgical anesthesia. This gascombination is weak in its power to control the re-flexes that result in muscular movements and rigiditycaused by the pain of surgery. It is unsatisfactory asa surgical anesthetic for the average case unless it issupported by adequate premedication and unless thedilution of the anesthetic gas is limited to 20 per cent-the proportion of vital oxygen in the atmosphere wenormally breathe.
Nitrous oxide is considered to be the least toxic ofall the inhalation anesthetics and is noninflammable.Consequently, it is quite worth while for the anes-thetist to make the effort necessary to become expertin the use of nitrous oxide-oxygen. Its possibilitiesas a surgical anesthetic are considerably wider than isgenerally appreciated. The technique calls for carefulattention to detail in several ways, as follows: (1) anendeavor to gain the patient's confidence and co-oper-ation and to allay apprehension; (2) adequate narcotic
71

premedication for relief of pain; (3) rinsing out of alldiluting air from the lungs and tissues of the body;(4) avoidance of painful manipulation during the in-duction period; and (5) gentle surgical handling of thebody tissues throughout the operation-a strong pleafor this anesthesia, for it is a well-recognized fact thatan important contributing cause of surgical shock istrauma to tissues.
Although undiluted nitrous oxide is practicallyodorless, nonirritating, not at all difficult to breathe,and unconsciousness is rapidly induced, the sensationsexperienced may be definitely unpleasant. Sometimesthese sensations have been described as a feeling of"being forcibly blown into a tunnel," or of one's head"bursting open." These discomforts are caused by thesudden deprivation of oxygen and can be entirelyprevented if about 10 per cent of oxygen is used withthe nitrous oxide from the start of the induction andloss of consciousness will be delayed for only a minuteor so. The patient's color must be watched carefully,and as soon as it becomes slightly dusky, or bluish,the oxygen should be increased to the minimum safemaintenance proportion of 20 per cent. In the case ofsmall children and the "poor risk" type of patient, itis wise to use 20 per cent of oxygen in the mixturefrom the start and a larger proportion during themaintenance stage.
From long experience in the use of nitrous oxide-oxygen anesthesia, for major as well as for minor sur-gery, the author is convinced that nothing is gained byreducing the proportion of oxygen during the mainte-nance stage below the 20 per cent of atmospheric oxy-gen, and, furthermore, that any degree of oxygendeficiency induces a corresponding degree of muscularrigidity or spasm. A demand from the surgeon fordeepening the plane of anesthesia is prompted by the
72 ANESTHESIA

need for adequate muscular relaxation, and the onlysafe and sensible thing to do in an effort to satisfythis need is to supplement the weak anesthetic gaswith some more potent drug. Usually the addition ofa small amount of the potent drug at infrequent in-tervals will prove sufficiently effective, and this willcause little untoward complication of the recoveryperiod.
The maintenance of a clear airway is essentialthroughout the period of unconsciousness. To preventthe relaxed, or congested, tongue from blocking thepharynx, it may be necessary to insert an oral or nasalairway tube. (Figure 4, Chapter V.) These tubes arecurved and of sufficient length to pass into the pharynxat the base of the tongue. The tube should be lubri-cated and inserted carefully. An oral tube is moresatisfactory when the tissues are relaxed and themouth easily opened as, despite care to avoid it,troublesome bleeding from sensitive nasal mucosamay be caused by the passage of a nasal tube. How-ever, if the obstruction is caused by congestion, therigidity of the jaw makes opening of the mouth sodifficult that the nasal tube is indicated. Under theseconditions the result when the nasal tube reaches thepharynx is gratifyingly spectacular.
Induction of nitrous oxide-oxygen anesthesia. Imme-diately before the patient is taken into the room wherethe anesthesia is to be started, the anesthetist shouldmake a final inspection of the gas-oxygen machine tomake sure that it is in good order, that no gas cylinderis empty or misplaced, and that ether is readily avail-able should it be needed for the control of an activestage of excitement. The gas-control valve for bothnitrous oxide and oxygen should then be closed andthe cylinder valves opened. The breathing bag is theninflated about three quarters full, with a measured
73GASEOUS ANESTHETICS

proportion of each gas to allow for at least 10 per centoxygen. (Most gas machines are equipped with anobturation valve so that the breathing bag can befilled beforehand without loss of gas.) When all is inreadiness, the patient is reassured, and a final inspec-tion made of his mouth for loose teeth, removabledentures, etc. The face mask is then gently applied tocover the nose and mouth, and the obturation valveis opened to release the gas mixture from the breath-ing bag. The patient meanwhile is instructed tobreathe normally. The exhaling valve is open at thistime, and a flow of the two gases is started in orderto replace that which is being intentionally lostthrough this valve.
As the patient becomes drowsy, the mask is securelyfastened onto the face. The oxygen proportion is in-creased sufficiently to keep the patient's color normal,and if a stage of active excitement is induced, a littleether vapor should be added to the anesthetic mixture.It should be remembered that though the patient isunconscious, a tolerance for ether vapor must beworked up gradually in order to prevent embarrass-ment of respiration. As soon as surgical anesthesia isestablished, the ether can be stopped and from thenon added intermittently when and if indicated.
If the machine is not equipped with a carbondioxide filter chamber, the flow of both gases in cor-rect proportion must continue throughout the anes-thesia in order to allow for the spillage of excesscarbon dioxide. But when the filter is to be used, theobject of the open exhaling valve and continuous flowof the anesthetic gas is to get rid of nitrogen from thepatient's lungs, which otherwise would too greatly di-lute the nitrous oxide. Depending upon the characterof the respiration, five to eight minutes are needed forthis purpose, after which the breathing bag is quickly
74 ANESTHESIA

GASEOUS ANESTHETICS
emptied by manual pressure and refilled with themaintenance proportions of the two gases. Then theexhaling valve is closed, the nitrous oxide flowstopped, and the filter turned into the circuit. Theflow of oxygen, adjusted to the probable metabolicneed of the individual patient, must continue through-out the time of anesthesia in order to replace theoxygen used in the metabolic processes. A flow ofoxygen at the rate of about 350 cc. per minute is sat-isfactory for the average adult.
A leakproof adjustment of the face mask is neces-sary if the rebreathing is to be complete, but precau-tion must be taken against the danger of injury to theface due to pulling the straps of the inhaler too tight.Frequent gentle massage of the face, especially aroundthe prominence of the cheekbones, stimulates the cir-culation of the area and thus helps in the preventionof pressure sores. When a continuous slight leakagecannot be safely prevented, the bag pressure shouldbe maintained by a compensating small continuousflow of the anesthetic gas with sufficient additionaloxygen to keep up the correct proportions. The breath-ing bag should be emptied and refilled with freshgases at about fifteen-minute intervals during the firsthour of anesthesia in order to get rid of traces ofdiluting nitrogen that are being gradually freed fromthe body tissues.
With the gaseous anesthetics the stages of anesthesiafollow each other too rapidily for detailed identifica-tion other than loss of consciousness, evidence of ex-citement, and the relaxation of normal sleep. Duringthe maintenance stage, when the patient's color isnormal, the eye signs that are helpful with ether anes-thesia are absent. The pupils as a rule remain con-tracted, and when the anesthetic is limited to nitrous
75

oxide-oxygen, a slow oscillation of the eyeball com-monly persists throughout the anesthesia.
The cardinal rule to follow with nitrous oxide-oxygen anesthesia is to keep the patient's color normalat all times because anoxia, oxygen deficiency, con-stitutes the sole danger. To prevent anoxia, in addi-tion to an adequate proportion of oxygen in thebreathing bag, a clear airway, free from mucus or anyform of obstruction, is essential. Color changes arenot as clearly evident in patients who are pale andanemic, and this type of patient is also hypersensitiveto medication and is easily anesthetized. It is, there-fore, well to keep more than the usual 20 per cent ofoxygen in the breathing bag during the maintenancestage with such cases. One can always resort to theaddition of a small quantity of a more potent drug ifnecessary for control of inconvenient reaction to pain.A proportion as high as 50 per cent oxygen withnitrous oxide sometimes will provide adequate anes-thesia for a patient in shock.
ETHYLENE-OXYGEN
Ethylene (C2H 4) is a highly volatile gas with aspecific gravity slightly less than that of air. It has apungent, somewhat disagreeable odor, but the gas isnonirritating, and on breathing it, one's sense of smellis so quickly abolished that this odor is of no greatimportance. The anesthetic potency of ethylene is alittle higher than the potency of nitrous oxide. Guedelranks the gas as 10 per cent higher in potency thannitrous oxide.3 Consequently, ethylene-oxygen is rathermore effective in controlling the reflexes of pain anda smooth anesthesia can be maintained more easily.
a Arthur E. Guedel, Inhalation Anesthesia. A Fundamental Guide,p. 60.
76 ANESTHESIA

The technique for the administration of ethylene-oxygen anesthesia is identical with that described fornitrous oxide-oxygen. The significant difference be-tween these two gases is the fact that ethylene ispotentially explosive and precautions must be takento avoid this danger. The use of this gas in the pres-ence of an open flame or sparking electric apparatusis unjustifiable. It is essential to bear in mind alsothat a potentially explosive combination is formedwhen ether is added to nitrous oxide-oxygen.
The importance of preventing anoxia of any degreeand of keeping the color of the blood consistentlynormal should be emphasized equally for ethylene-oxygen and for nitrous oxide-oxygen anesthesia.
CYCLOPROPANE-OXYGEN ANESTHESIA
Cyclopropane (C3H 6) is a volatile gas, considerablyheavier than air, with a slightly pungent not unpleas-ant odor. It is readily inflammable when mixed withoxygen or air. Unlike nitrous oxide and ethylene, thisgas is of high anesthetic potency. Guedel classes cyclo-propane with the volatile liquid anesthetics as havinga potency of 100 per cent,4 i.e., sufficient for all planesof surgical anesthesia.
In rough calculation, when oxygen alone is usedas the diluting agent, the proportions are the reverseof those needed for the weak anesthetic gases. Anaverage of 20 per cent cyclopropane and 80 per centoxygen is the rule. As with any powerful drug, how-ever, these proportions must be varied and adjustedcarefully to accord with the general condition of theindividual patient and the type and quantity of seda-tive premedication that he has been given.
Cyclopropane in anesthetic dosage has little toxic4 Ibid.
77GASEOUS ANESTHETICS

effect on the body tissues as a whole. This fact andthe possibility of using an abundance of oxygen withit make this anesthetic especially valuable for thevery sick patient and for the patient whose circulationor ventilatory capacity is seriously impaired. Anes-thesia is induced quickly and comfortably with cyclo-propane-oxygen and rarely is it complicated by a"stage of excitement." As a rule the recovery period isshort and equally uneventful. But the anesthetist whois unfamiliar with cyclopropane may have difficultyin defining the planes of anesthesia during the main-tenance stage. Both cyclopropane and a high propor-tion of oxygen tend to depress the respiration.Therefore, with this combination of gases the breath-ing is quiet and shallow; yet the patient's color re-mains excellent on account of the excess oxygen.Neither can the depth of anesthesia be defined by theappearance of the eyes, especially when morphine hasbeen given beforehand, for the pupils rarely dilateunless a profound anoxia has been allowed to develop.Fortunately, in the event of an overdose of cyclopro-pane, the respiration ceases before the heart actionstops, and the experienced anesthetist can restore nor-mal breathing by inflating the lungs a few times withoxygen. This is done by intermittent manual pressureon the breathing bag after it has been quickly emptiedof the anesthetic and refilled with oxygen. Of course,it must be ascertained that there is no obstruction ofthe patient's airway.
Cyclopropane anesthesia may cause cardiac arrhyth-mia at times, but this complication can be quicklycorrected by further dilution of the anesthetic withoxygen. Consequently, a developing arrhythmia shouldbe recognized as a sign that the percentage of cyclo-propane has been increased beyond the level of toler-ance for the drug that is safe for that individual pa-
78 ANESTHESIA

GASEOUS ANESTHETICS 79tient. For correction of the arrhythmia, dilution ofthe anesthetic gas should proceed gradually, and itshould be stopped as soon as the pulse resumes normalrhythm, otherwise the anesthesia may become too in-efficient for the surgeon to proceed with the operation.A little ether vapor can be added to the gases if it be-comes necessary to deepen the plane of anesthesiabeyond the point made possible by the patient's toler-ance for cyclopropane.
The reason for this complicating arrhythmia re-mains a matter of controversy, but it is probably awise precaution to avoid the use of epinephrine inany form during cyclopropane anesthesia, in case thisdrug might add to the cardiac irritability.
Many patients suffering from cardiac disease, show-ing marked arrhythmia, have been successfullyanesthetized with cyclopropane-oxygen, and if the con-dition of the patient is sufficiently good to warrant theuse of general anesthesia, this gas is not necessarilycontraindicated, 5 for it affords several advantages asan anesthetic. Special care should be taken, however,to avoid any increase of pulse irregularity, and highconcentrations of the gas should not be used.
As a general rule the pulse rate is moderately slowedduring cyclopropane anesthesia. A sudden marked de-crease or increase of the pulse rate, or an arrhythmiathat cannot be otherwise accounted for, should beaccepted as signs that the concentration of cyclopro-pane in the anesthetic atmosphere is too high forthat individual patient, and reduction of the concen-tration by addition of oxygen is indicated.
Although the patient's blood pressure has been sus-tained remarkably well throughout a prolonged cyclo-propane anesthesia for major surgery, it may be found
t Ralph M. Waters. Cyclopropane-a personal evaluation. Surgery,18:28.

to have fallen to a seriously low level soon after heis returned to the ward. This phenomenon is explainedon the principle that the shallow breathing typicalof this anesthesia reduces respiratory exchange andconsequently a high level of carbon dioxide accruesin the blood stream. The superabundance of carbondioxide has a stimulating effect on the circulation,and the blood pressure is sustained until the excesscarbon dioxide is washed out of the system. Thiselimination is effected during the patient's wakingmoments when, in response to pain and restlessness,the respiration is stimulated. With the loss of carbondioxide the blood pressure falls, and a more accuratepicture of the patient's circulatory condition becomesevident.6
When, from the severity of the operation, somedegree of surgical shock is to be expected, this con-dition may be revealed earlier if nitrous oxide-oxygenis substituted for the cyclopropane anesthesia tenminutes or so before the operation is completed. Re-storative measures can then be started before the pa-tient is returned to bed, should this precaution seemto be advisable, for a state of shock may be seriouslyincreased by the handling that is involved in the re-moval of the patient from the operating table to thebed and ward.
Cyclopropane-oxygen may be used for anesthesiaeither in single combination or mixed with heliumor air. Cyclopropane may play the dominating rolein either a nitrous oxide-oxygen or ethylene-oxygenanesthesia, or its powerful anesthetic properties canbe employed in the same way as the volatile liquidanesthetics-to supplement these weak anesthetic
0 Robert C. Dripps. The immediate decrease in blood pressure seen
at conclusion of cyclopropane anesthesia; "Cyclopropane Shock."Anesthesiology, 8:15.
80 ANESTHESIA

gases. This range in flexibility of cyclopropane as ananesthetic supports the reasons that have been ad-vanced against routinely limiting dilution of thispotent anesthetic gas to oxygen only. The followingreasons have been advanced: (1) less of the more toxiccyclopropane will be required when supplemented byone of the weak anesthetic gases (the more potent thedrug the higher the ratio of toxicity); (2) a high pro-portion of oxygen in the gas mixture increases thehazard of explosion; 7 (3) all of the inhalation anes-thetics and oxygen are absorbed very rapidly from thelungs, but the inert gases, nitrogen and helium, areslowly absorbed. 8 The addition of nitrogen or heliumto the anesthetic mixture therefore safeguards againstthe development of a localized atelectasis if bronchialpassages should become plugged temporarily withmucus; (4) excess oxygen in the blood may interferewith the mobility of carbon dioxide in the tissues ofthe body and with the acid-base balance; 9 (5) al-though a generous supply of oxygen increases thesafety of all anesthesias, the body can use only alimited quantity and cannot store oxygen; 10 and (6)the body is adjusted to the quantity of oxygen in theatmosphere at sea level, which is approximately 20per cent, and a marked increase above this over sev-eral hours of time may have toxic effects on the lungepithelium.ll
It is impracticable to administer cyclopropane-oxygen for surgical anesthesia except by the methodof closed rebreathing as the initial cost of this potent
7 Ralph M. Waters. Cyclopropane-a personal evaluation. Surgery,
18:28.8
Pol N. Coryllos and G. L. Birnbaum. Studies in pulmonary gasabsorption and bronchial obstuction. Part 8: A theory of gas absorp-tion and atelectasis. Am. J. M. Sc., 183:355.
9 Samson Wright, Applied Physiology, p. 405.10 Henry K. Beecher, The Physiology of Anesthesia, p. 124.Iloid., p. 126.
81GASEOUS ANESTHETICS

anesthetic gas is high. Cyclopropane anesthesia by thismethod, however, is not expensive, despite the highcost of the gas, for the exhaling valve can remainclosed throughout the operation and there is littlewaste of gas. This is in contrast to the technique re-quired for the weak anesthetics, nitrous oxide andethylene, when much gas is wasted in order to elimi-nate the diluting nitrogen from the body tissues. Inaddition to the saving of gas, the closed exhaling valveprovides for the rebreathing of exhaled carbon dioxideto increase respiratory excursion and so hasten theinduction of anesthesia, therefore the filter systemshould be cut out until the surgical stage of anesthesiais reached.
The following technique for the administration ofcyclopropane-oxygen anesthesia is similar to themethod originally described by Dr. Waters in 1934.12Over the years it has proved satisfactory for the aver-age patient. The breathing bag is inflated two thirdsfull with oxygen for adequate dilution of cyclopro-pane from the start. The inhaler is then gently ap-plied over the patient's nose and mouth and theobturator valve is opened. The control valves of thecyclopropane and oxygen are opened and set at a flowof 500 cc. of each gas; meanwhile the patient is in-structed to breathe regularly and reasonably deeply.There is slight odor to the gas in this great dilution,and it is nonirritating to the air passages. After a fewbreaths of the gas the patient's sensitivity as a wholewill be sufficiently dulled so that the inhaler strapcan be tightened and fastened without causing dis-comfort. When the breathing bag is full, the flow ofoxygen is reduced to the approximate quantity that
12 J. A. Stiles, W. B. Neff, E. A. Rovenstine, and R. M. Waters.Cyclopropane as an anesthetic agent: a preliminary clinical report.Anesth. & Analg., 18:56.
82 ANESTHESIA

is being consumed in the metabolic processes of theindividual patient, and this replacement of oxygencontinues throughout the operation. The quantity ofcyclopropane that will be needed in order to induceand maintain surgical anesthesia will also vary withindividual cases, and the 500 cc. flow of this gas iscontinued for one to three minutes accordingly. Thefilter is now turned into the circuit.
Cyclopropane anesthesia culminates rather slowly,and as soon as the patient is unconscious and quiet,the flow of the gas should be stopped temporarily forthe anesthesia will continue to deepen somewhat.This precaution is necessary in order to avoid thedanger of seriously depressing the occasional patientwho is hypersensitive to anesthetic drugs.
For the maintenance of an even plane of anesthesia,the addition of a small quantity of cyclopropane willbe required at intervals, though a leakproof systemmay seem to have been effected and the filter is func-tioning properly. This additional gas is needed tocompensate for dilution of the rebreathed vapor withnitrogen, which is being gradually freed from the bodytissues, and for the loss of cyclopropane by evapora-tion from cut surfaces and, possibly, by permeationof this gas through the rubber walls of the breathingbag.
In contrast to the strict anesthetic limitations ofnitrous oxide and ethylene, the plane of surgical anes-thesia can be adjusted with this highly potent gas tosuit the need of the moment without risk of the com-plication of anoxia. Usually, muscular relaxationunder cyclopropane anesthesia is good but not in-variably as good as is obtainable under ether anes-thesia. Ether vapor combines well with cyclopropaneand may be added to the rebreathed anesthetic mix-ture whenever necessary.
83GASEOUS ANESTHETICS

Helium can be used as a supplement to oxygen forthe dilution of cyclopropane when a very high pro-portion of oxygen is not especially indicated by thepatient's general condition. Combination of thesegases offers two distinct advantages: (1) reduction ofthe proportion of oxygen reduces the hazard of ex-plosion; and (2) the lighter anesthetic atmosphereobtained by the replacement of a quantity of oxygen,which has an atomic weight of 16, with helium, havingan atomic weight of 4, lessens resistance to breathing.This lighter atmosphere is especially helpful some-times in overcoming stridor that may result fromsudden painful manipulation while the anesthesia isinsufficiently deep.
The technique for the cyclopropane-helium-oxygenprocedure is similar to the one that has been givenfor cyclopropane-oxygen except that the initial two-thirds filling of the breathing bag is done with heliumand 25 per cent oxygen. Helium is added during themaintenance stage only if the bag has to be refilled.The proportion of oxygen in the mixture of gasesshould never be less than 25 per cent.
Nitrous oxide or ethylene, with 25 per cent oxygen,makes a good basal anesthesia for cyclopropane whena superabundance of oxygen is unnecessary. In com-parison to cyclopropane-oxygen in single combination,the advantages afforded by the basal group are asfollows: (1) there is less depression of respiration and,consequently, less abnormal stimulation of the circu-lation by retained carbon dioxide in the system; (2)less of the more toxic gas will be required when it issupplemented with another anesthetic; and (3) de-pressive overdosage may be detected earlier by eye andcolor signs than when the percentage of oxygen in therebreathed atmosphere is very high.
The technique to be followed is the same as for
84 ANESTHESIA

cyclopropane-oxygen with the exception that one ofthe weak anesthetic gases and 25 per cent of oxygenare used for the initial filling of the breathing bag.The basal anesthesia can be made more effective bypartially rinsing out the air from the lungs and airpassages with it before the cyclopropane is added tothe gas mixture. This is done by continuing the flowof nitrous oxide (or ethylene) and oxygen for two orthree minutes with the exhaling valve open when theanesthesia is first started. With cyclopropane-oxygenanesthesia some anesthetists prefer to keep up a con-tinuous flow of cyclopropane during the maintenancestage at a rate of about 20 to 30 cc. per minute forthe average case. It has been reported that the con-tinuous-flow method is usually essential for smoothmaintenance anesthesia when the patient is an infantor small child. The high metabolic rate, rapid pulse,and respiration, and the small body area that canserve as storage reservoir for the anesthetic are handi-caps these patients present towards a smooth anes-thesia.
Whenever the anesthesia has been maintained en-tirely by any one or combination of the gaseous anes-thetics, it should not be discontinued until the surgicalprocedure has been fully completed, including dress-ing of the wound. The patient recovers consciousnessquickly after the mask has been removed, and he maysuffer much discomfort and pain in being lifted fromthe operating table to the stretcher or bed. Unfortu-nately the tired "surgical team," adjusted to workingover an unconscious patient, seldom realize that con-sciousness has returned so quickly and are not suffi-ciently gentle in this last necessary handling of theirpatient.
85GASEOUS ANESTHETICS

Chapter 8
AVERTIN
TRIBROMETHYLALCOHOL, a white crystallinesalt synthetized by the German chemists Willstaetterand Duisberg and first used as a general anesthetic inGermany in 1926, was introduced into the UnitedStates two years later in liquid form, combined withamylene hydrate, under the trade name Avertin.
Each cc. of the fluid contains one gram of the salt.The dose, carefully adjusted to the individual patient,is administered slowly by rectal injection as a 21/-per-cent solution in distilled water. The drug israpidly separated from the solution into the bloodstream through the intestinal mucosa; consequently,withdrawal of a portion of the fluid subsequent tothe injection may be ineffective in reducing the dose,should such prove desirable.
Avertin is depressant to the central nervous systemand unconsciousness is induced by it very comfortablyand quickly; but the superficial nerve endings arelittle affected and large doses of the drug are neces-sary to prevent muscle reaction to pain. It is generallyaccepted that Avertin should be used only as a basalanesthetic to be supplemented, as necessary, by a morecontrollable method for complete surgical anesthesia.
!86

This is because of the well-recognized variation intolerance for anesthetic drugs and the fact that anyfairly long-acting drug given en masse in sufficientamount to obtain the desired effect cannot be keptunder control with the safety possible by the methodof inhalation or of intravenous injection.
Conservative small dosage of Avertin is effective incompletely abating excitement and fear. In additionto this psychic advantage, basal anesthesia increasesthe efficiency of the so-called "weak" gaseous anes-thetics, nitrous oxide and ethylene. It also greatlydecreases the quantity of ether, or other anesthetic ofhigh potency, that would otherwise be required toproduce satisfactory surgical anesthesia.
Unlike the common inhalation anesthetics, Avertinundergoes a definite chemical change in the body. It isdetoxicated in the liver by combination with glycu-ronic acid, in which form it is excreted by the kidneys.Elimination is affected by the rate of the body metab-olism. Therefore, conditions of abnormally lowmetabolic rate, or impeded liver function, are con-traindications to the use of Avertin. Conversely, toler-ance for the drug is increased in the presence of ahigh rate of metabolism.
Usually, with this drug, there is some initial fall ofblood pressure, the degree depending upon the speedof absorption and the size of the dose. Under rela-tively normal conditions, even when the fall of bloodpressure is marked, there are no accompanying signsof shock, and the pressure readily responds favorablyto some simple form of physical stimulation such aspreparation of the surgical field, or the start of thesupplementary anesthetic-with plenty of oxygen andthe careful maintenance of a clear airway. Greaterconservatism in dosage is indicated for the patientwith marked hypertension, or the fall of blood pres-
87AVERTIN

88 ANESTHESIA
sure will be more profound. The drug is definitelycontraindicated for the patient who is in a state ofshock.
A convenient scale of dosage is provided with eachpackage of fluid Avertin, computed on the basis of amaximum dose of 100 mgm. of the drug per kilogramof body weight. The scale ranges downward, in varia-tions of 10, to the dose of 60 mgm. per kilogram, withthe quantity of water calculated for each dose re-quired, to make the usual 21-per-cent solution. It isso arranged that the dose may be readily adjustedaccording to the state of health, or debility, andspecial needs of the individual patient. Included inthe directions for preparation of the solution is thewarning that obesity lessens the tolerance of an in-dividual for this drug. A maximum limit is set to thequantity that should not be exceeded as the initialdose for any patient.
It is possible, of course, to train oneself to "size up"the variation from the normal in the patient's weight,as well as other problems of individual tolerance, andto adjust the dose in accordance with what he shouldweigh rather than to what he actually does weigh,but judgment, with the less experienced, is more likelyto err than accurately calculated measurement. Ascale of dosage that has proved of much value in thisrespect over the years, was worked out on the basis ofsurface area.1 (Figure 5.) Comparing it with the stand-ard scale based on weight, the dose of Avertin is foundto be practically identical on both scales for patientsof normal weight for their height, but for the abnor-mal, the difference in dosage is significant. For in-stance, for a patient of 5 ft., 4 in., weighing 200 lbs.,the maximum dose computed by the surface area scale
1Alice M. Hunt. A newer method for computing the individualdosage of Avertin. J. Am. A. Nurse Anesthetists, 8:18.

AVERTIN DOSAGE TABULATED ACCORDING TO SURFACE AREA
Dosage Table Dosage Table Dosage Iabile Dosage Tial Dosage TablePatient's No, i No.
2 No. 3 No. 4 No. 5
362.5 mg. per 326.25 mg. per 290 mg. per 2,3.75 mig. per 217.5 mg-. perSurface Area 0.1 sq. meter 0.1 sq. meter 0.1 sq. meter 0.1 q. meter sq. meter
Square Meers Avertin Water Av1in Water Avertin Water Averrin Waer Averrin Water
3.00 10.9 436 9.8 392 8.7 348 7.6 501 6.5 260
2.90 10.5 420 9.5 380 8.4 336 7.4 296 6.3 252
2.80 10.2 408 9.1 364 8.1 324 7.1 284 6.1 244
2.70 9.8 392 8.8 352 7.8 312 6.9 276 5.9 236
2.60 9.4 376 8.5 340 7.5 300 6.6 264 5.7 228
2.50 9.1 364 8.2 328 7.3 292 6.3 252 5.4 216
2.40 8.7 348 7.8 312 7.0 280 6.1 244 5.2 208
2.35 8.5 340 7.7 308 6.8 276 6.0 2410 5.1 204
2.30 8.3 332 7.5 300 6.7 268 5.8 232 5.0 200
2.25 8.2 328 7.3 292 6.5 260 5.7 228 4.9 196
2.20 8.0 320 7.2 284 6.4 256 5.6 224 4.8 192
2.15 7.8 312 7.0 280 6.2 248 5.5 220 4.7 188
2.10 7.6 304 6.9 276 6.1 244 5.3 212 4.6 184
2.05 7.4 296 6.7 268 5.9 236 5.2 208 4.5 180
2.00 7.3 292 6.5 260 5.8 232 5.1 204 4.3 172
1.95 7.1 284 6.4 256 5.7 228 4.9 196 4.2 168
1.90 6.9 276 6.2 248 5.5 220 4.8 192 4.1 164
1.85 6.7 268 6.1 244 5.4 216 4.7 188 4.0 160
1.80 6.5 260 5.9 236 5.2 208 4.6 184 3.9 156
1.75 6.3 252 5.7 228 5.1 204 4.4 176 3.8 152
1.70 6.2 248 5.5 220 4.9 196 4.3 172 3.7 143
1.65 6.0 240 5.4 216 4.8 192 4.2 168 3.6 141
1.60 5.8 232 5.2 208 4.6 184 4.1 164 3.5 140
1.55 5.6 224 5.1 204 4.5 180 3.9 156 3.4 136
1.50 5.4 ,216 4.9 196 4.4 176 3.8 152 3.3 132
1.45 5.3 212 4.7 188 4.2 168 .3.7 148 3.2 128
1.40 5.1 204 4.6 184 4.1 164 3.6 144 3.1 124
1.35 4.9 196 4.4 176 3.9 156 3.4 136 2.9 116
1.30 4.7 188 4.2 168 3.8 152 3.3 132 2.8 112
1.25 4.5 180 4.1 164 3.6 144 3.2 128 2.7 108
1.20 4.3 172 3.9 156 3.5 140 3.0 120 2.6 104
1.15 4.2 168 3.8 152 3.3 1 2 2.9 116 2.5 100
1.10 4.0 160 3.6 144 3.2 128 2.8 112 2.4 96
1.05 3.8 152 3.4 136 3.0 120 2.7 108 2.3 92
1.00 3.6 144 3.3 132 2.9 116 2.5 100 2.2 88
0.95 3.4 136 3.1 124 2.8 112 2.4 96 2.1 84
0.90 3.3 132 2.9 116 2.6 104 2.3 92 2.0 80
0.85 3.1 124 2.8 112 2.5 100 2.2 88 1.8 72
0.80 2.9 116 2.6 104 2.3 92 2.0 80 1.7 68
0.75 2.7 108 2.4 96 2.2 88 1.9 76 1.6 64
0.70 2.5 100 2.3 92 2.0 80 1.8 72 1.5 60
0.65 2.4 96 2.1 84 1.9 76 1.6 64 1.4 56
0.60 2.2 88 2.0 80 1.7 68 1.5 60 1.3 52
0.55 2.0 80 1.8 72 1.6 64 1.4 56 1.2 48
0.50 1.8 72 1.6 64 1.45 72 1.3 52 1.1 44
Figure 5. Avertin dosage scale, tabulated according tosurface area.


is 7.1 cc., and by the kilogram scale, 9.1 cc., a differenceof 2 cc. Very little additional effort is involved in the,use of the surface-area method. The height, as well asthe weight, must be ascertained and the surface areais readily calculated by means of the DuBois chartused for computing basal metabolism. (Figure 6.) Itmust be remembered that in the case of small children,and of adults who are pathologically underweight, thedose based on surface area may exceed the dose basedon weight. A good rule to follow is to compare thedose on both scales and give the lesser quantity ofrecorded drug.
Detailed care is necessary in preparation of thesolution for injection. The salt is precipitated whenAvertin is mixed with cold water, and decomposedto a tissue irritant if the water is too warm. Fortydegrees Centigrade (104 degree Fahrenheit) is set asthe optimum temperature to be used. This must bedetermined accurately by a thermometer. A phial of1-1000 Congo-red solution is provided with each bottleof Avertin fluid so that the prepared solution can betested for assurance of its fit condition. A few dropsof the Congo red added to a normal solution gives ita definitely pink tinge. A blue or purple color denotesthe presence of hydrobromic acid, which, with theaccompanying dibromacidaldehyde, may cause atroublesome colitis upon injection into the bowel.Such a solution should, therefore, be discarded.
The rate of absorption is determined by the speedof injection of the fluid and the extent of the areaand the condition of the mucosa contacted by thesolution. So special care must be given to adequatecleansing of the colon by bland enemata and to theinjection of the anesthetic solution. Satisfactory prepa-ration of the bowel can usually be obtained by theuse of a simple laxative given in the morning of the
89AVERTIN

day before operation, followed in the evening by athorough enema of normal saline. Soap suds mayleave an obstructing film on the bowel mucosa. Un-less several hours are allowed to elapse between thegiving of a cleansing enema and any rectal medica-tion, the bowel is likely to be in too irritable a statefor the medication to be well retained. Enema shouldnot be deferred, therefore, until the morning of opera-tion.
If a small dose of morphine is deemed advisable, itshould be given three quarters of an hour before theAvertin in order that its effect may be noted and thedose of Avertin regulated accordingly. The Avertinsolution should be freshly prepared. It is not necessaryto keep it warm. It should be introduced slowlythrough a rubber catheter, approximately size 24 F,or a small rectal tube inserted carefully about threeinches into the rectum. The glass part of a Dakin'ssyringe or small funnel is attached to the tube. Thisshould be held a few inches above the buttocks withthe patient lying on either side or on his back if it isimpractical for him to be turned. Care should betaken to avoid the introduction of air. Five to tenminutes should be consumed in the process of in-jection of the anesthetic solution. In the case of in-fants, small children, and other irresponsible patients,a pad should be held over the anus for a few minutesafter the catheter is withdrawn or the buttocksstrapped together with adhesive plaster to preventexpulsion of the fluid. Usually the patient will becomedrowsy, or fall asleep, within five to six minutes afterthe injection is completed. Under ideal conditions ofpreparation and administration, it has been provedthat concentration of the drug in the solution hasdiminished one third within ten minutes after thecompletion of the injection, and more than one half
90 ANESTHESIA

DUBOIS BODY SURFACE CHART(As prepared by Boothby and Sandiford of the Mayo Clinic)
- 20---
10 0o o--
-17 -O 1- -
_-0
-- .7
i. *-:
- /jo /o - .o - 225
- 7 -too-I- SO 1 _ /o-
j- i , .-s-- : ,<
= c--i / 5
1355
r5
- -0o --
-- /- 1f - -$0
l6
S 00
4' .73-5
0_- "70 s
-10 - tS
i AS
..
9u .70
Figure 6. DuBois chart for computing surface area.


from the original strength within twenty to thirtyminutes. 2 In the occasional case where the patient,seemingly, remains conscious for ten minutes or more,a state of amnesia has usually developed and the pa-tient will have little remembrance of occurrences afterthe catheter was withdrawn.
The great advantage of Avertin is this period ofamnesia, both pre- and postoperatively, so comfortablybrought about. If the drug is given carefully and un-obtrusively to the patient in bed, before removal fromhis room or ward, he is spared the natural emotionalupset and fear of the journey to the operating room.When it is desirable, as in the case of small childrenand patients in such supersensitive states as that re-sulting from acute hyperthyroidism, the imminenceof the surgical operation need not be disclosed to thepatient until it is an accomplished fact. This form ofbasal anesthesia, in the small dosage that usually issufficient, is invaluable as a means of preventingpsychic shock for patients, especially children, need-ing repeated surgical operations or painful treatmentsat frequent intervals. It has also been proved a safeand effective treatment for control of the convulsionsof tetanus and of other causes. In such cases it hassometimes been given daily over a period of a week ormore with no deleterious results.3
Invariable success in the use of Avertin depends,as indeed with all anesthetics, upon the experienceand good judgment of the anesthetist, and carefulattention to detail, plus conservatism in dosage andthe realization that usually the desired effect of basalanesthesia can be brought about equally well withsmall, as with large, doses.
V Walter Sebening. Recent researches and clinical advances inAvertin narcosis. Anesth. & Analg., 11:145.
SRobert W. Huntington, Jr. The treatment of tetanus. Yale J.Biol. & Med., 8:207.
91AVERTIN

92 ANESTHESIA
Where it is desirable to prolong the period of sleep,as during a tedious surgical case restricted to supple-mentary local anesthesia, the catheter can be obtundedand left in situ to allow for the repetition of injectionof Avertin solution. The quantity of Avertin to beused under such conditions must be determined by thereaction of the patient to the initial dose, consideringalso his present general condition.

Chapter 9INTRAVENOUS ANESTHESIA
To produce general anesthesia, it is necessarythat the anesthetic drug be introduced or absorbedinto the blood stream. To a person familiar with themodern common practice of intravenous therapy, themethod of direct injection of this drug into a veinseems simple and logical. But safe intravenous therapyis of recent date-twenty-five years or so-and the dis-covery of anesthetic drugs suitable for such adminis-tration is of still more recent origin. The possibilityof producing sleep and anesthesia by this method wasrecognized by investigators much earlier; in 1872 theFrench scientist Ore reported the intravenous injec-tion of chloral hydrate for surgical anesthesia; ' butthe subsequent high mortality rate ascribed to it dis-couraged continued use of the practice. Other drugswere tried at intervals and later discarded as unsuit-able.
Early in the present century intravenous ether anes-thesia had a brief vogue of limited scope. The drugwas prepared as a 5-per-cent to 7-per-cent solution insterile normal saline, or Ringer's, solution. After the
James Tayloe Gwathmey, Anesthesia, p. 628.
93

94 ANESTHESIA
needle had been inserted into the vein, the solutionwas started at a moderately fast flow for the inductionof anesthesia and then gradually slowed to a rate offifty to sixty drops per minute for maintenance of thesurgical stage. Usually, the induction period was re-markably smooth and rapid in comparison with theinhalation ether method; the planes of anesthesiacould be kept readily under control by regulation ofthe rate of drop, and when the flow was stopped, thepatient quickly recovered consciousness. Though therewere also other advantages to this method, little post-operative nausea or vomiting or irritation of therespiratory tract, it involved the giving of large quan-tities of saline solution, an average of 1000 cc. perhour, with the grave risk of a resulting edema of thelungs and other body tissues. Consequently, themethod did not gain popularity.
As the synthesis of the barbituric acid derivativesevolved, several were given trial as intravenous anes-thetics; 2 but though a few of the early discoveriesproved very satisfactory experimentally, the period ofunconsciousness resulting from their use intravenouslywas too prolonged for safety, as t routine procedure,for the human subject. The introduction of Evipansodium (Evipal soluble) a very short-acting barbit-urate, by German chemists in 1932, established in-travenous anesthesia on the firm basis recognizedtoday.
Two years later, the use of a similar short-actingdrug for the purpose, pentothal sodium, a derivativeof thiobarbituric acid, was described by Dr. Lundy ofthe Mayo Clinic. This drug has stood the test of timevery well and has steadily displaced Evipal, at leastin America, on the basis of affording still higherpotency and lesser toxicity as an intravenous anes-
2R. Charles Adams, Intravenous Anesthesia, p. 185.

INTRAVENOUS ANESTHETICS
thetic. The thiobarbiturates contain a sulfur atomwhich is thought to hasten the destruction of the drugin the body. The sulfur gives a pale yellow color tothe sodium salt. The effects of these two barbituratesare otherwise very similar, and the technique of theirpreparation and administration is practically thesame. The drugs are commonly marketed in sealedglass ampoules containing 1/2 gram and 1 gram of thepowder. The powdered drug dissolves readily in waterand is prepared as a 21/2-per-cent to 5-per-cent solutionwith sterile distilled water. Freshly prepared solutionsare preferable, but they are sufficiently stable to bekept for several days, provided the solution is keptsterile and protected from light. The solution shouldnot be used if it has become cloudy or otherwisechanged from it original appearance.
Any normal vein of reasonably good size, which canbe conveniently exposed, may be used for the veni-puncture; those of the cubital fossa, dorsal area fhand and wrist, or the veins of the ankle are mostcommonly chosen. Of course, careful aseptic prepara-tion of the area and application of a tourniquet proxi-mal to the site are essential, as with any venipuncture.Choice in the size of the needle is influenced by thesize of the vein and subsequent method of procedurerequired.
Pentothal sodium may be used for the rapid andcomfortable blotting out of consciousness only as apreliminary to inhalation anesthesia. In this case, theneedle is quickly discarded so one of small caliberwill be adequate. The needle may be left securely in-serted in the vein when the anesthesia is to be main-tained or supplemented by interval injection of thesolution, when a larger needle is more likely to remainpatent over a long period of time. Should a supportinginfusion be desirable during the surgical operation,
95

the pentothal setup can be arranged so that the solu-tion can be given intermittently through the needleby means of a multiple-way stopcock; the continuousdrip of the infusion will prevent blockage of theneedle by blood clot.
Pentothal sodium may also be given by continuousdrip infusion, prepared in 0.5-per-cent to 1-per-centconcentration with normal saline. The depth of anes-thesia is regulated by the rate of the drop.
The nonvolatile anesthetics, in contrast to theliquid and gaseous agents, undergo more or lesschemical change in the body processes. It is generallyaccepted that they are detoxified, if not completelybroken down, in the liver and are excreted by thekidneys and that the outstanding contraindications tothe use of these drugs are signs of inefficient function-ing of these organs. Evidence that the liver plays littlepart in the detoxification of pentothal sodium hasrecently been reported following animal experiments. 3
Whether or not this holds true in regard to the humanbody also remains to be proved. It is known definitely,by the brevity of its effects, that pentothal sodium israpidly broken down in -the tissues.
This desirable brevity of effect applies only whenpentothal is used in moderate dosage, however, for thedrug seems to have cumulative properties. These areevidenced in the average case by progressive depres-sion of the respiration and circulation and delay inreturn of consciousness, which commonly follow largedoses of the drug regardless of the length of time con-sumed in the operative procedure. For these reasonsit is generally considered unwise to depend solelyupon pentothal sodium for prolonged surgical anes-thesia; but as a supplement to other drugs and meth-
SCharles H. Scheifley. Pentothal sodium: its use in the presence ofhepatic disease. Anesthesiology, 7:263.
96 ANESTHESIA

INTRAVENOUS ANESTHETICS
ods used for this purpose it is of great value. Forinstance, the hazard of explosion can be entirelyeliminated, while excellent anesthesia is maintained,by the skilled combination of pentothal and nitrousoxide-oxygen.
For brief surgical procedures, intravenous pentothalsodium anesthesia is very satisfactory for consciousnessis lost within one minute, rarely is there a stage ofexcitement, and muscular relaxation is sufficientlygood for minor surgery or reduction of fracture. Therecovery period is brief and rarely accompanied bynausea or vomiting.
Depression of respiration is the chief complicatingfactor of pentothal sodium anesthesia and this shouldbe counteracted by a continuous flow of oxygen. In-trapharyngeal insufflation, by means of a nasal cath-eter, is a convenient way in which to administer theoxygen if a supplementary gas-oxygen machine is notbeing used.
The technique for intravenous anesthesia calls forcareful attention to detail in preparation of the solu-tion and skill at venipuncture for infusion. The alka-line solution is irritant to the soft tissues, and it isessential that the needle be properly placed in thevein before any of the fluid is injected. In the case ofaccidental injection of a portion of the solution intothe tissues, gentle massage of the area and applicationof warm compresses aid in the absorption of the fluidand so decrease the discomfort. Should the discomfortbe severe, local injection in the area of a 1-per-centNovocain solution will give quick relief.
Warning should be given of the danger and possi-bility of accidental arterial puncture. Injection of thesolution into an artery causes a sharp burning sensa-tion distal to the point of entry, and complaint of thissensation by the patient calls for immediate with-
97

98 ANESTHESIA
drawal of the needle. Serious local interference of thecirculation, even to the point of causing gangrene, hasresulted from such accidental injection.4
The simplicity and ease of induction of intravenouspentothal sodium anesthesia should not mislead oneinto the belief that it can be safely undertaken by theinexperienced anesthetist, for the drug is very power-ful, and there is wide variation in individual tolerancefor it.
*R. R. Macintosh and P. S. A. Heyworth. Pentothal-arterial in-jection of, a warning. Lancet, 1943, pt. 2, p. 571.

Chapter 10
LOCAL ANESTHESIA
COCAINE and several synthetic salts that, forthe most part, are derivatives of benzoic acid are thedrugs most commonly used for local anesthesia. Theleast toxic and most popular of the synthetic drugs isNovocain (procaine hydrochloride). In order to in-duce anesthesia in a given area, a weak solution of ananesthetic drug is applied topically to mucous mem-brane, or injected hypodermically. The intact skincannot be anesthetized by surface application of anes-thetics.1
The high toxicity of the drug prohibits the hypo-dermic injection of cocaine, but mucous membrane isreadily penetrated by the solution. The field of use-fulness for cocaine as a local anesthetic is, therefore,limited to superficial areas of the eye, ear-nose-throat,and the urethra. Even this limited use of cocaine isbeing challenged by some of the synthetic drugs, no-tably Pontocaine and Butyn, which present advantagesof lessened toxicity and freedom from the danger ofhabituation inherent in the use of cocaine.
Many surgical procedures can be performed rela-tively painlessly under local anesthesia. Excellent re-
1 Henry K. Beecher, The Physiology of Anesthesia, p. 50.
99

suits depend largely upon allowing sufficient time foradequate infiltration of the drug before surgery isattempted and upon subsequent gentle handling ofthe tissues.
For anesthesia of mucous surfaces, the surgical areamay be sprayed with the anesthetic solution, swabbedwith cotton soaked in the solution, or narrow passagessuch as the nostrils may be packed for a short periodwith gauze wicking that has been saturated with thesolution. For anesthesia of the cornea the solution isapplied in drops to the eyeball. The anesthetic con-centration of the solution should be as low as is com-patible with satisfactory anesthetic results. This mayrange between 1 per cent and 10 per cent according tothe drug used and other conditions that influence anes-thetic practices in general. (Novocain is not satisfactoryas an anesthetic for topical application.)
Novocain for subcutaneous injection is most com-monly used in a 0.5-per-cent solution. The drug causesvasodilatation in the area of injection and a smallquantity of adrenalin, 1-25,000 to 1-100,000, is usuallycombined with the anesthetic solution in order tocounteract this effect and delay absorption of the an-esthetic into the blood stream. Slowing the absorptionof the drug prolongs the localized anesthesia andreduces the risk of toxicity since local anesthetics arequickly destroyed in the liver. 2 Overdosage is broughtabout largely by too rapid injection of the solution.
Careful, skilled injection will cause little discomfortafter the first superficial wheal is made by the enteringfluid, for each successive stab of the needle is madewithin the anesthetized area as that area is extended.When the field of operation is relatively deep, for in-stance, through the abdominal wall, a small-caliber
2John Adriani, The Pharmacology of Anesthetic Drugs, p. 48.
100 ANESTHESIA

LOCAL ANESTHESIA 101
short needle is used for superficial injection, and thisis replaced by a longer needle as the infiltrationspreads and deepens.
The necessary apparatus for the injection of localanesthetics consists of hypodermic needles and syr-inges and a vial or flask of the' anesthetic solution.Aseptic surgical technique is essential, of course, andthe simplicity of the whole procedure makes it pos-sible, and usually more convenient, for the anesthesiato be conducted by a member of the surgical team.The anesthesia can then be readily extended or pro-longed, whenever indicated, by repeated injection ofthe solution; this will be found necessary during ex-tensive operations as the average duration of Novo-cain anesthesia is limited to about one hour.
The danger of too rapid absorption of the drug ispresent when the injection of the drug is made intoinflamed tissues or highly vascular areas. Apart fromthis danger, and acute discomfort caused by injectionof the solution into acutely infected tissues, local an-esthesia under such conditions is rarely efficient. Thisis explained on the theory that the abnormal acidityof the tissues, resulting from the bacterial activity,prevents hydrolization of the anesthetic drug.3
Precaution is necessary to avoid accidental intra-venous injection of the anesthetic solution. The lethaldose of Novocain by intravenous injection is reportedto be one tenth that of the subcutaneous lethal dose.Idiosyncrasy to Novocain is occasionally met and, ofcourse, is a contraindication to further use of the drug.
Local anesthetics are stimulating to the centralnervous system and symptoms of overdosage are signsof excitement and restlessness, which in severe con-ditions may progress into convulsions and coma.
3 Ibid.

Intravenous injection of one of the short-acting bar-biturates is accepted as the best antidote when symp-toms portray severe overdosage. It is also accepted thatthe threshold of tolerance for local anesthetics may beraised considerably by sedative premedication of thepatient with a barbiturate, and consequently suchmedication is especially indicated with local anes-thesia.
Although the services of an anesthetist may not benecessary, constant watch must be kept of the patient'sgeneral condition and special care taken to insure hiscomfort. Unless the patient has been heavily premed-icated and is somnolent, lying awke completely stillfor a prolonged time can become very tiring, especiallyunder the condition of nervous tension evoked byanticipation of a surgical operation. An understand-ing nurse can contribute much to the success of localanesthesia by applying such little trifles of nursingcare as ice compresses to the forehead, mopping per-spiration from the face, giving the patient chips of iceto suck occasionally, and in various other ways dis-tracting his attention from the irksomeness of thesituation.
Preparation for operation under local anesthesiashould include adequate padding of the operatingtable, and after the patient is placed in the positionrequired by the surgeon, careful arrangement of padsand pillows for the avoidance of strain to muscles.The patient's hands should be comfortably placedand necessary restraining straps made inconspicuousand not fastened too tightly. Coverings for the patientshould be limited as much as possible to the minimumfor comfortable warmth, since the sterile coveringswill be superimposed. The patient's eyes should beshielded from glaring light.
Muscular reflex to pain stimuli in the surgical field
102 ANESTHESIA

during manipulation of highly sensitive tissues, undergeneral anesthesia, can be much diminished by resortto localized anesthesia. This supplementary local an-esthesia will be found to increase the effectiveness ofthe so-called weak general anesthetics and to decreasethe necessity for the maintenance of a profound depthof anesthesia when a general anesthetic drug of highpotency is being used. This combined anesthesia is ofgreat value, oftentimes, for the closure of the peri-toneum in the robust type of individual who is show-ing high resistance to anesthetic drugs.
Local anesthesia for the incision of a small,superficial abscess can be effected by the use of a finespray of ethyl chloride. The ampoule containing thedrug is held about ten inches above the area to beanesthetized and the ethyl chloride is released for thespray to strike the area. The rapid evaporation of thedrug in this way causes definite freezing with blanch-ing and hardening of the tissues. The anesthesia is ofbrief duration and the recovery period, as in any formof frostbite, is somewhat painful.
103LOCAL ANESTHESIA

Chapter 11
REGIONAL ANESTHESIA
THE term regional, or nerve-block, anes-thesia implies depression of the whole sensory nervesystem of a limited area of the body by the hypo-dermic injection of a local anesthetic solution at thefocal points of nerve supply of this area. A higherconcentration of the drug, Novocain 1 per cent to 2per cent, but a lesser quantity of the fluid is needed,usually, than for the infiltration method of local an-esthesia.
Regional anesthesia is applicable, for minor ormajor procedures, to practically all parts of the bodyand may involve very simple to very complicatedtechnique, according to the site, size, and nerve supplyof the area to be anesthetized. A single injection inthe vicinity of the branch of a nerve may suffice, orprecise identification of several nerves together withmultiple injection may be necessary. The method canbe used for surgical anesthesia and for therapeuticand diagnostic purposes.1 Because the injection is notmade directly into the surgical field, as is the case withinfiltration anesthesia, acute localized infection is not
1 C. Langdon Hewer, Recent Advances in Anesthesia and Analgesia,p. 164.
104

necessarily a contraindication to its use. Neither is thesurgical field distorted by an edema of the tissuescaused by infiltration of the solution, a condition thatmay seriously handicap extensive tendon repair orsimilar exploratory procedures.
Regional anesthesia may be sufficiently satisfactoryfor major surgery involving a wide area, and whenit is used in combination with a general anesthetic,the need for a deep plane of anesthesia is greatly min-imized.
The therapeutic use of regional-block anesthesiacan be of great benefit in the alleviation of the in-tractable pain of many diseases, such as inoperablelesions of cancer and tertiary syphilis. It is sometimeshelpful for the relief of herpes zoster (shingles) andin certain severe forms of bursitis, arthritis, and cir-culatory disorders. The treatment may have to berepeated a number of times, though under some cir-cumstances a single treatment gives lasting relief. Noentirely satisfactory explanation of the latter phenom-enon has, so far, been found. Anesthetic solutionscontaining oil, which greatly delays local absorption,are sometimes employed in order to prolong the anal-gesic effect.
Intraneural injection of 95 per cent alcohol is ofteneffective in controlling severe neuralgic pain for longperiods. Alcohol is sometimes injected into the stumpof the great sciatic nerve, during amputation of thethigh, to prevent the uncanny "pain in the foot" ofthe severed leg, a complaint that frequently followssuch surgical operations.
There is also increasing appreciation of the valueof regional anesthesia for diagnostic purposes in manybranches of medicine and surgery. Novocain block ofsympathetic-nerve ganglia may greatly facilitate diag-nosis of essential hypertension and of peripheral ar-
105REGIONAL ANESTHESIA

terial disease, and it may serve as a valuable guide inthe treatment and prognosis of these cases. 2
In order to make the induction of regional anes-thesia as painless as possible, the site of injectionshould be carefully anesthetized through an initialintradermal wheal made with a very fine hypodermicneedle, which may be replaced by longer and largerneedles as the need arises. Aspiration for assurancethat a blood vessel has not been inadvertently enteredis always essential before deep injection is niade, andespecially so when the more highly concentrated solu-tions are being used. The additional danger of acci-dental puncture of the arachnoid or pleural membraneis present when the injections are to be made in thearea of the neck, chest, and thorax, and this must, ofcourse, be guarded against.
Adrenalin in the solution is contraindicated forlocal or block anesthesia of the fingers and toes be-cause of the danger that the vasoconstrictor effect ofthe drug may be too prolonged. Gangrene of the tis-sues of a digit has occasionally resulted from suchinterference with circulation.
As a whole, regional-block anesthesia demands ofthe anesthetist much patience, practice, and skill andan intimate knowledge of anatomy. The duration ofanesthesia for surgery is limited and, on account ofvarying conditions, is usually unpredictable, and somesupplementary anesthesia should be available.
Similar consideration for the patient's general com-fort should, of course, be given, as has been outlinedunder the previous heading, local anesthetics. In thepostoperative care of the patient, warning should begiven of the danger of burning an anesthetized areaby treatments with heat in any form, applied at toohigh a temperature.
2 Alton Ochsner. Anesthesia of the sympathetic system: Editorial.Anesthesiology, 4:301.
106 ANESTHESIA

Chapter 12
SPINAL ANESTHESIA
SUBARACHNOID spinal anesthesia has passedthrough several phases of popularity since the incep-tion of the method early in the twentieth century.
A small quantity of relatively innocuous local an-esthetic, when injected into the spinal subarachnoidspace, produces a profound degree of anesthesia in awide area of the body without interference with con-sciousness. Compared to inhalation anesthesia, there-fore, spinal anesthesia would seem to be the wiserchoice for the poor-risk patient, whenever the methodis applicable in relation to the site of the proposedsurgical operation. Taking this supposition for grantedand failure to appreciate the potential dangers andlimitations of spinal anesthesia, together with the falsesense of security imparted by the simplicity and easeof the induction period, led to the indiscriminate useof spinal anesthesia. The inevitable accidents result-ing from ill-considered use of the method discreditedspinal anesthesia repeatedly, but, when used withdiscretion, the method has been of great value. Thechief advantage of spinal anesthesia is found in theexcellent muscular relaxation it affords the surgeon.
The special dangers of spinal anesthesia are those107

of serious depression of the respiration and circula-tion, conditions especially incompatible with poor-risk patients. How the depression is effected is stilla matter of controversy, but it is evident that thedegree of depression is influenced by the quantityand concentration of the drug, the rate of injectionand the level of anesthesia attained-the height towhich the drug penetrates into the spinal canal. Thelevel of anesthesia is the dominant factor, and whenthis goes above the costal margin there may be gravedanger of failure of respiration, due to paralysis of theintercostal and phrenic nerves.
The anesthetic is brought into contact with thenerve endings in the spinal canal by diffusion ofthe solution in the spinal fluid. Fortunately, this dif-fusion is relatively slow and, if careful considerationis given to the technique of injection, the level of an-esthesia can be approximated and stabilized fairlywell.
The principal factors affecting diffusion of the solu-tion are the difference in specific gravity of thesolution and the spinal fluid and the volume of thesolution and the speed or force with which it is in-jected. Unless the anesthetic solution is isobaric, i.e.,of the same specific gravity as the spinal fluid, the po-sition of the patient is also of much importance, for aheavier or lighter solution will sink or rise in thespinal fluid in conformance to the laws of gravity.For instance, the level of anesthesia will be raised,when a hyperbaric solution has been given, if thepatient is placed in the Trendelenburg position beforethe drug has become stabilized in the spinal canal. Asimilar effect will result when a hypobaric solutionhas been given, if the patient is placed in a sittingposition before the drug is stabilized.
The specific gravity of spinal fluid is approximately
108 ANESTHESIA

SPINAL ANESTHESIA 109
1.005. The drugs most commonly used in America forspinal anesthesia are Pontocaine in 1-per-cent solution,which is approximately isobaric, and Novocain in 10-per-cent solution, or in crystal form, which is def-initely hyperbaric. Since Pontocaine anesthesia lastsabout twice as long as that of Novocain but is isobaric,a proportion of Novocain crystals, or of glucose solu-tion, is frequently mixed with Pontocaine duringpreparation of the solution in order to make it hyper-baric.
Some of the highly potent local anesthetics inaqueous solution are hypobaric, as is also the propri-etary agent, Spinocaine, which is composed largely ofNovocain made hypobaric by the addition of alcohol.Despite careful consideration in one's choice of drugs,however, there is no fixed law regulating diffusion ofa solution in the spinal fluid, and the rate may be af-fected considerably by changes in the patient's res-piration, spinal blood circulation, and movements ofhis body.1
The original method of inducing spinal anesthesiaby the injection of a calculated single dose is alwayscomplicated by uncertainties with regard to the re-action of the individual patient to the drug and theduration of a satisfactory condition of anesthesia onceit has been established. The latter aspect may give thesurgeon an unfortunate sense of being hurried. Ameans for circumventing these uncertainties was pre-sented in 1940 by Dr. William T. Lemmon,2 when hepublished his method of continuous, or fractional,spinal anesthesia. With this method, the needle re-mains in the position of a subarachnoid spinal tapthroughout the operation, and to it is attached a
1 Henry K. Beecher, The Physiology of Anesthesia, p. 64.2 William T. Lemmon. A method for continuous spinal anesthesia,
a preliminary report. Ann. Surg., 111:141.

110 ANESTHESIA
length of fine rubber tubing connected with a stop-cock and a 10-cc. hypodermic syringe. In this way itis possible to test the patient's tolerance for the drugwith an initial small dose and prolong the anesthesia,as necessary, by repeated small doses. The methodcalls for substituting a flexible needle (made of mal-leable material, in order to lessen the danger of itsbreaking) for the usual rigid spinal needle and theuse of specially constructed rubber tubing. A dividedmattress, or other precaution, should be used to pre-vent pressure on the needle. A recent refinement intechnique was described by Dr. E. B. Tuohy of theMayo Clinic in 1944. It involves the substitution of aspecially constructed woven catheter for the perma-nent needle. The catheter is introduced a short dis-tance into the spinal canal through a larger, rigidspinal needle, which is then withdrawn. The cathetercan be secured to the back with adhesive tape; it willnot readily slip out, and the precautions against pres-sure are unnecessary.
The catheter technique has opened up possibilitiesof still greater control of spinal anesthesia in the formof "segmental anesthesia." 3 The term is used to in-dicate limitation of the area of anesthesia to thesurgical field. This is done by advancing the catheter,within the spinal canal, to the position of the rootsof the nerves that control that field, so that theanesthetic solution can be sprayed directly onto thesenerves. By thus avoiding dilution of the anestheticsolution with the spinal fluid in the canal and apply-ing it only where it is needed, the claim is made thatexcellent results can be attained with very weak solu-tions of Pontocaine or Novocain, and that there is
SMeyer Saklad, Clement S. Dwyer, Sanford Kronenberg, EdmundNeves, and Morris Sorkin. Intra-spinal segmental anesthesia, a pre-liminary report. Anesthesiology, 8:270.

required but a fraction of the total dose of the drugnecessitated by other methods of spinal anesthesia.
Advantages of satisfactory segmental anesthesia, forprolonged major surgery, are obvious when it is real-ized that the degree of toxicity of a local anesthetic tothe tissues of the body is in direct proportion, largely,to the degree of concentration of the injected drug,and that trifling chemical disturbances in the spinalfluid are caused by the very weak anesthetic solution.
One of the theories advanced in explanation of themarked fall of blood pressure, which so commonly ac-companies spinal anesthesia, is interference to thevenous return circulation due to the motor paralysisof the lower extremities. This paralysis can be avoidedwith segmental spinal anesthesia, and the circulationin general may be benefited thereby.
Spinal needles are from two and a half to three anda half inches in length with a gauge range of from16 to 22 (the finer needles cause less trauma to tissuesbut the larger ones are necessary for the passage ofthe catheters). The bevel should be short, 45 degrees,in order to avoid the risk of leakage of spinal fluid, orof anesthetic solution, into the surrounding tissuesfrom the point of the needle. The discomforts thatfollow spinal anesthesia, chiefly headache, can becaused by loss of fluid from the spinal canal.
The various methods of inducing spinal anesthesiainvolve minor differences of technique that must befollowed but need not be described in detail. Sufficeit to say that spinal anesthesia is usually induced withthe patient lying on one side, knees flexed on theabdomen, and head and shoulders drawn forward, inorder to bow the back and separate the spinal proc-esses. Sterile precautions in the preparation of fieldand instruments are necessary, of course, as for anyform of spinal tap. If the site of puncture is first care-
11SPINAL ANESTHESIA

fully infiltrated with 0.5-per-cent Novocain solution,the procedure is practically painless. Frequentlyspinal fluid is used for dissolving the Novocain crystalsand to make up the required volume of anestheticsolution. When a satisfactory spinal tap is confirmed,in such instances, by a continuous drip of clear fluidfrom the needle, a 10-cc. hypodermic syringe is at-tached and the necessary quantity of fluid withdrawn.
Immediately following injection of the anestheticsolution, the patient is carefully turned on his backand the position of the table is adjusted according tothe specific gravity of the solution that has been given.Hyperbaric solutions are the more commonly used,and in these cases the level of anesthesia may be raisedby lowering the table about 8 degrees Trendelenburgfor a minute or two. The patient's neck and headmust, meanwhile, be well raised in order to avoid thedanger of diffusion of the anesthetic to the respiratorycenter in the fourth ventricle. The level of anesthesiais tested by pinching the skin lightly with tissue for-ceps. When the desired level is attained, the tableis raised to the horizontal position and should remainso until the anesthetic drug has become "fixed." Atleast fifteen minutes should be allowed for this beforethe Trendelenburg position is used again.
Adequate sedative premedication is indicated withspinal anesthesia, and commonly ephedrine is givenshortly before the spinal injection is made in order tocounteract the anticipated fall of blood pressure.
The condition of the patient, in general, must becarefully watched throughout the operation by an an-esthetist who is prepared to give supportive treatmentincluding oxygen or supplementary anesthesia if in-dicated. Oxygen is helpful in controlling nausea thatmay result from a marked fall of blood pressure or asa reflex to manipulation in the upper abdomen.
112 ANESTHESIA

Chapter 13
OBSTETRICAL ANESTHESIA
THE technique for the control of pain forthe obstetric patient differs somewhat from that re-quired for general surgery, and it is in this field ofpractice, especially, that the nurse may be called uponto assume the role of anesthetist. For these reasons itseems advisable that the subject should be treated in-dividually.
During the first stage of labor, which often contin-ues for several hours, the pain may best be relievedby the judicious use of hypnotic and analgesic drugs.Scopolamine and the barbiturates, though having littleanalgesic effects, offer the great boon of amnesia andthe intermittent pains are quickly forgotten. Not in-frequently, however, patients who have been givensuch drugs become disoriented and difficult to controlduring the bouts of pain, and this many present seri-ous difficulties as the pains increase in frequency. Theaddition of an opiate to the medication will lessenthe disturbance, but most authorities agree that thespontaneous respiration of the baby, at birth, may becritically delayed when the mother has had morphineunless about four hours have elapsed since the dosewas given.
113

Rectal injection of ether and oil, advocated by Dr.Gwathmey, provides good analgesia during this stage,lasting for several hours. The injection is made whilethe patient lies on her left side with the buttocksslightly raised. A number 24-F rubber catheter, towhich a small funnel is attached, is well lubricated,filled with oil, and inserted gently into the rectum forthree to four inches. The ether-oil mixture, 21/2 oz.ether, 11/2 oz. oil, is then allowed to flow in slowly bygravity, at least ten minutes being allowed for this.Care must be taken, meanwhile, to prevent the intro-duction of air through the catheter. During a pain thesolution may be forced back into the funnel tempo-rarily, and provision should be made for this by notkeeping the funnel too nearly filled. When the injec-tion is completed, the catheter is gently withdrawn,and a pad and pressure with the hand applied overthe anus for several minutes until all desire to expelthe enema has subsided. The injection may be re-peated at three- to four-hour intervals if the labor isprolonged. Should the pains become too frequent andsevere, inhalation of a supplementary anesthetic maybe indicated in order to afford rest to the mother andto prevent circulatory interference with the fetusfrom incomplete relaxation of the uterine walls be-tween contractions. Intermittent inhalation of an an-esthetic at this time will often slow down uterinecontractions.
The characteristic pain of the first stage of labor islocated principally in the lower part of the back,radiating around to the abdomen. The patient shouldbe discouraged from "bearing down" at this stage forthe cervix is not fully dilated, and the useless effortwould needlessly tire her. On the other hand, with theonset of the second stage of labor, when the cervix isfully dilated, the expulsive nature of the pains stimu-
114 ANESTHESIA

OBSTETRICAL ANESTHESIA 115late an urge on the patient's part to "bear down," andshe should be encouraged to do so as persistently aspossible for the full duratiofi of each pain. The anes-thetist can greatly help the patient to a satisfactorytermination of the labor by teaching her in this wayto get the full value of each pain. The inhaled anes-thetic, at this time, should be limited to the quantitynecessary to induce analgesia only, the patient re-maining sufficiently conscious to be able to obey thesimple, definite directions of the anesthetist.
Though a patient may at first be reluctant to inhalean anesthetic, once she has been persuaded to do soshe is usually so impressed with the relief it affords herthat she begs for its continuance. If the need arisesfor an episiotomy or for the application of "low for-ceps," the analgesia is allowed to develop into anes-thesia. Full surgical anesthesia is necessary for a "highforceps" delivery, for the performance of version, andfor extensive perineal repair. Inhaled ether is too slowin its effects to be of much value for obstetrical inter-mittent analgesia, but nitrous oxide-oxygen, 80/20per cent, is very satisfactory since this anesthetic givesboth quick relief and recovery, and a state of anes-thesia can be readily superimposed whenever indi-cated. By the addition of a little ether vapor, orcyclopropane, after consciousness is lost, the plane ofanesthesia can be deepened at will.
When the analgesia technique is to be started, itshould first be explained to the patient that she is notgoing to be "put to sleep" and that she will only begiven enough anesthetic to dull the pain and make itbearable, so that she can work with it. She should betold to warn the anesthetist as soon as the pain begins,that the face mask will then be applied, and that sheshould take a deep breath of the anesthetic and "hold

it." It must be explained that if she will do so theanesthetic will seep into her lungs and give her muchmore relief from the pain than if she lets it escape byopening her mouth to cry out. Despite this prelim-inary explanation of the procedure which is to befollowed, usually the anesthetist has to repeat thedirections many times, in simplified form: "Take adeep breath, hold it!" When the cervix is fully dilated,these directions are amplified to: "Take a deepbreath, hold it, bear down!"
If waste of gas is prevented by a reasonably tightadjustment of the mask to the face, the exhalingvalve remaining closed meanwhile, the gas can beeffectively rebreathed and, often, one filling of the bagwill be sufficient for the control of each pain. Whenthe pain subsides the face mask is removed, and thebag is emptied and refilled with nitrous oxide andoxygen in readiness for the next pain.
Nausea can sometimes be relieved by an increase inthe proportion of oxygen, but it is well to turn thepatient's head to one side, and if vomiting occurs, themask must immediately be removed from the faceand further precautions taken against aspiration ofvomitus.
Pierequisite for the safe, simple, and economicaluse of nitrous oxide-oxygen is that the person who isto administer it be familiar with the gas-oxygen ap-paratus, and, at a moment's notice, be able to recog-nize the need for, and supply, additional oxygen.
Much publicity has been given in recent years tothe use of caudal anesthesia for control of the pain ofchildbirth, and under ideal conditions the method isspectacularly effective.' But it seems unlikely that
1 R. Charles Adams, John S. Lundy, and Thomas H. Seldon. Con-tinuous caudal anesthesia of analgesia: a consideration of the technic,various uses and some possible dangers. J.A.M.A., 122:152.
116 ANESTHESIA

OBSTETRICAL ANESTHESIA
caudal anesthesia for obstetrics will become routine,for skill in its application calls for considerable prac-tice and highly specialized technique. It is contrain-dicated with the highly emotional individual and inconditions that rather commonly complicate termpregnancy, i.e., low blood pressure, placenta previa,and infection near the site of injection.
In order to provide complete relief of pain from theuterine contractions, the level of anesthesia of theabdominal wall must extend to about midway be-tween the symphysis and the umbilicus, and it mustbe possible to supplement the anesthesia readily asthe effect wears off. These needs can be accomplishedby the application of a local-anesthetic solution to thenerves emerging into the sacral canal below the duralsac by means of an implanted malleable spinal needleor catheter setup, similar .to that described for con-tinuous spinal anesthesia. Entrance to the sacral canalis made through the sacral hiatus, which may be diffi-cult to identify, especially under the physical handi-caps presented by full-term pregnancy and in the obesepatient. Also, abnormalities of the sacral vertebraare not uncommon. 2 On insertion of the needle, initialaspiration is essential to avoid the grave risk of in-jection of the anesthetic solution into the bloodstream, or within the dural sac, as the area is very'vascular and, in some individuals, the dural sac ex-tends abnormally low. If blood or spinal fluid isaspirated, it is generally considered advisable to aban-don the procedure altogether. Meticulous aseptic pre-cautions to avoid contamination of the apparatus andsolution by vaginal and rectal excretions must betaken, and also special care against breakage or acci-
2 Robert A. Hingson and Waldo B. Edwards. Comprehensive reviewof continuous caudal analgesia for anesthetists. Anesthesiology, 4:181.
117

dental withdrawal of the needle or catheter must beexercised.
Progress of the labor is not readily evidenced whenall pain is abolished, and the patient needs the closeattendance of the obstetrician throughout the period ofanesthesia. It is generally conceded by proponents ofthis form of anesthesia that a greater proportion of thepatients require forceps delivery when the method isused. The main reason given for this is that, althoughthe first stage of labor may be shortened, often thesecond stage is prolonged because the patient has nourge to bear down and expel the fetus when the per-ineum is completely anesthetized. However, the pro-found muscular relaxation afforded by caudalanesthesia greatly increases the ease of application ofthe forceps and completion of the third stage of labor.Provided the mother does not experience a markedfall of blood pressure, the baby is little affected by theanesthetic and usually cries spontaneously on delivery.
The anesthetic drugs most commonly used for con-tinuous caudal anesthesia in obstetric practice aremetycaine 1.5 per cent or procaine 1.5 per cent inphysiological saline solution. Metycaine gives themore prolonged effect. The quantity of either drugrequired depends, of course, upon the point duringlabor at which the anesthesia is started and upon theduration of the labor.
The term "saddle-block anesthesia" is used to de-scribe a low spinal anesthesia induced by the carefulsubarachnoid injection of a single dose of a hyper-baric solution of a local anesthetic. This method ismore predictable of success, and easier of accomplish-ment, than caudal anesthesia when complete pelvicanesthesia is indicated for a relatively short time.3
'M. L. Berlowe and F. L. Herrick. Painless labor with heavynupercaine. Conn. St. Med. J. 12:417.
118 ANESTHESIA

OBSTETRICAL ANESTHESIA
A study of the effectiveness of "mind over matter"in regard to the pain of childbirth, now being con-ducted at the New Haven Hospital clinic, should beof special interest to nurses. It was inaugurated tostudy the principle that, being a natural function of awoman's body, childbirth should be devoid of painbecause "there is no physiological function in thebody which gives rise to pain in the normal course ofhealth." This theory has been emphasized particularlyby Dr. Grantly Dick Read of London. He also statesthat the parturient woman is deprived of experiencing"an ecstasy unsurpassed by any previous experience inher life" when her mental faculties are beclouded orobliterated at such a time by hypnotic or anestheticdrugs.,
It has long been a matter of historical interest thatto primitive woman children were born with surpris-ingly little discomfort. For instance, in the heyday ofthe American Indian when the tribe was on the march,it was commonplace for a pregnant squaw, at term, tostop alone by the wayside for her babe to be born,then, as a matter of course, to catch up with the tribeat their next resting place.
A tradition of fear of pain and of the unknown,built up throughout the ages of civilization, resultingin abnormal tension, is blamed by Dr. Read for mostof the pain during labor. From the scientific stand-point he explains that there are two types of uterinemuscles involved in labor, those of the fundus and ofthe cervix, controlled by different plexuses of nerves,which normally compensate each other. But if at thebeginning of labor the normal contractions of thefundus are interpreted as pain, fear of this pain stimu-lates the sympathetic nervous system, which controlsthe muscles of the cervix, causing these muscles tocontract while the fundus is trying to expel the fetus.
119

Opposition between these two sets of muscles givesrise to pain.
Dr. Read's book, Childbirth Without Fear,4 de-scribes how this fear, and consequent pain, can beprevented by cultivation of the patient's understand-ing of the physiology of pregnancy and labor and ofthe subsequent symptoms that she will probably ex-perience. In the large majority of normal cases, hestates, this will lead to the enthusiastic co-operationand satisfaction of the patient. The study in progressunder the auspices of the Department of Obstetricsand Gynecology of the Yale University School ofMedicine, at present totaling approximately one hun-dred cases, amply justifies this prediction.
Success depends largely upon the temperament andintelligence of the patient and the interested and un-derstanding effort of the obstetrician and all thoseattendant upon her. An essential contributing factoris that in view of the patient's general physical con-dition she must be expected to have a normal labor.
The process of labor is interpreted to the patientas it progresses, emphasis being given to the impor-tance of general muscular relaxation. She is assured,meanwhile, that she will not be required to sufferpain and that an anesthetic is at hand for her to resortto at will. Experience has shown that rarely does apatient feel the need of availing herself of this med-ication.
4Grantly Dick Read, Childbirth Without Fear, The Principles and
Practice of Natural Childbirth.
120 ANESTHESIA

Chapter 14
ENDOTRACHEAL ANESTHESIA
A PERFECT airway can practically always beassured, during general anesthesia, by the use of anendotracheal (intratracheal) tube. There are severalvarieties of this apparatus in sizes suitable for all agesof patients. The tube can be inserted while the pa-tient is conscious if adequate topical local anesthesiahas been effected beforehand, but, usually, intubationis not attempted until a stage of general surgical an-esthesia has been reached. The plane of anesthesianecessary for intubation depends largely upon theexperience and skill of the anesthetist in this partic-ular technique. "Practice makes perfect," and it isworth while for the anesthetist to acquire this skill,but the beginner must avoid haste and should notattempt intubation until the patient is in a relativelydeep plane of ether anesthesia. There are twomethods of introduction of the tube: (1) "Blind" in-tubation denotes passage of a curved, moderately softrubber tube through one of the nasal orifices, past theglottis, and into the trachea; proper curvature of thetube and position of the head and neck tend to pre-vent the point of the tube from entering the easilyaccessible esophagus. (2) "Direct vision" intubation
121

requires the use of a laryngoscope (Figure 7) to exposethe glottis, the tube being passed during inspiration.Twice the distance between the opening of the earand the ala of the nose provides a rough estimate forthe length of the tube required. The distal end of thetube must not quite reach the bifurcation of thetrachea. The mouth of the patient should be keptmoderately open by means of a rubber or firm gauze-roll prop inserted between the teeth, in order to pro-tect the proximal end of the tube from occlusion bybiting. Adaptors are available for connecting the tubeto the gas machine.
It is also quite possible to continue the anesthesiaby means of a face mask, either open or closed, theendotracheal catheter acting merely as an airway anda ready means for suctioning drainage from the lungsor bronchi.
If a closed circuit for rebreathing is desired, a leak-proof adjustment can be made by one of two methods:a balloon cuff can be attached to the catheter and in-flated to a size sufficient to fill in the lumen of thetrachea after the catheter has been introduced, orthe pharynx around the catheter can be lightlypacked with moistened gauze. Mineral oil is the bestmoistening medium. Either of these methods are val-uable also in preventing aspiration of emesis or ofdebris from surgery of the nose or mouth.
An endotracheal tube in situ is almost essential forthe safety of the patient in a certain few surgical pro-cedures. These include those that involve the dangerof aspiration of septic material, those in which thereis need for repeated suctioning of the deep air pas-sages during operation, those with obstructive lesionsof the respiratory system or its immediate neighbor-hood (the catheter can be inserted via a tracheotomywound, if necessary), and those where "controlled res-
122 ANESTHESIA

B
t
Figure 7. Endotracheal apparatus. Available in various sizes andtypes and from various firms. The instruments illustrated arefrom the Foregger Co., New York. A) laryngoscope; B)laryngoscope blade, child's size: C) endotracheal tubes, fornasal or oral route; D) endotracheal tubes, oral; E) ballooncuff, inflated.


ENDOTRACHEAL ANESTHESIA 123
piration" is indicated to offset the profound muscularrelaxation that may be required by the surgeon. How-ever, in the large majority of cases, a satisfactorilyclear airway can be maintained by more simple meansand the routine use of the endotracheal tube for thegeneral run of patients is condemned by many prac-titioners as potentially harmful and impracticable.

Chapter 15
CURARE
THE acceptance of curare as a therapeuticagent by the medical profession is another instance ofthe harnessing of a virulent poison for the service ofmankind. Curare is the drug that, for centuries, wasused by the South American Indians to poison the tipsof their arrows for hunting and warfare. Penetrationof the arrow, even in a nonvital part of the body,dramatically felled the victim in a state of completehelplessness. The poison was obtained from a brew ofleaves, bark, and roots of various plants indigenousto northern and western South America.
Samples of the crude drug, in the form of paste,which were obtained occasionally by foreign explorers,were investigated by European physiologists of thenineteenth and early twentieth centuries, and someinteresting discoveries were made regarding it.1 Amongthese discoveries were the facts that the drug, in con-trolled dosage, causes temporary paralysis of theskeletal muscles and that its primary poisonous effectis paralysis of the muscles of respiration. Research
1Richard C. Gill, Curare: Misconceptions regarding the discoveryand development of the present form of the drug. Anesthesiology,7:14.
124

CURARE 125
with the drug was greatly restricted by scarcity of theproduct and lack of knowledge of its origin.
The modern use of curare in clinical medicine wasmade possible by the American explorer and botanist,Richard C. Gill, 2 who, having been impressed by thetherapeutic possibilities of the drug by a previouspersonal experience, organized an expedition intoSouth America in order to learn the botanical sourceof curare and the methods by which the drug was ex-tracted and compounded. He spent many months inthe jungle and gained the confidence of the Indianssufficiently to be able to fulfill the purpose of the ex-pedition.
The following year, laboratory research with thecrude drug resulted in the production of a purifiedand stable preparation suitable for therapeutic use,which was put on the market in 1939 by E. R. Squibband Sons under the name Intocostrin, the activeprinciple of which is d-tubocurarine chloride.
The selective action of curare on the skeletal mus-cles of the body having been proved in the laboratory,it was to be expected that the early clinical use of thepurified drug would be in the treatment of convul-sions and various spastic conditions. The results ofsuch treatments suggested possibilities that the relax-ant effects of Intocostrin might be of value in generalsurgical anesthesia, and this impression was first con-firmed by Dr. Harold Griffith of Montreal. A reportof the first series of cases in which he used Intocostrinin conjunction with general anesthesia, was publishedin 1942.3 This spurred the interest of anesthetists andresulted in the current prominence attained by deriv-atives of curare in the practice of anesthesia.
2 Stuart C. Cullen. Curare: its past and present. Anesthesiology,8:479.
3 Harold R. Griffith and G. Enid Johnson. The use of curare ingeneral anesthesia. Anesthesiology, 8:418.

It is generally accepted, for it has long been evi-denced by the reaction of the patients, that the toxiceffect of a general anesthetic increases as the plane, ordepth, of anesthesia increases. As a rule, a patientshows signs of much more prostration following arelatively short anesthesia of high concentration thanafter a prolonged anesthesia carried in a light plane.But a light plane of anesthesia may be inefficient incontrolling the muscular reflex of movement or spasmstimulated by pain at the surgical field. This, in turn,may prove a serious handicap to the surgeon and mayhave disastrous results for the patient. Realizing thesedisadvantages and limitations, which complicate themaintenance of an ideal general anesthesia, surgeonsand anesthetists have sought to control muscular re-action by other means than by deepening the plane ofanesthesia. The blocking of sensory-nerve impulsesfrom the surgical field, with a local anesthetic, provedthe most effective means of doing this. The peripheralnervous system is not readily depressed by the generalanesthetic drugs, which are primarily central depres-sants. All forms of local anesthesia, however, havecertain drawbacks and are, in varying degree, timeconsuming. Once proof had been given that curarecould be safely used with general anesthesia, the easeand simplicity of its administration and the predict-ability of its effective results, in comparison to those oflocal anesthesia, assured its adoption by professionalanesthetists.
Curare is not an anesthetic. The effect of the drugon the skeletal muscles, marked flaccidity, is ascribedto its ability to interrupt nerve impulses at the neuro-muscular junction. In therapeutic dosage, this effectis transitory and can be kept well under control. Thedrug seems to be remarkably free from harmful side
126 ANESTHESIA

effects.4 A single small dose, given intravenously whenthe patient is in first-plane surgical anesthesia, im-mediately relaxes the muscles of the face, throat, neck,extremities, and abdomen in sequence. The mainte-nance of a perfectly clear airway is essential for thepatient's safety.
The dose is regulated in accordance with the an-esthetic drug that is being used and the age andweight of the patient. As in the case of all drugs, varia-tion in individual susceptibility to curare will befound and only the smallest effective dose should beused. Large doses cause paralysis of the intercostalmuscles and the diaphragm. This extreme conditionis sometimes intentionally effected in order to stillthe respiratory movements in the surgical field; res-piratory exchange is then maintained by rhythmicpressure of the breathing bag, which is kept well in-flated with the anesthetic vapor and an adequateproportion of oxygen.
Thus the value of curare lies in the fact that by itscarefully controlled use, muscular relaxation, adequatefor the surgeon's need, can be maintained while thepatient is kept in a plane of light anesthesia. On theother hand, the drug presents danger in that the char-acteristic signs of anesthesia are obliterated. Althoughin some instances unconsciousness has developed whencurare has been given, without an anesthetic, in dosagesufficient to cause paralysis of the respiration,5 it hasbeen proved that the patient may remain keenly sensi-tive to pain and fear while being unable to demon-strate his distress.6
4 Benjamin H. Robbins and J. S. Lundy. Curare and curare-like
compounds, a review. Anesthesiology, 8:348.6 R. J. Whitacre and A. J. Fisher. Clinical observations on the use
of curare in anesthesia. Anesthesiology, 6:124.6
Scott M. Smith, Hugh O. Brown, James E. P. Tomans, andLouis S. Goodman. The lack of cerebral effects of d-Tubocurarine.Anesthesiology, 8:1.
127CURARE

Two preparations of curare are available at thepresent time, Intocostrin and d-tubocurarine chloridesolution. One cc. of either preparation representstwenty units of standardized curare, 3 mgm. ofd-tubocurarine chloride. The solution is nonirritatingto the body tissues and may be given by intravenousor intramuscular injection. The former method is con-sidered to be the more readily controllable. The pe-riod of muscular relaxation is relatively short, for thedrug quickly disappears from the blood stream. There-fore, repeated small doses may be given if indicated.
Warning has been given that ether has a "curari-form action," 7 and that a much smaller dose of curareis indicated when the anesthesia is to be maintainedwith ether than when one of the anesthetic gases is tobe used. While prostigmine is the pharmacologicalantidote for the peripheral action of curare, its use isnot advocated when there is evidence that depressionof the central nervous system has resulted from anoverdose of the drug.8
From consideration of these characteristics of cu-rare, it is evident that clinical use of this drug shouldbe undertaken only by the highly skilled anesthetistand that preparation for intratracheal intubationshould always be in readiness in case the need forartificial respiration should arise.
7 Stuart C. Cullen. Clinical and laboratory observations on the use
of curare during inhalation anesthesia. Anesthesiology, 5:166.8Smith, Brown, Tomans, and Goodman, loc. cit.
128 ANESTHESIA

Chapter 16
DANGEROUS POTENTIALITIES
ACCIDENT cases and others admitted to thehospital for emergency operations often present com-plicating difficulties for the anesthetist, especially thatof the possibility of food being in the stomach. Thiscondition is a very serious hazard because of the prob-ability that the induction of general anesthesia mayprecipitate emesis and the unconscious patient may bechoked by masses of undigested food or that particlesof gastric contents may be aspirated and result in post-operative pneumonia or lung abscess. Many fatalitieshave been reported from such happenings.
A report that several hours have elapsed since thelast meal was eaten cannot safely be taken as proofthat the food has left the stomach. In the presence ofpain, fear, or the emotional disturbance occasionedby the accident and/or admission to the hospital,digestion may be markedly delayed or entirely stopped.This is particularly true if morphine has been givenearly. Proof of this interruption of digestion has beenabundantly evidenced.
Serious misunderstanding also can arise when thepatient's admission to the hospital for an electiveoperation is delayed until the day on which the opera-
129

tion is to be performed. The doctor's order of "nobreakfast" is commonly misconstrued as not to in-clude milk or even toast and cereal. The child patientmay have made a surreptitious "raid on the icebox"and hastily swallowed a glassful of milk which, later,during the anesthesia, may be vomited as a large,heavy, dangerously obstructing curd. The pernicioushabit of bribing a child to submit to the ordeal ofgoing to the hospital by treating him, en route, to abar or two of chocolate or an ice cream cone is to beanticipated. Admission of such misunderstandings andindiscretions may not be readily forthcoming untilafter the regrettable accident has happened.
The complication of a full stomach is frequentlymet in obstetrics and may be sometimes unavoidablewith the short labor of many multiparae. How bestto cope with this serious problem is often a bafflingquestion for the anesthetist. Gastric lavage is not suffi-ciently effective in removing solid food unless thepassage of the stomach tube precipitates spontaneousvomiting. An anesthetic which effects a smooth, quickinduction without anoxia (oxygen want) should bechosen in an effort to prevent stimulation of the vomit-ing center. On the first sign of impending vomiting,however, the anesthetic mask must be removed, themouth opened, and the head and shoulders of thepatient turned well to one side; it may be necessaryto slap the back sharply with the palm of the hand inorder to dislodge solid matter from the esophagus,and to swab out the patient's mouth. The patientshould be allowed to waken sufficiently to obey anorder to cough well in an effort to clear the air pas-sages. Suction apparatus is of little help unless thematerial is of liquid consistency only. The above pre-cautions should be followed also, when indicated, dur-ing the stage of recovery from anesthesia.
130 ANESTHESIA.

DANGEROUS POTENTIALITIES
Cases of acute intestinal obstruction, of advancedstage, are grave risks for general anesthesia. Peristalsisis sometimes reversed in this condition, causing a moreor less continuous flow of fluid intestinal material intothe stomach and up into the throat and mouth. Thechances of aspiration of some of this fluid, or preven-tion of drowning in it, may be lessened somewhat bykeeping the patient in Trendelenburg position forposture drainage. This is more effective if a stomachor intestinal tube has been inserted and left in place;the tube can pass from under one side of the face maskto drain by gravity or suction into a pan or bottle.
Another danger inherent in some forms of anesthesianowadays is that of explosion. This danger was intro-duced with the modern method of inhalation anes-thesia in which the anesthetic vapor, combined withoxygen, is enclosed in a rubber bag. Should the anes-thetic be inflammable and be accidentally ignited, theoxygen would greatly add to the force of the ex-plosion. If this should happen during the course ofanesthesia, a fatality due to rupture of the patient'slungs would be almost inevitable because the securelyfastened face mask is connected to the bag by rubbertubing.
By the open-drop method on the other hand, dangerfrom an inflammable anesthetic that might be ignitedby proximity to an open flame or sparking electricequipment is limited to that of fire, which may offersome chance of controllability. Whatever the methodemployed, however, the combined use of an inflam-mable anesthetic and an evident cause for its possibleignition is reprehensible because it is potentially verydangerous.
Unfortunately, the careful elimination of evidentmeans of ignition may not insure safety from explosionsince conditions sometimes contribute to a build-up
131

of static electricity in and about the gas-oxygen ma-chine, and should a "spark point" be reached (theelectrostatic potential be suddenly discharged), anexplosion might occur.
Static electricity is most prevalent in dry coldweather, as is commonly evident in the sparking, snap-ping, or clinging effect produced by friction on silkand woolen clothing and blankets. These articles arenonconductive to electricity and should not be wornin the operating room; rayon garments and noncon-ductive rubber-soled shoes are also sources of danger.The anesthetist must be careful to avoid all forms offriction in handling the anesthetic apparatus and thepillows and coverings about the patient's head.
Raising the humidity (water content) of the sur-rounding atmosphere is an effective means of lessen-ing the danger of electrostatic ignition; it is claimedthat the slight film of water, deposited on all objectswhen the relative humidity level is 54 per cent ormore, harmlessly dissipates static charges as they form.1
The inside of the face mask, breathing tubes, and bagshould be moistened with water before they are used.
A simple and inexpensive intercoupling apparatus 2
is available also for diminishing build-up of electro-static charges, but this protection is limited strictly tothe objects intercoupled, and constant vigilance isnecessary to prevent its being broken by contact witha person who happens to be highly charged.
The importance of stressing the risk of explosionis real, but the danger should not be overemphasized.With the experience of twenty-five years in a "teach-ing hospital" where inflammable gaseous anesthetics
1 Donald Guthrie and K. W. Woodhouse. Safety factors in ethyleneanesthesia. J.A.M.A., 114:1846.
2 The Horton intercoupler, devised by Professor J. Warren Hortonof Massachusetts Institute of Technology and obtainable from themanufacturers of gas-oxygen equipment and medical gases.
132 ANESTHESIA

DANGEROUS POTENTIALITIES 133
have been administered daily, under close supervision,by a great many inexperienced students, the authorfeels justified in endorsing the opinion that, with theobservance of reasonable precautions, explosion isone of the least of the hazards of anesthesia; we havehad the good fortune never to have suffered a fire orexplosion.

Chapter 17
OXYGEN THERAPY
OXYGEN therapy holds a place of wide signifi-cance today, and a brief review of the subject maywell be included in a review of anesthesia, for it owesits successful growth largely to the understanding anddevelopment of the gaseous anesthetics. The cylindersin which oxygen is stored and the equipment providedfor its delivery to the patient are practically identicalwith those used for all types of medical gases, and thesame care is necessary in handling them. Because theanesthetist is so familiar with the use and importanceof oxygen in anesthesia and with the essential equip-ment, it is logical that, increasingly, oxygen therapyis being included among the responsibilities of theanesthesia staff.
Normally, an ample supply of oxygen is availablein the atmosphere for the needs of the body, and thelevel of supply is kept very constant by the functionsof respiration and circulation. But if these functionsare impeded in any way, or the inhaled atmosphereis too rarefied, a state of anoxia (oxygen deficiency)will prevail in the body. The symptoms of distress, thetissue damage, and the possibility of fatality resultingfrom anoxia parallel the severity and duration of the
134

oxygen deficiency and the age and state of health ofthe individual concerned. In many cases the adminis-tration of additional oxygen, if it is given sufficientlyearly and in adequate quantity, will effectively offsetthese discomforts and dangers.
The most simple way of administering oxygen is bymeans of a nasal catheter. To avoid dilatation of thestomach by the oxygen, and to insure its adequateabsorption into the lungs, it is essential that the tipof the catheter be properly placed within the oro-pharynx 1 and its movement prevented by fasteningit securely to the face with adhesive tape. A means ofincreasing the humidity of the oxygen, to prevent dis-comforting drying of the mucosa of the pharynx, isprovided by a water bottle through which the gas isbubbled. Agitation of a generous quantity of wateris necessary for this purpose, but precaution must betaken against the possibility of overflow to the cath-eter. Therefore, it is important that the water bekept at the correct level, and this level should beplainly marked on the bottle.
The B.L.B. mask, especially designed for the pur-pose of oxygen therapy by Drs. Boothby, Lovelace, andBulbulian also affords a simple and effective means ofadministration of the gas, either by mouth or nasalbreathing. A single large cylinder of oxygen, suppliedwith a pressure-reducing gauge and humidifier, com-pletes the necessary equipment for either of thesemethods.
Several models of oxygen tents are on the marketbut the essential features of them all are devices forthe maintenance of the required proportion of oxygen,prevention of the accumulation of carbon dioxide, and
1 E. A. Rovenstine, I. B. Taylor, and K. W. Lemmer. Oropharyn-geal insufflation of oxygen: gas tensions in the bronchus. Anesth. &Analg., 15:10.
135OXYGEN THERAPY

136 ANESTHESIA
proper regulation of the temperature and humidity ofthe enclosed atmosphere. The tent should be largeenough and have plenty of visibility in the way ofclear window material so that the patient does not feeltoo "shut in." The mattress beneath the canopy needsto be covered securely by waterproof material in orderto prevent it from absorbing a high proportion of theoxygen.
If soda-lime is used for the absorption of carbondioxide, it should be understood that the period ofits efficiency depends upon the amount of carbondioxide that is being exhaled by the individual patientand that this is increased markedly by each additionaldegree of fever, by pain, fear, or activity. Consequently,the time of need for renewal of the charge of soda-lime may vary greatly, and the percentage of carbondioxide within the tent should be ascertained at fre-quent and regular intervals. If ice is used for the cool-ing system, a sufficient quantity must be maintainedand the drainage pipe kept clear to prevent accumula-tion of water in the chamber.
Elaborate, yet compact, apparatus is now available.It embodies automatic electric control of all the es-sential features of an oxygen tent, verification of whichis indicated on an illuminated instrument panel. Theevolution of such a machine, in this miracle age ofelectric control, was to be expected, and doubtless itwill simplify efficient management of this form ofoxygen therapy. But mechanical gadgets must not berelied upon to supplant human intelligence. A triflingmishap may put a stop to the most elaborate ma-chinery, and the pilot dare not sleep while the robotmanages the controls.
Although oxygen is not an inflammable gas, itgreatly intensifies combustion. For instance, in thepresence of free oxygen a barely smoldering cigarette

will burst into acute flame. Consequently, warning ofthe danger of fire when oxygen is being used must beplainly emphasized.
Combination of helium and oxygen is used to in-troduce oxygen when there is partial obstruction ofthe airway, which cannot be overcome by mechanicalmeans. The bronchial constriction of asthma, espe-cially during acute spasm, is the classical example ofsuch obstruction. The atomic weight of helium isonly 4, that of nitrogen is 14. When a combinationof 20 per cent oxygen and 80 per cent helium is sub-stituted for air, which consists of 20 per cent oxygenand 80 per cent nitrogen approximately, the atmos-phere breathed by the patient is only one third theweight of air and will pass through a constricted pas-sage much more readily.
For therapeutic use, the helium cylinder should al-ways contain at least 20 per cent oxygen, in order toavoid the risk of asphyxiation of the patient frompremature emptying of the oxygen cylinder whenseparate cylinders are being used. Sometimes a higherproportion of oxygen is indicated and this can readilybe made available by the insertion of a Y connectionin the delivery tube, to which is attached a cylinderof oxygen.
Oxygen under carefully controlled positive pressurehas been found very effective in the treatment of acutepulmonary edema due to cardiac ventricular failure. 2
This method of oxygen therapy requires the use of abreathing bag and close-fitting face mask or breathingtubes.
SAlvan R. Barach, John Martin, and Morris Eckman. Positivepressure respiration and its application to the treatment of acutepulmonary edema. Ann. Int. Med., 12:754.
137OXYGEN THERAPY


BIBLIOGRAPHY
Adams, R. Charles: Iitravenous Anesthesia. New York:Paul B. Hoeber, Inc., 1944.
Adams, R. Charles, Lundy, John S., and Seldon,Thomas H.: Continuous caudal anesthesia or analgesia:a consideration of the technic, various uses and somepossible dangers. J.A.M.A. 122 (1943).
Adriani, John: The Pharmacology of Anesthetic Drugs.Springfield, Illinois: Charles C. Thomas, 1941.
Barach, Alvan R., Martin, John, Eckman, Morris: Positivepressure respiration and its application to the treatmentof acute pulmonary edema. Ann. Int. Med. 12 (1938).
Beecher, Henry K.: The Physiology of Anesthesia. OxfordUniversity Press, 1938.
Berlowe, Max L., and Herrick, Francis L.: Painless laborwith heavy nupercaine. Conn. St. Med. J. 12 (1948).
Bourne, Wesley, and Sparling, Douglas W.: Some aspectsof vinyl ether (vinethene) anesthesia. Anesth. & Analg. 14(1935).
Bourne, Wesley, Bruger, Morris, and Dreyer, N. D.: Effectsof general anesthesia on function of the liver; the effectsof amytal and avertin, separately, on the blood, its re-action, the carbon dioxide combining power, and theconcentration; on body temperature; on the function ofthe liver; and on the rate of secretion and compositionof the urine. Anesth. & Analg. 10 (1931).
139

140 ANESTHESIA
Coryllos, Pol N., and Birnbaum, G. L.: Studies in pul-monary gas absorption and bronchial obstruction. Part3: A theory of gas absorption and atelectasis. Am. J. M.Sc. 183 (March 1932).
Cullen, Stuart C.: Clinical and laboratory observations onthe use of curare during inhalation anesthesia. Anesthe-siology 5 (1944).
Cullen, Stuart C.: Curare: its past and present. Anesthesi-ology 8 (1947).
Dripps, Robert D.: The immediate decrease in blood pres-sure seen at conclusion of cyclopropane anesthesia;"Cyclopropane Shock." Anesthesiology 8 (1947).
Fiilp-Miller, Ren6: Triumph Over Pain. (Translated byEden and Cedar Paul). New York: Literary Guild ofAmerica, Inc., 1938.
Fulton, John F., and Stanton, Madeline E.: The Centen-nial of Surgical Anesthesia: An Annotated Catalogue.New York: Henry Schuman, 1946.
Genauer, Mortimer B.: Post-anesthetic heat stroke. Anes-thesiology 7 (1946).
Gilbert, Gordon, and Dixon, Alfred B.: Observations onDemerol as an obstetric analgesic. Am. J. Obst. & Gynec.45 (1943).
Gill, Richard C.: Curare: Misconceptions regarding thediscovery and development of the present form of thedrug. Anesthesiology 7 (1946).
Goldschmidt, Samuel, Ravdin, I. G., Lucke, Baldwin,Muller, G. P., Johnston, C. G., and Ruigh, W. L.: Di-vinyl ether: experimental and clinical studies. J.A.M.A.102 (1934).
Goodman, Louis, and Gilman, Alfred: The Pharmacologi-cal Basis of Therapeutics. New York: The MacMillanCompany, 1941.
Griffith, Harold R., and Johnson, G. Enid: The use ofcurare in general anesthesia. Anesthesiology 3 (1942).
Guedel, Arthur E.: Inhalation Anesthesia. A FundamentalGuide. New York: The MacMillan Company, 1944.
Guedel, Arthur E.: Metabolism and reflex irritability inanesthesia. J.A.M.A. 83 (1924).

BIBLIOGRAPHY 141
Guthrie, Donald, and Woodhouse, K. W.: Safety factors inethylene anesthesia. J.A.M.A. 114 (1940).
Gwathmey, James Tayloe: Anesthesia. New York: TheMacMillan Company, 1925. (2nd Revised Edition).
Haight, Cameron: Intratracheal suction in the manage-ment of postoperative pulmonary complications. Ann.Surgery 107 (1938).
Henderson, Yandell: Adventures in Respiration. Baltimore,Maryland: The Williams and Wilkins Company, 1938.
Henderson, Yandell, and Haggard, Howard W.: NoxiousGases. and the Principles of Respiration InfluencingTheir Action. New York: Reinhold Publishing Cor-poration, 1943. (2nd Revised Edition).
Hewer, C. Langton: Recent Advances in Anesthesia andAnalgesia. Philadelphia: The Blakiston Company, 1939.(3rd Edition.)
Hingson, Robert A., and Edwards, Waldo B.: Compre-hensive review of continuous caudal analgesia for anes-thetists, Anesthesiology 4 (1943).
Hunt, Alice M.: A newer method for computing theindividual dosage of Avertin. J. Am. A. Nurse Anes-thetists 3 (1935).
Huntington, Robert W., Jr.: The treatment of tetanus.Yale J. Biol. & Med. 3 (1931).
Keys, Thomas E.: The History of Surgical Anesthesia. NewYork: Henry Schuman, 1945.
Lemmon, William T.: A method for continuous spinalanesthesia, a preliminary report. Ann. Surg. 111 (1940).
Levy, A. Goodman: Chloroform Anesthesia. New York:William Wood & Company, 1922.
Macintosh, R. R., and Heyworth, P. S. A.: Pentothal-arterial injection of, a warning. Lancet, 1943, Part 2.
Miller, Albert H.: The origin of the word "Anaesthesia."New Eng. J. Med. 197 (1927).
Nosworthy, M. D.: The Theory and Practice of Anesthesia.London: Hutchinson Scientific, 1935.
Ochsner, Alton: Anesthesia of the sympathetic system:Editorial. Anesthesiology 4 (1943).

142 ANESTHESIA
Read, Grantly Dick: Childbirth Without Fear. The Prin-ciples and Practice of Natural Childbirth. New York andLondon: Harper and Bros., 1944. (3rd Edition).
Robbins, Benjamin H., and Lundy, J. S.: Curare andcurare-like compounds, a review. Anesthesiology 8 (1947).
Rovenstine, E. A., Taylor, I. B., and Lemmer, K. E.: Oro-pharyngeal insufflation of oxygen: gas tensions in thebronchus. Anesth. & Analg. 15 (1936).
Saklad, Meyer, Dwyer, Clement S., Kronenberg, Sanford,Neves, Edmund, and Sorkin, Morris: Intra-spinal seg-mental anesthesia, a preliminary report. Anesthesiology8 (1947).
Scheifley, Charles H.: Pentothal sodium: its use in thepresence of hepatic disease. Anesthesiology 7 (1946).
Schumann, William R.: Demerol (S-140) and scopolaminein labor, a study of 1,000 cases. Am. J. Obst. & Gynec.47 (1944).
Sebening, Walter: Recent researches and clinical advancesin Avertin narcosis. Anesth. & Analg. 11 (1932).
Smith, Scott M., Brown, Hugh O., Tomans, James E. P.,and Goodman, Louis S.: The lack of cerebral effects ofd-Tubocurarine. Anesthesiology 8 (1947).
Stiles, J. A., Neff, W. B., Rovenstine, E. A., and Waters,R. M.: Cyclopropane as an anesthetic agent: a prelim-inary clinical report. Anesth. & Analg. 13 (1934).
Thoms, Herbert: Anesthdsie a la Reine. Am. J. Obst.& Gynec. 40 (1940).
Waters, Ralph M.: Advantages and technic of carbon di-oxide filtration with inhalation anesthesia. Anesth. &Analg. 5 (1926).
Waters, Ralph M.: Cyclopropane-a personal evaluation.Surgery 18 (1945).
Waters, Ralph M., and Schmidt, Erwin R.: Cyclopropaneanesthesia. J.A.M.A 103 (1934).
Whitacre, R, J., and Fisher, A. J.: Clinical observations onthe use of curare in anesthesia. Anesthesiology 6 (1945).
Wright, Samson: Applied Physiology. New York: OxfordUniversity Press, 1934. (5th Edition)
Yudin, Sergei S.: Refrigeration anesthesia for amputations.Anesth. & Analg. 24 (1945).

INDEX
A
Adrenalin, 100contraindication, 106
Airway, maintenance of ade-quate, 39
Alcohol, 105Alveoli, lung, 14Amytal, 24Anesthesia, art of, 54Arthritis, 105Asthma, 137Atropine, 25, 26, 30, 62Avertin, 11, 20, 40, 86
administration, 86, 90basal anesthetic, 87, 91
contraindications, 87dosage, 88premedication, 90preparation of solution, 89
B
Bath, cleansing, 34Bladder care, 84"Blow bottle," 41Bursitis, 105Butyn, 99
C
Cancer, 105-Carbon dioxide, 17, 42Care, preoperative and postoper-
ative, 32airway, maintenance of ade-
quate, 39bath, cleansing, 34bladder care, 34child, mental preparation of, 35
restraints, 37
143
diet, preoperative, 33enema, cleansing, 33head care, 34heat exhaustion, 37mouth hygiene, 34operating table, transfer to, 35patient, observation of, 40
position of, postoperative, 38preoperative, 36
protection from drafts, 39respiration, stimulation of, 41
"blow bottle," 41carbon dioxide, 42endotracheal catheter suc-
tion, 42restraints, 36
sedation, bedtime, 33postoperative, 40
water, 33Caudal or epidural anesthesia, 21
in obstetrics, 116contraindications, 117difficulties, 117metycaine, 118procaine, 118
Child, mental preparation of, 35restraints, 37
Chloroform, 9, 15, 56anesthesia, 56
advantages, 59dangers, 57disadvantages, 59technique, 58
Circulatory disorders, 105Cocaine, 4, 11, 99
Halstead, William, 11Koller, Carl, 11Niemann, Albert, 11
Codeine, 24, 29Curare, 124

144Curare, (Continued)
effect, 126ether and, 128history and research, 124prostigmine as antidote, 128uses, 126value, 127
Cyclopropane, 10in obstetrics, 115-oxygen, 77
complications, 78flexibility, 81helium, 84
technique, 84technique, 82
Waters, Ralph M., 10
DDangerous potentialities, 129
explosion, 131fire, 181
static electricity, 132precautions, 182
full stomach, 129in delayed operations, 129in emergencies, 129in obstetrics, 130precautions, 180
Davy, Sir Humphrey, 6Deficiency, oxygen, 17Demerol, 29Diet, preoperative, 38
EEndotracheal anesthesia, 121
introduction of tube, 121"blind," 121"direct vision," 121
necessity for, 122rebreathing, closed circuit for,
122Enema, cleansing, 33Ephedrine, 112Ether, 5, 40, 44
anesthesia, 44administration, 44
closed method, 45advantages, 45, 46disadvantages, 56
intrapharyngeal insuffla-tion, 44
method, 45rectal injection, 45
advantages, 46disadvantages, 46
INDEX
semiopen method, 44induction, 47
child, 55stages of anesthesia, 51
analgesia, 51excitement, 52maintenance, 52
technique, 48"frolics," 6-oil mixtures, 20
rectal injections in obstetrics,114
Ethyl chloride anesthesia, 59, 103advantages, 60disadvantages, 60general anesthesia, 59
closed method, 60open-drop, 59
local anesthesia, 60dental analgesia, 60
quick induction of ether anes-thesia, 60
Ethylene, 10-oxygen, 76
technique, 77anoxia, 77
Evipal soluble, 11, 94Evipan sodium, 94Explosion, 131
F
Fire, 181, 187
G
Gaseous anesthetics, 63apparatus, 63
accidents, 65care of, 65closed rebreathing, 67
filter chambers, 67circle, 67"to-and-fro," 68
identification, 64cyclopropane-oxygen, 77
complications, 78flexibility, 81helium, 84
technique, 84technique, 82
ethylene-oxygen, 76technique, 77anoxia, 77
nitrous oxide, 69analgesia, 70

INDEX
Gaseous anesthetics, (Continued)dental, 70obstetric, 71
surgical anesthesia, 71induction, 73
anoxia, 76ether, 74stages, 75
technique, 71General anesthesia, 19
inhalation, 19maintenance of adequate res-
piration, 20intravenous, 20
sodium pentothal, 20rectal, 20
Avertin, 20ether-oil mixtures, 20paraldehyde, 20
Gill, Richard C., 125Griffith, Harold, 125Guedel, A. E., 24Gwathmey, 20, 114
H
Halstead, William, 11Hashish, 4Head care, 84Heat exhaustion, 87Helium, 84, 137Henbane, 4Herpes zoster, 105Hickman, Henry H., 6History, 3
Avertin, 11chloroform, 9cocaine, 4, 11
Halstead, William, 11Koller, Carl, 11Niemann, Albert, 11
cyclopropane, 10Waters, Ralph M., 10
Davy, Sir Humphrey, 6ether, 5
"frolics," 6Paracelsus, 5
ethylene, 10Evipal soluble, 11Halstead, William, 11hashish, 4henbane, 4Hickman, Henry H., 6Holmes, Oliver Wendell, 8hyoscin, 4Jackson, Charles, 7
145Koller, Carl, 11Long, Crawford, 7mandrake, 4morphine, 4
Sertiirner, Friederich, W., 4Morton, William T. G., 7needle, hollow, 5
Wood, Alexander, 5Niemann, Albert, 11nitrous oxide, 6, 9
Davy, Sir Humphrey, 6novocain, 11opium, 4Paracelsus, 5pentothal sodium, 11Priestley, Joseph, 5Sertiirner, Friederich W., 4Simpson, James Y., 8"sweet vitriol," 5Victoria, Queen, 9Vinethene, 10Warren John C., 8Waters, Ralph M., 10Wells, Horace, 7Wood, Alexander, 5
Holmes, Oliver Wendell, 8Hyoscin, 4, 30Hypodermic injection, 25
I
Inhalation anesthesia, 19maintenance of adequate res-
piration, 20Intestinal obstruction, 181Intocostrin, 125Intravenous anesthesia, 20, 98
complications, 97contraindications, 96history, 93
evipan sodium, 94pentothal sodium, 94
sodium pentothal, 20technique, 95, 97
J
Jackson, Charles, 7
K
Koller, Carl, 11
LLavoisier, 16Lemmon, William T., 109

146Life, potential risk to, 16Lipoid solvents, 14Local anesthesia, 20, 99
application, 99concentration, 100
hypodermic, 20overdosage, 101
antidote, 102preparation, 102subcutaneous injection, 100
adrenalin, 100topical, 20
Long, Crawford, 7
M
Mandrake, 4Methods of inducing surgical an-
esthesia, 19general, 19
inhalation, 19maintenance of adequate
respiration, 20intravenous, 20
sodium pentothal, 20rectal, 20
Avertin, 20ether-oil mixtures, 20paraldehyde, 20
local, 20hypodermic, 20topical, 20
regional, 21caudal or epidural, 21nerve block, 21refrigeration, 21
advantages, 22spinal, 21
Metycaine, 118Morphine, 4, 26, 118
injection, 27intravenous, 27subcutaneous, 27
Sertirner, Friederich W., 4sulphate, 24
Morton, William T. G., 7Mouth hygiene, 34Mucus, 31
hazard of anesthesia, 31
N
Needle, hollow, 5Wood, Alexander, 5
Nembutal, 24, 26Nerve block, 21
INDEX
Nervous tissue, 13Niemann, Albert, 11Nitrous oxide, 6, 9, 69
analgesia, 70dental, 70obstetric, 71, 115
Davy, Sir Humphrey, 6surgical anesthesia, 71
induction, 73anoxia, 76ether, 74stages, 75
technique, 71Novocain, 11, 21, 99, 100, 104,
105, 109, 110
0
Obstetrical anesthesia, 113caudal anesthesia, 116
contraindications, 117difficulties, 117metycaine, 118procaine, 118
labor, first stage, 113drugs, analgesic, 113
hypnotic, 113rectal injection of ether and
oil, 114supplementary anesthesia,
114second stage, 115
analgesia, 115nitrous oxide-oxygen, 115
anesthesia, 115instructions, 116
pain and civilization, 119"mind over matter," 119normal labor, 119
"saddle-block anesthesia," 118Operating table, transfer to, 35Opium, 4Or6, 93"Overventilation," 17Oxygen, 16
deficiency, 17therapy, 184
administration, 135B.L.B. mask, 135nasal catheter, 135tent, 135ice, 136soda-lime, 136
fire, 137helium, 137pulmonary edema, 137

INDEX
PPantopon, 24, 28Paraldehyde, 20Paracelsus, 5Patient, observation of, 40
position of postoperative, 88preoperative, 36
protection from drafts, 89Pentothal sodium, 11, 40, 94
administration, 96Physiology, 13
alveoli, lung, 14Lavoisier, 16life, potential risk to, 16lipoid solvents, 14nervous tissue, 13oxygen, 16
deficiency, 17pressure, partial, 14respiration, normal, 17
carbon dioxide, 17"overventilation," 17
stage, induction, 15tension, anesthetic, 15tissue, fatty, 15
Pontocaine, 99, 109, 110Premedication, 23
advantages, 27agents, 24
Amytal, 24atropine, 25codeine, 29Nembutal, 24Pantopon, 24scopolamine, 25Seconal, 24
disadvantages, 28order, 26purpose, 23
Pressure, partial, 14Priestley, Joseph, 5Procaine, 118Prostigmine, 128
RRead, Grantly Dick, 119Rectal anesthesia, 20
Avertin, 20ether-oil mixtures, 20paraldehyde, 20
Refrigeration, 21advantages, 22
Regional anesthesia, 21, 104alcohol, 105
147caudal or epidural, 21induction, 106nerve block, 21refrigeration, 21
advantages, 22spinal, 21therapeutic, 105
arthritis, 105bursitis, 105cancer, 105circulatory disorders, 105herpes zoster, 105syphilis, tertiary, 105
Respiration, normal, 17carbon dioxide, 17"overventilation," 17stimulation of, 41
"blow bottle," 41carbon dioxide, 42endotracheal catheter suc-
tion, 42Restraints, 86
S
"Saddle-block anesthesia," 118Scopolamine, 25, 26, 80, 118Seconal, 24Sedation, bedtime, 88
postoperative, 40Segmental anesthesia, 110
advantages, 111Settirner, Friederich W., 4Simpson, James Y., 8Sodium pentothal, 20Solution, anesthetic, 108
hypobaric, 109Trendelenburg position, 108
isobaric, 108Spinal anesthesia, 21, 107
advantage, 107danger, 107induction, 109
catheter technique, 110needles, 111premedication, 112
ephedrine, 112segmental anesthesia, 110
advantages, 111solution, anesthetic, 108
hypobaric, 108Trendelenburg position, 108
isobaric, 108Spinocaine, 109technique, 111

148Spinocaine, 109Stage, induction, 15Static electricity, 182
precautions, 132"Sweet vitriol," 5Syphilis, tertiary, 105
T
Tension, anesthetic, 15Tissue, fatty, 15Tuohy, E. B., 110Trendelenburg position, 108
V
Vinethene, 10anesthesia, 61
advantages, 62disadvantages, 62methods, 62
closed rebreathing, 62open drop, 62
premedication, 62atropine, 62
quick induction of ether an-esthesia, 62
Volatile liquid anesthetic drugs,42
chloroform anesthesia, 56advantages, 59dangers, 57disadvantages, 59techniques, 58
ether anesthesia, 44administration, 44
closed method, 45advantages, 45, 46disadvantages, 56
intrapharyngeal insufflation,44
INDEX
method, 45rectal injection, 45
advantages, 46disadvantages, 46
semiopen method, 44induction, 47
child, 55stages of anesthesia, 51
analgesia, 51excitement, 52maintenance, 52
technique, 48complications, 50
ethyl chloride anesthesia, 59advantages, 60disadvantages, 60general anesthesia, 59
closed method, 60open drop, 59
local anesthesia, 60dental analgesia, 60
quick induction of ether an-esthesia, 60
vinethene anesthesia, 61advantages, 62disadvantages, 62methods, 62
closed rebreathing, 62open drop, 62
premedication, 62atropine, 62
quick induction of ether an-esthesia, 62
W
Warren, John C., 8Water, 33Waters, Ralph M., 10Wells, Horace, 7Wood, Alexander, 5