Embed Size (px)
Citation preview
CASE REPORT
Angle Class II, Division I malocclusion treated without premolar extraction
Stephen McCullough, DDS, MS" Yukon, Okla.
The treatment of an Angle Class II, Division I malocclusion without the extraction of premolars is described. Treatment was accomplished with the standard edgewise appliance using Merrifield directional forces systems. (AM J ORTHOD DENTOFAC ORTHOP 1994;106:317-21.)
W h e n one thinks of orthodontic treat- ment that employs the "Tweed Technique," a com- mon misconception is that the t reatment requires the removal of the four first premolars. Indeed, Tweed 's t reatment of a bimaxillary protrusion case that required this diagnosis forever changed orth- odontic thought. However, since Tweed 's era, there has been a constant refinement of the Tweed philosophy and of Tweed 's t reatment techniques. Levern Merrifield's studies of directional forces ~ and dimensions of the denture 2 and the subsequent development of his sequential force systems 3 has made it possible to properly diagnose, t reatment plan, and treat any type of ma locc lu s ion -no t just the Angle Class I or Class II with crowding and protrusion.
This case report will demonstra te the use of both the Tweed-Merrifield philosophy and the Merrifield force systems to correct an Angle's Class II, Division 1 dental malocclusion that was not complicated by substantial crowding or protrusion.
DIAGNOSIS
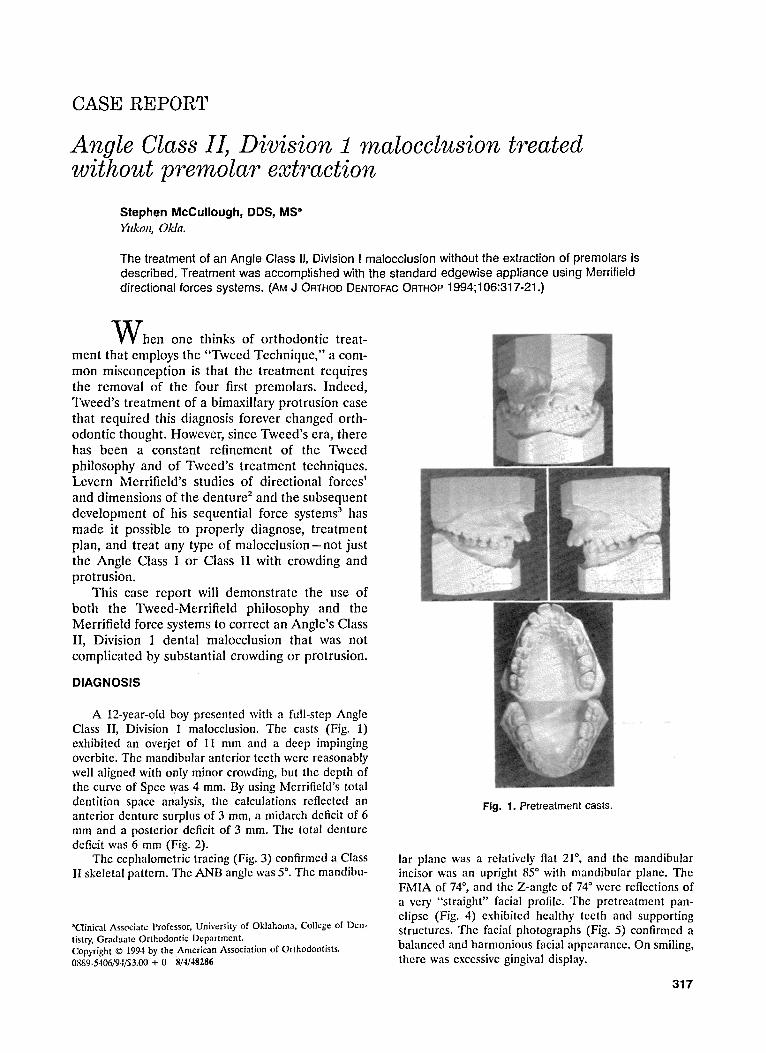
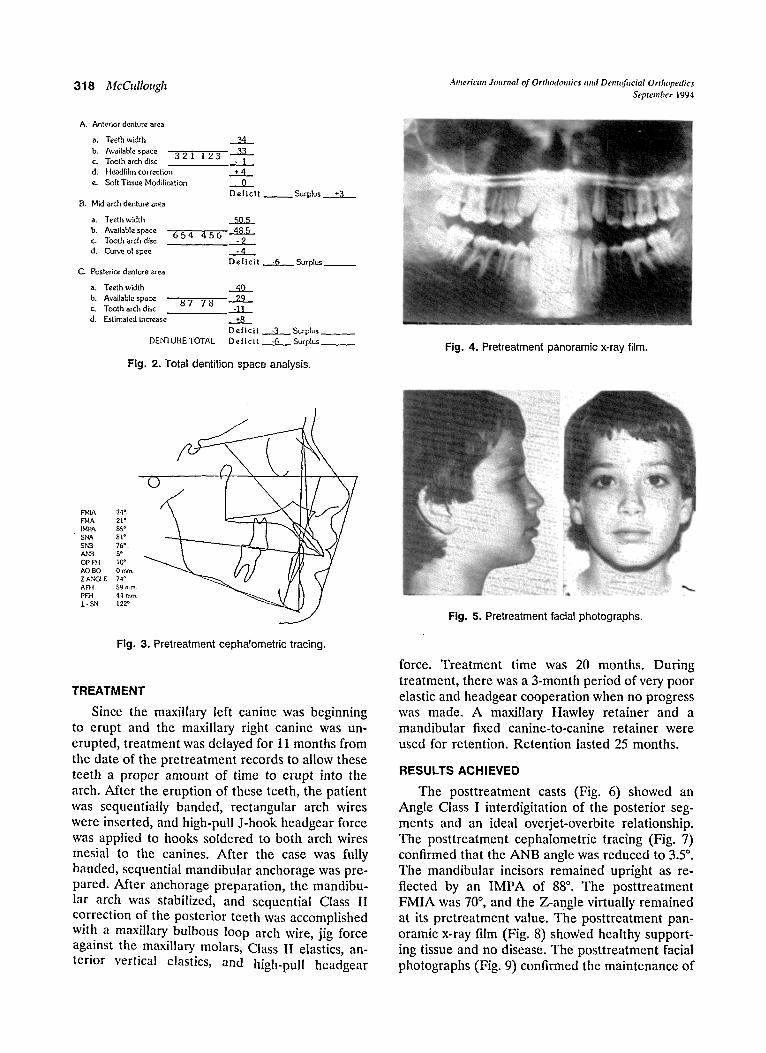
A 12-year-01d boy presented with a full-step Angle Class II, Division 1 malocclusion. The casts (Fig. 1) exhibited an overjet of I1 mm and a deep impinging overbite. The mandibular anterior teeth were reasonably well aligned with only minor crowding, but the depth of the curve of Spee was 4 mm. By using Merrifield's total dentition space analysis, the calculations reflected an anterior denture surplus of 3 mm, a midarch deficit of 6 mm and a posterior deficit of 3 ram. The total denture deficit was 6 mm (Fig. 2).
The cephalometric tracing (Fig. 3) confirmed a Class II skeletal pattern. The ANB angle was 5 ~ The mandibu-
aClinical Associate Professor, University of Oklahoma, College of Den- tistry, Graduate Orthodontic Department. Copyright �9 1994 by the American Association of Orthodontists. 0889-5406/94/$3.00 + 0 8/4/48286
Fig. 1. Pretreatment casts.
lar plane was a relatively flat 21 ~ and the mandibular incisor was an upright 85 ~ with mandibular plane. The FMIA of 74 ~ and the Z-angle of 74 ~ were reflections of a very "straight" facial profile. The pretreatmcnt pan- clipsc (Fig. 4) exhibitcd healthy teeth and supporting structures. The facial photographs (Fig. 5) confirmed a balanced and harmonious facial appearance. On smiling, there was excessive gingival display.
317
A. Anterior denture area
a. Teeth v,,idth ~t4
b. Available space 3 2 I 1 2 3 e. Tooth arch disc - 1 d. Headfilm correction + 4
e. S o f t l ' i s s u e M o d i f i c a t i o n 0
D e | l c i t B. Mid-arch denture area
a. Teeth width b. Available space c. l b o t h arch disc d, C u ~ ' e of spee
C, Posterior denture area
a, Teeth width b. Available space c. Tooth arch disc d. Estimated increase
50.5 6 5 4 4 5 6 48.5
• - ' t
D e l l c l t , "6
8 7 7 8
FbtlA 74 ~ FHA 21" LMPA 85* SNA 81 ~ SNB 76". ANB 5* OP-FH 10 ~ A O B O 0 mm Z ANGLE 74 ~ AF~ 59 turn.
PIER 4-~ ram.
1" SN 122"
., 40 29
-11 +8
D e l i c i t
Surplus +3
. .. S u r p l u s
"3 Surplus DENTURE TOTAL D e [ i c i t . -~ Surplus _
Fig. 2. Total dentition s p a c e analysis .
318 ]~lcCullough American Joun,al of Orthodontics and Dentofiwial Orthopedics September 1994
Fig, 4. Pretreatment panoramic x-ray film.
Fig. 3. Pretreatment cephalometric tracing.
TREATMENT
Since the maxillary left canine was beginning to erupt and the maxillary right canine was un- erupted, treatment was delayed for 11 months from the date of the pretreatment records to allow these teeth a proper amount of time to erupt into the arch. After the eruption of these teeth, the patient was sequentially banded, rectangular arch wires were inserted, and high-pull J-hook headgear force was applied to hooks soldered to both arch wires mesial to the canines. After the case was fully banded, sequential mandibular anchorage was pre- pared. After anchorage preparation, the mandibu- lar arch was stabilized, and sequential Class II correction of the posterior teeth was accomplished with a maxillary bulbous loop arch wire, jig force against the maxillary molars, Class II elastics, an- terior vertical elastics, and high-pull headgear
Fig. 5. Pretreatment facial photographs.
r.
force. Treatment time was 20 months. During treatment, there was a 3-month period of very poor elastic and headgear cooperation when no progress was made. A maxillary Hawley retainer and a mandibular fixed canine-to-canine retainer were used for retention. Retention lasted 25 months.
RESULTS ACHIEVED
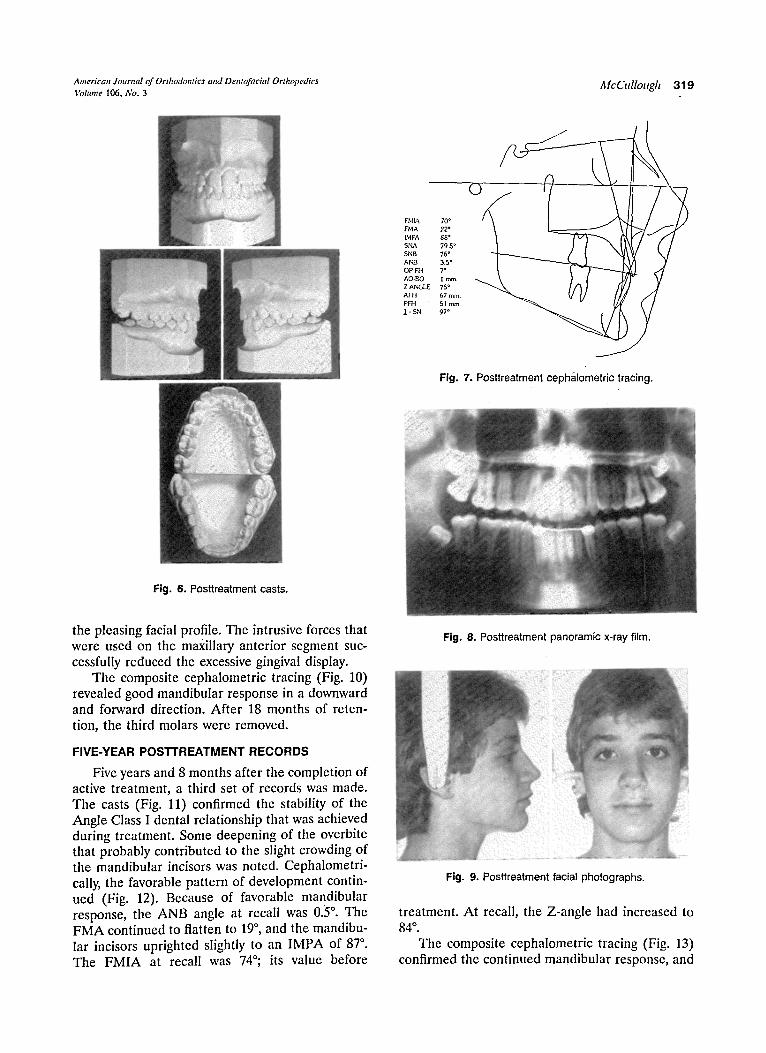
The posttreatment casts (Fig. 6) showed an Angle Class I interdigitation of the posterior seg- ments and an ideal overjet-overbite relationship. The posttreatment cephalometrie tracing (Fig. 7) confirmed that the ANB angle was reduced to 3.5 ~ The mandibular incisors remained upright as re- flected by an IMPA of 88 ~ The posttreatment FMIA was 70 ~ and the Z-angle virtually remained at its pretreatment value. The posttreatment pan- oramic x-ray film (Fig. 8) showed healthy support- ing tissue and no disease. The posttreatment facial photographs (Fig. 9) confirmed the maintenance of
American Journal of Orthodontics and Dentofilcial Orthopedics l~[cCllllollgh 319 Volume 1 0 6 , N o . 3
�9
FHIA 70 * IrMA 22* LHPA 88 ~ SNA 79 5* SNB 76* ANB 3.5* OP-Ht 7 ~ AO-BO I ram. Z ANGLE 75* AF}I 67 ram. PFH 51 mm. 1 - SN 97*
Fig. 7. Posttreatment ceph&lometric tracing.
Fig. 6. Posttreatment casts.
the pleasing facial profile. The intrusive forces that were used on the maxillary anterior segment suc- cessfully reduced the excessive gingival display.
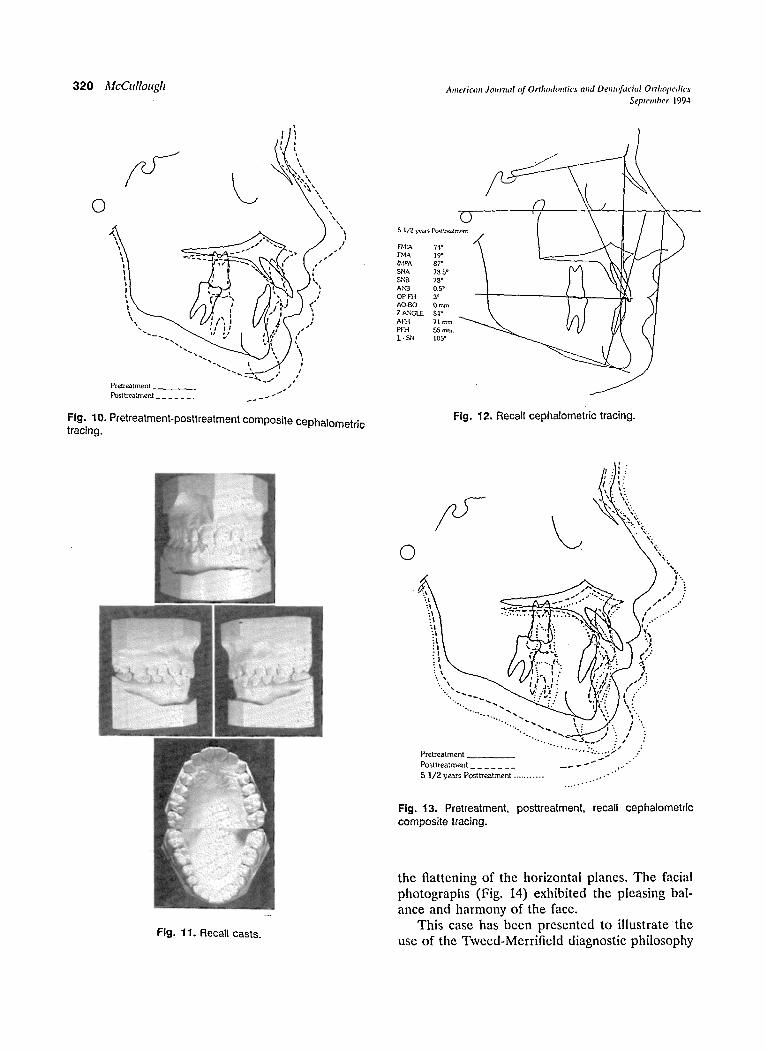
The composite cephalometric tracing (Fig. 10) revealed good mandibular response in a downward and forward direction. After 18 months of reten- tion, the third molars were removed.
FIVE-YEAR POSTI 'REATMENT RECORDS
Five years and 8 months after the completion of active treatment, a third set of records was made. The casts (Fig. 11) confirmed the stability of the Angle Class I dental relationship that was achieved during treatment. Some deepening of the overbite that probably contributed to the slight crowding of the mandibular incisors was noted. Cephalometri- cally, the favorable pattern of development contin- ued (Fig. 12). Because of favorable mandibular response, the ANB angle at recall was 0.5 ~ The FMA continued to flatten to 19 ~ and the mandibu- lar incisors uprighted slightly to an IMPA of 87 ~ The FMIA at recall was 74~ its value before
Fig. 8. Posttreatment panoramic x-ray film.
Fig. 9. Posttreatment facial photographs.
treatment. At recall, the Z-angle had increased to 84 ~ .
The composite cephalometric tracing (Fig. 13) confirmed the continued mandibular response, and
320 ~ [ c C t d l o t t g h A m e r i c a n Joz~rna! o f O r t l z o d o n t i c s a n d D e , z t t ~ t c i ( z l O r t h o p e d i c s
S e p t e m b e r 1 9 9 4
O o
- - - ~ -*~ F~,IA 19" I ~- - ~ - _ r ~, t 1,~4 PA 87* t I i l [ SNA 78 S* II '.�9 SNB 78* I r ANB 0.5 ~ I �9 O P - F ~ I 3*
AO'BO 0 ram. / I , Z ANGLE 84*
Pictreatment / Post treatment . . . . . . . ~ - - ~ ~ "
Fig. 10. Pretreatment-posttreatment composite cephalometric Fig. 12. Recall cephalometric tracing. t r a c i n g .
0
/9 , . " , -
, , . \ :
~ - - . -.. ,~.
';';..
t ~ i i ,-
~ f l . .~
�9 . , : . ~ . . , - . - . - - f . . . . " "
:1 ; : . . '..
--.__....-..<
P r e t r e a t m e n t
P o s l t r e a t m e n t . . . . . . .
5 1 / 2 years Pos t t rea tmen t . . . . . . . . . . .
�9 �9 ! . ' r
, VV:T: . , " t .?', : , ! '6; '?. �9 \ / . . " �9 . ,.: ~; ~: \ ,
�9 . . ~ ~," I :. I "
- . , . . . . . . . . . -: . . . . . . ,~t .
Fig. 13. Pretreatment, posttreatment, recall cephalometric composite tracing.
Fig. 11. Recall casts.
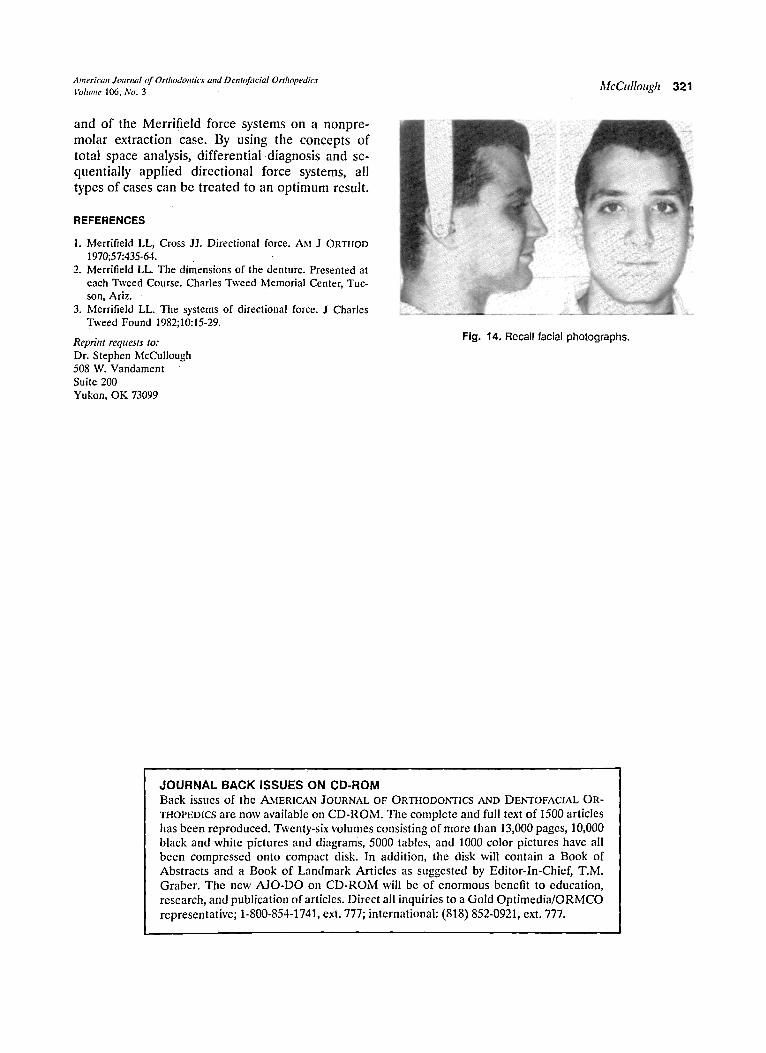
the flattening of the horizontal planes. The facial photographs (Fig. 14) exhibited the pleasing bal- ance and harmony of the face.
This case has been presented to illustrate the use of the Tweed-Merrifield diagnostic philosophy
American Journal o f Orthodontics and Dentofacial Orthopedics ~, . ~.. , . ~,lli#Cf'ltllOl'"ll 321 Volume 106, P,'o. 3
and o f the Mer r i f i e ld force systems on a nonp re - m o l a r ex t rac t ion case. By using the concep t s o f to ta l space analysis , d i f fe ren t i a l �9 and se- quen t i a l ly a p p l i e d d i rec t iona l force systems, all types o f cases can be t r e a t ed to an o p t i m u m resul t .
REFERENCES
1. Merrifield EL, Cross JJ. Directional force. AM J ORTIIOD 1970;57:435-64.
2. Merrifield LL. The dimensions of the denture. Presented at each Tweed Course. Charles Tweed Memorial Center, Tuc- son, Ariz.
3. Merrifield LL. The systems of directional force. J Charles Tweed Found 1982;10:15-29.
Reprint requests to: Dr. Stephen McCullough 508 W. Vandament Suite 200 Yukon, OK 73099
Fig. 14. Recall facial photographs.
JOURNAL BACK ISSUES ON CD-ROM Back issues of the AMERICAN JOURNAL OF ORTIIODONTICS AND DENTOFACIAL OR-
THOPEDICS are now available on CD-ROM. The complete and full text of 1500 articles has been reproduced. Twenty-six volumes consisting of more than 13,000 pages, 10,000 black and white pictures and diagrams, 5000 tables, and 1000 color pictures have all been compressed onto compact disk. In addition, the disk will contain a Book of Abstracts and a Book of Landmark Articles as suggested by Editor-In-Chief, T.M. Graber. The new AJO-DO on CD-ROM will be of enormous benefit to education, research, and publication of articles. Direct all inquiries to a Gold Optimedia/ORMCO representative; 1-800-854-1741, ext. 777; international: (818) 852-0921, ext. 777.