-
8/19/2019 Ankle Injury Orto ICO 2
1/76
-
8/19/2019 Ankle Injury Orto ICO 2
2/76
Ankle Injuries
Ankle injuries fall into the same basic categories asdo all
athletic injuries:
• Contusions•
Sprains• Strains• Fractures
-
8/19/2019 Ankle Injury Orto ICO 2
3/76
85% of all ankle sprains involve some plantar flexion of the
ankle and
inversion of the foot
!he remaining "5% consist of eversion mechanisms #hich are often
theresult of an outside force such as being fallen on from the
outside
-
8/19/2019 Ankle Injury Orto ICO 2
4/76
-
8/19/2019 Ankle Injury Orto ICO 2
5/76
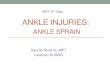
Lateral aspect of the joints of the right ankle region
1- anterior inferior tibio bular ligament2- anterior oblique
capsular reinforcement3- talonavicular ligament4- dorsal
cuboideonavicular ligament5- t e t!o limbs of t e bifurcate
ligament"- dorsal calcaneocuboid ligament#- e$tensor digitorum
brevis
%- cervical ligament&- anterior talo bular ligament1'-
lateral talocalcaneal ligament11- calcaneo bular ligament12-
posterior intermalleolar ligament13- posterior talo bular
ligament14- posterior talocalcaneal ligament
-
8/19/2019 Ankle Injury Orto ICO 2
6/76
!he s$ndesmosis ligament is often also injured#ith an eversion
force f the tibia and fibula
spread on the talus& the ankle mortise isdisrupted and the
ankle can become ver$unstable t is also not unusual to see
anassociated fibula fracture #ith an eversionmechanism 'see x(ra$s
belo#) Assessment of as$ndesmosis sprain #ill be difficult for
theinitial *+ to +8 hours f the ankle is ,uites#ollen and edematous
assessment of as$ndesmosis sprain ma$ be difficult until the
pain and s#elling have isolated to individualareas or x(ra$s
sho# some spreading of theankle mortise
-
8/19/2019 Ankle Injury Orto ICO 2
7/76
-
8/19/2019 Ankle Injury Orto ICO 2
8/76
-
8/19/2019 Ankle Injury Orto ICO 2
9/76Ankle (cc )mosis
-
8/19/2019 Ankle Injury Orto ICO 2
10/76
-istal Fibula fracture #ithassociated medial deltoid
ligamentdisruption !his injur$ is fre,uentl$the result of the foot
being planted
#ith a valgus load applied to theleg
-
8/19/2019 Ankle Injury Orto ICO 2
11/76
.otice the disruption of the medialdeltoid ligament and the
#idening
bet#een the medial malleolus andthe talus !his is indicative of
aruptured deltoid ligament
-
8/19/2019 Ankle Injury Orto ICO 2
12/76
Ankle dislocation #ith no fractures !his takes ahigh degree of
trauma and force n this case this#as generated as the result of a
high flip off of a
trampoline and impact #ith the ground !he ankle#as in a plantar
flexion and inverted position upon
impact !his #as an open dislocation
-
8/19/2019 Ankle Injury Orto ICO 2
13/76
Ankle Sprains
• *ost common at letic injur)+ 25, of allinjuries+
• e risk of ankle sprains varies !it t esport – 21-53,
basketball. 1#-2&, soccer. 25, volle)ball+
• Ankle sprains account for 1', to 15, of alllost pla)ing
time
• e medial malleolus is s orter t an t elateral mallelous so t
ere is naturall) moreinversion t an eversion+
-
8/19/2019 Ankle Injury Orto ICO 2
14/76
-
8/19/2019 Ankle Injury Orto ICO 2
15/76
Ankle Sprains• /reater inversion increases t e potential for
over-
stretc ing of t e lateral ligaments+• *ost sprains involve t e
lateral ligaments from
e$cessive inversion+• 0eltoid ligament is sprained less often
25, of
ankle sprains• f t e lateral ligments. t e A is sprained t e
most often follo!ed b) t e 6• 7prains ocur most often !it t e
foot in plantar
8e$ion and inversion+
-
8/19/2019 Ankle Injury Orto ICO 2
16/76
-
8/19/2019 Ankle Injury Orto ICO 2
17/76
Ankle 7prains
-
8/19/2019 Ankle Injury Orto ICO 2
18/76
Classification of Sprains
• 1st 0egree9 – Stretching of t e A – little or no edema –
tenderness – maintain function+
• 2nd 0egree – Partial tear of t e
A and:or 6
– moderate edema – some function loss
• 3rd 0egree – Complete tear A .6 . and:or ;
– total loss of function – signi cant edema
-
8/19/2019 Ankle Injury Orto ICO 2
19/76
Ankle Sprains by Grade
Sign/symptom Grade I Grade II Grade III
Tendon
Loss of functional ability
Pain
Swelling
Ecchy osis
!ifficulty bearing weight
No tear
"ini al
"ini al
"ini al
#sually not
$o
Partial tear
So e
"oderate
"oderate
%re&uently
#sually
Complete tear
Great
Se'ere
Se'ere
(es
Al ost always
-
8/19/2019 Ankle Injury Orto ICO 2
20/76
tta!a rules
• nnecessar)=-ra)s9 costl).timeconsuming. and possible ealt
risk
-
8/19/2019 Ankle Injury Orto ICO 2
21/76
• =-ra)s are onl) required if t ere is bon)pain in t e malleolar
?one A@0 an) oneof t e follo!ing9
• 1 B enderness along t e distal "cmof t e posterior edge of t e
tibia
• 2 B enderness along t e distal "cm
of t e posterior edge of t e bula• 3 B Inabilit) to bear !eig
t
immediatel) after injur) and in t e (C
-
8/19/2019 Ankle Injury Orto ICO 2
22/76
Treat ent
• AAFP (see table 3)• R.I.C.E.• Ice for 20 minutes on and 20
minutes off for the first
two hours.• After that, 20 min intervals over the next 48-72
hours,•
Compression wrap with donut or horse shoes to fillin gaps around
malleolus from 24-36 hours; after48-72 hours contrasts baths with
ROM exercises for4 minutes in warm and 1 min in ice water.
http://www.aafp.org/afp/980201ap/wexler.htmlhttp://www.aafp.org/afp/980201ap/wexler.htmlhttp://www.aafp.org/afp/980201ap/wexler.htmlhttp://www.aafp.org/afp/980201ap/wexler.html
-
8/19/2019 Ankle Injury Orto ICO 2
23/76
Achilles Tendonitists
• 6auses – Capidl) increasing training
eDort
– Adding ills or stair climbingto training – 7tarting too
quickl) after a
la)oD – ;oor foot!ear
– ($cessive pronation – ig t posterior leg muscles
• If left untreated. it ma)progress to a completerupture+
-
8/19/2019 Ankle Injury Orto ICO 2
24/76
Ac illes endon Cupture
• *ost frequentl) ruptured tendon• 6omplete ruptures are due
to
eccentric loading during abruptstopping. landing from a
jump+
• >suall) a popping sound iseard !it a complete tear+
• ere ma) or ma) not be anobvious gap 2 to " cm from t
ecalcaneus attac ment+
• reatment ma) or ma) notinclude surger) but bot
requireimmobili?ed for 3 mont s+
-
8/19/2019 Ankle Injury Orto ICO 2
25/76
Plantar Fasciitis
• e plantar fascia runs from t e calcaneus to t
emetatarsals+
• is tig t band acts like a bo! string to maintain t earc of t e
foot+
• ;lantar fasciitis refers to an in8ammation of t eplantar
fascia+
-
8/19/2019 Ankle Injury Orto ICO 2
26/76
;lantar asciitis
• In8ammation isusuall) due torepeated trauma to
! ere t e tissueattac es to t ecalcaneus+
• e trauma results inmicroscpic tears att e calcaneusattac ment
site+
• is ma) produce ealspurs
-
8/19/2019 Ankle Injury Orto ICO 2
27/76
;lantar asciitis
• ;ain is !orse in t emorning or after a
period of inactivit)• 6auses
– Eig arc
– ($cessive pronation – oot!ear !orn out. stiD – Increase in
intensit)
-
8/19/2019 Ankle Injury Orto ICO 2
28/76
Ankle Exercises
• 6alf stretc• 7oleus stretc• Cesisted dorsal
and plantar8e$ion
• Eeel raises
• 7tep-up• Fump rope
-
8/19/2019 Ankle Injury Orto ICO 2
29/76
A@G ( CA6 >C(
-
8/19/2019 Ankle Injury Orto ICO 2
30/76
(;I0(*I /H
• *ost ankle fractures are isolatedmalleolar fractures 2:3
•
-
8/19/2019 Ankle Injury Orto ICO 2
31/76
•
-
8/19/2019 Ankle Injury Orto ICO 2
32/76
CA0I /CA;EH
• tta!a Ankle rules 1'', sensitivit)for detecting ankle
fractures
• ;ain near malleoli
• Age J 55 )ears• Inabilit) to bear !eig t•
-
8/19/2019 Ankle Injury Orto ICO 2
33/76
CA0I /CA;EH
• 7tandard A;. ateral vie!s• *ortise vie!9 = ra) beam parallel
to
trans malleolar a$is;atient )s leg internal) rotated to 15
degrees
-
8/19/2019 Ankle Injury Orto ICO 2
34/76
CA0I /CA;EH
• = ra) measurements of alignmentand stabilit)9
• alo crural angle• Angle subtended b) line dra!n parallel
to
articular surface of distal tibia and oneconnecting tip of bot
malleoli
• 4 to 11 degrees• An) diDerence of 2-3 degrees to opposite
side is abnormal and indicates bulars ortening
-
8/19/2019 Ankle Injury Orto ICO 2
35/76
-
8/19/2019 Ankle Injury Orto ICO 2
36/76
CA0I /CA;EH
• *edial clear space•
-
8/19/2019 Ankle Injury Orto ICO 2
37/76
CA0I /CA;EH
• ibio bular clearspace9
• 7)ndesmosis injur)•
-
8/19/2019 Ankle Injury Orto ICO 2
38/76
6 A77I I6A I @7
• ;ott )s9 Anatomical• *ono malleolar•
-
8/19/2019 Ankle Injury Orto ICO 2
39/76
A>/(- EA@7(@6 A77I I6A I @
• Associates speci c fracture patterns !itmec anism of
injur)
• 7upination ($ternal rotation "',
• 7upination Adduction 2',• ;ronation ($ternal rotation and
;ronation
abduction 2',
• 1 st !ord- oot position at time of injur)• 2 nd !ord-
0irection of deforming force on
talus
-
8/19/2019 Ankle Injury Orto ICO 2
40/76
A>/(- EA@7(@6 A77I I6A I @
• it foot supinated. lateral supportstructures !ill fail rst
• it foot pronated medial supportstructures fail rst
• Injuries are graded 1 to 4 based onlevel of involvement and
severit)+
-
8/19/2019 Ankle Injury Orto ICO 2
41/76
-
8/19/2019 Ankle Injury Orto ICO 2
42/76
-
8/19/2019 Ankle Injury Orto ICO 2
43/76
;A (C@ I A CA6 >C(
• 7-(C9 7piral oblique fracture runsfrom antero inferior margin
upto
posterior superior corte$
• 7-A09 ransverse fracture distal tomortice or avulsion fracture
of
tip
• ;-(C9 Above s)ndesmosis. fromsuperior anterior corte$ to
posteroinferior corte$
• ;-A
-
8/19/2019 Ankle Injury Orto ICO 2
44/76
Supination E*ternal +otation Supination Adduction
-
8/19/2019 Ankle Injury Orto ICO 2
45/76
,igh fibula fracture with talar displace entPronation e*ternal
rotation in-ury
-
8/19/2019 Ankle Injury Orto ICO 2
46/76
0A@I7 (
-
8/19/2019 Ankle Injury Orto ICO 2
47/76
!A$.S /E0E+ CLASS.%.CAT.1$
-
8/19/2019 Ankle Injury Orto ICO 2
48/76
• H;( 69• Abduction injur)• 61 9 oblique K pro$ to disrupted
tibio bular
ligament• 62 9 Abduction L e$t+ rotation !it pro$ K ofbula and
interosseous membrane
-
8/19/2019 Ankle Injury Orto ICO 2
49/76
A 6 A77I I6A I @
•
-
8/19/2019 Ankle Injury Orto ICO 2
50/76
7 A< (:>@7 A< (
• >@7 A< (9•
-
8/19/2019 Ankle Injury Orto ICO 2
51/76
.f %ibula is fractured and talus not shifted
Look for edial side swelling
"edial side swelling 2
!eltoid liga ent in-ury
#$STA0LE
"edial side swelling 3
Stress +adiography
Talus shifts#$STA0LE
Talus does not shiftSTA0LE
7 A< (:>@7 A< (
-
8/19/2019 Ankle Injury Orto ICO 2
52/76
7H@0(7* I6 I@F>CI(7
• *ost commonl) due to ;(C and ;A<• i$ation indicated if
• ;ro$imal bula K !it a medial injur)
• 7)ndesmotic injur) J 5 cm pro$imal toplafond
• Integrit) of s)ndesmosis can be judged intra operativel)9 i$
bula.pull laterall) !it a ook. if laterals ift J 3-4mm t en
essential to $+
-
8/19/2019 Ankle Injury Orto ICO 2
53/76
• *aisonneuve )sfracture9
• 7piral K of t epro$imal bula
ssociated !itunstable ankle injur)
• ;ronation ($ternalrotation
• Cequires reductionand stabili?ation ofs)ndesmosis
-
8/19/2019 Ankle Injury Orto ICO 2
54/76
• < 7 C E )7 CA6 >C(9• e distal end of t e pro$imal
fragment of
bula gets displaced posterior to t e tibiaand ma) be locked b)
tibia )s postero lateralridge
• e bone cannot be released b)manupulation due to intact
introsseousmembrane
• ibula is e$posed and considerable force isrequired to release
t e bula. fracture t en
$ed operativel)
-
8/19/2019 Ankle Injury Orto ICO 2
55/76
C(A *(@
• Initial *anagement9 btain A;.lateral and mortice vie!s
• Ceduce talus immediatel)• ailure >rgent operative
intervention
CI 7panning e$ $6alcaneal
pin
-
8/19/2019 Ankle Injury Orto ICO 2
56/76
-
8/19/2019 Ankle Injury Orto ICO 2
57/76
7 A< ( I@F>CH :
• K protected in a s ort leg cast orbrace for 4-" !eeks. allo!
partial !t+bearing. < after 12 !eeks
-
8/19/2019 Ankle Injury Orto ICO 2
58/76
pen reatment
• @ot indicated in stable fractures. onl)if associated injuries
like talar K orosteoc ondral K of talar dome
• Indicated in all unstable fractures
-
8/19/2019 Ankle Injury Orto ICO 2
59/76
CI
• ibula i$ation9• 1:3 rd tubular plate if
K above ankle• ag scre!s
• Cus rod9 if Ktransverse
• < 9 if fragmentsmall
-
8/19/2019 Ankle Injury Orto ICO 2
60/76
CI
• *edial *alleolus9• 2 parallel 4+' mm ; 67• < if fragment
small and osteoporotic
• ;osterior *alleolus• i$ation important9 ot er!ise ma) lead to
posterior
sublu$ation of talus• 7i?e of fragment important 6 scan• If J
25, - 3', of joint surface $ation done• i$ associated K rst and t
en do an intra op
posterior dra!er test• Appl) 1:3 rd tubular plate posterior•
Anterior to posterior intra fragmentar) scre!
-
8/19/2019 Ankle Injury Orto ICO 2
61/76
• 7)ndesmotic i$ation• Indication9 ;ro$ bula K associated !it
medial injur)• en t e medial clear space !idens on intra op
stress vie!s after bula $ation• 7cre! $ed 2 -3 cm above ankle
joint and parallel to
it and angled 3' degrees anteriorl)• 4+5 mm scre! used- purc ase
4 cortices• ig t scre! in ma$imal dorsi8e$ion of ankle• ime of
scre! removal- controversialM++ *ost
surgeons prefer to remove t e scre! before !eig tbearing is
allo!ed "B% !eeks
• >se s)ndesmotic scre! onl). !it out $ing t e bula! en K
above mid bula
-
8/19/2019 Ankle Injury Orto ICO 2
62/76
; 7 ;(CA IN(
• Ankle immobili?ed in posteriorplaster splint
• 7plint removed after 3-4 da)s.replaced !it removable
splint
• C * e$ercises are begun• @
-
8/19/2019 Ankle Injury Orto ICO 2
63/76
A=IA A0I@/ I@F>CI(79 IC(7
• Articular and metap )sealcomminution
• Foint impaction• ;ro$imal displacement of talus• Eig energ)
trauma associated !it
soft tissue involvement• racture pattern depends upon
direction and position of foot
-
8/19/2019 Ankle Injury Orto ICO 2
64/76
AP and lateral 'iews of tibialPlafond showing articular
and"etaphyseal co inution
-
8/19/2019 Ankle Injury Orto ICO 2
65/76
The position of the foot at the ti e1f a*ial load deter ines
which part
1f the tibial plafond will fracture
-
8/19/2019 Ankle Injury Orto ICO 2
66/76
6 A77I I6A I @
• Cuedi- Allgo!erclassi cation9
• )pe 1 9@ondispaced
cleavage K• )pe 29 0isplaced
and minimall)comminuted K
• )pe 39 Eig l)
comminuted K
-
8/19/2019 Ankle Injury Orto ICO 2
67/76
6 A77I I6A I @
• A : A9• A9 @on- articular•
-
8/19/2019 Ankle Injury Orto ICO 2
68/76
C(A *(@
• Initial reatment9• Ceduce an) talar displacement• Articular
reduction t roug eit er closed or open
met ods
• 7plint t e fracture ! ic ma) require temporar)skeletal
traction
• reatment ptions9•
;late• 7panning e$ternal $ator• ($ternal $ator leaving t e
anlke
-
8/19/2019 Ankle Injury Orto ICO 2
69/76
A0NA@ A/(7: 0I7A0NA@ A/(7Fixation Techniques
!echni,ue Advantages -isadvantages
/pen reduction and internal fixation nvolves #ide exposure for
articularreductionAllo#s earl$ motion of ankle joint
-isrupts tenuous soft tissue envelopenvolves large subcutaneous
implants
0as highest incidence of #ound healing problemsincluding: 1ound
breakdo#n nfection /steom$elitis Amputation
2igid cross(ankle external fixation nvolves minimal disruption
of 3one ofinjur$
2igidl$ immobili3es ankle
4xternal fixation of same side of joint Allo#s motion at the
ankleAvoids large plates to stabili3e metaph$sis Cannot be used for
all fractures-isrupts 3one of injur$s technicall$ demanding
Articulated cross(ankle externalfixation
Allo#s motion at the ankle 'limited)s technicall$ easier to
appl$ fixator nvolves minimal disruption of 3one of
injur$
s difficult to align axis of hinge #ith axis of ankle
joint2e,uires pins in hind(foot bones
alue of motion through an articulated hinge is not proven
0(6I7I @ *AGI@/ A@0 A6 C7
-
8/19/2019 Ankle Injury Orto ICO 2
70/76
0(6I7I @ *AGI@/ A@0 A6 C7C( A I@/ > 6 *(
• 6losed reatment9 >ndisplaced t)peA. )pe < and )pe 61
fractures
• pen reatment9• Immediate CI obsolete due to severe soft
tissue complications and ig rate of
implant failure• @ot favoured an) longer
-
8/19/2019 Ankle Injury Orto ICO 2
71/76
• >rgent stabili?ation done eit er b)• 7panning e$ternal
$ator• ($ternal $ator sparing t e ankle joint• Illi?arov )s ring
$ator
• 6alcaneal pin traction
• Adequate time is given for t e soft tissueto eal 4-" !eeks
• 0e native procedure is done after softtissue eals
-
8/19/2019 Ankle Injury Orto ICO 2
72/76
• 7panning e$ternal $ator andIlli?arov e$ternal $ator can be
usedfor de nitive management
• Implants9• 7mall fragment 3+5 mm and 4+'' mm
scre!s for metap )seal stabili?ation
• 7mall plates- 1:3 rd tubular. 3+5 mm 06;.small clover leaf
plates or s aped platesdesigned for distal radius. $ed anglelocking
scre! plates
-
8/19/2019 Ankle Injury Orto ICO 2
73/76
C(7> 7
• Eig energ) trauma• Cesult not al!a)s good• 0epends on
associated degree of soft
tissue trauma. !ound condition andinfections
• Average interval for fracture to eal 12!eeks
• Average time to return to normal activit)-1 )ear
• Cate of ;ost op art iritis and c:o pain and
disabilit) --- EI/EOO
-
8/19/2019 Ankle Injury Orto ICO 2
74/76
7>**ACH
• 6ommon fractures• Anatomical reduction. restoration of
bular lengt . s)ndesmotic repairlead to e$cellent outcomes for t
epatient
• In plafond fractures management ofsoft tissue component and
adequatestable $ation *A@0A CH
-
8/19/2019 Ankle Injury Orto ICO 2
75/76
!hank $ou66
-
8/19/2019 Ankle Injury Orto ICO 2
76/76