Embed Size (px)
Citation preview

A Periodical of the Pedorthic Association of Canada | FALL 2017
ANKLE SURGERY: ARTHROPLASTY VS. ARTHRODESIS 07
ASSESSMENT AND TREATMENT OF CHRONIC ANKLE INSTABILITY 09
PEDORTHIC INTERVENTION IN TRANSMETATARSAL AMPUTEE: CASE STUDY 15
INTERVIEW: HEPATHLETE NIKI OUDENAARDEN 18
Ankle Disorders

HOW DO YOU CALCULATE SUCCESS?
E D U C A T I O N
T A L E N T
H A R D W O R K
T H E R I G H T T O O L SA N D . . .
SOLVE THE EQUATION WITH AMFIT
[email protected] 800.356.FOOT
S E R V I N G F O O T S P E C I A L I S T S S I N C E 1 9 7 7

A Periodical of the Pedorthic Association of Canada - Fall 2017
3
President’s MessagePETER MORCOM C. Ped (C)
As we move out of a hot dry summer, where BC saw its worst forest fires in my history, for once I am looking forward to some rain. The Fall is here, and as clinicians we usually see some of our busiest times. Families are getting back into routines and are able to take care of some of those nagging injuries.
As our clinics ramp up, so does the work done by PAC and its many volunteers. In October we will be hosting our first European Study Tour. Through some hard work from our association management team, Strauss, C. Ped (C)s will get to experience how clinics function from our friends in The Netherlands and Germany. This is a great opportunity to see how pedorthic treatment is done in other countries and I expect some good stories from the trip.
We also see some of our own C. Ped (C)s sharing their knowledge, with Michael Ryan, C. Ped (C), Kelly Robb, C. Ped (C), and Brian Stoodley, C. Ped Tech (C), C. Ped (C) speaking in Cologne and Mac Graydon, C. Ped Tech (C), C. Ped (C) in Florida. It is great to see other nations wanting to learn from some of our pedorthists who are continuing research in our field. I feel it is very important to continue to research how to make our practices as clinically sound as possible, and to stay on the leading edge when it comes to technology.
The countdown to IVO 2018, taking place from April 12-14 in Toronto has begun. Working with our contacts in other countries, it is looking like we will have a good international group when we meet. I am looking forward to meeting people from many nations, including Australia, Germany and France, with hopefully many more. Ryan Robinson, C. Ped Tech (C), C. Ped (C) and Graham Archer, C. Ped Tech (C), C. Ped (C) have already booked speakers and I expect it to be the best Symposium yet.
I hope you all had a great summer and are ready to deliver some amazing experiences to your many patients throughout the Fall!
All articles published in Pedorthics Quarterly are the property of the Pedorthic Association of Canada. Copyright ©2017 Pedorthics Canada All rights reserved. Reproduction in whole or in part is permitted only with the prior written consent of the Pedorthic Association of Canada. Address all requests to the PAC office. Trademarks and Registered. Trademarks used in this publication are the property of their respective owners and are used only for the purpose of information.
Help us be green!If you would like to receive Pedorthics Quarterly electronically instead of the paper version, contact the PAC office at [email protected].
To those of you who are already receiving the online version, thank you for helping us be green!
Did you know you can read past issues of the Pedorthic Association of Canada quarterly publication online? Go to www.pedorthic.ca and log in to your member record.
PQ FeedbackWe would appreciate your feedback on the PQ and its articles. Your ideas and thoughts are important
to us. Let us know what you think.
E-mail your letter (referencing the article title and PQ edition) to: [email protected]. Please include ‘PQ
- Letter to the Editor’ in the subject line.
If you are interested in contributing articles for the PQ, contact [email protected].
Pedorthics QuarterlyA Periodical of the Pedorthic Association of Canada
Pedorthics Quarterly is published by:
Pedorthic Association of CanadaSuite 503 – 386 BroadwayWinnipeg, Manitoba R3C 3R6Toll Free: 1.888.268.4404 Email: [email protected]
Printed by Unigraphics
Communications Committee ChairKristin Ohm-Pedersen, C. Ped (C)
Committee Members Dana Hall, C. Ped (C)Arian Sasani, C. Ped (C)Steve Stredulinsky, C. Ped (C)Lisa Welsh, C. Ped (C)
Publisher Information
Subscriptions: $199 per year in Canada

4
PedorthicsQuarterly
A Medical Approach To Assessment And Treatment Of Ankle Osteoarthritis
IntroductionOsteoarthritis is the most common form of arthritis, and although most patients present with joint pain and functional limitations, the age of disease onset, the sequence of joint involvement, and disease progression can vary between individuals. (1) OA can range from asymptomatic, incidental finding on clinical and/or radiographic examination to a fast progressive disorder that can lead to “ joint failure”(1). Ankle Arthritis can be described by narrowing of the joint spaces, osteophytes, cartilage lesions and loose bodies (2). This condition can be debilitating especially in athletes (2). Repetitive stresses and twisting injuries in soccer players can often lead to “footballer ankle” with anterior and posterior bone spurs, fibrous tissue impingement, and ligamentous instability (2). Leonardo and colleagues suggest that
there is no consensus on the best management of this condition, however supramalleolar osteotomy, distraction arthroplasty, ankle arthrodesis and total ankle replacement have been successful treatments in patients with end-stage osteoarthritis. (2) This study also suggests that in the early stages of ankle osteoarthritis, in young patients, ankle arthroscopy can help improve function and symptoms and additionally, it can prevent and delay any major surgery. (2)
Clinical ManifestationsThe primary symptoms of OA are joint stiffness, pain and locomotor restriction (1). The following signs and symptoms can be seen in patients with OA:
Pain: Pain in OA can be worse with joint use and relieved by rest. It is often the most common symptom and can often progress through three stages:
• Stage 1: Predictable, sharp pain usually brought on by a mechanical insult that eventually limits high-impact activities with modest effect on function (1).
• Stage 2: Pain becomes more constant and starts to affect daily activities.There may be unpredictable episodes of stiffness (1).
• Stage 3: Constant dull/aching pain punctuated by episodes of often unpredictable, intense, exhausting pain which results in severe limitations in function (1).
Not all patients go through these specific stages ,and pain progression can be stopped at any stage (1). Pain can be worse in the morning soon after waking up, late afternoon and early evening (1). In severe OA, there may also be night pain, which can interfere with sleep (1).
Tenderness: Joint-line tenderness suggests articular pathology whereas tenderness away from the joint line suggests periarticular soft-tissue pathology.
Limitation Of Motion: Reduced range of motion (equal for active and passive movement), which results from marginal
osteophytes and capsular thickening, but synovial hyperplasia and effusion can also contribute to the limitation. (1)
Bony Swelling: Bony swelling reflects remodeling of the bone and cartilage on either side of the joint and marginal osteophytes. (1)
Joint Deformity: Deformity is a sign of advanced joint damage. (1)
DiagnosisThe diagnosis of OA is clinical based on symptoms and characteristic signs previously described. When the diagnosis is unclear and alternative diagnoses is needed, multiple imaging modalities can be used to assess presence and severity of OA.
Radiography: Conventional radiography is the most commonly used imaging modality in OA and can help in detecting characteristic features of OA which includes: marginal osteophytes, joint space narrowing, subchondral sclerosis and cysts (1). Radiographs can also be used to measure joint space narrowing, which can also be used to measure cartilage loss (1). Radiographic changes in OA are insensitive, especially in early disease and can often correlate poorly with symptoms (1).
Magnetic Resonance Imaging: MRI is not necessary for
DR. MEHRNOOSH SHAMSI
In over 70% of ankle OA, the etiology is a post-traumatic event such as ankle fracture, malleolus fracture, or ligament rupture.

A Periodical of the Pedorthic Association of Canada - Fall 2017
5
most patients with symptoms suggestive of OA and/or typical radiographic features. MRI can help identify OA at earlier stages of the disease, before radiographic changes become apparent (1). These changes can include cartilage defects and bone marrow lesions (1). MRI can also be helpful in assessing other joint pathology not shown by radiography such as effusions, synovium and ligaments (1).
Ultrasonography: Ultrasonography can identify OA- associated structural changes and can be helpful in detecting synovial inflammation, effusion, and osteophytosis (1). Some limitations of ultrasound are that it is operator-dependent, and cannot assess deeper articular structures and subchondral bone (1).
TreatmentPain can be effectively treated with medication (nonsteroidal anti-inflammatory drugs), which can possibly suppress secondary inflammation, which to some extent may delay destruction of articular cartilage (3). Some studies suggest the benefits of disease-modifying drugs (chondroprotective drugs) that have the potential to modify the function of chondrocytes, and hence the structure of the articular cartilage (3). No adequate long-term follow up studies have shown significant efficacy of these treatments (3).
A study by Osti and colleagues 2016 suggest that ankle arthroscopy and associated management of secondary injuries, when performed in selected patients with mild to moderate degenerative changes to the ankle, can provide high rates of
satisfaction and positive functional results (2). Selected groups of patients may benefit after ankle arthroscopy in terms of pain relief and functional improvement (2). Other complex and invasive procedures such as supramalleolar osteotomy, ankle arthrodesis, or joint arthroplasty can be delayed or avoided (2). The study also suggests that there is no consensus on post-operative rehabilitation, and how much time is needed to return to activity after ankle arthroscopy (2). In this study, patients returned to full weight-bearing 6- 8 weeks after the surgery to allow osteoblasts to form new woven bone. and chondroblasts to produce a matrix which contains type II collagen and proteoglycans, all forming fibrocartilaginous tissue (2). After this time, a hyaline- like cartilage with a high component of type II collagen can be detected (2). The osteochondral defects are filled with mostly hyaline- like tissue (2).
In over 70% of ankle OA, the etiology is a post- traumatic event such as ankle fracture, malleolus fracture, or ligament rupture (3).
A study by Valderrabano and colleagues 2007 suggest that the goal of orthopaedic end- stage ankle OA treatment is to relieve symptoms, such as pain and stiffness, and to improve function (3). Arthrodesis is effective in relieving pain, however it can restrict joint motion, which increases the risk of overloading adjacent or contralateral joints (3). Ankle arthrodesis, also known as ankle fusion, has been chosen to be the orthopaedic treatment for ankle OA (3). Total ankle replacement (TAR) was introduced due to complications in ankle arthrodesis, such as degeneration of neighboring hindfoot joints (3).
Another approach to treatment of ankle OA is joint distraction (4). This surgical technique is based on the hypothesis that OA cartilage has reparative activity (4). This activity can be effective when the damaged cartilage is mechanically unloaded, preventing further wear and tear, while the intermittent synovial fluid pressure (essential for nutrition of cartilage) is maintained (4). “The joint is distracted by means of an external fixation frame which eliminates mechanical contact between the degenerating articular surfaces (4).” Intermittent fluid pressure is maintained by the use of hinges in the distraction frame (4). Walking is allowed within a few days after surgical placement of the fixator (4).
REFERENCESDoherty, M., & Abhishek, A. (2017, January 31). Clinical manifestations and diagnosis of osteoarthritis. Retrieved from https://www.uptodate.com/contents/clinicalmanifestations-and-diagnosis-of-osteoarthritis?source=see_link
Osti, L., Del Buono, A., & Maffuli, N. (2016). Arthroscopic debridement of the ankle for mild to moderate osteoarthritis: a midterm follow-up study in former professional soccer players. Journal of Orthopaedic Surgery and Research, 11(37), 1-7. doi:10.1186/s13018-016-0368-z
Valderrabano, V., Nigg, B. M., Von Tscharner, V., Stefanyshyn, D. J., Goepfert, B., & Hintermann, B. (2007). Gait analysis in ankle osteoarthritis and total ankle replacement. Clinical Biomechanics, 22, 894-904.
Marijnissen, A. C., Roermund, P. M., Van Melkebeek, J., Schenk, W., Verbout, A. J., Bijlsma, J. W., & Lafeber, F. P. (2002). Clinical Benefit of Joint Distraction in the Treatment of Severe Osteoarthritis of the Ankle. Arthritis & Rheumatism, 46(11), 2893- 2902. doi:10.1002/art.10612
Figure 2. Ankle Distraction Surgery (Post-Op)
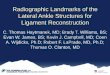
Figure 1. Ankle Arthrodesis

Apexfoot.com 800.252.2739
TM
Life IS BETTER ON APEX
Important Customer Enhancements!Shipping & duty now included in price. All returns to local CAN address.
091217_APEX- PAC Publication_Life is Better on Apex - Fall Ariya Boot.indd 1 9/14/2017 9:37:33 AM

A Periodical of the Pedorthic Association of Canada - Fall 2017
7
When shoe recommendations, custom orthotics, pain medication and physiotherapy leave a patient with pain, what’s next for the arthritic ankle? Total ankle arthroplasty (TAA, TAR, or more commonly known as ankle replacement) or ankle arthrodesis (commonly known as ankle fusion) offer the next course of treatment once conservative options have failed. Whenever surgery is indicated, notably with joint replacement, it’s up to the practitioners involved in the patient’s care to provide the most comprehensive, up-to-date advice so the client can make the best possible decision.
What Is A Total Ankle Replacement (TAA, TAR Or Athroplasty)?The first TAR procedures resulted in nearly 90% failure of components when performed in the 1970s (3). Currently available ankle replacement models result in much better results, and generally patients are satisfied when contacted years past their
surgery (3). Patients can now expect between 70-90% success rates with current methods (3).
Surgery is intensive, completed under anesthesia, and involves a lengthy post surgical rehabilitation process including “...gait training, proprioception exercises, gradual increase to
full weightbearing, local antiphlogistic therapy including lymph drainage, active and passive ankle mobility therapy, extension exercises, and therapy to strengthen the triceps surae muscle.” (3)
In terms of the actual procedure, most commonly an incision is made on the anterior aspect of the ankle, bone is cut to receive the new implant, and a multi-faceted surface articulation between tibia and talus allows range of motion once weight bearing. There are various implants available on the market, but most have metal anchoring pegs that are drilled into the end of the tibia and talus, with a polyethylene articulating surface replicating the hinge motion of the joint (4).
What is Ankle Arthrodesis (Ankle Fusion)?In this surgical procedure, the tibia and talus are fused together. Under anesthesia, cartilage is removed and surgical hardware fuses bone to bone in the most anatomically efficient position (1). Autologous bone grafts (harvested from the patients own bone) are commonly applied around the fusion site to increase strength of the fusion and promote healing of the surgical site (6). Most modern ankle arthrodesis procedures are now conducted arthroscopically, which minimizes time spent in hospital (5). Whether performed arthroscopically or via an open incision, overall outcomes are similar, but patient reports at one to two years post-surgery tend to be better with arthroscopic procedures (5).
Post surgery, the patient will not be able to dorsiflex or plantarflex their ankle. Considering the primary actions of the ankle joint, this up and down motion is generally what contributes to the pain of an arthritic ankle. By fusing the bones and removing this range of motion, theoretically, pain should be relieved. In the arthritic ankle, moving through the remaining range of motion is not beneficial, thus fusion can be a practical choice.
Who Should Consider TAR Or Arthrodesis?It is estimated that only 1% of the population suffers from severe ankle osteoarthritis or degeneration caused by previous
traumatic injury or the aging process (3). Unfortunately, this means that research and advancement of surgical methods regarding this relatively rare condition suffer. Regardless, those patients who have tried other conservative methods may need to consider the ‘last resort’ of surgery. As we know,
osteoarthritis cannot be reversed, but for those patients who can manage their ankle symptoms with alternative treatments, surgery should not be considered.
There are many factors that come into play when deciding on the appropriate course of treatment. Of paramount importance are:
• The patient’s foot and leg shape (congenital or acquired deformity, genu valgum/varum, pes planus/cavus, etc.)
• Biomechanics of the foot and entire lower extremity
• Activity level (sedentary vs. active, high impact sports vs. low to medium impact)
• Overall height and weight (BMI, obesity, etc.)
• Complicating medical conditions (heart disease, diabetes, circulatory issues, etc.)
Ankle Surgery: Arthroplasty vs. ArthrodesisDANA HALL C. Ped (C)

8
PedorthicsQuarterly
Those with normal mechanics, neutral foot and leg shape, normal BMI, and who do not engage in contact or high impact sport tend to have better outcomes with either type of surgery (3).
Which Is A Better Option?Total ankle replacement is a relatively new surgery that has become more common over the past decade, while ankle fusion has been the gold standard surgery for ankle degeneration for a much longer time period. Because of the relative rarity of the arthroplasty procedure and the lack of significant development in technology, many surgeons are reluctant to perform or suggest this type of surgery. It is also quite technically demanding with a steep learning curve, thus other options may be suggested and patients may have difficulty finding a surgeon willing to perform it (3).
Furthermore, when compared to total knee replacement (TKR) and total hip replacement (THR), ankle replacement revisions after 10 year follow-up are performed in 33 out of every 100 patients versus 13 out of 100 revisions for TKR and THR, making this one of the most revised joint procedures available (3). Further long term study is required in order to track the success of TAR over the course of 20 years or more. While current hardware is among the most durable and has improved, one study from 2010 revealed that one in five TAR surgeries failed within five years (2). Failure rates, revisions, or repairs do increase as time goes by: up to 90% of patient-reported success rates can be noted at five-year followups, dropping to 80% success at eight years post-operation (4).
One of the significant advantages of TAR versus ankle fusion is that the patient usually regains a modest range of motion post surgery: 25-30 degrees of ankle dorsiflexion and plantarflexion is
considered average, with up to 60 degrees of range reported in some highly successful patients (3). This can allow the patient to regain a more natural gait pattern once recovered from surgery.
The main disadvantages of ankle fusion is that due to the fact that the ankle joint will not move post surgery, the patient will likely have gait abnormalities. These discrepancies force the patient to learn a new pattern of movement which can put stress on other joints in the foot that have retained their normal range of motion.
Thus, there is no correct answer for every patient considering arthroplasty versus arthrodesis. For a sedentary individual with high BMI and unique leg shape, arthrodesis may be the best choice. For the younger athlete willing to give up on contact sports who has a very average leg shape, arthroplasty may be the best choice. Taking into account the patient’s age, level of severity of degeneration, activity level and lifestyle are also critical in making a decision between the two options, and to date there is a distinct lack of comparison studies between arthroplasty and arthrodesis (3). There is a tendency for patients to have more complications due to the more involved surgery involved with arthroplasty versus arthrodesis but, again, further study and advancement of techniques is warranted (3).
ConclusionNeither arthroplasty or arthrodesis are procedures that should be considered a first line treatment for ankle osteoarthritis. If surgery is considered the next step, careful consideration of the patient’s lifestyle and goals must be first and foremost when deciding between the two options. Both have their drawbacks and advantages, so educating the patient in order to make the best decision is paramount.
REFERENCES1. American Orthopedic Foot and Ankle Society (2017). Ankle
Arthrodesis. Retrieved from http://www.aofas.org/footcaremd/treatments/Pages/Ankle-Arthrodesis.aspx
2. Fillon, M. (2017). Ankle Surgery: Bone Fusion vs. Joint Replacement. Retrieved from http://www.arthritis.org/living-with-arthritis/treatments/joint-surgery/types/other/bone-fusion-joint-replacement-surgery.php
3. Barg, A., Wimmer, M. D., Wiewiorski, M., Wirtz, D. C., Pagenstert, G. I., & Valderrabano, V. (2015). Total Ankle Replacement: Indications, Implant Designs, and Results. Deutsches Ärzteblatt International, 112(11), 177–184. http://doi.org/10.3238/arztebl.2015.0177
4. Total Ankle Institute (2017). INBONE Total Ankle System. Retrieved from https://www.ortho.wustl.edu/content/Education/2915/Patient-Education/Educational-Materials/Total-Ankle-Replacements-FAQs.aspx
5. Townsend, D. Et al (2013). Arthroscopic Versus Open Ankle Arthrodesis: a Multicentre Comparative Case Study. Journal of Foot and Ankle Surgery, 95(2), 98-102.
6. DiGiovanni, C. Et al. (2016). The Importance of Sufficient Graft Materal in Achieving Foot or Ankle Fusion. Journal of Bone and Joint Surgery, 98(15), 1260-1267.
One of the significant advantages of TAR versus ankle fusion is that the patient usually regains a modest range of motion post surgery.

A Periodical of the Pedorthic Association of Canada - Fall 2017
9
Chronic ankle instabilities in athletes result from repeated trauma to the ligaments of the lower leg and foot. When dealing with athletes, most will complain that their ankle “gives out” or “keeps rolling”. The first part of the assessment is to take a detailed history that includes mechanism of injury, pain location, activity level and sport, etc. to try to get a better understanding of what the athlete may be doing to cause the injury.
The next step in the assessment is the observation component. This part of the assessment is where I get my first look at the ankle for swelling, deformities, and anything else that may influence the physical assessment. From there the physical assessment begins by going through active, passive and resisted ranges of motion. Completing the three types of range of motion will greatly narrow down the suspected injury site. Pain during active motion could mean that the injured structure is bone, ligament or muscle. Pain during passive motion would narrow the impacted structure to bone or ligament because the muscle is not activated. Pain during resisted motion would be a strong
indicator of muscle or bone injury, but would exclude ligament because the joints do not move in resisted motion. Paying close attention to ranges of motion will narrow the diagnosis greatly.
The final step to the assessment is to complete special tests and palpation of the entire area. Completing special tests is meant to give confirmation of previous suspicions throughout the assessment. There is only a need to test the structures that you believe may be injured. Palpation can be an essential aspect to any assessment. With some assessments you can have false positives throughout which can change the diagnosis. Palpation is the one part of the assessment that is able to confirm the diagnosis in an ankle assessment. The anatomy at the ankle is easy to palpate in comparison to other joints in the body, making it a reliable source to give a diagnosis.
Reaching a correct diagnosis is important, however creating an effective treatment plan is crucial to correct it. As an athletic therapist, we’re trained to effectively treat musculoskeletal issues while focusing on thirteen key rehabilitation principles. These include: decreasing pain, swelling and inflammation; increasing
Assessment And Treatment Of Chronic Ankle InstabilityMATTHEW DE GOOIJER CAT(C)
PARISORTHOTICS.COM
1.800.848.0838
NON-OPERATIVE TREATMENT OPTION FOR
CHRONIC CONDITIONS OF THE FOOT & ANKLE
CLINICAL INDICATIONS
• Adult Acquired Flatfoot (PTTD)• Lateral Ankle Instability• Charcot Deformity• DJD of the Ankle or Subtalar Joint• Mild Drop Foot Deformity
A CUSTOM ARTICULATED Ankle Foot Orthoses (AFO)

10
PedorthicsQuarterly
range of motion; increasing muscular strength, power and endurance; maintenance of cardiovascular fitness; re-establish neuromuscular control; improve stability and balance; addressing psychological factors to injury; posture and core stability; protect and prevent from further injury; focusing on kinetic chain/ joint above and below; sport specific adaptations; return to sport and activity considerations, and finally the development of a home program. For this article I’ll go through each rehabilitation goal and give a short description.
Reducing pain, swelling and inflammation: Let the heat versus ice debate begin. Personally I still prefer to use ice for pain and swelling; I’ve found it to still carry the best results and increases patient comfort. When an injury reaches the chronic stages, typically a patient has tried everything under the sun to help; therefore at this stage I will sometimes tell the patient that if they have more success with one thing over another; then stick with it. A lot of practitioners will use TENS and IFC to control for pain during a treatment. Although they can be effective in increasing patient comfort; for chronic ankle instability they just mask the problem and in my opinion are not an effective use of the patient’s time. Keeping this in mind, everything has a time and place.
Increasing range of motion: This goal of rehabilitation wouldn’t be emphasized because we’re dealing with instability; however during the assessment it is important to check the range of motion through the foot and knee. If there are restrictions in the foot and knee range of motion, this could be causing the ankle to compensate for the lack of range of motion elsewhere.
Increasing muscular strength: This is the meat and potatoes of treating chronic ankle instability. Typically the ligaments in the ankle have a greater amount of laxity from previous injuries; therefore a typical treatment plan involves strengthening all muscles involved at the ankle to improve stability. Two incredibly important muscles to focus on are the peroneals, as well as tibialis posterior. These two groups of muscles are directly responsible for controlling inversion and eversion at the ankle. Typically, you’ll find a weakness in one of these that can directly lead to the instability. Strengthening these will have the greatest impact at the joint.
Maintenance of cardio: Many times following an injury, individuals and athletes will “take time off” to heal. This typically involves greatly reducing or eliminating cardiorespiratory fitness while they recover. Cardio should never be stopped completely, especially to ensure a smooth transition back to full activity for athletes. For ankle instabilities I prefer cycling; as a therapist you’re able to control the training environment more effectively.
Neuromuscular control and balance: This is another very important aspect to chronic ankle instability. Being able to adapt to surface changes or the changes associated within a sport are critical to avoid re-injury. I always have my athletes train balance last in every rehabilitation plan. I do this so that they train and focus the neuromuscular component when they are tired. You can do this by using unstable surfaces in a controlled environment. Training balance and neuromuscular control at the end of a rehabilitation plan will attempt to simulate the later stages of an athlete’s activity. This will help to reduce re-injury by improving stability when an athlete is exhausted, and will help to avoid poor technique or a misstep late in a game.
Psychological factors: This goal is accomplished during rehab by simply talking with your athlete about concerns they may have. Sometimes it can take time address psychological implications of injury, while other athletes have no response whatsoever and hardly seem phased by the fact they’re injured. It is always beneficial to have the athlete complete their rehab at their training facility or near their teammates. It makes them feel that they are still part of the team even though they’re on the sidelines, and can act as a motivator to keep them compliant with rehab.
Posture and core stability: For chronic ankle instability this goal would not be the most necessary, however as a therapist it is always good to look at other areas to prevent injury. A strong core and good posture will always help to reduce other injuries.
Protect and prevent further injury: The athlete will have two choices for this goal. The first is that they can choose to brace the ankle. Most ankle braces are all very similar and usually have more bulk than the second option. The second option is to tape the ankle for practices or competition. A properly done ankle taping can be more comfortable, will provide equal or stronger
An injury at the ankle rarely impacts one joint.

A Periodical of the Pedorthic Association of Canada - Fall 2017
11
protection and will have less bulk than a brace. The downside to taping is that it can be costly over time, and in some cases, you may need a trained individual there to help with taping.
Kinetic chain: An injury at the ankle rarely impacts just one joint. In this case, it’s important to look at what is happening in the foot as well as the knee. It’s always good to keep in mind that chronic ankle instability will impact knee and hip movements. As an
athletic therapist I always look to incorporate exercises that cross multiple joints.
Sport specific adaptations: This aspect of a rehabilitation plan is by far the most fun. It’s a chance to get very creative and put together exercises that best reflects the athletes sport. An example for a football running back would be to have them make lateral cuts through cones. Creating a sport specific plan helps to engage the athlete more and keep them interested in the rehab.
Home program: Most active clientele and athletes have a personal or public gym space that they like to use; which makes the development of a rehabilitation exercise plan far easier (more options available). However, each exercise should be able to be adapted for a home program setup. Being resourceful with at-home objects for adapting exercises is very important to creating an effective at-home program.
In closing, there are a multitude of ways to treat chronic ankle instability. I did not include any specific exercises because there are a wide variety of options for each stage of the rehabilitation process. There is not a gold template on rehab. It’s important to remember the 13 goals of rehab; however the biggest focus for myself when treating chronic ankle instability would be improving strength, balance and muscular control. As an athletic therapist, I love having the ability to take an athlete through the entire rehab process; from seeing the initial injury occur, to clinical treatments, to return to play testing.
Strengthening (the peroneals as well as the posterior tibialis) will have the greatest impact at the joint.
buy cheap or buy smart
w w w . r e n i a . c o m · i n f o @ r e n i a . c o m
a s k y o u r l o c a l d e a l e r
vkb-werbung.de
H i g h T e c h A d h e s i v e s f o r P r o f e s s i o n a l s
Anz Erdbeere 215,9x139,7 USA:12 15.06.2012 8:42 Uhr Seite 1

12
PedorthicsQuarterly
Adult acquired flat foot (AAFF) describes a progressive flattening of the medial longitudinal arch resulting in pain and decreased function of the affected foot. The deformity is characterized by valgus hindfoot alignment, forefoot abduction and excessive medial longitudinal arch collapse. There are three main causes of AAFF including neuropathic changes, degenerative changes and the loss of supporting structures (1) .The most common form of the deformity is often a result of the deficiency in the supporting structures of the medial longitudinal arch, in particular the posterior tibialis tendon. Posterior tibialis tendon dysfunction (PTTD) is commonly seen in women above the age of 40 years old and is likely caused by a lifelong mechanical strain of the tendon. Risk factors such as pes planus, hypertension, diabetes mellitus, steroid injection around the tendon, and seronegative arthropathies are thought to contribute to chronic micro trauma leading to tendon degeneration (2). The initial signs and symptoms include pain and swelling of the medial ankle, which makes it commonly misdiagnosed as an ankle sprain or arthritic pain. It is speculated that by the time most patients present symptoms to a foot and ankle specialist, they have had the condition for several years and have consulted numerous doctors (1).
The posterior tibialis originates from the interosseus membrane of the tibia and fibula, passing behind the medial malleolus and inserts onto the navicular and the bottom of the midtarsus. It functions to invert the foot and facilitates plantar flexion, which makes it an important stabilizer of the medial longitudinal arch during gait. The action of the muscle aids in resupination of the foot by raising the medial longitudinal arch and locking the hindfoot (2,4). This allows the gastrocnemius to be more effective in plantar flexion and allows an efficient transition from midstance to toe off. The diminished action of the posterior tibialis muscle results in increased stress on the plantar ligamentous support of the longitudinal arch and in advanced stages, the characteristic features of the pes planus deformity seen in adult acquired flat foot (3,4).
The signs and symptoms indicative of PTTD are pain and swelling along the medial foot and ankle, difficulty walking and standing for long periods, and changes to the foot’s appearance as the dysfunction advances. Early recognition is an important part in preventing adult acquired flat foot and the rehabilitation
of the posterior tibialis tendon. A useful indicative test is the single heel raise, it is used to assess the ability of the tibialis posterior muscle to invert the hindfoot. The patient is asked to stand near a wall and balance on the affected foot, next he or she is asked to raise the affected heel by rolling forward onto the ball of the foot. The inability to complete the task or absence of hindfoot inversion signifies dysfunction of the tibialis posterior tendon. A normal single heel raise may elicit pain along the medial ankle in a patient with PTTD. Alternatively, the posterior tibialis muscle can be assessed with a first metatarsal rise test. The patient should stand full weight bearing as the affected limb is passively moved into a varus position, if the first metatarsal rises, this indicates dysfunction of the posterior tibialis tendon. The rise in the first metatarsal is caused by the flattening of the medial longitudinal arch, causing the stretching and fatigue of the plantar medial ligaments, allowing the gastrocnemius-soleus complex to act at the level of the first metatarsal head and cause dorsiflexion (2,3). The strength and ability to invert the foot should also be assessed bilaterally to compare and determine if a dysfunction exists. As the condition progresses, there is often a fixed valgus deformity of the hindfoot resulting in reduced range of motion of the subtalar joint and impingement of the sinus tarsi producing lateral ankle pain.
The presentation of PTTD can be categorized into three clinical stages, which were first described by Kenneth A. Johnson and David E. Strom in 1989 (4). Stage I is characterized by pain and swelling of the medial ankle that increases with activity. The tendon is intact and functional, producing a normal heel raise. In stage II of PTTD, the patient’s foot will begin to flatten causing a flexible pes planus structure characterized by valgus hindfoot alignment, forefoot abduction and excessive medial arch collapse. A single heel raise and first metatarsal rise tests are positive, suggesting the tendon is ruptured and functionally incompetent (1,2). The third stage is characterized by advanced degeneration and a fixed valgus deformity of the hindfoot.
Posterior Tibialis Tendon Dysfunction: Understanding Adult Acquired Flat FootWINNIE LAW C. Ped (C)
Stage I Stage II Stage III Stage IV
Medial pain
Swelling
Tendon is inflamed
Mild weakness
Medial pain and swelling
Tendon is elongated
Marked weakness
Flexible deformity
Medial and lateral pain
Marked weakness
Fixed deformity
Degeneration of subtalar joint
Medial and lateral pain
Marked weakness
Fixed deformity
Degeneration of subtalar joint

A Periodical of the Pedorthic Association of Canada - Fall 2017
13
There is also the onset of degenerative changes of the subtalar joint contributing to a loss of normal range of motion. The pain and swelling initially experienced along the medial ankle often diminishes as pain begins on the lateral column because of impingement of the fibula onto the sinus tarsi. In the fourth stage
later described in depth by Myerson, the fixed valgus position of the hindfoot causes a lateral tilt in the talocrual joint. Myerson also described insufficiency of the deltoid ligament as a result of the valgus positioning of the hindfoot and further subdivided stage IV into a flexible and fixed deformity (1,4).
Posterior tibialis tendon dysfunction can be successfully managed and treated when it is detected early, but may require more invasive, surgical action when the deformity becomes fixed. The goals of treatment include reducing clinical symptoms, improving hindfoot alignment and preventing the progression of the deformity (1,2). It is ideal to manage the inflammation in the early stages of PTTD by rest, ice, compression and elevation (RICE), and/or four-to-eight weeks of immobilization in a removable walker boot (1,3). Other conservative forms of treatment include non-steroidal anti-inflammatory drugs (NSAIDs), footwear, off the shelf insoles, custom foot orthotics and ankle foot orthoses. The goal of treatment is focused on reducing the valgus alignment of the hindfoot and restoring the function of the posterior tibialis tendon. Supportive footwear should be a focus for patients. Deep structured shoes with a strong heel counter will not only improve comfort, but will also allow better compliance with orthotics. Compliance with footwear is often difficult but the importance should be emphasized as an integral part of a success treatment plan. When the deformity is flexible, orthotics are used to reduce the pes planus features of the foot, alternatively when the deformity becomes fixed the goal of the orthotics will be mainly for accommodation. The use of custom and off-the-shelf bracing is also an effective tool in controlling PTTD by stabilizing the ankle and improving gait mechanics. Physiotherapy for rehabilitation of the tendon and muscle is also important in the early stages and should be
recommended. Surgical treatments need to be considered when improvement is not seen with any of the conservative methods. A soft tissue procedure such as a tenosynovectomy or tendon transfers from the flexor digitorium longus or anterior tibialis are effective for the flexible acquired flat foot but will not improve a fixed deformity (1,2,3). The degeneration seen in the subtalar and talocrual joint in the late stages of PTTD should be treated by arthrodesis and then managed by the continuation of supportive footwear and orthotics (1,4).
Posterior tibialis tendon dysfunction is a common condition that is easily managed and treated to prevent an adult acquired flat foot only when detected early. The gradual loss in the ability of the posterior tibialis to be a dynamic stabilizer in gait results in the progressive flattening of the medial longitudinal arch and valgus hindfoot seen in adult acquired flat foot. Patient education and conservative treatment are effective tools in the early stages of PTTD, but surgical treatment is necessary once the flat foot deformity is established.
REFERENCES1. Kohls-Gatzoulis J, Angel J.C, Singh D, Haddad F, Livingstone J, Berry
G. Tibialis posterior dysfunction: a common and treatable cause of adult acquired flatfoot. BMJ. 2004; 329: 1328-1333
2. Woll T. Scott MD. Posterior Tibial Tendon Dysfunction. WJM. 1993; 159: 485-486
3. Geideman W, Johnson J. Posterior Tibial Tendon Dysfunction. Journal of Orthopaedic & Sports Physical Therarpy. 2000; 30(2): 68-77
4. Abousayad M, Tartaglione J, Rosenbaum A, Dipreta J. Classifications in Brief: Johnson and Strom Classification of Adult-acquired Flatfoot Deformity. Clin Orthop Relat Res. 2016 Feb; 474(2): 588-593 doi: 10.1007/s11999-015-4581-6
It is speculated that by the time most patients present symptoms to a foot and ankle specialist, they have had the condition for several years and consulted numerous doctors.
- Christy Shantz, Owner & Certified Pedorthist

April 12 - 14, 2018 | 12 - 14 avril 2018 | 12. - 14. April 2018
Toronto, Canada
More than 500 Pedorthists, Orthopedic Shoemakers, Orthotists, Podiatrists, Chiropodist, Biomechanists and others concerned with lower extremity therapy will gather in Toronto, Canada on April 12 - 14, 2018.
The IVO World Congress is an international educational event known for bringing together some of the best keynote, plenary and workshop speakers from around the world.
The IVO serves to promote international cooperation in the �eld of pedorthics and orthopedic shoe technology.
The goal is for member countries to align in the �eld of education and training and grow the profession’s pro�le.
www.IVO2018.com
*The IVO World Congress will replace the PAC Symposium in 2018
The Pedorthic Association of Canada (PAC) is hosting
The IVO World Congress 2018

A Periodical of the Pedorthic Association of Canada - Fall 2017
15
April 12 - 14, 2018 | 12 - 14 avril 2018 | 12. - 14. April 2018
Toronto, Canada
More than 500 Pedorthists, Orthopedic Shoemakers, Orthotists, Podiatrists, Chiropodist, Biomechanists and others concerned with lower extremity therapy will gather in Toronto, Canada on April 12 - 14, 2018.
The IVO World Congress is an international educational event known for bringing together some of the best keynote, plenary and workshop speakers from around the world.
The IVO serves to promote international cooperation in the �eld of pedorthics and orthopedic shoe technology.
The goal is for member countries to align in the �eld of education and training and grow the profession’s pro�le.
www.IVO2018.com
*The IVO World Congress will replace the PAC Symposium in 2018
The Pedorthic Association of Canada (PAC) is hosting
The IVO World Congress 2018
This case study is based on a 71 year-old male who was diagnosed with Type 2 Diabetes from the age of 50, and a history of plantar foot ulcers, peripheral neuropathy, and peripheral arterial disease. He has high-risk diabetic feet and has undergone a transmetatarsal amputation on his right foot. His doctor has referred him to see a pedorthist to be assessed, and appropriately fitted with orthotics and shoes to restore functional gait and mobility.
Type 2 Diabetes is defined as a disease in which your pancreas does not produce enough insulin, or your body does not properly use the insulin it makes. As a result, glucose builds up in your blood instead of being used for energy. Diabetes can cause nerve damage (diabetes peripheral neuropathy) and poor blood flow or circulation to the legs and feet (peripheral arterial disease). As a result, people with diabetes are less likely
to feel a foot injury, such as a blister or cut. Diabetes can make these injuries more difficult to heal. Unnoticed and untreated, even small foot injuries can quickly become infected, potentially leading to serious complications (1).
As pedorthists we have seen many patients who suffer from Type 2 Diabetes, as it affects 6.9% of all Canadians ages 12 years and older, with 15-25% of that population being diagnosed with a foot ulceration (2).
Diabetic patients are four times more likely to have an amputation than those without the disease, with the rate rapidly increasing after the age of 40, in parallel with the increasing incidence of diabetes.
Our primarily concerns when treating patients of this sort are: possibility of skin breakdown, increased risk of further amputation, new wounds to the feet, instability in weight bearing activities, impaired pronation and supination during gait, and loss of active push-off during gait.
Most diabetic patients suffer from sensory neuropathy and lower extremity ischemia. Sensory neuropathy is a critical risk factor for
patients experiencing unnoticed, repeated trauma during walking that can lead to skin breakdown (3).
A study done by Dillon et al., (5) found that when treating a patient with transmetatarsal amputation, the treatment plan must incorporate each of the following to restore the effective foot length, a stiff forefoot, an anterior leg shell, and restrained dorsiflexion. When such a device was provided to the persons with transmetatarsal amputations, they found not only restoration of the effective foot length but also less exaggerated dorsiflexion, reduced loading on the sound limb during initial contact, and normalization of the ankle and knee moments during late stance as the device compensated for the limited contribution of the ankle plantar flexors.
Our treatment plan will include custom made foot orthotics, an ankle foot orthoses (AFO) and orthopaedic footwear.
When creating custom foot orthothics, we must address areas of high plantar and shear pressure that can lead to diabetic skin uclerations, and restore pressure distribution between the foot orthotics and the foot (6).
Pedorthic Intervention In Transmetatarsal Amputee: Case Study ISH SEHMBEY C. Ped (C) Diabetic patients
are four times more likely to have an amputation than those without the disease.

www.simsmedicalcorp.com1-888-655-4499

A Periodical of the Pedorthic Association of Canada - Fall 2017
17
The patient is casted using an impression foam box in semi-weight bearing. The orthotics are constructed using Tri-Lam, which is layers of Plastazote and PPT for more of an accommodative device, that is leveled using 65 durometer EVA, so when the patient stands on the orthotics, the entire plantar surface of the foot is distributing weight evenly and equalizing plantar pressures. Next, you post the anterior aspect of the orthotic to restore the calcaneal angle to neutral (40 degrees) and accommodate any leg length discrepancy if needed by posting on the posterior plantar aspect of the orthotic.
We now create a partial foot filler, to maintain the foot’s position in the shoe and preserve the residual foot from friction, pressure and shearing forces. Multiple layers of 6mm 55 durometer cork was used to shape and match the length, width and sagittal plane profile of the contralateral foot and fit the footwear.
The AFO would help restore gait and the lost lever arm function. There are a number of prefabricated AFO’s that can help our patient, however, given the patients weight scenario of over 300 pounds we have chosen the Allard BlueROCKER carbon fiber AFO because it is lightweight, low profile and strong enough to accommodate the patient’s weight.
A full plate dynamic carbon AFO like the Allard BlueROCKER will restore the lever arm to counteract the plantarflexion moment from the posterior muscle group. Ideally, a carbon-fiber foot plate that is more stable at the midfoot with the dynamic tapering down toward the toe will direct the forces toward the break in the shoe. Some of that force can be transferred via a strut to the anterior tibia and then be reflected back during the propulsive gait phase. A lateral strut was used as opposed to a medial strut, because, during initial contact phase of the gait, the subtalar joint pronates therefore not applying pressure into the strut.
An anterior shell is more suitable to a posterior shell due to the shearing forces occurring during gait in the third rocker, and the strut allows an energy transfer and transmits those forces to the anterior shell. Also, the anterior shell comes up to the tibial
tubercle height, and that will optimize the AFO’s lever arm function and distribute those forces over as wide an area as possible (4).
Fitting the client with the appropriate footwear is also important, because we would like to reduce peak plantar pressure on the distal residual and forefoot of the contralateral extermity. A study by Mueller et al., found that a rigid rocker soled footwear
in conjunction with a total contact orthotic is the most effective footwear combination to reduce pressure.
A rocker sole serves to rock the foot from heel strike to toe-off without bending the foot or shoe. The sole of the shoe is modified to resemble the base of a rocking chair. The basic biomechanical effects of rocker soles are the restoration of lost motion in the
foot and ankle due to pain, deformity, stiffness or fusion, resulting in an overall improvement in gait and offloading plantar pressure on some part of the foot. The rocker sole is the most effective way to offload the forefoot. The rocker sole is also a logical method by which the centre of pressure can be progressed anteriorly past the distal end of the residual foot in a partial foot amputee. (7)
Our client was fitted with a Brooks Addiction Walker shoe, as it accommodates the width and depth of his foot. The shoe has a stiff forefoot rocker, and wide base to provide stability during gait.
There are many treatment plans that can be effective in treating a patient with a transmetatarsal amputation. Consideration must be made to the level of amputation and realistic expectations when developing a treatment plan in order to maintain the highest level of function. Ultimately as a pedorthist, our goal is to maintain weight bearing and reduce force loading along the residual foot in order to reduce further skin breakdown and subsequent limb loss.
REFERENCES1. Living with Type 2 Diabetes. (2016). Retrieved from http://www.
diabetes.ca/diabetes-and-you/living-with-type-2-diabetes
2. Health Fact Sheets Diabetes, 2015. (2015). Retrieved from http://www.statcan.gc.ca/pub/82-625-x/2017001/article/14763-eng.htm
3. Mueller, M. J., Strube, M. J., & Allen, B.T. (1997). Therapeutic Footwear Can Reduce Plantar Pressures in Patients With Diabetes and Transmetatarsal Amputation. Diabetes Care. 20(4), 637-641.
4. Kennedy, S., & Meier, R. (2011, January) A Dynamic Approach To Managing Partial Foot Amputees. Retrieved from https://opedge.com/Articles/ViewArticle/2011-01_06.
5. Dillon, M. P., Fatone, S., & Hansen, A. H. (2011). Effect of Prosthetic Design on Center of Pressure Excursion in Partial Foot Prostheses. Journal of Rehabilitation Research and Development. 48(2), 161-178.
6. Forefoot, Toe Amputations and Prostheses: The Quest to Restore Normal Ambulation. (2003). Retrieved from https://www.healio.com/orthotics-prosthetics/pedorthics/news/online/%7Be3bd783a-0d3d-4edb-bd57-99e236aac395%7D/forefoot-toe-amputations-and-prostheses-the-quest-to-restore-normal-ambulation
7. Janisse, E., & Janisse, D. (2010, November). Partial Foot Amputation Pedorthic Management. Retrieved from http://lermagazine.com/article/partial-foot-amputation-pedorthic-management

18
PedorthicsQuarterly
Niki Oudenaarden is one of Canada’s top up-and-coming Heptathlete’s. She has had a difficult road to becoming the best female multi-sport athlete. In her recent win at the Canadian Track and Field Championships, she hit the magical 6,000 point mark for the first time (points are awarded in multi-sport events based on a mathematical equation, deriving from a standard performance benchmark. Each event has a minimum and maximum amount of points able to be awarded). Having competed nationally and internationally for Canada for some time now, including at both youth and senior levels, Niki discusses her road to recovery and where she believes she can go next.
To start off with, how long have you been competing in the Heptathlon?
I have competed in track and field for 13 years, and the Heptathlon for seven years.
With it being based on different events, do you have a favourite event?
Favourite events change depending on which is most successful usually. But I’ve always loved the long jump, throwing the javelin and high jump the most.
Did you compete in any other sports previously?
I used to compete in volleyball and basketball all through junior high and high school. I competed in these sports alongside track and field.
Can you tell me a little bit about your first injury and subsequent rehab/surgery?
My first injury was rolling my ankles. I rolled both my ankles a minimum of four times each, in junior high and high school. This
took me away from training for track and field (my favourite sport). Then my first severe injury resulting in surgery was my knee. I had grade three chondromalacia. That was my first surgery. It took 6 months of rehabilitation to be running
comfortably again, without agitation. That happened during my first year of university in San Diego.
Unfortunately you had a second, severe injury. Can you tell me a bit about that injury and the subsequent surgery and rehabilitation?
My next surgery was just short of a year after my first. I had severe Morton’s neuroma. The nerve in my foot was calloused over, with fibrous tissue, and every time it was touched or pressed on it would shock my foot. This was not a comfortable thing for a runner. Before the surgery I had 3 cortisone injections, each 2.5 months apart from each other starting in January. Since that didn’t offer relief I had surgery following NCAA’s. That surgery took me only 3 months to fully recover.
But with these two surgeries and constant alterations in my gait and strength of my body, I was constantly in severe pain
Interview: Heptathlete Niki Oudenaarden STEVE STREDULINSKY C. Ped (C)
(My third surgery) was an ankle reconstruction on the lateral aspect.

A Periodical of the Pedorthic Association of Canada - Fall 2017
19
and discomfort. Even with rehabilitation exercises daily for an additional two-plus hours with my training, I noticed I was suffering from chronic pain all the time.
Finally, I left the NCAA system and moved to Calgary to be coached under Les Gramantik. He tried his best to help me recover and compete my first year in Canada, but both of us knew I needed another surgery to clean things up again. So once again, after Nationals and my FISU appearance, I went under the knife again, for my third surgery.
This was an ankle reconstruction on the lateral aspect. At first I was optimistic about this surgery and my recovery time. But as time wore on and the pain in my ankle didn’t subside and the strength was slow to return, I was disheartened. Honestly at that time I thought I was going to retire from track and field.
After a complete year of rehab exercises, physio, treatments and adjusted training, I began to feel relief.
How did it feel to return to competition after that time away?
It felt amazing! Now I am experiencing the best season so far of my career. My ankle is now stronger than it ever was before. Of course there are aches and pains here and there, but I believe it has been healed and I am on track (literally) for my return emergence into the athletics world.
Recently, two of Canada’s most decorated athletes retired, and both happened to be Heptathletes. Jessica Zelinka and Brianne Theisen-Eaton were constantly battling for 1st and 2nd place in the National Rankings, and battling to represent Canada internationally. With Zelinka and Thiessen-Eaton retiring, the door has opened a bit for female heptathlon. Do you feel more motivated? More stressed to perform?
Of course, I feel more motivated now that these two fantastic Heptathlete’s have retired. But I truly loved learning from them and watching them perform. I wish I had the opportunity to
compete against them simply because as an athlete you want to compete against the best. Winning is necessary for your mental development, but competing against someone better than you forces you to push and fight for every point. The only stress I can carry on myself is my expectation to perform. Otherwise it doesn’t matter what others think. I was told by numerous people to quit and walk away during my injuries, if I listened to them I wouldn’t be here. Same thing goes for when I am competing well, I have to focus only on my cues and training. That is how I will get better and stronger.
What does your season look like this year?
My season so far has been a very successful one. I have competed in multiple pentathlons indoor and heptathlons
outdoor and have almost PB’d (personal best) in every one. I also recently won the overall Heptathlon title at the Canadian Track and Field Championships. I focused on my training until the World Universiade Games (FISU) which were in Taiwan at the end of August.
Final question, do you have any immediate goals and future goals you are excited for?
I believe goals are crucial in the development of athletics and personal success. Daily goals keep you grounded and focused as well as constantly trying to better yourself. They could be as simple as showing up to practice and remembering all your shoes (having seven events can be daunting sometimes), to even bigger goals, like aiming for the World Championships. That was my lofty goal this summer, and since I didn’t achieve that, I am more committed to FISU and doing my absolute best at that competition. Both for Canada and for myself.
Great, thanks so much Niki I really appreciate you taking the time to chat, and I wish you best of luck for staying healthy and for FISU.

20
PedorthicsQuarterly
HEALTHY FEET ARE THE FOUNDATION OF A HEALTHFUL LIFE.
We’re obsessed with foot health and on a mission to deliver comfort without compromise so that even hard-to-fit feet can find their perfect match.
SIZES & WIDTHSAvailable in expansive sizes and widths to provide every woman with the 360º fit.
REMOVABLE ORTHOTICSCustomize each shoe with removable footbeds for healthy feetthat feel great.
ADJUSTABLE CLOSURESDiscreet, adjustable closures offer a personalized fit without sacrificing style.
Funding for the PRFC comes from the generosity of pedorthists, and the board would like to thank all who have contributed to this charity. It is very important for the profile of our profession to be seen as contributing to evidence-based research in our field. We are currently embarking on a fundraising endeavor at the corporate level so that we are able to continue to fund top quality research on an ongoing basis.
The 2016 grant was awarded to Laura Welte, a Master’s student at Queen’s University in Kingston, ON. Welte’s team is performing research on feet with plantar fasciitis, examining foot mechanics using ultrasound, CT Scan, and bi-planar x-ray video. This is newer technology that is not available to many researchers due to its high cost. It allows them to accurately study the foot in motion, supported by an orthotic, inside a shoe (which is not easy to do with skin-marker motion
capture systems). They will be using custom orthotics fabricated by a C. Ped (C). We are very excited to be funding this project and look forward to their presentation at the Annual Symposium in April, 2019.
The PRFC supported work by Michael Hunt’s group at the University of British Colombia that was the first to examine the interaction between foot posture with the use of a lateral wedge in patients with knee osteoarthritis (OA). As a result of Dr. Hunt’s work, we are revising our Clinical Practice Guidelines to omit the contraindication of using a lateral wedge for knee OA patients that have a highly pronated foot posture (through his introduction of a ‘supportive wedge’).
We are seeking grant proposals for a 2018 award. Spread the word!
Autumn 2017 - Update
Maclean Graydon, C. Ped Tech (C), C. Ped (C) Chair, Pedorthic Research Foundation of Canada
www.pedorthicresearchcanada.org
The Pedorthic Research Foundation of Canada is a charity that raises money to fund research that is relevant to the pedorthic profession. The foundation aspires to enhance the profile of our profession through research. All health professions are adapting to a culture of evidence-based practice, and in order to continue to be considered leaders in the biomechanics world, pedorthists need scientific evidence to legitimize our clinical practices.

A Periodical of the Pedorthic Association of Canada - Fall 2017
21
Notice of DisciplineMr. Kenneth Brubacher, COFS was disciplined on May 30, 2017. A PANEL OF THE DISCIPLINE COMMITTEE OF THE COLLEGE OF PEDORTHICS OF CANADA ORDERED AND DECLARED that Kenneth Brubacher did commit conduct contrary to the Code of Ethics and Standards of Practice of The College of Pedorthics of Canada. Mr. Brubacher is hereby required to register for and complete the University of Western Ontario Pedorthics Course (PEDS 6021) by way of online
enrollment and to be completed in accordance with the requirements of the said Pedorthics Course.
Geoff PowellExecutive Director and RegistrarThe College of Pedorthics of Canada
OKAPED Inc. is currently accepting applications for a full time clinical position sharing time at our Salmon Arm and Vernon clinics in beautiful BC.
OKAPED is a leader in Pedorthic care and treatment in Canada. We utilize slow motion HD video analysis when assessing patients along with Canada’s first Pedorthic EMR online patient management system we introduced to our profession over 12 years ago. Our clinical, administrative and lab teams work together to make the work environment a great place to be. Applicants should have minimally 2 years of clinical experience and possess fabrication skills and knowledge for orthotic and footwear adjustments and modifications. Experience in managing a Pedorthic clinic would also be an asset but is not a prerequisite. The position is salaried with a benefits plan allowance as well as full coverage of professional fees and insurance.
The Okanagan is rated as one of the best places to live in Canada! Vernon and Salmon Arm offer an outdoor paradise with local skiing, biking, hiking, wineries and stunning lakes adjacent to both city centers. For more info on OKAPED simply go to www.okaped.com. More information on this position is also available at the Career Centre of the PAC website. If you have interest in this position please contact Jeff Fink at [email protected].
Job Opportunity

22
PedorthicsQuarterly
John Foster C. Ped (C)
John Foster’s career in pedorthics began long before he received his certification.
It started when he was 14 years-old, working in his father’s warehouse at Foster’s Shoes and Pedorthics in Toronto. At 17 years-old, he was working on the floor after school and on Saturdays.
“I didn’t really choose the field of pedorthics, rather it was a long indoctrination,” says John, whose father Bill Foster co-founded the company.
Foster’s Shoes and Pedorthics started in Toronto in 1953, with another location opening in Winnipeg in the 1960s, and was the first children’s specialty shoe store.
“A lot of it was pediatric prescription work,” remembers John. “I found it quite interesting, and of course there was a component of sometimes helping children with disabilities, which was a good eye opener for a teenager.”
In the 1970s, the family expanded the business into adult footwear. Around this time, John says there was changing research in children’s orthopedic shoes.
“(The research) stated that children’s orthopedic shoes with strong counters, wedging, arch supports etc. should not be prescribed as there was no evidence to support the fact they corrected children’s flat feet and that only children who were symptomatic
Member ProfilesSandra Gullion C. Ped (C)
When Sandra Gullion received her first set of orthotics as a patient at Orthotics East in Halifax, Nova Scotia, she was introduced to the world of pedorthics.
She knew it would be an interesting career, and set out to learn more about it.
Sandra, who grew up in rural Nova Scotia on the Acadian French shore, started her career as a licensed practical nurse at the Nova Scotia Rehabilitation Centre. For 10 years, she worked with hemiplegic, spinal cord and head injured patients, and those with various other conditions.
“I was always interested in the work that was done in Prosthetics/Orthotics in the rehab department, but was always intimidated by my lack of knowledge to venture into their space,” says Sandra, who is now a pedorthist at Soles in Motion in Dartmouth, Nova Scotia.
After a decade at the Nova Scotia Rehabilitation Centre, and the birth of her son, she decided to work in management at a home health care department.
“The retail world was new for me and it was a challenge learning about diabetic aids, as well as compression therapy and the orthopedic bracing,” she says. “It was a learning curve, but one I enjoyed.”
She remained there for five years, until she was given the opportunity to work for Curwin Health and Sport.
Here, Brian Stoodley guided her as she embarked on her pedorthic career. Sandra considers him a great mentor who gave her plenty of learning opportunities.
When Brian moved on, Sandra says she had another great mentor - Janice Stewart from Paris Orthotics.
She quickly realized that it is important for a clinician and lab liaison to have a strong relationship, and she remembers regularly calling Janice for advice.
“She is the first person I called when I passed my C. Ped (C) exam,” Sandra recalls.
Over the years, Sandra proctored with many other pedorthists while working at Curwin. She says she learned a lot from her colleagues – including how important it is to work in a multidisciplinary clinic that includes physiotherapists, massage therapists, and podiatrists.
“I think it is vital to recognize the importance of other health care professionals when dealing with your patients, and to keep in mind that you cannot fix everyone - but to give them other options for their recovery,” Sandra says.
She worked at Curwin Health and Sport for 12 years, and moved onto Brian Stoodley’s Biotech Orthotic Lab in Elmsdale.
Sandra has worked at Soles in Motion for the past two years, and says she enjoys working with the public in a brand new multidisciplinary clinic.
“I have been working in the field of pedorthics for the past 18 years, and find my work quite fulfilling – especially with repeat patients that come back and say, ‘You have changed my life,’” she says.
Sandra currently volunteers for PAC as a proctor for the C. Ped Tech (C) and C. Ped (C) exams. She also speaks about footwear and pedorthics to various running groups.
In her spare time, Sandra enjoys working out at her local gym, reading, meditation and going for long hikes.

A Periodical of the Pedorthic Association of Canada - Fall 2017
23
should be treated in any way,” John explains, adding that the business also shifted as the baby boomer generation became adults.
As the business was changing, John attended Ryerson University where he received his three-year diploma in Business Administration. He then received his American certification in pedorthics, since there was no Canadian option then.
“I was about 23, and with no strong inclination to do something else and with a ready job available, I decided to give the pedorthic field a two-year try,” he says. “The next thing I knew, it was 40 years later.”
John and his brother, Ted, entered the business in the 1980s and later became the principals of the company.
Over the years, John has enjoyed many aspects of the job – including keeping up with technology, and always trying to find a mix of footwear, orthotics and foot care products that make the business better.
After 40 years, he also still finds the job rewarding every day.
“Definitely the most rewarding part of the job is still being able to help people that are dealing with chronic pain or mobility issues, and knowing that in however small a way, you have helped them,” John says.
As a pedorthist who has trained 12 others, he adds that he usually doesn’t like to give advice to others starting out in the field, as they are much more advanced than he was at a similar age – but sticks with advice his father gave him.
“My father, to me, was someone who led more by example than with words,” John says. “But one thing he said to me that I always will remember was, ‘It’s a good idea to do what you say you are going to do.’ That was probably after I had messed something up! Remembering that has kept me out of a lot of trouble ever since, and made me careful as to what I promise customers as a pedorthist.”
In his spare time, John enjoys the outdoors with his wife, Stephanie, whom he met through their mutual love of wilderness canoe tripping.
“Now that we are older and creakier, we do most of our outdoor activities like kayaking, rowing, swimming or cross country skiing from our cottage north of Toronto or her family cottage in the Laurentians north of Montreal,” he says. “We also find the cottage a great place to do a little quiet reading or walk the dog in the woods.”
Job OpportunitiesOttawa Opportunity - Turnkey• Profitable turnkey business opportunity for a pedorthist.
• Established stable practice in a desirable community.
• Over 2,500 orthotic patient files.
• Full on-site laboratory.
• Footwear and compression product sales.
• Pedorthic clinic 25 years at this prime location.
• Transition partnering and/or partial financing available.
Contact in confidence:
Alvin Burnard, C.Ped [email protected]
BioPed Kitchener - Full TimeBioPed Kitchener is looking for a full time Canadian Certified Pedorthist C. Ped (C) to cover a maternity leave starting in January 2018. The successful candidate will become a part of a busy multidisciplinary clinic with another Pedorthist, Chiropodist and a Footcare Nurse on Staff.
This position will offer a competitive salary as well as benefits and the probability of retaining full time after the maternity leave is completed in neighbouring BioPed clinics.
If interested please submit your resume and cover letter to Brandon Wittig at [email protected].

Have you logged in to take advantage of your free module and earn CE Credits? Don’t wait! Expand your knowledge of the Footcare industry by learning from world-class speakers!
The best part is that you can do it all within the comfort of your own home, from any device! Visit learn.bioped.com today and register with promo code “PAC2017” to get your free module!
T H E F O O T & L O W E R L I M B E X P E R T S I N C A N A D A F O R O V E R 3 0 Y E A R S
facebook.com/biopedfootcare @bioped_footcare
Get Your Free Module and Earn CE Credits Today!
www.bioped.com