Embed Size (px)
Citation preview
Annual Nursing ConferenceProgramme8:30 - 9:00 Registration and breakfast
9:00 - 9.15 Welcome - Helen Davenport, Director of Nursing, Quality and Governance - WFCCG9:15 - 9:30 Setting the scene – Dr Jackie Morris, Vice President - Patients Association9:30 - 9:45 Enhancing support to care homes – Gail Foord, Associate Director of Strategic Commissioning and Jenny
Waller, Commissioning Support Manager - WFCCG09:45 - 10:00 Discharge to access - Paul Larrisey, Deputy Nurse Director of Safeguarding and Continuing Healthcare - WFCCG
10:00 - 10:25 Introductions and reflections10:25 - 10:45 Optimising medicines for people residing in care homes - Ada Onyeagwara,
Assistant Director of Medicines Optimisation; Dr Sabeena Pheerunggee, Named GP for safeguarding - WFCCG andAmanda Da Costa, Prescribing Support Pharmacist
10:45 - 11:05 Enhancing support with The Relatives and Residents Association (R&RA) “Keys to care” - Judy Downey, Chair - R&RA
11:05 - 11:30 Coffee Break11:30 - 11:45 Photography opportunity11:45 - 12:15 Workshops12:15 - 12:45 Feedback12:45 - 13:15 Covert medication – Heather Eardley, Director of Development -Patients Association13:15 - 13:25 Ella Otomewo, Poet and Spoken Word Artist13:25 - 14:25 Lunch and networking14:25 - 14:45 What does great care look like? How to measure and improve – Anne Walker, Deputy Nurse Director of Quality and
Clinical Governance - WFCCG14:45 - 15:10 Training and education – Mick Cornett, Sector Delivery Manager - London Ambulance Service
15:10 - 15:40 Questions and answers from delegates15:40 - 16:00 Plenary
{ Dr Jackie Morris MB FRCP Vice President of the Patients Association
The case for care home medicine

{
Adelaide Tambo18 July 1929 – 31 January 2007
432,000 people live in care homes
Average number of diagnoses – 6.2 Median number of medications – 8 2/3 had some form of behavioural symptom 30% malnourished • 56% at risk of malnutrition 75%cognitive impairment 66% have behavioural problems Average life expectancy – 1 year for nursing
homes – 2 years for residential homes
Headline figures
Effective healthcare responses will have :... have expertise in management of: – Multiple diagnoses – Immobility Skin care Bowel and bladder care Frailty Swallowing/Mouth care Challenging behaviour ( Behavioural and Psychological
aspect of Dementia Polypharmacy Medication review Malnutrition / Dehydration End-of-life care Comprehensive geriatric assessment and review
Health status of UK care home residents Adam Gordon et 2013 & JEM
GP’s deliver care as part of GMS....although sometimes they don’t(!) GP:care home ratios
vary 1:1-1:50 Variation in number of GPs 1-35 visit
What happens now?
Reactive care models predominate Multidisciplinary team access is limited
Roles and responsibilities aren’t clearly specified
What happens now?
What should happen?
Resident focused- What matters to you?Life storiesStaff competencies?Staff supportedStaff empoweredTeam work/Care plans with resident/NOKProactive workIdentification of sick residents/ frailtyNo assumptions about Dementia and or old ageDignity and humanity ( Behind closed doors)Pain and distress identifiedEnd of life care/ Emergency care plans /CPR/DNARMatch care to needs(Slide 4)
Vanguard care improvement project Enhanced GP care ? Comprehensive geriatric assessment Community linked geriatrician Skilled care home staff Supported technology End of life care Care home pharmacist Crisis response service
Better care Hertfordshire

{
Adelaide Tambo18 July 1929 – 31 January 2007
Gordon AL, Franklin M, Bradshaw L et al. Health status of UK care home residents: a cohort study. Age Ageing 2014; 43: 97–103. http:// dx.doi.org/10.1093/ageing/aft077
AL Gordon What is the case for care home medicine? The geriatrician’s perspectiveJ R CollPhysicians Edinb 2015; 45: 148–53
References
Care Homes PilotAnnual Nursing Conference28th NovemberGail Foord – Associate Director Commissioning
Jenny Waller – Commissioning Support Manager
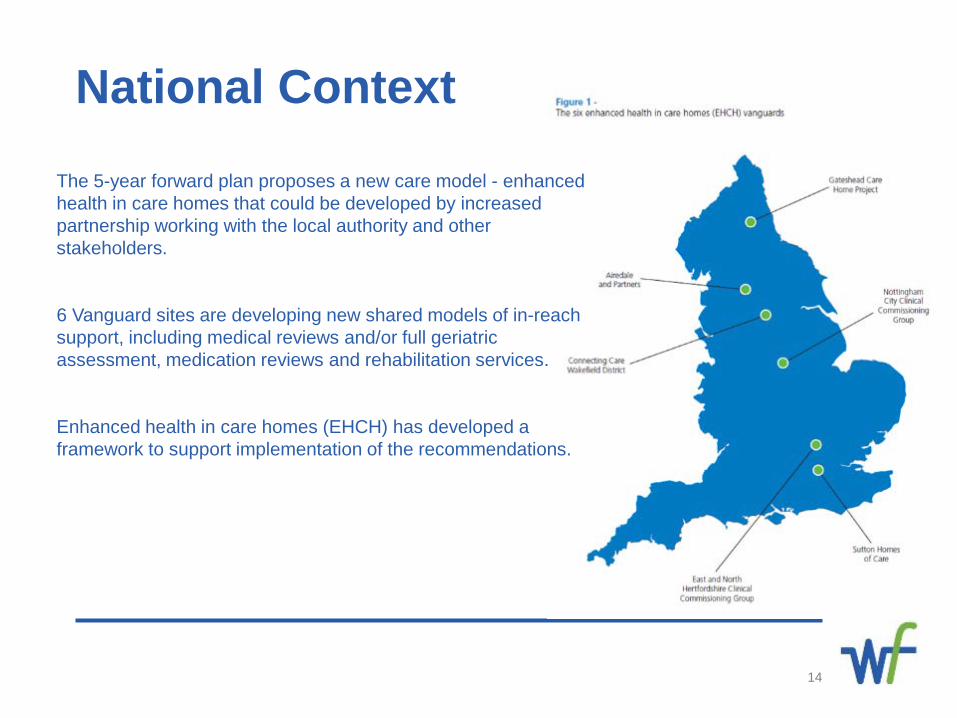
National ContextThe 5-year forward plan proposes a new care model - enhanced health in care homes that could be developed by increased partnership working with the local authority and other stakeholders.
6 Vanguard sites are developing new shared models of in-reach support, including medical reviews and/or full geriatric assessment, medication reviews and rehabilitation services.
Enhanced health in care homes (EHCH) has developed a framework to support implementation of the recommendations.
14
15
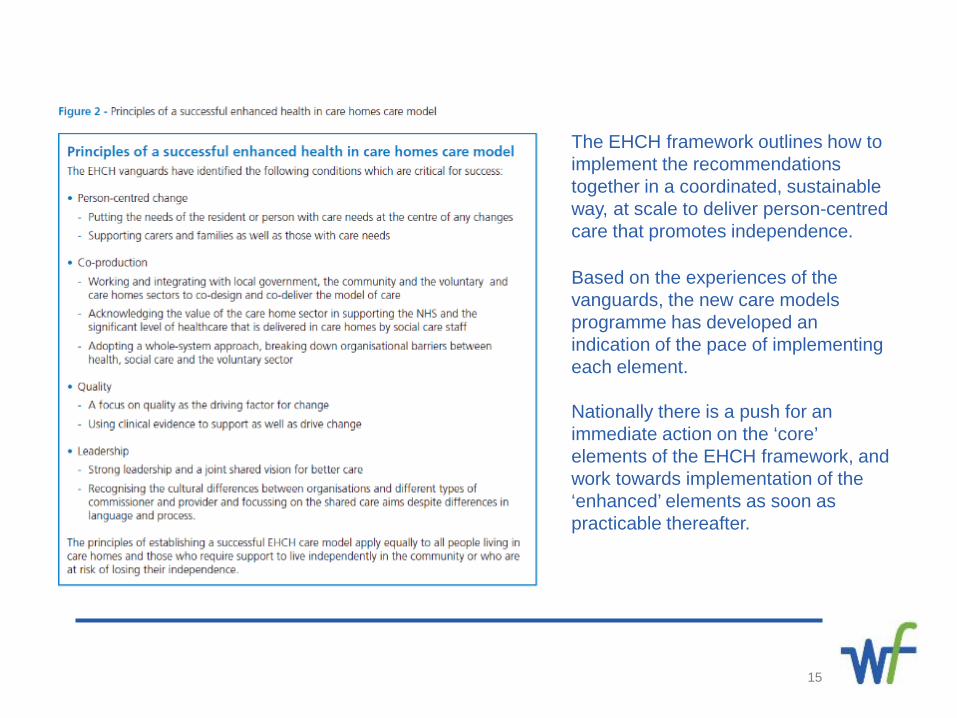
The EHCH framework outlines how to implement the recommendations together in a coordinated, sustainable way, at scale to deliver person-centred care that promotes independence.
Based on the experiences of the vanguards, the new care models programme has developed an indication of the pace of implementing each element.
Nationally there is a push for an immediate action on the ‘core’ elements of the EHCH framework, and work towards implementation of the ‘enhanced’ elements as soon as practicable thereafter.
Local ProvisionThe current care homes market in Waltham Forest is a composite of local authority, private sector and not for profit organisations with 64 care homes in the borough providing nursing and personal care accommodation for people who may not be able to live independently. 218 beds in Nursing Homes, with a total capacity of 1064 beds across the borough.
The CCG set out a proposal to develop an enhanced service model to support care homes in the borough in conjunction with the development of a sustainable training programme for care home staff, the focus was on improving the quality of life and safety for residents living within the ‘care home’ setting.
The pilot took learning from the 6 vanguard’s to develop the model.
Rapid ResponseThe Rapid Response services (NELFT) provides open referral for triage advice or visit prior to escalating concerns to primary or secondary care to a limited number of care homes. This includes first response and care of minor injuries, assessment diagnostics and support for palliative care.
16
The Pilot
17
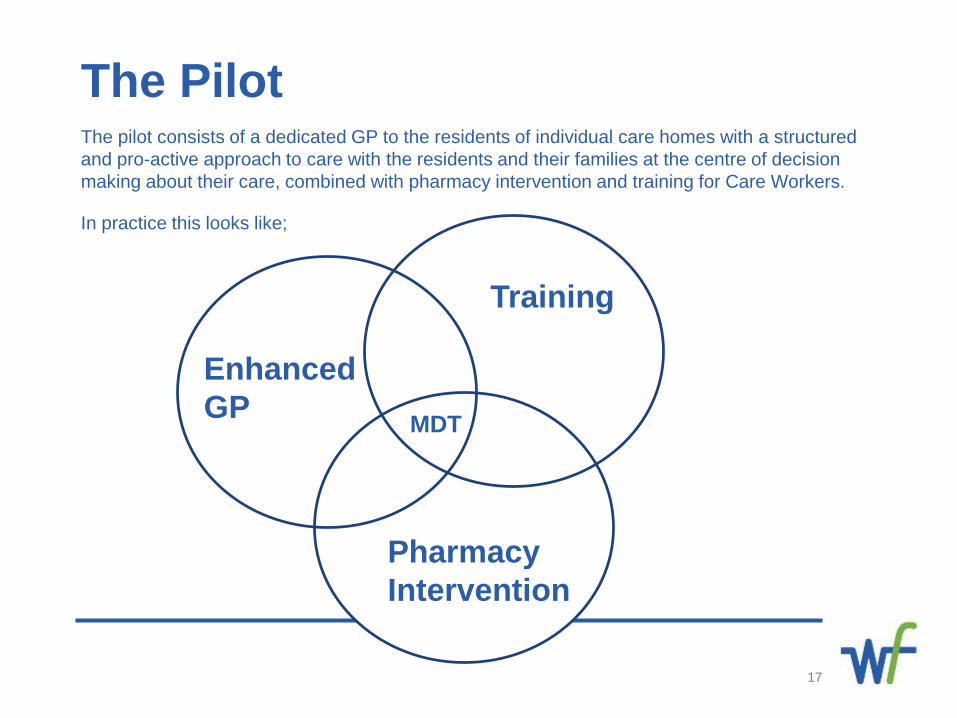
The pilot consists of a dedicated GP to the residents of individual care homes with a structured and pro-active approach to care with the residents and their families at the centre of decision making about their care, combined with pharmacy intervention and training for Care Workers.
In practice this looks like;
Enhanced GP
Pharmacy Intervention
Training
MDT
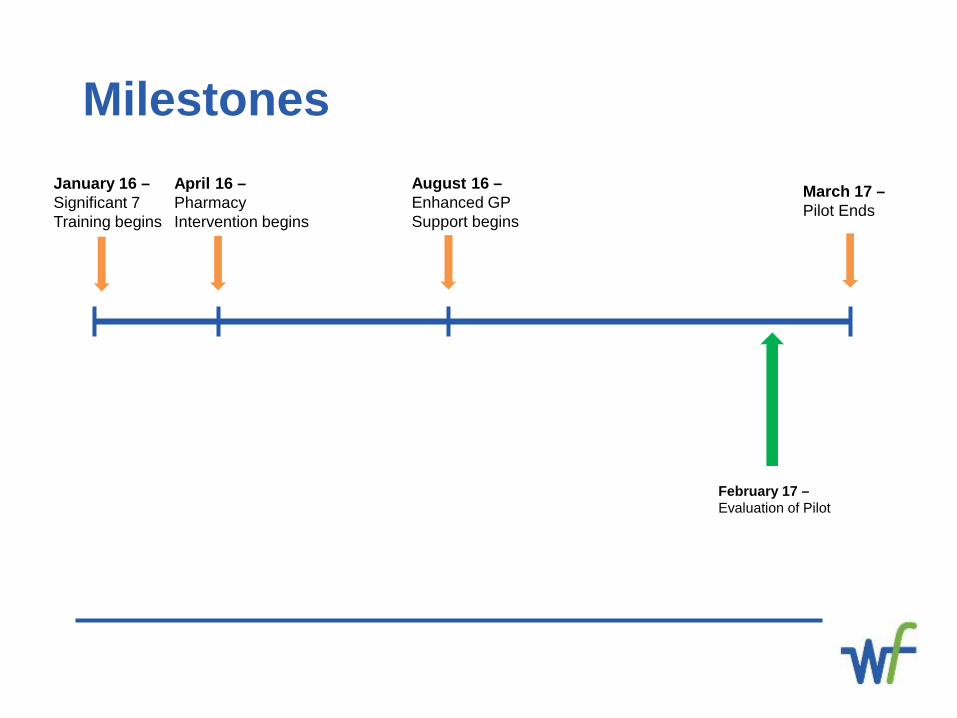
January 16 –Significant 7 Training begins
April 16 –Pharmacy Intervention begins
August 16 –Enhanced GP Support begins
March 17 –Pilot Ends
February 17 –Evaluation of Pilot
Milestones
19
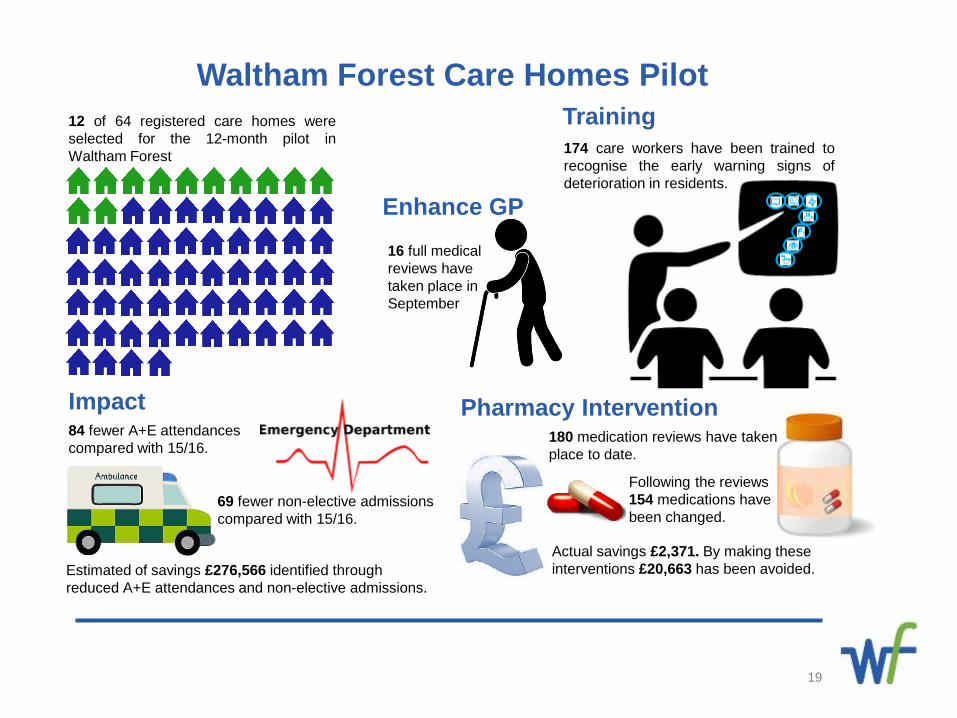
12 of 64 registered care homes wereselected for the 12-month pilot inWaltham Forest
Waltham Forest Care Homes Pilot
16 full medical reviews have taken place in September
Enhance GP
174 care workers have been trained torecognise the early warning signs ofdeterioration in residents.
Training
180 medication reviews have taken place to date.
Following the reviews 154 medications have been changed.
Actual savings £2,371. By making these interventions £20,663 has been avoided.
Pharmacy Intervention84 fewer A+E attendances compared with 15/16.
69 fewer non-elective admissions compared with 15/16.
Impact
Estimated of savings £276,566 identified through reduced A+E attendances and non-elective admissions.
Significant 7 Training
20
Significant 7 programme developed by BHR & NELFT for level 1 care workers and helps staff to recognise, manage and reduce avoidable deterioration and improves communications with the care home.
The training nurse was funded to begin delivering the Significant 7 training from January. Early indications were that the training was having a positive impact on care home staff skill level empowering them to keep residents in the home and in turn reduce non-elective admissions. The training was well received by all participants.
Prior to Sig 7 training, one home had very high incidence of pressure ulcers. I invited Tissue Viability Nurse to come and teach on pressure ulcer prevention and advise. This has led to a significant reduction in pressure ulcer related incidence. Anita Tagoe, Significant 7 Training Nurse, NELFT
Pharmacy Intervention
21
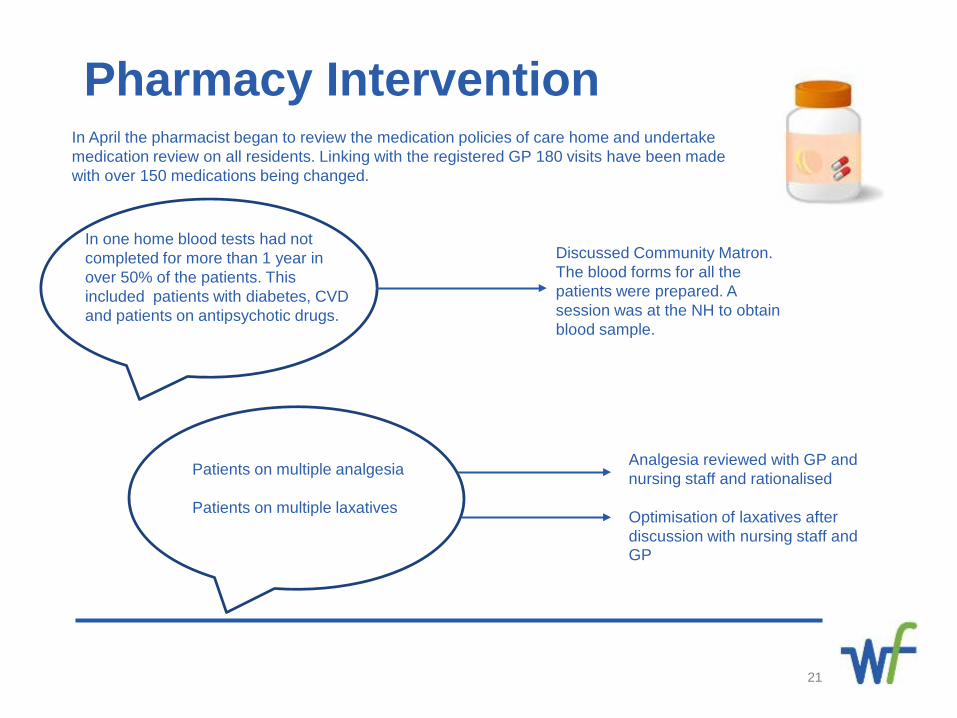
In April the pharmacist began to review the medication policies of care home and undertake medication review on all residents. Linking with the registered GP 180 visits have been made with over 150 medications being changed.
In one home blood tests had not completed for more than 1 year in over 50% of the patients. This included patients with diabetes, CVD and patients on antipsychotic drugs.
Discussed Community Matron. The blood forms for all the patients were prepared. A session was at the NH to obtain blood sample.
Patients on multiple analgesia
Patients on multiple laxatives
Analgesia reviewed with GP and nursing staff and rationalised
Optimisation of laxatives after discussion with nursing staff and GP
Enhanced GP Support
22
Enhanced GPs began visiting the care homes to complete medical reviews on the residents, some GPs were including family members in the medical reviews from the outset.
The Care Home Pilot Scheme has proven to be a great success at Aspray House. We are now in receipt of regular visits and support, from our GP practice, pharmacist and community matrons, which has resulted in our Service Users receiving medical assistance and support, in a timely manner. We have received positive feedback from some of our family members, as their relatives have not had to wait too long for a visit, and the GP has took time to discuss any concerns they may have into their relatives medical diagnosis.- Sharon Osbourne, Aspray House Manager
The home have been inviting the family to our planned meetings, this has really helped in completing DNAR form. - Pilot GP, Waltham Forest
The pilot has allowed me protected time to completed ‘ward rounds’ in the care home rather than using time over lunch.- Pilot GP, Waltham Forest
What is the data telling us?
23
Early results look promising however it is acknowledged that there are quality issues with the source of admission and destination codes which makes analysis difficult. The data is generated using care home post codes to identify non-elective admissions and A&E attendance.
Note: A small number of nursing and residential homes have the same post code e.g. Ross Wyld NH and Aston Grange RH and there is the potential to identify non care home related activity – a full audit trail has been maintained.
24
20
25
30
35
40
45
50
Apr May Jun Jul Aug Sep
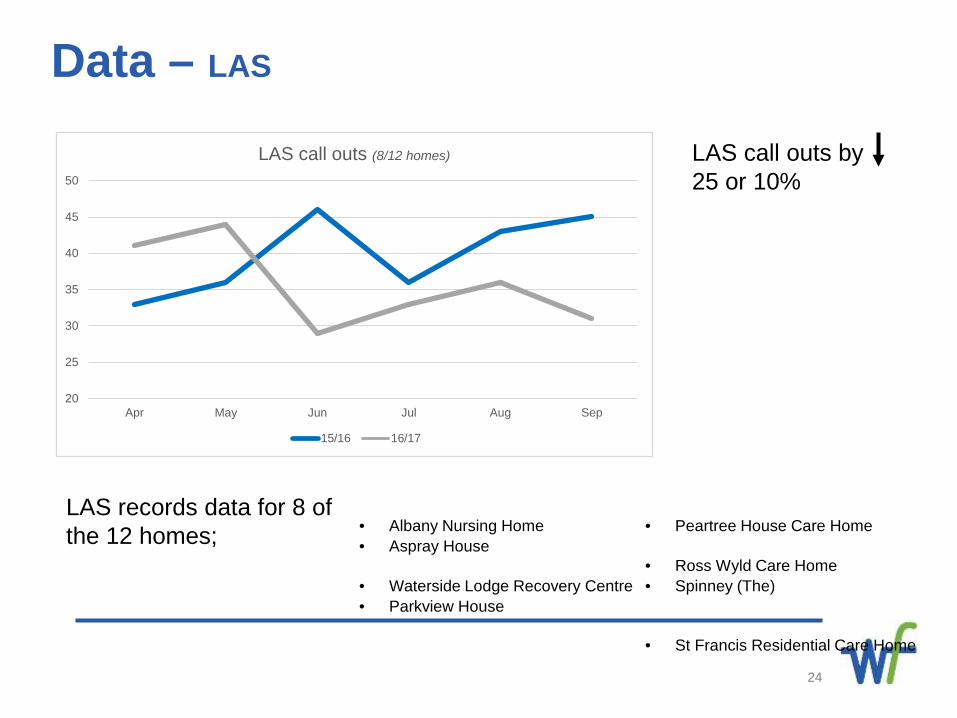
LAS call outs (8/12 homes)
15/16 16/17
Data – LAS
• Albany Nursing Home• Aspray House
• Waterside Lodge Recovery Centre• Parkview House
LAS records data for 8 of the 12 homes; • Peartree House Care Home
• Ross Wyld Care Home• Spinney (The)
• St Francis Residential Care Home
LAS call outs by 25 or 10%
25
Data – LAS
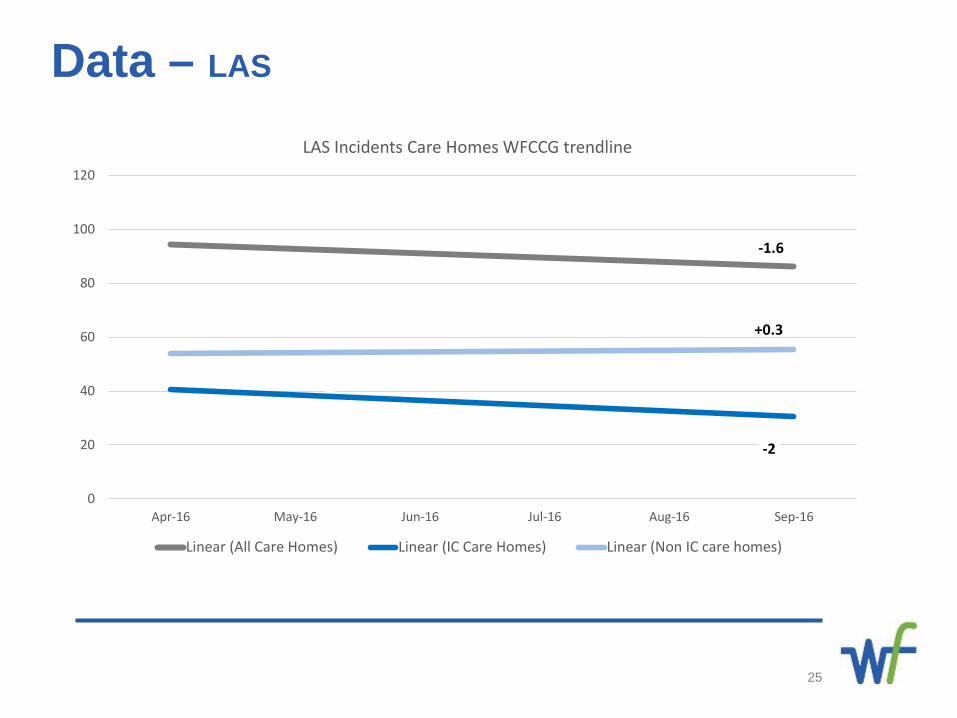
-1.6
-2
+0.3
0
20
40
60
80
100
120
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16
LAS Incidents Care Homes WFCCG trendline
Linear (All Care Homes) Linear (IC Care Homes) Linear (Non IC care homes)
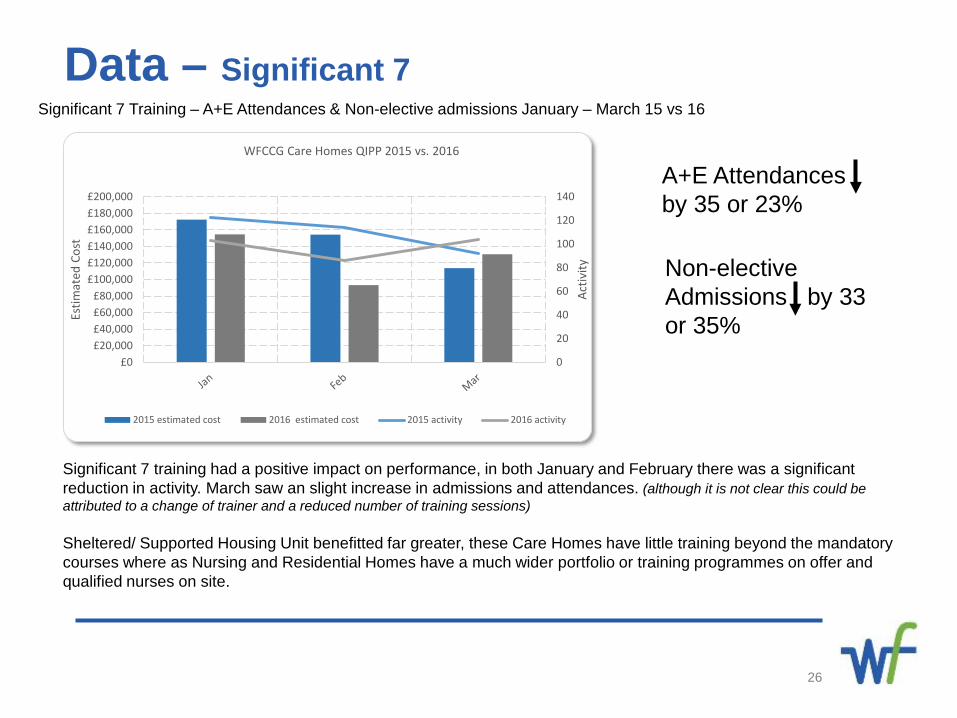
Data – Significant 7Significant 7 Training – A+E Attendances & Non-elective admissions January – March 15 vs 16
26
0
20
40
60
80
100
120
140
£0£20,000£40,000£60,000£80,000
£100,000£120,000£140,000£160,000£180,000£200,000
Activ
ity
Estim
ated
Cos
t
WFCCG Care Homes QIPP 2015 vs. 2016
2015 estimated cost 2016 estimated cost 2015 activity 2016 activity
Significant 7 training had a positive impact on performance, in both January and February there was a significant reduction in activity. March saw an slight increase in admissions and attendances. (although it is not clear this could be attributed to a change of trainer and a reduced number of training sessions)
Sheltered/ Supported Housing Unit benefitted far greater, these Care Homes have little training beyond the mandatory courses where as Nursing and Residential Homes have a much wider portfolio or training programmes on offer and qualified nurses on site.
A+E Attendances by 35 or 23%
Non-elective Admissions by 33 or 35%
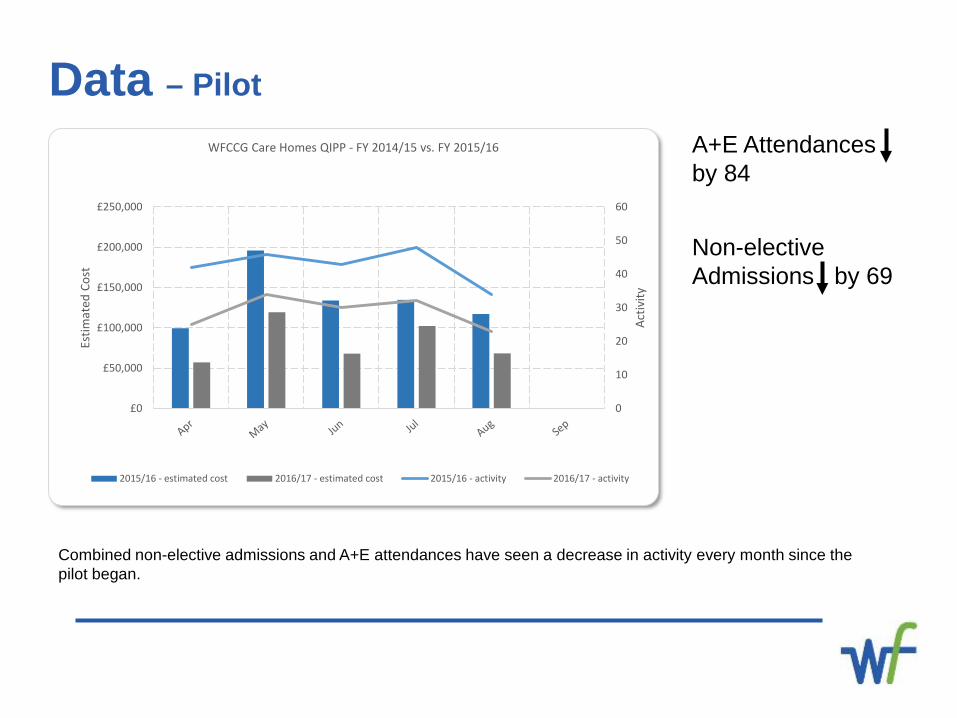
Data – Pilot
Combined non-elective admissions and A+E attendances have seen a decrease in activity every month since the pilot began.
0
10
20
30
40
50
60
£0
£50,000
£100,000
£150,000
£200,000
£250,000
Activ
ity
Estim
ated
Cos
t
WFCCG Care Homes QIPP - FY 2014/15 vs. FY 2015/16
2015/16 - estimated cost 2016/17 - estimated cost 2015/16 - activity 2016/17 - activity
A+E Attendances by 84
Non-elective Admissions by 69
What’s going wellReduction in A&E attendance and unplanned admission
WF Care Home Market Position – greater understanding of the range of care homes, bed numbers and performance of care homes in the borough
Engagement – there has been a significant development in the relationships between the CCG and Care Homes.
Newsletter – there will be a monthly newsletter shared between GP for best practice
Sharing – Care Homes Managers and GPs have been willing to share ideas and templates already developed
Quality Improvement – it has been reported how happy the residents family are with improve service
Interoperability – with GPs covering care homes where the residents are not registered with the same GP there have been IT difficulties
Low data number – low numbers has meant that data cannot be reported from the outset
LAS – lack of communication, neighbouring CCG’s integrate LAS into their joint care homes meetings, WF to adopt this approach.
Phlebotomy – 4 month wait for community phlebotomy service. GPs lack skills in taking bloods, nursing staff not signed off on competencies, not within rapid response remit.
Paperless – Care home use faxing to share information with General Practice, explore use of NHS mail.
28
Lessons Learnt
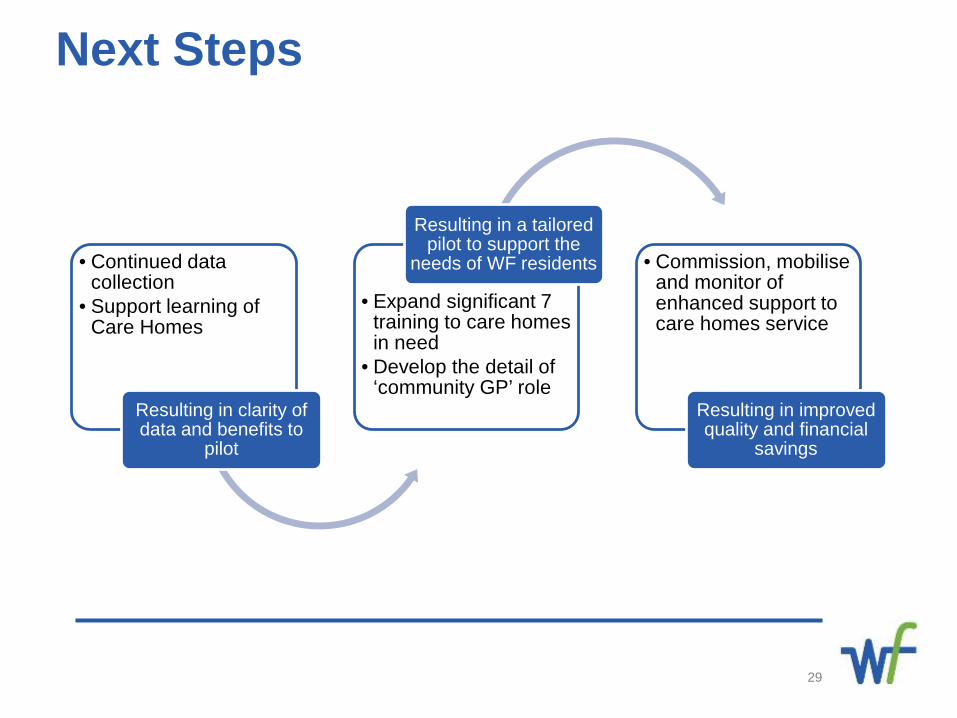
Next Steps
29
• Continued data collection
• Support learning of Care Homes
Resulting in clarity of data and benefits to
pilot
• Expand significant 7 training to care homes in need
• Develop the detail of ‘community GP’ role
Resulting in a tailored pilot to support the
needs of WF residents • Commission, mobilise and monitor of enhanced support to care homes service
Resulting in improved quality and financial
savings
30
A Journey to no delays in Hospital Discharge
Moving from Discharge to Care Transition
Paul Larrisey
What is a Delayed Transfer ofCare (DToC)A delayed transfer of care is defined as a person who is occupying an
acute hospital bed that is “medically optimised” i.e. no longer requires
the care of an acute hospital care
32
What is the impact?
It is more likely that DToC Patients are Older
People. We know that Older People decondition
by being in hospital both physically & cognitively they longer they stay.
33
By not ensuring that people are discharged when ready,
hospital beds are blocked for more acutely unwell
patients, which has a knock-on impact across services
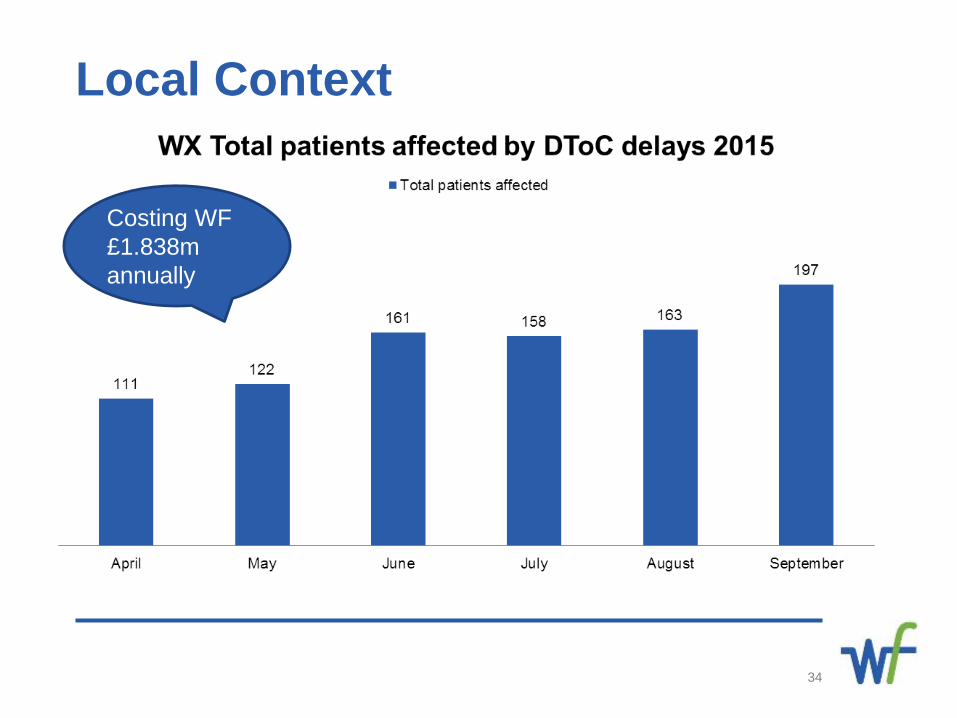
34
Local Context
Costing WF £1.838m annually
Local Context • Helping people to transfer smoothly and appropriately through
the health and care system is one of the most complex tasks
that the system faces.
• Frontline care and health staff have been dealing with this challenge for many
years, but the pressure is increasing as our population ages and resources are
stretched. And of course many of us have personal experience of the stress that
avoidable hospital admissions and delays in transferring to the next level of care can
cause.
• Last Year in Whipps Cross Hospital Waltham Forest residents used almost 15,000
bed days waiting to be discharged to another setting.
This means 41 acute hospital beds are in constant use for people who don’t need to
be in hospital.
35
STOP!
We Need to Change Our thinking and
Approach
Discharge to Assess
• NHSE have identified Discharge to Assess Pathways as part of Eight High
Impact Changes that supports patient flow across services;
• In essence discharge to assess in Waltham Forest incorporates the ethos
that reablement and rehabilitation should not be delivered from a hospital
bed, and decisions about long term care needs are not made whilst an
individual is in an acute hospital setting.
The aims of discharge to assess are to:
• Minimise hospital stay;
• maximise independence and wherever possible support a return to home
for individuals.
37
Right patient, right place, right time! Discharge to Assess
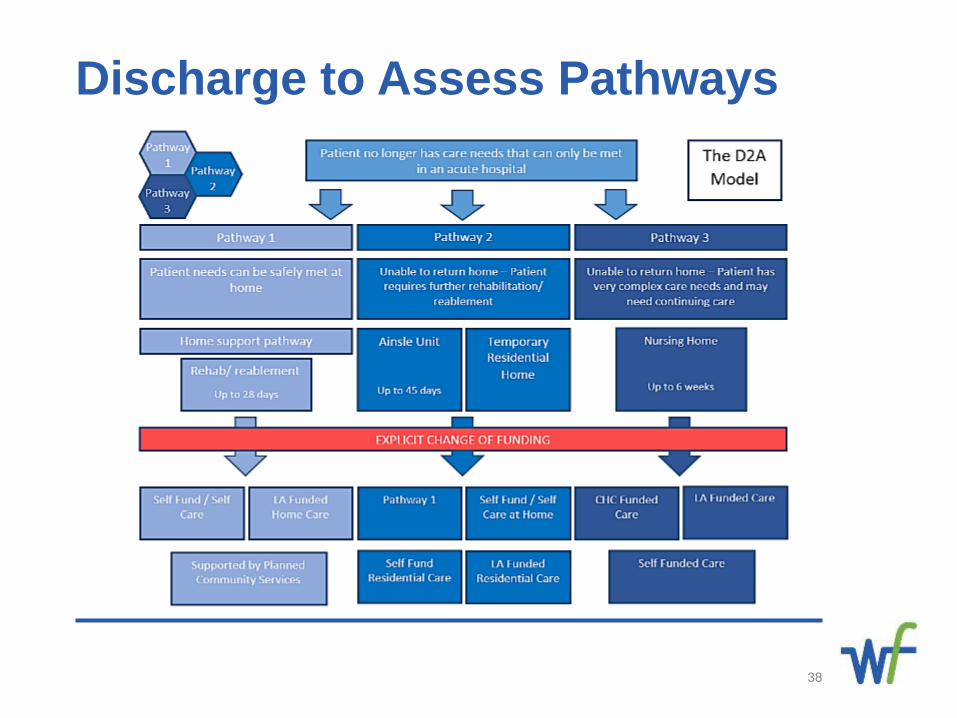
Discharge to Assess Pathways
38
Patient & System Benefits Anticipated Benefits;
• Increasingly joined up care/more seamless for patients/patients in the right
place right time;
• Reduction in dependency on one part of the system;
• Integrated roles and workforce working across the unified system not in
organisational silos i.e. have therapists following patients across the system
and where most needed;
• Aim to improve effective use of pooled resources;
39
Next steps• Evaluate
• Identify system changes required
• Commission
• Monitor
• Improve
40

Optimising medicines for people residing in care homes Ada Onyeagwara- Assistant Director, Medicines Optimisation
Dr Sabeena Pheerunggee- Named GP for safeguarding
Amanda Da Costa- Prescribing Support Pharmacist
National Guidance • NICE Managing medicines in care homes, Social care guideline [SC1]
Published date: March 2014
Recommendations for good practices for systems and process for
managing medicines in care home
• The Royal Pharmaceutical Society
“better utilisation of pharmacists’ skills in care homes will bring
significant benefits to care home residents, care homes providers
and the NHS.”
42
Residents in care homes:
• Have the same rights and responsibilities in relation to NHS care as those who do not live in care homes;
• More likely to be older and frail
• Have multiple health problems
• Prescribed many medicines
• Increased risk from errors with medicines
43
Patient centred careHelping residents to look after and take their own medicines is important in enabling residents to retain their independence. • When a person moves into a care home, staff
should assume that the person can look after and manage their own medicines, unless indicated otherwise.
• Each resident should have an individual risk assessment to determine the level of support they need to manage their own medicines.
44
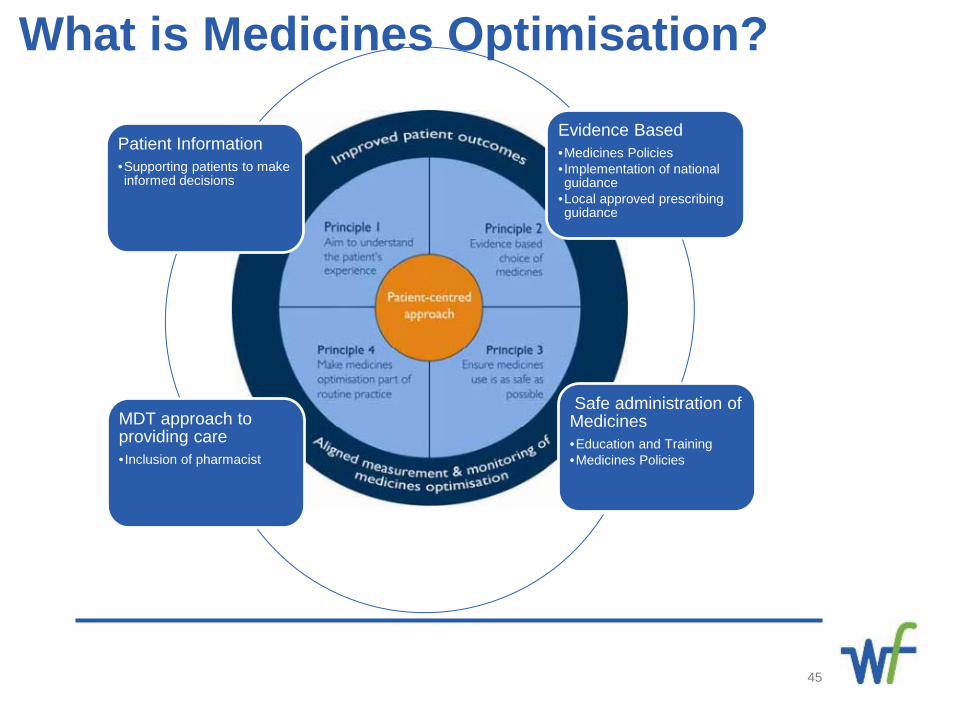
What is Medicines Optimisation?
45
Evidence Based•Medicines Policies• Implementation of national guidance
•Local approved prescribing guidance
Safe administration of Medicines•Education and Training•Medicines Policies
MDT approach to providing care•Inclusion of pharmacist
Patient Information•Supporting patients to make informed decisions
Principles of safe and appropriatehandling of medicines (1)
• People who use social care services have freedom of choice in
relation to their provider of pharmaceutical care and services
including dispensed medicines.
• Care staff know which medicines each person has and the social
care service keeps a complete account of medicines.
• Care staff who help people with their medicines are competent.
• Medicines are given safely and correctly, and care staff preserve
the dignity and privacy of the individual when they give medicines
to them.
46
Principles of safe and appropriatehandling of medicines (2)• Medicines are available when the individual needs them and
the care provider makes sure that unwanted medicines are
disposed of safely.
• Medicines are stored safely.
• The social care service has access to advice from a
pharmacist.
• Medicines are used to cure or prevent disease, or to relieve
symptoms, and not to punish or control behaviour.
47
Role of the pharmacistSupport Medicines Optimisation by:
• Medication reviews
• Education and Training
• Quality assurance visits
• Reviewing medication errors
• MDT membership
• Clinical Advice
• Signposting to other services
48
Care Home work in Waltham ForestThe Medicines Optimisation team have supported • A local Nursing Home • The CCG commissioned care home service
49
Care Home work in Waltham Forest-The Team
50
Dr Sabeena Pheerunggee Amanda Da Costa
Care Home work in Waltham Forest-Case Study
The work includes:• Working as a part of the MDT• Review of all medicines related policies• Clinical and safety audits• Joint wards rounds with GPs and other healthcare
professionals• Covert administration reviews
51
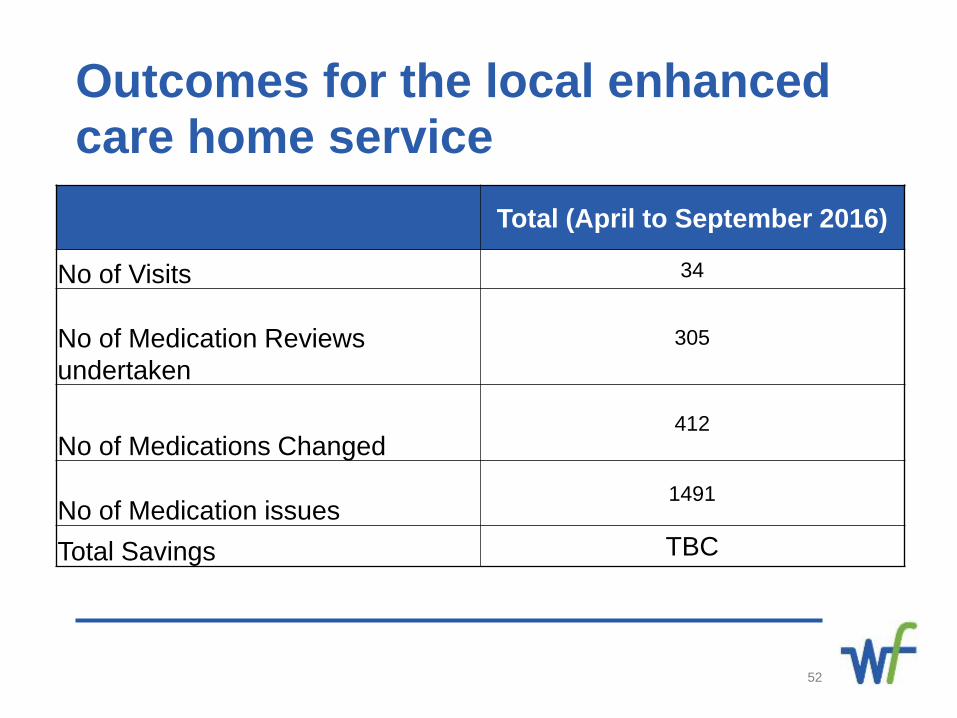
Outcomes for the local enhanced care home service
52
Total (April to September 2016)
No of Visits 34
No of Medication Reviews undertaken
305
No of Medications Changed412
No of Medication issues1491
Total Savings TBC
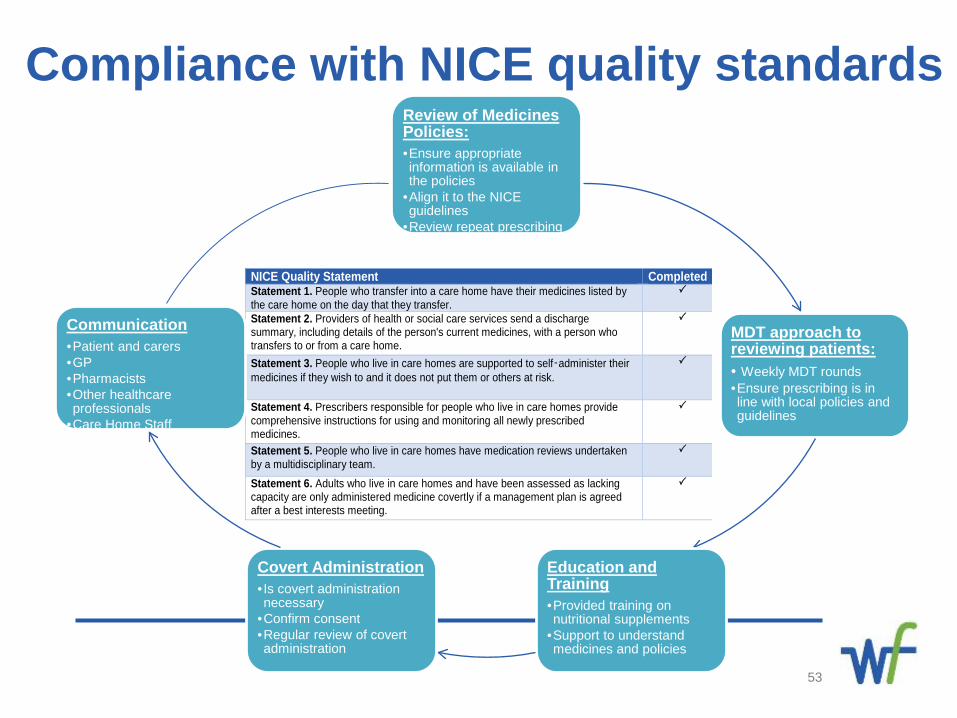
NICE Quality Statement Completed Statement 1. People who transfer into a care home have their medicines listed by the care home on the day that they transfer.
Statement 2. Providers of health or social care services send a discharge summary, including details of the person's current medicines, with a person who transfers to or from a care home.
Statement 3. People who live in care homes are supported to self‑administer their medicines if they wish to and it does not put them or others at risk.
Statement 4. Prescribers responsible for people who live in care homes provide comprehensive instructions for using and monitoring all newly prescribed medicines.
Statement 5. People who live in care homes have medication reviews undertaken by a multidisciplinary team.
Statement 6. Adults who live in care homes and have been assessed as lacking capacity are only administered medicine covertly if a management plan is agreed after a best interests meeting.
Compliance with NICE quality standards
53
Review of Medicines Policies:•Ensure appropriate information is available in the policies
•Align it to the NICE guidelines
•Review repeat prescribing process
MDT approach to reviewing patients:• Weekly MDT rounds•Ensure prescribing is in line with local policies and guidelines
Education and Training •Provided training on nutritional supplements
•Support to understand medicines and policies
Covert Administration• Is covert administration necessary
•Confirm consent•Regular review of covert administration
Communication•Patient and carers•GP•Pharmacists•Other healthcare professionals
•Care Home Staff
Best practice for Medicines Optimisationfor Care Homes
• Collaborative working between all healthcare professionals
• Joint ward rounds• Robust medicines policies• MDT approach to delivering care
Difficult Conversations and identifying patients for End of Life Care54
Useful links• NICE guidance: The NICE Guidance; Management of medicines in care homes (March 2014) clearly states how
commissioners, managers of care homes and other healthcare professionals involved in care homes should work in a
standardised format with clear consideration for process and safety : https://www.nice.org.uk/guidance/sc1
• Royal Pharmaceutical Society The Handling of Medicines in Social Care sets out principles of good practice and legislation
governing the handling of medicines applicable to providers of care services, managers and care workers in many social
care settings : https://www.rpharms.com/social-care-settings-pdfs/the-handling-of-medicines-in-social-care.pdf
• Care Quality Commission The Care Quality Commission (CQC) regulates the management of medicines in care homes.
The Essential Standards guide is designed to help providers of health and adult social care comply with the Health and
Social Care Act 2008 (Regulated Activities) Regulations 2010 and the Care Quality Commission (Registration) Regulations
2009 CQC Essential standards of quality and safety
55
Further queriesMedicines Optimisation TeamNHS Waltham Forest Clinical Commissioning GroupTelephone: 020 3688 2654E-mail: [email protected]
Difficult Conversations and identifying patients for End of Life Care56
The Relatives & Residents Association
Judy DowneyChair
With thanks to Comic Relief who financed “Keys to Care”
Enhancing support withR&RA’s ‘Keys to Care’
57
National charity founded in 1993
We support, inform and campaign on behalf of older people in care
We employ the unique perspective of residents and their relatives to help improve services for all those thinking about or living in care homes
R&RAWho we are
58
What we do
HelplineCampaigningResourcesPublications & Projects
59
R&RA’s HelplineOffers accurate, up-to-date informationabout the transition to residential care.
For example about
Who pays? What to pay? Whether to pay? Advocacy and support Concerns about care
As well as a sympathetic andcompassionate response
Our Helpline empowers callers with the information they need
0207 359 8136 open from Monday to Friday 9.30am – 4.30pm
60
R&RA Campaigns
To improve the quality of life for older people needing care.
We argue for:
Higher status for care workers
Mandatory training for all care staff
Minimum staff ratios
Better regulation
61
WHY WE NEED HIGHER STATUS FOR HEALTH AND CARE WORKERS?
Because of the increasing needs of those needing care
Because people at the end of life deserve the best care
Because the workforce deserves better pay and conditions
Because this won’t happen without a better career structure
All these depend on having a national mandatory, recognised and transferable qualification, which will increase pay and job satisfaction, reduce turnover and promote the status care needs and deserves
62
TRAINING IN THE SECTOR IS SIMPLY INADEQUATE
Almost 50% of the adult social care workforce have “no relevant social care qualifications”*
Over 90% of care home workers are not working towards any qualification**
Fewer than half have any training in medication handling and awareness, mental capacity and deprivation of liberty or dementia care*
Only 10% have received training in malnutrition care and assistance with eating**
*Skills for Care – State of the Adult Social Care Sector and Workforce in England, 2016**Skills for Care - National Minimum Data Set for Social Care, November 2016
63
WHY THE CURRENT SITUATION IS JUST NOT GOOD ENOUGH
The latest “Safeguarding Adults” Annual Report* showed that people in care homes are more vulnerable than any other group in the adult population.
The total number of adults at risk for whom safeguarding concerns were investigated and concluded came to 124,940.
This number does not include separate referrals to other agencies.
* Safeguarding Adults Annual Report, England 2015-1664
WHY THE CURRENT SITUATION IS JUST NOT GOOD ENOUGH
The vast majority of referrals about a risk of abuse concerned people over 65 i.e. 63% - 6 out of every 10 referrals.
The largest group within this were over 85 i.e. 29,760
Adults aged 75-84 were three times more likely, and
Those aged 85 and over were more than 10 times more likely to have a Section 42 Enquiry than the England average.
65
WHY THE CURRENT SITUATION IS JUST NOT GOOD ENOUGH
The place of risk was most frequently the home of the adult at risk (43%) or the care home (36%).
Over 9 million people over 65 live in their own homes.
45,897 were concluded referrals affecting individuals in care homes.
Fewer than 400,000 older people live in care homes.
66
R&RA CampaignsWe need CQC to be:
More efficient and effective
More focused on improvement
More vigilant with more frequent inspections using trained and experienced inspectors
More accessible with signed and readable reports which avoid jargon
AND a return to investigating complaints
67
WHY DID WE PRODUCEKEYS TO CARE?
Their development was prompted by the worries and distress of residents, relatives and others to our Helpline about poor or rushed care.
And the obvious need for more support for staff and those in the front line of caring for frail, elderly people.
Our team has produced this practical training resource with the benefit of specialist advice and the help of people who live and work in a range of care settings, with charitable funding and the endorsement of Skills for Care and theDepartment of Health
68
Keys to Care The Keys to Care - 12 little cards on a keyring covering topics, ranging from the practicalities of the Care Plan, Continence Care and Mouth & Teeth Care to the deeply sensitive issues of Dementia and End of Life Care.
The key things toThink about Ask Do
It is more an aide-memoire, a checklist, a reminder of what matters and yes, a reassurance that you’re doing the right thing.
69
Keys to Care
The Keys to Care resource was designed primarily for care workers and healthcare assistants and also found useful for relatives and others.
Jargon free, practical, easy to read and use.
“A brilliant idea and so well executed.” Sharon Allen, CEO of Skills for Care
70
The Keys to Care resource is unique because it is:
Designed for the busy health and care worker
Easy to read and use
Attractive and durable
Flexible in use
Keys to Care
71
Keys to Care Evaluation* –Impact on QualityHow has Keys to Care resource impacted the quality of care you provide? More than 50% of care workers agreed or strongly agreed with these statements:
I seek more advice and guidance
about doing my job
I look for ways to improve what I do
I am more involved in deciding how to
care for people
I know better what I and others should
be doing
I care more about the person and/or
my job
I am better at my job
72
*University of Worcester, Association for Dementia Studies, Evaluation of the Keys to Care Resource, February 2016
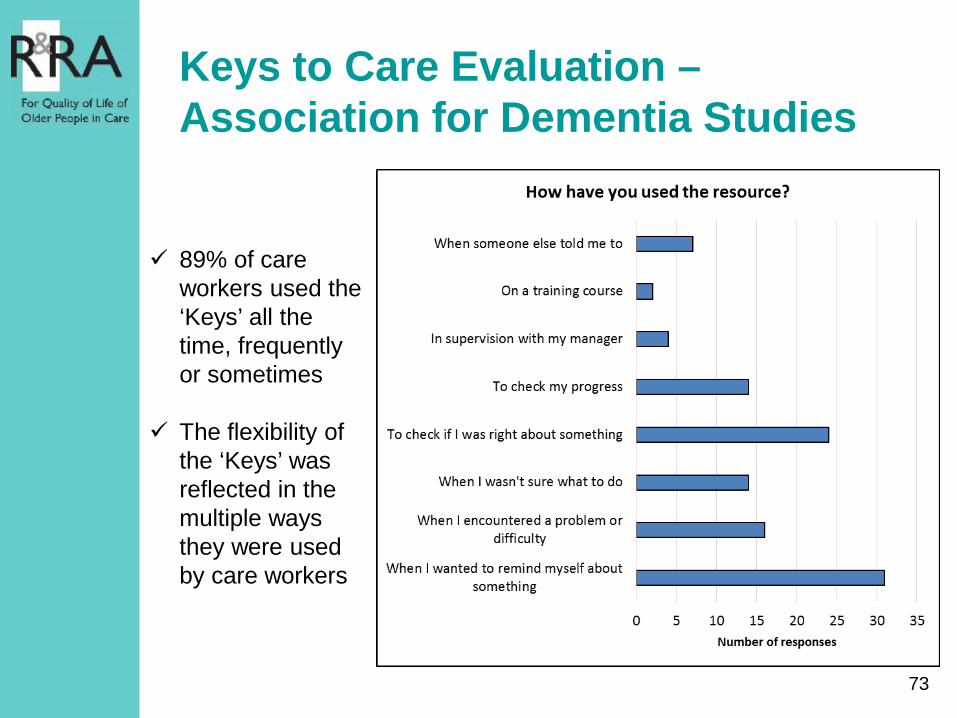
Keys to Care Evaluation –Association for Dementia Studies
89% of care workers used the ‘Keys’ all the time, frequently or sometimes
The flexibility of the ‘Keys’ was reflected in the multiple ways they were used by care workers
73
Feedback from Care Workers
“I like the fact you can look up more information. I feel that the more information you can get, the better.”*
“These should be given to everyone who is going to work to support people. You can tell they are written by people who are receiving or giving care.”*
“It’s all a really good guide for care planning.”*
“They are good for reminding people what they should be doing, particularly for new and agency staff.”*
“Reminds me that it is so important to do my job well.”*
“Great prompts and reminders.Nice to have the information at hand -saves time.”*
74
* Quotes from the Royal Hospital Chelsea, The Orders of St John Care Trust and The Extra Mile Care Company

Designed for Care Workers
‘It is so easy to slip in to a routine, and they (the Keys to Care) remind you to think about the person and look after people as individuals’
‘They help us focus and remember what is important to caring, as people can become complacent and forget’
by the care sector
75
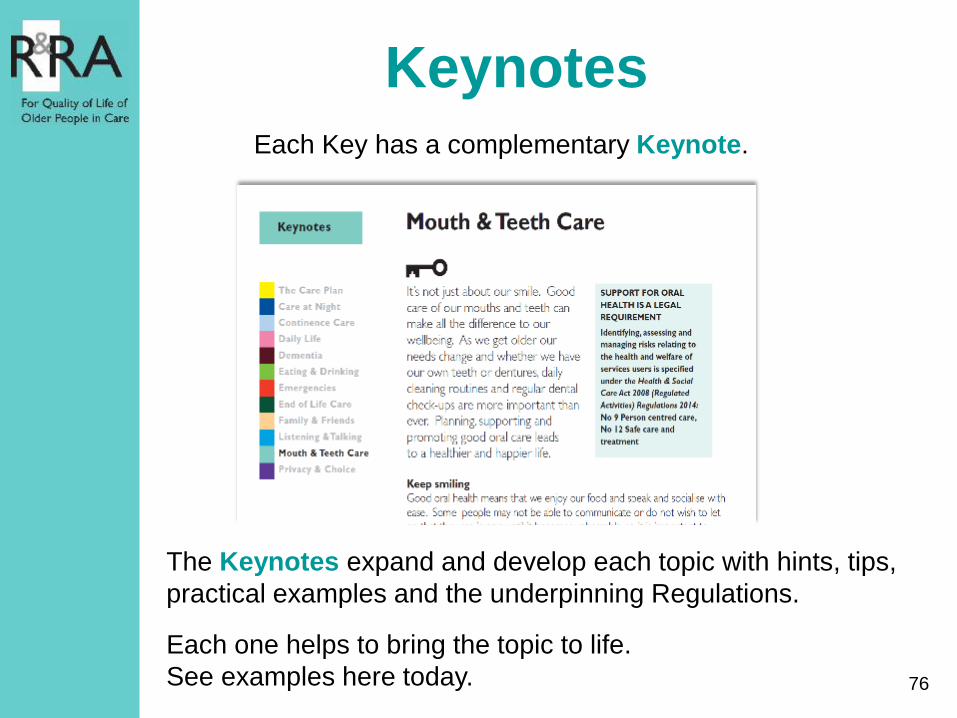
KeynotesEach Key has a complementary Keynote.
The Keynotes expand and develop each topic with hints, tips, practical examples and the underpinning Regulations.
Each one helps to bring the topic to life.See examples here today. 76
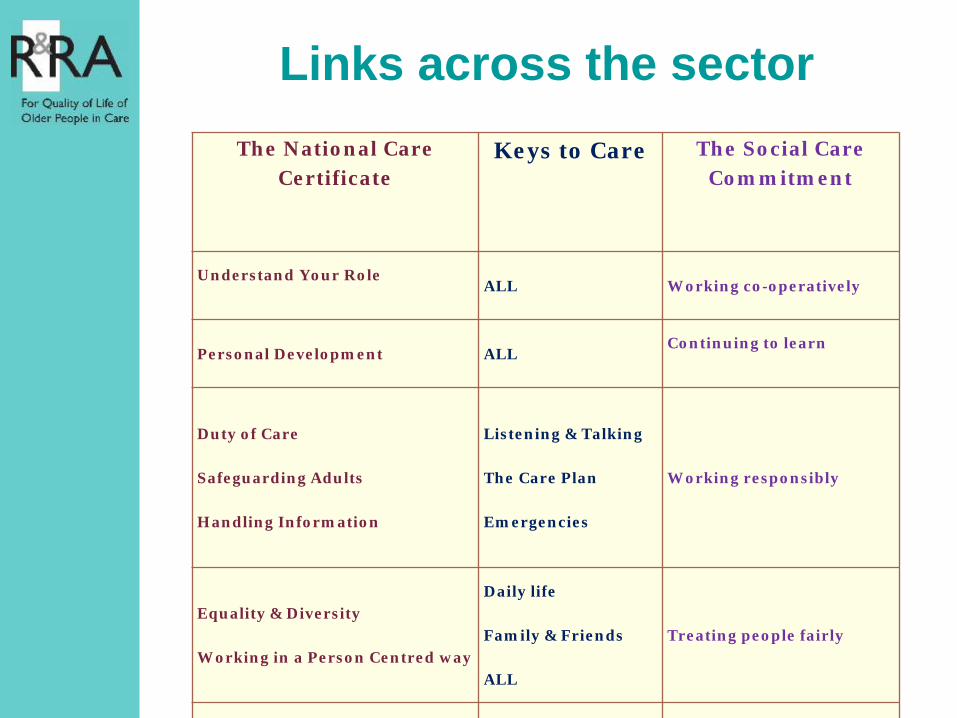
The National Care Certificate
Keys to Care The Social Care Commitment
Understand Your RoleALL Working co-operatively
Personal Development ALLContinuing to learn
Duty of Care
Safeguarding Adults
Handling Information
Listening & Talking
The Care Plan
Emergencies
Working responsibly
Equality & Diversity
Working in a Person Centred way
Daily life
Family & Friends
ALL
Treating people fairly
Links across the sector

R&RA Membership
YOU care about residents’ quality of life
YOU are committed to improving standards
YOU care about your workforce
Joining The Relatives & Residents Association shows that:
78www.relres.org [email protected] 020 7359 8148
Workshop 2 – Key issues1. Personal reflections on key issues (yellow post it
notes)2. Table discussion on Key issues (themes)
• Patients• Relatives• Care homes staff• Others
3. What needs to be in place for good quality care?
79
Medicines related care of residents with dysphagia in care homes
Heather Eardley, Development Director
The Patients Association
• Long established national independent charity • Non-disease specific• Campaigning on patients’ and carers’ issues• National Helpline• Working with NHS trusts, providers and
regulators on patient improvement project
Basis for report
• Reports to our helpline of swallowing difficulties being a challenge
• Telephone survey of 30 care homes based on structured questionnaire
• Care homes had between 20 and 90 residents
Major findings
• Incidence of swallowing difficulties varied - 1 manager reported that 50% of her residents had some form of difficulty in swallowing.
• Over 100 people had profound swallowing difficulties
• In over two thirds of homes crushing, melting, dispersing or splitting medication happening daily
• In over two thirds of homes mixing medication with food happening daily
Major findings 2
• Many managers referred to advantages of liquid forms of medication but
• Over two thirds of homes reported GP concerns about the cost of liquid medication and this was a factor in prescribing practice
• Holding off doses due to difficulty in administering medication was an increasing issue
Issues presented
• Swallowing problems can lead to residents choking or having coughing fits
• Changing structure of medication alters normal arrangement for absorption
• Common cause of administration error• Crushing = greater liability to prescriber,
dispenser and administer of medication• Risk of residents being covertly treated with
medication disguised in food
Training
• Most managers had limited detailed understanding of legal position or problems with crushing medication
• Significant minority unaware of circumstances under which acceptable to give drugs covertly
• Only one fifth of homes had received training in admin of drugs to people with dysphagia in last 5 years
Assessment
• Problems with Deprivation of Liberty Assessments for covert administration
• Representation of private fee payers• Variable delay for assessments of swallowing
by a Speech and Language Therapist
Good practice
• No instances of blanket authority for crushing – decision on ‘case by case’ basis
• 27 homes had a specific protocol for covert administration
• Vast majority of homes taking advice from pharmacists
• Local Enhanced Serviced in Sheffield offers useful model for GP involvement in care homes
Recommendations
• 21 recommendations in total directed at care homes, CCGs and CQC include:– risks of crushing medication covered in induction
+ refresher training for all staff– The best form of treatment rather than cost
should be primary consideration– DoLS assessments should be prioritised for
instances of possible covert medication– CQC should review medication practices for
people with dysphagia in targeted inspections
Media • New report highlights ‘worrying trends’ in care of the elderly - The
Patients Association• Medication training urged as study shows care home residents struggle
swallowing - BT News• New dysphagia recommendations for care homes - Dispensing Doctors’
Association • 50% of care home residents affected by swallowing difficulties - Care
Industry News• Concerns over medication crushed into food - QCS • New Report Highlights Worrying Trend in Care Homes – Care News Today• Medication training urged as study shows care home residents struggle
swallowing - Care Appointments
Interviews
• BBC Radio 5 Live’s Morning Reports• Sky News Radio• BBC1 Breakfast• 5 Live Breakfast • Nine regional BBC radio stations
Next steps • Report from Round table • Commitments from CQC & Waltham Forest CCG• Individual briefings • Dysphagia Advisory group • Resident and Relatives Association conference • Patient safety groups• Look at other aspects of swallowing – e.g. food
Advisory group • Advisory Group met three times since the report
– May, September and November 2016• Martin Vernon, National Clinical Director for
Older People and Integrated Person Centred Care, NHS England and Acosia Nyanin, Head of Inspection, Care Quality Commission both attended last meeting to hear from group
• Advisory Group developing framework for dysphagia and medicines management in care homes- includes patient expectations and staff information.
In development….
• Protocol/ resource pack for ‘dysphagia and medicines in care homes’. Will include:
• Information and advice about swallowing difficulties
• Legal implications of covert medication• Importance of decision specific capacity• Charter re use of medication in care homes.• Care home networks to share good practice to
help prevent isolation and facilitate collaboration.
Other projects with WFCCG
• Reaching for a gold standard• Patients Participation Groups in GP practices• Care academy with Leyton Sixth Form CollegeAnd with other trusts:• Complaints handling improvement – peer
review, patient review panels, staff training , independent investigation
• Others

The Patients AssociationPO BOX 935, Harrow, Middlesex, HA1 3YJEmail: [email protected]
Telephone: 020 8423 9111Fax: 020 8423 9119
Email: [email protected]
Reflections of the pastElla Otomewo, Poet and Spoken Artist
What Does Great Care Look Like?
How to Measure and Improve
Anne Walker - Deputy Nurse Director Quality and Clinical Governance
2/1/2017Nursing Conference WF CCG November 2016
99
Good news does not sell newspapers!
Providing Healthcare That is Great! Often choosing a home happens at pace, families working
under pressures and stresses of moving a loved one to a
new home.
Health care is high credence and intangible, you can not
see what great care looks like, so how do you instill
confidence in patients and families and help them make the
right decision?
What one perceives as good is different to another?
What can you see?
2/1/2017Nursing Conference WF CCG November 2016
100
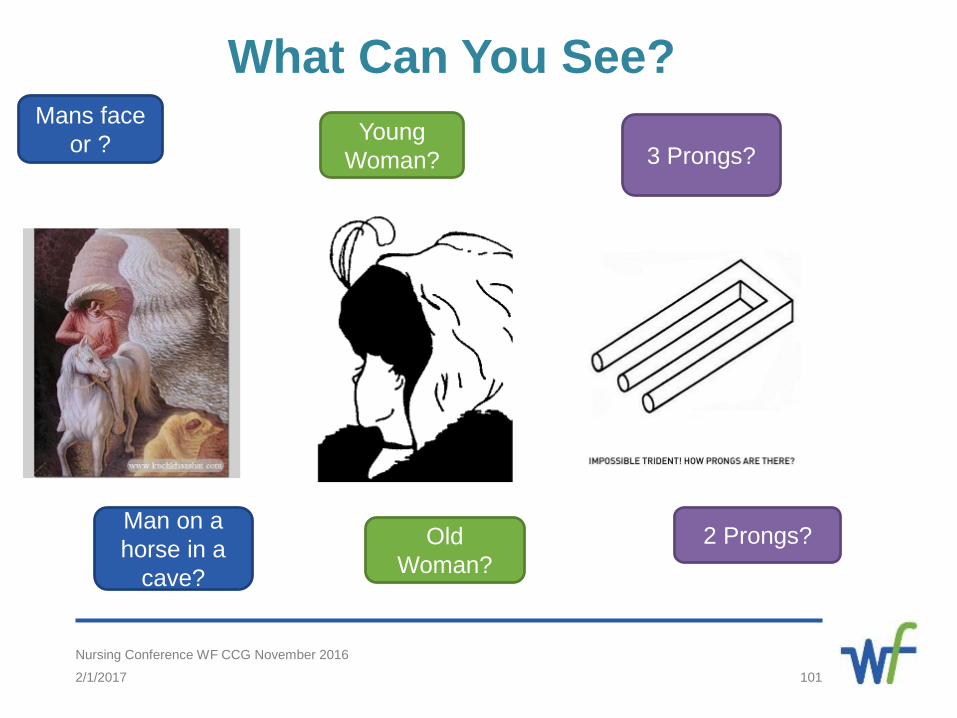
What Can You See?
2/1/2017Nursing Conference WF CCG November 2016
101
Mans face or ?
Man on a horse in a
cave?
Young Woman?
Old Woman?
3 Prongs?
2 Prongs?
Who is Quality Important to?
Patient/Resident
Staff
Clinical Commissioning Groups
Local Authority
Care Quality Commission
2/1/2017Nursing Conference WF CCG November 2016
102
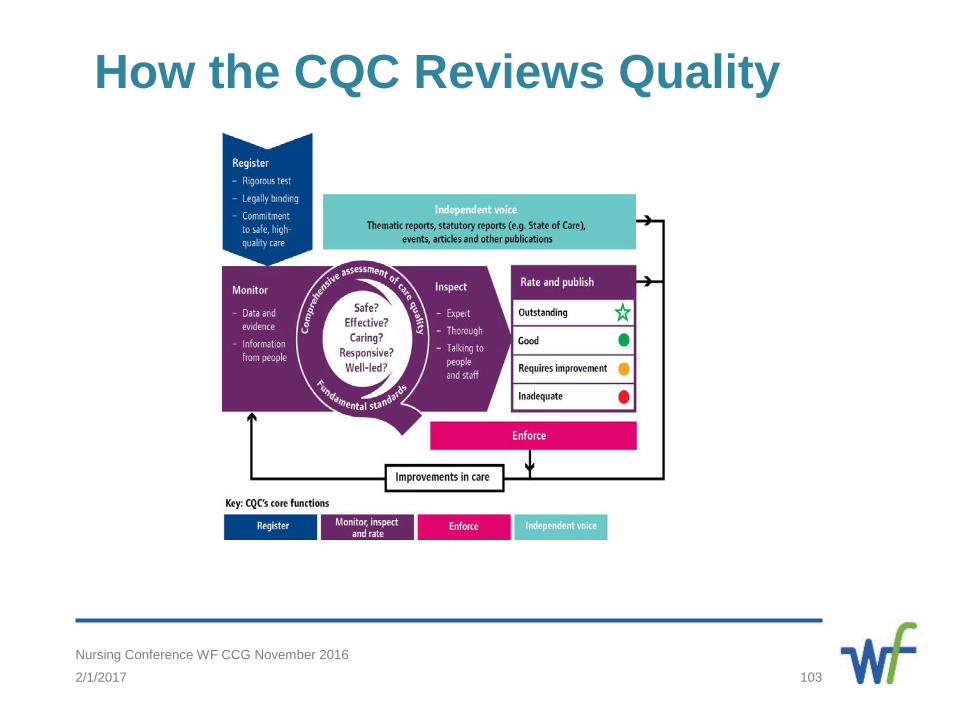
How the CQC Reviews Quality
2/1/2017Nursing Conference WF CCG November 2016
103
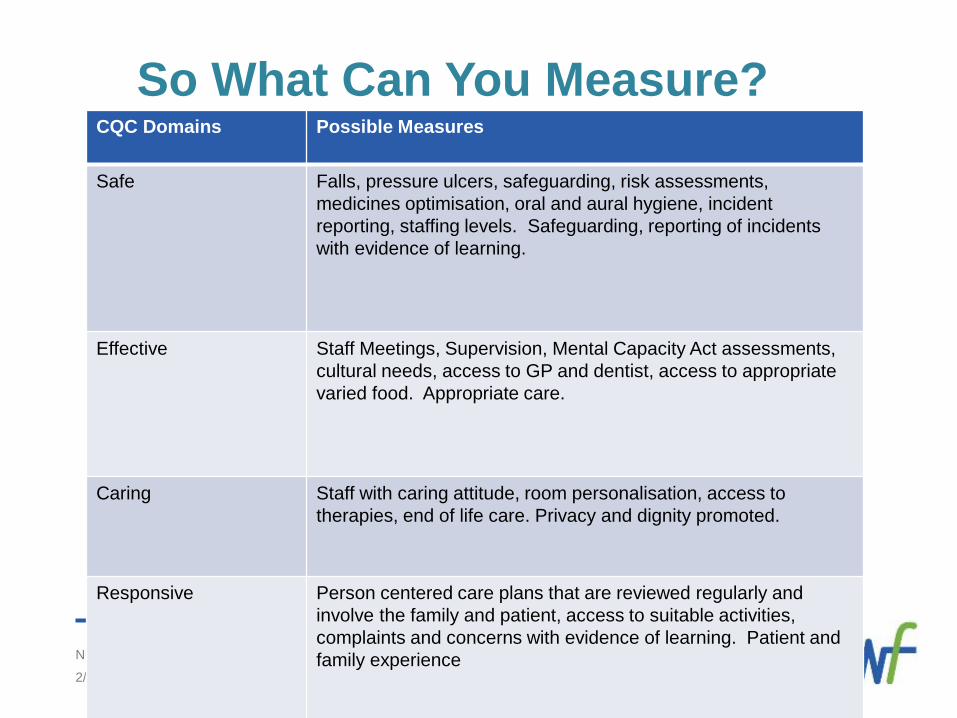
So What Can You Measure?
2/1/2017Nursing Conference WF CCG November 2016
104
CQC Domains Possible Measures
Safe Falls, pressure ulcers, safeguarding, risk assessments, medicines optimisation, oral and aural hygiene, incident reporting, staffing levels. Safeguarding, reporting of incidents with evidence of learning.
Effective Staff Meetings, Supervision, Mental Capacity Act assessments, cultural needs, access to GP and dentist, access to appropriate varied food. Appropriate care.
Caring Staff with caring attitude, room personalisation, access to therapies, end of life care. Privacy and dignity promoted.
Responsive Person centered care plans that are reviewed regularly and involve the family and patient, access to suitable activities, complaints and concerns with evidence of learning. Patient and family experience
Remember What is important to you may not be to someone else.
What gets measured gets done.
Make sure you and your staff talk about quality every day.
Don’t underestimate the value of patient and family feedback
about quality and experience.
Quality improvement is never ending.
Quality measurement is important for you and your staff as
much as it is for external bodies.
Next steps – why not talk to colleagues in the room, set up
peer reviews – “Fresh Eyes”
2/1/2017Nursing Conference WF CCG November 2016
105
Great Care – Happy People
2/1/2017Nursing Conference WF CCG November 2016
106
Thank you – Questions
“We are what we repeatedly do. Excellence, then, is not an act but a habit.” Aristotle