Embed Size (px)
Citation preview

Annual Cost of Care for Crohn’s Disease:A Payor PerspectiveBrian G. Feagan, M.D., Mary Glenn Vreeland, M.H.A., Leanne R. Larson, M.H.A., andMohan V. Bala, Ph.D.University of Western Ontario, London, Ontario, Canada; Ovation Research Group, Highland Park, Illinois;and Centocor, Inc., Malvern, Pennsylvania
OBJECTIVE: The aim of this study was to estimate the annualcost of care of patients with Crohn’s disease according totreatment setting.
METHODS: Using a 1994 integrated claims database, pa-tients with a Crohn’s-related medical claim (ICD-9 code555) from 10/01/94 to 09/30/95 were included in this anal-ysis. These patients were stratified into three mutually ex-clusive disease severity groups: group 1, required hospital-ization for Crohn’s; group 2, required chronicglucocorticoid or immunosuppressive drug therapy for.6months; group 3, all remaining patients. Direct charges(based on reimbursement) and utilization of resources werereported for each group.
RESULTS: Six-hundred-seven patients were analyzed:117(19%) in group 1, 31(5%) in group 2, and 459(76%) ingroup 3. Average age of all patients was 48 years and 43%of these patients were men. Average annual charges for allpatients totaled $12,417. Group 1 patients experienced thehighest mean charges ($37,135), whereas patients in groups2 and 3 incurred $10,033 and $6,277. Approximately 25%of patients accounted for 80% of the total charges.
CONCLUSIONS: Crohn’s disease is associated with high cost.Although a minority of Crohn’s patients required hospital-ization, they tended to have higher utilization and wereresponsible for a majority of total expenditures. New ther-apies have the potential to reduce overall cost of care, if theyprevent Crohn’s-related hospitalizations. (Am J Gastroen-terol 2000;95:1955–1960. © 2000 by Am. Coll. of Gastro-enterology)
INTRODUCTION
Crohn’s disease is a chronic, relapsing inflammatory disor-der of the gastrointestinal tract that affects approximately380,000 to 480,000 people in the United States (1). Asubstantial body of data is currently available regarding thebiology, epidemiology, and clinical course of Crohn’s dis-ease. The etiology of Crohn’s, however, remains unclear(2). Because the disease typically presents in early adult-hood (2, 3), people affected with Crohn’s disease sufferconsequences throughout much of their working lives. As a
result, patients frequently experience diminished productiv-ity (4) and decreased quality of life (5). Once diagnosed, apatient’s course of illness often fluctuates, varying amongmild, moderate, and severe disease states, or remission (6).Because patients require frequent monitoring and medicalcare, the expenditures for these services can accumulate toimportant levels over the course of a lifetime.
Since patients with Crohn’s disease have a near normallife expectancy, the focus of treatment is on controllingsymptoms and improving quality of life (7). Current medicalmanagement of Crohn’s includes aminosalicylates, cortico-steroids, immunomodulators, and antibiotics. The benefitsof aminosalicylates and antibiotics are debatable, whereascorticosteroids and immunomodulators are associated with awide range of adverse effects (7). Although patients expe-riencing mild symptoms may enter remission with medicaltherapy, others continue to experience symptoms despitetreatment. Severely ill patients may require hospitalizationor surgery, or both. The latter group of individuals is likelyresponsible for most of the treatment costs (8, 9).
Few studies have examined the costs of Crohn’s disease.The most frequently referenced cost information was pub-lished in 1992 by Hay and Hay (8, 9) who evaluated medicalcharges at a major San Francisco Bay area teaching hospital.These study data estimated an average annual per patientcharge of $6,561 (8, 9) and found that 56% of the costsassociated with Crohn’s treatment are incurred as a conse-quence of hospitalization. These findings suggest that theprovision of care for inpatients is the most costly element oftreatment.
Because there have been few subsequent initiatives toexamine the cost of Crohn’s, we performed a claims-basedeconomic analysis to explore the settings in which Crohn’spatients currently receive care and to examine the potentialfor cost savings.
MATERIALS AND METHODS
This retrospective claims analysis examined the costs ofcare of Crohn’s disease. Direct-charges (defined as theamount reimbursed by the insurer) and resource utilizationwere obtained from Hewitt Associates, a benefits consulting
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 95, No. 8, 2000© 2000 by Am. Coll. of Gastroenterology ISSN 0002-9270/00/$20.00Published by Elsevier Science Inc. PII S0002-9270(00)01053-4

firm that processes prescription drug and medical claimsfrom employees of approximately 50 of the largest employ-ers in the United States. This integrated database (10) in-cludes claims from January 1992 through December 1996and represents 7.5 million life-years of follow-up. Medicalclaims in this database were identified according to ICD-9codes, and medication names appear on all pharmacyclaims. These coding and naming conventions allowed allclaims to be identified and then categorized.
To be eligible for this analysis, patients had to be con-tinuously enrolled in their health plans for 3 years (January1, 1994 to December 31, 1996). From this population, datafrom patients with a Crohn’s-related medical claim (ICD-9code 555) between October 1, 1994, to September 30, 1995,were selected for analysis. Using this primary diagnosticgroup, patients were then stratified into three mutually ex-clusive disease severity groups: group 1, required an inpa-tient hospitalization associated with a primary/secondarydiagnosis of Crohn’s disease; group 2, required aggressivepharmacotherapy, defined as chronic glucocorticoid (.10mg/day) or immunosuppressive drug (purine antimetabo-lites/methotrexate) therapy, for.6 months; or group 3, allremaining patients.
After all patients were categorized, we also examined thecharacteristics of patients with fistulizing Crohn’s. Thesepatients were identified as Crohn’s patients with a fistula-related medical claim (ICD-9 code 565.1 or 569.81) be-tween October 1, 1994, and September 30, 1995.
Patient demographics (age and gender) were examinedfor each group. Healthcare resource utilization and chargeswere calculated for a common period (October 1, 1994 toSeptember 30, 1995). Medical claims were further identifiedaccording to place of service: inpatient hospitalization, out-patient clinic, physician office, emergency room, homehealth, skilled nursing facility, and other (e.g., psychiatricservices, rehabilitation units, unknown place of service).Annual direct charges, reflecting the amount reimbursed bythe insurer, were calculated based on medical and pharmacyresource utilization. Appropriate descriptive statistics wereused to evaluate potential intra- and intergroup differencesin patient characteristics, service type, place of service, andother variables. To test for group differences in continuousvariables (e.g., age, cost, claims), analysis of variance andttests were used; categorical variables were tested using theChi-square statistic.
RESULTS
Table 1 shows that a total of 607 patients were identifiedwith a Crohn’s-related medical claim during the selectedtime period: 117 (19%) in group 1, 31 (5%) in group 2, and459 (76%) in group 3. When all patients (n5 607) wereconsidered, the average age was 48 years; 43% of thispopulation were men. The average age within the patientgroups was 48.9 years in group 1, 50.0 years in group 2, and47.8 years in group 3. Within these same groups, menconstituted 35%, 65%, and 43%, respectively, of the patientpopulation.
Table 2 presents both average and median charges bydisease severity group. The aggregate average annualizedper patient charge for all patients was $12,417; this totalcomprised $11,973 in medical service charges and $444 indrug treatment. Group 1 patients were associated with thegreatest overall average charges at $37,135; the majority ofthese charges ($36,407) were for medical services. Theaverage total charges for groups 2 and 3 patients were$10,033 and $6,277, respectively. The annual mediancharges followed a similar pattern.
Further analyses were undertaken to examine averagecharges according to the place of service in which specificmedical resources were consumed (Table 3). These resultsrevealed that, for all patients, inpatient hospitalizations($7,115) and outpatient services ($2,936) were the largestcontributors to overall charges. These charges were fol-lowed by physician office visits ($1,054) and prescriptionmedications ($444). Group 1 patients incurred the greatestcharges for inpatient hospitalizations ($28,283), whereasgroup 2 patients experienced considerable charges for pre-scription medications ($1,363).
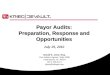
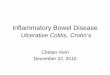
When charges for all patients were examined, the major-ity (57%) were attributed to inpatient hospitalizations; thisresult is illustrated in Figure 1. Figures 2 to 4 show thatgroup 1 patients had 76% of overall charges related tohospitalizations, whereas patients in groups 2 and 3 had23% and 33%, respectively. Inpatient charges incurred bygroup 1 patients reflect both Crohn’s-related admissions aswell as admissions for other reasons. Patients in groups 2and 3, by definition, were not hospitalized for Crohn’s. Theymay, however, have been admitted for other medical/surgi-cal reasons. When charges were examined for all patients, itwas notable that 25% of patients accounted for 80% of thetotal charges (Fig. 5). This group consisted primarily of
Table 1. Demographics by Group
DemographicCharacteristics
Group 1(n 5 117)
Group 2(n 5 31)
Group 3(n 5 459)
pValue*
AllPatients
(n 5 607)
Average age (yr) 48.9 50.0 47.8 0.656 48.0Percent men 35% 65% 43% 0.012 43%
* p value represents differences among groups 1, 2, and 3.
1956 Feagan et al. AJG – Vol. 95, No. 8, 2000

patients in group 1, indicating that hospitalization is animportant cost contributor.
Table 4 shows medication use among the different patientgroups. Steroids were used in a large proportion of group 1and 2 patients. An increased use of antidepressants was alsoobserved in patients in groups 1 and 2 compared to patientsin group 3.
Among the 607 Crohn’s disease patients, a total of 27patients (56% in group 1, 7% in group 2 and 37% in group3) were identified with a fistula-related medical claim. Thesepatients had an average annual cost of treatment of $31,370(Table 5). A majority of these charges ($22,252) wereassociated with the provision of inpatient services.
DISCUSSION
These data show that Crohn’s disease is associated with highcost. This retrospective analysis of a large benefit claimsdatabase provided a cross-sectional view of the healthcareresources utilized, and their associated charges. These anal-yses show that, despite recent advances in treatment, the
cost of treating patients with Crohn’s disease remains sub-stantial.
Our data confirm that hospitalization is an importantcontributor to the overall costs of the disease, supporting theearlier findings of Hay and Hay as well as a recent Univer-sity of Chicago study (which estimated the cost of a surgicaladmission at over $25,000) (11). In our study, 57% of totalcosts were associated with hospitalization. Interestingly,these results are very similar to those of Hay and Hay, whichfound that 56% of the total costs of managing Crohn’sdisease were associated with hospitalization (8). Despiterecent emphasis on preventative disease management strat-egies and on outpatient care, hospitalization remains a sub-stantial and costly component of Crohn’s disease care.Moreover, evidence from this analysis suggests that patientsrequiring hospitalization tend to have increasedoverall uti-lization and, as a result, are responsible for a majority of thetotal expenditures.
Of the patients in our database, we found that 19% werehospitalized (group 1), and another 5% required aggressivemedical therapy (group 2) in the chosen year. The 24% of
Table 2. Charges by Group (per Patient per Year)
Type of ClaimsGroup 1
(n 5 117)Group 2(n 5 31)
Group 3(n 5 459)
pValue*
All Patients(n 5 607)
MedicalAverage (95% CI) $36,407 $8,670 $5,967 0.0001 $11,973
($27,584, $45,231) ($3,422, $13,917) ($4,702, $7,232) ($9,802, $14,143)Median (IQR) $20,982 $3,533 $2,302 $3,283
($11,404, $35,535) ($1,935, $12,810) ($924, $5,038) ($1,258, $11,404)Pharmacy
Average (95% CI) $728 $1,363 $310 0.0004 $444($326, $1,130) ($991, $1,735) ($155, $465) ($297, $591)
Median (IQR) $926 $1,089 $459 $595($280, $2,155) ($565, $2,244) ($160, $1,005) ($207, $1,317)
TotalAverage (95% CI) $37,135 $10,033 $6,277 0.0001 $12,417
($28,227, $46,043) ($4,666, $15,401) ($5,006, $7,547) ($10,226, $14,607)Median (IQR) $21,671 $5,581 $2,703 $3,668
($11,738, $35,535) ($2,888, $13,723) ($1,063, $5,865) ($1,417, $12,107)
* p value represents differences among groups 1, 2, and 3.CI 5 confidence interval; IQR5 interquartile range.
Table 3. Average Charge by Place of Service and Group (per Patient per Year)
Type of ServiceGroup 1
(n 5 117)Group 2(n 5 31)
Group 3(n 5 459)
pValue†
AllPatients
(n 5 607)
Inpatient* $28,283 $2,312 $2,043 0.0005 $7,115Outpatient $4,737 $4,438 $2,376 0.0001 $2,936MD office $1,226 $1,515 $979 0.0325 $1,054Medications $728 $1,363 $310 0.0004 $444Emergency room $619 $113 $102 0.1909 $202Home care $884 $23 $215 0.8230 $334Skilled nursing facility $371 $2 $168 0.0359 $199Other $287 $267 $86 0.1338 $134Total $37,135 $10,033 $6,277 0.0001 $12,417
* Hospitalizations include those associated with Crohn’s as well as non-Crohn’s-related. As a result of patient stratification, patients in groups 2and 3 did not have anyCrohn’s-related hospitalizations.
† p value represents differences among groups 1, 2, and 3.
1957AJG – August, 2000 Annual Cost of Crohn’s Disease

Crohn’s disease patients who belong to groups 1 and 2represent the moderate-to-severe, treatment refractory sub-set of Crohn’s disease patients who incur substantial costs.
We also found that patients with fistulae incurred sub-stantial charges ($31,370 per year). This population of pa-tients contributed to both higher cost of hospitalization forCrohn’s disease, as well as the higher cost of overall care.As is usually noted in cost-of-illness studies, a population isresponsible for a disproportionate amount of the charges,which explains the difference between median and averagecosts. Improvements in care directed toward these patients
may present an opportunity to impact the clinical and eco-nomic outcomes of this disease.
It is important to note the limitations of this study, whichwas a retrospective analysis of a claims database. This studycaptured direct charges as reported through patient claims.A Crohn’s disease patient would have been included in theanalysis only if the patient had a medical claim with anICD-9 code of 555. Because many patients with mild dis-ease would not actively seek treatment, patients with lesssevere forms of illness may have been excluded from thisdatabase. In contrast, Silverstein et al. (12) recently used a
Figure 1. Charge distribution by place of service and group (allpatients).
Figure 2. Charge distribution by place of service and group (group1 patients).
Figure 3. Charge distribution by place of service and group (group2 patients).
Figure 4. Charge distribution by place of service and group (group3 patients).
1958 Feagan et al. AJG – Vol. 95, No. 8, 2000

Markov model to project the lifetime clinical course andcosts of Crohn’s disease in a 24-year population-based in-ception cohort. This model accounted for time spent in eachCrohn’s disease state as well as respective lifetime costs.When all patients were considered, the annual direct med-
ical cost of the disease was estimated at $4,466 (1996 USdollars).
These contrasting findings ($4,466vs$12,417) are likelyattributable to differences in disease severity of the cohortsand differences in estimates based on the use of costs (MayoClinic) versuscharges (current study). Patients in the MayoClinic cohort include a spectrum of patients with widelyvarying disease severity, whereas patients in the retrospec-tive analysis are reflective of those actively incurringcharges. From a payor’s perspective, however, our resultsare a valid and accurate representation of disease-relatedexpenditures.
Also, when working with claims data, it is difficult tospecifically define “attributable” charges. For example, inthis analysis we defined Crohn’s-related hospitalization asan inpatient admission with a primary/secondary diagnosisof Crohn’s disease (ICD-9 555). Because Crohn’s is a con-dition that is associated with a continuum of intestinal andextraintestinal complications, this definition excluded ad-missions occurring as a result of comorbid conditions andcomplications.
This study also did not address the issue of indirect costsincurred by patients with Crohn’s disease. Hay and Hay (8)estimate these disability costs-of-illness at approximately$0.6 to $1.1 billion annually and approximate that between5% and 10% of all patients with inflammatory bowel diseaseare so greatly incapacitated that they are unable to work.
Key to Figures 1–4.
Figure 5. Proportion of charges by proportion of patients.
1959AJG – August, 2000 Annual Cost of Crohn’s Disease

Although our study was not able to capture these costs,nonetheless, they are of great economic consequence, andare of increasing importance to employers, payors, andpatients alike.
In conclusion, our study provides new informationregarding the cost of treating Crohn’s disease. The in-creased levels of resource utilization—and resultantcost— of patients in groups 1 and 2 reflect the currentlimitations in the medical management of Crohn’sdisease. Opportunities remain for improved treatmentfrom both clinical and economic perspectives in thesepatient groups. With the development of new thera-pies, it is possible that fewer hospitalizations will berequired to manage this disease. Given the high cost ofhospitalizations, these newer therapies may contribute toan overall reduction in the cost of managing Crohn’sdisease in specific groups of patients.
ACKNOWLEDGMENT
The development of this manuscript was supported by agrant from Centocor, Inc., Malvern, PA.
Reprint requests and correspondence:Mary Glenn Vreeland,M.H.A., Ovation Research Group, 600 Central Avenue, HighlandPark, IL 60035.
Received Oct. 4, 1999; accepted Feb. 25, 2000.
REFERENCES1. Calkins B, Mendeloff A. Epidemiology of inflammatory
bowel disease. Epidemiol Rev 1996;8:60–91.2. Tooson JD, Varilek GW. Inflammatory diseases of the colon.
Inflammatory Dis 1998;98:46–74.3. Eisen GM, Sandler RS. Update on the epidemiology of IBD.
Prog Inflammatory Bowel Dis 1994;15:1–8.4. Wyke RJ, Edwards FC, Allan RN. Employment problems and
prospects for patients with inflammatory bowel disease. Gut1998;29:1229–35.
5. Gregor JC, McDonald JWD, Klar N, et al. An evaluation of theutility measurement in Crohn’s disease. Inflammatory BowelDis 1997;3:265–76.
6. Elton E, Hanauer SB. Review article: The medical managementof Crohn’s disease. Aliment Pharmacol Ther 1996;10:1–22.
7. Hanauer SB, Schulman MI. New therapeutic approaches. Gas-troenterol Clin North Am 1998;24:523–40.
8. Hay JW, Hay AR. Inflammatory bowel disease: costs-of-illness. J Clin Gastroenterol 1992;14:309–17.
9. Hay AR, Hay JW. Inflammatory bowel disease. J Clin Gas-troenterol 1992;14:318–27.
10. Hewitt Associates. Integrated Health Information System(IHIS) normative database; 1994.
11. Cohen RD, Larson LR, Roth JM, et al. The cost of hospitaliza-tions in Crohn’s disease. Am J Gastroenterol 2000;95:524–30.
12. Silverstein MD, Loftus EV, Sandborn WJ, et al. Clinical courseand costs of care for Crohn’s disease: Markov model analysis ofa population-based cohort. Gastroenterology 1999;117:49–57.
Table 4. Medication Use by Group
MedicationName
Group 1(n 5 117)
Group 2(n 5 31)
Group 3(n 5 459)
All Patients(n 5 607)
N (%) N (%) N (%) N (%)
Sulfasalazine 39 33% 8 26% 12 3% 59 10%Mesalamine 49 42% 13 42% 22 5% 84 14%Prednisone 43 37% 16 52% 30 7% 89 15%Methotrexate 0 0% 3 10% 0 0% 3 ,1%Azathioprine 0 0% 5 16% 6 1% 11 2%6-mercaptopurine 0 0% 15 48% 6 1% 21 3%Cyclosporine 1 1% 1 3% 0 0% 2 ,1%Antidepressants 10 9% 4 13% 15 3% 29 5%
Table 5. Fistula Patients: Demographics and Average Chargesby Place of Service (per Patient per Year)
All Patients(n 5 27)
Average age (yr) 46.1Percent men 41%Type of service $ (%)
Inpatient $22,252 71%Outpatient $5,545 18%MD office $1,168 4%Medications $812 3%Emergency room $59 ,1%Home care $1,031 3%Skilled nursing facility $4 ,1%Other $499 2%Total $31,370 100%
1960 Feagan et al. AJG – Vol. 95, No. 8, 2000