Embed Size (px)
Citation preview

An Orthotopic MurineModel of Sinonasal MalignancyAlexander Gelbard,1,3 Michael E. Kupferman,1SamarA. Jasser,1Wantao Chen,4 Adel K. El-Naggar,2
Jeffrey N.Myers,1and Ehab Y. Hanna1
Abstract Purpose: Malignant sinonasal tumors are clinically challenging due to their proximity to vitalstructures and their diverse histogenesis and biological behavior. To date, no animal modelsaccurately reflect the clinical behavior of these malignancies.We developed an orthotopic murinemodel of sinonasal malignancy that reproduces the intracranial extension, bony destruction, andspread along neural fascial planes seen in patients with aggressive sinonasal malignancies ofvarious histologies.Experimental Design: Human squamous cell carcinoma line (DM14) and adenoid cysticcarcinoma line (ACC-3) were implanted in the right maxillary sinus or soft palate in male nudemice. Animals were monitored for tumor growth and survival. Tumor specimens were removedfor histopathologic evaluation to assess for intracranial extension, orbital invasion, bony invasion,perineural invasion, and distant metastasis. Statistical analysis was done to calculate P valueswith the Student’s t test for individual tumor volumes. Differences in survival timeswere assessedusing the log-rank test.Results: Mice with DM14 or ACC-3 implanted in either the maxillary sinus or the soft palatedeveloped large primary tumors. A statistically significant inverse correlation between survivaland the number of tumor cells implanted was found. Histopathologic evaluation revealed orbitalinvasion, intracranial extension, pulmonary metastasis, lymph node metastasis, and perineuralinvasion.Conclusions:We describe the first orthotopic model for sinonasal malignancy. Our modelfaithfully recapitulates the phenotype andmalignant behavior of the aggressive tumor types seenin patients. This model offers an opportunity to identify and specifically target the aberrantmolecular mechanisms underlying this heterogeneous group of malignancies.
Malignant sinonasal tumors are clinically challenging becauseof their rarity, their proximity to vital structures, and theirhistologic variety within a complex anatomic region. Thesetumors comprise <3.6% of all malignancies seen in the headand neck (1). With an annual incidence of only 0.5 to 1 per100,000 per population, these tumors have been difficult tostudy in large clinical trials, leaving treatments and outcomes tobe based primarily on limited retrospective data.
The most common sinonasal malignancies are squamous cellcarcinoma (SCC) followed by adenoid cystic carcinoma (ACC).Most (70-80%) of these tumors originate in the maxillary sinus,but only 25% remain confined to the sinus (2). Patterns ofinvasion include direct extension into the orbit or skull base viaperineural spread and bony destruction, spread to the regionallymphatics, and distant metastasis. Recurrence generally reflectslocal tumor regrowth rather than distant metastasis (3, 4).Despite improved surgical approaches, refined radiotherapytechniques, and cytotoxic chemotherapies, 3-year disease-specific survival remains <35% in patients with T3 and T4
lesions (5). Future progress in disease-specific morbidity andmortality will require the identification of novel prognostictumor markers and the implementation of molecular-basedtherapies.
One of the challenges to developing molecularly targetedapproaches in sinonasal malignancies has been the lack ofpreclinical models facilitating laboratory-based investigations.In contrast to the use of traditional cytotoxic agents, which relyon differential killing of rapidly dividing cells, effectivemolecular approaches require a thorough understanding oftumor cell biology in the context of the native tumormicroenvironment (6, 7). The vast majority of the informationpertaining to the molecular pathways mediating vital cellprocesses and therapeutic response has been based on in vitromonolayer cultures (8, 9). The application of these modelsassumes that the growth and metastatic mechanisms of a tumor
CancerTherapy: Preclinical
Authors’Affiliations: Departments of 1Head and Neck Surgery and 2Pathology,The University of Texas M. D. Anderson Cancer Center ; 3Bobby R. AlfordDepartment of Otolaryngology-Head and Neck Surgery, Baylor College ofMedicine, Houston,Texas and 4Laboratory of Oral Tumor Biology, Ninth People’sHospital, Shanghai JiaoTong University School of Medicine, Shanghai, People’sRepublic of ChinaReceived 4/14/08; revised 7/15/08; accepted 7/31/08.Grant support:The RNRCross Foundation,The Patricia Knebel Memorial Fund ofthe Pittsburgh Foundation, Adenoid Cystic Carcinoma Organization International,The University of Texas M. D. Anderson Cancer Center Pantheon Project, NIHCancer Center support grant CA016672, and NIH National Research Servicefellowship awardT32 DC 007367.The costs of publication of this article were defrayed in part by the payment of pagecharges.This article must therefore be hereby marked advertisement in accordancewith18 U.S.C. Section1734 solely to indicate this fact.Requests for reprints: EhabY. Hanna, Department of Head and Neck Surgery,The University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Boulevard,Box 0441, Houston,TX 77030-4009. Phone: 713-745-1815; Fax: 713-794-4462;E-mail: [email protected].
F2008 American Association for Cancer Research.doi:10.1158/1078-0432.CCR-08-0977
www.aacrjournals.orgClin Cancer Res 2008;14(22) November15, 2008 7348
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

cell in vitro resemble those in situ. Although a valuable tool inthe study of cellular functions, they may not reflect the naturalhost-tumor microenvironment interactions associated withtumor development and progression (10–13). Attempts tocompensate for this inherent limitation of the in vitro conditionhave included implanting human tumor cells as subcutaneousxenografts in immunocompromised mice (14). Althoughsubcutaneous growth occurs in vivo, it does not replicate thenormal tumor-host interactions for these tumors and thusremains an inferior system for preclinical modeling (15, 16).
Current animal models of sinonasal malignancy consist ofseveral purely intracranial murine brain tumor models (17) andisolated rabbit models of maxillary sinus cancer that do notshow local spread or skull base invasion (18, 19). Heterotopicengraftment models have also been established from humansinus cancer cell lines (20, 21). However, to date, no animalmodel is established to study the clinical and biologicalbehavior of these malignancies. Therefore, the aim in ourcurrent study was to create an orthotopic murine model ofsinonasal malignancy that could reproduce the intracranial
extension, orbital involvement, bony destruction, and spreadalong neural facial planes frequently seen in patients withaggressive sinonasal malignancies of various histologies.
Materials andMethods
Cell lines. To produce tumors, ACC (ACC-3; human salivary ACCcell line provided by Dr. Wantao Chen, Laboratory of Oral TumorBiology, Ninth People’s Hospital, Shanghai Jiao Tong University Schoolof Medicine; previously established from an ACC of the parotid gland;ref. 20) and SCC (DM14; derived in our laboratory from floor ofmouth cancer cell line TU167) were harvested from subconfluentcultures maintained in frozen stocks. ACC-3 cells were maintained asmonolayer cultures in RPMI 1640 containing penicillin-streptomycin(Flow Laboratories), nonessential amino acids, sodium pyruvate,L-glutamine, and 10% fetal bovine serum. DM14 cells were grown inDMEM supplemented with 10% fetal bovine serum, penicillin/streptomycin, sodium pyruvate, glutamate, and nonessential aminoacids. We maintained adherent monolayer cultures at 37jC in 5%CO2 and 95% air. The cultures were maintained free of Mycoplasmaspecies and no longer than 12 weeks after recovery from frozen stocks.For injections, the cells were trypsinized and resuspended in serum-freeHBSS at appropriate concentrations. Cells from both of the humantumor lines were prepared in 30 AL HBSS in the following concen-trations: 5 � 105, 2 � 105, 5 � 104, and 5 � 103.
Animal care and implantation of tumor cells. Male nude mice(ages 6-8 weeks) were purchased from the Animal Production Areaof the National Cancer Institute-Frederick Cancer Research andDevelopment Center. The mice were maintained in a pathogen-freeenvironment and fed irradiated mouse chow and autoclaved reverseosmosis-treated water at facilities in accordance with current regulationsand standards. The mice were used in accordance with the Animal Careand Use Guidelines of The University of Texas M. D. Anderson CancerCenter. All of the animal procedures were done in accordance with aprotocol approved by the Institutional Animal Care and UseCommittee. We injected experimental animals with tumor cells fromtwo human cancer lines (previously described) in either the maxillarysinus or the soft palate to determine the optimal site of orthotopictumor implantation. All mice were anesthetized with intraperitonealsodium pentobarbital (50 mg/kg body weight) before injection. Weused groups of five mice for each concentration and each cell line. Micewere euthanized with CO2 when they lost >20% of their body weight,had ulcerated tumors, or became moribund in accordance withInstitutional Animal Care and Use Committee guidelines.
Maxillary sinus model. We sought to determine if human xenograft
tumors could be established in the maxillary sinus of mice. Mice were
anesthetized with an intraperitoneal phenobarbital injection. After
confirming the degree of anesthesia, we placed the mice in a supine
position. Tumor cells were implanted via transcutaneous injection
underneath the infraorbital muscle groups, with the needle angled
Translational RelevanceMalignant sinonasal tumors are an aggressive and rare
cancer subtype. As a consequence of their clinically rarity,few tools exist to model these malignancies, leavingtreatment primarily based on limited retrospective data.The experience with this disease stands in sharp contrastto the rapid progress that has been made in our under-standing of the molecular alterations contributing to thedevelopment of SCC arising outside the sinonasal tract.As evidenced by the discovery of EGFR signaling in headand neck cancer, targeting aberrant molecular signalinghas been directly translated into tangible patient benefit.Yet, our understanding of the molecular biology ofsinonasal malignancies and their potential for molecularlytargeted therapy has not yet been able to reap the full ben-efit of current research efforts centered on disease outsidethe sinonasal cavity. This work is an investigation of anunderstudied tumor type and offers a potentially noveltool to other investigators in the field of head and neckcancer to apply several of the well-established moleculartherapeutics to amalignancy with precious few therapeuticoptions.
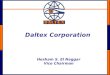
Fig. 1. A, magnetic resonance images ofnormal mouse show the sinonasalanatomy. Red, left maxillary sinus.Variousconcentrations of cells from human tumorlines were injected transcutaneously anteriorto the orbit. B, sagittal diagram, magneticresonance image, and H&E-stained sectionof normal mouse depict the anatomy of thesoft palate.
OrthotopicMurineModel of SinonasalMalignancy
www.aacrjournals.org Clin Cancer Res 2008;14(22) November15, 20087349
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

CancerTherapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2008;14(22) November15, 2008 7350
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

toward the lateral wall of the maxillary sinus. We used a 1 mL
tuberculin syringe (Hamilton) with a 30-gauge hypodermic needle for
the injections. The absence of a fluid leak from the nasal cavity
confirmed a successful injection. The mice were observed until the
effects of anesthesia had resolved.Soft palate model. We sought to determine if human xenograft
tumors could be established in the soft palate of mice. Mice wereanesthetized with an intraperitoneal phenobarbital injection. Afterconfirming the degree of anesthesia, we placed the mice in a supineposition. The mandible was depressed, and the tongue was retracted toshow the junction of the hard and soft palate. After identifying the softpalate, we implanted tumor cells via direct injection into the muscle ofthe soft palate using a 30-gauge hypodermic needle and a 1 mLtuberculin syringe (Hamilton). After injection, a well-localized whealover the soft palate and the absence of a fluid leak from the nasal or oralcavity confirmed a successful injection. The mice were observed untilthe effects of anesthesia had resolved.
Survival assessment. Initial survival studies were done to determine
the proper time to euthanize the animals for the tumor growth study.
During the initial survival studies, we checked the animals daily for
hypomotility and absence of grooming behavior. The body weights of
animals were measured twice a week to detect weight loss. We
euthanized mice with CO2 when they became moribund or when their
weight loss was >20%. At the conclusion of the study, survival curves
were plotted for time of animal death according to the above-mentioned
criteria. Kaplan-Meier estimation was used to graph the survival curve
using moribundness and >20% weight loss as surrogates for survival.Necropsy and tissue preparation. For tumor growth and invasion
evaluation, we euthanized the animals with CO2 18 days after cell lineimplantation. At the time of death, the full heads of the mice wereobtained, fixed in a periodate-lysine-paraformaldehyde solution for24 h, and decalcified in Immunocal formic acid bone decalcified(Decal) for 10 to 12 days. Each head was divided into blocks by onemedian and two paramedian sagittal sections. All head samples wereembedded in OCT compound (Tissue-Tek OCT Compound; SakuraFinetek) after going through successive passage in 10%, 15%, and 20%sucrose concentrations. H&E staining was done on histologic sections ofthe head to determine the extent of tumor growth and the degree ofinvasion into surrounding structures. Also at the time of euthanasia,tumors were measured and volume was estimated with the formula:volume of a sphere = 4 / 3pr3. Additionally, the cervical lymph nodes andlungs were removed and placed in 10% buffered formalin solutionovernight for fixation. Each specimenwas stained withH&E and evaluatedunder light microscopy for the presence of regional or distant metastasis.
Statistical analysis. Statistical analysis was done with SPSS software.In the tumor volume studies, an ANOVA was done to assess whether anoverall difference existed between the mean volumes of the tumorsgrowing from cell suspensions of different concentrations. If the testshowed that a significant difference existed, two-tailed Student’s t testswere done. The t test comparisons were used to compare the differencesbetween tumor volume and the initial tumor cell concentration. Alltests were done separately for the maxillary sinus and soft palate data.The level of significance was set at 5% (P < 0.05). In survival studies, thelog-rank test was used to determine if differences in survival times weresignificant (P < 0.05).
Results
Orthotopic implantation is technically feasible and can be usedwith a spectrum of human tumor xenografts. Maxillary sinus isseen on computed tomography of normal mouse (imagesprovided courtesy of VoxPort); red shaded regions denotemaxillary sinus (Fig. 1A). Normal soft palate is seen onillustration (Color Atlas of Anatomy of Small Laboratory Animals,Volume II. Popesko, Rajtova, and Horak. Elsevier; 2002. p. 123);sagittal computed tomography section of normal mouse(images provided courtesy of VoxPort) and H&E-stainedsection from normal mouse (Fig. 1B).Human SCC line DM14 forms large bulky tumors when
injected into either the maxillary sinus or the soft palate of nudemice. Successful implantation and tumor formation wasachieved with 5 � 105 cells of the human SSC cell line DM14implanted into either the maxillary sinus (Fig. 2A-C) or the softpalate (Fig. 2D-F) of nude mice. High rates of local invasionwere seen within 30 days in mice with tumor implanted ineither the maxillary sinus or the soft palate, showing thefeasibility of these orthotopic injection techniques for xenograftimplantation and growth.
To further characterize the model and to establish optimaltime points for euthanasia and histologic evaluation, weperformed a longitudinal observational study in mice injectedwith various concentrations of DM14 cells implanted in eitherthe soft palate (Fig. 2G) or the maxillary sinus (Fig. 2H). In themaxillary sinus model, the Kaplan-Meier survival analysisrevealed a statistically significant difference in survivalwhen mice injected with 5 � 105 cells were compared withmice injected with 5 � 104 (P = 0.002) or 5 � 103 (P = 0.002)cells. The difference between mice bearing 5 � 105 cellsand mice bearing 2 � 105 cells was not statistically significant(P = 0.926). For the group of mice injected in the soft palate,the Kaplan-Meier survival analysis revealed a statisticallysignificant difference in survival between mice injected with5 � 105 cells and all other groups (versus 2 � 105, P = 0.004;versus 5 � 104, P = 0.0018; and versus 5 � 103, P = 0.0018).Using the Kaplan-Meier survival analysis, we determinedthe median survival time for mice that received 5 � 105 cellsin the maxillary sinus was 25.50 days. The median survival timefor mice that received 5 � 105 cells implanted in the soft palatewas 18.5 days. To maximize the number of surviving micebearing tumor for histologic analysis, we elected to euthanizeall mice at 18 days in the next experiment.Human SCC line DM14 shows local tissue invasion and
regional and distant metastasis when injected into either themaxillary sinus or the soft palate of nude mice. Mice thatreceived 5 � 105 DM14 cells in the maxillary sinus developedtumors that invaded through the lamina papyracea into the
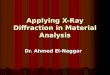
Fig. 2. Orthotopic mouse model of SCC of the paranasal sinuses. A, frontal view of mouse shows human SCC line DM14 implanted transcutaneously in the right maxillarysinus and the resulting proptosis. B, superior view of the same mouse as in A. C, H&E staining of axial section through the orbit from the mouse in A and B shows massivetumor infiltration.G, globe;M, orbital musculature; gl, gland; arrow, retina;T, tumor.D, frontal viewof visible tumor fromhuman SCC line DM14 implanted in the soft palate ofa mouse. E, superior view of the same mouse as in D. F, H&E staining of sagittal section through the cranial midline of the mouse shown in D and E and the resultingenlarging tumor in the soft palate with extension toward the cranial vault. Cb, cerebellum; C, cerebrum;T, tumor in soft palate; t, tongue; arrow, cricoid cartilage. Both themaxillary sinus images and the soft palate images are representative of those for 5mice each injectedwith of 5�105 tumor cells in 30 ALHBSS. All photographswere taken atthe time of euthanasia 18 days following tumor implantation. G, Kaplan-Meier survival curves for mice with tumors implanted in the soft palate revealing a statisticallysignificant difference in survival betweenmice injected with 5� 105 cells and all other groups [versus 2� 105 (P = 0.004), versus 5� 104 (P = 0.0018), and versus 5� 103
(P = 0.0018)]. H, Kaplan-Meier survival curves for mice with tumors implanted in the maxillary sinus showing statistically significant differences in survival times betweenmice injectedwith 5�105 cells andmice injectedwith 5�104 (P = 0.002) or 5�103 (P = 0.002).The difference in survival times betweenmice bearing tumors from5�105
cell density inoculations (median,18.5 days) and those bearing tumors from 2� 105 cell density inoculations (median, 25.5 days) was not statistically significant (P = 0.926).
OrthotopicMurineModel of SinonasalMalignancy
www.aacrjournals.org Clin Cancer Res 2008;14(22) November15, 20087351
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

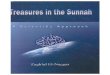
Fig. 3. Malignant phenotype of orthotopic model of SCC of the maxillary sinus and soft palate. A, H&E staining of axial sections through the orbit shows invasion oftumor through the lamina papyracea into the orbital cavity. G, globe;T, tumor; arrow, retina; B, bone. B, cervical lymph node harvested at the time of death from a mousereceiving 5�105DM14 cells implantedwithin themaxillary sinus showsmetastasis.L, lymphnode;T, tumor.C, intracranial extensionof DM14 tumor implantedwithin the softpalate.T, tumor; S, base of skull; C, cerebrum. D, left lung from the mouse that received 5 � 105 DM14 cells in the soft palate shows extensive bulky tumor metastasis.T, tumor;A, alveoli. E, high-powermagnification of pulmonary metastasis from themouse pictured inD.T, tumor;A, alveoli;Bv, blood vessel. F, perineural invasion visualizedwithin the histologic sections of the lateral maxillary wall of an animal that received 5 � 105 DM14 cells implanted within the maxillary sinus. N, nerve;T, tumor;arrow, tumor spread along the interior of the perineurium.
CancerTherapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2008;14(22) November15, 2008 7352
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

orbital cavity (Fig. 3A). Tumors were not restricted to localinvasion and also showed regional metastasis to the cervicallymphatics (Fig. 3B). When 5 � 105 DM14 cells were implantedin the soft palate, mice developed tumors that invadedsuperiorly into the cranial vault (Fig. 3C). Tumors in the softpalate showed metastasis to the lungs (Fig. 3D and E).Additionally, tumors implanted in the maxillary sinus dis-played perineural invasion as evidenced on histologic sectionsfrom the lateral maxillary wall (Fig. 3F).
At sacrifice, the tumor volume measured in external cross-section was directly correlated with the implanted cellconcentration (Fig. 3G and H). For mice injected in the softpalate, differences between groups were statistically significant
in two comparisons (5 � 105 versus 5 � 104, P = 0.020; 5 � 105
versus 5 � 103, P = 0.001). Similar significant differences intumor volumes were seen between groups of mice injected inthe maxillary sinus (5 � 105 versus 5 � 104, P = 0.008; 5 � 105
versus 5 � 103, P = 0.001). Tumors growing in the maxillarysinus were of larger volume for all cell densities whencompared with tumors growing in the soft palate. Furtherinvestigation is needed on whether this difference was relatedto the physical restrictions imposed by the anatomy of the softpalate or microenvironmental cues.
For the human SCC cell line DM14, we observed a spectrumof tumorigenicity related to initial concentration and site ofinjection. These trends are described in Table 1.Human adenoid cystic tumor cell line ACC-3 forms tumors
when implanted orthotopically in either the maxillary sinus or thesoft palate. In initial survival studies and Kaplan-Meieranalysis of mice bearing cell line ACC-3 tumors in eitherthe maxillary sinus or soft palate, the median survival timewas 24 days (data not shown). When injected into themaxillary sinus, these mice developed bulky, large tumors(seen in coronal view; Fig. 4A) that also invaded the orbitaltissues (Fig. 4B) and showed infiltration and destruction ofthe bony paranasal sinus suprastructure (Fig. 4C). Similarly,when mice were injected in the soft palate, they developedbulky, large tumors (seen in sagittal view; Fig. 4D), whichshowed bone and intracranial invasion (Fig. 4E). When themice were euthanized on day 24, tumor volume measured inexternal cross-section was found to be directly correlated to thecell concentration in the tumor cell inoculum (Fig. 4F and G).When comparing the different volumes of the tumors in themaxillary sinus, we found significant differences in mean tumorvolume between groups receiving different tumor cell concen-trations: (5 � 105 versus 5 � 104, P = 0.006; 5 � 105 versus 5 �103, P = 0.008; 2 � 105 versus 5 � 104, P = 0.004; 2 � 105
versus 5 � 103, P < 0.0001). There was no evidence of asignificant difference between the mean volume of the 5 � 105
and 2 � 105 densities (P = 0.16) or between the 5 � 104 and5 � 103 cell concentration inocula (P = 0.071). Whencomparing volumes of the tumors in the soft palate, thedifference in mean tumor volume between groups of micereceiving 5 � 105 versus 5 � 103 cell density inocula was notsignificant (P = 0.056). However, a significant difference wasfound between the groups injected with cells at the 2 � 105 and5 � 103 densities (P = 0.023).Human adenoid cystic tumor cell line ACC-3 shows local tissue
invasion and regional and distant metastasis when injected intoeither the maxillary sinus or the soft palate of nude mice. Todetermine the reliability of our model in replicating thephenotype of human ACC, we examined the histologiccharacteristics of nude mice with the human tumor lineACC-3 implanted in their maxillary sinus and soft palate. Afterbeing sacrificed on day 24, mice that were injected with 5 � 105
ACC-3 cells in the soft palate developed tumors that locallyinvaded the soft palate and paranasal sinuses (Fig. 5A); theyalso showed perineural invasion and invasion inside thecranial vault (Fig. 5B). Histologic examination showed thatthese tumors compressed the medulla (Fig. 5C). Intracranialinvolvement was not restricted to tumors originating from cellsinjected into the soft palate. Mice bearing 5 � 104 ACC-3 cellsimplanted in the maxillary sinus also showed intracranialextension of tumor and brainstem compression in sagittal
Fig. 3. G, relationship between the injected tumor burden and the tumor volume(measured in mm3) at the time of death in mice that received DM14 (at variousconcentrations in 30 AL saline) injected into the soft palate. Differences werestatistically significant [5 � 105 versus 5 � 104 (P = 0.0020) and 5 � 105 versus5 � 103 (P = 0.0001)]. H, relationship between the injected tumor burden and thetumor volume (measured in mm3) at the time of death in mice that received DM14(at various concentrations in 30 AL saline) via injection into the maxillary sinus.Differences in final tumor volumes were statistically significant [5 � 105 versus5 � 104 (P = 0.0008) and 5 � 105 versus 5 � 103 (P = 0.0001)].
OrthotopicMurineModel of SinonasalMalignancy
www.aacrjournals.org Clin Cancer Res 2008;14(22) November15, 20087353
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

sections (Fig. 5D). When these cells were implanted in the softpalate, tumors showed upward extension and bony destructionthough the cribiform plate (Fig. 5E). When 5 � 105 ACC-3 cellswere implanted in the maxillary sinus, tumors extendedlaterally into the bony structures of the nasal and paranasalsinuses (Fig. 5F). Tumors showed capacity for distant spreadregardless of the injection site; mice with 5 � 105 cellsimplanted in the soft palate developed cervical lymph nodemetastasis (Fig. 5G) and mice with 5 � 105 cells implanted inthe maxillary sinus developed pulmonary metastasis (Fig. 5H).
Discussion
Our study is the first description of an orthotopic preclinicalmodel of sinonasal malignancy that closely mimics thebehavior of human disease. Our model shows extension intothe cranial vault, orbital invasion, perineural spread, anddistant metastasis. Using the human SCC line DM14 and theACC cell line ACC-3, our model manifests marked resemblanceto the phenotype and the malignant behavior of two ofthe most aggressive human tumor types that are seen inthis complex anatomic area.
Numerous retrospective studies have shown that tumor type,stage, and extent of direct extension are significant predictors ofpatient outcome. Multivariate analysis of 220 patients treatedbetween 1975 and 1994 showed that factors associated withworse 5-year carcinoma specific actuarial survival were tumorhistology, extension into the pterygomaxillary fossa, andinvasion of the dura (21). Another retrospective review of100 patients with sinonasal malignancies showed factorsassociated with worse 5-year survival to be recurrence followingcraniofacial tumor resection, involvement of the orbital softtissues, and invasion of the sphenoid sinus (22). A multivariatestudy of 334 patients from 17 institutions identified localinvasion into surrounding structures with worse outcome.Additionally, surgical margins, histology, and the intracranialextent of tumor were independent predictors of overall, disease-specific, and recurrence-free survival (23). Clinical experiencewith human disease strongly suggests an intrinsic relationshipbetween survival and extent of local spread, bone invasion, andperineural spread. For any animal model to accuratelyrecapitulate this disease, it must reliably and reproduciblyshow these characteristics.
A hallmark of orthotopic cancer models is the ability tomodel the disseminated metastasis seen in human cancer.Subcutaneous models are a valuable tool, but they are limited
by a lymphatic drainage and vascular supply that are vastlydifferent than those of the orthotopic site (24). Thus,subcutaneous xenografts cannot reproduce the patterns ofregional and distant metastasis that are characteristic ofsinonasal cancers. Additionally, the differences in the stromalcellular composition and the extracellular matrix between theorthotopic and subcutaneous microenvironments contribute tothe extremely low metastatic rates of subcutaneously estab-lished tumors. Therefore, orthotopic models of highly meta-static cancers have been established in nude mice forcarcinomas of the colon, stomach, pancreas, breast, bladder,lung, thyroid, and tongue (7, 24–29). Similarly, our orthotopicmodel of sinonasal malignancy provides an experimentalsystem for exploring the events associated with metastasiswithin both the regional draining lymphatic basin and indistant sites.
Orthotopic models of cancer are also able to reproduce thesite-specific spectrum of clinical findings and thereby permitanalysis of the effects these findings have on survival. As seen inpatients with malignant sinonasal tumors, our orthotopicallygenerated sinonasal tumors in nude mice reproduciblypenetrated the cranial vault, invaded the orbit, and spreadthrough bone and perineurium within 18 to 30 days after thetumor cells were implanted. This model can now be used toinvestigate the genetic and molecular aberrations that may serveas a novel substrate for targeted therapeutic strategies. Thesetherapies must be able to specifically address the characteristicsthat render these malignancies clinically aggressive.
Rapid progress has been made in our understanding of themolecular alterations contributing to the development of SCCarising outside the sinonasal tract (30). As evidenced by thediscovery of epidermal growth factor receptor signaling in headand neck cancer, targeting aberrant molecular pathways hasbeen directly translated into tangible patient benefit (31, 32).However, our understanding of the molecular biology ofsinonasal malignancies and their potential for molecularlytargeted therapy has not yet been able to reap the full benefitof current research efforts centered on disease outside thesinonasal cavity. Our model offers a mechanism to applyseveral of the well-established molecular therapeutics to amalignancy with precious few therapeutic options.
Our model offers a validated preclinical tool to test ifSCC and ACC arising in the sinonasal cavity can besuccessfully treated with reagents targeting specific molecularpathways. These include drugs targeting growth factors andtheir receptors, signal transduction molecules, oncogenes,
Table 1. Relationship between initial tumor burden and orbital invasion, bone invasion, intracranial extension,and perineural invasion in mice with DM14 implanted in either the maxillary sinus or soft palate
Initial tumor burden Orbital invasion (%) Bone invasion (%) Intracranial invasion (%) Nasal cavity (%)
Maxillary sinus5 � 105 100 100 60 1002 � 105 80 80 60 605 � 104 80 100 60 605 � 103 0 0 0 0
Soft palate5 � 105 100 100 80 802 � 105 100 100 80 805 � 104 60 60 60 405 � 103 0 0 0 0
CancerTherapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2008;14(22) November15, 2008 7354
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

hormones, apoptosis-related molecules, angiogenesis-relatedfactors, as well as inhibitors of cell motility, invasion, andproteolysis. Decreased tumor size coupled with reductions inperineural invasion and lymphatic and pulmonary metastasis
following therapy can serve as quantitative endpoints forefficacy evaluation.
Beyond the established reagents for epidermal growth factorreceptor (33), small-molecule inhibitors of nuclear factor-nB
Fig. 4. Orthotopic mouse model of ACC of the paranasal sinuses. A, coronal stained section of a mouse that received 5 � 105 ACC-3 cells implanted within the maxillarysinus. Star, epicenter of tumor; arrows, pattern of spread; O, retro-orbital musculature; arrowheads, invasion of bony medial orbital wall by tumor;m, mandible; t, tongue;S, contralateral uninvolved sinus. B, magnified (�20) histologic section shows the orbital invasionwith tumor (T) surrounding the optic nerve (O).Arrowhead, medial orbitalwall and orbital musculature. C, higher-power (�20) coronal H&E section showing tumor (T) infiltration and destruction of the bony paranasal sinus suprastructure.Arrowhead, normal sinus mucosa. D, sagittal H&E section from a mouse that received 5 � 105 ACC-3 cells implanted in the soft palate. Star, tumor epicenter; B, brain; E,erosion of skull base; arrow, hard palate; arrowhead, hard palatemucosa; t, tongue. E, on a higher-powered view (�40) of the same animal, tumors (T) showed invasion anddestruction of the bony anterior skull base (Sb), brain (arrowhead), and oropharyngeal mucosa (Om). O, oropharynx for reference. F, relationship between the injectedtumor burden and tumor volume (measured in mm3) at the time of death in mice that received human adenoid cystic tumor lineACC-3 (at various concentrations in 30 ALsaline) injected into the maxillary sinus. MeanF SD of 5 mice from each group.The mean tumor volumes were significantly different depending on the density of cellsused for tumor implantation: 5 � 105 versus 5 � 104 (P = 0.006), 5 � 105 versus 5 � 103 (P = 0.008), 5 � 105 versus 2� 104 (P = 0.004), and 2 � 105 versus 5 � 103
(P < 0.0001).There was no evidence of a significant difference between the mean volume of tumors in mice implanted with 5 � 105 and 2 � 105 cell densities (P = 0.16) or5� 104 and 5� 103cell densities (P = 0.071).G, relationship between injected tumor burden and tumor volume (measured in mm3) at the time of death inmice that receivedhuman adenoid cystic tumor lineACC-3 (at various concentrations in 30 AL saline) injected into the soft palate. MeanF SD of 5 mice from each group.The difference inmeanvolume of tumors growing from cells implanted at densities of 5�105 and 5�103was not significant (P = 0.056). However, a significant differencewas foundbetweenthe volumes of tumors from 2 � 105 and 5 � 103 cell density inoculations (P = 0.023).
OrthotopicMurineModel of SinonasalMalignancy
www.aacrjournals.org Clin Cancer Res 2008;14(22) November15, 20087355
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

(34), farnesyl transferase inhibitors that inhibit the rasoncogene and its downstream mediators (35), small moleculestargeting signal transducers and activator of transcription3 (36), antisense oligonucleotides targeting human telomer-ase reverse transcriptase mRNA (37), and angiogenesis inhib-itors (38, 39) can all be rapidly tested with the model describedin this work.
Additionally, given that the degree of direct extension is asignificant predictor of patient outcomes in sinonasal malig-nancy, reagents designed to limit this process may influencepatient survival. Studies of epithelial malignancies haveconsistently shown that loss of cell adhesion and theacquisition of mesenchymal features, a process termed epithe-lial-mesenchymal transition, precede their invasion and pro-gression. Epithelial-mesenchymal transition is a complexprocess induced by modifications of multiple pathwaysleading to a spectrum of epithelial cellular changes includingloss of polarity and cohesion, increased motility, and acquisi-tion of mesenchymal phenotype. Of these pathways, theprotein tyrosine kinase Src is a common target of differentgrowth factor receptor activation in epithelial-mesenchymaltransition (40). Preclinical evaluations have shown a strongrationale for targeting Src in head and neck SCC (41, 42). Othertargets involved in extracellular matrix proteolysis, includingmatrix metalloproteinases and urokinase-type plasminogenactivator and its receptor may prove fruitful lines of researchas well.
Beyond the application of established therapies, our modelmay also allow for selective targeting of novel pathwaysassociated with tumorigenesis. One recent example is the role
of h-catenin signaling in the cancer stem cells postulated to befundamental to SCC growth, invasion, and metastasis (43). Inthis exciting new work, the authors show multiple commonmolecular characteristics of both cancer stem cells andnonmalignant skin stem cells. Interestingly however, cancerstem cells were critically dependent on highly active h-cateninsignaling and unique in their ability to initiate tumors wheninjected, at a very low number, into mice. Silencing h-cateninsignaling led to the regression of skin tumors while leavingnormal skin homeostasis apparently untouched, thus providinga strong rationale for therapeutic targeting of h-catenin in SCCarising within the sinonasal tract.
Orthotopic nude mouse models allow dissection of themolecular and cellular mechanisms of tumor growth andmetastasis (44). They serve a critical role in identifying safeand effective therapies. Yet, nude mouse models are notwithout limitations. Insights gleaned from these modelsneed additional substantiation from complementary studiesin immunocompetent models coupled with analysis ofarchival human tumor specimens. Together, these studiesmay generate insight into the pathogenesis and molecularbiology of sinonasal cancer. They also may provide theinformation critical to preclinical assessment of new drugsdesigned to combat a diverse and aggressive subset ofmalignancies.
We have developed an orthotopic model of sinonasalcancer in nude mice that reproduces the clinical andpathologic features of sinonasal malignancy in humans.Our model is technically feasible and can be used withmultiple human tumor xenografts. The model should allow
Fig. 5. Malignant features of the human adenoid cystic tumor cell lineACC-3 implanted in the maxillary sinus and soft palate. A, when euthanized on day 24, mice thatreceived inoculations of 5 � 105 ACC-3 cells in the soft palate developed tumors (T) that locally invaded the soft palate and paranasal sinuses. B, bony hard palate;M, soft palate musculature; Om, oropharyngeal mucosa. O, oropharynx for reference. B, tumors (T) implanted in the soft palate exhibited perineural invasion (N) anddestruction of the bony anterior skull base (Sb) leading to extension (arrow) of the tumor inside the cranial vault (star). t, tongue; B, brain for reference. C, when5� 105 ACC-3 cells were implanted in the soft palate, mice developed tumors that compressed the brainstem. Histologic examination showed the tumor (T) eroding throughthe bony anterior skull base (B) and compressing the medulla (M). D, intracranial involvement was not restricted to the soft palate injection site. Mice bearing 5 � 104
ACC-3 cells implanted in the maxillary sinus also showed intracranial involvement by tumor (T) and brainstem (B) compression. E, when the cell line was implanted in themaxillary sinus, tumors showed upward extension and bony destruction though the cribiform plate (stars, sheets of tumor cells). F, tumors (T) in the maxillary sinus alsoextended laterally into the bony structures of the nasal and paranasal sinuses.M, normal mucosa.G, tumors were not restricted to local invasion.When 5� 105 cells/AL wereinjected in the soft palate, mice developed cervical lymph node metastasis (star). L, uninvolved portion of lymph node.H, metastatic behavior was not unique to the softpalate.When 5� 105 ACC-3 cells/AL were implanted in the maxillary sinus, mice developed pulmonary metastasis (star). A, alveoli; P, pulmonary parenchyma.
CancerTherapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2008;14(22) November15, 2008 7356
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

further studies that enhance our understanding of themolecular and cellular mechanisms underlying the pathogen-esis of sinonasal malignancy. We believe our model willfacilitate the development and evaluation of new therapiesfor a disease subset whose rarity leads to difficulty inaccruing sufficient patients to adequately power large humantrials.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
We thank Kristi M. Speights for excellent editorial assistance.
References1. Barnes L. Surgical pathology of the head and neck.2nd ed. NewYork: Marcel Dekker; 2001.2.RiceDS. Surgical therapy of the nasal cavity, ethmoidsinus and maxillary sinus tumors. In: Thawley SE,PanjeW, BatsakisJ, Lindberg, R, editors. Comprehen-sive management of head and neck tumors. 2nd ed.Philadelphia:WBSaunders; 1999.3. Roush GC. Epidemiology of cancer of the nose andparanasal sinuses: current concepts. Head Neck Surg1979;2:3^11.4.ConstantinoMM. Cancer of the nasal vestibule, nasalcavity, and paranasal sinusLsurgicalmanagement. In:Harrison RSL, HongW, editors. Head andneck cancer,a multidisciplinary approach. 2nd ed. Philadelphia:LippincottWilliams &Wilkins; 2004.5.McKay SP, ShibuyaTY, ArmstrongWB, et al. Cell car-cinoma of the paranasal sinuses and skull base. AmJOtolaryngol 2007;28:294^301.6.Camphausen K, Purow B, Sproull M, et al. Influ-ence of in vivo growth on human glioma cellline gene expression: convergent profiles underorthotopic conditions. Proc Natl Acad Sci U SA 2005;102:8287^92.7. NakamuraT, Fidler IJ, Coombes KR. Gene expressionprofile of metastatic human pancreatic cancer cellsdepends on the organ microenvironment. Cancer Res2007;67:139^48.8. Zaitseva M,Vollenhoven BJ, Rogers PA. In vitro cul-ture significantly alters gene expression profiles andreduces differences between myometrial and fibroidsmooth muscle cells. Mol Hum Reprod 2006;12:187^207.9. Deschavanne PJ, Fertil B. A review of human cell ra-diosensitivity in vitro. Int J Radiat Oncol Biol Phys1996;34:251^66.10. Kenny PA, Bissell MJ.Tumor reversion: correctionofmalignant behavior by microenvironmental cues. Int JCancer 2003;107:688^95.11. HaraY, OgataY, Shirouzu K. Early tumor growth inmetastatic organs influenced by the microenviron-ment is an important factor which provides organspecificity of colon cancer metastasis. JExp ClinCan-cer Res 2000;19:497^504.12. Camphausen K, Purow B, Sproull M, et al.Orthotopic growth of human glioma cells quantita-tively and qualitatively influences radiation-inducedchanges in gene expression. Cancer Res 2005;65:10389^93.13. Fidler IJ,Wilmanns C, Staroselsky A, Radinsky R,Dong Z, Fan D. Modulation of tumor cell response tochemotherapy by the organ environment. CancerMe-tastasis Rev1994;13:209^22.14. Dong Z, Radinsky R, Fan D, et al. Organ-specificmodulation of steady-state mdr gene expression anddrug resistance in murine colon cancer cells. J NatlCancer Inst 1994;86:913^20.15. Fidler IJ. Rationale and methods for the use of nudemice to study the biology and therapy of human cancermetastasis. CancerMetastasis Rev1986;5:29^49.
16. Hoffman RM. Orthotopic is orthodox: why areorthotopic-transplant metastatic models differentfrom all other models? JCell Biochem1994;56:1^3.17. Baia GS, Dinca EB, OzawaT, et al. An orthotopicskull base model of malignant meningioma. BrainPathol 2007;18:172^9.18.TakadaY, NoguchiT, OkabeT, Kajiyama M. Superox-ide dismutase in various tissues from rabbits bearingtheVx-2 carcinoma in the maxillary sinus. Cancer Res1982;42:4233^5.19. YuraY,Tsujimoto H, Kusaka J, Harada K,Yoshida H,Sato M. Induction of carcinomas and sarcomas by9,10-dimethyl-1,2-benzanthracene administration intothe hamster maxillary sinus. J Oral Pathol Med 1995;24:120^4.20. He RG, Zhang XS,Wang Z, Zhang XL, QiuWL.Theestablishment of cell lines of adenoid cystic carcinomaof human salivary glands (Acc-2, Acc-3) and a studyof morphology.West ChinJ Stomatol 1988;6:1^4.21. Dulguerov P, Jacobsen MS, Allal AS, LehmannW,CalcaterraT. Nasal and paranasal sinus carcinoma: arewe making progress? A series of 220 patients and asystematic review. Cancer 2001;92:3012^29.22. Suarez C, Llorente JL, Fernandez De Leon R,Maseda E, Lopez A. Prognostic factors in sinonasaltumors involving the anterior skull base. Head Neck2004;26:136^44.23. Ganly I, Patel SG, Singh B, et al. Craniofacial resec-tion for malignant paranasal sinus tumors: report of aninternational collaborative study. Head Neck 2005;27:575^84.24. Kim S, Park YW, Schiff BA, et al. An orthotopicmodel of anaplastic thyroid carcinoma in athymicnudemice. Clin Cancer Res 2005;11:1713^21.25. Fu XY, Besterman JM, MonosovA, Hoffman RM.Models of human metastatic colon cancer in nudemice orthotopically constructed by using histological-ly intact patient specimens. Proc Natl Acad Sci U S A1991;88:9345^9.26. FurukawaT, Fu X, KubotaT,Watanabe M, KitajimaM, Hoffman RM. Nude mouse metastatic models ofhuman stomach cancer constructed using orthotopicimplantation of histologically intact tissue. Cancer Res1993;53:1204^8.27. Oshinsky GS, ChenY, JarrettT, Anderson AE,WeissGH. A model of bladder tumor xenografts in the nuderat. JUrol 1995;154:1925^9.28. Onn A, IsobeT, Itasaka S, et al. Development of anorthotopic model to study the biology and therapy ofprimary human lung cancer in nude mice. Clin CancerRes 2003;9:5532^9.29. Myers JN, Holsinger FC, Jasser SA, Bekele BN,Fidler IJ. An orthotopic nude mouse model of oraltongue squamous cell carcinoma. Clin Cancer Res2002;8:293^8.30. Choi S, Myers JN. Molecular pathogenesis of oralsquamous cell carcinoma: implications for therapy.JDent Res 2008;87:14^32.31. Burtness B, Goldwasser MA, Flood W, Mattar B,
Forastiere AA. Phase III randomized trial of cisplatinplus placebo compared with cisplatin plus cetuximabin metastatic/recurrent head and neck cancer: anEastern Cooperative Oncology Group study. J ClinOncol 2005;23:8646^54.32. Bonner JA, Harari PM, Giralt J, et al. Radiotherapyplus cetuximab for squamous-cell carcinoma of thehead and neck. NEnglJMed 2006;354:567^78.33. Caponigro F, MilanoA, OttaianoA, Iaffaioli RV. Epi-dermal growth factor receptor as a major anticancerdrug target. ExpertOpinTherTargets2006;10:877^88.34. Rehman AO,Wang CY. SDF-1apromotes invasionof head and neck squamous cell carcinoma by activat-ing NF-nB. JBiol Chem 2008;283:19888^94.35. Takada Y, Khuri FR, Aggarwal BB. Proteinfarnesyltransferase inhibitor (SCH 66336) abolishesNF-nB activation induced by various carcinogensand inflammatory stimuli leading to suppression ofNF-nB-regulated gene expression and up-regulationofapoptosis. JBiol Chem2004;279:26287^99.36. Leeman RJ, LuiVW, Grandis JR. STAT3 as a thera-peutic target in head and neck cancer. Expert OpinBiolTher 2006;6:231^41.37.Tao Z, Chen S,Wu Z, Xiao B, LiuJ, HouW.Targetedtherapy of human laryngeal squamous cell carcinomain vitro by antisense oligonucleotides directed againsttelomerase reverse transcriptase mRNA. J LaryngolOtol 2005;119:92^6.38. Sano D, Kawakami M, Fujita K, et al. Antitumoreffects of ZD6474 on head and neck squamous cellcarcinoma. Oncol Rep 2007;17:289^95.39. Fujita K, Sano D, KimuraM, et al. Anti-tumor effectsof bevacizumab in combination with paclitaxel onhead and neck squamous cell carcinoma. Oncol Rep2007;18:47^51.40. Kornberg L, Earp HS, Parsons JT, Schaller M,Juliano RL. Cell adhesion or integrin clusteringincreases phosphorylation of a focal adhesion-as-sociated tyrosine kinase. J Biol Chem 1992;267:23439^42.41. Johnson FM, Saigal B,Talpaz M, Donato NJ. Dasa-tinib (BMS-354825) tyrosine kinase inhibitor sup-presses invasion and induces cell cycle arrest andapoptosis of head and neck squamous cell carcinomaand non-small cell lung cancer cells. Clin Cancer Res2005;11:6924^32.42.Mandal M, Myers JN, Lippman SM, et al. Epithelialto mesenchymal transition in head and neck squa-mous carcinoma: association of Src activation withE-cadherin down-regulation, vimentin expression,and aggressive tumor features. Cancer 2008;112:2088^100.43. Malanchi I, Peinado H, Kassen D, et al. Cutaneouscancer stem cell maintenance is dependent on h-cat-enin signalling. Nature 2008;452:650^3.44. Killion JJ, Radinsky R, Fidler IJ. Orthotopic modelsare necessary to predict therapy of transplantabletumors in mice. Cancer Metastasis Rev 1998;17:279^84.
OrthotopicMurineModel of SinonasalMalignancy
www.aacrjournals.org Clin Cancer Res 2008;14(22) November15, 20087357
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2008;14:7348-7357. Clin Cancer Res Alexander Gelbard, Michael E. Kupferman, Samar A. Jasser, et al. An Orthotopic Murine Model of Sinonasal Malignancy
Updated version
http://clincancerres.aacrjournals.org/content/14/22/7348
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/14/22/7348.full#ref-list-1
This article cites 40 articles, 13 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/14/22/7348.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/14/22/7348To request permission to re-use all or part of this article, use this link
Research. on March 28, 2021. © 2008 American Association for Cancerclincancerres.aacrjournals.org Downloaded from