Embed Size (px)
Citation preview

Anorectal Carcinomas of Extra-Mucosal Origin *
YALE H. ZIMBERG, M.D., SAUL KAY, M.D.
From the Departments of Surgery and Surgical Pathology, Medical College of Virginia,Richmond, Virginia
IN THE PAST 25 YEARs numerous articleshave appeared in the world literature de-scribing cancers of the anorectal regionthat are unique either in cell type, site oforigin, or in primary location. Such titles as"Carcinoma of the Rectum Arising in Fis-tula-in Ano,"'10 "Basal Cell Carcinoma ofthe Rectum and Anus," "MucoepidermoidCarcinoma of the Anal Canal," 8 "SquamousCell Carcinoma of the Rectum," 15 "Pseudo-inflammatory Colloid Carcinoma of theRectum" 1 and "Adenocarcinoma of theIschiorectal Fossa" have frequently ap-peared in medical journals and for themost part have been viewed as separateentities. It is the purpose of this paper toshow a possible common origin for theextramucosal and "aberrant" anorectal car-cinomas, to call aftention to the misleadingsigns and symptoms that often precludeearly diagnosis and treatment, to add threenew cases to the literature, and to suggesta method of treatment for this unusualtype of neoplasm.
In 1880 Hermann described the histo-logic presence of tubular structures in theanorectal submucosa which occasionallyextended into the internal anal sphincter.Tucker and Hellwig 20 in 1934 revived in-terest in these ducts, and showed histo-logically that they frequently extendedfrom the crypts of Morgagni into the sub-mucosa and were often the primary sitesof infection in many cases of cryptitis.These authors showed well formed glandsin rabbits, cats, guinea pigs and dogs, andconcluded that the glands in humans werevestiges. In a series of cases studied micro-
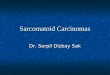
scopically, after abdomino-perineal resec-tion of the anus and rectum, the presenceof these glands was noted to be rather con-stant, if looked for. These structures, oftencalled intramuscular glands, were noted tobe branched and tubular, and were linedby columnar cells in their depth with tran-sition to squamous cells toward the mucousmembrane, a large part of the gland transi-tional type cells (Fig. 1). The presence ofthree cell types in the glands is of somesignificance when considering the poten-tialities of the ducts. Following these his-tologic presentations, many investigatorsconcluded that cryptitis, ischiorectal ab-scess and fistula-in-ano were frequentlycaused by these cul-de-sacs, and this viewis beink widely accepted today.
In 1931, Rosser 16 at the meeting of theAmerican Proctological Society reportedseven cases of carcinoma of the rectum thatlay primarily outside of the anorectal canal.These tumors, two epitheliomas and fiveadenocarcinomas, were postulated to havearisen from previously existing fistulae-in-ano since most of the patients had hadchronic fistulae. A review of the casesshowed that only one neoplasm had directcontinuity with the anorectal mucosa. Ros-ser concluded that the origin of these tu-mors must have been from the transitionalcells at the dentate line, since, at that time,he did not accept the presence of glandsbelow this area.
In the years following this report, nu-merous articles appeared describing car-cinomas arising in fistulae-in-ano and alsolateral to the anorectal canal. Marino,12 in1934, reported a case of an adenocarcinoma* Submitted for publication August 11, 1956.
344

ANORECTAL CARCINOMAS 345
FIG. 1. Longitudinal section through the pars analis recti. From a human embryo 187 mm.Note intramuscular glands in the zone of the rectal columns. (Reproduced from Textbook ofHistology by J. L. Bremer, M.D. Courtesy of The Blakiston Division, McGraw Hill Book Co.)
of the ischiorectal fossa without a mucous
membrane lesion. Manning,1" in 1937, de-scribed an adenocarcinoma of the rectumarising at the posterior commissure of theanus and concluded that the origin mighthave been a sweat gland, hair follicle or
fistulous tract. Dukes,3 in 1946, stressed the
fact that colloid carcinoma of the rectumcould supposedly arise in a fistula-in-anoand extend widely without any obviousmucous membrane involvement. Willis,21in his textbook on tumors, described a caseof neoplasm involving the anorectal sub-mucosa and internal sphincter without
Volume 145Number 3

346 ZIMBERG A
microscopic evidence of mucosal continu-ity. McAnally,13 in 1949, reported threecases from the Mayo clinic of carcinomaof the anorectal region that showed no in-volvement of the mucous membrane andno internal sinuses. One case was an epi-thelioma and two were adenocarcinomas.In 1951, O'Brien and Meehan 15 wrote oftwo cases of squamous cell carcinoma ofthe rectum arising four centimeters abovethe pectinate line. These tumors were con-
spicuous in that both had widespread sub-mucosal extension as compared to mucosalinvolvement. Gupta,7 in 1952, reported an
interesting case of an adenocarcinoma ofthe ischiorectal fossa with no history offistula-in-ano and no mucosal involvement.Stockman,'0 in 1953, stated that 64 cases ofcarcinoma associated with an anorectalfistula had been reported and added a case
of his own, showing no involvement ofmucous membrane. Binkley and Quan,1 in1954, described a slow growing colloid car-
cinoma of the anorectal region that showeda concomitant low grade chronic inflamma-tion. They reported six cases, all withinreach of the finger, and all showing indura-tion that initially was localized to the sub-mucosa, and later spread beyond the bowelwall with mucosal involvement only latein the disease. Close,2 in a comprehensivearticle in 1955, reported one case of a 54-year-old white man who had a one centi-meter nodule at the dentate line with sup-
posedly normal mucous membrane over
this lesion. The tumor was excised locally,and was found to be a "mucoepidermoidcarcinoma" with local lymphatic invasion.These reports are only a few of the many
which have described neoplasms that hadseemingly arisen adjacent to the anorectalmucosa and that had involved the mucosa
late in their development. The postulatedetiologies have included sweat glands, hairfollicles, transitional cells at the dentateline, fistula-in-ano and bowel reduplica-tions. Cognizance of the work of Hellwigand Tucker 20 on the anal glands leads one
,ND KAY Annals of SurgeryMarch 1957
to a logical common origin for these neo-plasms. The fact that the anal or intra-muscular glands lie outside the mucousmembrane and often contain three typesof cells (squamous, transitional and colum-nar) could explain the origin of many ofthe adenocarcinomas and squamous cellepitheliomas that have involved primarilythe submucosa and ischiorectal fossae. Itcould also explain the squamous cell epi-theliomas of the rectum and the adenocar-cinomas of the anus that have had exten-sive spread. The question of malignancyarising in a fistula-in-ano seems to offer noserious objection to this conclusion for thereason that many physicians treating ano-rectal disease now believe that fistulae fre-quently occur secondary to infections aris-ing in the anal glands. In addition, it isgenerally appreciated that many neoplasmsin their evolution may cause fistulae by ex-tension and necrosis. This view of etiologyis not original since the anal glands haveoccasionally been mentioned as a possiblesource of bizarre neoplasms of the anorec-tal region. In 1953, Grinvalsky and Hel-wig6 reviewed the cases of neoplasms ofthe anorectal region at the Armed ForcesInstitute of Pathology and concluded thatmany probably arose from the vestigialanal glands. The acceptance of this con-cept of origin of primarily extramucosalneoplasms of the anorectal region leads toan easy appreciation of the frequent diffi-culties encountered in early diagnosis andsuggests logical changes in our presentmodes of therapy.On reviewing the many descriptive terms
and titles that have been used for the extra-mucosal neoplasms of the anorectal region,it is easily seen that these lesions must haveclinically presented in various ways. Theconventional symptoms of change in bowelhabits with occasional blood-streaked stoolshave been reported in lesions that have pri-marily involved the ischiorectal fossae, andhave involved the anorectal mucosa as a latestage. Various case reports have shown that

ANORECTAL CARCINOMAS
indurations and masses adjacent to the analregion and out onto the buttocks have beenessentially asymptomatic and have goneunattended for long periods of time, withthe patient's concern being aroused onlywhen his stools have changed in characterand have contained blood. Painful defeca-tion has been a cardinal symptom in thosepatients who have had perianal or perirec-tal tumors that have produced an unyield-ing and fixed submucosa with resultinganal fissure formation. Chronic and persist-ent draining fistulae, either internal or ex-
ternal, have plagued a large number of thepeople found to have extramucosal ano-
rectal malignancies. The presence of a mass
in the perianal or gluteal region, though in-frequent as an initial symptom of these neo-
plasms, has been reported as the cause forseeking medical attention.A palpable or visible lesion of the mu-
cous membrane offers no serious problemin diagnosis; however, in those cases foundto have very small neoplasms of the mu-
cous membrane as compared to the sub-mucosal or lateral extension of tumor, one
should consider the origin as the analglands. Occasionally patients are examinedbecause of change of bowel habits, andare found to have only anorectal submu-cosal induration. Too frequently this hasbeen attributed to chronic infection. In thesix cases of so-called "pseudoinflammatorycolloid carcinoma of the rectum" reportedby Binkley and Quan,1 the initial findingswere simply submucosal induration whichlater spread laterally and involved mucous
membrane late. Chronic fistulae have beenexploited as possible harbingers of neo-
plasms, and it seems only necessary to reit-erate that fistulae of long standing, espe-
cially those that have not responded tosurgical treatment, should be suspected ofneoplasm. Perianal and perirectal masses
and masses extending into the buttocks,even though presenting the clinical pictureof chronic or acute infection, should beevaluated with a high index of suspicion.
In those cases where incision and drainageor excision of a mass in the anorectal regionhas produced a chronically inflamed, slowhealing wound, the possibility of an occultmalignancy should be entertained. This hasbeen emphatically shown in the cases ofMarino 12 and Noss.'4 The cardinal prin-ciples involved in making the diagnosis ofextramucosal anorectal cancer, therefore,seem to be to suspect the presence of a
malignancy despite the resemblance to a
purely inflammatory lesion and to persistin deep and frequent biopsies in those cases
that appear inflammatory, but fail to healwith the usual medical and surgical treat-ment.The surgical pathologic specimens at the
Medical College of Virginia from 1950 to1955 have been reviewed with the idea offinding cases of anorectal neoplasms thathave arisen extramucosally. It is immedi-ately seen that such a survey has manygross limitations. Numerous cases were
found which clinically seemed to be neo-
plasms that arose primarily beyond themucous membrane of the anus or rectum,but when finally sectioned in the pathologylaboratory showed gross or microscopic in-
volvement of mucous membrane in addi-tion to widespread lateral extension. Suchcases, though clinically acceptable, were
not included in our present series. The fol-lowing are three case reports of extramu-cosal, anorectal cancers that did have widelateral extensions without gross or micro-scopic evidence of involvement of contigu-ous mucous membrane.
CASE REPORTS
1. E. C., a 57-year-old colored man, was re-
ferred to St. Philip Hospital on May 6, 1954, withthe chief complaint of "boils on the buttocks."
This patient was in good health until October1953, when he noticed gluteal pain on sitting. Thepain became worse and finally a "boil" appeared,which ruptured and drained. The patient was
treated symptomatically for an inflammatory le-sion. In the latter part of October 1953, other"boils" appeared and drained spontaneously. In
Volume 145Number 3 347

348 ZIMBERG AND KAY
FIG. 2. Case 1. Gross appearance of abdomino-perineal resection. Note indurated pen-anal tissues,and multiple incised wounds.
the 2 or 3 months prior to admission, the drainagehad increased and the patient had become con-stipated.
Past history revealed that the patient had beentreated surgically for an anal fistula in 1932.
Physical examination was essentially negativeexcept as related to the buttocks and anal region.The entire perianal and gluteal region containedmany fistulous tracts with induration spreading7 to 8 cm. beyond the anal orifice. No lesion ofthe anal or rectal mucous membrane was noted.There was considerable induration felt in the ano-rectal submucosa. No mention was made of theinguinal nodes. On May 14, 1954, an excisiontype biopsy of the perianal lesion was done andthe microscopic diagnosis was lymphogranulomaof the anal region and carcinoma, colloid type,arising in fistula-in-ano.
On May 27, 1954, a wide abdomino- perinealresection was done. At the laparotomy the viscera
Annals of SurgeryMarch 1957
showed no evidence of metastasis, and there wereno enlarged periaortic nodes. Postoperatively thepatient did well and was discharged to be fol-lowed in the Outpatient clinic. However, he failedto return.
Pathologic Findings. Gross Description. Thespecimen consisted of sigmoid colon, rectum andperianal tissues. The length of the bowel was 35cm. and the perianal portion of the specimeni15 X 8 X 4 cm. The perianal tissues were indurated and showed multiple surgical incisions (Fig.2). The mucous membrane of the colon and rec-tum were intact and without focal lesions. Twofistulous tracts were identified, with openings 3 cm.above the pectinate line, and on the skin. A thirdtract opened into the rectum, 6 cm. above thepectinate line (Figs. 3, 4).
Microscopic Description. Sections showed acolloid carcinoma apparently arising in rectal cuta-neous fistulae. Typically the tumor showed largeirregular pools of mucin set in fibrous stroma.Some of the pools showed linings of well differen-tiated, orderly, colonic-types epithelium (Fig. 5).In other areas there were atypical dilated glandslined by similar epithelium. The fistulae were par-tially ulcerated and partially lined by non-neo-plastic colonic epithelium as well as tumorousglands (Figs. 6, 7). None of the paracolic andmesenteric lymph nodes were involved by metas-tatic tumor.
2. H. H., an 80-year-old white male farmer,was admitted to the Medical College of VirginiaHospital on January 17, 1952, because of an.ulcerated mass involving his left buttock. Thepatient had had recurrent episodes of prolapse ofrectal mucosa and hemorrhoids for 60 years, with
Fic. 3. Case 1. Rectum opened to show ab-sence of mucosal lesion and the presence of threefistulous tracts.

ANORECTAL CARCINOMAS
FIG. 4. Case 1. Coronal section through rectumrevealing fistulous tract surrounded by neoplastictissue. The rectal mucosa is above the tract.
occasional rectal bleeding for 20 years. Approxi-mately 20 years before admission he developed a
small nodule of the left buttock. Three years priorto admission the perianal lesion had increased insize and had occasionally bled and drained a
seropurulent material. In the 6 months beforecoming to the hospital the lesion had progres-sively enlarged and had ulcerated. There was no
history of change in bowel habits. Physical ex-
amination on admission revealed a well developed,thin, hypertensive man in no acute distress. Ab-dominal palpation revealed no masses. There wasbilateral inguinal lymphadenopathy, some nodesmeasuring 2 to 3 cm. in diameter. No lesion ofthe anal or rectal mucous membrane was felt or
seen. On the right buttock there was a 7.5 cm.
ulcerated lesion with surrounding inflammationand fistulae. Genito-urinary examination showedno pathologic condition of the bladder or prostate.Laboratory studies were essentially negative as
was the chest film and barium enema. A biopsy ofthe mass revealed a colloid carcinoma of the leftgluteal region. On February 6, 1952, a cauteryexcision of the mass was done. Approximately 5to 7.5 cm. above the anus the lesion approachedthe rectal wall. The growth was excised as closeto the rectum as possible and was packed. Theoperator felt that the entire lesion had not beencompletely removed. The excision site healedslowly and finally closed. The patient was lastseen in the Tumor Clinic on March 10, 1953, withsmall nodules in the scar of the previous excision.There was no intramucosal lesion felt at this time.
Pathologic Findings. Gross Description. Thisspecimen consisted of an elliptical mass of skin-covered tissue 8 X 6.5 X 6 cm. A tract was presentat one pole, extending throughout the entire thick-
FIG. 5. Case 1. A large mucinous pool surroundedby neoplastic columnar epithelial cells.
ness of the specimen. The cut surface showedragged, glistening and mucoid tumor tissue.
Microscopic Description. Sections showed skinand subcutis with a colloid-type carcinoma in thedepth. The tumor was composed of large pools ofmucinous material surrounded by strips and islandsof tall columnar epithelium which were generallyof the goblet-cell variety (Fig. 8). The nuclei ofthe epithelium were bizarre and often stratified.
3. C. R., a 55-year-old colored man, was ad-mitted to the St. Philip Hospital surgical serviceon April 27, 1953, with 5 month history of a drain-ing and bleeding lesion of the perianal skin andprogressive constipation. Past history and systemicreview were essentially negative. Physical examina-tion revealed a well developed, fairly well nour-ished man in moderate discomfort. Inguinal nodeswere enlarged bilaterally. A perianal fungatinglesion, almost completely blocking the anal orificewas present. No mucous membrane lesion in theanus or rectum could be felt. Initial laboratorystudies revealed marked anemia. Chest x-rayshowed cardiomegaly, but no metastasis. Cysto-scopic examination showed no involvement of thebladder by the tumor. A biopsy of the perianallesion was reported as carcinoma of the anal re-gion. On May 14, 1953, an abdomino-perineal re-section was done. At the operation no evidence ofintra-abdominal metastasis was noted. Postopera-tively the patient developed a wound infectionwhich finally healed, and he was discharged onJuly 30, 1953.
He was readmitted on October 1, 1953, witha 5 day history of crampy abdominal pain, nauseaand vomiting. Physical examination and x-raystudies showed evidence of small bowel obstruc-tion. The inguinal nodes were enlarged and firm.
Volume 145Number 3 349

350 ZIMBERG AND KAY
FIG. 6. Case 1. Low power view of fistuloustract which is partially ulcerated and partiallylined by colonic-type epithelium.
He was re-explored and was found to have a largehepatic metastasis and recurrent carcinoma in thefloor of the pelvis with extension to the smallbowel. A palliative resection of small bowel wasdone. Postoperatively the patient developed awound infection and later a fecal fistula. He wentprogressively downhill and died on November 20,1953. Autopsy was not -permitted.
Pathologic Findings. Gross Description. Themajor specimen consisted of the rectum, anus anda large circular portion of skin, 11 cm. in diameter,around the anus. The rectum was approximately9 cm. in length and surrounded by fragments oflevator ani muscles. The cutaneous surface was ir-regularly nodular with foci of ulceration. The skinwas partially replaced by the tumor mass approx-imately 6 x 8 cm. and the surface nodules werehard (Fig. 9). About 1.5 cm. posterior to the analopening was a fistulous tract with hemorrhagicfluid exuding therefrom. This could be probed fora distance of 3 to 4 cm. When the rectum wasopened the mucosa was found to be uninvolvedby tumor except for a small area of induration andretraction on the left lateral wall, approximately5 cm. from the anal opening (Fig. 9). In thissame area there were at least 2 tracts, one ofwhich tunneled under the mucosa leaving twoopenings. These tracts did not appear to com-municate with the exterior. Transverse sectionswere made at 4 levels through the mass of tumor.These sections revealed a markedly extensive, in-filtrating, irregular, white to red tumor with areasof yellow fat or necrosis scattered throughout andwith multiple abscesses 3 to 7 mm. in diameter.Seen also were multiple fistulous tracts scatteredat various places throughout the mass of the tumor
Annals of SurgeryMarch 1957
FIG. 7. Case 1. High power view to show neo-plastic glandular elements lining a portion of thefistulous tract.
(Fig. 10). The tumor extended up to and into theskin in some areas, as was noted previously fromthe external surface.
Microscopic Description. Sections showed amoderately well differentiated carcinoma exten-sively invading the perianal muscle, fat and skinwith extension into the musuclaris and submucosaof the rectum. Several fistulous tracts and ab-scesses were present. Some of the tracts werelined by both squamous and epithelium and tumor(Fig. 11). Tumor also partially ulcerated the peri-anal skin. The tumor was composed mainly ofrather well-formed glands in a disorderly arrange-ment, with only a few small solid nests of tumorcells (Fig. 12). The glands often showed consider-able production of mucus. The tumor cells showedmoderate pleomorphism and had a granular, oftenvacuolated cyto plasm, with large oval or irregularvesicular nuclei and prominent nucleoli. Manybizarre nuclei were seen and mitoses averaged 2to 3 per high power field. The tumor decreased inextent at progressively higher levels above theanus. In sections 5 cm. above the anus, granuloma-tous areas were seen, probably due to intestinalcontents since no acid fast bacilli could be demon-strated. Nowhere was the rectal or anal mucosainvolved by tumor. None of the regional lymphnodes harbored metastases.
DISCUSSION
The treatment of anorectal, extramucosalneoplasms has assumed as many forms asthe varied names given to this interestinglesion, It is apparent that confusion with

Volume 145 ANORECTAINumber 3
chronic inflammatory lesions and late diag-nosis has, in many cases, made treatmentpiece-meal and inadequate. The literaturedeals with many cases that have had at-tempts at local extirpation with and with-out removal of the anorectal canal and withand without the inclusion of pelvic andinguinal nodes. Needless to say, the recur-rence rate in these cases has been high. Inlarge lesions adjacent to the anorectal canalirradiation has been tried but with poorlong term results. Some cases that haveshown considerable involvement of theanorectal mucous membrane have beentreated by abdomino-perineal resection. Areview bf the cases so treated has showntwo interesting things. The incidence of in-volvement of superior hemorrhoidal andinferior mesenteric nodes has been fairlylow and the incidence of local recurrencewith the conventional abdomino-perinealresection has been high.Rundle and Hales,17 in 1953, reported 17
cases of mucoid carcinoma supervening onfistula-in-ano. Four of the patients had in-guinal nodes that were positive for tumor.Since all of their cases did not have rou-tine inguinal node dissections or biopsy, theincidence of carcinoma in the inguinalnodes in this series might have been higher.Dukes 4 in a recent article on neoplasmsof the anorectal region, presented two cases
....
. J ., . f ^
FIG. 8. Case 2. Low power view to show typicalfield of colloid carcinoma,
L CARCINOMAS 351
FIG. 9. Case 3. Opened specimen of abdomino-peroneal resection. Note absence of mucosal lesion,and neoplastic tissue replacing the pen-anal tissues.
of extramucosal anorectal carcinomas thatmetastasized to the inguinal nodes. Cat-tell, Williams, Bacon and Pack reportedlydo routine radical excision of inguinal andiliac nodes plus an abdomino-perineal re-section with squamous cell carcinomas ofthe anus because they feel that in low le-sions the lymphatic spread to the inguinaland iliac nodes is a pathway that has tobe removed in addition to the superiorhemorrhoidal lymphatic route. In 1952,Sauer and Bacon,18 in an attempt to im-prove their results in carcinoma of the anusand rectum, described an addition to theMiles procedure which helps encompassthe lateral spread of tumor. For anorectalneoplasms, these authors have done theabdomino-perineal resection described to-gether with an excision of the fascia fromthe pelvic wall and have removed the lym-phatics of the iliac vessels. In their hands,the incidence of positive nodes found in

352 ZIMBERG A
FiG. 10. Case 3. Coronal section of perirectalarea to show sinus tract deep to mucosal surface(arrow) surrounded by neoplastic tissue.
this wider resection seems to justify theprocedure.
In Gray's Anatomy 5 the lymphatics fromthe anus and perineum are shown to pass tothe superficial inguinal nodes. The spreadfrom the anal canal is noted to accompanythe middle and inferior hemorrhoidal ar-teries and end in the hypogastric nodes.The lymphatic channels of the rectum govia the pararectal glands to the sigmoidmesocolon, and then onto the preaorticnodes around the origin of the inferiormesenteric artery.
Since adequate surgical therapy for can-cer demands the wide excision of the locallesion with its concomitant lymphatic path-ways, this principle of management mustbe followed in extramucosal, anorectal neo-plasms. It has been shown that lesionswhich arise just adjacent to the anorectalmucosa and involve the levator ani musclesand ischiorectal fossae and occasionally theperineal skin, may spread not only throughthe superior hemorrhoidal channels butmay metastasize to the inguinal, iliac and
ANDKAY ~~~~~~~Annals of SurgeyAND KAY March 1957
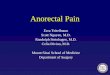
hypogastric nodes (Fig. 13). This consid-eration shows the inadequacy of local ex-cisions and the conventional abdomino-perineal resection. To properly treat thepatient who is found to have an extramu-cosal, anorectal neoplasm, it would seemthat the logical operative procedure shouldbe a wide abdomino-perineal resectionwith the removal of the inferior mesenteric,hypogastric and external iliac lymphaticsand the fascia of the pelvic walls. The in-clusion of a superficial groin dissectionshould probably be reserved for neoplasmsthat are very low in the anus and/or in-volve the integument of the perineum andfor those that have clinical and/or micro-scopic evidence of metastasis to superficialinguinal nodes. Admittedly, the practice ofroutine biopsy or dissection of superficialinguinal lymph nodes, or despite the lackof enlarged glands, is a moot point that isworthy of serious consideration.
SUMMARY AND CONCLUSION
1. The literature contains many cases ofneoplasms that involve primarily the tis-sues adjacent to the anorectal canal.
2. The anal glands have been shown tobe a logical source for many of thesemalignancies.
3. The signs and symptoms are variedand frequently mislead to a diagnosis ofan inflammatory condition.
FIG. 11. Case 3. Low power view to show sinustract with its partial squamous epithelial lining.

Volume 145 ANORECTAL CARCINOMAS 353Number 3
FIG. 12. Case 3. High power view to show detailof tract with neoplastic glands in the wall.
4. The diagnosis of an extramucosal ano-rectal malignant tumor will be made earlierand more frequently if the presence of ma-lignancy is suspected despite the trappingsof an inflammatory lesion and if frequentdeep biopsies are taken in these supposedinflammatory lesions that fail to heal withthe usual medical and surgical measures.
Ve, CaV
t rieenterc a-su.Lp /Illllfldlt//tCom.diocia
hernovehom
FIG.13.Diagram Hylymphaticodrnaesric
ofid hemorrhroidalSubing ~~~~~~~~~Obturtor oenode s/ etaucs nod
rectal neopla s ae r .Ischiorectinf.heA ionaoprtn r tossxamucosalanorectal malignaLnevator amni
FIG.13o Diagram of lymphatic drainageof the anorectal region.
5. Three new cases of extramucosal ano-rectal neoplasms are reported.
6. A rational operation for the extra-mucosal anorectal malignancies, despite thedegree of late involvement of mucous mem-brane, should consist of a wide abdomino-perineal resection of the anorectal canalwith the inclusion of the pelvic fascia, iliacand hypogastric lymphatics and nodes and,at times, bilateral dissection of the inguinalregions.
ACKNOWLEDGMfENT
We wish to thank Dr. Carrington Williams,Sr., whose objective criticisms were most helpfulin the final compilation of this article.
BIBLIOGRAPHY
1. Binkley, G. E. and S. H. 0. Quan: Pseudo-inflammatory Colloid Carcinoma of the Rec-tum. Cancer, 7: 1020, 1954.
2. Close, A. S. and R. L. Schwab: A History ofthe Anal Ducts and Anal-Duct Carcinoma.Cancer, 8: 979, 1955.
3. Dukes, C. E.: Peculiarities in the Pathologyof Cancer of the Ano-Rectal Region. Proc.Roy. Soc. of Med., 39: 763, 1946.
4. Dukes, C. E. and C. Galvin: Colloid Car-cinoma Arising Within Fistulae in the Ano-Rectal Region. Annals of the Royal Collegeof Surgeons of England, 18: 246, April, 1956.
5. Gray, H.: Anatomy of the Human Body. Leaand Febiger, Phila. Twenty-Fifth Edition,pp. 715-717, 721, 1948.
6. Grinvalsky, H. T. and E. B. Helwig: Car-cinoma of the Perianal Ducts. Abstract, Am.Jour. of Path., 29: 610, 1953.
7. Gupta, S. C.: Anal Duct (Case Report of aRare Complication). Indian Journal Surg.,14: 185, 1952.
8. Kay, S.: Mucoepidermoid Carcinoma of theAnal Canal and Its Relation to the AnalDucts. Cancer, 7: 359, 1954.
9. Kratzer, G. L. and M. B. Dockerty: SquamousCell Epitheliomas of the Rectum. Ann.Surg., 131: 392, 1950.
10. Long, C. H.: Carcinoma Arising in Fistula-in-ano. Jour. Tenn. State Med. Asso., 44:502, 1951.

354 ZIMBERG AND KAY Annals of Surgery
11. Manning, V. R.: Adenocarcinoma of the Anus.Trans. Am. Proc. Soc., pp. 70-74, 1937.
12. Marino, A. W. M.: Primary Mucous Adeno-carcinoma of the Areolar Tissue on theIschiorectal Fossa. Tr. Am. Proc. Soc., pp.113-116, 1934.
13. McAnally, A. K. and M. B. Dockerty: Car-cinoma Developing in Chronic DrainingCutaneous Sinuses and Fistulas. S. G. & O.,88: 87, 1949.
14. Noss, J. C.: Malignant Degeneration of Fis-tula-in-ano. Trans. Am. Proct. Soc., pp. 144,1940.
15. O'Brien, P. 0. and D. J. Meehan: SquamousCell Carcinoma of the Rectum. Annals ofSurgery, 133: 283, 1951.
16. Rosser, C.: The Etiology of Anal Cancer. Am.Jour. Surg., 11: 328, 1931.
17. Rundle, F. F. and I. B. Hales: Mucoid Car-cinoma Supervening on Fistula-in-ano, ItsSurgical Pathology and Treatment. Ann.Surg., 137: 215, 1953.
18. Sauer, I. and H. E. Bacon: A New Approachfor Excision of Carcinoma of the Lower Por-tion of the Rectum and Anal Canal. S. G. &O., 95: 229, 1952.
19. Stockman, J. M. and V. T. Young: CarcinomaAssociated with Ano-Rectal Fistula. Trans.Am. Proct. Soc., pp. 560-561, 1953.
20. Tucker, C. A. and C. A. Hellwig: Histopathol-ogy of Anal Crypts. S. G. & O., 58: 145,1934.
21. Willis, R. A.: Pathology of Tumors. St. Louis,C. V. Mosby Co., pp. 428, 1948.
0)G4Ilk