Embed Size (px)
Citation preview
2012
Annual Benefits Enrollment
Employee Benefit Options
The Benefits Enrollment period is from July 1st through July 23rd. During this time you have the opportunity to review benefit choices and add, delete, or change coverage. Any benefit changes made during this time will become effective August 1st and will remain in effect until the next Benefit Enrollment period. Your premium for each benefit will be divided and deducted from your paycheck(s) each month, according to your specified pay period. Keep in mind that all employees are eligible as long you are considered a full time employees, working 30+hours a week, and as long as you have met your 90 day probationary period.
Per IRS guidelines, changes to your benefits after July 23rd cannot be made unless there is a “family status change”, which is referred to as a Qualifying Event. Please see them listed below.
1. 90-day waiting period for new hires 2. Birth 3. Death 4. Marriage 5. Divorce 6. Adoption 7. Loss of coverage under spouse’s employment 8. Change of employment status from part-time to full-time or change in position.
Should you wish to add, delete or change coverage during one of these qualifying events, please complete the appropriate enrollment forms and return to the Benefits Department.
If you have any questions, Jessica Rodriguez or Janie Saucedo are ready to assist you. You can use the following resources to reach them:
Office (210) 344-2088
Fax (210) 344-2777
Email: [email protected] [email protected]
Kind Regards,
The Benefits Department
EMPLOYEE BENEFITS
Table of Contents: Page
1. Major Medical Benefits 1
2. Starbridge Limited Medical Benefit 5 3. Patient Plus Discount Card 9
4. Gap Plan Reimbursement Benefit 10 5. United Concordia Dental 12 6. Cigna Dental 13
7. Aetna Dental 14
8. VSP Vision Benefit 15
9. UNUM Life Benefit 16
10. Principal Short Term Disability 18
11. Aflac 19
12. Retirement Plan Options – Call for details (the plan is customized for each client)

Page 1
$2000 Deductible 100/70 Co-Pay Plan Your Benefits Summary – Buy-Up Plan
PLAN FEATURES NETWORK BENEFITS NON-NETWORK BENEFITS
Deductible (per calendar year) $ 2,000 Individual $ 4,000 Individual $ 6,000 Family $ 12,000 Family Member Co-payments do not accumulate towards the Deductible. All individual Deductible amounts will count toward the family Deductible, but an individual will not have to pay more than the individual Deductible amount. This benefit plan contains a Per Occurrence Deductible that applies to certain Covered Health Services. This Per Occurrence Deductible must be met prior to and in addition to the Annual Deductible.
Out-of-Pocket Maximum-Individual No Out-of-Pocket Maximum $ 8,000 per year Out-of-Pocket Maximum-Family No Out-of-Pocket Maximum $ 24,000 per year Member Co-payments do not accumulate towards the Out-of-Pocket Maximum. All individual Out-of-Pocket Maximum amounts will count toward the family Out-of-Pocket Maximum, but an individual will not have to pay more than the individual Out-of-Pocket Maximum amount. The Out-of-Pocket Maximum does not include the Annual and Per Occurrence Deductibles.
Benefit Plan Co-Insurance 100% after Deductible has been met 70% after Deductible has been met
Lifetime Maximum Policy Benefit Combined Network and Non-Network Maximum of $5,000,000 per Covered Person.
Physician’s Office Services –Sickness & Injury Primary Physician Office Visit 100% after $25 Co-Payment 70% after Deductible has been met Specialist Physician Office Visit 100% after $50 Co-Payment 70% after Deductible has been met In addition to the visit Co-Payment, the applicable Co-Payment or Deductible/Co-Insurance applies when these services are done: CT, PET, MRI, Nuclear Medicine: Pharmaceutical Products; Scopic Procedures; Surgery; Therapeutic Treatments.
Preventative Care Services Primary Physician Office Visit 100% after $25 Co-Payment 70% after Deductible has been met Specialist Physician Office Visit 100% after $50 Co-Payment 70% after Deductible has been met Lab, X-Ray or other preventive tests 100%; Deductible does not apply 70% after Deductible has been met
Urgent Care Center Services 100% after $75 Co-Payment 70% after Deductible has been met In addition to the visit Co-Payment, the applicable Co-Payment or Deductible/Co-Insurance applies when these services are done: CT, PET, MRI, Nuclear Medicine; Pharmaceutical Products; Scopic Procedures; surgery; Therapeutic Treatments.
Emergency Health Services-Outpatient 100% after $200 Co-Payment 100% after $200 Co-Payment Request for Pre-authorization of Services required if results in an Inpatient Stay for Preferred and Non-Preferred care.
Hospital-Inpatient Stay 100% after Deductible has been met 70% after Per Occurrence Deductible of $500 and Annual Deductible have been met. Request for Pre-authorization of Services is required.
Ambulance Service –Emergency & Non-Emergency Ground Ambulance 100% after Deductible has been met 100% after Network Deductible has been met Air Ambulance 100% after Deductible has been met 100% after Network Deductible has been met Request for Pre-authorization of Services required for Non-Emergency Ambulance for both Network and Non-Network.
Page 2
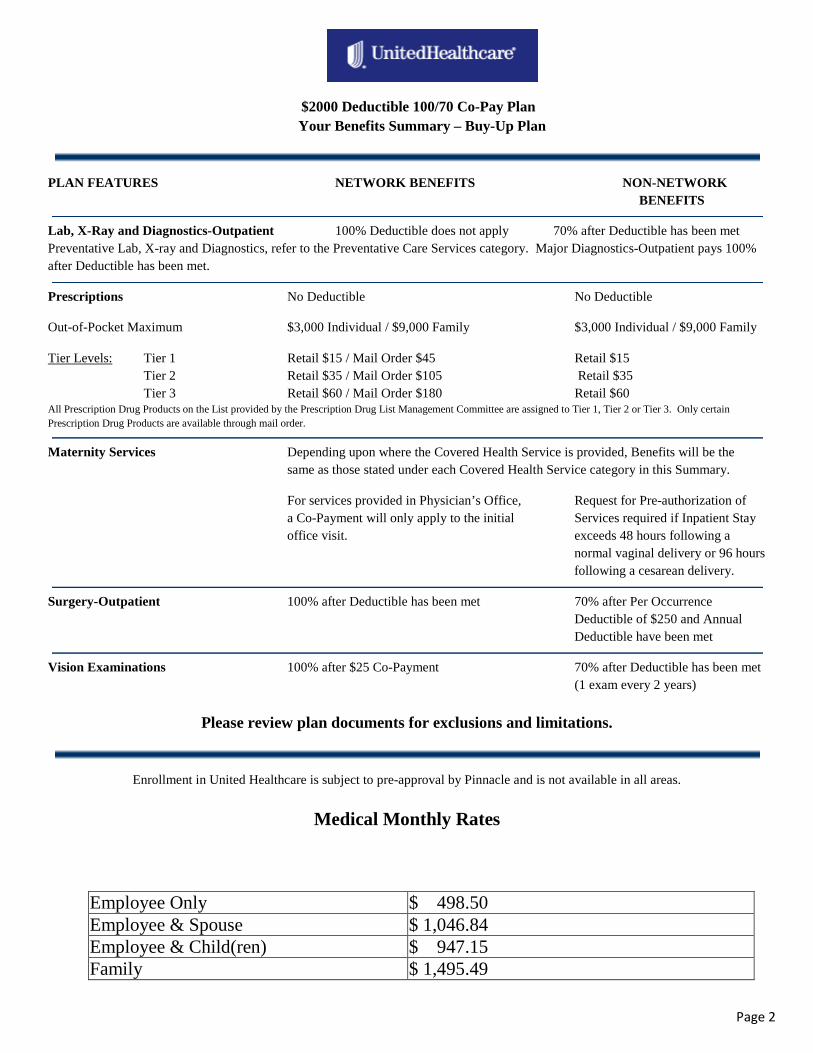
$2000 Deductible 100/70 Co-Pay Plan Your Benefits Summary – Buy-Up Plan
PLAN FEATURES NETWORK BENEFITS NON-NETWORK BENEFITS
Lab, X-Ray and Diagnostics-Outpatient 100% Deductible does not apply 70% after Deductible has been met Preventative Lab, X-ray and Diagnostics, refer to the Preventative Care Services category. Major Diagnostics-Outpatient pays 100% after Deductible has been met.
Prescriptions No Deductible No Deductible
Out-of-Pocket Maximum $3,000 Individual / $9,000 Family $3,000 Individual / $9,000 Family
Tier Levels: Tier 1 Retail $15 / Mail Order $45 Retail $15 Tier 2 Retail $35 / Mail Order $105 Retail $35 Tier 3 Retail $60 / Mail Order $180 Retail $60 All Prescription Drug Products on the List provided by the Prescription Drug List Management Committee are assigned to Tier 1, Tier 2 or Tier 3. Only certain Prescription Drug Products are available through mail order.
Maternity Services Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Summary.
For services provided in Physician’s Office, Request for Pre-authorization of a Co-Payment will only apply to the initial Services required if Inpatient Stay office visit. exceeds 48 hours following a normal vaginal delivery or 96 hours following a cesarean delivery.
Surgery-Outpatient 100% after Deductible has been met 70% after Per Occurrence Deductible of $250 and Annual Deductible have been met
Vision Examinations 100% after $25 Co-Payment 70% after Deductible has been met (1 exam every 2 years)
Please review plan documents for exclusions and limitations.
Enrollment in United Healthcare is subject to pre-approval by Pinnacle and is not available in all areas.
Medical Monthly Rates
Employee Only $ 498.50 Employee & Spouse $ 1,046.84 Employee & Child(ren) $ 947.15 Family $ 1,495.49
Page 3
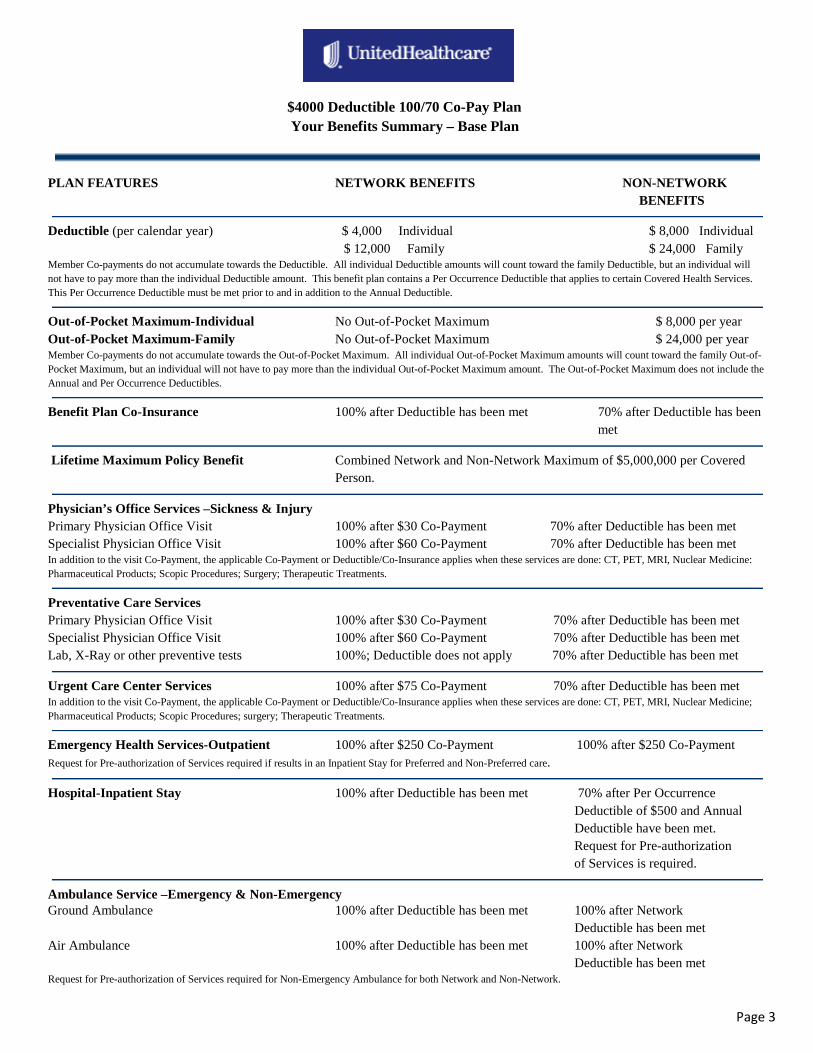
$4000 Deductible 100/70 Co-Pay Plan Your Benefits Summary – Base Plan
PLAN FEATURES NETWORK BENEFITS NON-NETWORK BENEFITS
Deductible (per calendar year) $ 4,000 Individual $ 8,000 Individual $ 12,000 Family $ 24,000 Family Member Co-payments do not accumulate towards the Deductible. All individual Deductible amounts will count toward the family Deductible, but an individual will not have to pay more than the individual Deductible amount. This benefit plan contains a Per Occurrence Deductible that applies to certain Covered Health Services. This Per Occurrence Deductible must be met prior to and in addition to the Annual Deductible.
Out-of-Pocket Maximum-Individual No Out-of-Pocket Maximum $ 8,000 per year Out-of-Pocket Maximum-Family No Out-of-Pocket Maximum $ 24,000 per year Member Co-payments do not accumulate towards the Out-of-Pocket Maximum. All individual Out-of-Pocket Maximum amounts will count toward the family Out-of-Pocket Maximum, but an individual will not have to pay more than the individual Out-of-Pocket Maximum amount. The Out-of-Pocket Maximum does not include the Annual and Per Occurrence Deductibles.
Benefit Plan Co-Insurance 100% after Deductible has been met 70% after Deductible has been met
Lifetime Maximum Policy Benefit Combined Network and Non-Network Maximum of $5,000,000 per Covered Person.
Physician’s Office Services –Sickness & Injury Primary Physician Office Visit 100% after $30 Co-Payment 70% after Deductible has been met Specialist Physician Office Visit 100% after $60 Co-Payment 70% after Deductible has been met In addition to the visit Co-Payment, the applicable Co-Payment or Deductible/Co-Insurance applies when these services are done: CT, PET, MRI, Nuclear Medicine: Pharmaceutical Products; Scopic Procedures; Surgery; Therapeutic Treatments.
Preventative Care Services Primary Physician Office Visit 100% after $30 Co-Payment 70% after Deductible has been met Specialist Physician Office Visit 100% after $60 Co-Payment 70% after Deductible has been met Lab, X-Ray or other preventive tests 100%; Deductible does not apply 70% after Deductible has been met
Urgent Care Center Services 100% after $75 Co-Payment 70% after Deductible has been met In addition to the visit Co-Payment, the applicable Co-Payment or Deductible/Co-Insurance applies when these services are done: CT, PET, MRI, Nuclear Medicine; Pharmaceutical Products; Scopic Procedures; surgery; Therapeutic Treatments.
Emergency Health Services-Outpatient 100% after $250 Co-Payment 100% after $250 Co-Payment Request for Pre-authorization of Services required if results in an Inpatient Stay for Preferred and Non-Preferred care.
Hospital-Inpatient Stay 100% after Deductible has been met 70% after Per Occurrence Deductible of $500 and Annual Deductible have been met. Request for Pre-authorization of Services is required.
Ambulance Service –Emergency & Non-Emergency Ground Ambulance 100% after Deductible has been met 100% after Network Deductible has been met Air Ambulance 100% after Deductible has been met 100% after Network Deductible has been met Request for Pre-authorization of Services required for Non-Emergency Ambulance for both Network and Non-Network.
Page 4
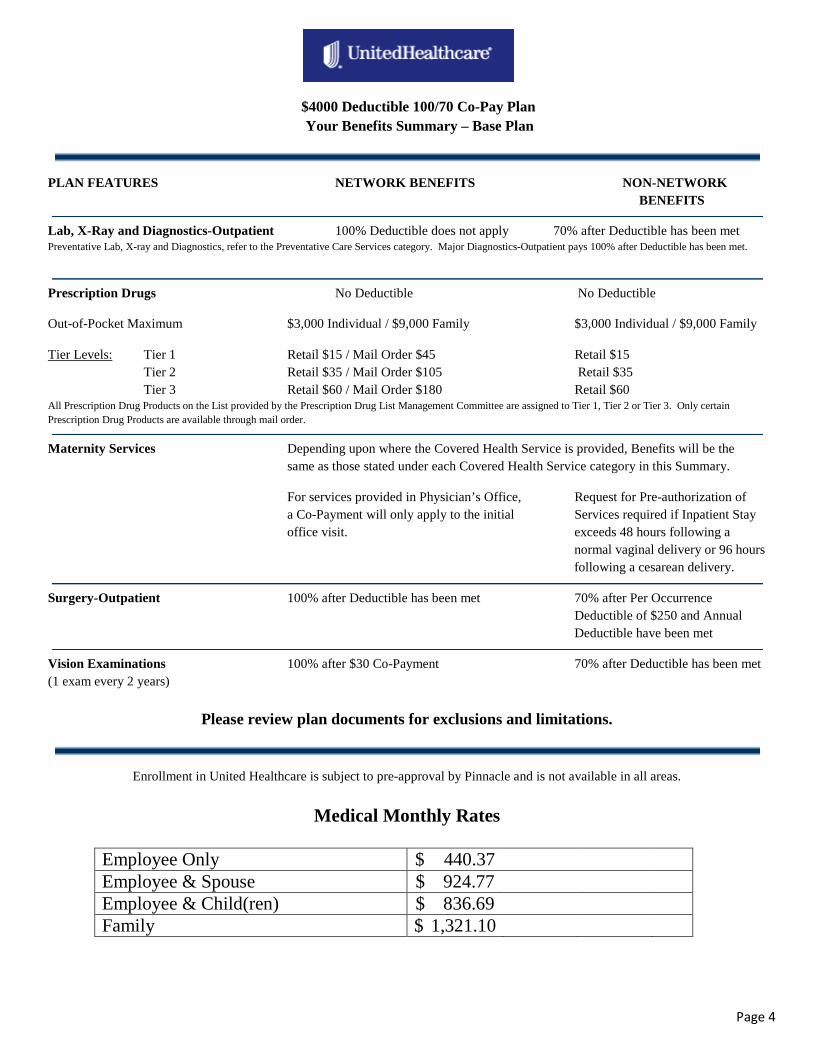
$4000 Deductible 100/70 Co-Pay Plan Your Benefits Summary – Base Plan
PLAN FEATURES NETWORK BENEFITS NON-NETWORK BENEFITS
Lab, X-Ray and Diagnostics-Outpatient 100% Deductible does not apply 70% after Deductible has been met Preventative Lab, X-ray and Diagnostics, refer to the Preventative Care Services category. Major Diagnostics-Outpatient pays 100% after Deductible has been met.
Prescription Drugs No Deductible No Deductible
Out-of-Pocket Maximum $3,000 Individual / $9,000 Family $3,000 Individual / $9,000 Family
Tier Levels: Tier 1 Retail $15 / Mail Order $45 Retail $15 Tier 2 Retail $35 / Mail Order $105 Retail $35 Tier 3 Retail $60 / Mail Order $180 Retail $60 All Prescription Drug Products on the List provided by the Prescription Drug List Management Committee are assigned to Tier 1, Tier 2 or Tier 3. Only certain Prescription Drug Products are available through mail order.
Maternity Services Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Summary.
For services provided in Physician’s Office, Request for Pre-authorization of a Co-Payment will only apply to the initial Services required if Inpatient Stay office visit. exceeds 48 hours following a normal vaginal delivery or 96 hours following a cesarean delivery.
Surgery-Outpatient 100% after Deductible has been met 70% after Per Occurrence Deductible of $250 and Annual Deductible have been met
Vision Examinations 100% after $30 Co-Payment 70% after Deductible has been met (1 exam every 2 years)
Please review plan documents for exclusions and limitations.
Enrollment in United Healthcare is subject to pre-approval by Pinnacle and is not available in all areas.
Medical Monthly Rates
Employee Only $ 440.37 Employee & Spouse $ 924.77 Employee & Child(ren) $ 836.69 Family $ 1,321.10
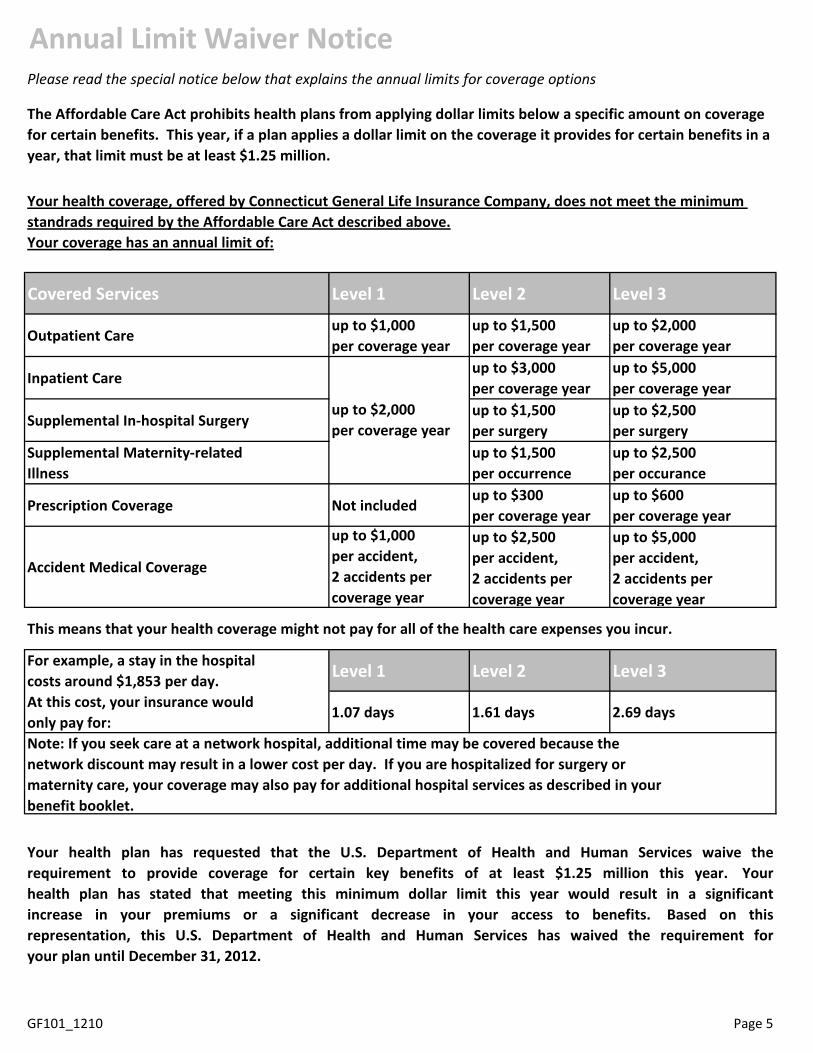
Annual Limit Waiver NoticePlease read the special notice below that explains the annual limits for coverage options
Your coverage has an annual limit of:
Covered Services Level 1 Level 2 Level 3
Outpatient Careup to $1,000per coverage year
up to $1,500per coverage year
up to $2,000per coverage year
Inpatient Careup to $3,000per coverage year
up to $5,000per coverage year
Supplemental In-hospital Surgeryup to $1,500per surgery
up to $2,500 per surgery
Supplemental Maternity-related Illness
up to $1,500per occurrence
up to $2,500 per occurance
Prescription Coverage Not includedup to $300 per coverage year
up to $600 per coverage year
Accident Medical Coverage
up to $1,000per accident,2 accidents per coverage year
up to $2,500 per accident, 2 accidents per coverage year
up to $5,000 per accident, 2 accidents per coverage year
This means that your health coverage might not pay for all of the health care expenses you incur.
Level 1 Level 2 Level 3
1.07 days 1.61 days 2.69 days
GF101_1210 Page 5
Your health plan has requested that the U.S. Department of Health and Human Services waive therequirement to provide coverage for certain key benefits of at least $1.25 million this year. Yourhealth plan has stated that meeting this minimum dollar limit this year would result in a significantincrease in your premiums or a significant decrease in your access to benefits. Based on thisrepresentation, this U.S. Department of Health and Human Services has waived the requirement foryour plan until December 31, 2012.
The Affordable Care Act prohibits health plans from applying dollar limits below a specific amount on coverage for certain benefits. This year, if a plan applies a dollar limit on the coverage it provides for certain benefits in a year, that limit must be at least $1.25 million.
Your health coverage, offered by Connecticut General Life Insurance Company, does not meet the minimum standrads required by the Affordable Care Act described above.
up to $2,000per coverage year
For example, a stay in the hospitalcosts around $1,853 per day.At this cost, your insurance would only pay for:Note: If you seek care at a network hospital, additional time may be covered because the network discount may result in a lower cost per day. If you are hospitalized for surgery or maternity care, your coverage may also pay for additional hospital services as described in your benefit booklet.
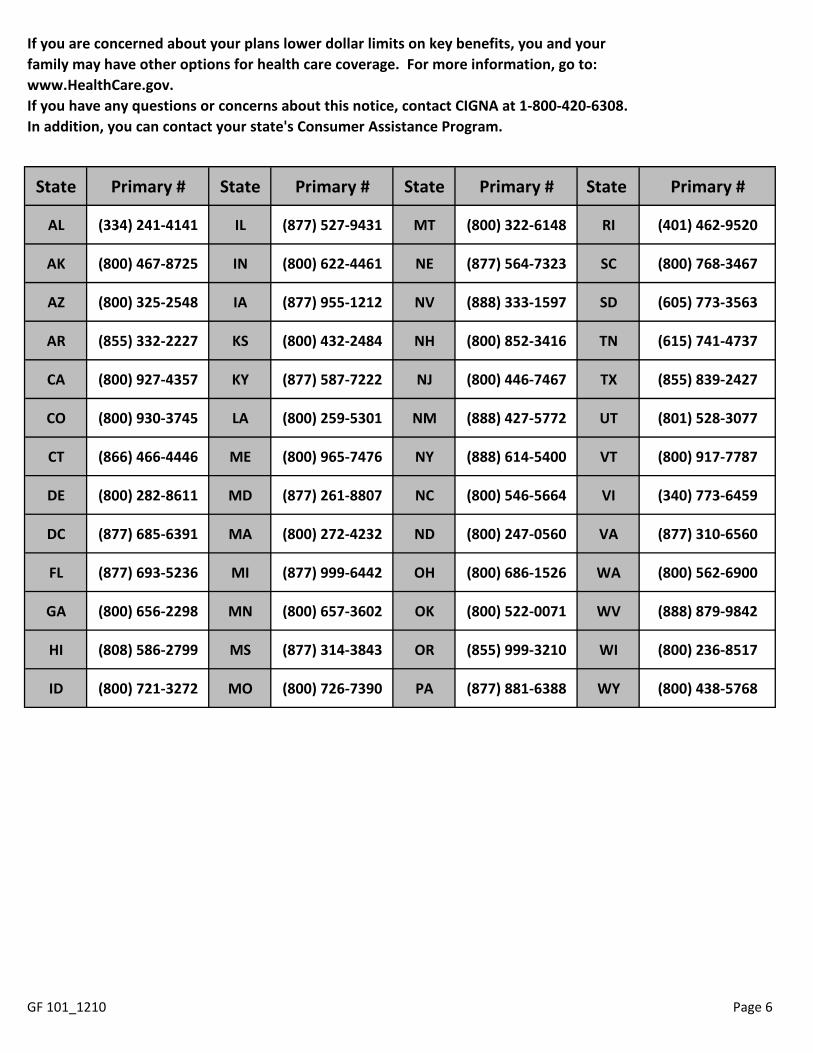
State Primary # State Primary # State Primary # State Primary #
AL (334) 241-4141 IL (877) 527-9431 MT (800) 322-6148 RI (401) 462-9520
AK (800) 467-8725 IN (800) 622-4461 NE (877) 564-7323 SC (800) 768-3467
AZ (800) 325-2548 IA (877) 955-1212 NV (888) 333-1597 SD (605) 773-3563
AR (855) 332-2227 KS (800) 432-2484 NH (800) 852-3416 TN (615) 741-4737
CA (800) 927-4357 KY (877) 587-7222 NJ (800) 446-7467 TX (855) 839-2427
CO (800) 930-3745 LA (800) 259-5301 NM (888) 427-5772 UT (801) 528-3077
CT (866) 466-4446 ME (800) 965-7476 NY (888) 614-5400 VT (800) 917-7787
DE (800) 282-8611 MD (877) 261-8807 NC (800) 546-5664 VI (340) 773-6459
DC (877) 685-6391 MA (800) 272-4232 ND (800) 247-0560 VA (877) 310-6560
FL (877) 693-5236 MI (877) 999-6442 OH (800) 686-1526 WA (800) 562-6900
GA (800) 656-2298 MN (800) 657-3602 OK (800) 522-0071 WV (888) 879-9842
HI (808) 586-2799 MS (877) 314-3843 OR (855) 999-3210 WI (800) 236-8517
ID (800) 721-3272 MO (800) 726-7390 PA (877) 881-6388 WY (800) 438-5768
Page 6
If you are concerned about your plans lower dollar limits on key benefits, you and your family may have other options for health care coverage. For more information, go to: www.HealthCare.gov. If you have any questions or concerns about this notice, contact CIGNA at 1-800-420-6308. In addition, you can contact your state's Consumer Assistance Program.
GF 101_1210
Page 7
ww.aetna.com
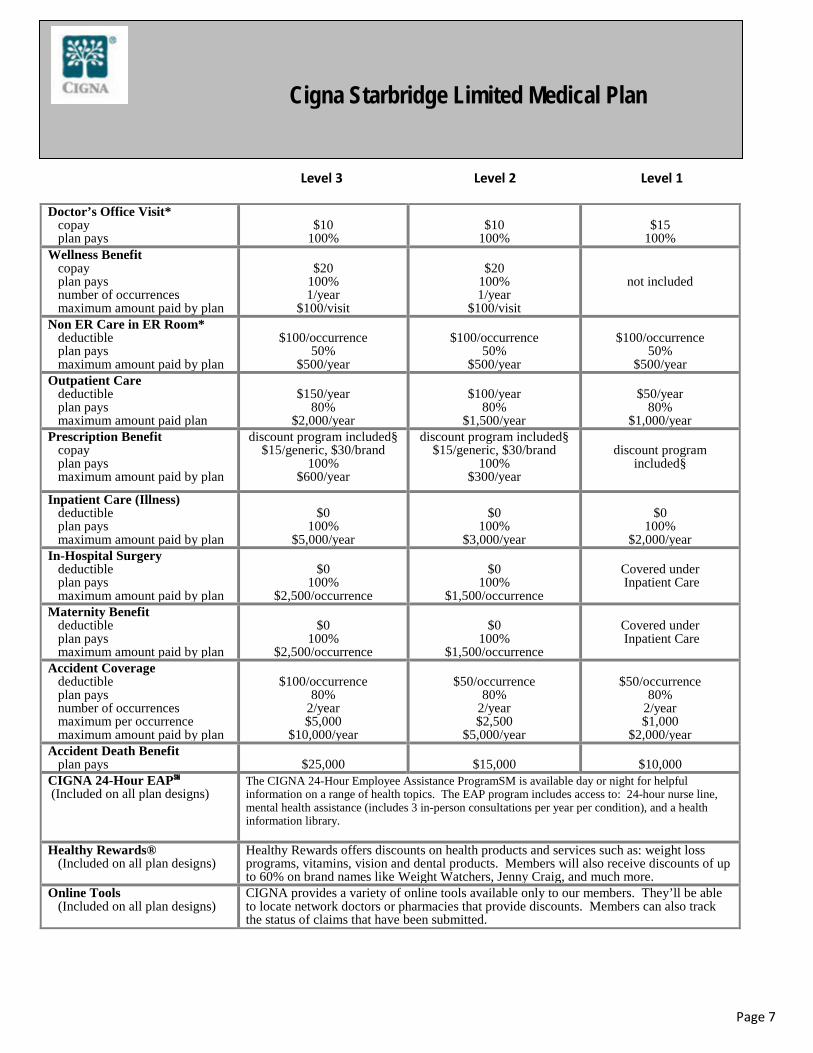
Level 3 Level 2 Level 1
Doctor’s Office Visit* copay plan pays
$10
100%
$10
100%
$15
100% Wellness Benefit copay plan pays number of occurrences maximum amount paid by plan
$20
100% 1/year
$100/visit
$20
100% 1/year
$100/visit
not included
Non ER Care in ER Room* deductible plan pays maximum amount paid by plan
$100/occurrence
50% $500/year
$100/occurrence
50% $500/year
$100/occurrence
50% $500/year
Outpatient Care deductible plan pays maximum amount paid plan
$150/year
80% $2,000/year
$100/year
80% $1,500/year
$50/year
80% $1,000/year
Prescription Benefit copay plan pays maximum amount paid by plan
discount program included§ $15/generic, $30/brand
100% $600/year
discount program included§ $15/generic, $30/brand
100% $300/year
discount program
included§
Inpatient Care (Illness) deductible plan pays maximum amount paid by plan
$0
100% $5,000/year
$0
100% $3,000/year
$0
100% $2,000/year
In-Hospital Surgery deductible plan pays maximum amount paid by plan
$0
100% $2,500/occurrence
$0
100% $1,500/occurrence
Covered under Inpatient Care
Maternity Benefit deductible plan pays maximum amount paid by plan
$0
100% $2,500/occurrence
$0
100% $1,500/occurrence
Covered under Inpatient Care
Accident Coverage deductible plan pays number of occurrences maximum per occurrence maximum amount paid by plan
$100/occurrence
80% 2/year $5,000
$10,000/year
$50/occurrence
80% 2/year $2,500
$5,000/year
$50/occurrence
80% 2/year $1,000
$2,000/year Accident Death Benefit plan pays
$25,000
$15,000
$10,000
CIGNA 24-Hour EAP℠ (Included on all plan designs)
The CIGNA 24-Hour Employee Assistance ProgramSM is available day or night for helpful information on a range of health topics. The EAP program includes access to: 24-hour nurse line, mental health assistance (includes 3 in-person consultations per year per condition), and a health information library.
Healthy Rewards® (Included on all plan designs)
Healthy Rewards offers discounts on health products and services such as: weight loss programs, vitamins, vision and dental products. Members will also receive discounts of up to 60% on brand names like Weight Watchers, Jenny Craig, and much more.
Online Tools (Included on all plan designs)
CIGNA provides a variety of online tools available only to our members. They’ll be able to locate network doctors or pharmacies that provide discounts. Members can also track the status of claims that have been submitted.
Cigna Starbridge Limited Medical Plan
Page 8
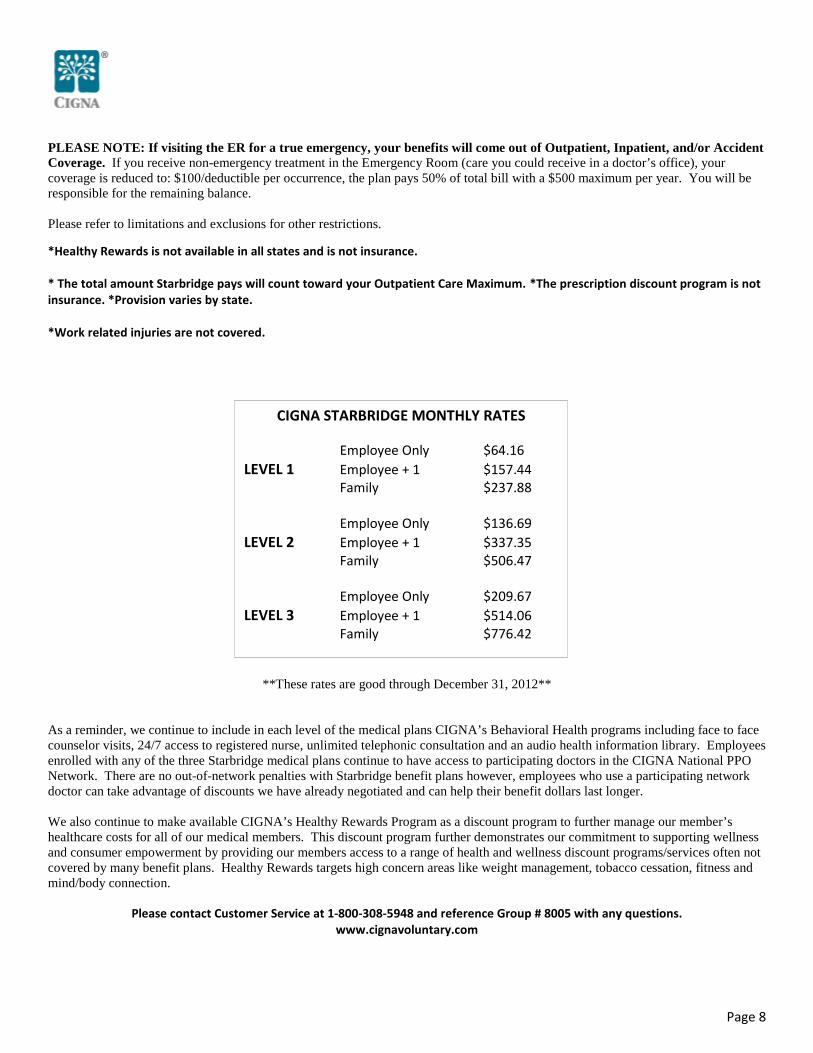
PLEASE NOTE: If visiting the ER for a true emergency, your benefits will come out of Outpatient, Inpatient, and/or Accident Coverage. If you receive non-emergency treatment in the Emergency Room (care you could receive in a doctor’s office), your coverage is reduced to: $100/deductible per occurrence, the plan pays 50% of total bill with a $500 maximum per year. You will be responsible for the remaining balance. Please refer to limitations and exclusions for other restrictions.
*Healthy Rewards is not available in all states and is not insurance. * The total amount Starbridge pays will count toward your Outpatient Care Maximum. *The prescription discount program is not insurance. *Provision varies by state.
*Work related injuries are not covered.
**These rates are good through December 31, 2012** As a reminder, we continue to include in each level of the medical plans CIGNA’s Behavioral Health programs including face to face counselor visits, 24/7 access to registered nurse, unlimited telephonic consultation and an audio health information library. Employees enrolled with any of the three Starbridge medical plans continue to have access to participating doctors in the CIGNA National PPO Network. There are no out-of-network penalties with Starbridge benefit plans however, employees who use a participating network doctor can take advantage of discounts we have already negotiated and can help their benefit dollars last longer. We also continue to make available CIGNA’s Healthy Rewards Program as a discount program to further manage our member’s healthcare costs for all of our medical members. This discount program further demonstrates our commitment to supporting wellness and consumer empowerment by providing our members access to a range of health and wellness discount programs/services often not covered by many benefit plans. Healthy Rewards targets high concern areas like weight management, tobacco cessation, fitness and mind/body connection.
Please contact Customer Service at 1-800-308-5948 and reference Group # 8005 with any questions.
www.cignavoluntary.com
CIGNA STARBRIDGE MONTHLY RATES
Employee Only $64.16 LEVEL 1 Employee + 1 $157.44 Family $237.88 Employee Only $136.69 LEVEL 2 Employee + 1 $337.35 Family $506.47 Employee Only $209.67 LEVEL 3 Employee + 1 $514.06 Family $776.42
Page 9
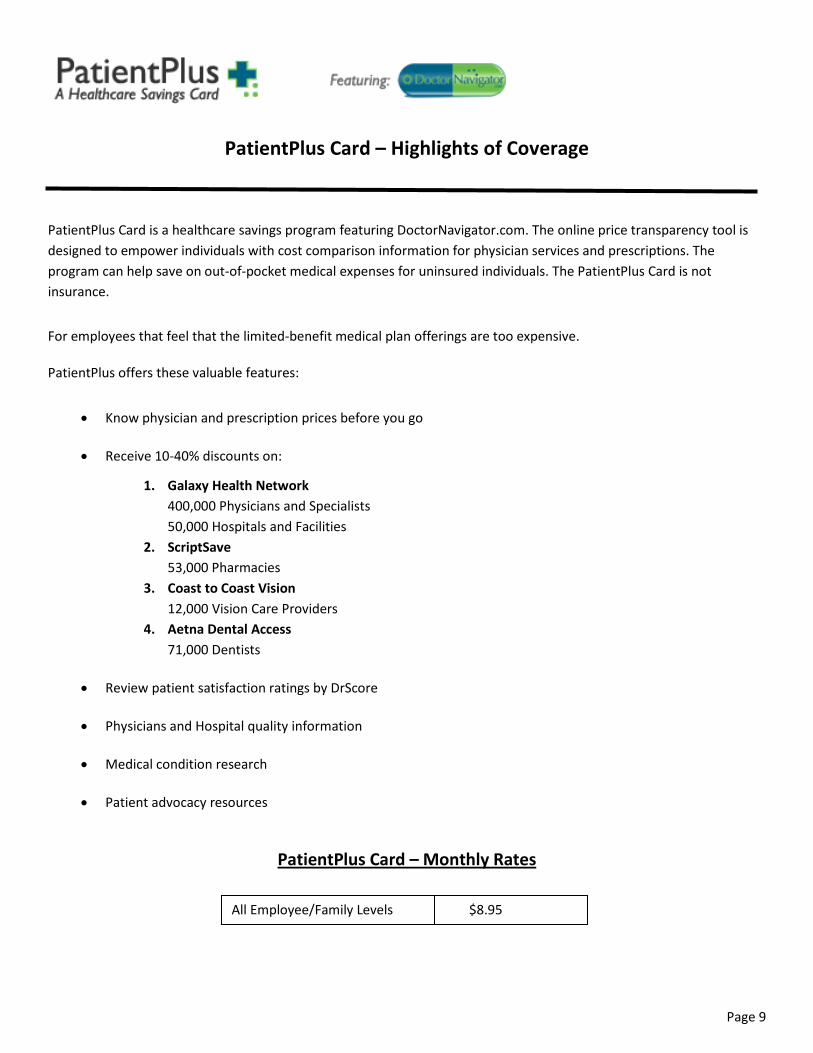
PatientPlus Card – Highlights of Coverage
PatientPlus Card is a healthcare savings program featuring DoctorNavigator.com. The online price transparency tool is designed to empower individuals with cost comparison information for physician services and prescriptions. The program can help save on out-of-pocket medical expenses for uninsured individuals. The PatientPlus Card is not insurance.
For employees that feel that the limited-benefit medical plan offerings are too expensive.
PatientPlus offers these valuable features:
• Know physician and prescription prices before you go
• Receive 10-40% discounts on:
1. Galaxy Health Network 400,000 Physicians and Specialists 50,000 Hospitals and Facilities
2. ScriptSave 53,000 Pharmacies
3. Coast to Coast Vision 12,000 Vision Care Providers
4. Aetna Dental Access 71,000 Dentists
• Review patient satisfaction ratings by DrScore
• Physicians and Hospital quality information
• Medical condition research
• Patient advocacy resources
PatientPlus Card – Monthly Rates
All Employee/Family Levels $8.95
Page 10
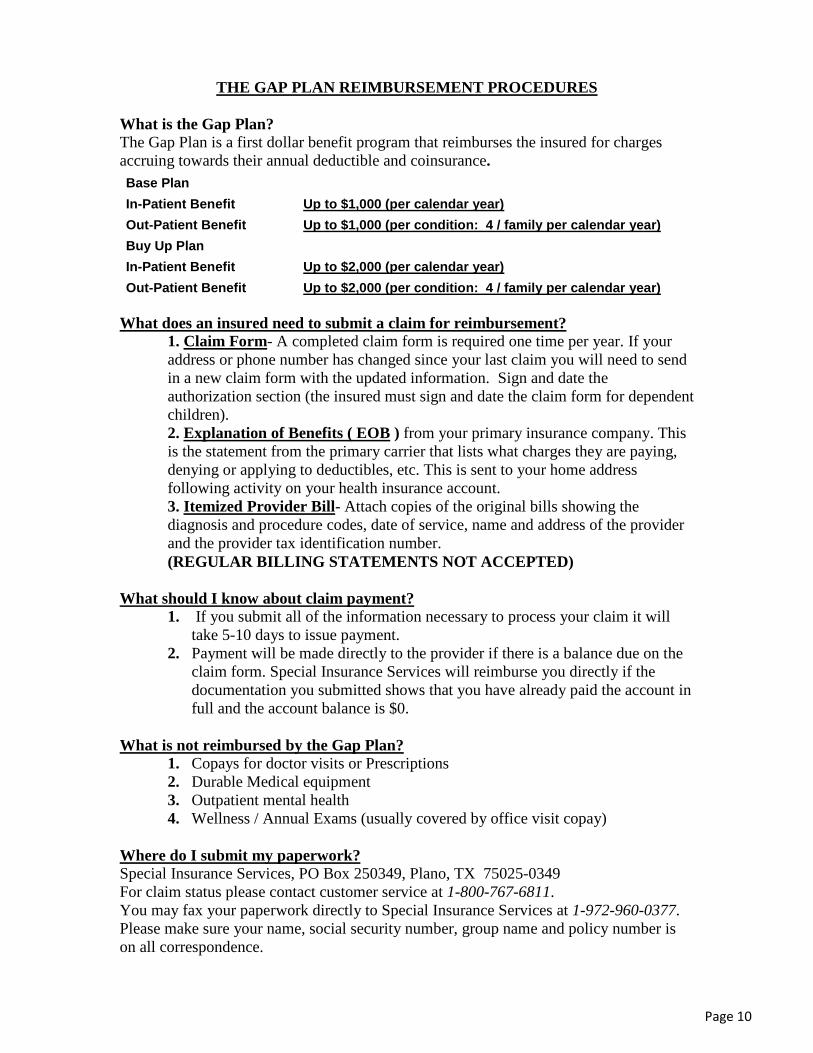
THE GAP PLAN REIMBURSEMENT PROCEDURES
What is the Gap Plan? The Gap Plan is a first dollar benefit program that reimburses the insured for charges accruing towards their annual deductible and coinsurance. Base Plan In-Patient Benefit Up to $1,000 (per calendar year) Out-Patient Benefit Up to $1,000 (per condition: 4 / family per calendar year) Buy Up Plan In-Patient Benefit Up to $2,000 (per calendar year) Out-Patient Benefit Up to $2,000 (per condition: 4 / family per calendar year)
What does an insured need to submit a claim for reimbursement?
1. Claim Form- A completed claim form is required one time per year. If your address or phone number has changed since your last claim you will need to send in a new claim form with the updated information. Sign and date the authorization section (the insured must sign and date the claim form for dependent children). 2. Explanation of Benefits ( EOB ) from your primary insurance company. This is the statement from the primary carrier that lists what charges they are paying, denying or applying to deductibles, etc. This is sent to your home address following activity on your health insurance account. 3. Itemized Provider Bill- Attach copies of the original bills showing the diagnosis and procedure codes, date of service, name and address of the provider and the provider tax identification number. (REGULAR BILLING STATEMENTS NOT ACCEPTED)
What should I know about claim payment? 1. If you submit all of the information necessary to process your claim it will
take 5-10 days to issue payment. 2. Payment will be made directly to the provider if there is a balance due on the
claim form. Special Insurance Services will reimburse you directly if the documentation you submitted shows that you have already paid the account in full and the account balance is $0.
What is not reimbursed by the Gap Plan?
1. Copays for doctor visits or Prescriptions 2. Durable Medical equipment 3. Outpatient mental health 4. Wellness / Annual Exams (usually covered by office visit copay)
Where do I submit my paperwork? Special Insurance Services, PO Box 250349, Plano, TX 75025-0349 For claim status please contact customer service at 1-800-767-6811. You may fax your paperwork directly to Special Insurance Services at 1-972-960-0377. Please make sure your name, social security number, group name and policy number is on all correspondence.
Page 11
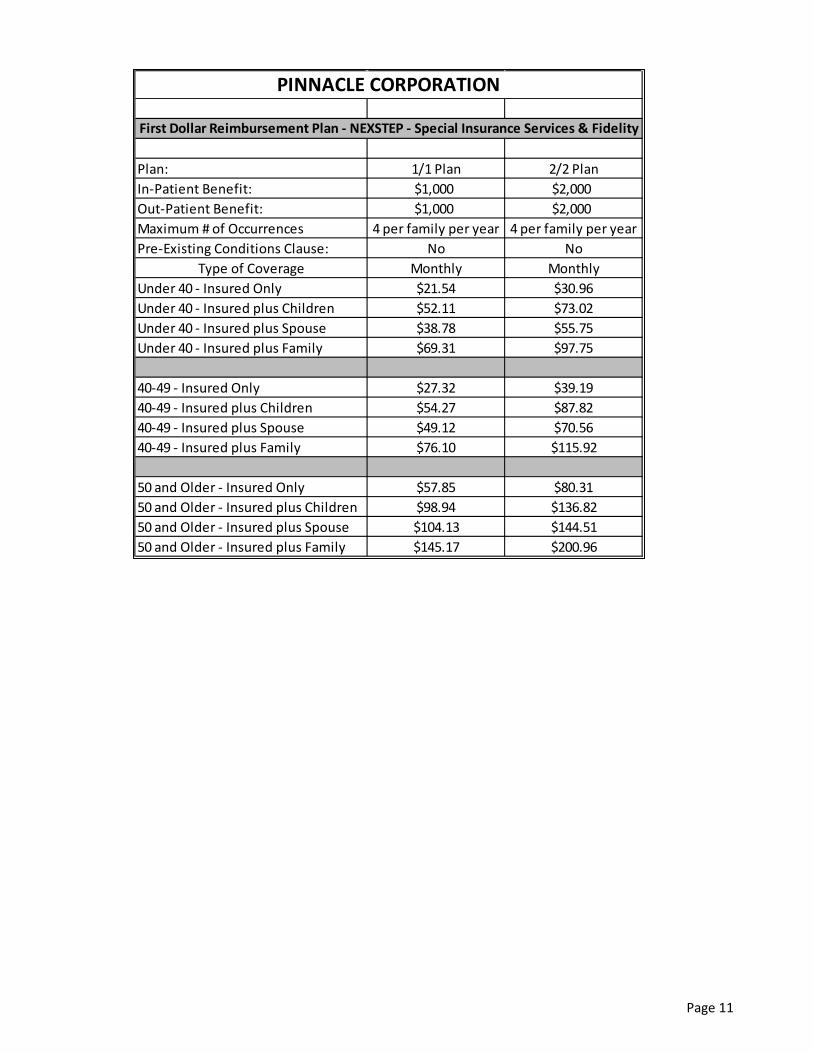
Plan: 1/1 Plan 2/2 PlanIn-Patient Benefit: $1,000 $2,000Out-Patient Benefit: $1,000 $2,000Maximum # of Occurrences 4 per family per year 4 per family per yearPre-Existing Conditions Clause: No No
Type of Coverage Monthly MonthlyUnder 40 - Insured Only $21.54 $30.96Under 40 - Insured plus Children $52.11 $73.02Under 40 - Insured plus Spouse $38.78 $55.75Under 40 - Insured plus Family $69.31 $97.75
40-49 - Insured Only $27.32 $39.1940-49 - Insured plus Children $54.27 $87.8240-49 - Insured plus Spouse $49.12 $70.5640-49 - Insured plus Family $76.10 $115.92
50 and Older - Insured Only $57.85 $80.3150 and Older - Insured plus Children $98.94 $136.8250 and Older - Insured plus Spouse $104.13 $144.5150 and Older - Insured plus Family $145.17 $200.96
First Dollar Reimbursement Plan - NEXSTEP - Special Insurance Services & Fidelity
PINNACLE CORPORATION
Page 12
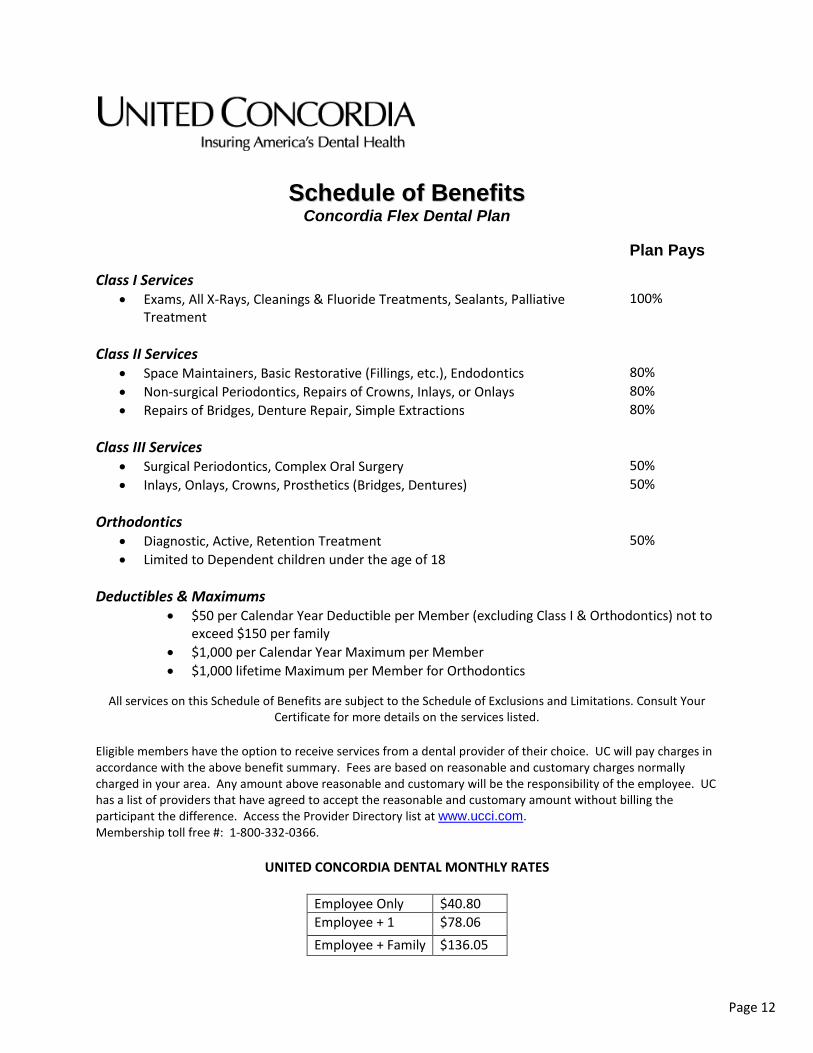
SScchheedduullee ooff BBeenneeffiittss Concordia Flex Dental Plan
Plan Pays
Class I Services • Exams, All X-Rays, Cleanings & Fluoride Treatments, Sealants, Palliative
Treatment 100%
Class II Services
• Space Maintainers, Basic Restorative (Fillings, etc.), Endodontics 80% • Non-surgical Periodontics, Repairs of Crowns, Inlays, or Onlays 80% • Repairs of Bridges, Denture Repair, Simple Extractions 80%
Class III Services
• Surgical Periodontics, Complex Oral Surgery 50% • Inlays, Onlays, Crowns, Prosthetics (Bridges, Dentures) 50%
Orthodontics
• Diagnostic, Active, Retention Treatment 50% • Limited to Dependent children under the age of 18
Deductibles & Maximums
• $50 per Calendar Year Deductible per Member (excluding Class I & Orthodontics) not to exceed $150 per family
• $1,000 per Calendar Year Maximum per Member • $1,000 lifetime Maximum per Member for Orthodontics
All services on this Schedule of Benefits are subject to the Schedule of Exclusions and Limitations. Consult Your
Certificate for more details on the services listed. Eligible members have the option to receive services from a dental provider of their choice. UC will pay charges in accordance with the above benefit summary. Fees are based on reasonable and customary charges normally charged in your area. Any amount above reasonable and customary will be the responsibility of the employee. UC has a list of providers that have agreed to accept the reasonable and customary amount without billing the participant the difference. Access the Provider Directory list at www.ucci.com. Membership toll free #: 1-800-332-0366.
UNITED CONCORDIA DENTAL MONTHLY RATES
Employee Only $40.80 Employee + 1 $78.06 Employee + Family $136.05
Page 13
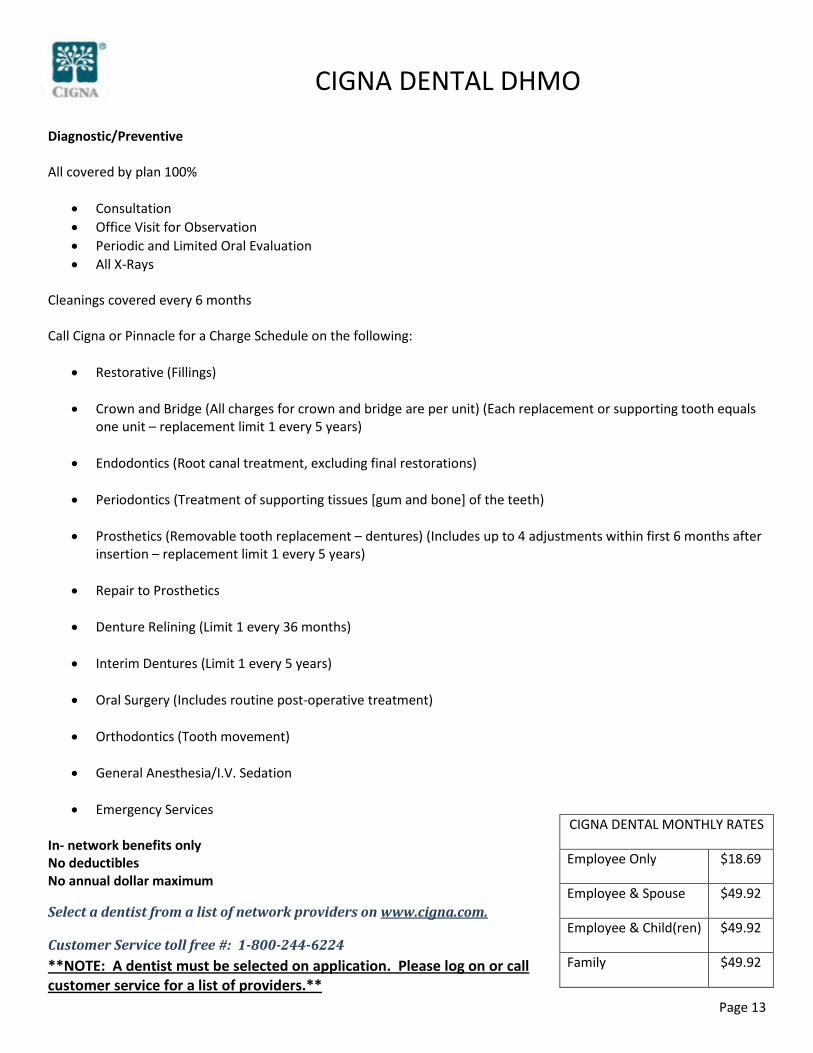
CIGNA DENTAL DHMO
Diagnostic/Preventive All covered by plan 100%
• Consultation • Office Visit for Observation • Periodic and Limited Oral Evaluation • All X-Rays
Cleanings covered every 6 months Call Cigna or Pinnacle for a Charge Schedule on the following:
• Restorative (Fillings)
• Crown and Bridge (All charges for crown and bridge are per unit) (Each replacement or supporting tooth equals one unit – replacement limit 1 every 5 years)
• Endodontics (Root canal treatment, excluding final restorations)
• Periodontics (Treatment of supporting tissues [gum and bone] of the teeth)
• Prosthetics (Removable tooth replacement – dentures) (Includes up to 4 adjustments within first 6 months after
insertion – replacement limit 1 every 5 years)
• Repair to Prosthetics
• Denture Relining (Limit 1 every 36 months)
• Interim Dentures (Limit 1 every 5 years)
• Oral Surgery (Includes routine post-operative treatment)
• Orthodontics (Tooth movement)
• General Anesthesia/I.V. Sedation
• Emergency Services In- network benefits only No deductibles No annual dollar maximum
Select a dentist from a list of network providers on www.cigna.com.
Customer Service toll free #: 1-800-244-6224 **NOTE: A dentist must be selected on application. Please log on or call customer service for a list of providers.**
CIGNA DENTAL MONTHLY RATES
Employee Only $18.69
Employee & Spouse $49.92
Employee & Child(ren) $49.92
Family $49.92
Page 14
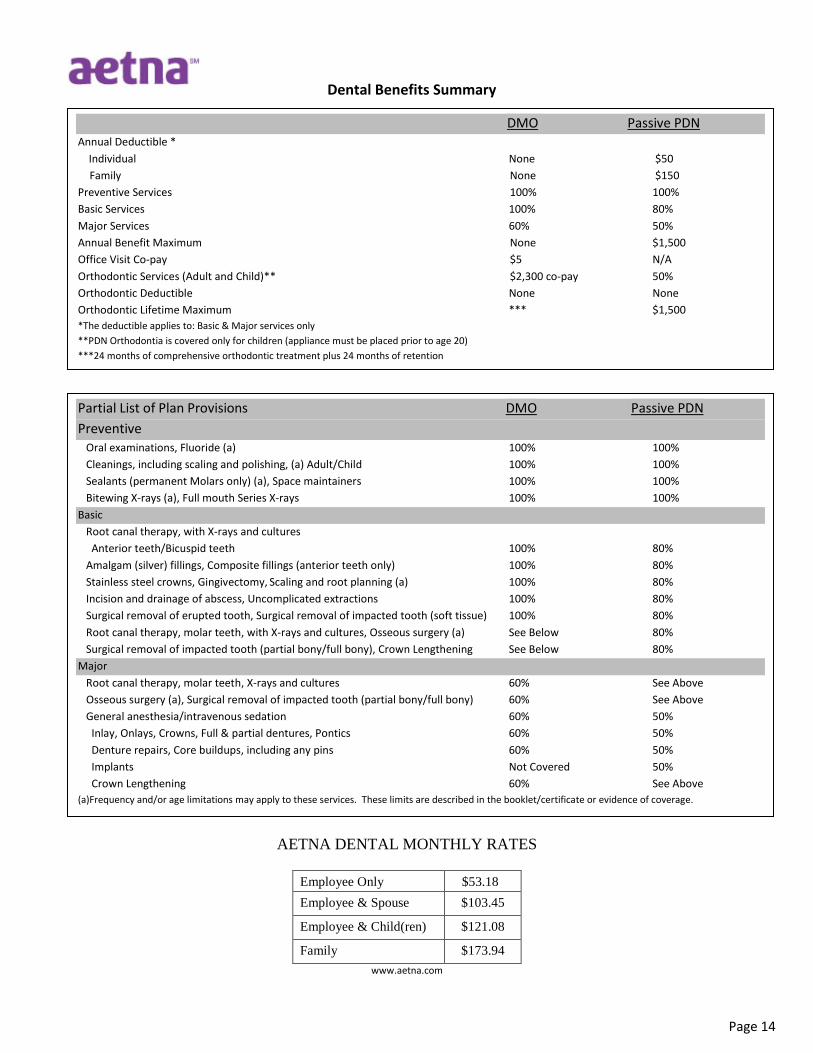
Dental Benefits Summary
AETNA DENTAL MONTHLY RATES
Employee Only
$53.18
Employee & Spouse
$103.45
Employee & Child(ren)
$121.08
Family
$173.94 www.aetna.com
DMO Passive PDN Annual Deductible * Individual None $50
Family None $150 Preventive Services 100% 100% Basic Services 100% 80% Major Services 60% 50% Annual Benefit Maximum None $1,500 Office Visit Co-pay $5 N/A Orthodontic Services (Adult and Child)** $2,300 co-pay 50% Orthodontic Deductible None None Orthodontic Lifetime Maximum *** $1,500 *The deductible applies to: Basic & Major services only **PDN Orthodontia is covered only for children (appliance must be placed prior to age 20) ***24 months of comprehensive orthodontic treatment plus 24 months of retention
Partial List of Plan Provisions DMO Passive PDN Preventive Oral examinations, Fluoride (a) 100% 100% Cleanings, including scaling and polishing, (a) Adult/Child 100% 100% Sealants (permanent Molars only) (a), Space maintainers 100% 100% Bitewing X-rays (a), Full mouth Series X-rays 100% 100% Basic Root canal therapy, with X-rays and cultures Anterior teeth/Bicuspid teeth 100% 80% Amalgam (silver) fillings, Composite fillings (anterior teeth only) 100% 80% Stainless steel crowns, Gingivectomy, Scaling and root planning (a) 100% 80% Incision and drainage of abscess, Uncomplicated extractions 100% 80% Surgical removal of erupted tooth, Surgical removal of impacted tooth (soft tissue) 100% 80% Root canal therapy, molar teeth, with X-rays and cultures, Osseous surgery (a) See Below 80% Surgical removal of impacted tooth (partial bony/full bony), Crown Lengthening See Below 80% Major Root canal therapy, molar teeth, X-rays and cultures 60% See Above Osseous surgery (a), Surgical removal of impacted tooth (partial bony/full bony) 60% See Above General anesthesia/intravenous sedation 60% 50% Inlay, Onlays, Crowns, Full & partial dentures, Pontics 60% 50% Denture repairs, Core buildups, including any pins 60% 50% Implants Not Covered 50% Crown Lengthening 60% See Above (a)Frequency and/or age limitations may apply to these services. These limits are described in the booklet/certificate or evidence of coverage.
0699562 - 11/18/11
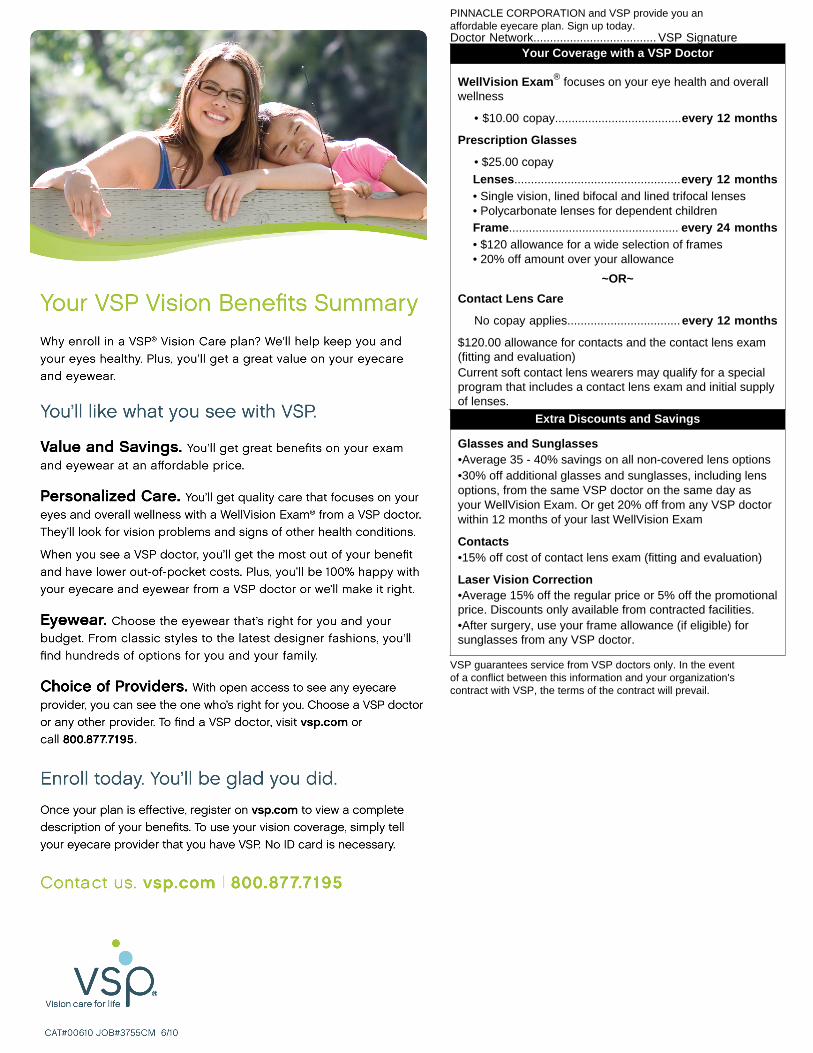
PINNACLE CORPORATION and VSP provide you anaffordable eyecare plan. Sign up today.Doctor Network..................................... VSP Signature
Your Coverage with a VSP Doctor
WellVision Exam® focuses on your eye health and overallwellness
• $10.00 copay......................................every 12 months
Prescription Glasses
• $25.00 copay
Lenses..................................................every 12 months• Single vision, lined bifocal and lined trifocal lenses
• Polycarbonate lenses for dependent childrenFrame................................................... every 24 months• $120 allowance for a wide selection of frames
• 20% off amount over your allowance
~OR~
Contact Lens Care
No copay applies..................................every 12 months
$120.00 allowance for contacts and the contact lens exam(fitting and evaluation)
Current soft contact lens wearers may qualify for a specialprogram that includes a contact lens exam and initial supplyof lenses.
Extra Discounts and Savings
Glasses and Sunglasses •Average 35 - 40% savings on all non-covered lens options •30% off additional glasses and sunglasses, including lensoptions, from the same VSP doctor on the same day asyour WellVision Exam. Or get 20% off from any VSP doctorwithin 12 months of your last WellVision Exam
Contacts •15% off cost of contact lens exam (fitting and evaluation)
Laser Vision Correction •Average 15% off the regular price or 5% off the promotionalprice. Discounts only available from contracted facilities. •After surgery, use your frame allowance (if eligible) forsunglasses from any VSP doctor.
VSP guarantees service from VSP doctors only. In the eventof a conflict between this information and your organization'scontract with VSP, the terms of the contract will prevail.
Page 16
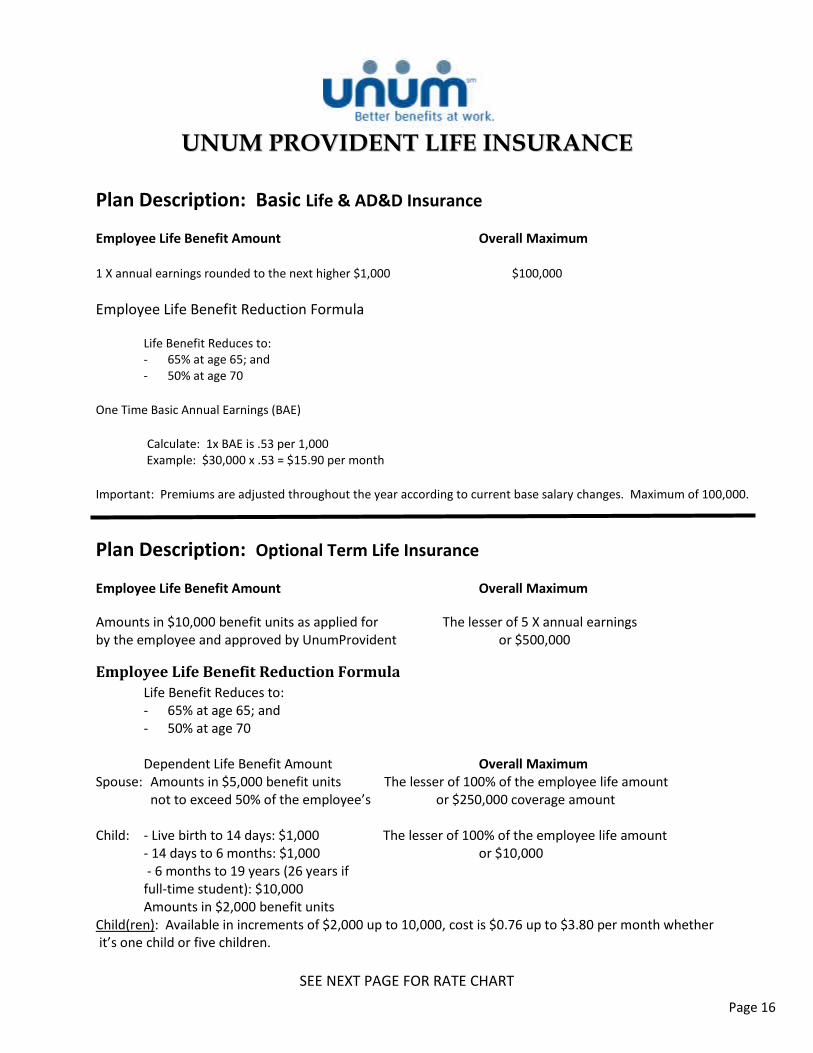
UUNNUUMM PPRROOVVIIDDEENNTT LLIIFFEE IINNSSUURRAANNCCEE
Plan Description: Basic Life & AD&D Insurance
Employee Life Benefit Amount Overall Maximum
1 X annual earnings rounded to the next higher $1,000 $100,000
Employee Life Benefit Reduction Formula Life Benefit Reduces to: - 65% at age 65; and - 50% at age 70
One Time Basic Annual Earnings (BAE)
Calculate: 1x BAE is .53 per 1,000
Example: $30,000 x .53 = $15.90 per month
Important: Premiums are adjusted throughout the year according to current base salary changes. Maximum of 100,000.
Plan Description: Optional Term Life Insurance
Employee Life Benefit Amount Overall Maximum
Amounts in $10,000 benefit units as applied for The lesser of 5 X annual earnings by the employee and approved by UnumProvident or $500,000
Employee Life Benefit Reduction Formula Life Benefit Reduces to: - 65% at age 65; and - 50% at age 70
Dependent Life Benefit Amount Overall Maximum
Spouse: Amounts in $5,000 benefit units The lesser of 100% of the employee life amount not to exceed 50% of the employee’s or $250,000 coverage amount
Child: - Live birth to 14 days: $1,000 The lesser of 100% of the employee life amount - 14 days to 6 months: $1,000 or $10,000 - 6 months to 19 years (26 years if full-time student): $10,000 Amounts in $2,000 benefit units
Child(ren): Available in increments of $2,000 up to 10,000, cost is $0.76 up to $3.80 per month whether it’s one child or five children.
SEE NEXT PAGE FOR RATE CHART
Page 17
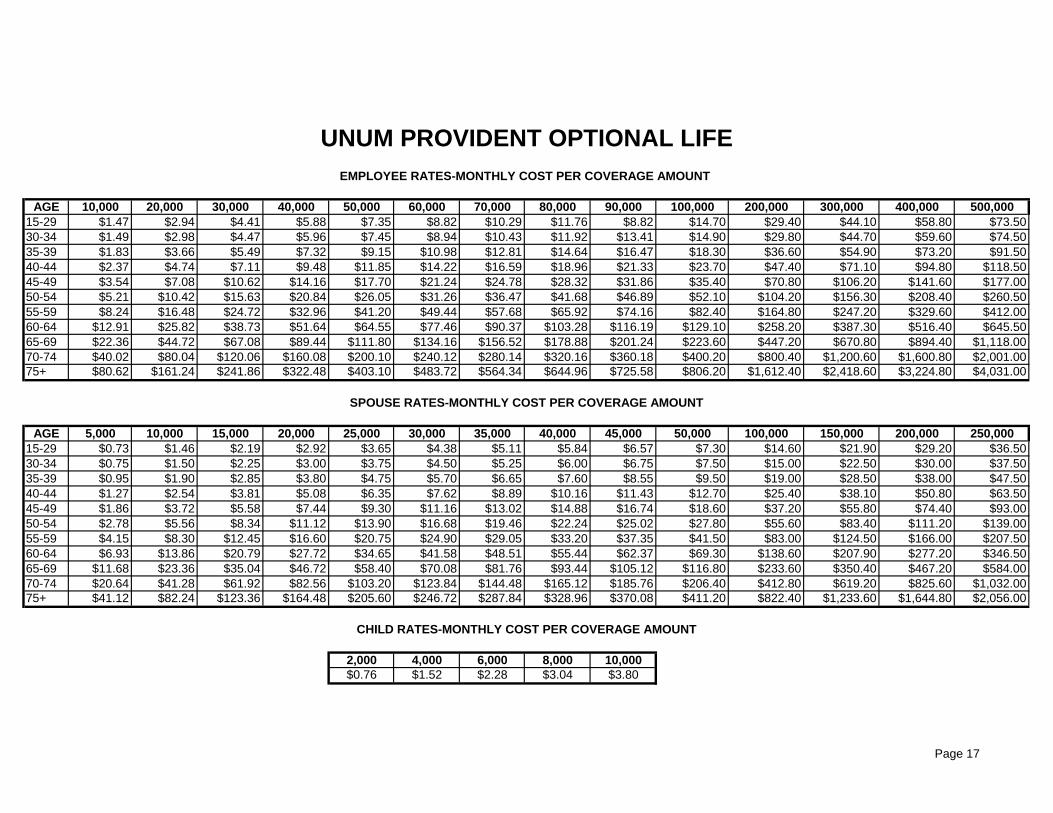
AGE 10,000 20,000 30,000 40,000 50,000 60,000 70,000 80,000 90,000 100,000 200,000 300,000 400,000 500,00015-29 $1.47 $2.94 $4.41 $5.88 $7.35 $8.82 $10.29 $11.76 $8.82 $14.70 $29.40 $44.10 $58.80 $73.5030-34 $1.49 $2.98 $4.47 $5.96 $7.45 $8.94 $10.43 $11.92 $13.41 $14.90 $29.80 $44.70 $59.60 $74.5035-39 $1.83 $3.66 $5.49 $7.32 $9.15 $10.98 $12.81 $14.64 $16.47 $18.30 $36.60 $54.90 $73.20 $91.5040-44 $2.37 $4.74 $7.11 $9.48 $11.85 $14.22 $16.59 $18.96 $21.33 $23.70 $47.40 $71.10 $94.80 $118.5045-49 $3.54 $7.08 $10.62 $14.16 $17.70 $21.24 $24.78 $28.32 $31.86 $35.40 $70.80 $106.20 $141.60 $177.0050-54 $5.21 $10.42 $15.63 $20.84 $26.05 $31.26 $36.47 $41.68 $46.89 $52.10 $104.20 $156.30 $208.40 $260.5055-59 $8.24 $16.48 $24.72 $32.96 $41.20 $49.44 $57.68 $65.92 $74.16 $82.40 $164.80 $247.20 $329.60 $412.0060-64 $12.91 $25.82 $38.73 $51.64 $64.55 $77.46 $90.37 $103.28 $116.19 $129.10 $258.20 $387.30 $516.40 $645.5065-69 $22.36 $44.72 $67.08 $89.44 $111.80 $134.16 $156.52 $178.88 $201.24 $223.60 $447.20 $670.80 $894.40 $1,118.0070-74 $40.02 $80.04 $120.06 $160.08 $200.10 $240.12 $280.14 $320.16 $360.18 $400.20 $800.40 $1,200.60 $1,600.80 $2,001.0075+ $80.62 $161.24 $241.86 $322.48 $403.10 $483.72 $564.34 $644.96 $725.58 $806.20 $1,612.40 $2,418.60 $3,224.80 $4,031.00
AGE 5,000 10,000 15,000 20,000 25,000 30,000 35,000 40,000 45,000 50,000 100,000 150,000 200,000 250,00015-29 $0.73 $1.46 $2.19 $2.92 $3.65 $4.38 $5.11 $5.84 $6.57 $7.30 $14.60 $21.90 $29.20 $36.5030-34 $0.75 $1.50 $2.25 $3.00 $3.75 $4.50 $5.25 $6.00 $6.75 $7.50 $15.00 $22.50 $30.00 $37.5035-39 $0.95 $1.90 $2.85 $3.80 $4.75 $5.70 $6.65 $7.60 $8.55 $9.50 $19.00 $28.50 $38.00 $47.5040-44 $1.27 $2.54 $3.81 $5.08 $6.35 $7.62 $8.89 $10.16 $11.43 $12.70 $25.40 $38.10 $50.80 $63.5045-49 $1.86 $3.72 $5.58 $7.44 $9.30 $11.16 $13.02 $14.88 $16.74 $18.60 $37.20 $55.80 $74.40 $93.0050-54 $2.78 $5.56 $8.34 $11.12 $13.90 $16.68 $19.46 $22.24 $25.02 $27.80 $55.60 $83.40 $111.20 $139.0055-59 $4.15 $8.30 $12.45 $16.60 $20.75 $24.90 $29.05 $33.20 $37.35 $41.50 $83.00 $124.50 $166.00 $207.5060-64 $6.93 $13.86 $20.79 $27.72 $34.65 $41.58 $48.51 $55.44 $62.37 $69.30 $138.60 $207.90 $277.20 $346.5065-69 $11.68 $23.36 $35.04 $46.72 $58.40 $70.08 $81.76 $93.44 $105.12 $116.80 $233.60 $350.40 $467.20 $584.0070-74 $20.64 $41.28 $61.92 $82.56 $103.20 $123.84 $144.48 $165.12 $185.76 $206.40 $412.80 $619.20 $825.60 $1,032.0075+ $41.12 $82.24 $123.36 $164.48 $205.60 $246.72 $287.84 $328.96 $370.08 $411.20 $822.40 $1,233.60 $1,644.80 $2,056.00
2,000 4,000 6,000 8,000 10,000$0.76 $1.52 $2.28 $3.04 $3.80
UNUM PROVIDENT OPTIONAL LIFEEMPLOYEE RATES-MONTHLY COST PER COVERAGE AMOUNT
CHILD RATES-MONTHLY COST PER COVERAGE AMOUNT
SPOUSE RATES-MONTHLY COST PER COVERAGE AMOUNT

Page 18
PRINCIPAL DISABILITY PLAN
Your group short term disability benefits All Members Eligible Employees All active, full-time employees (except part-time, seasonal,
temporary or contract employees) who work at least 30 hours per week
B E N E F I T Q U A L I F I C A T I O N Definition of Disability Zero day residual disability Income Loss Requirement 20% Elimination Period Benefits begin on:
The 1st day for disability due to injury The 8th day for disability due to sickness
B E N E F I T S P A Y A B L E Benefit Percentage 60% of predisability earnings Definition of Earnings Weekly average of W-2 earnings for the prior 2 calendar year(s) Maximum Weekly Benefit $1,500 Minimum Weekly Benefit $15 Coordination of Benefits Direct integration Social Security Integration Primary and family Benefit Duration 13 weeks
R E H A B I L I T A T I O N B E N E F I T S
Reasonable Accommodation Benefit $500
A D D I T I O N A L F E A T U R E S Coverage for non work-related disabilities Mandatory rehabilitation The policy does not provide state mandated disability benefits in CA, NY, NJ, RI or HI.
RATE SHEET (EXAMPLES)
ANNUAL SALARY WEEKLY BENEFIT
APPROXIMATED MONTHLY COST
$10,000.00 $115.38 $13.23
$15,000.00 $173.08 $19.85
$20,000.00 $230.77 $26.47
$25,000.00 $288.46 $33.09
$30,000.00 $346.15 $39.70
$40,000.00 $461.54 $52.94
$50,000.00 $576.92 $66.17
$60,000.00 $692.31 $79.41
$100,000.00 $1,153.85 $132.35
Page 19
AFLAC NOTICE TO EMPLOYEES
AFLAC is the leading provider of Guaranteed Renewable insurance programs in the world. Their programs provide CASH benefits to the plan holder, and coverage is available for spouses and children. Some of the plans being offered through Payroll Deduction are: Accident Indemnity, Cancer Indemnity, Short Term Disability (2 year maximum coverage), Personal recovery Plus (Heart Attacks, strokes, comas, etc) and a Hospital Indemnity Plan. A brief description of each is as follows: PERSONAL ACCIDENT INDEMNITY PLAN AFLAC’s newest and most innovative policy is our Personal Accident Indemnity Plan and offers a full range of benefits. Some important features of the insurance policy are:
• Accident Emergency Treatment Benefit • Accidental-Death and Dismemberment Benefits • Initial Accident Hospitalization Benefit • Accident Hospital Confinement Benefit • Intensive Care Unit Confinement Benefit • Wellness Benefit • Major Diagnostic Exams, Physical Therapy
Benefit, Appliances Benefit, Prosthesis Benefit • Blood/Plasma/Platelets Benefit, Ambulance
Benefit, Transportation Benefit & Family Lodging Benefit
PERSONAL CANCER INDEMNITY PLAN Our Cancer Expense Policy provides benefits to assist you in meeting the high cost of cancer treatment. Some important features of the insurance policy are:
• First Occurrence Benefit • Transportation and Lodging Benefit • Hospital Confinement Benefit • Hospice Benefit • Outpatient Hospital Surgical Benefit • Any many more…..
PERSONAL SHORT-TERM DISABILITY AFLAC’s Personal Short-Term Disability insurance is your personal income protection plan; it is designed to help close the financial gap that can be created by your being disabled. Some of the Important features of the insurance policy are:
• Different benefit periods are available. • 14-day waiting period. • Guaranteed-renewable to age 70, subject to the
company’s right to change premium by class. • Short-Term Disability insurance stays with you
regardless of job or occupation change. PERSONAL RECOVERY PLUS Some important features of the insurance policy are:
• First Occurrence Benefit • Hospital Confinement Benefit • Continuing Care Benefits for Heart Attack &
Coronary Artery Bypass Surgery • Stroke, Coma & Paralysis
• Ambulance Benefit • Transportation Benefit
HOSPITAL INDEMNITY Hospital Indemnity Insurance Policy (H.I.P.) was designed to help cover the rising costs of hospital confinement. Some important features of the insurance policy are:
• Annual Hospitalization Confinement Benefit • Surgical Benefit • Invasive Diagnostic Exams • Plus…more
If interested in any of the policies listed above, or for further information please contact the Benefits Dept. at 210-344-2088 to request for the AFLAC representative to contact you for an on-site presentation.