Embed Size (px)
Citation preview

8/26/2016
1
2nd Annual Osteopathic CME
Flagstaff, AZ
8/27/16
My goals for this session are to:
1. Introduce the concept of Biotensegrity as a model that explains how structure and function are intimately related
2. Briefly touch on the idea of sequencing
3. Demonstrate and have a lab for treating ilial somatic dysfunction

8/26/2016
2
Dr. Fred Mitchell Sr. developed muscle energy technique over a 30 year period. His starting point was understanding pelvic mechanics and developing a model to treat and balance the pelvis.
*As relayed by Dr. Stiles: Fred Mitchell Jr. badly burned at age 5 after Halloween costume caught on fire, ARF, family told he would not survive.
*The Mitchells insisted that Dr. Owens (Dr. Chapmans’ son‐in‐law) be allowed to see Fred Jr.‐ He found the Chapmans point and treated it for 30 min. Fred Jr. survived
*Fred Mitchell Sr. was an engineer, felt Osteopathy saved his son’s life, became a DO. Was taught by Owens that you never treat Chapmans’ reflexes until the pelvis is balanced first.
*Mitchell Sr. spent 30 years working out the mechanics of the pelvis.
…Dr. Ed Stiles trained with Dr. Mitchell Sr. The thought process of problem solving when treating with OMT was emphasized through sequencing, finding the “key lesion”, treating in the correct order for each patient.
Dr. Schiowitz, at the very end of his life started teaching a “master class” to relay his thinking process, not his techniques, but how he approached treating patients, why he would treat in essentially the sequence that he did.
“Sequencing adds order to our application of knowledge, it adds intelligence and skill to our assessment” (? Quote AT Still)

8/26/2016
3
• The body is a unit‐ we are each a unit of body, mind and spirit
• The body is capable of self regulation, self maintenance and self healing.
• Structure and function are reciprocally related
• The rational for treatment is based on the above 3 principles
• This idea is unique to the Osteopathic approach to patients particularly when applying Osteopathic Manipulative Treatment (OMT).
• To me, it essentially means‐ Forces/strains introduced into the Neuro‐MSK‐Fascial system can effect the normal anatomic relationship within joints, bone, muscle and their tendinous and fascial attachments, ligaments, and the fascial envelopes containing all of the associated nerve, arterial, venous and lymphatic structures, including organ systems.
• These forces can be can be simple as in stepping off a curb with a straight leg, slipping on the ice and falling on your sacrum or more significant such as going through a difficult vaginal delivery or extreme such as falling 60 ft off a cliff.
8/26/2016
4
“Impaired or altered function of related
components of the somatic (body framework) system: skeletal, arthrodial and myofascial structures and their related neural, vascular and lymphatic components” (from Foundations of Osteopathic Medicine)
• Impaired function of fundamentally normal anatomy, it is not pathology. It is thought to however predispose to and once established, maintain pathology
• Somatic dysfunction may occur as functional impediment due to soft tissue (muscular, ligamentous, fascial) tensions, articular motion restriction, or any combination of these components.
• What maintains somatic dysfunction is a whole other discussion; peripheral vs spinal vs central neural regulatory mechanisms. For example: facilitated segments, “virus in the software” model, local injury with swelling and hypertonicity.
8/26/2016
5
Somatic Dysfunction might not be a joint or a muscle problem but a Software problem and the muscle guarding is only the bodies protective mechanism and expression of the C.N.S adaptive efforts.
Proposes that freeing up motion restriction of a restricted articulation stimulates mechanoreceptors which in turn inhibits nocioceptors(B.Wyke) and effects a change in CNS patterning.
Introduction of a “virus” into the software of a computer; it can no longer function properlyFrom slide‐ Dr. Stiles Muscle Energy Essentials, from the work of Dr. Robert Williams II, Engineering Mechanics of Human Motion
Applying the principles of tensegrity to Osteopathic diagnosis and treatment shifts our paradigm from a classical biomechanical (linear‐ ie Hookes law where the amt a material changes in length or strain is equally proportional to the force or stress applied to it) to a bio‐dynamic (non‐linear) approach.
It explains the relationship that structure and function are reciprocally related, that each patient is unique, that no two patients present the same way, that the body is capable of instantaneous and lasting changes once we; ”remove the hindrance (find it), fix it and leave it alone.” ‐AT Still
8/26/2016
6
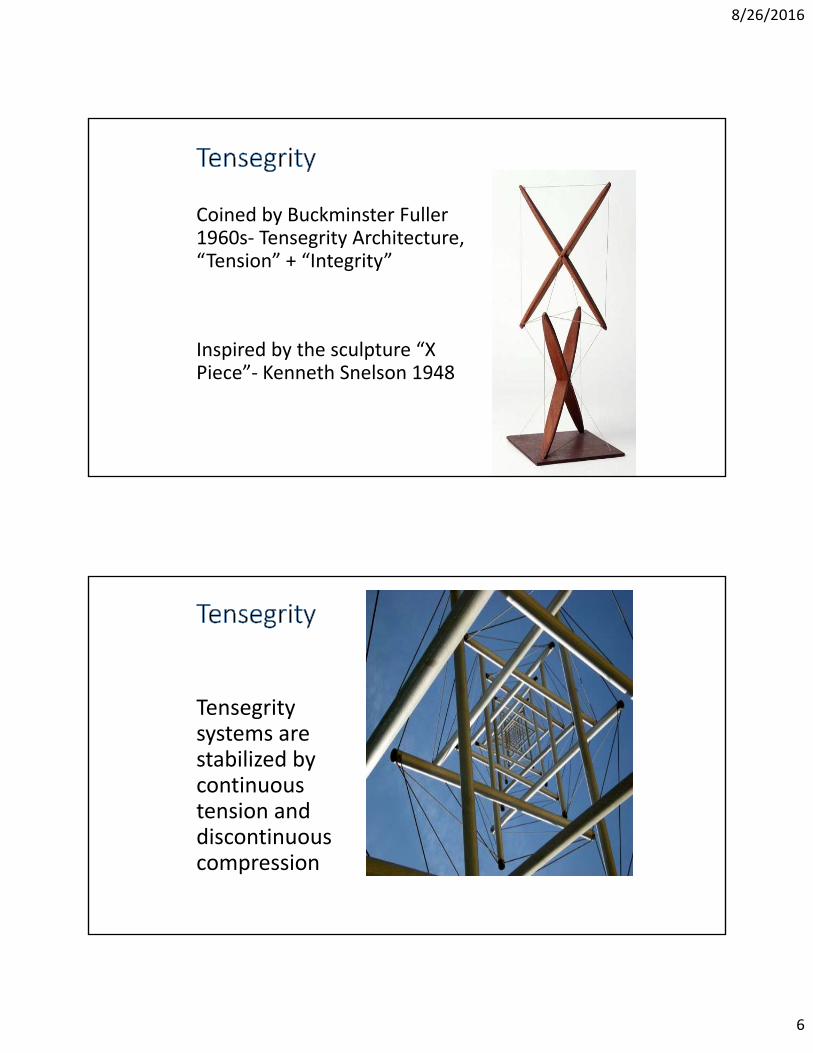
Coined by Buckminster Fuller 1960s‐ Tensegrity Architecture, “Tension” + “Integrity”
Inspired by the sculpture “X Piece”‐ Kenneth Snelson 1948
Tensegritysystems are stabilized by continuous tension and discontinuous compression
8/26/2016
7
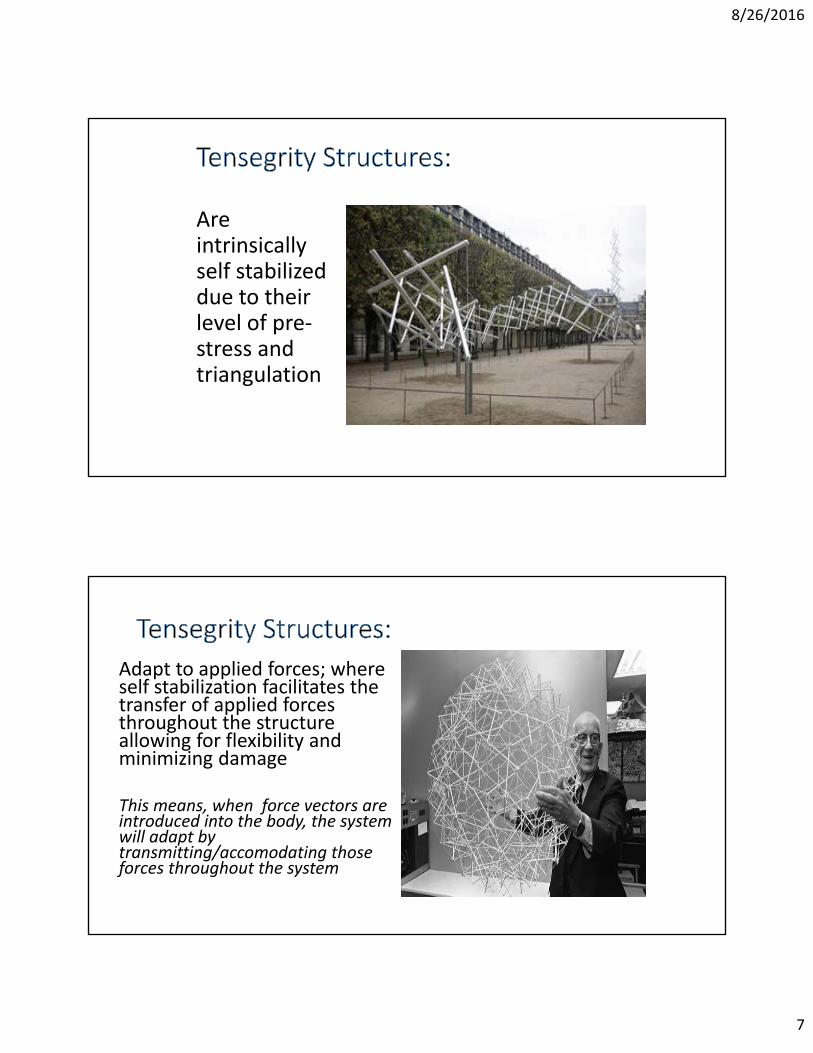
Are intrinsically self stabilized due to their level of pre‐stress and triangulation
Adapt to applied forces; where self stabilization facilitates the transfer of applied forces throughout the structure allowing for flexibility and minimizing damage
This means, when force vectors are introduced into the body, the system will adapt by transmitting/accomodating those forces throughout the system
8/26/2016
8
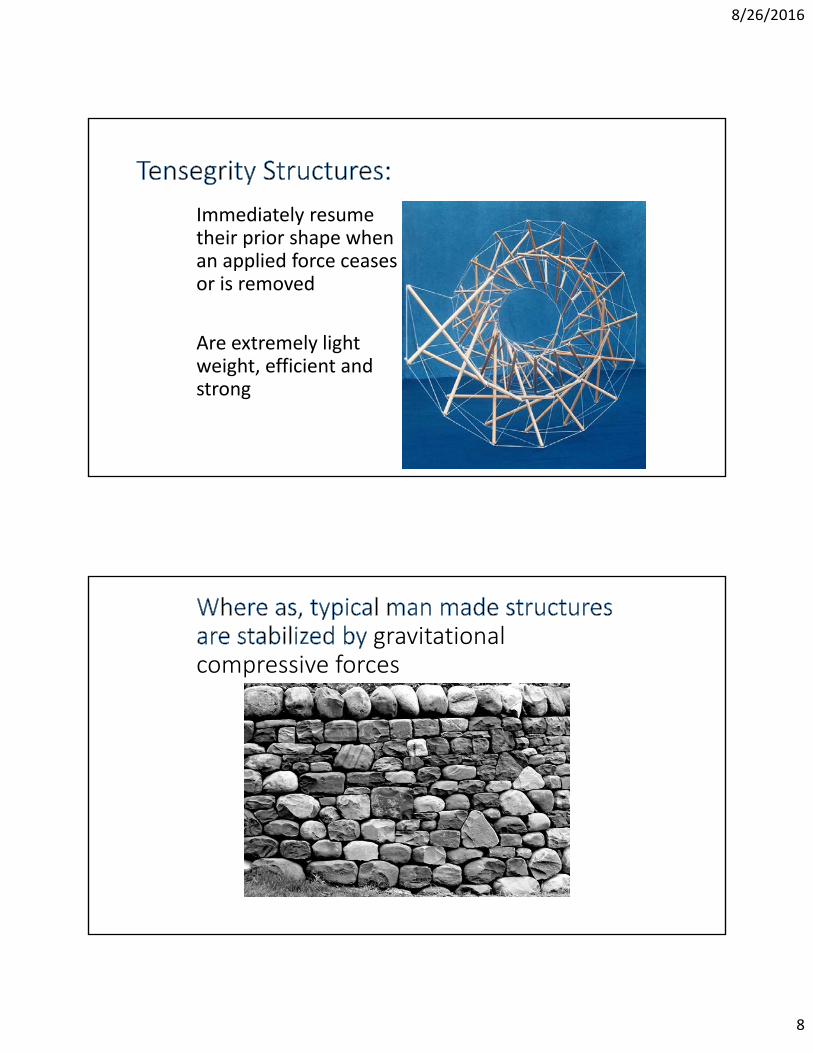
Immediately resume their prior shape when an applied force ceases or is removed
Are extremely light weight, efficient and strong
gravitational compressive forces
8/26/2016
9
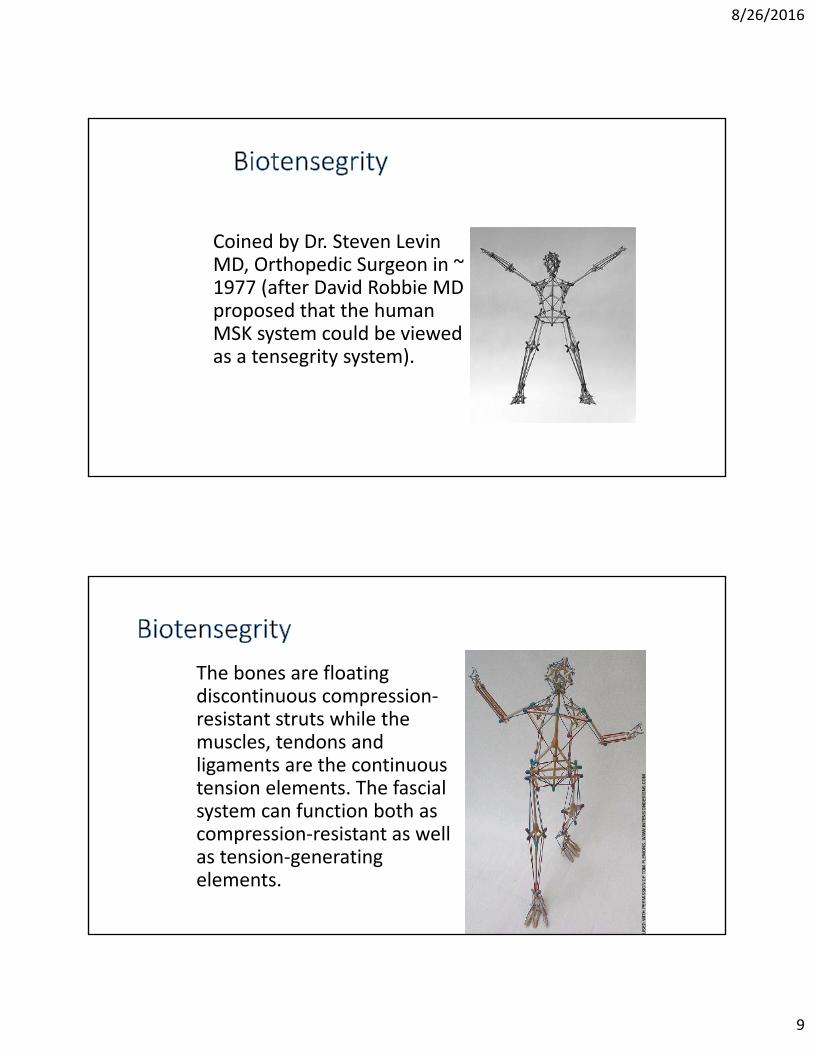
Coined by Dr. Steven Levin MD, Orthopedic Surgeon in ~ 1977 (after David Robbie MD proposed that the human MSK system could be viewed as a tensegrity system).
The bones are floating discontinuous compression‐resistant struts while the muscles, tendons and ligaments are the continuous tension elements. The fascialsystem can function both as compression‐resistant as well as tension‐generating elements.
8/26/2016
10
“Fascia is a soft connective tissue that plays an important role in the transfer of tension and, until recently, was generally considered to be little more than mere packing(Van der Wal, 2009). Now fascia is more widely recognized as a tissue that is continuous with the extra‐cellular matrix that surrounds virtually every cell in the body(Ingber, 2006); a hierarchical structure that links every bone, muscle, nerve, blood vessel and skin, etc. into a single functioning unit (Schleip et al., 2012, Guimberteau, 2005) and part of a global biotensegritysystem (Levin and Martin, 2012)”. ‐From Scarr pg. 81
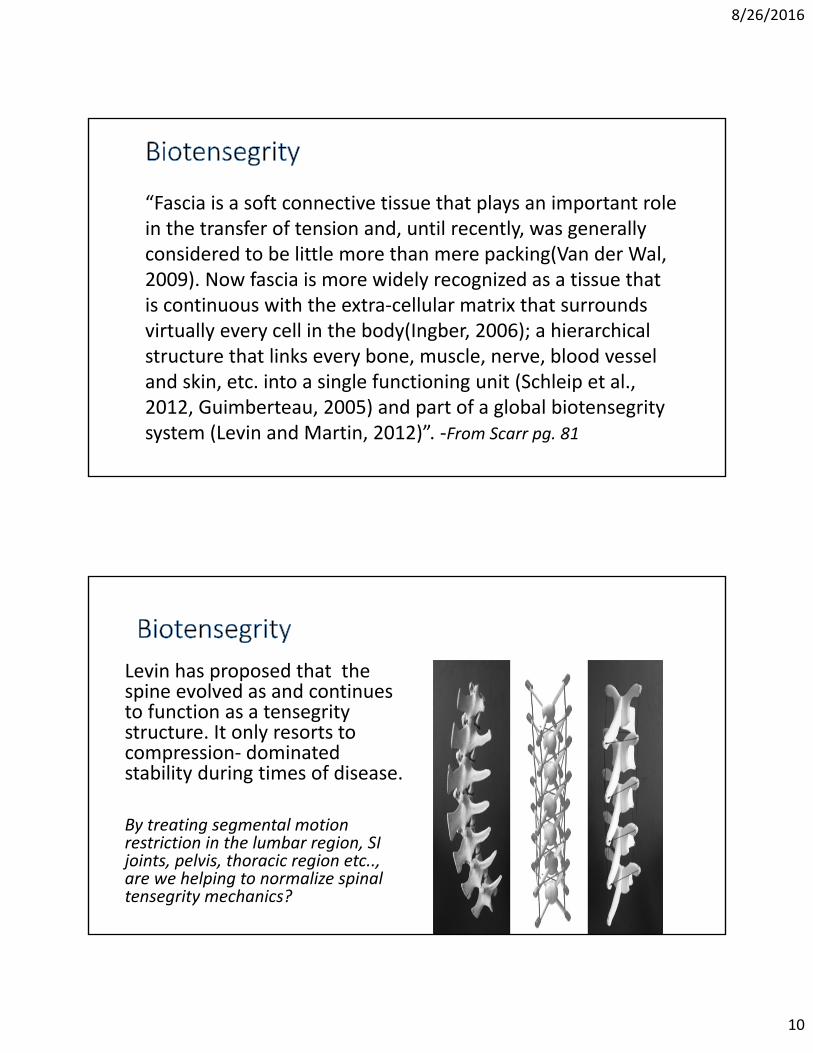
Levin has proposed that the spine evolved as and continues to function as a tensegritystructure. It only resorts to compression‐ dominated stability during times of disease.
By treating segmental motion restriction in the lumbar region, SI joints, pelvis, thoracic region etc.., are we helping to normalize spinal tensegrity mechanics?
8/26/2016
11
Chen and Ingber described the femur as a tensegrity structure; due to its shape and anatomic relationship with the acetabulum, gravitational compressive force from the weight of the body is transmitted through the femur in a curvilinear fashion. At the proximal and distal ends (of all long bones) the bone widens.
Compact bone is replaced with cancellous bone organized around geometric triangulation with some struts under tension and some resisting compression. This arrangement provides maximal stability and aids in receiving and dissipates force throughout the joints.
Biotensegrity likely explains how the
Mass of the largest dinosaurs was
supported by their structure
8/26/2016
12
• Started working on the theory that cells are tensegrity structures as a graduate student in ~1975
• After 25 yrs of research Ingber and others have established that cells are pre‐stressed tensegrity structures with tension producing (ie. Microfilaments) and compression resistant ( ie. Microtubules) elements.
• Is a fundamental building block of biological organisms
• It can be demonstrated at all size scales from the musculoskeletal system to organs (such as the lungs), tissue, cellular and molecular levels. Each system is linked in a hierarchical organization with the level above and below.
• There is a hierarchical organization of biological systems within systems within systems.

8/26/2016
13
• Cells to respond to changing external forces by transmitting forces throughout the cell
• Transmembrane proteins called integrins form focal adhesion proteins that couple (integrate) proteins of the ECM to those that form cytoskeletal tensegrity system (microfilaments and microtubules).
• Studies on cultured cells have confirmed a direct connection exists through the cytoskeleton of cells down into its nucleus
• Mechanical signals are received via pre‐stressed tensegrity cells linked hierarchically to the ECM and nucleus. These mechanical signals are integrated with other biochemical signals producing an orchestrated cellular response‐essentially effecting cellular processes such as protein synthesis and messenger RNA transcription.
8/26/2016
14
• “These Principles can demonstrate the structure‐ function relationship at all size scales of the human body”‐R. Swanson DO, PhD
• Tensegrity structures distribute strain throughout the structure along the lines of tension, the tensegrity structure may “give” at some weak point far removed from the area of the applied strain
• “One of the truths of a tensegrity system is that it always tries to protect the weakest area” (somatic dysfunction)‐Ed Stiles DO,
”…how the bones on either side of a joint can remain stable yet move with a minimum of effort, and how the soft tissues are able to guide them. It describes how each tissue can be integrated into a complex tensional network that extends in all directions, and forms an ’automatic shifting suspension complex’ that couples multiple joints (and the entire body) into a functioning unit”. (G. Scarr pg 68)

8/26/2016
15
• A patient presents for OMT with the complaint of low back pain. After evaluating that patient it is not uncommon to find that clinically, the area of greatest restriction (AGR), the place we treat first, may not be in the lumbar region.
• Dr. Ed Stiles‐ retrospectively reviewed 100 charts of patients with mechanical LBP, 60% of them the AGR (area of greatest restriction or “key lesion”) was either in the thoracic or rib regions.
How is it that the “key” somatic dysfunction (area of greatest restriction) might not be where the chief complaint is?I think the idea of the body as a tensegrity structure explains this quite well
By not identifying and starting treatment with the area of greatest restriction are we just “chasing pain” and treating the bodies compensation without treating the root of the problem?

8/26/2016
16
• The diagnosis and treatment of somatic dysfunction addresses each patient as a unique whole, a unique biotensegrity structure.
• Each pt is unique, therefore each treatment is unique and based upon the palpatory findings of that individual.
• The somatic dysfunction that feels the most brittle, the most unyielding and has a very hard end feel, is the area of greatest restriction. (I wanted to at least introduce the concept of sequencing, starting with the AGR as I feel that this model truly approaches each pt as a unique tensegrity structure)
“You can have 100 patients with the same diagnosis but remember that they all got there by a different (unique) route” –Irwin M Korr PhD
…Therefore expect unique findings for each patient.
“Find it, Fix it and Leave it alone”‐AT Still
8/26/2016
17
“The aim of treatment whether functional or structural technique (HVLA) is applied, is to re‐establish motion that is consistent with the structure.
The goal of manipulative therapy is harmonious (integrated) motion.
Motion is the added dimension to the structure”
Fred Mitchell Sr. DO, FAAO 1967
I thought that I would focus on pelvic somatic dysfunction for the lab portion of this talk.
I have treated a number of patients with LBP, lateral hip pain, lower extremity pain, pubic pain, thoracic pain, headache etc.. who have failed other treatment modalities. One of the common themes I have found is that they had significant ilialand or sacral somatic dysfunction that was not addressed.
8/26/2016
18
34 yr old G4P5, 11 months postpartum c/o daily non‐radicular LBP, left groin and left abdominal pain that started at 25 wksgestation and did not improve after NSVD, the pregnancy was complicated by polyhydramnios. She delivered a healthy FT baby.
Pain worse with activity and sitting long periods time
Nothing helping her pain‐ Is going to PT, tried Ibuprofen
Impact‐ hopeless, unable to walk comfortably, unable to lift her kids without pain, sometimes effects her sleep.
Gait‐ decreased ilial motion all phases of gait on the left,
Pelvis‐Left anterior ilial rotation with inferior pubic shear
SI‐left U/L sacral flexion, b/l SI restriction
Lumbar‐PVMS left, decreased segmental motion with forward bendingT12‐L1 & L3 down, L5FRSr, inc. lumbar lordosis
Ribs‐left L‐T jxn, b/l lower ribs restriction
8/26/2016
19
Started with her ilial SD‐ instant relief, broke into tears
FPR to ilial, SI and lumbar somatic dysfunction, MFR/BLT to L‐T and L‐S jxns, lower ribs and pubic compression/decompression.
After treatment her gait was improved and she stated she felt better.
2 week follow up‐stated was better than had been in awhile, breathing better, posture felt better, had more energy and able to do more activity.
C/O discomfort in the L‐T region, left groin and PSIS.
F/U 2 months later continued to improve, working out, walking with her kids an hour at a time.
Tissue texture changes
Asymmetry
Restricted Motion
Tenderness
8/26/2016
20
• Start with structural exam:
• Observe gait • Check static symmetry
• Check for lateral and AP curves• Observe for segmental motion restriction of the lumbar spine with forward bending
• Standing and seated flexion tests• Check for segmental motion restriction and TART
1. Diagnosis of ilial and pubic somatic dysfunction
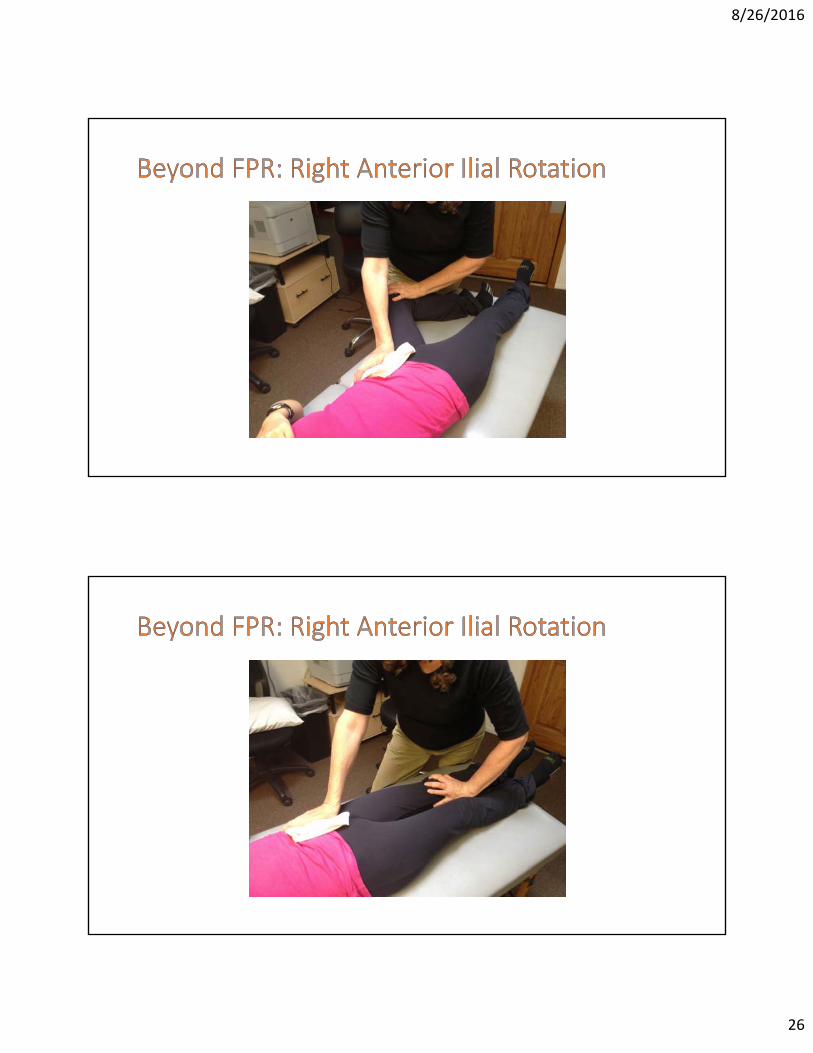
2. Beyond FPR for Anterior Ilial rotation
3. Beyond FPR for Posterior ilial rotation
4. Articular technique for superior ilial shear
5. Treatment of ilial down shear
6. Pubic compression/decompression
8/26/2016
21
• The standing flexion test helps to determine if and on which side there is an ilio‐sacral problem
• The pt stands with their feet 6‐8” apart• Place your thumbs under the PSIS’s
• Have the pt slowly bend forward until they are at maximum forward bending
• Have the pt straighten up about 30 degrees and reset your thumbs making direct contact with the inferior surface of the PSISs
• Have the pt fully bend forward again
• As your thumbs roll up with the motion of the PSISs, measure the distance each has moved.
• The side that has moved the most is interpreted as the restricted side
• **There must be at least ½” difference in motion to say that you have a positive test (according to Dr. Schiowitz).
8/26/2016
22
• PT supine• Have your partner place their middle finger across the PSIS to the SI joint (middle transverse axis) with their pointer just above the level of the PSIS (superior transverse axis) and their ring finger just below (Inferior transverse axis) to help you to localize your forces
• Place your hands over each ASIS• Aim a slight compressive force into the SI joint, localizing your force at each of the 3 transverse axes)
• Note which axis or axes feel restricted
• +SFT lateralizes side of ilial dysfunction• Abnormal ilial motion with gait often correlates with dysfunction
• Compression test‐3 horizontal axes
• ASIS static symmetry and palpation of relative ilial rotation
• Static symmetry medial malleoli
• Functional vs Structural leg length discrepancy
8/26/2016
23
• Check static symmetry of the superior pubic rami
• U/L pubic dysfunction is named for the same side as the positive standing flexion test
• Pubic compression findings: tissue texture changes in the pubic region, TTP over the pubic symphysis, ASIS springing may be + b/l, superior and inferior gliding and posterior spring are all restricted, superior rami are level (unless a shear is present).
Dysfunction side:
+ Standing flexion test
+ Compression test (inferior transverse axis)
ASIS inferior
Ilial rotation anterior
PSIS superior
Medial malleolus inferior (relative long leg)
8/26/2016
24
Dysfunctional side:
+Standing flexion test
+Compression test (inferior transverse axis)
ASIS superior
Ilial Rotation Posterior
PSIS inferior
Medial malleolus superior (relative short leg)
Dysfunctional side:
+Standing flexion test
+Compression test (all 3 transverse axes)
ASIS superior
Ilial rotation posterior
PSIS superior
Medial Malleolus superior (relative short leg)
8/26/2016
25
Dysfunctional side:
+Standing flexion test
+Compression test (restriction all 3 transverse axes)
ASIS inferior
PSIS inferior
Medial malleolus inferior
Findings:
Anterior ilial rotation
Fixed superior malleolus
Compensatory lumbar convexity following sacral base un‐leveling (on the side of the short leg).
8/26/2016
26
8/26/2016
27
• The pt is supine• Stand on the same side of the table as the functional short leg (right side)
• Have the pt flex their hip and knee placing their right foot flat on the table next to their left knee.
• Letting the pt know what you are going to do, adduct the pts knee over midline, causing the right buttock to raise off the table.
• Place your left hand on the table, palm up with fingers pointing caudad, under the ptsraised buttock.
• Bring the pts knee back so that the ptsbuttock rests on your left palm.
• Flex the fingers of your left hand so that they hook onto the pts ischial tuberosity.
8/26/2016
28
8/26/2016
29
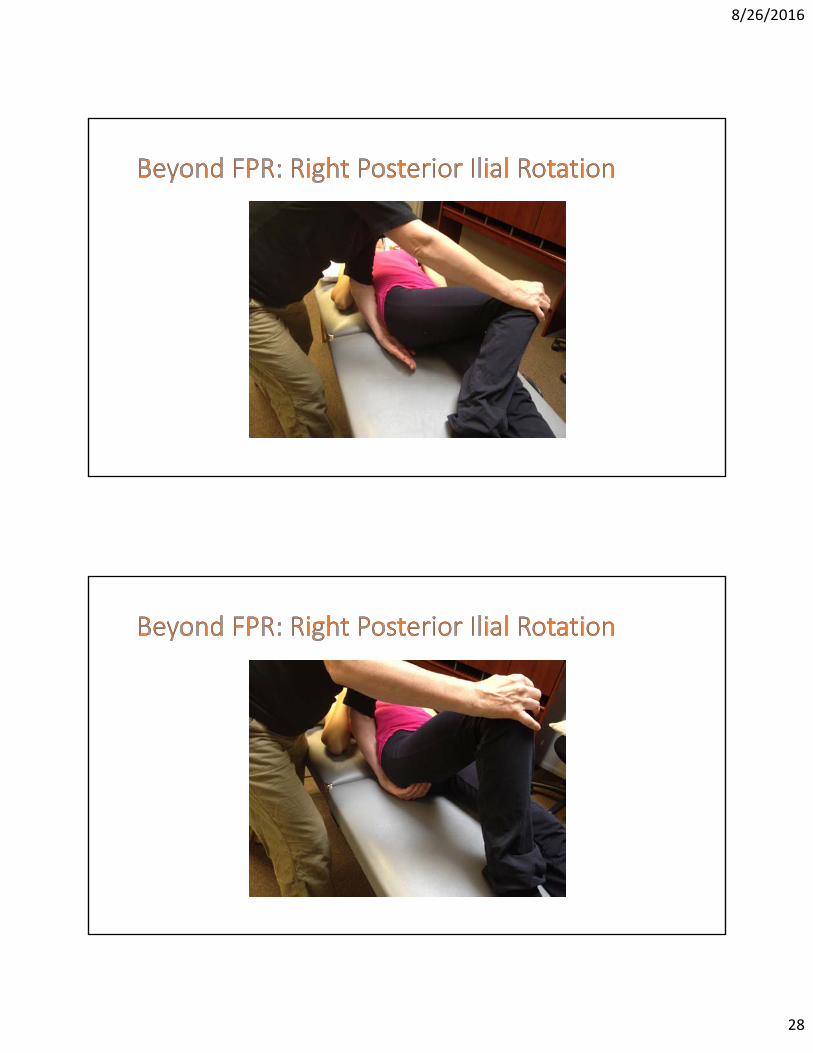
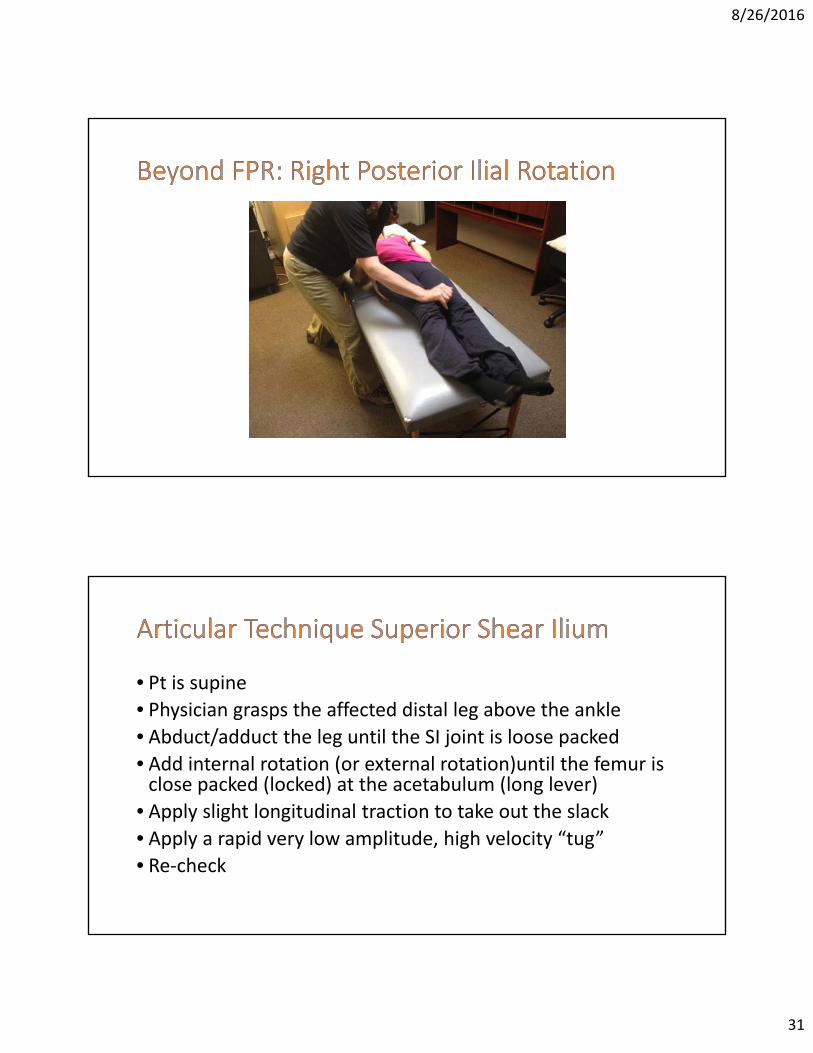
• Have the pt place the plantar surface of their right foot flat against the medial surface of their knee (“frog leg” position).
• Again, tell the pt that when you ask them, to straighten their leg by sliding their right foot down the left leg.
• With your right hand, place a mild downward counterforce on the pts medial knee (a few pounds)
• Ask the pt to slide their foot down their leg. As they do, use your left hand to pull/rotate the ischium in a cephalad direction, maintaining the counter force on the knee, until the pts right leg is straight.
• Recheck

8/26/2016
30
8/26/2016
31
• Pt is supine• Physician grasps the affected distal leg above the ankle• Abduct/adduct the leg until the SI joint is loose packed• Add internal rotation (or external rotation)until the femur is close packed (locked) at the acetabulum (long lever)
• Apply slight longitudinal traction to take out the slack• Apply a rapid very low amplitude, high velocity “tug”
• Re‐check
8/26/2016
32
• Patient is supine• Place the middle finger of the cephalad hand at SI jt. at the level the PSIS (middle transverse axis) with the pointer just above (superior transverse axis)and the ring finger just below (inferior transverse axis)
• Abduct/adduct the leg until the SI joint feels as relaxed as possible (balancing all 3 transverse axes)
• Internally rotate ( or externally rotate) the leg until the femur locks (close pack) in the acetabulum (long lever).
• Have the patient take a deep breath, on the exhale glide the ilium cephalad‐ this can be accomplished by grasping the knee and applying a cephalad force or grasping the bottom of the foot. You can glide the ilium cephalad, applying low amplitude springing, or lean into the leg and provide a gentle thrust.
• recheck

8/26/2016
33
• Patient supine with hips and knees flexed, feet on the table 10‐12” apart
• Hold the patients knees together, ask them to push their knees apart while offering an isometric counterforce for 3‐5 seconds, relax 3‐5 seconds and repeat.
• Next, have the pt spread their knees apart, place the heel of one hand at the medial aspect of one knee and the palm of the other hand at the medial aspect of the other knee.
• Ask the patient to push their knees together for 3‐5 seconds, again while offering an isometric counterforce. Relax for 3‐5 seconds and repeat 2‐3 times.

8/26/2016
34
References1. Findley,T‐ Fascia Research 2015‐State of the Art
(Summary) 2. Findley,T‐ Fascia research, 100 years Since Andrew
Taylor Still‐ Video of Lecture, Fascia Research Society
3. Myers,T‐ Anatomy Trains, Churchill, Livingstone, Elsevier 2014, pgs 1‐61
4. Nelson,K ed.‐Somatic Dysfunction in Osteopathic Family Medicine, Lippincott Williams and Wilkins 2007, pgs 1‐15
5. Scarr, G ‐Biotensegrity: The structural Basis of Life Handspring Publishing Limited 2014
References
6. Stiles, Ed. DO, FAAO‐ Various Written Course material and personal notes7. Swanson,R‐ Biotensegrity: A Unifying Theory of Biological Architecture with Application to Osteopathic Education and Research‐A Review and Analysis JAOA 1/13 vol. 113, pg. 34‐528. Wearing, Schleip, Chaitow, Klinger, Findley editors‐ Fascia Research IV: Basic Science and Implications for Conventional and Complementary Health Care, Kiener, Munich 2015