Embed Size (px)
Citation preview

a CoMpreheNSive report oN the
Quality oF Care iN aMeriCa’S NurSiNg
aNd rehabilitatioN FaCilitieS
Annual Quality Report2011


TA B LE O F CO N T EN T S 1
Table of Contents
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change . . . . . . . . . . . . . . . . . . . . . . 10
Quality Trends: By the Numbers . . . . . . . . . . . . . .26
Special Update: Advancing Excellence in America’s Nursing Homes . . . . . . . . . . . . . . . . .36
Hospitalization of Nursing Home Residents . . . 44
Focus on Rehabilitation Measures . . . . . . . . . . . .58
Transitional Care: Challenges and Opportunities for Nursing Home Residents . . . .70
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .78

2011 A N N UA L QUA L I T Y R EP O R T2
Overall, the long-term
and skilled nursing care
community’s commitment to
ongoing and sustained quality
improvement is paying off
with positive trends in quality
measures, quality indicators
and patient outcomes.
Executive Summary

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 3
Executive SummaryDavid Gifford, MD, MPH
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix
Executive Summary

2011 A N N UA L QUA L I T Y R EP O R T4
The American Health Care Association (AHCA)
and the Alliance for Quality Nursing Home Care
(Alliance) are committed to improving quality in
our nation’s nursing facilities. The third annual
2011 Quality Report provides details on our efforts
to improve quality on behalf of our patients,
residents and employees in the last year. In
large part, this report compiles the research and
analysis of independent and highly regarded
issue area experts to illustrate trends in skilled
nursing and rehabilitative care and to identify
areas that should be pursued to further enable
providers to achieve performance excellence
through improved patient outcomes and quality
of life for residents and staff alike.
Skilled nursing facilities serve a critical role in the care of patients discharged from hospitals who require ongoing medical care and rehabilitation for a full recovery. Of all Medicare beneficiaries who require ongoing post-acute care after discharge from a hospital, 50 percent go directly to a skilled nursing facility for care and services, before they can safely return home. The primary goal of skilled nursing care is to help individuals maximize their functional ability and restore independence so that they can return to their prior living situation. Just over a third of individuals admitted to skilled nursing facilities return to their prior living situation, usually to their home or an assisted living community. In this year’s report, we focus on several of the key quality areas related to our community’s increasing role as post-acute care providers.
The 2011 Quality Report features expert analyses by Avalere Health; Mary Jane Koren, MD, MPH; Andrew Kramer, MD; and Mary Naylor, PhD, FAAN, RN. As in past years, the report also includes quality data and trends as reported by the Centers for Medicare and Medicaid Services (CMS) and the most recent consumer and employee satisfaction data as compiled by My InnerView, an independent research company that collected satisfaction data from nursing facility employees, residents, and family members.
This year’s report builds on the data and analyses presented in previous Quality Reports. With growing public and private initiatives for our nation’s health system to deliver integrated and coordinated care across settings, contributing authors to this report evaluate the role of skilled nursing facilities in these
Executive Summary

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 5
new models and discuss important measures that appropriately assess quality throughout the health delivery system.
AHCA and the Alliance stand strong in our commitment to advance quality in nursing facilities nationwide. We look forward to working with Congress and the Administration to develop and implement effective and integrated post-acute care policies so that patients receive essential nursing and rehabilitative care in the most appropriate setting for them to recover and safely return home.
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System ChangeIn this year’s report, Avalere Health evaluates the state of nursing facilities in the health care profession and the evolving role of skilled nursing facilities (SNFs), particularly in regards to the establishment of a sustainable, accurate quality measurement system. This chapter asserts that the current quality measurement system is flawed and requires substantial changes, and the future of Medicare payment reform initiatives depends on the development of a robust quality measurement framework.
As the primary provider of post-acute care services to the Medicare population, SNFs are a pivotal piece of the post-acute care continuum and will play an important role in the success of new payment reforms. The evolution of nursing facilities as providers who serve two distinct populations – short-stay, post-acute patients and long-stay residents – has created challenges for the standardized quality measurement. Of particular concern, according to this report, is the increase in post-acute treatment plans that include rehabilitation services. Rehabilitation is an essential
DAVID GIFFORD, MD, MPH
Dr. David Gifford
joined the American
Health Care Association
and National Center
for Assisted Living in
May 2011 as Senior
Vice President of
Quality and Regulatory
Affairs. As one of the
nation’s leading experts
on nursing home
quality, Dr. Gifford
will help further advance the community’s quality
improvement efforts.
Prior to joining AHCA/NCAL, Dr. Gifford served as the
Director of the Rhode Island Department of Health. In this
capacity he refocused the nursing home survey process
to promote a more home-like, person-centered model of
care. He has continuously advocated for public reporting
of quality of care, which resulted in Rhode Island being the
first state to publicly report consumer satisfaction data for
all hospitals, nursing homes and home health agencies.
Dr. Gifford has also served as Chief Medical Officer for
Quality Partners of Rhode Island where he directed CMS’
national nursing home-based quality improvement effort.
Dr. Gifford participates in or chairs numerous national, state
and local health-related committees. Dr. Gifford serves
as council chair for the National Quality Forum’s Public
& Community Health Council and is a member of the
National Commission on Prevention Priorities. He served
on the National Governors’ Association Health Information
Communication and Data Exchange Task Force.
He also currently holds a position as clinical Associate
Professor of Medicine and Community Health at
Brown University.

2011 A N N UA L QUA L I T Y R EP O R T6
component of care, yet such treatment plans are accompanied by other core complexities, such as increased medical data, a decrease in the average length of patient stays, and an increase in severity of illness patient categorization.
Though at one time appropriate, the current quality measurement framework does not accurately capture the care provided today by nursing facilities. The current nursing facility quality measure set does not adequately assess improvement in functionality or the most common conditions. The current measure set is dominated by long-stay measures, leaving a need for comprehensive, sophisticated short-stay quality measures. Avalere also reports on the need for a more robust risk-adjustment methodology, as the current system does not reflect all of the important distinctions across health care settings and patient populations.
Avalere offers recommendations to policymakers regarding potential improvements to the nursing facility quality measurement system, including the development of more measures specific to short-stay nursing facility patients; the refinement of risk-adjustment methodologies; and the development of new measures to be used across post-acute care settings.
Quality Trends: By the Numbers As in previous reports, AHCA and the Alliance present publicly available data pertaining to the quality of care delivered in our nation’s rehabilitation and skilled nursing facilities.
Historically, CMS has tracked and released this quality data. The data is grouped into two sets known as Quality Indicators (QI) and Quality Measures (QM). The QIs help staff identify potential patient complications or problems that may require additional attention. The indicators also help facilities track trends, compare performance to similar facilities
across the state, and identify areas for improvements, while QM reports are used to evaluate aspects of care on a facility-by-facility basis.
The data presented indicate nursing facilities are continuing to improve in a majority of QMs and QIs. Since 2009, nursing facilities have made measureable improvements in nine out of 10 QMs. The report also tracks trends in 26 QIs since 2000, which show improvement in 16 key quality areas.
The report also shows trends in facility health survey citations and facilities cited for substandard quality of care, both of which have steadily declined since 2009.
Last, we borrow data from independent researchers My InnerView to highlight trends in the nursing facility consumer (resident/family member) satisfaction and employee satisfaction. The positive trends in overall satisfaction with nursing facility care – on both the consumer and employee levels – seem to indicate that the implementation of quality improvement initiatives on the facility level leads to increased satisfaction and improved care.
Special Update: Advancing Excellence in America’s Nursing HomesThe Advancing Excellence in America’s Nursing Homes campaign, launched in 2006, is an example of a successful quality-improvement initiative that is positively impacting quality in our nation’s nursing facilities. This dynamic public/private partnership is made up of more than 30 long-term care stakeholder organizations who are working together to offer guidance in the quality improvement process and free educational resources to nearly half of all nursing homes nationwide.
Increased participation in the Advancing Excellence campaign is a strong indication of the profession’s

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 7
dedication to improving quality care. Participating nursing homes commit to and set individual performance targets for at least three aggressive campaign goals. One impressive feature of the campaign are the Local Area Networks of Excellence (LANEs), which are localized organizations that provide direct state support to participants in achieving their clinical and organizational goals. The principal purpose of LANEs is to provide easily accessible education and training to increase performance in participating homes. Currently, there are 52 established LANEs, including all 50 states, the District of Columbia and the Virgin Islands.
Entering Phase 2 of Advancing Excellence, more than 47 percent of America’s nursing facilities are participating in the Campaign and that number continues to climb.
Hospitalization of Nursing Home ResidentsMany of the elderly who require post-acute care are frail, with multiple medical conditions, and have multiple functional limitations. Thus, it is not surprising that many are at risk for rehospitalization. In fact, nearly one in four elderly patients returns to the hospital during their covered Medicare stay, and nearly one in three long-term care residents are rehospitalized in a given year. Many of these elderly individuals find themselves circling between the hospital, the emergency room and the skilled nursing facility.
The circling between a nursing facility and the hospital has been recognized as an important public policy issue because of the relationship to poor quality of care and as a significant driver of health care costs. Recent efforts to prevent rehospitalizations have resulted in significant reductions in hospitalization rates of nursing facility residents. Unfortunately, current payment systems do not

2011 A N N UA L QUA L I T Y R EP O R T8
reward providers for implementing these practices and often create a financial disincentive to implement changes to reduce hospitalizations.
In recent years, nursing homes have increasingly admitted post-acute patients that pose unique challenges that differ from managing traditional hospital discharges to home. Providing services to prevent or treat acute illness and avoid hospitalization has always been a high-priority quality concern.
In this chapter, Dr. Andrew Kramer examines some of the challenges facing nursing homes in preventing readmission, identifying avoidable hospitalizations, and measuring their success as well as policy imperatives and their implications for nursing homes.
Specifically, the report finds that pressure to shorten acute hospital length of stay has resulted in sicker patients being discharged sooner to SNFs, resulting in increased hospitalization. Challenges facing nursing homes involve the development and use of valid measures to track hospitalization rates and to compare rates between facilities and over time; the need to develop a proper risk-assessment system to evaluate patients when using rehospitalization rates as a proxy for quality; the development of a measurement to determine if there are avoidable readmissions, how to define such readmissions, and how to prevent them.
Dr. Andrew Kramer discusses strategies for reducing readmissions, such as creating accurate measurement and monitoring of risk-adjusted hospitalization rates. Nursing homes must continue to meet all the needs of short-term residents while at the same time enhancing care and quality of life for the increasingly complex population of long-term residents. While the focus on reducing readmissions to hospitals from all settings is driven by many factors including policy changes and the need to improve care transitions, SNF providers have a great opportunity to be an effective part of the solution.
Focus on Rehabilitation MeasuresDespite the importance of skilled nursing care, there are very few quality measures available to inform customers, policy makers, and payers about care outcomes. Without sufficient measures, for all patient types and conditions, it is difficult to evaluate the effectiveness and value of these services. Currently the quality measures approved by the National Quality Forum for skilled nursing care only focus on three clinical areas: pain management, pressure ulcer prevention, and immunizations. In addition, the CMS Nursing Home Compare website, designed to help consumers evaluate the quality of care provided by skilled nursing centers, examines only four areas: pain, pressure ulcers, delirium and immunizations. While these clinical areas are important, none of them address the primary goal of skilled care, which is to maximize the individual’s functional abilities and independence.
Across the post-acute spectrum, SNFs care for a majority of patients requiring rehabilitative therapies and treat the most varied and disabled populations. Therapy interventions are essential components for short-stay patients to regain strength and the ability to return home and for long-stay residents to maintain function and prevent decline.
Dr. Andrew Kramer assesses the current quality measures utilized across post-acute settings, highlighting the inconsistencies across providers and the need for reform. With the current system that includes multiple transfers to different levels of care, the creation of longer-term and more global measures of function to better track the quality of rehabilitative care are needed.
In his analysis, Dr. Kramer writes that “rather than policy efforts in SNFs to constrain and limit the use of rehabilitation services, SNFs should be encouraged with payment incentives to optimize rehabilitation outcomes through a combination of good nursing,

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 9
medical, and multidisciplinary therapy services. The benefits of investing in optimizing function far outweigh the short-term costs of improved rehabilitation services.” Developing measures that follow patients across episodes of care and track discharge home are consistent with policy efforts to develop better-integrated care with improved transitions across settings.
Transitional Care: Challenges and Opportunities for Nursing Home ResidentsAs elderly individuals transition between care settings and their home, the information exchange is crucial to ensure best outcomes for patients. Frequently, critical information needed to deliver optimum care is not communicated during these transitions. Similarly, patients returning to home often do not receive information about what they need to do to manage their conditions or who to contact when problems arise. Recent efforts on improving transitional care focus on patient and family communication, coaching related to self-management, and knowing when to seek follow-up care. While existing transition of care programs have produced significant reductions in rehospitalizations, current payment models, regulations and information systems do not support effective transitions and again, often create disincentives to implementing effective strategies to improve transitions of care.
Expert authors Katharine Abbot, PhD MGS; Karen Hirschman, PhD MSW; and Mary Naylor, PhD, RN, FAAN highlight opportunities for health care providers, including nursing facilities, to enhance the care and outcomes for the elderly and reduce costs by improving transitions between care settings.
There are multiple challenges to improving transitional care. For instance, the authors identify the lack of
consistent, reliable channels of communication between caregivers. Without the development of proper communication methods, data transfers between settings are inaccurate or incomplete, which is an increasingly difficult problem as nursing facilities see a rise in patient complexity.
Various intervention models illustrate how improved care transitions lead to reduced avoidable rehospitalizations; most notable is the Transitional Care Model (TCM) out of the University of Pennsylvania. This approach, which focuses on the needs of high risk, community-based chronically ill older adults experiencing episodes of acute illness, emphasizes a streamlined plan of care in collaboration with the patient, family caregivers, physicians and other health team members. The National Institute of Health funded a study of this approach and found that the TCM interventions resulted in reductions in time to first readmission or death, all-cause rehospitalizations rates, and total hospital days.
The availability of models such as TCM indicates a drive in the profession to improve the rehospitalization rates of patients and the overall quality care served. Though research is needed to determine the types of interventions best for each patient (e.g., cognitively impaired, short term or long term residents), the opportunity has arrived for facilities and care providers to improve this area of quality care. Additionally, improvements in performance measures of effective transitions and person-centered outcomes must provide the motivation for investment in interventions, coupled with the correct payment incentives. In conclusion, the researchers state, “transitional care approaches…should be made accessible to benefit nursing home residents and are critical to assuring high value care for our society.”

2011 A N N UA L QUA L I T Y R EP O R T10
More short-stay measures
are needed to improve
the comprehensiveness
of the measure set to
ensure that post-acute
care patient outcomes are
accurately assessed.
NEXT STEPS IN NURSING HOME QUALITY MEASUREMENT:
Adapting to a Changing Patient Population AND HEALTH SYSTEM CHANGE

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 11
NEXT STEPS IN NURSING HOME QUALITY MEASUREMENT:
Adapting to a Changing Patient Population AND HEALTH SYSTEM CHANGE
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Avalere Health, LLC : Kathleen O’Connell, Emil Parker, Sally Prendergast, Anne Tumlinson
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix

2011 A N N UA L QUA L I T Y R EP O R T12
The future of Medicare payment reform
depends on robust quality measurement of the
care provided within and across health care
settings. In order for reform initiatives, such as
accountable care organizations, post-acute care
bundling pilots, and value-based purchasing to
be successful, purchasers will need to be able to
identify high quality, cost-effective settings of
care. As the primary provider of post-acute care
services to the Medicare population, nursing
facilities will play an important role in the success
of these payment reforms. However, the quality
measurement framework for nursing facilities is
flawed and will require substantial changes in order
to support the goals of payment reform.
The current nursing facility quality measurement
system largely reflects the historical role of nursing
facilities in providing care to long-stay residents,
rather than to short-stay Medicare post-acute
patients. Long-stay residents are frail, functionally
limited (i.e., unable to perform many basic activities
without assistance), and in many cases cognitively
impaired. Much of this care is financed by Medicaid
or private out-of-pocket payments. Because nursing
facilities have served historically as the residence
for a vulnerable population, these long-stay-
focused measures were developed out of concern
for resident safety and to address serious quality
deficiencies. Accordingly, the quality measures for
long-stay residents generally assess a facility’s
ability to avoid certain negative outcomes, rather
than the quality of care more broadly.
The evolution of nursing facilities as providers who
serve these two distinct populations – post-acute
and long-stay patients – has created challenges for
the standardized measurement of quality of care
provided to nursing facility patients and residents.
There is a very limited set of quality measures for
post-acute care patients, which largely does not
measure improvement in function necessary to
return patients to the community. This chapter will
describe the changing nursing facility post-acute
care patient population and the improvements in
quality measurement necessary to prepare the
system for upcoming Medicare payment and care
delivery system reforms.
NEXT STEPS IN NURSING HOME QUALITY MEASUREMENT:
Adapting TO A CHANGING PATIENT POPULATION AND HEALTH SYSTEM CHANGE

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 13
Nursing Facilities Serve a Post-Acute Care Population Needing Skilled Nursing and Rehabilitation ServicesOver 16,000 nursing facilities provide services to more than 2.5 million post-acute care (PAC) patients and long-stay residents admitted to nursing facilities annually.1 About 1.3 million of the individuals or 52 percent are Medicare or short-stay patients.2, 3 The short-stay, post-acute care patients have significant acute care needs, and receive medical, rehabilitative, and therapeutic care in order to help restore their functioning so that they can return home.
Medicare patients receive post-acute care in other settings as well, such as long-term acute care hospitals (LTACHs), inpatient rehabilitation facilities (IRFs), or at home with home care services. However, nursing facilities are the dominant providers of Medicare post-acute care services, treating over half of all Medicare beneficiaries that are discharged from the hospital to post-acute care.4 Among post-acute providers, only LTACHs have a greater share of high-severity patients (i.e., a higher-acuity population) than nursing facilities.5
Over the years, the post-acute care patients treated in nursing facilities have become more medically complex and functionally impaired. Decreasing
1 Avalere analysis of the 2009 Medicare Healthcare Cost Report Information System (HCRIS) and Point of Service (POS) data bases from the Centers for Medicare and Medicaid Services.
2 Payment sources for the remaining 1.2 million long-stay residents include Medicaid (about 425,000) and private pay or insurance (770,000).
3 Avalere analysis of the 2009 Medicare Healthcare Cost Report Information System (HCRIS) and Point of Service (POS) data bases from the Centers for Medicare and Medicaid Services.
4 Avalere analysis of the 2009 Medicare 100 Percent Standard Analytic File (SAF) claims data base from the CMS.
5 Avalere analysis of 2009 Medicare 100 Percent SAF claims data base from the CMS for Long-Term Acute Care Hospitals, Skilled Nursing Facilities, Inpatient Rehabilitation Facilities, Home Health Agencies and Inpatient Hospitals.
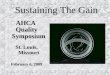
inpatient hospital length of stay may be partly driving this increase in medical complexity. From 2005 to 2009, the average length of hospital stay for Medicare patients discharged to nursing facilities dropped from 7.76 to 7.15 days.6 During the same period of time the acuity of patients discharged to nursing facilities from hospitals increased substantially as demonstrated by the increase in severity of illness scores. The severity of illness (SOI) categories are numbered sequentially from 1 to 4 and indicate, respectively, minor, moderate, major, or extreme severity of illness.7 The portion of nursing facility patient days categorized as major or extreme severity of illness increased from 45.4 to 52.5 percent from 2005 to 2009 (Figure 1).8
Nursing facilities are serving a post-acute population that has substantial comorbidities. From 2005 to 2009, the proportion of Medicare patients discharged from hospitals to nursing facilities with nine or more diagnoses increased from about 66 percent to over 81 percent.9 Of these nine, the top five most common are atrial fibrillation, congestive heart failure, renal failure, hypertension, and urinary tract infections.10 The percentage of patients taking 11 medications or more has also increased since 2005. In 2005, about 43 percent of nursing facility patients
6 Avalere analysis of 2005, 2006, 2007, 2008, and 2009 Medicare 100 Percent SAF claims data base from the CMS for the Skilled Nursing Facilities (SNFs) and Inpatient Hospitals.
7 Patients are assigned their SOI based on their specific diagnoses and procedures performed during their medical encounter, which is generally an inpatient hospital stay. Patients with higher SOI (e.g., major or extreme) are more likely to consume greater healthcare resources and have more serious comorbidities (i.e., the presence of one or more disorder(s)/disease(s) in addition to a primary disease/disorder) than patients with a lower SOI. For example, the severity of illness categorization for respiratory diagnoses progresses from bronchitis (minor), to asthma (moderate), to viral pneumonia (major), and finally to respiratory failure (extreme).
8 Avalere analysis of 2005, 2006, 2007, 2008, and 2009 Medicare 100 Percent SAF claims data base from the CMS for the Skilled Nursing Facilities (SNFs) and Inpatient Hospitals.
9 Ibid.10 Ibid.

2011 A N N UA L QUA L I T Y R EP O R T14
reported using 11 or more medications in the last seven days. By 2009, this number had increased to over 61 percent.11
A key focus of nursing facility care is rehabilitation. Rehabilitation services help patients re-gain speech and motor function as well as master key daily activities, such as bathing and dressing, thereby accelerating patient discharge and decreasing nursing facility length of stay. These services can help patients who can return home do so as soon as possible.12
11 Avalere analysis of 2005, 2006, 2007, 2008, and 2009 Medicare Skilled Nursing Facilities Minimum Data Set data.
12 Jette, Diane L., Reg L. Warren and Christopher Wirtalla. “The Relation between Therapy Intensity and Outcomes of Rehabilitation in Skilled Nursing Facilities.” Archives of Physical Medicine and Rehabilitation 86: 373–379, 2005.
Long-Stay Measures Dominate Current Nursing Facility Quality MeasurementThe nursing facility quality measurement system for this increasingly complex population has its roots in the Omnibus Budget Reconciliation Act (OBRA) of 1987. OBRA ’87 overhauled the regulatory framework related to nursing facility quality and mandated the collection of clinical data for every nursing facility patient. The data collection instrument that evolved from this requirement is the Minimum Data Set (MDS), a set of clinically-relevant information that includes: demographics; medical conditions, diagnoses, treatments, and therapies; cognitive, physical, emotional, and social function levels; and medication use. The MDS provides the basis for quality measures collected by the Centers for Medicare & Medicaid Services (CMS); once tested, these measures go through an endorsement process conducted by the National Quality Forum (NQF).
The CMS currently reports nursing facility performance on 21 quality measures that are derived from data within the MDS. Most of the 21 measures are outcome measures, which assess patient status, but there are also process measures, which primarily assess whether certain tests or treatments were performed, such as the administration of an influenza vaccine or use of a catheter. The measures are predominantly focused on long-stay residents; there are six measures for short-stay patients and the remaining fifteen measures are for long-stay residents.
LONG-STAY MEASURES
The long-stay measures assess outcomes in areas such as urinary tract infections, pain, pressure sores, falls, incontinence, and weight loss. The long-stay measure set also includes four process measures and two newly-endorsed patient experience surveys (Table 1).
CHANGE IN SEVERITY OF ILLNESS FOR NURSING FACILITY PATIENTS
FIGURE 1
2005 2006 2007 2008 2009
0
20
40
60
80
100
0
20
40
60
80
100
Major and Extreme Severity
Moderate Severity
Minor Severity
Unknown
Shar
e of
Med
icare
Day
s
Major or Extreme Severity
Moderate Severity
Minor Severity
Unknown
2005 2006 2007 2008 2009
45.4% 49.2% 49.8% 51.2% 52.5%
42.0% 41.5% 40.5% 38.8% 37.1%
10.2% 9.2% 9.0% 8.7% 8.3%
Source: Avalere analysis of the 2005, 2006, 2007, 2008, and 2009 Medicare 100 percent SAF claims data base from CMS for the SNFs and Inpatient Hospitals.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 15
SHORT-STAY MEASURES
In comparison to the long-stay measure set, the short-stay measure set is very limited. Table 2 displays the six NQF-endorsed nursing facility quality measures for short-stay patients.
Current Short-Stay Nursing Facility Quality Measures Lack Comprehensiveness and SophisticationBecause nursing facility quality measures are based on information from the MDS, a tool that was conceived with long-stay patients in mind, there
are relatively few measures that focus on short-stay/PAC patients. More short-stay measures are needed to improve the comprehensiveness of the measure set to ensure that post-acute care patient outcomes are accurately assessed. Additionally, there are weaknesses within the existing long- and short-stay measures that further decrease the reliability of nursing facility quality measurement. This section describes three shortcomings in the existing quality measurement system that researchers have identified as necessary to address in order to improve its accuracy and value.
NURSING FACILITY LONG-STAY QUALITY MEASURES ENDORSED BY NQF
Measure Title Measure Type
Physical Therapy for New Balance Problem Process
Percent of Residents Whose Need for Help with Activities of Daily Living Has Increased Outcome
Percent of Residents Who Were Assessed and Given the Seasonal Influenza Vaccine Process
Percent of Residents Who Were Assessed and Given the Pneumococcal Vaccine Process
Percent of High Risk Residents with Pressure Ulcers Outcome
Percent of Low Risk Residents Who Lose Control of Their Bowel or Bladder Outcome
Percent of Residents Who Have Symptoms of Major Depression Outcome
Percent of Residents with Moderate to Severe Pain Outcome
Percent of Residents Who Have/Had a Catheter Inserted and Left in Their Bladder Process
Percent of Residents Who Lose Too Much Weight Outcome
Percent of Residents Who Were Physically Restrained Outcome
Percent of Residents with a Urinary Tract Infection Outcome
Percent of Residents Experiencing One or More Falls with Major Injury Outcome
Consumer Assessment of Health Providers and Systems (CAHPS®)* Nursing Home Survey: Discharged Resident Instrument
Patient/Family Experience
Consumer Assessment of Health Providers and Systems (CAHPS®) Nursing Home Survey: Family Member Instrument
Patient/Family Experience
* The Consumer Assessment of Healthcare Providers and Systems (CAHPS)® program is an initiative to develop standardized surveys of patient experiences using various health care providers and systems.
Source: National Voluntary Consensus Standards for Nursing Homes: A Consensus Report. The National Quality Forum, 2011.
TABLE 1

2011 A N N UA L QUA L I T Y R EP O R T16
THE COMPARABILITY OF NURSING FACILITY QUALITY MEASURES IS COMPROMISED BY INADEQUATE RISK ADJUSTMENT
Researchers believe that the MDS-based nursing facility quality measures are not adequately risk-adjusted.13, 14 A robust risk adjustment methodology is important to ensure that quality measurement
13 Li, Yue et al. “National Release of the Nursing Home Quality Report Cards: Implications of Statistical Methodology for Risk Adjustment.” Health Services Research 44(1), 2009.
14 Risk adjustment is a statistical process used to identify and adjust for variation in patient outcomes that may be due to differences in patient characteristics, or risk factors, across health care facilities.
reflects differences in patient care rather than differences in patient populations. In other health care settings, such as hospitals, quality measures are adjusted by certain factors to allow for comparison across providers with different types of patients, so as to avoid inadvertently penalizing those that care for sicker patients. The nursing facility quality measures currently reported by CMS are minimally risk adjusted and the adjustment methods used are relatively simple. For example, most nursing facility quality measures are adjusted by excluding certain patients from the denominator of the quality rating, which does not address any characteristics of the remaining patients included in the measure. Studies suggest that improving risk adjustment methodologies for these quality measures would improve their value and validity.15
Many resident characteristics may affect outcomes, and the distribution of these characteristics across facilities is not random and thus can bias quality ratings. The incorporation of more risk factors or additional MDS data could improve the reliability of the quality measures. In one study, researchers applied a variety of risk adjustment methodologies to the publicly reported, MDS-based quality measure that assesses long-stay residents’ decline in the performance of activities of daily living (ADLs).16 The authors noted that this measure was chosen because it is a key component of the well-being of nursing facility residents. As currently reported by CMS, this measure is minimally adjusted using an exclusion method. The study found that regression-based risk adjustment that incorporates a broad set of clinical characteristics had higher validity than the exclusion-based CMS adjustment method. In terms of facility rankings, the
15 Berlowitz, Dan and Margaret Stineman. “Risk Adjustment in Rehabilitation Quality Improvement.” Topics in Stroke Rehabilitation 17(4), 2010.
16 Li, Yue et al. “National Release of the Nursing Home Quality Report Cards: Implications of Statistical Methodology for Risk Adjustment.” Health Services Research 44(1), 2009.
NURSING FACILITY SHORT-STAY QUALITY MEASURES ENDORSED BY NQF
Measure Title Measure Type
Percent of Nursing Home Residents Who Were Assessed and Given the Seasonal Influenza Vaccine
Process
Percent of Residents Who Were Assessed and Given the Pneumococcal Vaccine
Process
Percent of Residents with Moderate to Severe Pain
Outcome
Percent of Residents with Pressure Ulcers that Are New or Have Not Improved
Outcome
The Percentage of Residents on a Scheduled Pain Medication Regimen on Admission Who Report a Decrease in Pain Intensity or Frequency
Outcome
Consumer Assessment of Health Providers and Systems (CAHPS®) Nursing Home Survey: Discharged Resident Instrument
Patient Experience
Source: National Voluntary Consensus Standards for Nursing Homes: A Consensus Report. The National Quality Forum, 2011.
TABLE 2

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 17
exclusion-based adjustment method misclassified some facilities when ranking the top performing ten percent, lowest performing ten percent, and middle eighty percent. These findings are consistent with other studies that point out the inadequacies of current nursing facility quality measure risk adjustment methodologies and potential benefits of more sophisticated risk adjustment methods.17
Due to the considerable variation within the patient populations treated by different facilities, risk adjustment is particularly important when measuring the quality of nursing facility care. Within nursing facilities, there is significant variation in the types of patients who are admitted, which can be related to volume, proximity to hospitals, rural versus urban setting, competencies of nursing and ancillary care staff, and physician involvement. Thus, the patient populations served by different nursing facilities vary dramatically, even within geographic locations. This variation has a significant impact on nursing facility resource utilization, lengths of stay, patient outcomes, and post-discharge destinations.
Inadequate risk adjustment that does not control for varying patient characteristics leads to quality measures that may not be comparable across facilities. An analysis of annual nursing facility survey data and quality measures found that indicators such as patient ADL difficulties and acuity levels were lower among facilities with high ratings on the quality measures.18 That is, facilities whose residents were healthier to begin with scored better on the quality measures, which suggests that the current nursing facility measure risk adjustment methodologies do not incorporate enough clinical factors to allow for fair comparisons of quality across facilities.
17 Ibid.18 Mor, Vincent et al. “Changes in the Quality of Nursing Homes
in the US: A Review and Data Update.” Milbank Quarterly 87(3), 2009.
Going forward, measure development should ensure comparability of patient populations before comparing quality between facilities.
THE CURRENT NURSING FACILITY QUALITY MEASURE SET DOES NOT ADEQUATELY ASSESS IMPROVEMENT IN FUNCTIONALITY
The goal of post-acute care is to help patients achieve or improve upon the level of functioning they had before developing the condition that necessitated the hospital stay. Nursing facilities provide a wide array of therapy services to help achieve this goal, including physical, occupational, and speech therapies. In nursing facilities, speech language pathologists assist with communication, frequently working with stroke patients, while physical therapists assist patients with mobility challenges by improving strength, endurance, and ability to utilize assistive devices. Occupational therapists seek to improve patients’ fine motor skills and ability to complete basic activities, such as bathing and dressing. Ultimately, these therapy modalities are intended to improve patients’ functional status and ideally, to allow them to live independently.
The most commonly used measures of functional status are based on a patient’s ability to complete ADLs such as eating and dressing, as well as instrumental activities of daily living (IADLs) such as using the telephone, shopping, and managing money. The three outcome measures currently reported for short-stay patients, however, do not capture the impact of this therapy on patients’ ability to perform ADLs or IADLs. In addition, none of the measures currently reported indicate whether the patient was discharged to his or her home or other settings.
Quality measures that assess changes in functioning and rehabilitation outcomes are available for use in post-acute care settings and are routinely collected by some PAC providers. As part of the patient

2011 A N N UA L QUA L I T Y R EP O R T18
assessment process, IRFs collect data that form the basis for Functional Independence Measures (FIMs).19 Though nursing facilities are not required to collect or report FIMs data, some do utilize FIMs measures or other functional improvement measures. Some nursing facilities collect these data in order to compare patient outcomes both over time within their own facilities as well as with outcomes data collected in other post-acute settings. However, as the collection of FIMs or other functional improvement measures is not mandatory, functional outcomes data for nursing facilities are limited. Given these limitations, it is not possible to provide meaningful assessments of the value of post-acute care provided within nursing facilities or across PAC settings.
19 FIMs assess several domains of patient characteristics, including mobility, ability to perform activities of daily living, ability to manage care needs, and cognitive function.
THE CURRENT NURSING FACILITY QUALITY MEASURE SET DOES NOT ADEQUATELY ASSESS THE MOST COMMON CONDITIONS
In addition, none of the nursing facility quality measures are designed to gauge the appropriateness and effectiveness of treatment provided for the most common conditions found in short-stay nursing facility patients, including whether the treatment was in accordance with established best practices for the conditions.
The short-stay nursing facility quality measures do not capture the outcomes or processes of care related to these commonly treated conditions, though they do assess the presence of pain and pressure ulcers, conditions that could accompany the diagnoses in Table 3 below. In order to adequately assess outcomes for post-acute care patients, the quality measure set should include measures that assess specific outcomes related to these conditions, including the extent to which they were able to regain functioning and return to their homes.
TOP TEN MOST COMMON HOSPITAL DIAGNOSIS-RELATED GROUPS FOR MEDICARE BENEFICIARIES DISCHARGED TO NURSING FACILITIES, 20091
1. Major Joint Replacement or Reattachment of Lower Extremity without Major Complications
2. Septicemia or Severe Sepsis without Mechanical Ventilation for 96+ Hours with Major Complications
3. Kidney & Urinary Tract Infections without Major Complications
4. Heart Failure & Shock with Major Complications
5. Hip & Femur Procedures Except Major Joint with Complications
6. Simple Pneumonia & Pleurisy with Complications
7. Heart Failure & Shock with Complications
8. Kidney & Urinary Tract Infections with Major Complications
9. Nutritional & Misc. Metabolic Disorders without Major Complications
10. Simple Pneumonia & Pleurisy with Major Complications
Source: Avalere analysis of 2009 Medicare 100 Percent SAF claims data base from CMS for SNFs.
TABLE 3

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 19
The Nursing Facility Quality Measurement System Must Change to Support Medicare Payment ReformsThe urgency of addressing quality measurement shortcomings is increasing as the health care system shifts towards shared responsibility and coordinated, patient-centered care under the Affordable Care Act (ACA) initiatives. The ACA requires CMS to develop and submit a plan for nursing facility value-based purchasing by October 1, 2011. The theory of value-based purchasing is that buyers should hold providers accountable for both cost and quality. Value-based purchasing programs are being applied in the Medicare payment systems for other types of providers, including hospitals and physicians, to encourage the delivery of high quality, cost-effective care. In order to accurately identify and reward nursing facilities that provide high quality care, CMS needs a robust set of quality measures.
Value-based purchasing will not work as intended unless CMS can accurately measure quality across nursing facilities and relate it to the cost of care (see the discussion of risk-adjustment on pages 16 and 17). Other payment reforms, such as bundled payments and accountable care organizations (ACOs), will also create demand for highly evolved measures that can allow for comparison of the quality of care within and across post-acute care providers such as LTACHs, IRFs, and home health agencies (HHAs), as well as nursing facilities.
ACA ENVISIONS A ROBUST QUALITY INFRASTRUCTURE TO SUPPORT PAYMENT AND DELIVERY REFORMS
The ACA envisions a focused and comprehensive quality framework as one of the underpinnings of a number of payment and delivery reforms and
puts in place mechanisms to identify gaps within current measurement systems. To guide agency-wide quality improvement efforts, the ACA mandated that the Department of Health and Human Services (HHS) create a National Quality Strategy. The legislation calls for HHS, in developing the strategy, to emphasize the importance of patient-centered, coordinated care and reaching a consensus on specific measures, data sources, and data collection procedures to be used to encourage better care. Within the National Quality Strategy, HHS must focus on aligning quality measurement activities within value-based purchasing programs.20
In addition to establishing a National Quality Strategy, the ACA prioritizes certain types of quality
20 Department of Health and Human Services. “National Strategy for Quality Improvement in Health Care.” 21 March 2011. Accessed at: http://www.healthcare.gov/center/reports/quality03212011a.html

2011 A N N UA L QUA L I T Y R EP O R T20
measures, such as patient and family experience; resource use; functional status; health information technology; and other measures.21 To identify gaps in the measures currently used by various providers and systems, the ACA assigns new duties to the NQF, including the convening of a multi-stakeholder group tasked with providing input to HHS on the selection of measures for public reporting and payment programs.22
Table 4 displays the nine measure types that are prioritized in the ACA language and the extent to which available nursing facility quality measures reflect these priorities.
THE NURSING FACILITY QUALITY MEASURE FRAMEWORK IS NOT ADEQUATE FOR VALUE-BASED PURCHASING; REFINEMENTS AND ADDITIONS TO THE MEASURE SET ARE NEEDED
The current nursing facility quality measurement system was conceived as a way to address safety concerns regarding poorly performing nursing facilities, rather than a system of quality measurement that could be used to inform purchasing of post-acute care. To accurately measure (and pay for) the value and quality of care provided by nursing facilities, CMS will need to develop and add new measures to the current framework and may need to modify or not use some of the existing measures. The measures in the revised framework must be rigorously tested and risk adjusted to ensure comparability of scores across facilities.
CMS is currently conducting a Nursing Home Value-Based Purchasing (VBP) Demonstration that offers financial incentives to nursing facilities that meet certain thresholds for providing high quality
21 Section 931 of the Affordable Care Act of 2010.22 The National Quality Forum. “Establishment of MAP.” Accessed
at: http://www.qualityforum.org/Setting_Priorities/Partnership/Establishment_of_MAP.aspx
care.23 CMS will assess each participating nursing facility’s quality based on four domains: staffing, appropriate hospitalizations, MDS outcomes, and survey deficiencies; and will create an overall quality score based on performance on each of the domains.24 CMS used MDS-based quality measures in this demonstration, including five long-stay and three short-stay measures. The three short-stay measures assess improvements and declines in functional status, but these measures are not part of the current set of short-stay measures for nursing facilities, nor are they NQF-endorsed. Adding the short-stay measures from the VBP demonstration to the nursing facility quality measurement set could help close some of the gaps in the measurement system, especially regarding the assessment of improvement in function and ability to perform basic activities.
The design of the VBP demonstration for nursing facilities, particularly CMS’ use of measures not currently reported, further emphasizes the need for additional nursing facility quality measures as well as refinements to existing measures. To add to the measure set, CMS could utilize available measures that are not yet endorsed by NQF, make modifications to measures used in other settings, or support the development of new nursing facility measures. For example, the FIMs, which are already being collected in some nursing facilities, could be modified for use with nursing facility patients and added to the measure set. Additionally, the home health sector currently reports data that form the basis of measures related to rehabilitation services provided in the home; these measures could be adapted for use in other settings, such as nursing facilities.
23 Abt Associates. “Nursing Home Value-Based Purchasing Demonstration.” March 2009. Accessed at: http://www.cms.gov/DemoProjectsEvalRpts/downloads/NHP4P_Refinements_Report.pdf
24 Ibid.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 21
THE AFFORDABLE CARE ACT’S PRIORITIES FOR NEW QUALITY MEASURE DEVELOPMENT AND CORRESPONDING NURSING FACILITY MEASURES
Measure Type, as specified by Section 931 of the Affordable Care Act Available Nursing Home Measure
Health outcomes and functional status of patients Standardized MDS-based quality measures assess outcomes, particularly for long-stay patients, but more functional status measures are needed for short-stay patients
Management and coordination of health care across episodes of care and care transitions for patients across the continuum of providers, health care settings, and health plans
No standardized care transition or coordination measures are currently used in nursing facilities
The experience, quality, and use of information provided to and used by patients, caregivers, and authorized representatives to inform decision making about treatment options
No standardized measures related to informed or shared decision making are currently used in nursing facilities
Meaningful use of health information technology No standardized health information technology measures are currently used in nursing facilities
The efficiency of care No standardized efficiency measures are currently used in nursing facilities
The safety, effectiveness, patient-centeredness, appropriateness, and timeliness of care
The newly-endorsed CAHPS® survey instruments for long- and short-stay patients and, in the case of long-stay patients, their families, are being implemented as part of nursing facilities’ federal quality reporting activities. This survey may address some, but not all, of the goals for this measure type
The equity of health services and health disparities across health disparity populations and geographic areas
No standardized health disparity measures are currently used in nursing facilities
Patient experience and satisfaction The CAHPS® survey is meant to assess the patient’s experience
The use of innovative strategies and methodologies No standardized measures assessing innovative strategies are currently used in nursing facilities
Source: Section 931 of the Affordable Care Act, March 2010; Avalere analysis of existing quality measures for use in the SNF setting.
TABLE 4

2011 A N N UA L QUA L I T Y R EP O R T22
NURSING HOME VALUE-BASED PURCHASING DEMONSTRATION QUALITY INDICATORS
Measure Title or Type Measure Description Current Status of Measure Reporting
Staffing Adjusted by case mix, the staffing measures calculate:
■■ Registered nurse (RN) and Director of Nursing (DON) hours per resident day
■■ Certified Nurse Aide (CNA) hours per resident day
■■ Nursing staff turnover (RNs, Licensed Practical Nurse (LPN), CNA)
■■ Licensed staff (RN/DON/LPN) hours per resident day
■■ Nursing facilities are currently assessed on two staffing measures: RN hours per resident day and total staffing hours (RN+ LPN+ nurse aide hours) per resident day
■■ The staff turnover measure is included in the demonstration due to CMS’ belief that staff turnover may be related to increased rates of rehospitalizations
Potentially Avoidable Hospitalizations
Also risk-adjusted, this measure will calculate:
■■ Rate of potentially avoidable hospitalizations per resident day for long-stay residents
■■ Rate of potentially avoidable hospitalizations per stay for short-stay residents
■■ Nursing facilities do not currently report standardized data on potentially avoidable hospitalizations for quality measurement purposes
MDSBased Quality Measures
CMS is collecting the following MDS-based measures:
■■ Measures for long-stay residents:
— Percentage of residents whose need for help with daily activities has increased
— Percentage of residents whose ability to move in and around their room got worse
— Percent of high-risk residents with pressure sores
— Percentage of residents who had a catheter inserted and left in their bladder
— Percentage of residents who were physically restrained
■■ Measures for short-stay residents:
— Percentage of residents with improved level of ADL functioning
— Percentage of residents who improve status on mid-loss ADL functioning
— Percentage of residents with failure to improve bladder incontinence
■■ The long-stay resident measures used in the demonstration represent a subset of the currently reported long-stay quality measures
■■ The same exclusion criteria, minimum required sample thresholds, and risk adjustment methodologies used in the publicly reported long-stay quality measures will be used in this demonstration
■■ However, the short-stay measures used in the demonstration are not part of the current set of NQF-endorsed short-stay measures currently reported to CMS. In its design report for the demonstration, CMS notes that these measures were chosen based on their ability to measure rehabilitation – a key goal of post-acute care
TABLE 5
Source: Abt Associates. “Nursing Home Value-Based Purchasing Demonstration.” March 2009. Accessed at: http://www.cms.gov/DemoProjectsEvalRpts/downloads/NHP4P_Refinements_Report.pdf

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 23
The inclusion of measures related to potentially avoidable rehospitalizations reflects CMS’ increased emphasis on reducing rehospitalizations from all care settings. Researchers found that nursing facility quality of care and staff resources were related to the prevention of hospitalizations and these findings supported the use of rehospitalization rates as a measure of nursing facility quality.25 The topic of rehospitalizations from nursing facilities is discussed in depth in the chapter entitled Focus on Rehabilitation Measures (page 62).
Though there are many potentially relevant measures that CMS could include in its nursing facility value-based purchasing plan, not all quality measures are intended to guide payment decisions. When determining the measures on which to base payment under a value-based purchasing system it is essential to consider the relative utility of all of the measures and include only those measures that most meaningfully assess the processes and outcomes of care.
25 Ibid.
FUTURE REFORMS, SUCH AS BUNDLED PAYMENT, WILL REQUIRE CROSS-SETTING MEASURES FOR POST-ACUTE CARE PATIENTS
Currently, it is not possible to compare the quality or efficiency of care provided across PAC settings, which creates challenges for future ACA initiatives. The Center for Medicare and Medicaid Innovation, created by the ACA, is recruiting participants for a demonstration project that will test a variety of bundled payment models, some of which include PAC services. Under the bundled payment model, a single payment is made to an entity (the holder of the bundle) for all services provided to a patient during a specific time period or for a discrete episode of care. The entity controlling the bundle will want to compare quality information across the PAC settings to which patients could be referred, as part of the process of determining the most appropriate site of care.
These comparisons are currently not possible across PAC settings. A key reason for the lack of comparability is the fact that each post-acute care setting is required to collect different data on patients and care provided. CMS could address this
Measure Title or Type Measure Description Current Status of Measure Reporting
Survey Deficiencies
Survey deficiencies within state surveyor data will be used in two ways:
■■ To disqualify any nursing home that, in the demonstration year, received a citation for substandard quality of care or that had one or more citations for actual harm or higher in certain regulatory groups
■■ Individual citations, both related to health and life safety, will be assigned values according to their scope and severity
■■ Nursing facilities are currently assessed on state surveyor data, but overall scores are determined slightly differently for purposes of the demonstration
TABLE 5
NURSING HOME VALUE-BASED PURCHASING DEMONSTRATION QUALITY INDICATORS (CONT.)

2011 A N N UA L QUA L I T Y R EP O R T24
obstacle by mandating use of a standardized patient assessment tool. One such tool is the Continuity of Assessment Record and Evaluation (CARE) tool, which is intended to facilitate the collection of standardized information on patient outcomes and costs across post-acute care settings. The CMS demonstration testing the CARE tool is slated to end this year.26
IRFs and LTACHs do not yet report data on standardized quality measures (i.e., even on measures limited to those settings). They are required under the ACA to report on CMS-designated quality measures beginning in fiscal year 2014.27 Within the recently released fiscal year (FY) 2012 final rules, CMS set out guidelines for the development of these quality measurement systems, which utilize some of the measures currently reported by hospitals and nursing facilities.
26 RTI International. “Overview of the Medicare Post Acute Care Payment Reform Initiative.” Accessed at: http://www.cms.gov/DemoProjectsEvalRpts/downloads/PACPR_RTI_CMS_PAC_PRD_Overview.pdf
27 Section 3004 of the Affordable Care Act of 2010.
A new model of care delivery and payment, the ACO will increase demand for quality information. In the ACO model, nursing facilities may enter in agreements with other provider systems to coordinate care for patients across the health care system.28 The potential cost-savings achieved due to this increased efficiency and quality of care will be shared between purchaser (Medicare) and provider organization (ACO). To achieve savings, ACOs will need sophisticated quality information and will want to identify the most cost-effective site of care to treat a particular patient.
The implementation of these delivery and payment reforms, and the corresponding demand from the participating entities for quality information across PAC settings, should increase the sense of urgency in developing uniform PAC measures. In the post-acute care continuum, the quality measurement infrastructure must be strong yet able to adapt to value-based purchasing, bundled
28 Cirillo, Anthony. “Nursing homes’ new mission: Fitting into accountable care organizations.” McKnight’s Long-Term Care News and Assisted Living. November 3, 2010.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 25
payments and shared savings arrangements. Though much uncertainty remains around how these new delivery and payment systems will be implemented, it is clear that the success of these systems is dependent on participants’ ability to access comprehensive and accurate information around quality.
ConclusionNursing facilities serve two distinct and changing patient populations, long-stay residents and post-acute care patients. While there are concerns about the risk adjustment applied to the full set of nursing facility quality measures, especially in light of the increasing severity of illness in nursing facility patients, a more pressing concern is the lack of measures available to assess post-acute care. The six NQF-endorsed post-acute care measures for nursing facilities provide an incomplete picture of care. For example, there are no measures that assess the effectiveness of the treatments for the most common conditions found in PAC patients. Perhaps most problematic is the fact that while the major goal of post-acute care is to assist patients in regaining function, and the vast majority of post-acute care treatment plans include rehabilitation services, none of the current nursing facility PAC measures assesses improvement or decline in function (e.g., ability to perform ADLs and/or IADLs) over time.
Realizing the potential of the payment reforms in the Affordable Care Act – value-based purchasing, bundling, and ACOs – will require a set of PAC-focused, cross-setting, and adequately risk-adjusted quality measures. These measures will allow purchasers to accurately assess the quality and efficiency of care and make purchasing decisions accordingly. This will in turn require development of new measures, and modification or deletion of others,
to build a new measurement framework that can serve as one of the building blocks of an improved PAC payment and service delivery system.
Policymakers should consider potential improvements to the nursing facility quality measurement system. These could include:
■■ Developing and endorsing more measures related to the care provided to short-stay nursing facility patients, particularly measures that assess functional improvement
■■ Refining and strengthening the risk adjustment methodologies currently applied to the nursing facility measure set
■■ Developing new measures, or revising current measures, to be used across post-acute care settings

2011 A N N UA L QUA L I T Y R EP O R T26
Quality Trends: BY THE NUMBERS
Since 2009, nursing facilities
have made measureable
improvements in nine out of 10
Quality Measures.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 27
Quality Trends: BY THE NUMBERS
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the NumbersCenters for Medicare and Medicaid Services data compiled by American Health Care Association, Research Department, My InnerView
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix

2011 A N N UA L QUA L I T Y R EP O R T28
America’s skilled nursing and rehabilitation
facilities collect data to regularly measure
the quality of care available in individual
nursing facilities. These data are widely
utilized by consumers when exploring options
for themselves, or their family, in choosing a
nursing facility. The key areas of quality currently
measured, based on the latest research in
nursing care, are reviewed and updated on a
routine basis. For the provider community, these
standard measurements allow facilities to track,
assess, and evaluate the effectiveness of quality
improvement programs.
Historically, the Centers for Medicare and
Medicaid Services (CMS) has tracked and
released quality data. These data are grouped
into two sets known as Quality Indicators (QI)
and Quality Measures (QM). The QIs and QMs
used in this section of the report illustrate
where quality has improved, and where further
improvements are needed. QIs and QMs are
publicly available at the state and national
levels. Only QMs are publicly available at the
facility level.
BOX 1
Quality Trends: BY THE NUMBERS
HOW CHANGES TO MDS IMPACT THE DATA
On October 1, 2010, CMS required that all nursing facilities
implement a new MDS system known as MDS 3.0. Prior
to this implementation, facilities employed the previous
MDS 2.0 system. CMS mandated this transition based on
long term care (LTC) provider concerns that MDS 2.0 failed
to capture information collected directly from patients and
other clinical details. The updated assessment tool was
designed to improve the ability of nursing facilities, and CMS,
to measure care quality and evaluate facility performance.
MDS 3.0 allows for enhanced accuracy and improves system
credibility through more reliable data.
The implementation of MDS 3.0 has caused a delay of
the publicly available QI and QM data until April 2012.
In previous Quality Reports, quality trends were reported
using QI and QM data collected in the fourth quarter of each
year from the CMS Nursing Home Compare database. Due
to the interruption in available data, this chapter will show
results from the third quarter data of each year, as this is the
latest information available from CMS.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 29
CMS produces a Quality Indicator Report on a quarterly basis that summarizes 34 indicators found within the Minimum Data Set (MDS). The MDS is completed by nursing facility staff, and are used to collect information about resident and patient clinical assessments on functionality, psychosocial and health status. CMS aggregates the data collected through the MDS process to create facility-specific and state-level reports.
QIs help facility staff identify potential patient complications or problems that may require additional attention. Additionally, the QI Report can be used by facilities to review trends, compare its performance to facilities across the state, and identify areas for improvement. QIs are also used by state survey agencies to determine survey and quality monitoring efforts.
In addition, CMS uses the MDS instrument to generate Quality Measure (QM) reports, which are also used to evaluate aspects of care on a facility-by-facility basis. Facilities are assigned a score for each QM calculated by the proportion of the number of eligible residents in a facility with a specific condition versus the sum of total residents in the facility. QMs, updated quarterly by CMS, are also used by facilities to identify areas for quality improvement.
QM data is available at www.medicare.gov and QI data is available at www.cms.gov
CMS NURSING FACILITY AVERAGE QUALITY MEASURE SCORES FOR THE U.S.
Nursing Facility Average Quality Measures 2009 2010 *DifferencePercentage
Improvement
LONGSTAY
Activities of Daily Living (ADL) 14.3% 13.9% 0.4% 2.8%
Pain 3.4% 3.2% 0.2% 5.9%
High-Risk Pressure Ulcer 10.9% 10.3% 0.6% 5.5%
Indwelling Catheter 5.1% 4.8% 0.3% 5.9%
Mobility 10.9% 10.7% 0.2% 1.8%
Urinary Tract Infection (UTI) 9.1% 9.0% 0.1% 1.1%
Physical Restraint 3.1% 3.3% 0.2% -6.5%
SHORTSTAY
Delirium 1.4% 1.2% 0.2% 14.3%
Pain 19.4% 19.1% 0.3% 1.6%
Pressure Ulcer 12.9% 11.8% 1.1% 8.5%
Source: CMS Nursing Come Compare (3rd Quarter each year) American Health Care Association, Research Department.
TABLE 1

2011 A N N UA L QUA L I T Y R EP O R T30
NURSING FACILITY MDS QUALITY INDICATORS
Nursing Facility MDS Quality Indicators 2000 2010
Point Difference 2000–2010
ACCIDENTS
Incidence of new fractures 1.5% 1.4% -0.1%
Prevalence of falls 14.8% 13.0% -1.8%
BEHAVIOR/EMOTIONAL/COGNITIVE PATTERNS
Residents who have become more anxious or depressed 14.2% 14.9% 0.7%
Prevalence of behavioral symptoms affecting others 26.0% 16.6% -9.4%
Prevalence of symptoms of depression with anti-depressant therapy 7.2% 4.5% -2.7%
Incidence of cognitive impairment 10.8% 12.5% 1.7%
CLINICAL MANAGEMENT
Use of nine or more different medications 41.8% 71.3% 29.5%
INCONTINENCE CARE
Low-risk residents who lost control of their bowels or bladder 42.1% 51.0% 8.9%
Residents who have/had a catheter inserted and left in their bladder 7.7% 7.0% -0.7%
Prevalence of occassional or frequent bladder or bowel incontinence without a toileting plan
42.6% 52.3% 9.7%
Prevalence of fecal impaction 0.4% 0.0% -0.4%
INFECTION CONTROL
Residents with a urinary tract infection 8.3% 9.7% 1.4%
NUTRITION/EATING
Residents who lose too much weight 11.9% 8.6% -3.3%
Prevalence of tube feeding 7.0% 6.4% -0.6%
Prevalence of dehydration 1.1% 0.1% -1.0%
PAIN MANAGEMENT
Residents who have moderate to severe pain* 10.3% 7.5% -2.8%
PHYSICAL FUNCTIONING
Residents whose need for help with daily activities has increased 15.4% 14.6% -0.8%
Residents who spend most of their time in a bed or in a chair 6.8% 4.6% -2.2%
Residents whose ability to move in and around their rooms got worse* 16.6% 14.6% -2.0%
Incidence of decline in range of motion 8.9% 6.6% -2.3%
PSYCHOTROPIC DRUG USE
Prevalence of antipsychotic use, in the absence of psychotic conditions 16.3% 18.5% 2.2%
Prevalence of antianxiety/hypnotic drug use 17.3% 23.4% 6.1%
Prevalence of hypnotic use more than two times in the last week 3.9% 5.5% 1.6%
QUALITY OF LIFE
Residents who were physically restrained 9.1% 2.6% -6.5%
Prevalence of little or no activity 19.9% 5.3% -14.6%
SKIN CARE
Pressure ulcers 9.2% 11.9% 2.7%
*Initial data point is from 2005Source: CMS, MDS National Quality Indicator System, 3rd Quarters of Each Year.
TABLE 2

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 31
RESIDENTS WHO LOSE TOO MUCH WEIGHT
Source: CMS, MDS National Quality Indicator System, 3rd Quarters of Each Year.
RESIDENTS WHO WERE PHYSICALLY RESTRAINED
Source: CMS, MDS National Quality Indicator System, 3rd Quarters of Each Year.
PREVALENCE OF LITTLE OR NO ACTIVITY
Source: CMS, MDS National Quality Indicator System, 3rd Quarters of Each Year.
PREVALENCE OF DEHYDRATION
Source: CMS, MDS National Quality Indicator System, 3rd Quarters of Each Year
RESIDENTS WHO HAVE MODERATE TO SEVERE PAIN
Source: CMS, MDS National Quality Indicator System, 3rd Quarters of Each Year.
FIGURE 1
FIGURE 4
FIGURE 2 FIGURE 3
FIGURE 5
0
2
4
6
8
10
12
2000 20100
2
4
6
8
10
2000 2010
0
5
10
15
20
2000 2010
0.0
0.2
0.4
0.6
0.8
1.0
1.2
2000 2010
0
2
4
6
8
10
12
2000 2010
QUALITY INDICATOR TRENDS

2011 A N N UA L QUA L I T Y R EP O R T32
NURSING FACILITY SURVEY PERFORMANCE
Federal law requires that every Medicare and Medicaid certified nursing facility in America is surveyed at least once every 15 calendar months. Surveys are completed by state surveyors that are contracted by CMS to inspect and assess how well a facility is meeting federal regulations, which facilities must comply with in order to take part in the Medicare and Medicaid programs. These regulations address many aspects of the nursing facility, including quality of patient care, quality of life, physical plant and safety. If a facility fails to meet a particular regulation, a surveyor will assign that facility a citation. Additionally, facilities can be cited for “substandard quality of care” if the surveyor finds
that failure to meet a particular regulation directly jeopardizes patient safety.
Since 2000, the percentage of facilities cited with a substandard quality of care designation has dropped by 1.7 percent, while the average number of citations has increased slightly. However, since 2009, nursing facility health survey citations have been on a steady decline and have dropped nearly a full percentage point in two years.
All survey data is publicly available in CMS’s Certification and Survey Provider Enhanced Reporting (CASPER) system, previously known as Online Survey, Certification, and Reporting System (OSCAR).
AVERAGE NUMBER OF STANDARD HEALTH SURVEY CITATIONS AND PERCENT OF FACILITIES CITED FOR SUBSTANDARD QUALITY OF CARE (SQC): 2000–2011
FIGURE 6
012345678 SQC
Avg Cit
0
1
2
3
4
5
6
7
8
Num
ber o
f Cita
tions
Average Citations
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
SQC Cited Facilities
0
6%
5%
4%
3%
2%
1%
Facil
ities
Source: Computed by the American Health Care Association, Research Department using CMS Facility CASPER Standard Health Survey Data, March of each year.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 33
Consumer and Workforce Satisfaction Compiled directly from the 2010 National Survey of Consumer and Workforce Satisfaction in Skilled Nursing and Rehabilitation Facilities.
Contributions to this report were made by the following members of My InnerView‘s research team: Eric Lewerenz, M.S., Katherine Gechter, MPH and Joe Johnson.
My InnerView is an applied research company that has been researching, measuring and reporting on consumer and workforce satisfaction in nursing and rehabilitation facilities since 2005. This multi-year series of national reports helps foster greater accountability in the use of public and private resources for long-term and rehabilitative care services. It also provides greater transparency, which helps consumers make informed decisions when seeking skilled nursing care.
The information presented in Figures 7–12 is from the sixth annual report published by My InnerView and represents the most comprehensive summary ever taken of skilled nursing facility consumers and staff in the United States. Encompassing 589,100 in 5,466 skilled nursing and rehabilitation facilities nationwide, the 2010 report is the largest national database of the opinions of 90,576 residents, 140,828 family members and 257,676 facility employees.

2011 A N N UA L QUA L I T Y R EP O R T34
CONSUMERS: RECOMMENDATION TO OTHERS
RESIDENTS: RECOMMENDATION TO OTHERS
NURSES: RECOMMENDATION FOR JOB
FAMILIES: RECOMMENDATION TO OTHERS
WORKPLACE: RECOMMENDATION FOR JOB
NURSING ASSISTANTS (CNAs): RECOMMENDATION FOR JOB
FIGURE 7
FIGURE 9
FIGURE 11
FIGURE 8
FIGURE 10
FIGURE 12
CUSTOMER AND WORKFORCE SATISFACTION
Satisfaction rates for each category represent the combined percentages for “excellent” and “good” scores.
2005 2006 2007 2008 2009 2010
908886848280
Perc
ent
2005 2006 2007 2008 2009 2010
Perc
ent
908886848280
2005 2006 2007 2008 2009 2010
Perc
ent
706866646260
2005 2006 2007 2008 2009 2010
Perc
ent
908886848280
2005 2006 2007 2008 2009 2010
Perc
ent
706866646260
2005 2006 2007 2008 2009 2010
Perc
ent
686664626058
Source: The 2010 National Survey of Consumer and Workforce Satisfaction in Nursing Homes conducted by My InnerView.
Source: The 2010 National Survey of Consumer and Workforce Satisfaction in Nursing Homes conducted by My InnerView.
Source: The 2010 National Survey of Consumer and Workforce Satisfaction in Nursing Homes conducted by My InnerView.
Source: The 2010 National Survey of Consumer and Workforce Satisfaction in Nursing Homes conducted by My InnerView.
Source: The 2010 National Survey of Consumer and Workforce Satisfaction in Nursing Homes conducted by My InnerView.
Source: The 2010 National Survey of Consumer and Workforce Satisfaction in Nursing Homes conducted by My InnerView.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 35
IMPROVEMENTS IN CONSUMER AND WORKFORCE SATISFACTION
Overall, the number of consumers, both residents and family members, who would recommend a skilled nursing or rehabilitation facility remains high at 87 percent, five percentage points higher than 2005. The measure of “willingness to recommend” is especially important because it relates to loyalty which is a very robust indicator of customer’s perception of quality. Resident satisfaction continues to be stable at 88 percent, six percentage points higher than 2005. The steady increases in satisfaction since 2005 are evidence that more providers are implementing practices recommended by national quality-improvement initiatives and using this data to measure progress.
Total workforce satisfaction has also increased since My InnerView first completed this research in 2005. While satisfaction among nurses and nursing assistants is lower than the satisfaction of all job categories, the rates for both nurses and nursing assistants has been on an upward trend since 2005.
Workforce and consumer satisfaction are positively correlated. Facilities with higher workforce satisfaction also have higher family and resident satisfaction. An effective strategy for quality improvement must include a sustained focus on staff skills, commitment and satisfaction, particularly those staff that directly care for residents and communicate with family members.

2011 A N N UA L QUA L I T Y R EP O R T36
More than 7000 nursing
facilities nationwide are
participating the Advancing
Excellence, a partnership
that has proven to improve
performance.
SPECIAL UPDATE: Advancing Excellence IN AMERICA’S NURSING HOMES

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 37
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Mary Jane Koren, MD, MPH
Hospitalization of Nursing Home Residents
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix
SPECIAL UPDATE: Advancing Excellence IN AMERICA’S NURSING HOMES

2011 A N N UA L QUA L I T Y R EP O R T38
A Public-Private Partnership that Works
The Advancing Excellence in America’s Nursing
Homes campaign was launched in 2006 and is
still going strong. It is a dynamic public/private
partnership that has improved performance and
established a rich learning community across
the country. The purpose of the Campaign is to
help nursing homes improve their performance
in eight measures of clinical and organizational
quality through a process of quality improvement
and with the help of free educational resources.
Thirty stakeholder organizations (Box 1) are
united in this initiative to improve the quality
performance of nursing homes across the
country. These organizations represent service
providers, long-term care (LTC) professionals,
staff, consumers, culture change leaders, and
many other organizations whose missions focus
on high performance in the field. The Campaign
is a voluntary learning collaborative. Participation
and access to practical resources and tools to
lead quality improvement are free of charge.
The goals of the Campaign focus on staff turnover, consistent assignment, restraints, pressure ulcers, pain, advance care planning, customer and staff satisfaction. These goals were chosen because they are included in one or more of the national quality initiatives in LTC. By selecting these goals the Campaign aligns its considerable educational resources and state
infrastructure to drive improved performance in these key areas.
Today more than 7000, or 47 percent, of all nursing homes nationwide are participating in the Campaign. Participating nursing homes must commit to, and set individual performance targets
SPECIAL UPDATE:
Advancing Excellence IN AMERICA’S NURSING HOMES

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 39
for, at least three Campaign goals. For each of the goals the Campaign has established a performance target to ensure that achievement is both meaningful and measurable. The goals with the highest number participants are pain, pressure ulcers, and customer satisfaction assessment. The intense focus on these goals is a testament to the willingness within the field to voluntarily undertake work on improving performance (Table 1).
Local Area Networks of Excellence (LANEs)LANEs are one of the powerful features of the Campaign. LANEs are the central organizations that provide direct state support to participants in achieving their clinical and organizational goals. The LANEs are catalysts for nursing home improvement and the “go to” networks for new ideas and approaches. Just like the Steering Committee at the national level, LANEs too are comprised of the wide array of stakeholder groups from nursing home associations to survey agencies and ombudsmen, to quality improvement organizations, and consumer advocacy groups, and LTC professionals. The principal purpose of the LANEs is to provide easily accessible education and training to increase performance. LANEs also provide a regular forum for networking amongst the stakeholder groups that promotes even more opportunities. In addition, the network of state LANEs is a source for sharing success that can be replicated by their counterparts. Partnerships among stakeholders within the LANEs continue to grow. Currently 50 states and the District of Columbia have established a framework for stakeholder coalitions. Many LANEs have been working for four-plus years, and have become formidable change agents within their states.
ADVANCING EXCELLENCE BOARD MEMBERS■■ Administration on Aging
■■ Agency for Healthcare Research and Quality
■■ Alliance for Quality Nursing Home Care
■■ Alzheimer’s Association
■■ American Academy of Nursing – Expert Panel on Aging
■■ American Association for Long Term Care Nursing
■■ American Association of Nurse Assessment Coordinators
■■ American College of Health Care Administrators
■■ American Health Care Association
■■ American Health Quality Association
■■ American Medical Directors Association
■■ Association of Health Facility Survey Agencies
■■ Centers for Disease Control and Prevention
■■ Centers for Medicare & Medicaid Services and its contractors, the Quality Improvement Organizations (QIOs) and State Survey Agencies
■■ Department of Veterans Affairs
■■ Foundation of the National Association of Long Term Care Administrator Boards
■■ Gerontological Advanced Practice Nurses Association
■■ Institute for Healthcare Improvement
■■ LeadingAge – formerly the American Association of Homes and Services for the Aging
■■ National Association of Directors of Nursing Administration in Long Term Care
■■ National Association of Health Care Assistants
■■ National Association of State Long-Term Care Ombudsman Programs
■■ National Gerontological Nursing Association
■■ NCCNHR – The National Consumer Voice for Quality Long-Term Care
■■ Paraprofessional Healthcare Institute
■■ Pioneer Network
■■ Service Employees International Union
■■ The Commonwealth Fund
■■ The Evangelical Lutheran Good Samaritan Society
■■ The John A. Hartford Foundation’s Institute for Geriatric Nursing
BOX 1

2011 A N N UA L QUA L I T Y R EP O R T40
PHASE I: 2006–2008
The initial Campaign was a two-year effort that focused on four clinical outcomes (high-risk pressure ulcers, physical restraints, pain in the long-stay resident and pain in the acute or short-stay resident) and four organizational goals (target-setting, staff turnover, consistent assignment and resident/family satisfaction). The Campaign developed free, evidence-based, user-friendly toolkits with a variety of complementary materials for nursing home leaders and staff, as well as consumers. The Campaign also sponsored webinars and videos on the eight goals and archived the material for nursing home use on the Campaign’s website. The Campaign website was central to the Campaign and
served as the registration vehicle and library for all Campaign materials. Response to the Campaign and its technical assistance materials was overwhelming – on one Thursday afternoon, there were more than 1,800 nursing homes listening to a webinar on how to prevent and heal pressure ulcers! Almost 50 percent of all nursing homes in the nation participated in Phase 1 of the Campaign.
The results from Phase 1 included:
■■ Nursing homes that joined the Campaign improved faster than non-participants in all things measured.
ADVANCING EXCELLENCE GOALS AND PERFORMANCE TARGETS
Goal
Number of Providers Selecting
this Goal Performance Target
Staff Turnover 2,901 The average annual turnover rates for participating nursing homes will be at or below 65% for registered nurses, 35% for licensed practice nurses, and 65% for certified nursing assistants.
Consistent Assignment 2,020 50% of participants selecting this goal will have adopted CNA consistent assignments for residents.
Restraints 2,255 The national average of daily use of physical restraints will be <2%.
Pressure Ulcers 4,798 The national average for high risk pressure ulcers will be at or below 9%.
Pain 4,985 The national average of moderate or severe pain experienced by long-stay residents will be at or below 2%. The national average of moderate or severe pain experienced by post-acute residents will be at or below 16%.
Advance Care Planning 1,715 75% of the nursing homes choosing this goal will have discussions with newly admitted or re-admitted residents on their preferences for advance care planning.
Customer Satisfaction 3,833 85% or more of nursing homes will regularly assess resident satisfaction and incorporate the results to improve performance.
Staff Satisfaction 2,588 The national average of nursing homes that regularly assess staff satisfaction and incorporate the results into their quality improvement activities will exceed 75%.
TABLE 1

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 41
■■ Nursing homes that joined the Campaign and selected specific goals to work on improved faster for those goals than non-participants.
■■ Nursing homes that joined the Campaign, selected specific goals to work on, and set a target for those goals, improved even faster for those goals than non-participants and participants that selected other goals.
PHASE 2: 2009–2011
The successes and momentum of Phase I led to Phase 2, which extended the Campaign. In Phase 2, a new goal was added which focuses on advance care planning. This goal speaks to the importance of reaching out to residents, and their families, during their stay. Making sure the resident’s voice is heard and used to individualize the plan of care goes to the very heart of person-centered care, a philosophy which is fundamental to the Campaign. To further support improved quality performance the website was upgraded so that participants are required to benchmark and set improvement targets for each
LANEs PARTICIPATION IN ADVANCING EXCELLENCE CAMPAIGN
FIGURE 1
More than 50% nursing home participation
Accelerating LANE performance states
100% nursing home participation

2011 A N N UA L QUA L I T Y R EP O R T42
of the goals they selected. This reinforces the importance of measurement in process improvement methodology.
Phase 2 required re-enrollment for nursing homes to continue their participation. This could have been an obstacle, but instead 5,000 nursing homes re-enrolled within 3 months. Four states – Arkansas,
Georgia, Rhode Island and South Dakota – recruited 100 percent of the nursing homes in their state (Figure 1).
The major and most exciting change from Phase 1 to Phase 2 of the Campaign is the shift from a focus of recruitment to one of action and performance. The LANEs are catalysts driving a series of improved performance projects. Fifteen states are working on statewide quality improvement projects which include decreasing the incidence of pressure ulcers and restraints, improving staff stability, and increasing the use of consistent assignment. Results of the projects will be shared with the LANE community so that others can use these tactics to improve their own performance results.
Figure 2 shows the relative improvement in national quality measures from September 2006 through September 2010. No quality measures data is available beyond this point because of the transition phase to the MDS 3.0. This data will be released in the spring of 2012.
CHANGE AND RELATIVE IMPROVEMENT IN NATIONAL QMs: Q3 2006 TO Q3 2010
FIGURE 2
Q3 2006
Q3 2010Restraints Pressure
UlcersChronic
Care PainAcute
Care Pain
0%
5%
10%
15%
20%
25%
-58%
-18%
-37%
-12%

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 43
Another project underway in Phase 2 is the Critical Access Nursing Homes Pilot. This pilot is designed to assess if the collaborative education model of the Campaign can help to reduce the disparities in care experienced by residents living in inner city, resource-challenged nursing homes. Four LANEs are participating in the pilot which concludes later this year. Early results show that improvement is occurring.
THE FUTURE
In 2011, the 30 members of the national coalition for Advancing Excellence moved forward to found a new non-profit organization, the “Advancing Excellence in America’s LTC Collaborative.” The Collaborative’s mission will certainly resonate with consumers and providers alike that, “Each individual receiving long term care supports and services achieves
the highest practicable level of physical, mental, and psychosocial well-being.” The Collaborative’s Board has developed a strategic plan to enhance the momentum and the results of the Campaign. The plan focuses on:
■■ the use of measureable indicators for quality of care and quality of life for individuals receiving long-term care supports and services;
■■ the enrichment of the LANEs; and
■■ the inclusiveness and sustainability of the Collaborative.
In conclusion, the Advancing Excellence in America’s Nursing Homes is alive and well. With almost half of the nation’s nursing homes enrolled, the Campaign is an active partner working with others to advance the quality agenda.

2011 A N N UA L QUA L I T Y R EP O R T44
Nursing home operators can
see reducing readmissions
as an opportunity to bring
creative solutions to the
table and increase their value.
Hospitalization OF NURSING HOME RESIDENTS

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 45
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Andrew Kramer, MD, CEO, Providigm LLC Professor of Medicine, University of Colorado
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix
Hospitalization OF NURSING HOME RESIDENTS

2011 A N N UA L QUA L I T Y R EP O R T46
One of today’s leading topics in discussions of
health care quality is admission to acute care
hospitals. Skilled Nursing Facilities (SNFs), which
admit post-acute patients with multiple comorbid
diseases and functional impairments, have unique
challenges that differ from managing traditional
hospital discharges to home. Additionally,
increasingly frail chronic nursing home residents
also have substantial risk of hospitalization. In
nursing homes, providing services to prevent
or treat acute illness and avoid hospitalization
has always been one of many competing quality
concerns, but not until recently did this become a
leading policy issue.
This chapter begins with a discussion of the current
policy imperatives related to hospital readmission
and their implications for nursing homes. The current
focus on readmissions among hospital discharges
has made this a major issue for SNFs. In addition,
nursing home value-based purchasing is designed to
incentivize nursing homes to reduce readmission to
hospitals for not only post-acute patients, but also
to reduce hospitalization among chronic long-stay
nursing home residents.
One challenge facing nursing homes involves the
development and use of valid measures to track
hospitalization rates, and to compare rates between
facilities and over time. Essential measurement issues
are identifying hospitalizations that are potentially
avoidable, and adequately adjusting for differences
in risk of readmission for the varied population of
nursing home residents. From both a policy and
practice perspective, these are critical.
The chapter concludes with a discussion of evidence-
based approaches to reduce admissions to hospital
that have been developed specifically for the nursing
home sector. Given both the residents that nursing
homes treat and the resources they have and do not
have available, strategies that target specific types of
residents and those that take a more global approach
are considered. In both policy and practice, solutions
for nursing homes must be tailored to the unique
problems and needs of the sector.
Hospitalization OF NURSING HOME RESIDENTS

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 47
Public Policy: The Driving ForceConcerns about hospital readmission of Medicare patients were a predictable consequence of the Hospital Prospective Payment System (PPS) enacted in the early 1980s. As hospital stays were shortened in order to reduce acute care costs, patients were discharged “sicker and quicker” to various post-acute settings. Nursing homes providing Medicare SNF care responded by admitting and treating these more medically complex patients; changes that were already evident by 1986.1
Because of continued pressures to contain hospital costs, the trend of shortening hospital lengths of stay continued, and the role of nursing homes in providing post-acute care grew. Between 1993 and 2006, hospital length of stay for Medicare heart failure patients had a relative decrease of over 25 percent, associated with a relative increase in SNF discharges of 53 percent (Table 1).2 Over this 14-year period, 30-day hospital readmissions had a relative increase of 16 percent.
Thus, declining acute hospital stays resulted in a substantial increase in the use of SNFs for post-hospital care. Nevertheless, readmissions to the hospital increased, suggesting that some patients were discharged from the acute hospital before they were
1 Shaughnessy, P.W., and A.M. Kramer. “The Increased Needs of Patients in Nursing Homes and Patients Receiving Home Health Care.” New England Journal of Medicine 322:21–27, Jan 1990.
2 Bueno et al. “Trends in Length of Stay and Short-term Outcomes Among Medicare Patients Hospitalized for Heart Failure.” JAMA 303(21):2141–2147, 2010.
stable enough for post-acute care, at least the post-acute care available in 2006. While mortality in 30 days decreased over this same period, that decrease was particularly pronounced in the acute care hospital probably due to improved treatments. Reducing these rising readmissions for heart failure, for example, is the aim of current the current policy.
The heart failure findings are consistent with trends for all Medicare patients. For all conditions, the hospital readmission rate within 60 days for Medicare discharges increased from 23 percent to 31 percent, over the 26-year period between 1976–78 and 2003–04.3 This represents about a 25 percent relative increase in readmissions over this 27-year period.
3 Jencks, Stephen F., Mark V. Williams and Eric A. Coleman. “Rehospitalizations Among Patients in the Medicare Fee-for-Service Program.” New England Journal of Medicine 360:1418–1428, April 2009.
DECREASING LENGTH OF ACUTE HOSPITAL LENGTH OF STAY IS ASSOCIATED WITH AN INCREASE IN SNF DISCHARGES AND AN INCREASE IN READMISSION RATE FOR HEART FAILURE
Year
1993–94 2005–06 %Change
Hospital Length of Stay (days)
8.6 6.4 -25.5%
SNF Discharges (%) 13.0 19.9 +53.1%
30-day Readmission Rate (%)
17.3 20.1 +16.1%
30-day Mortality (%) 12.8 10.7 -16.4%
Source: Trends in Length of Stay and Short-term Outcomes Among Medicare Patients Hospitalized for Heart Failure, 1993-2006. Héctor Bueno, Joseph S. Ross, Yun Wang, Jersey Chen, María T. Vidán, Sharon-Lise T. Normand, Jeptha P. Curtis, Elizabeth E. Drye, Judith H. Lichtman, Patricia S. Keenan, Mikhail Kosiborod, Harlan M. Krumholz. JAMA 303(21): 2141–2147, 2010.
TABLE 1

2011 A N N UA L QUA L I T Y R EP O R T48
Not surprisingly, rising readmission rates shifted the policy focus from reducing hospital lengths of stay to reducing readmissions to hospital. Public reporting on the Hospital Compare website started reporting readmissions to hospital for heart failure, pneumonia, and acute myocardial infarction discharges along with the hospital mortality rates for these conditions that had been previously reported.4
As required by the Patient Protection and Affordable Care Act (ACA) this will result in monetary penalties for hospitals with higher than expected readmission rates for specific discharge diagnoses. Beginning in 2012, hospitals with the worst performance on readmission of hospital discharges for the above three conditions will face a reduction in total Medicare reimbursement. In 2015, the reductions will be more significant and other conditions will be added, including chronic obstructive pulmonary disease and several cardiovascular surgical procedures and vascular conditions.
While the focus of the ACA is hospitals, and to some extent physicians who manage patients during and after the hospital stay, 50 percent of the patients receiving post-acute care in 2008 were admitted to SNFs.5 In addition, pneumonia and heart failure were two of the most prevalent admitting diagnoses to SNFs, representing 3.6 percent and 4 percent, respectively, of SNF admissions in 2008. With the rising rate of hospital discharges to SNFs and the increasing complexity of SNF admissions, readmissions to hospital from nursing homes is a major issue for hospitals. The result is that preventing hospital readmissions is becoming a major focus of nursing home performance efforts.
4 www.hospitalcompare.hhs.gov/hospital-search.aspx5 American Health Care Association and Alliance for Quality
Nursing Home Care. 2010 Annual Quality Report.
Increasing this emphasis is the Value-Based Purchasing Demonstration for Nursing Homes that is also aimed at reducing readmissions to hospital. In this demonstration, the most heavily weighted performance measures are rates of readmission for short-stay admissions to nursing homes, and hospital admission rates for long-stay nursing home residents. In fact, the cost savings that will be gained by reducing admission to hospitals are the proposed source for the incentive pool that will be used to pay for improved nursing home performance.
These pressures on nursing homes to reduce hospitalization have always been present in Medicare-risk managed care environments, but not in the traditional Medicare program. The potential for financial loss or gain associated with hospital use under capitation has always created incentives for managed care organizations to reduce hospital readmission from nursing homes.
With all these policies, however, nursing homes may well find themselves challenged to reduce readmissions to the hospital for short-stay patients, and the frequency of admissions for long-stay residents. Nursing homes that choose to compete for higher reimbursed Medicare patients and participate in Accountable Care Organizations (ACOs) will be compelled to demonstrate their performance in this regard.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 49
The Challenges That Nursing Homes Face
MEASURING PERFORMANCE BASED ON READMISSION TO HOSPITAL
In the hospital sector, the initial focus was on developing a standardized approach to measuring performance based on readmission of hospital discharges. The current measure for hospitals is the rate at which patients discharged from hospitals are readmitted in a 30-day time period.
In comparing readmission rates among hospitals and creating financial incentives to reduce readmissions, a major problem is that the risk of readmission among discharged patients varies considerably. If this differential risk is not taken into consideration, rates cannot be compared across hospitals. In fact, as found in the early releases of hospital mortality rates, those hospitals that treat the most acute and complex patients generally have higher unadjusted readmission rates. And not surprisingly, those hospitals that are best equipped and highest quality often admit the most complex patients, leading to higher mortality and readmission rates.
Condition-specific performance measures have been used in the hospital sector in order to control for differences in readmission risk for patients with different conditions. The rates of readmission differ for patients with different conditions, and the comorbid diseases that increase the readmission risk for one condition differ from those that increase the risk for another condition. Thus, the measures on Hospital Compare are stratified by patient condition (i.e., heart failure, pneumonia, acute myocardial infarction), and then they are risk-standardized differently for each discharge diagnosis in order to
make valid comparisons across settings.6, 7, 8 By risk standardizing these readmission measures, CMS reduces the incentive for hospitals to selectively admit lower risk patients as a strategy to reduce hospital readmissions.
The same rigor as applied in hospitals has to be applied to measurement of readmissions from nursing homes. The measures, however, are different from the nursing home perspective. For example, the denominator for nursing home rates is nursing home admissions, not discharges, since the nursing home admission corresponds to the time of hospital discharge.
In addition, the rate of readmissions to hospital for nursing home admissions is highest in the first weeks after start of nursing home care and decreases gradually until about 90–100 days, when the rate of readmissions becomes fairly steady (Figure 1). The risk of readmission is not constant in this initial period: it is highest immediately after admission
6 Krumholz et al. “Hospital 30-Day Heart Failure Readmission Measure Methodology,” 2008.
7 Krumholz et al. “Hospital 30-Day Acute Myocardial Infarction Readmission Measure Methodology,” 2008.
8 Krumholz et al. “Hospital 30-Day Pneumonia Readmission Measure Methodology,” 2008.

2011 A N N UA L QUA L I T Y R EP O R T50
SNF DAYS UNTIL REHOSPITALIZATION
FIGURE 1
7
14
21
28
35
42
49
56
63
70
77
84
91
98
0
0 1 2 3 4 5Percent of Hospitalized Residents
Day
s
Source: Andrew Kramer, MD, Theresa Ellertsen, BS, Glenn Goodrich, MS, Sung-joon Min, PhD, “Understanding Temporal Changes in and Factors Associated with SNF Rates of Community Discharge and Rehospitalization,” MedPAC, June 12, 2007, table C, pg. A6.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 51
to the nursing home and gradually decreases. Thus, within the first 100 days it makes sense to measure the rate at which patient stays end in an admission to a hospital over the total number of admissions.
Once the rate of hospital admissions becomes fairly steady at about 100 days, then the risk of admission is relatively constant for each day. For long-term residents of nursing homes, therefore, the more logical hospital admission measure is the number of admissions to hospital per nursing home day (or 100 days), pooling days across residents. Researchers clearly distinguish between hospitalizations of new admissions and long-stay residents because they reflect different policy and care issues.9, 10 For these reasons, the value-based purchasing demonstration for nursing homes has separate measures for short- and long-stay residents.
Because nursing home care and hospitalization of nursing home residents is often unrelated to a resident’s primary diagnosis, disease-specific hospitalization measures defined by the hospital discharge diagnosis or primary admitting diagnosis to the nursing home are less appropriate. Rather, the focus in nursing homes is on reducing avoidable admissions. The challenge is to determine whether there are avoidable admissions, how to do define them, and how to prevent them.
9 Grabowski, David C., A. James O’Malley, and Nancy R. Barhydt. “The Costs And Potential Savings Associated With Nursing Home Hospitalizations.” Health Affairs 26(6):1753–1761, 2007.
10 Mor, Vince, Orna Intrator, Zhanlian Feng, and David C. Grabowski. “The Revolving Door of Hospitalization from Skilled Nursing Facilities.” Health Affairs 29:57–64, 2010.
ARE THERE AVOIDABLE HOSPITAL READMISSIONS FROM NURSING HOMES?
Over the past decade, several different methods have been used to determine the extent to which hospital readmissions from nursing homes are avoidable. Although variability exists in the estimated rates of avoidable hospitalizations, a consensus has emerged that a significant number of readmissions or first-time admissions to hospital are avoidable. In addition, a great deal has been learned about the causes of hospital admissions and the types of nursing home residents at greatest risk.
A structured implicit record review led to the first well-publicized estimate of “appropriateness” of hospital transfers and Emergency Department visits for nursing home residents.11 This approach involved two physicians conducting a chart review to “rate a transfer or admission appropriate when no lower level of care would suffice to deliver safely the services the resident required.” This study concluded that 40 percent of hospital transfers were
“inappropriate,” which increased to 45 percent when advanced directives were taken into consideration. Characteristics of the acute illness, resource needs and availability of services, and the quality of acute care in the nursing home all contributed to reviewer’s determination of the appropriateness of hospital transfers.
11 Saliba, D., R. Kington, J. Buchanan et al. “Appropriateness of the Decision to Transfer Nursing Facility Residents to Hospital.” Journal of the American Geriatric Society 48:154–163, 2000.

2011 A N N UA L QUA L I T Y R EP O R T52
Ten years later, a larger and modified structured implicit record review found that 67 percent of hospitalizations were “potentially avoidable.”12
The expert panel most commonly cited greater availability of physicians, NPs, and PAs for on-site assessment of acute changes in clinical status of nursing home residents; the need to improve overall care quality for residents with acute changes in condition; and the ability to obtain diagnostic tests and administer intravenous fluids as important in preventing avoidable hospitalizations. They also cited the need to reduce the amount of futile care and improve advance care planning to reduce avoidable hospitalizations.
These studies clearly suggested that a significant portion of hospitalizations could be prevented; however, it should not be inferred that these rates of “inappropriate” or “potentially avoidable” hospitalizations are the actual proportion of hospitalizations that were unnecessary. Retrospective assessment, or hindsight, differs from making the decision of whether or not to hospitalize a nursing home resident in real time.
The studies did provide valuable insight into the causes of readmission and the challenges facing nursing homes. Both studies concluded that the quality of acute care in nursing homes, availability
12 Ouslander et al. “Potentially Avoidable Hospitalizations of Nursing Home Residents: Frequency, Causes, and Costs.” Journal of the American Geriatric Society 58:627–635, 2010.
of acute care resources in a nursing home (including MDs or NPs), and the presence of advanced directives were critical determinants of preventing hospitalizations. These are all under the influence of a nursing home and therefore make a strong case that hospital admission rates can be viewed as a performance measure for nursing homes. In the current policy climate, this performance measure has gained importance.
RATES OF READMISSION TO HOSPITAL FROM SNF AT 30 AND 100 DAYS FOR POTENTIALLY AVOIDABLE CONDITIONS USED IN NURSING HOME VALUE-BASED PURCHASING
30DAYS (N=2,128,978)
100 DAYS (N=2,107,333)
HOSPITAL ADMISSION DIAGNOSIS
Any reason 17.7 22.4
ANY OF FIVE CONDITIONS BELOW: 13.9 17.5
CHF 7.9 8.7
Electrolyte imbalance 6.8 8.6
Respiratory infection 4.6 5.8
Sepsis 2.4 3.0
UTI 4.7 6.2
Readmission rates are based on the presence of an acute or critical care access hospitalization within 30 (100) days of the SNF admission date, with no intervening claim. Stays for residents who are discharged to community within 30 (100) days and then hospitalized within 3 days of the discharge are considered readmitted. The admission diagnosis can be either the primary or a secondary diagnoses listed on the claim for that hospitalization. Residents who died prior to the end point of the outcome period (e.g., 30 days) were excluded from the measure.
Source: Donelan-McCall, N., T. Eilertsen, R. Fish, and A. Kramer. “Small Patient Population and Low Frequency Event Effects on Stability of SNF Quality Measures – Final Report” Medicare Payment Advisory Commission. Washington, DC, September 14, 2006.
TABLE 2

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 53
HOW TO IDENTIFY POTENTIALLY AVOIDABLE HOSPITALIZATIONS AND MEASURE RATES
Other studies have emphasized how to more easily identify potentially preventable hospitalizations using the data available in administrative data sets, rather than through retrospective chart review. One approach was to identify potentially preventable hospitalizations based on Ambulatory Care Sensitive Conditions (ACSCs), for which it is believed that good outpatient care can potentially prevent the need for hospitalization.
These “Prevention Quality Indicators” include potentially preventable hospitalizations for chronic diabetes, respiratory conditions, and circulatory conditions, as well as for acute dehydration, bacterial pneumonia, and urinary tract infections.13 In 2008, about 17 percent of hospitalizations from all settings (largely the community) were considered potentially preventable because they occurred for one of these conditions.14 Others have used these or different subsets of ACSCs to identify potentially preventable hospitalizations from nursing homes.15, 16
Based on literature related specifically to hospitalization of nursing residents, five conditions were identified as “potentially avoidable” hospitalizations for nursing home residents.17 These five conditions include
13 Agency for Healthcare Research and Quality. “Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions.” Version 3.1; March 2007. http://www.qualityindicators.ahrq.gov
14 Stranges, E. and C. Stocks “Potentially Preventable Hospitalizations for Acute and Chronic Conditions,” 2008. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb99.pdf
15 Carter, Mary W. “Factors Associated with Ambulatory Care-Sensitive Hospitalizations Among Nursing Home Residents.” Journal of Aging and Health 15:295–331, 2003.
16 Intrator, O., J. Zinn and V. Mor. “Nursing Home Characteristics and Potentially Preventable Hospitalizations of Long-Stay Residents.” Journal of the American Geriatric Society 52: 1730–1736, 2004.
17 Kramer, A.M. and R. Fish. “The Relationship Between Nurse Staffing Levels and the Quality of Nursing Home Care.” Appropriateness of Minimum Nurse Staffing Ratios in Nursing Homes: Phase II Final Report; Chapter 2, Abt Associates, Inc., 2001.
hospitalizations for a primary or secondary diagnosis of: heart failure, respiratory infection, urinary tract infection, sepsis, and/or electrolyte imbalance (Table 2).
MedPAC chose to use this rate of potentially avoidable hospitalizations as the basis for their performance measure for SNFs.18 Extensive study of this measure led to the following conclusions.19 First, the minimum number of admissions for a stable measure of readmissions was found to be 25 admissions. Second, in nursing homes there was a high correlation among the condition-specific rates so it was determined that they could be validly combined into a single composite measure of readmission for any of the five conditions. Finally, an adequate risk adjustment model was estimated to control for differences in risk of hospitalization between nursing homes and over time in the same home.
The validity of this performance measure is demonstrated in part by the relationship to staffing levels for skilled staff. Higher rates of hospitalization using this measure were shown to be associated with lower nursing home staffing ratios for RN staffing hours and for combined RN, ADON, and DON staffing hours.20 Also, higher staff turnover for RNs and licensed staff were associated with increased hospitalization using this measure.
Because this measure and these methods have proven to be robust, they are being used for performance measurement in the Nursing Home Value-Based
18 Medicare Payment Advisory Commission. “Report to Congress: Medicare Payment Policy.” Section 3A: Skilled Nursing Facilities. March 2007.
19 Donelan-McCall, N., T. Eilertsen, R. Fish and A.M. Kramer. “Small Patient Population and Low Frequency Event Effects on Stability of SNF Quality Measures – Final Report.” Medicare Payment Advisory Commission. September 2006.
20 Kramer, A.M., S. Elder, G. Goodrich, R. Fish, N. Donelan-McCall. “Relationship Between Staffing Measures and Community Discharge, Rehospitalization, and Post-Acute Care Quality Measures for Short-Stay Residents.” Colorado Foundation For Medical Care. January 2008.

2011 A N N UA L QUA L I T Y R EP O R T54
Purchasing Demonstration by CMS, and by MedPAC to monitor rates of potentially avoidable hospitalizations for nursing homes.
From a clinical perspective, potentially avoidable hospitalizations defined in this manner were never intended to mean that no hospitalizations should occur from nursing homes for these conditions – they are not all preventable. In fact, some patients definitely should be hospitalized for acute treatment of these conditions. Hospitalizations for these conditions are just more likely to be avoidable than hospitalizations for many other conditions, yielding lower hospitalization rates for these conditions with high quality nursing home care. Thus, interventions aimed at reducing hospitalizations for these conditions make sense as a starting place for nursing homes that are trying to reduce hospitalization rates.
Recommended Approaches to Reducing Avoidable HospitalizationsThe recent emphasis on care transitions and for hospital discharges for the CMS specified conditions relates largely to primary care and follow-up for the larger number of Medicare patients discharged home, often without any post-acute care. While solutions such as more intensive follow-up after hospital discharge with case management, patient empowerment, improved transfer of patient information, improved communication, and remote monitoring have been successful in these types of transitions, only some of these address the issues that arise in nursing homes. The patients discharged to nursing homes are different in many respects and the systems issues, while sometimes similar, are not identical.
Preventing readmission from nursing homes requires solutions designed for the SNF population and the nursing home environment. An important policy issue is the recognition of this distinction and encouragement of interventions that are aimed at reducing readmissions for the more complex and frail patients who are discharged to SNFs. These involve approaches that enhance the capacity of SNFs to provide the necessary services to avoid readmissions. Some approaches are targeted on specific types of patients and others are more global systemic approaches (Box 1).
STRATEGIES FOR REDUCING AVOIDABLE HOSPITALIZATIONS
Targeted Strategies
■■ Disease Management Programs for ACA conditions frequently discharged to SNFs (e.g., heart failure and pneumonia)
■■ Assessing Patient Risk for Readmission
■■ Increasing Advanced Care Planning (e.g., MAPP) for those at high mortality risk
Global Strategies
■■ Measuring and Monitoring Risk-Adjusted Rates
■■ Intervention Toolbox (e.g., INTERACT II)
■■ Advanced Practice Nurses/Physician Assistants
■■ Dedicated Physician Coverage Aimed at Managing Acute Decline
BOX 1

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 55
TARGETED APPROACHES TO REDUCING AVOIDABLE HOSPITALIZATIONS
Given that the ACA will go into effect in 2012, the nursing home sector can demonstrate value in the fee-for-service system by partnering with hospitals to reduce readmissions particularly for patients with pneumonia and heart failure, which represent significant numbers of SNF admissions. This can be accomplished in part with initiatives for management of patients with these two conditions, including specialized programs. The same type of monitoring systems that are used in outpatient settings can be adapted to nursing home care for these conditions.
However, the hospital readmission rates that CMS calculates are not based solely on readmissions for the same diagnosis as the discharge diagnosis. Even when a SNF does a superb job managing heart failure for a patient with this hospital diagnosis related group, if the patient is readmitted for COPD or a fall, then it will count as a readmission for that discharge diagnosis. That is, the rates are for all-cause readmissions among patients with the selected hospital discharge diagnosis.
Thus, while managing pneumonia, heart failure, and acute MI is important, nursing home care still needs to focus on preventing readmissions for any reason. The set of readmission conditions used in the Value-Based Purchasing demonstration is much broader (it does include respiratory infections and heart failure), and is based on both primary and secondary diagnoses, which is more tailored to the nursing home population.
SNF patients are often at risk for readmission due to their multiplicity of diseases, their functional disabilities, and in many cases cognitive deficits.
If a targeted strategy is used, therefore, it should go beyond a narrow disease management focus. Such a strategy should involve assessing each patient’s risk for readmission for all causes and identifying the specific sources of risk. Interventions can then be targeted on the patients and patient problems with the greatest risk of readmission. This is still a targeted approach, but it is targeted on patients at highest risk of readmission from SNF and the sources of their risk.
One successful intervention targeted reducing hospitalizations for patients at high risk of death through an intensive intervention related to advanced directives. Site of death in the hospital as opposed to the nursing home has been shown to vary widely and is most strongly associated with presence of Do Not Resuscitate (DNR) or Do Not Hospitalize (DNH) orders.21 Given that just 32 percent of Medicare SNF patients had DNR orders and 2 percent had DNH orders in one national study, interventions aimed at obtaining advanced directives have the potential to reduce hospitalizations.22 Although advanced care planning is important for all nursing home residents, this intervention used a targeted approach by screening to identify those at highest risk of death, and then providing intensive discussions and initiating palliative care. This targeted strategy and the tools in this program, termed Making Advanced Planning a Priority (MAPP), markedly reduced hospitalizations among nursing home residents with high mortality risk.23
21 Levy, C.R., R. Fish and A.M. Kramer. “Site of Death in the Hospital Versus Nursing Home of Medicare Skilled Nursing Facility Residents Admitted Under Medicare’s Part A Benefit.” Journal of the American Geriatric Society 52(8):1247–54, August 2004.
22 Levy, C.R., R. Fish and A.M. Kramer. “Do-Not-Resuscitate and Do-Not-Hospitalize Directives of Persons Admitted to Skilled Nursing Facilities Under the Medicare Benefit.” Journal of the American Geriatric Society 53(12):2060–8, December 2005.
23 Levy, C., M. Morris and A. Kramer. “Improving End-of-Life Outcomes in Nursing Homes by Targeting Residents at High-Risk Mortality for Palliative Care: Program Description and Evaluation.” Journal of Palliative Medicine 11(2):217–25, March 2008.

2011 A N N UA L QUA L I T Y R EP O R T56
GLOBAL STRATEGIES FOR REDUCING READMISSIONS
An important part of any strategy to reduce readmissions is accurate measurement and monitoring of risk-adjusted hospitalization rates. The above measurement discussion is important from the perspectives of comparing hospital admission rates across nursing homes, tracking rates within a single facility over time, and determining whether interventions are having a favorable effect. All of this requires rigorous measurement methods to ensure that one is not misled by anecdotes or by not controlling for exogenous and endogenous factors. Clearly defining universal readmission measures and methods (e.g. risk adjustment) for nursing homes is a high policy priority if we are going to be able to compare sites and interventions.
With respect to care, the challenge is to effectively intervene before it is too late. The most comprehensive global toolbox that is currently available for reducing hospital admission is Interventions to Reduce Acute Care Transfers, or Interact II.24 Interact II includes communication tools, care paths, advanced care planning tools, and forms for quality improvement. Interact II was found to reduce unadjusted hospitalization rates by 17 percent when used over six months in a collaborative that also involved leadership education, nursing staff education, facility champions, and conference calls.25
With respect to improving the quality of response to acute illness in nursing homes, many studies have
24 www.interact.geriu.org25 Ouslander et al. “Interventions to Reduce Hospitalizations from
Nursing Homes: Evaluation of the INTERACT II Collaborative Quality Improvement Project.” Journal of the American Geriatric Society 59:745–753, 2011.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 57
shown the favorable impact of advanced practice nurses.26, 27 Even more effective is the use of Geriatric Nurse Practitioners/Physicians Assistants working in collaboration with dedicated and knowledgeable physicians. The Evercare model, with its widespread success in reducing hospitalizations, is one model of such care.28 Without the financial incentives under this managed care model, organizations must find creative ways to more fully engage physicians in the care of nursing home residents and fund advanced practice nurses.
ConclusionsThe imperative for reducing readmissions to hospitals from all settings, and decreasing potentially avoidable hospitalizations for nursing home residents comes from many sources. These include the evolution of hospital policies; the changing relationships between hospitals and nursing homes; new nursing home policies; and most importantly, recognition of the disruption that care transitions cause for residents. Although a decline in nursing home care quality is not the cause of this growing problem; nursing homes can be an important part of the solution. Nursing home operators can see this as an opportunity to bring creative solutions to the table and increase their value. Because this has not in the past been the focus of care in nursing homes, solutions are in the early stages and will substantially improve with experience.
26 Intrator, O., J. Zinn, and V. Mor. “Nursing Home Characteristics and Potentially Preventable Hospitalizations of Long-Stay Residents.” Journal of the American Geriatric Society 52: 1730–1736, 2004.
27 Shaughnessy, P.W., A.M. Kramer, D.F. Hittle, and J. Steiner. “Quality of Care in Teaching Nursing Homes: Findings and Implications.” Health Care Financing Review 16(4):55–83, 1995.
28 Kane, R.L., G. Keckhafer, S. Flood et al. “The Effect of Evercare on Hospital Use.” Journal of the American Geriatric Society 51:1427–1434, 2003.
While embracing these opportunities, nursing home providers need to balance the resources devoted to this issue with all other aspects of nursing home quality. Nursing home providers must address this challenge while continuing to meet all the needs of short-term residents, such as the provision of effective rehabilitation care, and continuing to enhance care and quality of life for the increasingly complex population of long-term residents.
The use of condition-specific hospital readmission measures that are risk adjusted has important implications for nursing homes. First, the stratification by condition means that nursing homes may be able to specialize in care for patients with selected clinical conditions, and reduce the risk of readmission. Second, the risk adjustment reduces the incentive for nursing homes to admit only lower risk patients as a strategy to demonstrate their value to hospitals by a low rate of readmissions to hospital. Third, these methods set a rigorous standard for measuring hospitalization rates in nursing homes.

2011 A N N UA L QUA L I T Y R EP O R T58
Nursing facilities should be
encouraged to optimize
rehabilitation outcomes
through a combination
of good nursing, medical,
and multidisciplinary
therapy services.
FOCUS ON Rehabilitation Measures

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 59
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Focus on Rehabilitation MeasuresAndrew Kramer, MD, CEO, Providigm LLC Professor of Medicine, University of Colorado
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix
FOCUS ON Rehabilitation Measures

2011 A N N UA L QUA L I T Y R EP O R T60
FOCUS ON Rehabilitation MeasuresAs stated by T. Franklin Williams, a founder of
the field of Geriatric Medicine, “Rehabilitation
is an approach, a philosophy, and a point of view
as much as it is a set of techniques. The aim of
rehabilitation, to restore an individual to his/her
former functional and environmental status, or,
alternatively, to maintain or maximize remaining
function, should be at the heart of all care of
aging persons in order to help them continue to
live as full a life as possible.”1
Using this holistic definition, rehabilitation is
appropriate for virtually all patients admitted to
Skilled Nursing Facilities (SNFs), and a subset of
long-term residents. The rehabilitation “approach,
philosophy, and point of view” should be integral
to all aspects of SNF care. Understandably,
realistic rehabilitation goals vary considerably
based on each resident’s condition, motivation,
and potential for recovery. Thus, one of the
greatest challenges faced by SNFs is determining
1 Williams, T .F . “Introduction: Rehabilitation in the Aging: Philosophy and Approaches .” Rehabilitation in the Aging . Editor, T . Franklin Williams . New York : Raven Press, ©1984 . page xiii .
and measuring each resident’s potential for
recovery or maintenance of function. In many
cases recovery is unpredictable, and it is only
through a trial of rehabilitation services that we
come to understand a patient’s actual potential.
With older persons, allowing sufficient time for
recovery is critical; it can be months or even years.
In the present climate, the narrow definition of rehabilitation stands in the way of both good policy and good clinical care. The policy focus is on proving that progress is being made using a granular set of measures, over time periods that are too short to detect the full impact of rehabilitation. In striving to measure these short-term gains, we lose track of the
all-important patient’s perspective and the long-term gains that are the true goals of rehabilitation.
SNFs provide post-acute rehabilitation care to more frail elders than any other post-acute setting. Unlike most post-acute alternatives, SNFs provide rehabilitation care to a varied and highly disabled

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 61
population. While some of this care is provided exclusively in SNFs, rehabilitation is increasingly provided in episodes that involve multiple providers and care transitions among these settings. Shorter stays in each setting and transitions across settings require a paradigm shift in our thinking about how to measure quality of rehabilitation care.
The Critical Role of Skilled Nursing Facilities in Rehabilitation In 2009, 1.6 million Medicare fee-for-service beneficiaries had 2.4 million SNF stays.2 Ninety-two percent (92%) of these SNF days were in large part for rehabilitation. Many of these SNF patients were also clinically complex requiring skilled nursing services as well. These nursing needs complicate the provision of rehabilitation care, but in no way diminish the need for and significance
2 Medicare Payment Advisory Commission. “Report to Congress: Medicare Payment Policy,” Chapter 7: Skilled Nursing Facility Services. March 2011a. medpac.gov/chapters/Mar11_Ch07.pdf
of rehabilitation services. Thus, rehabilitation was a major focus of care for about 2.3 million Medicare SNF stays in 2009 (Table 1).
In sharp contrast, Inpatient Rehabilitation Facilities (IRFs) had only 360,000 Medicare stays in 2009.3 Requirements that IRF patients participate in three hours of therapy per day and regulations requiring a focus on selected musculoskeletal and neurological disorders appropriately limit the use of this more specialized resource for patients who are not too frail to benefit from such intensive rehabilitation services.
Relative to SNF patients receiving rehabilitation, IRF patients have been found to have significantly better baseline function, and then following the acute event, have less cognitive impairment, greater social supports, greater levels of participation in therapeutic and recreational activities, and a lower
3 Medicare Payment Advisory Commission. “Report to Congress: Medicare Payment Policy,” Chapter 9: Inpatient Rehabilitation Facility Services. March 2011b. medpac.gov/chapters/Mar11_Ch07.pdf
SKILLED NURSING FACILITIES PROVIDE MORE MEDICARE FEE-FOR-SERVICE POST-ACUTE REHABILITATION THAN ANY OTHER PROVIDER TYPE, 2009
Provider Type
SNF IRF Home Health
Volume of Stays 2.3 Million 360 Thousand 1 Million*
Medicare Payments $24 Billion $6 Billion $5–6 Billion*
Eligibility Criteria 3-day Hospitalization 60% of Medicare stays for one of 10 diagnoses
Homebound but able to live at home
Therapy Services Receive 45 minutes to 720 minutes per week
3 hours per day required 1 to 14+ in-home therapy visits
*Proportion of total visits that are therapy visits applied to number of home health users and total Medicare home health expenditures
Source: MedPAC 2011.
TABLE 1

2011 A N N UA L QUA L I T Y R EP O R T62
prevalence of severe speech and language impairment and depression.4 Stroke patients admitted to SNFs, for example, had worse pre-stroke ADL function, worse admission function, and worse cognition than IRF stroke patients (Figure 1).5 Thus, the challenge in SNF rehabilitation is unique: optimizing functional outcomes for frail patients with multiple limitations.
Post-acute home health care usage has increased significantly in recent years for homebound Medicare beneficiaries. Home health care rehabilitation is an important rehabilitation alternative for patients who are able to reside in their homes, with therapy visits representing 28 percent of total home health visits received by the 3.3 million Medicare Home Health users in 2009.6 Relative to SNF patients, however, home health patients have substantially better cognitive and physical function, greater social supports, better self-reported health, a lower prevalence of speech and language problems, and less depression Kramer et al 2006 b).7, 8, 9 Thus, the home
4 Kramer et al. “Outcomes and Costs after Hip Fractures and Stroke: A Comparison of Rehabilitation Settings.” JAMA 277(5):396–404, 1997.
5 Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Patterns of Post-Acute Care Following Implementation of PPS,” A Study of Post-Acute Care Costs and Outcomes: Final Report, Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. December 28, 2006 a: pg 57. http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
6 Medicare Payment Advisory Commission. “Report to Congress: Medicare Payment Policy,” Chapter 8: Home Health Services. March 2011c. medpac.gov/chapters/Mar11_Ch08.pdf
7 Kramer, A.M., P.W. Shaughnessy, M.L. Pettigrew. “Cost-Effectiveness Implications Based on a Comparison ofNursing Home and Home Health Case Mix.” Health Services Research 20(4):387405, 1985.
8 Liu, K., D. Wissoker, and C. Rimes. “Determinants and Costs of Post-Acute Care Use of Medicare SNFs and HHAs.” Inquiry 35(1):49–61, 1998.
9 Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Patterns of Post-Acute Care Following Implementation of PPS,” A Study of Post-Acute Care Costs and Outcomes: Final Report, Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. December 28, 2006 b: pg 57. http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
SNF STROKE PATIENTS HAD LOWER FUNCTIONAL STATUS THAN IRF AND HOME HEALTH PATIENTS
* Higher is better function: Dressing, Bathing, Grooming, Eating, Transferring, Toileting
** Higher is better function: Barthel Index – eating, transferring, grooming, toileting, bathing, dressing, walking, bowel incontinence, and bladder incontinence
*** Higher is better function: Mini-mental status score (0–30)
Source: Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Patterns of Post-Acute Care Following Implementation of PPS,” Chapter 4 in A Study of Post-Acute Care Costs and Outcomes: Final Report, Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. December 28, 2006 a : pg 57 http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
FIGURE 1
0
5
10
15
20
SNF IRF HH
0
20
40
60
80
SNF IRF HH
0
5
10
15
20
25
SNF IRF
Pre-
stro
ke A
DLFu
nctio
n (0
–18)
*Ad
miss
ion
ADL
Func
tion(
0–90
)**
Adm
issio
n Co
gniti
veFu
nctio
n (0
–30)
***
HH

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 63
health population receiving rehabilitation is less frail and disabled than SNF patients (Figure 1).
In addition to providing rehabilitation to a large and varied population following acute hospital care, SNFs also serve as a major subsequent site of care for patients first discharged to IRFs. For example, IRF stroke patients with more significant physical and cognitive impairments and fewer social supports are generally discharged to SNFs. Whereas those who are less impaired are discharged home with home rehabilitation, outpatient rehabilitation, or sometimes no further rehabilitation services.10
Due to the large number of patients with significant impairments receiving rehabilitation in SNFs, Medicare expenditures for SNF rehabilitation far exceed Medicare expenditures for rehabilitation in other post-acute settings. About $24 billion of Medicare FFS expenditures in 2009 were for services provided to SNF patients receiving rehabilitation care.11 Despite the substantially higher cost of IRF stays, Medicare FFS expenditures for IRFs totaled $6 billion in 2009.12 Medicare home health payments for rehabilitation visits were in the range of $5 to $6 billion in 2009. In addition, managed care organizations heavily utilize SNFs for rehabilitation in contrast to more expensive alternatives.13, 14
10 Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Patterns of Post-Acute Care Following Implementation of PPS,” A Study of Post-Acute Care Costs and Outcomes: Final Report, Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. December 28, 2006 c : pgs 55–71. http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
11 MedPAC March 2011a. 12 MedPAC March 2011c.13 Kramer, A.M., J.C. Kowalsky, M. Lin, J. Grigsby, R. Hughes, and J.F.
Steiner. “Outcome and Utilization Differences for Older Persons with Stroke in HMO and Fee-For-Service Systems.” Journal of the American Geriatrics Society 48(7):726–734, 2000.
14 Coleman, E.A., A.M. Kramer, J.C. Kowalsky, D.G. Eckhoff, M. Lin, E.J. Hester, N. Morgenstern, and J.F. Steiner. “A Comparison of Functional Outcomes after Hip Fracture in Group/Staff HMOs and Fee-for-Service Systems.” Effective Clinical Practice 3(5):229–239, 2000.
The cost and intensity of rehabilitation services provided by SNFs varies substantially, leading to differences in rehabilitation outcomes. One national study that was conducted prior to implementation of SNF PPS compared therapy intensity and outcomes for Medicare patients between high-Medicare volume SNFs (i.e., subacute SNFs) and more traditional SNFs. Stroke patients received more therapy in subacute SNFs than in traditional SNFs (means of 7.9 vs. 5.3 hours per week). These numbers represent averages across the stay; in fact, therapy intensity was provided much more intensively in the early days of the SNF stays and then was reduced over time.15 The stroke patients had substantially longer stays than hip fracture patients in both traditional and subacute SNFs, resulting in many more total therapy hours during their stay.
Stroke patients admitted to subacute SNFs, where therapy intensity was greater, however, were 6.8 times more likely to be discharged to community than stroke patients from traditional SNFs. These studies and others like them that compare different rehabilitation environments clearly suggest a strong relationship between therapy intensity and outcomes in SNFs.16 Thus, incentives to provide higher intensity therapy service in SNFs should be preserved, and will pay off in reduced total healthcare costs because more patients will be living independently in the community.
Rehabilitation for more traditional long-stay nursing facility residents is covered under Medicare part B. Much less is known about the benefits and costs of chronic rehabilitation services in nursing facilities.
15 Kramer, A.M., R.E. Schlenker, T.B. Eilertsen, and C.A. Hrincevich. “Stroke Rehabilitation in Nursing Homes.” Topics in Stroke Rehabilitation 4(1):53–63, 1997b.
16 Kramer, A.M., J.C. Kowalsky, M. Lin, J. Grigsby, R. Hughes, and J.F. Steiner. “Outcome and Utilization Differences for Older Persons with Stroke in HMO and Fee-For-Service Systems.” Journal of the American Geriatrics Society 48(7):726–734, 2000.

2011 A N N UA L QUA L I T Y R EP O R T64
This should not, however, be interpreted as a lack of benefit. Maintenance of function and prevention of decline for frail nursing facility residents is clearly an important aspect of rehabilitation. Preserving function should be central to nursing facility care both because it enhances quality of life and can reduce falls, contractures, and other injuries that can lead to further functional losses. Given the acute care rather than prevention bias of US health care and the Medicare program, it is critical that we preserve Medicare part B reimbursement for therapy services in nursing facilities and strive to demonstrate the benefits of ongoing therapy services beyond the 100 days of the Medicare part A benefit.
Quality Measures Traditionally Used for RehabilitationThe most widely used measures of rehabilitation quality are outcomes based on setting-specific data that are collected for clinical purposes to monitor patient progress, make treatment decisions, and/or determine resource needs. Functional data are used to objectively identify and monitor deficits at a granular level in order to optimize treatment in all rehabilitation settings. The measures are tailored to the patient populations and clinical needs of each setting. Thus, it is not surprising that different data and measures have evolved for different rehabilitation settings.
In SNFs, the measures pertinent to rehabilitation in the Minimum Data Set (MDS) relate to needs for assistance in Activities of Daily Living (ADLs), mobility, cognitive deficits, speech and language deficits, activity participation, and daily routines – all of which have to be taken into consideration in treating SNF residents. With the more narrow population in IRFs, the IRF Patient Assessment Instrument (IRF-PAI) based on the Functional Independence Measure (FIM) is used. These
measures are designed to be sensitive to granular changes in physical function over the much shorter IRF stays. Although some SNF rehabilitation programs use the FIM in addition to the required MDS measures, this is not a Medicare requirement, so there is limited ability to compare these clinical outcomes across settings.
The OASIS for home care includes a broader array of functional measures, including Instrumental Activities of Daily Living (IADLs), which are appropriate to assess for individuals residing in their homes. The different wording, scaling, and data collection intervals make comparisons across settings problematic.
Limitations of Traditional Rehabilitation Quality MeasuresUsing setting-specific, clinical outcome measures for policy, such as comparing rehabilitation outcomes across settings, and also for performance measurement is problematic for several reasons. A major problem is that they are collected only during the relatively short intervals in which patients are receiving rehabilitation in a specific setting. In IRFs, for example, functional recovery as measured by the FIM has been shown to continue for at least three months; well beyond the time of discharge from rehabilitation care (Table 2).17 Other studies that follow SNF and IRF patients for periods of up to a year demonstrate that many patients continue to improve for much longer than three months (Figure 2).18
17 Ottenbacher, K.J., P.M. Smith, S.B. Illig, R.T. Linn, G.V. Ostir, and C.V. Granger. “Trends in Length of Stay, Living Setting, Functional Outcome, and Mortality Following Medical Rehabilitation” JAMA 292:1687–1695. 2004.
18 Johnson, M., A.M. Kramer, M. Lin, J. Kowalsky, and J. Steiner. “Outcomes of Older Persons Receiving Rehabilitation for Medical and Surgical Conditions Compared with Hip Fracture and Stroke.” Journal of the American Geriatrics Society 48(11):1389–1397, 2000.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 65
IRF PATIENTS RECEIVING REHABILITATION CONTINUE TO IMPROVE AFTER ACUTE REHABILITATION DISCHARGE FOR AT LEAST 90 DAYS FOR ALL REHABILITATION CONDITIONS
Hip Fracture StrokeNeurological Conditions Brain Spinal Cord
N=67,564 48,055 8,871 13,275 11,042
Admission FIM Score 81 63 73 61 72
Discharge FIM Score* 105 87 94 87 96
Follow-up FIM Score** 113 97 98 97 100
* Median for hip fracture 11 days, for stroke 20 days, for neurological conditions 16 days, for brain dysfunction 18 days, spinal cord dysfunction 17 days
** Median 89–90 days: interquartile range 84–97
Source: Ottenbacher et al. 2011.
TABLE 2
FUNCTION CONTINUES TO IMPROVE FOR UP TO A YEAR FOR MANY REHABILITATION PATIENTS
FIGURE 2
0
1
2
3
4
5 Stroke
Med/Surg
Hip
0
1
2
3
4
5
Num
ber
of A
DLS
with
No
Diff
icul
ty (0
–5)
One Month Prior
Rehab Admission
3 Months 6 Months 9 Months 1 Year
Timepoint
Hip
Stroke
Med/Surg
4.37
3.88
2.5
3.62
3.16
1.36
4.35
1.45
3.83
3.9
3.34 3.34
3.78
4.02
3.88
4.01
3.38
3.92
Source: Journal of the American Geriatrics Society 48(11), November 2000.

2011 A N N UA L QUA L I T Y R EP O R T66
A second issue is that most patients receive care in multiple settings during an episode of rehabilitation.19, 20 For stroke patients for example, 170 different patterns of post-acute rehabilitation care were found in the first 90 days among only 642 stroke patients discharged from the hospital for rehabilitation. Eighty-two percent (82%) received rehabilitation care in two or more settings during the 90-day period.21
Third, the measures are not comparable. Without comparable data, data collection, and time intervals, rehabilitation outcomes are difficult to compare. While in some studies these measures have been mapped to similar functional indices, the granularity of the
19 DeJong, G., W. Tian, R.J. Smout, S.D. Horn, K. Putman, P. Smith, J. Gassaway, and J.E. DaVanzo. “Use of Rehabilitation and Other Health Care Services by Patients with Joint Replacement After Discharge from Skilled Nursing and Inpatient Rehabilitation Facilities.” Archives of Physical Medicine and Rehabilitation 90:1297–305, 2009.
20 Tian, W., G. DeJong, M.C. Munin, and R. Smout: “Patterns of rehabilitation after hip arthroplasty and the association with outcomes: An episode of care view.” American Journal of Physical Medicine and Rehabilitation 89:905–922, 2010.
21 Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Patterns of Post-Acute Care Following Implementation of PPS,” A Study of Post-Acute Care Costs and Outcomes: Final Report. December 28, 2006 c: pgs 55–71. http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
measures is lost in that mapping.22 Given the multiple purposes of the functional data that are used for these rehabilitation outcome measures (e.g. reimbursement, care planning) and the differences in the patient populations, it is complex to move towards a uniform set of functional measures within these different settings.
Fourth, even when one of these measures is applied across more than one setting, it is difficult to control for selection differences. Gains or losses in these measures are influenced substantially by patient characteristics that are not easily measureable, such as motivation, stamina, initiative, and affective states. Thus, it is not surprising that comparisons of short-term gains between treatment settings, using risk-adjusted FIM gain for example, lead to inconsistent results even for specific conditions, such as knee and hip joint replacement.23, 24
These limitations of extant outcome measures for rehabilitation suggest the need for a paradigm shift in how we measure rehabilitation outcomes to assess performance and for policy purposes.
22 Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Functional Measures,” A Study of Post-Acute Care Costs and Outcomes: Final Report, Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. December 28, 2006 d: 37–50. http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
23 DeJong, G., W. Tian, R.J. Smout, S.D. Horn, K. Putman, P. Smith, J. Gassaway, and J.E. DaVanzo. “Use of Rehabilitation and Other Health Care Services by Patients with Joint Replacement After Discharge from Skilled Nursing and Inpatient Rehabilitation Facilities.” Archives of Physical Medicine and Rehabilitation 90:1297–305, 2009.
24 Mallinson et al. “A Comparison of Discharge Functional Status After Rehabilitation in Skilled Nursing, Home Health, and Medical Rehabilitation Settings for Patients After Lower-Extremity Joint Replacement Surgery.” Archives of Physical Medicine and Rehabilitation 92:712–20, 2011.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 67
A Paradigm Shift in Rehabilitation Performance Measurement
FUNCTIONAL CHANGE OVER LONGER TERM FIXED INTERVALS
Longer-term functional outcomes, measured over fixed time intervals, are of greater value when assessing performance of rehabilitation care and for policy purposes. From a performance measurement perspective, short-term gains that may or may not be sustained are of less interest than sustained functional improvement. From a policy perspective, measures need to capture long-term and sustained functional gain rather than short-term and setting-specific change. Functional measures should cover multiple domains such as ADLs, IADLs, ambulation/mobility, and social/role function.25
As patients move across settings and may at some point return home with no care, individual provider assessments are both difficult to obtain, and actually become less relevant than patient (or proxy) reported function. Reported difficulty that patients experience in accomplishing activities such as bathing, dressing, ambulating specified distances, cooking, cleaning, and engaging in social and recreational activity are in fact what we hope to minimize with rehabilitation.26, 27
Patient’s (or proxy’s) perspectives are in fact the realities that patients experience. These define their limitations better than provider assessments of functional performance. Patient or proxy reports of function can be collected either in person or by
25 Kramer, A.M., D. Holthaus, G. Goodrich, and A. Epstein. “Functional Measures,” A Study of Post-Acute Care Costs and Outcomes: Final Report December 28, 2006 d : 37–50. http://aspe.hhs.gov/daltcp/reports/2006/strokePAC.htm
26 Kramer, A.M. “Rehabilitation Care and Outcomes from the Patient’s Perspective.” Medical Care 35(6):JS48–JS57, 1997.
27 Kramer, A.M. and E.A. Coleman. “Stroke Rehabilitation in Nursing Homes: How Do We Measure Quality?” Clinics in Geriatric Medicine 15(4):869–884, 1999.
telephone. They can be collected at fixed intervals regardless of the setting in which a patient is receiving care or even if they are no longer receiving rehabilitation at home but continuing to improve.
Such patient- or proxy-reported measures have been used successfully to compare rehabilitation outcomes between treatment settings28 and between systems of care such as HMOs vs. fee-for-service care.29, 30 In addition to measuring functional change following musculoskeletal and neurological events (e.g. hip fracture and stroke), similar measures have been used to assess rehabilitation outcomes after medical and surgical events, which are frequently treated in SNFs.31
RETURN TO THE COMMUNITY
A global measure of rehabilitation performance for post-acute patients that encompasses all of these domains is return to living in the community or to ones prior living situation.32 For a great many patients undergoing rehabilitation following acute events, returning to their prior living situation is the most important outcome. If they cannot return to their prior living situation, they are interested in returning to the most independent setting possible. While this seems like a gross measure of rehabilitation success, often very modest changes in function
28 Kramer et al. “Outcomes and Costs after Hip Fractures and Stroke: A Comparison of Rehabilitation Settings.” JAMA 277(5):396–404, 1997.
29 Kramer, A.M., J.C. Kowalsky, M. Lin, J. Grigsby, R. Hughes, and J.F. Steiner. “Outcome and Utilization Differences for Older Persons with Stroke in HMO and Fee-For-Service Systems.” Journal of the American Geriatrics Society 48(7):726–734, 2000.
30 Coleman, E.A., A.M. Kramer, J.C. Kowalsky, D.G. Eckhoff, M. Lin, E.J. Hester, N. Morgenstern, and J.F. Steiner. “A Comparison of Functional Outcomes after Hip Fracture in Group/Staff HMOs and Fee-for-Service Systems.” Effective Clinical Practice 3(5):229–239, 2000.
31 Johnson, M., A.M. Kramer, M. Lin, J. Kowalsky, and J. Steiner. “Outcomes of Older Persons Receiving Rehabilitation for Medical and Surgical Conditions Compared with Hip Fracture and Stroke.” Journal of the American Geriatrics Society 48(11):1389–1397, 2000.
32 MedPac 2011a.

2011 A N N UA L QUA L I T Y R EP O R T68
make it possible for patients to return to a more independent setting. Return to community can be assessed for a patient over time and across settings by contacting the patient or a proxy at regular intervals.
Clearly there are patient and social support factors that influence whether patients can return to their prior living situation from SNFs. Thus, risk adjustment is critical when comparing SNFs or examining trends over time. However, many of the risk factors are measureable and the models to predict likelihood of return to community are more predictive (c statistic =0.79) than models for more granular measures of functional recovery. Risk adjustment models are better in fact than the models used to predict acute events such as hospitalization33 or mortality for conditions like coronary artery bypass surgery, which are widely used for public reporting.
33 Min, S., R. Fish, A. Kramer. “Updates to SNF Quality Measures Risk Adjustment.” Division of Health Care Policy and Research, University of Colorado Denver. MedPAC, June 2010. www.medpac.gov/documents/Jun10_SNFRiskAdjustment_CONTRACTOR_CC.pdf
Community discharge in 100 days has been shown to be stable over time in SNFs with 25 admissions or more.34 Risk-adjusted rates of return to community from SNFs have been increasing gradually, averaging 36 percent in 2008.35 However, even after risk adjustment, wide variation exists across SNFs in rates of return to community (Table 4).
MedPAC has recommended using this SNF quality measure for payment incentives since currently there is no incentive for facilities to optimize rehabilitation and return residents to community or their prior living situation. Studies are needed relating to periods beyond the 100 days of the Medicare part A benefit to determine if patients continue to be discharged to community settings beyond 100 days, given that function continues to improve. If this is the case, continued coverage for rehabilitation services under Medicare part B should be strongly considered.
34 Donelan-McCall, N., T. Eilertsen, R. Fish, and A. Kramer. “Small Patient Population and Low Frequency Event Effects on Stability of SNF Quality Measures – Final Report.” MedPAC 2006. www.medpac.gov/chapters/Mar07_Ch03a.pdf
35 MedPAC 2011a.
SUBSTANTIAL VARIATION EXISTS AMONG ALL SNFs IN 2008 IN RISK-ADJUSTED PERCENT OF SNF ADMISSIONS DISCHARGED TO COMMUNITY
Percentile
10TH 50TH 90TH
Percent discharged to community 16.0% 35.2% 52.3%
Source: MedPAC 2011, table 7-5, page 157
TABLE 4

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 69
Conclusions And RecommendationsSkilled Nursing Facilities are clearly the largest provider of post-acute rehabilitation care and treat the most varied and disabled rehabilitation population. Rather than policy efforts in SNFs to constrain and limit the use of rehabilitation services, SNFs should be encouraged to optimize rehabilitation outcomes through a combination of good nursing, medical, and multidisciplinary therapy services. The benefits of investing in optimizing function and ultimately independence of living situation far outweigh the short-term costs of more intensive rehabilitation services.
A broader definition of rehabilitation in older persons is appropriate in contrast to the narrow focus on neurological and musculoskeletal events. Rehabilitation is an approach to care of older persons that focuses on maximizing recovery, or preserving and maintaining function and quality of life, in a holistic sense. SNFs need to be encouraged to approach every admitted resident from this perspective. This argues for continuing payment policy that provides incentives to deliver necessary rehabilitation services in addition to the nursing care that SNF patients require.
Restoration of function can take time; time that far exceeds the typical lengths of stay in any rehabilitation setting. As a result, post-acute care has gravitated to a system of multiple transfers to different levels of care. With this evolution, it is critical that measures of rehabilitation quality follow patients across these transitions over fixed time intervals rather than during individual stays.
Although granular, short-term, setting-specific functional data are necessary for clinicians to identify, treat, and monitor deficits, measures using these data are not optimal for performance measurement and policy decisions. Longer-term and more global measures of functional change in various domains, and return to prior living situation are recommended to track quality of rehabilitation care. To measure performance, these require following patients at fixed intervals over a minimum of three months, and even longer for some outcomes.
Thus, post-acute rehabilitation performance measurement requires a paradigm shift. This can be accomplished with patient- or proxy-reported function that can be obtained after rehabilitation discharge as function continues to change. Patient’s (or a proxy’s) perceived functional ability is arguably the most important viewpoint.
Rehabilitation is also about maintaining function at the highest possible level, where performance may be measured in maintaining capacities rather than the traditional focus on improvement. The alternative is gradual decline in conditioning and health that ultimately can lead to acute injury and the need for post-acute rehabilitation – a much less desirable cycle that characterizes much of our current acute-care oriented health care system.

2011 A N N UA L QUA L I T Y R EP O R T70
There are several
opportunities to enhance
the care and outcomes
of elderly nursing home
residents experiencing acute
health transitions while
reducing costs.
TRANSITIONAL CARE: Challenges and Opportunities FOR NURSING HOME RESIDENTS

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 71
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Katherine M. Abbott, PhD, MGS Karen B. Hirschman, PhD, MSW Mary D. Naylor, PhD, RN, FAAN
Appendix
TRANSITIONAL CARE: Challenges and Opportunities FOR NURSING HOME RESIDENTS

2011 A N N UA L QUA L I T Y R EP O R T72
In the U.S., older adults receiving care in
nursing homes experience frequent transitions
in health that often result in acute illnesses.
Age-related changes complicated by multiple
chronic conditions and frailty contribute to high
rates of acute hospitalizations for this population.1
In 2006, the hospitalization rate of all older
adults residing in nursing homes was 38 percent,
with 41 percent of this group having two or more
hospital admissions.2 That same year, 51 percent
of this population had at least one emergency
department visit and half of these residents
had two or more emergency department visits.
Hospitalizations among this vulnerable group
have been associated with poor health outcomes,
including accelerated cognitive and physical
functional decline and high rates of medical errors
and potentially avoidable rehospitalizations.3, 4
Fortunately, numerous studies reveal that there
are several opportunities to enhance the care
and outcomes for elderly nursing home residents
experiencing acute health transitions while
reducing costs.
1 Konetzka, R .T ., W . Spector, and M .R . Limcangco . Reducing hospitalizations from long-term care settings . Med Care Res Rev. 65(1):40–66, 2008 .
2 Jacobson, G ., T . Neuman, and A . Damico . Medicare spending and use of medical services for beneficiaries in nursing homes and other long-term care facilities: A Potential for Achieving Medicare Savings and Improving the Quality of Care .
3 http://www .kff .org/medicare/upload/8109 .pdf . Accessed December 1, 2010 .
4 Thompson, R .S ., N .K . Hall, and M . Szpiech . Hospitalization and mortality rates for nursing home-acquired pneumonia . Journal of Family Practice 48(4):291–293 . 1999 .
TRANSITIONAL CARE:
Challenges and Opportunities FOR NURSING HOME RESIDENTS

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 73
Current ChallengesInadequate transfer of relevant information poses a major barrier to high value care for some residents. Systematic communication of meaningful data between staff members in nursing home and acute care settings (emergency departments or hospitals) can contribute to substantial improvements in the delivery of person-centered care. Information regarding the unique functional needs of hospitalized residents or changes made in medication regimens would assist staff in both settings to more effectively and efficiently address individualized resident needs. Timely communication of treatment choices may help to prevent the use of aggressive and costly medical therapies when residents have chosen palliative care as the desired option.
Despite the increasing complexity of residents’ care needs, current quality and financial incentives have stifled the implementation of evidence-based delivery models that foster high value care for this population, especially during episodes of acute illness. Some nursing home staff members do not have the skills or easy access to health care providers who could prevent or identify early and manage acute problems. Clinicians in hospitals, for example, often focus on the acute problem but may not effectively address the long-term care needs of residents such as cognitive impairment that, if unaddressed, increase risk for adverse clinical events and complicate the recovery of those with such deficits.
Studies of care management approaches designed to address the health care challenges experienced by nursing home residents have demonstrated great promise in improving quality and reducing costs with similar high-risk groups. Findings from these studies suggest that between 30 percent to 67 percent of hospitalizations among elderly nursing home residents could be prevented with targeted
interventions.5, 6 Reports by many clinical and health services researchers who evaluated relevant care management innovations via federal (Program of All-Inclusive Care for Elders [PACE]), State (e.g., North Carolina, Vermont) and provider-led initiatives (e.g., Evercare Model) have informed our understanding of the unique needs of the frail elderly population, especially during common health transitions and highlighted the potential of avoiding preventable hospitalizations.7 In the Evercare Model, for example, nurse practitioners team with care managers to provide intensive primary care to older adults residing in nursing homes and other settings. A 25 percent reduction in hospitalizations for this population could have saved Medicare an estimated $2.1 billion in 2010.8 These analyses do not take into consideration additional savings that could be accrued from decreased emergency department visits.
Many health and long-term care leaders concur that effective transitional care is a core strategy to improve outcomes and decrease costs for those residents for whom hospitalizations are essential.9 Interventions targeting transitions from hospitals to homes have been the subject of 21 randomized clinical trials reported to date. A review of these studies yielded a wide range of successful innovative strategies, including comprehensive discharge planning and follow-up,
5 Fried, T.R., M.R. Gillick, and L.A. Lipsitz. Short-term functional outcomes of long-term care residents with pneumonia treated with and without hospital transfer. Journal of the American Geriatrics Society 45(3):302–306, 1997.
6 Saliba, D., R. Kington, J. Buchanan et al. Appropriateness of the decision to transfer nursing facility residents to the hospital. Journal of the American Geriatrics Society 48(2):154–163, 2000.
7 Grabowski, D.C., A.J. O’Malley, and N.R. Barhydt. The costs and potential savings associated with nursing home hospitalizations. Health Affairs (Millwood)26(6):1753–1761. 2007.
8 Jacobson, G., T. Neuman, and A. Damico. Medicare spending and use of medical services for beneficiaries in nursing homes and other long-term care facilities: A Potential for Achieving Medicare Savings and Improving the Quality of Care.
9 Konetzka, R.T., W. Spector, and M.R. Limcangco. Reducing hospitalizations from long-term care settings. Med Care Res Rev 65(1):40–66, 2008.

2011 A N N UA L QUA L I T Y R EP O R T74
coaching and redesigning discharge planning and case management.10 While none of the reviewed studies specifically examined the impact of transitional care on acutely ill nursing home residents, available evidence has helped us to understand core components of multidimensional interventions such as the need for improved cross-site communication and enhanced preparation of sending and receiving staff for their important role in avoiding gaps in care and promoting continuity of care to assure residents’ positive outcomes.
The most rigorously studied of the evidence-based approaches is the Transitional Care Model (TCM). The TCM, designed and tested by a multidisciplinary team at the University of Pennsylvania (Penn), focuses on the needs of high risk, community-based chronically ill older adults throughout episodes of acute illness. The model emphasizes identification of each older adult’s health goals and preferences; design, implementation and evaluation of a streamlined plan of care in collaboration with the older adult, family caregivers, physicians and other health team members; and, continuity of care throughout the entire episode provided by an advanced practice registered nurse (APRN). Three NIH funded randomized clinical trials (RCT) reported to date11, 12, 13 have consistently demonstrated the capacity of
10 Grabowski, D.C., A.J. O’Malley, and N.R. Barhydt. The costs and potential savings associated with nursing home hospitalizations. Health Affairs (Millwood) 26(6):1753–1761. 2007.
11 Naylor, M., D. Brooten, R. Jones et al. Comprehensive discharge planning for the hospitalized elderly. A randomized clinical trial. Ann Intern Med 120(12):999–1006, 1994.
12 Naylor, MD, D. Brooten, R. Campbell et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 281(7):613–620, 1999.
13 Naylor, MD, D.A. Brooten, R.L. Campbell et al. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. Journal of the American Geriatrics Society 52(5):675–684, 2004.
TCM derived interventions to improve health and quality of life outcomes, increase satisfaction and decrease health care costs among community-based cognitively intact older adults when compared to standard care.14 In the most recently reported RCT, for example, all-cause rehospitalization among older adults hospitalized for acute episode of heart failure were significantly reduced through one year post-index hospital discharge when compared to patients in the control group, at a mean savings of $5,000 per Medicare beneficiary.15 Recently, the Penn team reported preliminary findings from an on-going NIH-funded study revealing that a TCM intervention resulted in reductions in time to first readmission or death, all-cause rehospitalization rates and total hospital days among hospitalized, community-based, cognitively impaired older adults through six months post-index hospital discharge when compared to interventions of lower intensity.
The TCM used APRNs with advanced knowledge and skills in the care of the target population. Key elements of this APRN led, team-based model are:
■■ In-hospital assessment, preparation, and development of an evidenced-based plan of care;
■■ Regular home visits by the APRN with available, ongoing telephone support;
■■ Strong physician-nurse collaboration (accompanying patients to at least the first follow-up office visit);
■■ Comprehensive, holistic focus on each patient’s needs including the reason for the primary hospitalization as well as other complicating or coexisting events;
14 Naylor, MD, E.T. Kurtzman, and M.V. Pauly. Transitions of elders between long-term care and hospitals. Policy Polit Nurs Pract 10(3):187–194, 2009.
15 Naylor, MD, D.A. Brooten, R.L. Campbell et al. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. Journal of the American Geriatrics Society 52(5):675–684, 2004.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 75
■■ Active engagement and participation of patients and family caregivers;
■■ Emphasis on early identification and response to health care risks and symptoms to achieve longer term positive outcomes and avoid adverse and untoward events that lead to hospital readmissions;
■■ Multidisciplinary approach that includes the patient, family, and formal caregivers as part of a team;
■■ Effective communications to, between, and among the patient, family and informal caregivers, and health care providers and professionals.
On average, the model is initiated at hospital admission and continues for about two months following the index hospitalization, substituting for traditional visiting nurse service care. APRNs are available seven days per week (which includes at least weekly home visits during first month and at least weekly telephone outreach throughout the intervention), continually reassessing the patient’s status and the care plan with the patient, family caregiver and primary care clinicians. APRNs initiate at least monthly telephonic outreach to monitor patients’ progress. This approach to care has been successfully translated into practice, demonstrated positive health and cost outcomes for Medicare Advantage members.16
Adaptations of proven transitional care interventions such as the TCM to meet the unique needs of nursing home residents should be a high priority and will require the engagement and commitment of staff in hospitals as well as skilled and long-term care facilities. Such modifications should stress the opportunity to prevent unnecessary hospitalizations and to assure more effective and efficient transitions
16 Naylor, MD, K.H. Bowles, K.M. McCauley et al. High-value transitional care: translation of research into practice. J Eval Clin Pract. 2011.
between hospitals and nursing homes when such transfers are necessary. The unique challenges of caring for acutely ill older adults whose needs are complicated by cognitive impairment also will need to be highlighted . Additionally, a focus on palliative and hospice care will be central to effective and efficient transitional care solutions for this vulnerable population.
Policy RecommendationsThe responsibility to improve transitions for this population rests equally on the long-term and acute care settings. The following policy recommendations are intended to foster adaption of transitional care and strengthen the long-term care and acute care workforce to deliver these types of interventions.

2011 A N N UA L QUA L I T Y R EP O R T76
ADAPTATION OF EFFECTIVE TRANSITIONAL CARE INTERVENTIONS
Adaptation and testing of transitional care, such as the TCM, in the nursing home setting is essential to determine if such approaches could address aforementioned challenges. Interventions should be adapted based on known effectiveness of the intervention to achieve the desired outcomes (e.g., earlier access to palliative care, improved quality of life, decreased rehospitalization rates). Research is needed to determine which interventions are most suitable for this environment and to identify the groups of residents best served by these interventions (e.g., cognitively impaired, short-term or long-term residents). Additionally, robust performance measures of effective transitions and person-centered outcomes are needed to motivate the investment in such interventions coupled with the correct payment incentives.
WORKFORCE DEVELOPMENT
Preparation of the current and future hospital and long-term care workforce is necessary to provide effective transitional care. This includes not only a commitment at the organizational level (e.g., health care systems, nursing homes) but at the individual provider level (e.g., physicians, nurses, social workers, mental health professionals) to change care and outcomes for this population of elderly nursing home residents. Available evidence suggests that nurses – particularly those with advanced practice preparation – supported by a team of health professionals are best suited to take on the transitional care role between the acute and home care setting. Additionally, adaptation of transitional care will also require investment in knowledge and skill development of nurse assistants who often are the front line providers in nursing homes.

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 77
In summary, improving the quality of lives and reducing costs for the 1.5 million frail, elderly nursing home residents in the U.S. is a significant challenge.17 Nursing home residents are representative of a growing population of elderly recipients of long-term services in the U.S., currently estimated at 6.5 million and expected to double by 2050.18 Among nursing home residents in particular, hospitalizations are frequent, disruptive, costly and often associated with poor outcomes, including avoidable hospital readmissions. Many scholars and leaders in health and long-term care have identified transitional care as essential to simultaneously improving the quality of life for this population and achieving substantial health care savings.19, 20, 21
17 CDC. National Nursing Home Survey. June 2008; http://www.cdc.gov/nchs/about/major/nnhsd/ResidentTables_Estimates.htm#Demographics. Accessed February 24, 2008, 2009.
18 CDC. National Nursing Home Survey. June 2008; http://www.cdc.gov/nchs/about/major/nnhsd/ResidentTables_Estimates.htm#Demographics. Accessed February 24, 2008, 2009.
19 Konetzka, R.T., W. Spector, and M.R. Limcangco. Reducing hospitalizations from long-term care settings. Med Care Res Rev 65(1):40–66. 2008.
20 Grabowski, D.C., A.J. O’Malley, and N.R. Barhydt. The costs and potential savings associated with nursing home hospitalizations. Health Aff (Millwood) 26(6):1753–1761. 2007.
21 Medicare Payment Advisory Commission. Payment policy for inpatient readmission. Report to Congress: Promoting Greater Efficiency in Medicare. Washington, DC: MedPAC; 2007.
Transitional care approaches, proven successful in achieving these goals for other similar populations, should be made accessible to benefit nursing home residents and are critical to assuring high value care for our society.

2011 A N N UA L QUA L I T Y R EP O R T78
Appendix

A CO M P R EH EN S I V E R EP O R T O N T H E QUA L I T Y O F C A R E 79
Executive Summary
Next Steps in Nursing Home Quality Measurement: Adapting to a Changing Patient Population and Health System Change
Quality Trends: By the Numbers
Special Update: Advancing Excellence in America’s Nursing Homes
Hospitalization of Nursing Home Residents
Focus on Rehabilitation Measures
Transitional Care: Challenges and Opportunities for Nursing Home Residents
Appendix
Appendix

2011 A N N UA L QUA L I T Y R EP O R T80
ADL Pain High Risk Pressure Ulcer Low Risk Pressure Ulcer Incontinence Indwelling Catheter Bedfast
US avg. 14.3% 13.9% 0.4% 2.5% 3.4% 3.2% 0.1% 4.2% 10.9% 10.3% 0.5% 5.0% 1.9% 1.8% 0.1% 5.3% 50.7% 51.6% -1.0% -1.9% 5.1% 4.8% 0.3% 5.2% 4.0% 3.9% 0.1% 1.9%
AK 13.8% 13.8% 0.0% 0.0% 5.0% 5.7% -0.7% -13.3% 8.2% 6.6% 1.6% 19.5% 2.5% 10.0% -7.5% -300.0% 52.6% 55.2% -2.6% -4.9% 7.2% 7.3% -0.1% -1.9% 6.4% 5.7% 0.7% 11.5%
AL 11.2% 9.6% 1.6% 13.9% 2.0% 1.8% 0.3% 12.9% 9.2% 9.1% 0.1% 1.1% 1.1% 1.5% -0.3% -29.8% 48.0% 48.3% -0.3% -0.6% 4.2% 3.7% 0.6% 13.0% 6.2% 6.2% 0.0% 0.4%
AR 13.0% 13.8% -0.8% -6.1% 2.4% 2.0% 0.4% 18.0% 9.7% 9.2% 0.6% 5.9% 1.6% 1.6% 0.0% 1.3% 42.0% 43.1% -1.1% -2.6% 4.8% 4.4% 0.4% 8.0% 3.8% 3.7% 0.1% 2.4%
AZ 13.2% 12.2% 1.0% 7.8% 4.4% 4.8% -0.4% -8.5% 9.7% 9.9% -0.2% -2.4% 2.6% 2.1% 0.5% 19.0% 53.6% 53.5% 0.1% 0.2% 6.0% 5.6% 0.4% 6.5% 3.6% 4.4% -0.8% -21.9%
CA 10.3% 10.4% -0.1% -0.9% 3.8% 3.6% 0.2% 4.0% 12.6% 11.6% 1.0% 7.7% 1.8% 1.5% 0.3% 14.4% 57.4% 57.7% -0.3% -0.5% 4.4% 4.1% 0.3% 6.3% 5.2% 5.1% 0.1% 1.7%
CO 14.8% 13.8% 1.0% 6.9% 3.3% 3.1% 0.3% 8.0% 8.1% 7.6% 0.5% 6.3% 1.5% 1.6% -0.1% -5.3% 46.6% 48.1% -1.5% -3.1% 6.7% 6.8% -0.0% -0.5% 1.9% 1.9% -0.0% -1.7%
CT 15.4% 14.8% 0.6% 3.9% 2.3% 2.3% 0.0% 2.1% 8.6% 8.3% 0.3% 3.4% 1.4% 1.3% 0.0% 0.7% 51.1% 51.6% -0.4% -0.8% 3.9% 3.7% 0.2% 5.1% 2.2% 2.1% 0.1% 4.3%
DC 11.6% 11.9% -0.3% -2.2% 0.6% 0.6% -0.0% -4.6% 11.6% 11.8% -0.2% -1.8% 0.9% 0.6% 0.3% 34.7% 53.9% 57.4% -3.5% -6.5% 2.3% 2.9% -0.6% -27.2% 1.6% 2.1% -0.6% -35.5%
DE 14.0% 16.9% -2.9% -20.8% 2.6% 2.5% 0.1% 4.3% 8.9% 10.1% -1.2% -13.8% 2.8% 2.4% 0.4% 13.8% 51.3% 51.1% 0.1% 0.2% 3.8% 3.4% 0.4% 9.4% 3.5% 4.4% -0.9% -27.3%
FL 12.1% 11.4% 0.6% 5.3% 2.8% 2.4% 0.4% 15.3% 12.0% 11.6% 0.5% 4.0% 2.5% 2.2% 0.3% 12.8% 52.8% 53.4% -0.6% -1.2% 4.9% 4.6% 0.3% 5.6% 4.2% 4.0% 0.2% 4.3%
GA 13.7% 12.6% 1.1% 8.2% 3.7% 3.1% 0.6% 15.7% 10.4% 10.1% 0.3% 3.2% 1.6% 1.6% 0.1% 3.3% 51.3% 51.8% -0.5% -1.0% 3.7% 3.4% 0.3% 8.8% 7.0% 6.8% 0.2% 2.4%
HI 10.8% 10.8% 0.1% 0.7% 1.8% 2.4% -0.6% -36.1% 6.7% 7.3% -0.6% -9.1% 1.8% 1.5% 0.3% 16.7% 62.8% 61.2% 1.7% 2.6% 2.3% 2.8% -0.5% -20.6% 6.3% 5.2% 1.1% 17.8%
IA 12.8% 13.6% -0.9% -6.9% 3.5% 3.6% -0.1% -4.2% 7.5% 7.2% 0.3% 3.9% 2.0% 2.4% -0.4% -20.4% 44.3% 45.3% -1.0% -2.2% 6.7% 5.9% 0.8% 11.6% 1.2% 1.1% 0.1% 5.1%
ID 11.2% 13.2% -2.0% -17.8% 4.3% 4.5% -0.2% -4.3% 8.2% 6.8% 1.4% 17.0% 0.0% 0.8% -0.8% N/A 55.7% 58.5% -2.7% -4.9% 7.2% 6.3% 0.9% 12.2% 2.5% 2.8% -0.3% -13.9%
IL 13.5% 13.9% -0.4% -3.2% 3.9% 3.9% -0.0% -0.0% 13.3% 12.3% 1.0% 7.3% 2.0% 1.8% 0.2% 8.4% 42.2% 44.4% -2.2% -5.2% 5.1% 4.9% 0.2% 3.3% 2.0% 2.0% 0.0% 1.4%
IN 20.5% 19.9% 0.6% 3.1% 2.7% 2.6% 0.1% 4.7% 10.0% 9.3% 0.7% 6.6% 1.7% 1.5% 0.1% 8.2% 49.6% 50.6% -1.0% -2.1% 5.7% 5.3% 0.4% 7.0% 2.9% 3.0% -0.1% -4.0%
KS 14.5% 13.4% 1.2% 8.0% 3.7% 3.8% -0.1% -1.6% 9.0% 8.1% 0.9% 9.8% 1.9% 1.8% 0.2% 9.8% 43.1% 44.5% -1.4% -3.3% 5.4% 5.0% 0.4% 7.0% 1.6% 1.7% -0.1% -6.1%
KY 16.2% 15.9% 0.3% 1.9% 3.3% 2.6% 0.7% 21.3% 10.8% 9.8% 1.0% 8.9% 2.3% 1.6% 0.7% 29.7% 51.1% 52.5% -1.4% -2.7% 6.2% 5.8% 0.4% 6.1% 7.6% 7.2% 0.4% 4.8%
LA 19.5% 19.5% -0.0% -0.0% 3.6% 3.5% 0.2% 4.2% 15.6% 14.2% 1.4% 8.7% 1.9% 1.5% 0.4% 18.9% 41.4% 42.0% -0.6% -1.5% 5.6% 5.0% 0.6% 11.4% 8.4% 7.7% 0.8% 9.0%
MA 12.5% 12.2% 0.4% 2.8% 1.8% 1.7% 0.1% 4.1% 9.1% 8.5% 0.6% 6.1% 1.5% 1.3% 0.2% 11.5% 63.0% 63.5% -0.5% -0.8% 4.4% 4.3% 0.1% 2.1% 1.9% 1.9% 0.0% 0.5%
MD 13.4% 13.9% -0.5% -3.9% 1.4% 1.5% -0.2% -13.4% 12.2% 11.4% 0.7% 6.2% 2.1% 1.8% 0.2% 11.6% 57.0% 59.0% -1.9% -3.4% 3.7% 3.4% 0.3% 9.3% 5.4% 5.5% -0.1% -1.7%
ME 14.7% 14.7% 0.0% 0.2% 3.4% 3.3% 0.2% 5.4% 8.8% 8.1% 0.7% 7.8% 0.0% N/A N/A N/A 70.0% 69.9% 0.1% 0.1% 6.1% 5.0% 1.0% 17.3% 4.9% 5.1% -0.3% -5.7%
MI 12.3% 11.9% 0.3% 2.8% 3.0% 3.1% -0.1% -2.4% 9.3% 9.7% -0.4% -4.3% 1.6% 1.6% -0.1% -4.0% 52.5% 53.1% -0.7% -1.3% 4.8% 4.8% 0.0% 0.5% 3.1% 3.1% 0.0% 1.2%
MN 14.5% 13.5% 1.0% 6.6% 3.4% 3.4% -0.0% -1.4% 6.5% 6.9% -0.4% -6.2% 1.2% 2.1% -0.8% -66.6% 52.8% 54.3% -1.5% -2.8% 5.8% 5.7% 0.1% 1.9% 1.2% 1.3% -0.0% -2.6%
MO 11.7% 11.2% 0.5% 4.2% 3.7% 3.8% -0.1% -1.6% 11.4% 9.6% 1.8% 15.9% 2.0% 1.9% 0.0% 0.2% 36.5% 39.0% -2.5% -6.9% 4.8% 4.7% 0.1% 2.3% 1.9% 1.7% 0.2% 10.7%
MS 15.2% 13.9% 1.3% 8.3% 3.0% 3.4% -0.4% -11.7% 11.2% 11.2% -0.1% -0.6% 1.1% 1.1% -0.1% -5.1% 48.0% 49.7% -1.7% -3.5% 4.0% 3.7% 0.3% 7.9% 8.4% 7.9% 0.5% 5.6%
MT 14.2% 14.4% -0.2% -1.6% 4.2% 4.2% 0.1% 1.3% 7.1% 7.3% -0.2% -2.7% 1.9% 1.1% 0.8% 44.4% 48.0% 51.2% -3.3% -6.8% 6.8% 6.7% 0.1% 1.7% 2.4% 2.4% 0.0% 1.2%
NC 21.4% 19.6% 1.8% 8.4% 2.6% 2.4% 0.2% 8.0% 10.4% 10.5% -0.1% -0.9% 1.8% 2.1% -0.4% -21.2% 57.9% 60.4% -2.5% -4.4% 4.1% 4.0% 0.1% 2.6% 8.1% 7.9% 0.2% 3.0%
ND 15.2% 15.9% -0.6% -4.3% 3.5% 4.0% -0.6% -15.8% 6.2% 8.2% -2.0% -31.8% 1.5% 2.5% -1.0% -66.7% 45.5% 47.0% -1.4% -3.1% 7.1% 7.1% -0.0% -0.4% 1.9% 2.1% -0.2% -11.7%
NE 14.3% 13.3% 1.0% 7.1% 3.8% 3.7% 0.2% 4.7% 6.6% 6.6% 0.0% 0.4% 2.2% 2.2% 0.0% 0.6% 47.6% 48.7% -1.1% -2.3% 7.8% 7.1% 0.7% 8.9% 1.3% 1.4% -0.2% -12.0%
NH 17.1% 16.6% 0.5% 2.8% 2.5% 2.9% -0.3% -12.5% 7.4% 7.2% 0.3% 3.5% 2.6% 2.3% 0.3% 11.6% 52.3% 52.5% -0.1% -0.3% 5.8% 5.8% -0.0% -0.6% 2.5% 2.8% -0.4% -15.2%
NJ 11.2% 12.8% -1.6% -14.1% 1.9% 2.0% -0.1% -4.4% 14.9% 14.6% 0.3% 1.8% 2.4% 2.3% 0.1% 2.3% 46.2% 47.1% -0.9% -2.0% 4.2% 4.1% 0.1% 1.4% 2.8% 3.1% -0.4% -13.9%
NM 16.7% 13.5% 3.2% 19.3% 4.7% 3.2% 1.6% 33.5% 10.1% 9.2% 0.9% 9.0% 1.8% 1.6% 0.3% 15.8% 52.7% 53.6% -0.9% -1.7% 4.7% 4.6% 0.0% 0.9% 1.9% 1.7% 0.3% 13.3%
NV 18.9% 16.4% 2.5% 13.1% 4.0% 4.1% -0.1% -2.2% 12.0% 11.4% 0.6% 5.2% 1.7% 1.9% -0.2% -13.3% 53.9% 54.9% -1.0% -1.9% 6.4% 6.3% 0.1% 1.5% 8.7% 8.5% 0.2% 1.9%
NY 14.0% 13.3% 0.7% 5.1% 2.3% 2.2% 0.1% 4.5% 12.7% 12.0% 0.8% 6.0% 2.0% 1.8% 0.2% 10.7% 52.5% 53.5% -1.0% -1.8% 4.4% 4.1% 0.3% 6.2% 1.8% 1.8% 0.0% 0.5%
OH 12.9% 12.2% 0.7% 5.6% 5.3% 4.6% 0.7% 13.9% 10.3% 9.9% 0.4% 4.3% 1.6% 1.5% 0.0% 3.0% 46.7% 48.0% -1.3% -2.7% 6.1% 5.8% 0.3% 4.7% 4.2% 4.1% 0.1% 2.0%
OK 12.3% 11.9% 0.4% 3.2% 5.1% 4.9% 0.2% 3.4% 13.9% 12.1% 1.9% 13.6% 2.9% 1.8% 1.1% 38.0% 40.2% 40.8% -0.6% -1.6% 5.4% 5.1% 0.3% 5.8% 5.5% 5.4% 0.2% 3.2%
OR 9.3% 9.9% -0.7% -7.3% 4.3% 4.8% -0.6% -13.3% 10.9% 9.4% 1.5% 13.7% 3.8% 3.5% 0.2% 6.7% 58.4% 59.7% -1.3% -2.2% 8.0% 7.5% 0.5% 6.6% 6.9% 7.0% -0.1% -1.8%
PA 18.0% 17.4% 0.5% 2.9% 3.0% 3.0% 0.1% 2.4% 10.4% 9.9% 0.4% 4.3% 1.8% 2.0% -0.1% -6.5% 62.8% 63.0% -0.2% -0.4% 5.1% 4.8% 0.3% 5.2% 3.2% 3.0% 0.2% 6.2%
RI 14.4% 12.4% 2.0% 14.1% 2.1% 1.8% 0.3% 12.0% 11.1% 8.5% 2.5% 23.0% 2.0% 2.4% -0.4% -20.1% 45.8% 46.8% -1.1% -2.3% 4.0% 4.0% -0.0% -0.3% 1.9% 2.0% -0.1% -3.2%
SC 12.8% 12.2% 0.6% 5.0% 1.8% 1.8% -0.1% -3.5% 11.5% 10.8% 0.6% 5.5% 2.1% 2.3% -0.1% -6.3% 62.5% 62.9% -0.4% -0.6% 3.2% 3.1% 0.1% 3.6% 5.4% 5.5% -0.1% -1.9%
SD 14.9% 15.0% -0.1% -0.4% 3.7% 3.6% 0.2% 4.3% 7.4% 7.4% -0.0% -0.0% 2.4% 1.9% 0.5% 22.3% 48.6% 49.8% -1.2% -2.5% 7.1% 6.8% 0.3% 4.9% 1.4% 1.5% -0.1% -7.5%
TN 11.7% 12.2% -0.5% -4.3% 2.5% 2.1% 0.3% 13.6% 10.4% 10.1% 0.3% 2.5% 1.5% 1.1% 0.4% 27.5% 48.9% 49.4% -0.5% -1.0% 4.9% 4.5% 0.4% 8.7% 6.4% 6.0% 0.4% 6.1%
TX 18.4% 18.0% 0.4% 2.3% 3.8% 3.8% 0.0% 1.0% 11.9% 11.4% 0.5% 3.8% 1.7% 1.6% 0.0% 1.3% 46.8% 47.1% -0.4% -0.8% 4.4% 4.4% 0.1% 1.3% 5.4% 5.1% 0.3% 5.8%
UT 12.6% 14.6% -2.0% -15.9% 9.9% 8.6% 1.3% 13.5% 9.0% 8.7% 0.3% 3.8% 3.8% 1.5% 2.3% 60.0% 54.4% 51.5% 2.8% 5.2% 7.1% 6.4% 0.6% 9.1% 3.2% 3.3% -0.1% -3.5%
VA 16.6% 16.6% -0.0% -0.1% 2.4% 2.1% 0.3% 12.5% 11.7% 10.7% 0.9% 8.0% 1.4% 1.8% -0.4% -25.1% 58.7% 59.1% -0.5% -0.8% 4.1% 3.9% 0.2% 4.4% 5.3% 5.6% -0.2% -4.6%
VT 16.0% 15.5% 0.5% 2.8% 3.1% 3.8% -0.6% -20.2% 8.3% 7.7% 0.5% 6.6% 2.3% 3.0% -0.7% -28.6% 58.1% 60.7% -2.7% -4.6% 7.8% 6.4% 1.4% 17.8% 5.2% 4.5% 0.7% 13.5%
WA 11.9% 10.0% 1.9% 16.1% 4.5% 4.8% -0.3% -6.4% 11.4% 10.4% 1.0% 9.2% 1.8% 2.1% -0.3% -18.5% 59.2% 59.2% -0.0% -0.0% 7.3% 7.0% 0.3% 3.6% 5.2% 5.3% -0.0% -0.5%
WI 14.3% 13.7% 0.6% 4.0% 3.5% 3.6% -0.1% -3.2% 8.8% 8.1% 0.7% 8.2% 2.2% 2.3% -0.1% -4.9% 48.4% 50.1% -1.7% -3.5% 6.8% 6.5% 0.3% 4.4% 1.8% 1.9% -0.1% -3.1%
WV 16.8% 16.9% -0.1% -0.7% 2.9% 2.8% 0.1% 4.1% 11.4% 11.2% 0.2% 1.4% 2.3% 2.3% 0.0% 0.1% 55.2% 55.7% -0.5% -0.9% 5.8% 5.5% 0.2% 4.3% 6.5% 6.6% -0.1% -0.9%
WY 14.3% 13.1% 1.2% 8.7% 4.7% 4.4% 0.3% 6.5% 8.3% 6.1% 2.2% 26.7% 1.7% 1.9% -0.2% -14.0% 42.6% 46.8% -4.1% -9.7% 7.4% 6.5% 0.9% 11.6% 1.7% 1.8% -0.1% -3.3%
APPENDIX 1
CMS NURSING FACILITY AVERAGE QUALITY MEASURE SCORES BY STATE
Stat
e
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence

A Co m p r eh en s i v e r ep o r t o n t h e QuA l i t y o f C A r e iv
locomotion uti Depression physical restraint pAC Delirum pAC pain pAC pressure ulcer Weight loss
US avg. 10.9% 10.7% 0.2% 2.1% 9.1% 9.0% 0.1% 1.3% 14.4% 14.1% 0.3% 1.9% 3.3% 2.6% 0.6% 19.9% 1.4% 1.2% 0.2% 15.6% 19.4% 19.1% 0.3% 1.4% 12.9% 11.8% 1.1% 8.7% 7.5% 7.4% 0.0% 0.5%
AK 7.0% 11.6% -4.6% -65.7% 4.8% 8.0% -3.2% -66.7% 12.2% 12.7% -0.5% -3.8% 0.8% 0.8% -0.0% -4.2% 1.5% 2.3% -0.8% -55.6% 34.3% 28.0% 6.3% 18.2% 17.3% 14.0% 3.3% 19.2% 9.2% 8.0% 1.2% 13.0%
AL 8.6% 8.0% 0.6% 6.7% 7.7% 7.0% 0.7% 9.6% 8.4% 8.5% -0.1% -1.2% 1.8% 1.4% 0.4% 23.6% 0.8% 0.7% 0.1% 12.6% 14.6% 13.8% 0.9% 5.9% 12.6% 11.7% 0.9% 7.2% 7.4% 7.7% -0.3% -4.0%
AR 10.1% 10.7% -0.6% -5.9% 8.3% 6.9% 1.4% 16.4% 9.7% 8.9% 0.8% 8.6% 4.2% 3.3% 1.0% 23.4% 1.4% 1.1% 0.4% 25.5% 13.1% 11.4% 1.8% 13.5% 11.5% 10.0% 1.5% 13.0% 6.9% 6.5% 0.4% 5.5%
AZ 10.0% 8.7% 1.3% 12.8% 9.8% 8.9% 0.9% 9.5% 12.2% 12.0% 0.2% 1.2% 2.1% 1.5% 0.7% 31.9% 1.2% 1.1% 0.1% 7.7% 26.4% 28.3% -1.9% -7.1% 11.3% 10.4% 0.9% 8.0% 6.7% 6.5% 0.2% 3.2%
CA 8.8% 9.2% -0.5% -5.3% 7.9% 7.6% 0.3% 4.1% 9.2% 9.0% 0.3% 2.8% 6.6% 5.1% 1.6% 23.4% 0.6% 0.5% 0.1% 10.8% 24.5% 23.9% 0.6% 2.4% 18.3% 17.0% 1.3% 7.3% 6.4% 6.3% 0.1% 1.1%
CO 10.5% 10.4% 0.1% 1.2% 8.5% 8.7% -0.1% -1.6% 15.7% 15.0% 0.7% 4.5% 3.4% 2.4% 1.0% 30.7% 1.7% 1.0% 0.7% 41.5% 22.3% 22.0% 0.3% 1.1% 9.7% 8.4% 1.2% 12.8% 8.0% 7.3% 0.7% 8.5%
CT 13.0% 11.3% 1.8% 13.6% 7.4% 7.0% 0.4% 5.8% 12.1% 10.8% 1.3% 10.8% 2.3% 1.7% 0.6% 25.0% 1.4% 1.2% 0.2% 13.7% 19.3% 19.9% -0.6% -3.0% 12.6% 11.1% 1.5% 12.0% 7.5% 7.3% 0.2% 2.4%
DC 7.6% 8.2% -0.5% -7.1% 6.0% 6.9% -0.9% -15.7% 6.9% 5.7% 1.2% 17.8% 1.8% 1.4% 0.4% 22.7% 1.0% 1.5% -0.5% -46.7% 10.1% 10.7% -0.5% -5.3% 14.2% 12.5% 1.7% 12.0% 7.7% 6.4% 1.3% 17.4%
DE 13.1% 10.9% 2.2% 16.9% 10.1% 9.8% 0.4% 3.6% 11.5% 12.2% -0.6% -5.5% 1.4% 1.2% 0.2% 13.1% 0.9% 0.6% 0.4% 39.7% 20.1% 17.4% 2.8% 13.7% 10.2% 10.1% 0.0% 0.3% 7.1% 8.2% -1.1% -15.7%
FL 8.9% 8.4% 0.5% 5.8% 11.0% 10.9% 0.0% 0.4% 9.7% 9.7% -0.0% -0.3% 4.3% 3.4% 0.9% 20.9% 1.0% 0.8% 0.2% 19.5% 18.9% 17.3% 1.7% 8.8% 15.4% 13.7% 1.7% 10.9% 8.0% 8.1% -0.0% -0.6%
GA 10.1% 8.8% 1.2% 12.4% 9.7% 9.2% 0.4% 4.3% 15.1% 14.5% 0.6% 4.1% 3.2% 2.2% 1.0% 31.1% 2.1% 1.6% 0.4% 21.1% 16.7% 15.3% 1.3% 8.1% 12.9% 11.5% 1.4% 10.5% 8.3% 8.0% 0.3% 4.0%
HI 12.5% 12.6% -0.1% -1.0% 6.3% 6.2% 0.1% 1.6% 11.5% 12.1% -0.6% -5.1% 2.1% 1.6% 0.5% 22.1% 1.6% 0.8% 0.8% 51.1% 16.5% 19.3% -2.8% -16.9% 11.2% 9.8% 1.4% 12.5% 7.7% 6.7% 1.1% 13.8%
IA 9.9% 9.7% 0.2% 1.9% 9.6% 9.4% 0.2% 1.6% 16.6% 16.6% -0.1% -0.4% 1.3% 1.3% 0.0% 1.8% 2.9% 2.8% 0.0% 1.2% 25.8% 24.3% 1.5% 5.8% 10.5% 8.4% 2.1% 19.9% 5.4% 5.6% -0.2% -3.8%
ID 8.5% 8.5% 0.0% 0.1% 10.0% 8.9% 1.1% 11.4% 17.5% 15.2% 2.3% 13.0% 3.1% 2.3% 0.8% 26.6% 3.1% 2.1% 1.0% 33.1% 30.7% 30.6% 0.1% 0.4% 10.5% 9.4% 1.1% 10.3% 8.7% 8.7% 0.0% 0.0%
IL 10.9% 11.1% -0.2% -1.4% 8.5% 9.1% -0.6% -7.5% 15.4% 16.5% -1.1% -7.0% 3.2% 2.8% 0.4% 12.8% 2.0% 1.7% 0.3% 15.8% 20.1% 19.1% 1.0% 4.8% 13.8% 12.2% 1.6% 11.3% 8.4% 8.6% -0.2% -2.6%
IN 12.2% 12.8% -0.7% -5.4% 8.8% 9.2% -0.4% -4.0% 15.7% 16.0% -0.3% -1.9% 2.6% 2.0% 0.6% 22.7% 0.8% 0.7% 0.0% 4.9% 17.0% 17.7% -0.7% -3.9% 9.5% 8.8% 0.7% 7.8% 7.3% 7.7% -0.3% -4.4%
KS 10.7% 9.8% 0.8% 7.8% 10.1% 10.1% 0.0% 0.5% 16.9% 16.7% 0.2% 1.2% 0.7% 0.6% 0.1% 16.0% 1.9% 2.2% -0.4% -18.6% 18.0% 18.2% -0.2% -1.3% 11.7% 9.5% 2.2% 18.4% 7.1% 7.6% -0.5% -7.7%
KY 11.4% 11.8% -0.4% -3.8% 11.5% 10.9% 0.6% 4.9% 18.4% 16.5% 1.9% 10.1% 5.1% 4.2% 0.9% 18.5% 0.6% 0.6% 0.0% 8.0% 17.0% 16.6% 0.4% 2.2% 11.1% 10.3% 0.8% 7.2% 9.3% 8.6% 0.8% 8.2%
LA 9.5% 9.2% 0.3% 3.4% 10.1% 10.4% -0.3% -3.0% 15.5% 14.3% 1.2% 7.5% 6.9% 6.1% 0.8% 12.2% 2.3% 2.4% -0.0% -0.5% 13.8% 14.1% -0.4% -2.6% 13.8% 12.4% 1.4% 10.4% 8.1% 8.4% -0.3% -3.5%
MA 11.8% 11.8% 0.0% 0.2% 8.8% 8.6% 0.1% 1.4% 14.5% 14.2% 0.3% 1.8% 3.5% 2.8% 0.6% 18.5% 1.4% 1.2% 0.2% 16.5% 18.4% 18.8% -0.5% -2.6% 12.2% 11.2% 1.0% 8.5% 6.3% 6.2% 0.1% 1.8%
MD 11.2% 11.1% 0.2% 1.5% 8.9% 8.6% 0.2% 2.4% 9.1% 9.1% 0.0% 0.5% 2.4% 1.9% 0.5% 21.4% 1.0% 0.8% 0.2% 19.8% 13.3% 14.1% -0.8% -6.1% 13.5% 12.3% 1.3% 9.3% 7.6% 7.7% -0.2% -2.1%
ME 14.6% 15.4% -0.8% -5.5% 8.6% 8.1% 0.5% 5.4% 30.9% 31.1% -0.1% -0.5% 0.9% 0.5% 0.4% 43.3% 1.8% 0.9% 0.8% 47.5% 23.9% 25.5% -1.6% -6.9% 11.7% 8.8% 2.9% 24.5% 8.7% 8.4% 0.3% 4.0%
MI 9.7% 9.3% 0.4% 4.2% 9.0% 8.6% 0.4% 4.4% 13.1% 13.1% 0.0% 0.1% 3.5% 3.3% 0.2% 6.8% 1.7% 1.2% 0.4% 26.6% 19.7% 20.6% -0.9% -4.6% 10.5% 10.0% 0.5% 4.7% 7.8% 7.8% -0.1% -1.1%
MN 11.2% 10.4% 0.8% 7.4% 6.8% 6.6% 0.2% 2.3% 23.3% 22.5% 0.7% 3.2% 1.5% 1.3% 0.2% 13.9% 1.4% 1.2% 0.2% 14.0% 22.1% 24.3% -2.2% -9.9% 8.7% 8.1% 0.6% 6.7% 7.0% 7.4% -0.4% -5.9%
MO 8.7% 8.6% 0.1% 0.9% 8.9% 9.0% -0.1% -0.7% 10.5% 10.4% 0.1% 0.7% 3.0% 2.2% 0.8% 25.9% 2.1% 2.0% 0.1% 6.1% 19.8% 18.8% 1.0% 5.0% 10.5% 9.6% 1.0% 9.1% 6.7% 6.5% 0.2% 2.9%
MS 10.6% 9.9% 0.7% 6.2% 9.0% 9.5% -0.4% -4.8% 13.4% 13.2% 0.2% 1.4% 5.8% 5.6% 0.1% 2.4% 1.5% 1.0% 0.5% 34.1% 13.4% 14.1% -0.7% -5.0% 11.1% 11.4% -0.3% -2.9% 8.4% 7.4% 1.0% 12.3%
MT 10.8% 11.3% -0.5% -4.5% 8.2% 8.5% -0.3% -3.2% 18.0% 16.5% 1.5% 8.2% 1.9% 1.3% 0.6% 30.1% 2.1% 1.7% 0.4% 17.8% 29.5% 34.5% -5.0% -17.1% 11.4% 9.3% 2.1% 18.3% 8.8% 7.8% 0.9% 10.6%
NC 12.4% 11.7% 0.7% 5.3% 10.8% 10.8% -0.0% -0.1% 15.5% 14.5% 1.0% 6.2% 3.1% 2.4% 0.7% 22.9% 1.3% 1.1% 0.2% 17.8% 17.0% 16.2% 0.8% 4.7% 11.0% 9.5% 1.5% 13.9% 9.2% 9.2% -0.0% -0.3%
ND 11.0% 11.7% -0.6% -5.8% 7.8% 7.9% -0.1% -1.5% 22.7% 24.0% -1.3% -5.6% 1.3% 1.1% 0.1% 11.6% 3.3% 1.6% 1.7% 51.7% 24.7% 30.0% -5.4% -21.7% 10.8% 12.1% -1.2% -11.2% 7.6% 8.3% -0.8% -10.1%
NE 11.7% 11.1% 0.5% 4.6% 8.5% 8.3% 0.3% 3.0% 19.0% 18.6% 0.4% 2.0% 1.1% 0.9% 0.2% 15.4% 2.7% 2.1% 0.6% 22.7% 22.6% 21.5% 1.1% 5.0% 9.7% 9.3% 0.4% 4.4% 6.2% 6.2% -0.0% -0.1%
NH 13.3% 15.2% -1.9% -14.2% 8.5% 8.2% 0.3% 3.6% 19.5% 18.3% 1.2% 6.2% 1.1% 0.5% 0.6% 51.4% 1.5% 1.0% 0.4% 29.2% 22.6% 23.5% -0.9% -4.1% 10.7% 9.6% 1.1% 10.2% 7.0% 7.5% -0.5% -7.1%
NJ 9.1% 9.9% -0.8% -8.5% 7.2% 7.8% -0.6% -8.2% 9.0% 9.9% -1.0% -10.7% 3.1% 2.9% 0.2% 7.3% 0.7% 0.6% 0.0% 6.3% 14.3% 14.0% 0.3% 1.8% 17.6% 16.1% 1.5% 8.4% 8.3% 8.0% 0.3% 3.9%
NM 12.6% 10.3% 2.3% 18.2% 8.4% 9.5% -1.2% -14.2% 13.3% 10.1% 3.2% 23.8% 3.7% 2.9% 0.7% 20.3% 0.7% 1.0% -0.3% -41.6% 22.7% 22.1% 0.7% 2.9% 10.6% 9.6% 1.1% 10.0% 8.9% 8.4% 0.5% 5.3%
NV 16.3% 14.5% 1.9% 11.4% 9.6% 10.4% -0.8% -8.8% 12.5% 11.7% 0.8% 6.3% 3.2% 2.5% 0.8% 24.1% 1.5% 0.9% 0.6% 39.3% 22.0% 22.1% -0.0% -0.1% 14.1% 12.3% 1.8% 12.7% 8.4% 7.4% 1.0% 11.8%
NY 12.4% 11.9% 0.4% 3.5% 7.8% 7.5% 0.3% 3.7% 13.2% 12.6% 0.5% 4.0% 2.7% 2.3% 0.3% 12.5% 1.0% 0.9% 0.2% 15.5% 14.8% 15.1% -0.3% -1.7% 15.8% 14.8% 1.0% 6.1% 7.3% 7.5% -0.2% -2.1%
OH 10.4% 9.6% 0.8% 7.5% 10.9% 10.6% 0.3% 2.7% 18.2% 17.1% 1.1% 6.1% 4.2% 3.5% 0.7% 17.0% 1.4% 1.3% 0.1% 9.4% 24.3% 23.1% 1.2% 4.9% 12.4% 11.2% 1.2% 9.8% 7.6% 7.4% 0.2% 3.2%
OK 8.2% 8.1% 0.2% 2.2% 10.0% 9.6% 0.4% 4.2% 9.9% 8.9% 1.0% 9.7% 3.4% 1.9% 1.5% 43.3% 1.8% 1.8% 0.0% 0.6% 22.6% 21.6% 1.0% 4.6% 15.1% 11.7% 3.4% 22.4% 7.5% 7.9% -0.4% -5.7%
OR 7.6% 8.6% -1.0% -12.7% 10.8% 11.1% -0.4% -3.3% 12.7% 12.4% 0.2% 1.9% 3.5% 2.7% 0.8% 22.6% 2.2% 1.5% 0.6% 29.1% 31.5% 29.8% 1.7% 5.3% 10.9% 10.4% 0.5% 4.8% 8.5% 8.4% 0.2% 1.8%
PA 16.1% 15.4% 0.7% 4.5% 7.3% 7.1% 0.2% 2.1% 18.7% 19.3% -0.5% -2.9% 2.2% 1.8% 0.4% 18.3% 1.3% 1.1% 0.2% 12.8% 20.5% 20.3% 0.2% 1.0% 13.4% 12.1% 1.3% 9.8% 7.3% 7.2% 0.1% 1.1%
RI 11.9% 10.2% 1.7% 14.2% 10.7% 9.3% 1.3% 12.6% 11.3% 11.0% 0.3% 2.2% 1.4% 1.1% 0.3% 19.4% 1.5% 1.7% -0.2% -13.2% 18.5% 16.5% 2.0% 10.7% 12.5% 10.3% 2.2% 17.5% 6.0% 6.4% -0.4% -7.5%
SC 9.6% 10.0% -0.4% -4.0% 10.8% 10.5% 0.3% 3.0% 11.7% 11.9% -0.2% -1.4% 5.8% 4.4% 1.4% 23.9% 1.1% 0.9% 0.2% 18.6% 14.6% 14.0% 0.6% 4.3% 13.7% 11.9% 1.8% 13.1% 8.1% 8.1% 0.0% 0.4%
SD 10.6% 12.2% -1.6% -14.6% 6.8% 7.1% -0.3% -4.5% 25.7% 25.3% 0.4% 1.5% 1.7% 1.2% 0.6% 32.6% 2.0% 1.5% 0.5% 25.0% 22.6% 23.1% -0.5% -2.4% 9.2% 10.3% -1.1% -12.5% 6.5% 7.8% -1.3% -20.4%
TN 8.9% 9.0% -0.1% -0.9% 10.3% 9.7% 0.5% 5.2% 10.1% 10.0% 0.1% 1.2% 5.3% 4.5% 0.8% 14.7% 1.3% 1.0% 0.3% 24.0% 14.1% 13.2% 0.8% 6.0% 13.3% 12.0% 1.3% 10.0% 8.5% 8.4% 0.1% 1.3%
TX 11.9% 12.0% -0.1% -0.8% 9.0% 9.3% -0.3% -3.6% 12.8% 12.8% 0.0% 0.0% 2.4% 1.8% 0.6% 25.5% 1.8% 1.4% 0.3% 19.0% 14.6% 14.3% 0.4% 2.5% 11.2% 10.8% 0.4% 3.6% 6.4% 6.3% 0.1% 1.0%
UT 12.1% 12.3% -0.2% -1.7% 10.5% 9.1% 1.3% 12.6% 19.2% 21.3% -2.1% -10.8% 5.4% 4.6% 0.8% 15.1% 2.0% 1.8% 0.3% 13.5% 35.7% 39.1% -3.3% -9.3% 10.6% 10.7% -0.1% -1.1% 6.0% 5.7% 0.3% 4.2%
VA 13.1% 12.7% 0.4% 2.9% 10.8% 10.5% 0.3% 2.8% 16.0% 15.1% 0.9% 5.4% 1.5% 1.0% 0.5% 32.4% 1.4% 1.1% 0.4% 27.2% 16.4% 15.9% 0.5% 3.0% 12.2% 11.6% 0.6% 5.0% 9.1% 8.5% 0.7% 7.4%
VT 14.4% 14.5% -0.2% -1.1% 9.5% 9.4% 0.1% 0.8% 20.5% 21.4% -0.9% -4.4% 1.3% 1.1% 0.3% 19.2% 2.2% 1.6% 0.6% 26.9% 23.0% 24.1% -1.1% -4.7% 11.0% 12.4% -1.3% -12.0% 7.6% 7.5% 0.1% 1.3%
WA 9.8% 8.9% 0.9% 9.3% 10.7% 10.2% 0.5% 5.1% 20.8% 19.8% 1.0% 4.8% 1.7% 1.3% 0.4% 24.9% 1.9% 2.0% -0.2% -9.1% 28.4% 29.2% -0.8% -2.7% 11.4% 11.0% 0.4% 3.6% 8.5% 8.4% 0.0% 0.4%
WI 11.3% 10.5% 0.8% 7.2% 8.9% 8.4% 0.5% 5.6% 18.3% 17.2% 1.1% 6.0% 1.3% 1.0% 0.3% 22.8% 1.8% 1.4% 0.4% 21.6% 26.4% 26.9% -0.4% -1.7% 10.3% 9.4% 0.9% 8.3% 7.8% 7.5% 0.3% 3.6%
WV 12.2% 12.2% 0.0% 0.1% 11.8% 11.8% -0.0% -0.2% 16.3% 15.0% 1.3% 8.1% 2.8% 2.3% 0.5% 17.0% 1.5% 0.7% 0.8% 52.1% 18.8% 18.8% 0.0% 0.2% 14.1% 15.0% -0.9% -6.3% 9.3% 9.6% -0.3% -3.7%
WY 10.6% 9.5% 1.1% 10.0% 8.0% 8.8% -0.8% -9.6% 16.5% 17.1% -0.6% -3.5% 2.4% 1.4% 1.0% 42.1% 1.7% 1.4% 0.3% 14.8% 21.5% 22.8% -1.3% -5.8% 9.1% 9.5% -0.3% -3.6% 9.3% 9.0% 0.3% 2.7%
Appendix 1
CMS NurSiNg FaCility average Quality MeaSure SCoreS by State (CoNt.)
stat
e
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence
2009
2010
Diffe
renc
e
% D
iffer
ence

www.aqnhc.org www.ahca.org
Annual Quality Report