Embed Size (px)
Citation preview

Foot and Ankle Fractures
Foot and Ankle Foot and Ankle
FracturesFractures

Anatomy
Three groups of stabilizing ligaments:
1)Lateral
-anterior talofibular ligament (ATFL)
-calcaneofibular ligament (CFL)
-posterior talofibular ligament (PTFL).
-limit ankle inversion and prevent anterior and lateral subluxation of the talus


Anatomy
2)Medial
-deltoid ligament (group of four ligaments)
-anterior and posterior tibiotalar
-tibionavicular
-tibiocalcaneal
-stabilize the joint during eversion and prevent talar subluxation
-20-50% stronger than lateral ligaments

History
• History
-mechanism of injury
-ankle and foot position during the injury
-any sounds heard at the time injury
-previous history of ankle injury, any knee or foot pain
-degree of function after the event.

Physical ExamInspection
-deformity, ecchymosis, swelling, perfusion ROM (normal)
-30 to 50 degrees plantar flexion
-20 degrees dorsiflexion-25 degrees inversion and eversion -15 degrees of adduction -30 degrees of abduction
Palpation-individual ligaments (MCL,LCL, syndesmotic) and tendons -the joints above and below the ankle
-important: proximal fibula (“Maisonneuve fracture”) and the base of the fifth metatarsal ("dancer's fracture").

Special TestsAnterior Drawer
-integrity of the ATFL
-grasp the heel with one hand and apply a posterior force to the tibia with the other hand, while drawing the heel forward.-laxity is compared with the opposite (uninjured) ankle.
-positive test: a difference of 2 mm subluxation compared with the opposite side
or a visible dimpling of the anterior skin of the affected ankle (suction sign) Squeeze Test
-tests the integrity of the syndesmotic ligaments -examiner places his hand 6 to 8 inches below the knee and squeezes the tibia and fibula together-positive test: results in pain in the ankle, which indicates injury of the syndesmotic ligament

X-rays
X-rays-approx. 10-15% of all traumatic radiographs are of the ankle
-80% of all ankle injuries get an x-ray, fewer than 15% have a significant fracture
Views-AP, lateral, mortise view (15-20 degrees of internal rotation)
-AP : malleoli, plafond, talar dome, lateral process of the talus-Lateral : ant/post tibial margins, talar neck, post, talar
process and calcaneus
-Mortise : most important view, medial clear space should not
exceed 4mm


Xray Measurments

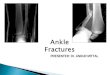
Ankle Fractures

Classification
Danis-Weber
-based on mechanism of injury
-three fracture types (i.e., A, B, C ), defined by the location of the fibular fracture
-A - below the tibiotalar joint
-B - at the level of the tibiotalar joint
-C - above the tibiotalar joint

Unimalleolar Fractures
Lateral
-any avulsion <3mm in size can be treated as an ankle sprain

Unimalleolar Fractures- Lateral
Stability depends on the location of the fracture-Type A (below tibiotalar joint)-no medial tenderness-BN walking cast-f/u 1wk to ensure no displacement-non-wt bearing x3wks then wt bearing for another 3-5 wks-medial tenderness (check mortise for displacement)-ortho consult

Unimalleolar Fractures- Lateral
Type B and C (at or above the tibiotalar
joint)
-orthopedic consult ?ORIF
-type B : 50% associated with tibiofibular disruption

Unimalleolar Fractures-Medial
Medial-commonly associated with lateral and posterior malleolar disruption-need to examine entire length of the fibula (Maisonneuve #)
Isolated medial fracture (nondisplaced)-non wt bearing x3 wks, f/u after 1 wk -wt bearing another 3-5 wks-if very active can ORIF initially!!!

Bimalleolar Fractures
Management
-disruption of two elements of the ring
-ortho consult
-management controversial (ORIF vs closed reduction and close f/u)

Trimalleolar Fractures (Cotton’s fracture)
Management
-disruption of three parts of the ring (medial/lateral/posterior)
-ortho consult
-ORIF

Pilon #?

Pilon Fractures (Bad!)
Mechanism-axial compression-talus driven into the plafond-usually comminuted and displaced with extensive soft tissue swelling-look for associated injuries-calcaneus, femoral neck, acetabulum, lumbar vertebrae
Management -emergent ortho consult

Tillaux #?

Tillaux fracture (Pediatric)
SH type III of the lateral tibial epiphysis
-extreme eversion and lateral rotation
-adolescence
-medial aspect of epiphysis is closed
-fracture of the lateral aspect and into joint
Management
-ortho consult ORIF


Foot Fractures

Anatomy
Anatomy-27 bones, 57 articulations-Hindfoot : calcaneus and talus -Midfoot : cuboid, navicular, and three cuneiforms-Forefoot : metatarsals, phalanges, and sesamoids-Subtalar joint
-formed by three articulations between the inferior talus and calcaneus-Inversion and eversion of the hindfoot through the subtalar joint

Anatomy
-Tarsometatarsal, or Lisfranc's joint
-connects the midfoot and the forefoot
-Blood supply
- anterior and posterior tibial arteries
-Nerve supply
-peroneal (deep and superficial), posterior tibial, saphenous and sural nerves

X-rays
Xrays
-AP, lateral, oblique(45 degrees of internal
rotation)
-AP and oblique
-best image for the forefoot and midfoot
-Lateral
-best image for the hindfoot and soft tissues

Foot Fractures

Talar #
TalusGeneral
-second most common fractured tarsal-3 parts : head, neck, body-prone to dislocation with foot in plantar
flexion-tenuous blood supply – risk of avascular necrosis

Fractures - Talus
Minor-chip #’s treated like sprainsTreatment-as above tx as sprain-fragments >5mm may need excision
Major-involve head (5-10% of all talar #’s), neck (50% of all major #’s) and body (23% of all talar #’s)-high energy mechanism

Fractures – TalusClassification
Classification (Hawkins)Type I fractures
-nondisplaced and lack joint involvementrisk AVN : approx. 10% Type II fractures
-displacement of the talar neck with subluxation or dislocation of the subtalar joint and preservation of the ankle joint
Type III fractures -displaced with dislocation of the talus from both the subtalar and ankle joints-risk AVN : >70%
Type IV fracture
-type II injury with associated talar head dislocation

Fractures - Talus
Treatment
-all require ortho consult
-any significant displacement/dislocation, attempt closed reduction in the ED
-grasp midfoot and apply longitudinal traction while plantar flexing the foot

Calcaneus (Lover’s #)General-5x more common in men-largest and most frequently fractured tarsal bone-falls (axial load) or twisting mechanisms-extra-articular (25-35%) – good prognosis-intra-articular (70-75%) – not so good prognosis!-look for associated fractures->50 % cases have associated other extremity or spinal fractures-7% bilateral-50% will have long-term disability

Calcaneus #’s
X-ray
-Boehler’s angle (20-40 degrees)
-suspect fracture if <20 degrees
Treatment
-ortho consult
-?ORIF vs conservative management

Navicular
General-most common midfoot #-blood supply tenuous, risk AVN-classification: dorsal avulsion # (47% all
navicular #’s), tuberosity and body #’s-mechanism usually eversion injury-pain over the dorsal and medial aspect of foot with swelling

Navicular
TreatmentAvulsion
-walking cast 4-6wks and ortho f/uTuberosity and body
-not displaced, cast (non wt bearing initially) with close f/u -if displaced or >20% articular surface area will require ORIF

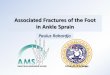
LisFranc ?

Lisfranc Injury (tarsometatarsal fractures/dislocations)
General-damage to the tarsometatarsal joint (any # or dislocation to this area is termed a Lisfranc injury)
-commonly missed injury-4% incidence per year of tarsometatarsal injuries in collegiate football players-early recognition and anatomical alignment with internal fixation is necessary for satisfactory results-mechanism : high-energy needed to disrupt ligament, rotational force( e.g MVA) -clinical: severe midfoot pain, significant swelling and ecchymosis, inability to wt bear

Classification
Classification
1)Total Incongruity
2)Partial Incongruity
3)Divergent
(Homolateral/Divergent, Type A,B,C)

X-ray Findings
• 1. The medial shaft of the second metatarsal should be aligned with the medial aspect of the middle cuneiform on the anteroposterior view.
• 2. The medial shaft of the fourth metatarsal should be aligned with the medial aspect of the cuboid on the oblique view.
• 3. The first metatarsal cuneiform articulation should have no incongruency.
• 4. A "fleck sign" should be sought in the medial cuneiform-second metatarsal space. This represents an avulsion of the Lisfranc ligament.
• 5. The naviculocuneiform articulation should be evaluated for subluxation.6. A compression fracture of the cuboid should be sought.

Lisfranc - Treatment
Treatment
The key to successful outcome in the Lisfranc
injuries is anatomical alignment
-Nondisplaced
-treated with a non-weight-bearing cast for 6 weeks followed by a weight-bearing cast for
an additional 4 to 6 weeks.
-Displaced fractures (>2mm) – ORIF

Metatarsal #’s
Treatment-2nd – 4th – conservative with well paddedshoe-1st - ORIF
Exception-displaced (>3mm or angulated-plantar direction >10 degrees)-closed reduction-+/- pinning if unstable-non wt bearing cast 4-6 wks

Jones #
Jones #-transverse # >15mm from the proximal end of the bone (high rate delayed/nonunion) -occur in >50% pts with conservative therapy)
Treatment-ortho f/u-non-wt bearing cast 6-8 weeks or ORIF

X-Rays