Embed Size (px)
Citation preview

ANTELOPE VALLEY COLLEGE
ASSOCIATE DEGREE
NURSING PROGRAM
REVISED: 5/09 UPDATED: 6/09, 12/09, 7/10, 12/10, 7/11, 11/11, 1/12, 5/12, 11/12, 5/13, 11/13, 5/14, 12/14
Mandatory Resource Manual
(The ADN Student Survival Kit)
INTERSESSION/SPRING 2015
1
TABLE OF CONTENTS
PAGE NO. Module 1 Philosophy/Conceptual Framework 4 Module 2 Policies and Regulations 14 Module 3 Nursing Theory 34
Assessment Guides 50 Module 4 Nursing Process and Nursing Care Plans 68
Nursing Diagnoses: Universal 73
Nursing Diagnoses: Developmental 76
Nursing Diagnoses: Health-Deviation 77 Module 5 Survival Skills 102
Strategies for Answering Multiple Choice Questions 105
Test Taking Strategies 113
Make Notes for Studying 118
Study Groups 121 Module 6 Math for Nurses 124
2
ANTELOPE VALLEY COLLEGE
ASSOCIATE DEGREE NURSING PROGRAM
ADMINISTRATION Office Phone Number Dr. Karen Cowell HS 190 661-722-6300, Ext. 6402 Dean, Career Technical Education
STAFF Sylvia Waller HS 198 661-722-6300, Ext. 6402 Clerical Assistant III Karen Smith HS 188 661-722-6300, Ext. 6193 Coordinator
FACULTY Victoria Beatty HS 228 661-722-6300, Ext. 6410 Instructor
Bonnell Curry HS 226 661-722-6300, Ext. 6405 Assistant Professor
Debra Dickinson HS 222 661-722-6300, Ext. 6406 Assistant Professor
Linda Harmon HS 220 661-722-6300, Ext. 6748 Instructor
Sandra Hughes HS 218 661-722-6300, Ext. 6407 Associate Professor Annette Jones HS 202 661-722-6300, Ext. 6118 Instructor Candace Martin HS 200 661-722-6300, Ext. 6408 Assistant Professor
Sandra Robinson HS 214 661-722-6300, Ext. 6412 Associate Professor
Dr. Casey Scudmore HS 212 661-722-6300, Ext. 6847 Professor
Susan Snyder HS 210 661-722-6300, Ext. 6017 Instructor Marianne Stewart HS 208 661-722-6300, Ext. 6413 Professor
Elizabeth Sundberg HS 206 661-722-6300, Ext. 6414 Professor
L. Denise Walker HS 204 661-722-6300, Ext. 6026 Instructor

3
PURPOSE OF MANUAL The purpose of this manual is to provide information and guidance to students in the Associate Degree Nursing Program. Faculty will post updated manuals online each semester and will reinforce any changes with the students. The students are responsible for reviewing the manual and noting any changes. Material and information in this manual will be referred to throughout the Associate Degree Nursing Program. This manual was written by the Associate Degree Nursing faculty and cannot be reproduced without their permission.

4
MODULE 1
PHILOSOPHY AND CONCEPTUAL FRAMEWORK
5
ANTELOPE VALLEY COLLEGE ASSOCIATE DEGREE NURSING PHILOSOPHY The nursing faculty of Antelope Valley College believes that people are spiritual, psycho-socio-physiological beings who are rational and responsible for themselves. People exist in an environment that contains biological, physical, psychological, social, developmental, cultural and spiritual components. Individuals are constantly in interaction with their environment. People are affected by, and respond to the environment by acting upon self, society, and all aspects of the environment. Health is a state of wholeness or integrity of individuals. It includes mental, biological, interpersonal, cultural, social, and spiritual well-being. Health is a dynamic state and is relative to the environment of individuals. Illness is viewed as a deviation from norms established by individuals and the environment. Health and illness are viewed as a continuum from optimal wellness to severe illness. Birth to death is viewed as a developmental continuum. These two continua intersect at any point on either continuum. The philosophy of the nursing program at Antelope Valley College is based upon Dorothea Orem’s Self-Care Theory that defines nursing as the creative effort of one human being to help another. This faculty believes that nursing practice, through the self-care approach, has a unique contribution to make to society. The condition that validates the requirement for nursing is the presence of health-related action limitations. These limitations impair the ability to maintain the amount and quality of self-care that is therapeutic in sustaining life, health and well-being, in recovering from illness or injury, or in coping with the effects of health and illness. The nurse-patient relationship is contractual and complimentary. The goal of nursing is to maximize the full capacities of the individual to achieve and maintain their optimal health. The goal of the Associate Degree Nursing Program at Antelope Valley College is to prepare students for entry-level practice in the nursing profession. The program fosters the intellectual, personal and professional development of the students and provides an educational foundation for articulation with universities and colleges. The faculty believes in career ladder mobility and encourages Licensed Vocational Nurses to enter the program. In this program, both the faculty and students contribute and share in the learning experience. The faculty believes that its responsibility is to provide an environment conducive to learning, to plan learning experiences, to provide direction, to act as a resource person, to offer feedback and to stimulate critical thinking. Students learn best in an atmosphere where there is a high regard for the individual and a deep respect for human dignity. Learning is the acquisition of knowledge, skill and professional attitude throughout the educative process. This occurs within the learner and occurs optimally when students assume responsibility and accountability for themselves, participate in all activities, utilize all available resources and conduct continuous self-evaluations along with faculty evaluations. This shared approach to learning affords students the opportunities to attain mastery. The faculty believes that diversity enriches the students and faculty and enhances the nurse-patient relationship. Students in a community college reflect a variety in learning styles; therefore the nursing program utilizes various methodologies to facilitate learning. Instruction progresses
6
PHILOSOPHY (CONTINUED) from the general to the specific, the usual to the unusual, and the simple to the complex, to provide for transfer of principles, in part or whole, to other situations. The faculty conducts ongoing evaluations of the curriculum in response to diverse and changing community needs. Nursing education integrates other disciplines in the arts and sciences. It is based on the premise that nurse agency results from cognitive knowledge, understanding of affective feelings, and development of psychomotor skills. Knowledge essential for use in nursing practice includes knowledge of: (1) all aspects of the person, (2) nursing as a professional and an occupation, including legal consideration, (3) nursing history, (4) nursing ethics, (5) nursing sciences and (6) interdisciplinary theories with an emphasis on Maslow’s hierarchy of needs and Erickson’s theory of development. The Associate Degree Registered Nurse functions within a structured healthcare setting and is responsible for the management of patients and their self-care deficits. General management activities required to provide care to patients include: communication and collaboration among health team members, priority setting, delegation of patient care, supervision of patient care, and patient and family education.
7
CONCEPTUAL FRAMEWORK
The conceptual framework of the Antelope Valley College Associate Degree Nursing Program is based upon the self-care theory of Dorothea E. Orem. Inherent in this theory is the belief that people are rational and responsible for themselves. The ultimate responsibility for the state of health or illness rests with individuals. Patients are the primary decision-makers in matters related to their health care. Self-care can be defined as the practice of the activities that individuals initiate and perform on their own behalf or on the behalf of dependents in maintaining life, health and well-being. All people have common requirements to meet basic human needs. The requirements to meet basic human needs are called requisites by Dorothea E. Orem. She describes three sets of self-care requisites: universal self-care requisites, developmental self-care requisites and health deviation self-care requisites. The universal self-care requisites are common to all persons during all stages of the life cycle. They encompass the needs for air, water, food, rest/activity, elimination, safety, solitude and social interaction and a realistic self-concept. Developmental self-care requisites are those associated with the developmental process and events occurring throughout the life cycle. There are two categories of developmental requisites. There are maturational self-care requisites and situational self-care requisites. Health deviation self-care requisites are those requisites associated with structural and functional defects or deviations and their effects before, during and after medical diagnosis and treatment. They include the need to seek /secure medical assistance with exposure/evidence of conditions associated with pathology, be aware/attend to effects of pathological states, carry out medically prescribed measures to prevention/regulation/ compensation for pathology, be aware/attend to/regulate discomforting/deleterious effects of prescribed measures, modify self-concept in acceptance of particular state, learn to live with effects of health state and/or prescribed measures so that the lifestyle promotes personal development. Self-care requisites are individualized by the basic conditioning factors, which include: age, gender, developmental state, relevant life experiences, health state, health system requirements, socio-cultural orientation and available resources. The self-care requisites, influenced by the basic conditioning factors, result in therapeutic self-care demands. A therapeutic self-care demand is the sum total of the actions needed to be performed in order to meet a known self-care requisite. Agency is the knowledge, power and ability of persons to act. It includes cognitive knowledge, affective feelings and psychomotor development. Self-care Agency is the ability of individuals to initiate and perform health activities for themselves in order to maintain life, health and well-being. Self-care agency includes the power components. These are specific abilities required by individuals to engage in self-care. They include: awareness of self and surroundings, physical energy, ability to reason, motivation, ability to control movement, ability to make decisions, ability to gain and use knowledge, knowledge of required skills, ability to set priorities and ability to perform self-care actions continuously. These abilities are influenced by the basic conditioning factors. Those who cannot provide for their own self-care in relation to therapeutic self-care demands require assistance from another agent. The provider of infant care, child care or dependent adult care is referred to as a dependent-care agent. When the self-care agency is unable or unwilling to meet the therapeutic self-care demand, a self-care deficit exists. The self-care deficit is health related. Health is a dynamic state of wholeness or integrity of the individual and is relative to an individual’s environment. Illness is a dynamic deviation from norms established by individuals and society. Health and illness are viewed as a continuum. The continuum is developmental, as it begins with birth and ends with death. The health-illness continuum and the birth-death continuum are constantly perpendicular to each other so that people can fluctuate between optimal wellness and acute illness at any point in their life.
8
CONCEPTUAL FRAMEWORK (CONTINUED) When a self-care deficit exists there is a need for nursing. Nursing has as its special concern individuals’ needs for self-care. The management of these needs assists individuals to sustain life and health, recover from illness or injury and cope with the effects of health and illness. A nurse-patient relationship exists when an individual, family member or significant other seeks nursing care either directly or indirectly through the health care system. This complementary relationship requires that the nurse act to help patients assume responsibility for their health related self-care.
Nursing agency is composed of specialized abilities that enable nurses to provide care that compensates for or aids in overcoming self-care deficits. The nursing agency of individual nurses varies with the extent and depth of their clinical experience and educational preparation. Nursing responsibility is to determine with the patient the patient’s therapeutic self-care demands, the patient’s ability or inability to meet these demands and the self-care deficits. Through the nursing process a nursing system of care is designed. The nurse determines the nursing system based upon the identified self-care deficits. There are three types of nursing systems: wholly compensatory in which the nurse assumes responsibility for providing all physical care to the patient; partly compensatory in which the nurse and the patient have a shared responsibility for the patient’s physical care; and supportive educative in which the nurse performs only in a consultative/educative role. The use of a nursing system will involve the application of one or more methods of assisting. These include: (1) acting for the patient, (2) teaching, (3) guiding, (4) supporting and (5) providing a developmental environment. Nursing process is a process of determining why a person needs nursing, designing a system of nursing assistance, planning for the delivery of the specified nursing assistance and providing and controlling the delivery of nursing assistance. The nursing process has five steps: (1) assessment, (2) diagnosis, (3) planning, (4) implementation and (5) evaluation. This results in a plan of care including identifying the self-care deficit, the goals and the actions. Nursing prudence enables the nurse to initiate, conduct and control actions to carry out the plan and evaluate nursing care to determine the effectiveness of the care provided. The faculty of Antelope Valley College Associate Degree Nursing Program believes that if nurses follow the principles of self-care deficit theory, the profession and patients will benefit.

9
FIGURE 1
SELF-CARE AGENCY AS AN OPEN SYSTEM
External Environment
Knowledge
Affective
Psychomotor
Basic Conditioning Factors
Internal Environment
10
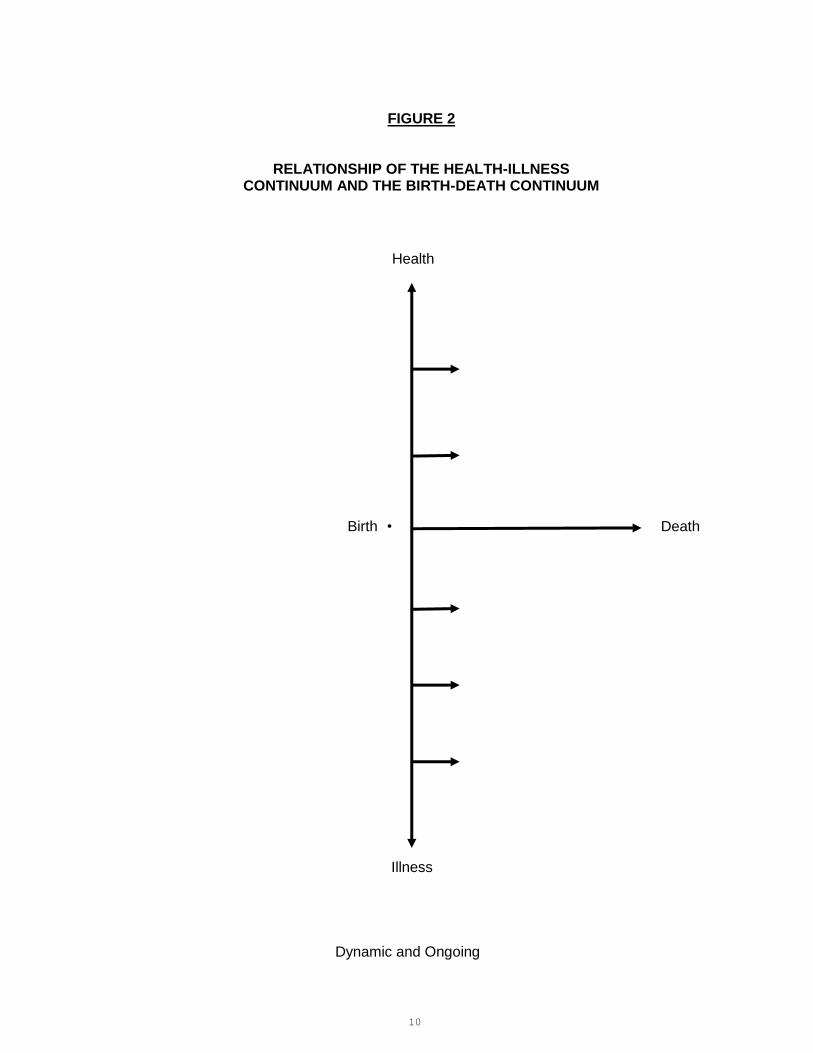
FIGURE 2
RELATIONSHIP OF THE HEALTH-ILLNESS CONTINUUM AND THE BIRTH-DEATH CONTINUUM
Illness
Dynamic and Ongoing
Health
Death Birth •

11
ASSOCIATE DEGREE NURSING LEVEL OBJECTIVES
1ST LEVEL OBJECTIVE 2ND LEVEL OBJECTIVE (PROGRAM OBJECTIVE)
Upon completion of the first year of the Associate Degree Nursing Program, the student will:
Upon completion of the Associate Degree Nursing Program, the graduate will:
1.
Apply legal, ethical, and regulatory framework of nursing and standards of professional nursing practice with instructional guidance.
Practice nursing within legal, ethical and regulatory frameworks of nursing and standards of professional nursing practice.
2.
Apply principles of therapeutic and social communi-cation to establish professional relationships with patients and significant others with instructional guidance.
Utilize therapeutic communication to establish therapeutic relationships with patients and significant others.
3.
Practice the student role in advocating for patients’ and significant others’ rights.
Advocate for the rights of patients and significant others.
4.
Use the nursing process to safely care for one to two patients; reports and documents accurate patient information in a timely professional manner under the guidance of an instructor.
Use the nursing process to safely care for patients in a supervised, controlled situation; reports and documents appropriate patient information in a timely professional manner.
5.
Demonstrate caring behavior towards the patient, significant other(s), peers, and other members of the health care team respecting human diversity.
Demonstrate caring behavior towards the patient, significant other(s), peers, and other members of the health care team, providing an environment that respects human rights, values, and cultural and spiritual beliefs.
6.
Apply theory to make appropriate clinical decisions.
Use critical thinking to provide the foundation for appropriate clinical decision making.
7.
Utilize information technology with guidance to support and communicate the planning and provision of patient care.
Utilize information technology to support and communicate the planning and provision of patient care.
8.
Apply the principles of growth and development to the delivery of nursing care to patients across the lifespan with instructional guidance.
Consistently apply the principles of growth and development to the delivery of nursing care to patients across the lifespan.
9.
Teach the patient and significant other(s) the information and skills needed to meet the patient’s self-care demands to improve self-care agency.
Design and implement an individualized teaching plan for the patient and significant other(s) to meet the patient’s self-care demands to improve self-care agency.
10.
Recognize the need for collaboration in the decision making process with the patient, significant other(s), and members of the health care team.
Facilitate the decision making process by collaborating with the patient, significant other(s), and other members of the healthcare team.
11.
Demonstrate accountability for nursing care given by self.
Demonstrate accountability for nursing care given by self and/or delegated to others.
12.
Recognize the need for lifelong learning and professional development in nursing.
Promote excellence in nursing by pursuing lifelong learning and professional development.

12
PURPOSE Antelope Valley College prepares students as Vocational Nurses and/or Associate Degree Nurses in order to help meet the health care needs of the community. These health care needs are met in the following ways:
(1) The graduates help the local agencies to meet the demands for nursing personnel.
(2) The graduates perform as members of the health care team.
(3) By implementing self-care theory in nursing practice, the graduates improve the quality of nursing care in the community.
13
ASSOCIATE DEGREE NURSING
PROGRAM OBJECTIVES Knowledge/skill acquisition and application of nursing principles are stressed throughout the learning experience. Students are afforded opportunities to apply knowledge in a variety of clinical settings and interact with patients throughout the life span. Learning experiences are structured from general to specific in terms of degree of complexity. Instruction is presented through didactic and experiential modes. Skills are introduced in the learning laboratory under instructor supervision, including demonstration and return demonstration by students. In the clinical setting students apply knowledge and skill in provision of nursing care to assigned patients. Throughout the learning process, nursing knowledge and skills are reinforced through continuous application, review and evaluation in the classroom and clinical setting.

14
MODULE 2 POLICIES AND REGULATIONS

15
POLICIES AFFECTING DRESS
CLASSROOM ATTIRE ON CAMPUS
The student will follow the policy of Antelope Valley College: No Shirt, No Shoes, No Service.
Nursing students are representatives of their profession. They should be aware of their physical appearance and their interpersonal conduct when engaged in the educational activities of the program. UNIFORM REQUIREMENTS FOR CLINICAL SITES
Students must wear the approved student uniform to the hospital and clinical agencies. The uniform consists of a white top, candy blue pants and a candy blue jacket (optional). The jacket and top will be embroidered with the program name on the right upper side of the uniform. A school patch (purchased from the Marauder Bookstore) must be affixed and centered one-half inch below the embroidered program name on both the top and the jacket.
Students may not wear unapproved uniforms. No additions to the uniform are permitted, other than the approved candy blue jacket. In cool environments, students may wear white undergarments that have a rounded neck, but no turtleneck, and sleeves as long as three-quarter length. Sweatshirts, “hoodies,” sweaters, or other outerwear may not be worn once the student enters the door of the clinical agency. Items of clothing may not have the wording “registered nurse” or “registered nursing” on them.
Deviations from the uniform may result in disciplinary action, such as being sent home from the clinical agency for the day (considered an unexcused absence) or immediate correction of the deviation, if possible. The clinical instructor will decide whether the uniform deviation can be corrected immediately or not.
White leather uniform shoes, with closed toes and heels, are required.
Instructions will be given before clinic for dress specific to mental health nursing.
Equipment requirements for the clinical site are:
Photo identification badge Pencil Plain white socks or non-textured hose Pen with black and red ink Bandage scissors Penlight Kelly forceps Stethoscope Watch with a second hand Blood pressure cuff Calibers (optional) Calculator (optional) Spiral notebook, 3” x 5” Fine tip black Sharpie pen
The complete uniform is worn during pre-clinical preparation, simulation or actual clinical practice at all the health agencies and while in the dining room or conference room. The instructor must approve any deviation from the standard uniform. There may be some clinical sites where uniforms are not required; your instructor will inform you of this.
Good hygiene is expected. This includes, but is not limited to, clean hair, absence of body odor, smell of cigarette smoke and halitosis. No perfumes, cologne or other strong fragrances should be applied prior to the clinical experience. Uniforms must be clean and pressed. The only acceptable jewelry to be worn are wedding rings, wrist watch, and one pair of small (4 mm) plain studs in pierced lower ear lobes, if you choose to wear earrings. Visible body piercing jewelry is not permitted. Body art should be covered to the maximum extent possible. Hair style and color should be fashioned to promote safety and professionalism, and should be worn above the collar and away from the face. Facial hair must be neatly trimmed and close to the face. No acrylic or gel nails are permitted in the clinical area. No nail polish may be worn. Chewing gum in the clinical facilities is not permitted.

16
POLICIES AFFECTING ATTENDANCE, GRADES AND ADMISSION
ATTENDANCE
1. It is the policy of Antelope Valley College as stated in the catalog that a college student is expected to attend all sessions of the classes in which he/she is enrolled. It is the responsibility of the student to notify the instructor when he/she is ill, to arrange in advance for unavoidable absence, to explain the reason for the absence to the instructor, and to attend class regularly. This applies to classroom absence as well as clinical absence.
2. Policies of the Health Sciences Division:
a. Your enrollment in this course constitutes an agreement between yourself and Antelope Valley College and its faculty for this course. Your obligation is to attend class and meet the objectives of the course. Antelope Valley College’s and the faculty’s obligation is to provide an atmosphere that facilitates learning and opportunities to assist you in successful completion of this course. The attendance policy is on page 26 of this module.
b. Orientation is mandatory for all courses. Failure to attend the first clinical day will result in the student being dropped from the course unless the instructor has been notified in advance.
c. Students will be given copies of this policy at the beginning of each Nursing Science course. The students are required to sign their copy of this policy.
d. Absence from class because of death in the family or illness is an excused absence. At the discretion of the instructor a doctor's verification of illness may be requested.
e. Requested make-up days for excused absences may be granted at the discretion of the lead and clinical instructor. Make-up days will be considered if a student’s request is made during the first week of return from illness. Make-ups must constitute a complete clinical day. This does not apply to Nursing Science 241.
f. Tardiness to the clinical area is considered in the total evaluation of the day's performance.
g. Absence from a scheduled examination
The student should notify the instructor if it will be necessary to be absent from the examination. The examination is taken upon the first day the student returns to class. The examination will be given at the convenience of the instructor. It is the student's responsibility to arrange this with the instructor. Any examination not taken will result in a score of 0.
h. Absence from clinical
The student is responsible for personal notification of the clinical instructor prior to the beginning of the day.
i. Clinical duty hours and breaks
Assigned breaks and lunches must be approved by clinical instructors. Students must remain in the assigned clinical facility or on the campus of the clinical facility during breaks.
j. Assignment to clinical groups
Students register for clinical groups according to the schedule of classes. Students who have satisfactorily completed prerequisite courses in first through third semesters are guaranteed space in the class in the subsequent semester.
Students can register for clinical courses for second through fourth semesters once they have met three conditions:
17
ATTENDANCE (CONTINUED)
(1) Students must have satisfactorily completed all prerequisite courses.
(2) Students must have current physical examinations, CPR cards and tuberculosis testing on file in the division office.
(3) Students must have a valid registration date.
Up until the first day of the semester, students may use the college registration system to register or switch clinical groups. After the first day of the semester, students cannot trade clinical groups.
HEALTH
1. In the event that a student has a health problem that could be unsafe for him/her or others, he/she should not attend the hospital for clinical experience. This decision is the student's responsibility.
2. Upon entry into the program, students will be required to have an initial physical examination by a licensed physician or certified nurse practitioner. The examination must show that the student is free from communicable disease and does not have a physical and/or mental illness that may endanger the health or safety of a patient. Impairment by controlled substances or alcohol during class or clinical experience violates college policy and compromises physical and emotional patient safety. Therefore, impairment by substance abuse or alcohol abuse that affects class or clinical performance is reason for dismissal from the nursing program.
3. The following immunizations are required: measles, mumps, rubella, chicken pox, Tdap (with boosters), hepatitis B and the seasonal flu vaccine. These are required by health care facilities in which the student will be practicing as a student nurse. The college does not provide immunizations.
4. Each year the student must present a document stating a negative Mantoux skin test or negative chest x-ray prior to entering the clinical area. A two-step TB testing procedure will be required for students who allow one year or longer between TB tests.
5. A physical examination will be required upon re-entry into the program.
GRADES (Also Refer to Antelope Valley College Catalog)
1. A minimum grade of "C" (70%) is mandatory in all required nursing courses. See registered nursing prerequisites for other courses.
2. Students will have a limited amount of time to review exams. In full-term classes, students will have two weeks after the date of the exam to review their exams. In part-of-term classes, students will have one week after the date of the exam to review their exams.
3. In nursing science courses, the total course grade is based upon both knowledge and performance skills. Theory taught is concurrently applied in the clinical setting. Clinical performance involves application of theoretical knowledge in a practice setting. The student must be satisfactory in all clinical behaviors on the last clinical day to pass. Therefore, any student unable to meet the clinical performance objectives for the course is considered unsatisfactory and will receive a maximum grade of "D" for the course. The student must receive a course grade of "C" to successfully complete the course.
4. There will be a math exam at the beginning of the first course taken in each semester of the nursing science program. The mandatory passing score for this exam is 90 percent. If the student does not attain a score of 90 percent or higher on the first exam, the student must remediate and retake the exam. The syllabus for the course will indicate the number of retakes allowed and the time frame for completing the exam. If the score is below 90 percent on the final attempt, the student will be dropped from the course.

18
GRADES (CONTINUED) 5. All students will be advised of unsatisfactory performance at the time the unsatisfactory incident
occurs, or as soon after as possible. When a student has demonstrated a pattern of unsatisfactory performance, the instructor will arrange a conference with the student. At the conference the instructor will give the student a written summary of the unsatisfactory incidents along with suggestions to assist the student in improving these behaviors. The student, together with the instructor, will develop a plan stating goals to be attained and dates by which the goals must be met. In the event that the goals agreed to in the plan are not met, the student will receive a maximum grade of "D" for the course.
6. In Nursing Science 241, a student with two unsatisfactory clinical rotations, or an unsatisfactory evaluation in the final rotation, is considered unsatisfactory and will receive a maximum grade of "D" for the course.
7. A student may withdraw from the course at any time through the twelfth (12th) week for the first and fourth semester course without penalty, and will receive a "W" on the course transcript. After the twelfth week, a letter grade must be given, as stated in the College Catalog. Withdrawal from a second or third semester short-term course is based upon the number of days in the course, and the individual instructors will give the withdrawal date.
8. Cheating will be handled according to College Board Policy. ACADEMIC VIOLATIONS
1. Violation of the Academic Honesty Policy: Dishonesty, including but not limited to, cheating or plagiarism. Plagiarism – from the Latin word for “kidnap” – involves using another’s work without giving proper credit, whether done accidentally or on purpose. This includes not only words and ideas, but also graphs, artwork, music, maps, statistics, diagrams, scientific data, software, films, videos, and the like. Plagiarism is plagiarism whether the material is from published or unpublished sources. It does not matter whether ideas are stolen, brought, downloaded from the Internet, or written for the student by someone else – it is still plagiarism. Even if only bits and pieces of other sources are used, or outside sources reworded, they must still be cited. To avoid problems, students should cite any source(s) and check with the instructor before submitting an assignment or project. Students are always responsible for any plagiarism in their work.
2. An instructor who determines that a student has cheated or plagiarized has the right to give an “F” grade for the assignment or examination.
REASONABLE ACCOMMODATION
Students with disabilities who anticipate they may need reasonable accommodation to participate in the nursing program should contact the Office for Students with Disabilities (OSD). The Health Sciences Division will work closely with OSD to determine if reasonable accommodations are required to perform essential job functions and identify effective accommodations that would not pose an undue hardship. TRANSPORTATION
Each student is responsible for his/her own transportation.
CLINICAL EXPERIENCE
No student is to participate in patient care without the permission of an instructor.
A current American Heart Association Cardiopulmonary Resuscitation (BCLS for the Health Care Provider) card is required in the clinical area. Please provide a copy to your instructor.
19
INSURANCE
Medical Service
1. Students pay a health fee, which provides physical, dental and mental health services as well as health education and prevention activities.
2. All injuries occurring while in class or laboratory experience must be reported at once to the instructor in that area. It is the responsibility of the instructor to guide the student so that appropriate care is obtained. Personal Liability Insurance
Students are required to purchase their own personal liability insurance. Information about personal liability insurance is available from the Health Sciences Division office. Students must show proof of this insurance before their first clinical day and the policy must be maintained during enrollment in the program. BACKGROUND SCREENING
Students will be required to demonstrate proof that they have been fingerprinted and/or screened for felonies, misdemeanors, fraud or abuse before entering the clinical facility. The background screen also includes social security number verification. LICENSURE REQUIREMENT FOR LICENSED VOCATIONAL NURSES
Licensed vocational nurses are required to maintain a license while they are enrolled in the program. REPORTING PRIOR CONVICTIONS OR DISCIPLINE AGAINST LICENSES
The Board of Registered Nursing (BRN) may deny licensure to individuals who have been convicted of a felony.
Applicants are required under law to report all misdemeanor and felony convictions. “Driving under the influence” convictions must be reported. Convictions must be reported even if they have been adjudicated, dismissed or expunged or even if a court ordered diversion program has been completed under the Penal Code or under Article 5 of the Vehicle Code. Also, all disciplinary action against an applicant’s registered nurse, practical nurse, vocational nurse or other health care related license or certificate must be reported. Also any fine, infraction, or traffic violation over $1,000 must be reported.
Failure to report prior convictions or disciplinary action is considered falsification of application and is grounds for denial of licensure or revocation of license. When reporting prior convictions or disciplinary action, applicants are required to provide a full written explanation of: circumstances surrounding the arrest(s), conviction(s), and/or disciplinary action(s); the date of incident(s), conviction(s) or disciplinary action(s); specific violation(s) (cite section of law if convicted), court location or jurisdiction, sanctions or penalties imposed and completion dates. Provide certified copies of arrest and court documents and/or disciplinary proceedings against any license as a registered nurse or any health care related license; include copies of state board determinations/decisions, citations and letters of reprimand.
NOTE: For drug and alcohol convictions include documents that indicate blood alcohol content (BAC) and sobriety date.
20
REPORTING PRIOR CONVICTIONS OR DISCIPLINE AGAINST LICENSES (CONTINUED)
To make a determination in these cases, the Board considers the nature and severity of the offense, additional subsequent acts, recency of acts or crimes, compliance with court sanctions, and evidence of rehabilitation.
The burden of proof lies with the applicant to demonstrate acceptable documented evidence of rehabilitation. Examples of rehabilitation evidence would include, but not be limited to:
Recent, dated letter from applicant describing the event and rehabilitative efforts or changes in life to prevent future problems or occurrences.
Recent and signed letters of reference on official letterhead from employers, nursing instructors, health professionals, professional counselors, parole or probation officers, support group facilitators or sponsors, or other individuals in positions of authority who are knowledgeable about your rehabilitation efforts.
Letters from recognized recovery programs and/or counselors attesting to current sobriety and length of time of sobriety, if there is a history of alcohol or drug abuse.
Submit copies of recent work evaluations.
Proof of community work, schooling, self-improvement efforts.
Court-issued certificate of rehabilitation or evidence of expungement, proof of compliance with criminal probation or parole, and orders of the court.
All of the above items should be mailed directly to the Board by the individual(s) or agency who is providing information about the applicant. Have these items sent to the Board of Registered Nursing, Licensing Unit, P.O. Box 944210, Sacramento, CA 94244-2100.
It is the responsibility of the applicant to provide sufficient rehabilitation evidence on a timely basis so that a licensing determination can be made. All evidence of rehabilitation must be submitted prior to being found eligible for licensure.
An applicant is also required to immediately report, in writing, to the Board any conviction(s) or disciplinary action(s) which occur between the date the application was filed and the date that a California registered nursing license is issued. Failure to report this information is grounds for denial of licensure or revocation of license.
Note: The application must be completed and signed by the applicant under the penalty of perjury.
GRATUITIES
It is unethical to accept gratuities and gifts from patients. In order to maintain a nurse/patient relationship students should not give gifts to patients.
SUSPENSION OR DISMISSAL
The Health Sciences Division supports and utilizes the guidelines of student conduct as outlined in the Antelope Valley College Catalog. In the event that unprofessional or incompetent conduct does occur, it will be handled according to college policy.
GRIEVANCE POLICY
The official student discipline policy for Antelope Valley College including due process procedures and grievance policy are contained in Antelope Valley College Administrative Policies #AP 5520 (Procedure for Discipline Related to Standard of Conduct), #AP5530 (Student Rights and Grievance), and Board Policy #BP 5500 (Standard of Conduct). Students are encouraged to discuss any grievance with the course instructor. For further clarification, the Dean of Health Sciences is available for counseling.
21
STUDENT ATTENDANCE AT FACULTY, CURRICULUM AND PROGRAM PLANNING AND EVALUATION MEETINGS
Students are encouraged to attend these meetings. Each year a student will be elected by each nursing class to represent them at these meetings. The purpose of this participation is for student input into the nursing program. There may be executive sessions for which students will be excused. CHANGES IN RECORDS DATA
It is essential that you notify the Health Sciences Division promptly of all changes of name, address, telephone number, family doctor, and the person to notify in case of emergency. The division office also needs to be notified of changes on applications and transcripts. Students are asked to maintain a current address with the Health Sciences Division after graduation to assist in maintaining a complete up-to-date record of all students and graduates.
CONFIDENTIALITY
It is the moral and professional responsibility (and obligation) of the nurse to at all times and in all places to keep absolute and confidential all information concerning patients. Duplication of any medical record is not permitted. A student must read charts or gather information from charts for the sole purpose of clinical experience and learning. This information should be shared only when a particular patient's care is discussed for the benefit of the entire group under the direction of the instructor.
POLICY REGARDING RE-ENROLLMENT IN NURSING SCIENCE COURSES (Revised 5/03; updated 11/07, 3/14)
Students are expected to complete the registered nursing program in four semesters after initial admission.
Students may re-enroll in the nursing science program once. A student will not be allowed to re-enroll in the program after two unsuccessful completions or withdrawals from any nursing science course. Nursing Science 200 (Nursing Transition) is considered a nursing science course in the program.
Students and faculty often refer to non progression in the program as “strikes.” Examples of “strikes” are:
Grade of D or F in a nursing science course.
Withdrawal from a nursing science course for any reason after attending any portion of the class or clinical, even if the withdrawal does not appear on a transcript.
In rare circumstances, a student may be eligible for removal of a strike. Circumstances in this category include personal injury, prolonged illness, or similar crises that result in a student’s inability to complete a course successfully. If a student is requesting an exception for unsuccessful completion or withdrawal, the student must have satisfactory standing at the time of withdrawal.
The procedure for requesting removal of a strike is:
Student writes a letter explaining the unique circumstances to the Dean of Health Sciences.
Student includes documentation supporting the circumstances with the letter.
Student has an attrition assessment on file.
All requests for removal of strikes must be filed with the Dean within 30 days of the end of the semester in which the student failed (or received a grade of D) or withdrew from the course.
Requests for removal of strikes are reviewed by the RN faculty. Students are notified of the faculty’s decision by mail.
22
POLICY REGARDING RE-ENROLLMENT IN NURSING SCIENCE COURSES (CONTINUED)
A student who leaves the program during the first semester or receives an unsatisfactory grade at the conclusion of the first semester must submit a new application (including current transcripts showing unsuccessful completion of the first nursing course(s)) to the Health Sciences Program Coordinator. The student must have a completed attrition assessment form on file.
The student will be placed on the list for enrollment in the order in which the application packet is received.
Second, third and fourth semester students and students who elected the LVN-to-RN option must submit a letter of intent to re-enroll and an attrition assessment form each time they plan to re-enroll. If the number of students who apply to re-enroll in a course exceeds the number of available spaces in the course, the dean conducts a lottery for the spaces that are available. Students are placed in the lottery by student identification number and are admitted in the order in which their number is drawn. Students who are not given spaces in the course will not be entered in a second lottery; they will be admitted in the order in which their numbers were drawn in the initial lottery. Re-enrollment is on a “space available” basis. The revisions to this policy take effect on August 18, 2014. It applies to all students who are enrolled in the first semester on or after that date (even if re-enrolling), transfer students and LVN-RN students entering the program in fall 2014 or later (not NS 200 students who entered the program in summer 2014).
POLICY REGARDING STUDENTS LEAVING THE PROGRAM BEFORE GRADUATION
Students must complete an attrition assessment form when leaving the program before graduation. If this form is not completed, the student will not be permitted to re-enter.
PHOTO IDENTIFICATION BADGES
Photo identification badges for Antelope Valley College must be purchased through the Student Development Office. The individual instructors will give you information on this. Please do not go to the Student Development Office to purchase your photo identification badge until you are instructed to do so by your instructor.
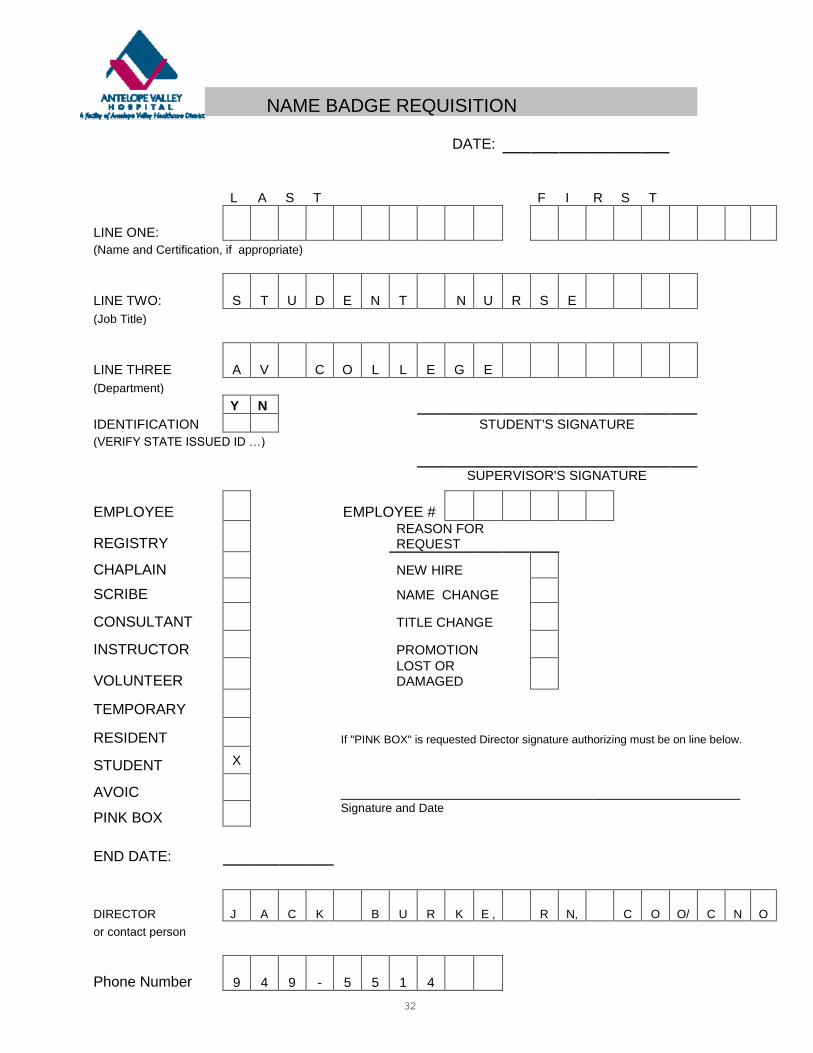
A photo identification badge is also required for Antelope Valley Hospital. In order to obtain this badge, a name badge requisition form must be filled out by the student and signed by the instructor. The student may not work in the hospital without the Antelope Valley Hospital photo identification badge.
The Antelope Valley Hospital photo identification badges will be collected by the instructor when the student leaves the program. Any inappropriate or unauthorized use of the badge may result in the immediate dismissal of the student from the program. SIMULATION The guidelines and confidentiality agreement for clinical simulation are on pages 27-28 of this module. ELECTRONIC DEVICES The policy regarding the use of electronic devices in the classroom and during clinical experiences is on pages 29-30 of this module.
23
What is the BRN Diversion Program?
The Board of Registered Nursing (BRN) is one of several professional regulatory boards and bureaus that exist within the Department of Consumer Affairs. The BRN has the primary responsi-bility of licensing and regulating registered nurses in California. The BRN's responsibilities come from the Nursing Practice Act, which is composed of California statutes that give the BRN, among other functions, the authority to manage a Diversion Program for registered nurses.
The Diversion Program is a voluntary, confidential program for registered nurses whose practice may be impaired due to chemical dependency or mental illness. The goal of the Diversion Program is to protect the public by early identification of impaired registered nurses and by providing these nurses access to appropriate intervention programs and treatment services. Public safety is protected by suspension of practice, when needed, and by careful monitoring of the nurse.
What Service Does the Program Provide? For the Public:
Immediate intervention to protect the public, as an effective alternative to longer disciplinary process.
Confidential consultation with the concerned public, employers, co-workers, family members, friends and consumers of nursing care.
Assistance in preparing to talk to a registered nurse about an apparent problem. Consultation with employers to assure a safe and smooth transition back to nursing practice
for the nurse participant.
For the Registered Nurse in the Program:
Confidential consultation when considering entering the program. Assessment and referral for appropriate detoxification or treatment. Development of a rehabilitation plan for chemical dependency or mental illness. Consultation with employers to assure a safe and smooth transition back to nursing practice
for the nurse participant. Random body fluid testing. Referrals to local support services. Encouragement, support, and guidance for the registered nurse in recovery as an effective
alternative to disciplinary action, and determination that the registered nurse is able to resume nursing practice.
Why is the Program Needed?
Registered nurses are not immune from the diseases of chemical dependency or mental illness. Experts estimate that at least 10% of the general population will have a problem with alcohol or drugs at some point in their lives. Health care professionals, including registered nurses, may be particularly susceptible to substance abuse problems due to the stresses of working in a health care environment and due to an increased opportunity to obtain controlled substances.
Many registered nurses who experience problems with chemical dependency are able to find the help and support they need to stay clean and sober without BRN involvement.

24
BRN DIVERSION PROGRAM (CONTINUED)
Mental illness, although not as prevalent, is also a disease that may affect a registered nurse's ability to practice safely. For example, untreated major depression can seriously impair an individual.
Unfortunately, most people suffering from chemical dependency or mental illness deny the problem. Many times they are the last to recognize and admit that they need help. If mental illness or chemical dependency problems are left untreated, they may eventually jeopardize patient health and safety. They can also threaten the life of the person afflicted.
In these cases, it becomes imperative that those individuals who detect a chemical dependency or mental health problem in a registered nurse take action. Without intervention, diseases have predictable courses and outcomes. The BRN's Diversion Program aims to identify symptoms, intervene, and change the outcomes.
The Diversion Program also provides an effective alternative to the traditional disciplinary process.
Who is Eligible? Registered Nurses Who:
Are licensed and reside in California. Are mentally ill or abuse alcohol or drugs to the extent that their nursing practice may be
affected. Voluntarily agree to enter the program and provide consent for appropriate medical or
psychiatric evaluations.
Registered Nurses are Ineligible for the Program if They Have:
Previously been disciplined by the Board for chemical dependency or mental illness. Been terminated previously from this program, any other diversion program for non-
compliance. Sold drugs. Caused patient harm or death.
How Does an RN Get Into the Program? Nurses enter the program in one of two ways:
Self-Referral – Registered nurses who would like assistance may contact the program directly.
Board-Referral - Registered nurses are referred to the Diversion Program by the BRN as a result of a complaint indicating the RN may be impaired due to chemical dependency or mental illness. If a nurse chooses not to enter the program, the complaint is referred to the Enforcement Program for investigation and possible disciplinary action.

25
BRN DIVERSION PROGRAM (CONTINUED)
Is the Diversion Program Successful?
Yes! Over 1,200 registered nurses have successfully completed the program. To complete the Diversion Program, a chemically dependent nurse must demonstrate a change in lifestyle that supports continuing recovery and have a minimum of 24 consecutive months of clean, random, body-fluid tests. A nurse with a history of mental illness must demonstrate the ability to identify the symptoms or triggers of the disease and be able to take immediate action to prevent an escalation of the disease.
The success of the Diversion Program is due to close monitoring of participants for an average of three years, but more importantly, it is attributable to the encouragement, support and guidance provided to nurses by other nurses.
Is the Program Confidential?
Diversion Program staff are available for confidential consultation regarding possible referral to the Diversion Program.
The confidentiality of participants is protected by law. Once a nurse enters the program, the information gathered to assist in developing a rehabilitation plan, and all other information in their record, is confidential.
When a nurse successfully completes the Diversion Program, the Diversion Program records are destroyed. If a nurse does not successfully complete the program, the original complaint, if any, is investigated by the Board's Enforcement Program. (As of January 1, 2000, Diversion Program records may be forwarded to the Board's Enforcement Program if a registered nurse who is terminated from the Diversion Program presents a threat to the public or his or her own health and safety.
Where Can I Get Additional Information About the Diversion Program?
For general program information, to schedule intake appointments or interventions, and for questions regarding monitoring nurses in the program, call 1-800-522-9198.
For questions regarding the Diversion Program or the Board of Registered Nursing's role in protecting public safety and identifying impaired practitioners, contact the Board's Diversion and Probation Programs Manager and staff at (916) 322-3350.
COPIED FROM BRN WEBSITE (WWW.RN.CA.GOV) JANUARY 2013

26
ANTELOPE VALLEY COLLEGE
Health Sciences Division
ASSOCIATE DEGREE NURSING PROGRAM
ATTENDANCE POLICY
It is the policy of Antelope Valley College as stated in the catalog that a college student is expected to attend all sessions of the classes in which he/she is enrolled. Your enrollment in Nursing Science classes constitutes an agreement between yourself, Antelope Valley College and its faculty for the classes. Your obligation is to attend class and meet the objectives of the course. Antelope Valley College’s and the faculty’s obligation is to provide an atmosphere that facilitates learning and opportunities to assist you in successful completion of this course.
Attendance and punctuality are requirements in demonstrating satisfactory performance in meeting course objectives, as well as vital components of professional behavior and accountability. It is the responsibility of the student to attend class regularly, to notify the instructor when he/she is ill, or will be late, to arrange in advance for unavoidable absences, and to explain the reason for the absences to the instructor. This applies to classroom absences as well as clinical absence.
Lecture hours cannot be made up. The maximum number of lecture hours that may be missed is the number of hours the course meets per week based on a 16 week semester. These hours are as follows:
Nursing Science 110 3 hours Nursing Science 200 1 hour Nursing Science 111 3 hours Nursing Science 230 1 hour Nursing Science 120 1 hour Nursing Science 231 4.5 hours Nursing Science 121 3.5 hours Nursing Science 232 4 hours Nursing Science 122 5.5 hours Nursing Science 240 1 hour Nursing Science 241 4.5 hours
Participation in clinical hours is required in order for faculty to evaluate satisfactory completion of the clinical objectives. A student’s failure to participate in the minimum number of clinical hours will result in that student’s dismissal from this course. Only excused clinical absences will be allowed to be made up. Absence from class because of death in the family or illness is an excused absence. Each clinical tardy will constitute a minimum absence of one hour. Requested make-up days for excused absences may be granted at the discretion of the lead and clinical instructor. Make-up days will be considered if a student’s request is made during the first week of return from illness. Make-up days will only be allowed if an entire shift is completed.
The maximum number of clinical hours that may be missed without being made up will vary from course to course based upon the number of hours in each clinic. These hours are as follows:
Nursing Science 111 7 hours Nursing Science 200 1 hour Nursing Science 121 4 hours Nursing Science 231 4 hours Nursing Science 122 4 hours Nursing Science 232 4 hours Nursing Science 241 12 hours
I have read the Antelope Valley College Associate Degree Nursing Attendance Policy. I understand the contents and I agree to comply with the said policy.
_________________________________ __________________________ Student’s Name (Please Print) Student’s Signature
___________________________ Date

27
ANTELOPE VALLEY COLLEGE Health Sciences Division
NURSING SCIENCE COURSES
SIMULATION GUIDELINES 1. Simulations in the skills laboratory are considered clinical hours. 2. Students are to wear the Antelope Valley College nursing uniform and abide by other dress code policies listed in the Mandatory Student Resource Manual. 3. The simulation manikin and room will be considered a patient and hospital room. 4. The performance at the bedside is not graded, but expected professional behaviors will be reflected on the clinical formative evaluation. 5. Students will sign a confidentiality agreement which indicates that the simulations will not be discussed with others outside of the simulation room and debriefing time. 6. When not in the actual simulation students will be expected to:
a. Behave professionally.
b. Complete assignments provided by the instructor.
c. Perform activities pertinent to course content such view videos or use computer programs. 7. Students are expected to come prepared for simulations. This includes reviewing the
objectives and completing any assignments. Some courses may include graded assignments or quizzes.

28
ANTELOPE VALLEY COLLEGE C
(661) 722-6300, Ext. 6402 • Fax (661) 722-6403
Confidentiality Agreement for Clinical Simulation Nursing Science
I have access to confidential clinical simulation information and need to be aware of and abide by procedures that apply to simulation information. Confidential simulation information is defined as anything that I, or those individuals with whom I interact, would expect to remain private including information relating to:
Simulation patients;
Standardized patients;
Patient models; and
Students As a student, I am required to comply with the clinical simulation guidelines relating to confidential information. I understand that: 1. I may have access to confidential simulation information.
2. I am responsible for protecting all simulation information.
3. Confidential simulation information may only be used as needed to perform my assigned activities. I may:
Not share any simulation scenario information with others outside of my clinical group;
Not share or disclose specific simulation patient health information;
Not share student performance with anyone other than those in my clinical simulation group and clinical faculty;
Not misuse or be careless with simulation information.
4. Violating this agreement may subject me to loss of simulation privileges and a clinical unsatisfactory grade in professional behavior.
By signing below, I acknowledge that I have read and understand the above agreement and agree to abide by the terms of this agreement. __________________________________ _____________________________ PRINTED NAME DATE OF AGREEMENT ___________________________________ SIGNATURE 12/09
29
ANTELOPE VALLEY COLLEGE
Health Sciences Division
ASSOCIATE DEGREE NURSING PROGRAM
Use of Electronic Devices in the Classroom
Technology use in the classroom is intended to enhance the learning environment for all students. Any use of technology that substantially degrades the learning environment, promotes dishonesty or illegal activities will be prohibited by the instructor. Classroom disruptions: Consistent with Board Policy 5500, it is the course instructor who decides whether student behaviors are disruptive in her/his classroom. If the instructor determines that the student behavior is disruptive the student will be asked to leave the classroom. If a student is asked to leave class, the instructor is not obligated to allow make up of examinations/quizzes or other graded assignments missed during the session in which the student was not in class. Cellular telephones: Students must not abuse the use of cell phones in class. Ringtones must be turned off in class. If there is a need to check for and/or receive a call, the student must inform the instructor in advance that the student may need to excuse him/herself to take an important call. Students must not engage in text messaging in the classroom. Students who create disturbances with ringing cell phones or text messaging may be asked to leave the class session. Laptop computers: Students are allowed to use laptop computers to take notes and for any other use authorized by the course instructor. However, laptops may not be used for instant messaging, game playing, and Internet surfing during class time. Audio-video recording devices: Students may be permitted to record during classroom sessions at the discretion of the instructor. All devices must be on the desk/table surface in full visibility of the instructor. All recording devices must be turned off during classroom breaks. Recording devices must be turned off when the instructor or a student shares a patient-based or personal story. All recordings are for the personal use of the student. They may not be copied, shared or downloaded to anyone who is not a member of the class. Recordings must not be posted on any online site. All recordings must be deleted after the course content has been tested. Electronic devices and academic dishonesty: As students at Antelope Valley College you are required to uphold academic honesty in all aspects. Any student who, during an examination, quiz or examination review is found “in possession” of a wireless transmitting/receiving/recording device shall be assumed to possess said device(s) for the purpose of academic dishonesty, and shall receive a zero on the examination or quiz in question. Said devices include but are not limited to: cellular telephones, computers, cameras, electronic recorders, MP3 players, PDAs and similar devices. Students who bring an electronic device to an examination, quiz, or examination review are to place those devices on the instructor’s desk or in a backpack in the front of the room during the exam or exam review. Electronic devises and illegal activities: An instructor will prohibit activities that she/he knows will violate laws, such as those related to intellectual property rights, confidentiality, copyrights, or invasions of privacy.
30
Use of Electronic Devices During Clinical Experiences
The use of personal cellular phones or other wireless communication devices must be used with discretion and a heightened awareness with regard to confidentiality and HIPAA protection. All facility policies will be enforced. Cellular telephones: Personal cell phones must be turned off when in the clinical setting. Students are expected to discuss appropriate times for phone calls with their families and friends, letting them know that during clinical time the caller will need to leave a message and the student can address the issues during break. Wireless communication devises: Cell phones or resource material downloaded to a wireless device may only be used in the break rooms. Electronic devices are not allowed to be used in patient care rooms or in the patient care corridors. Camera: Under no circumstances may a camera be operated within patient care areas. Students who violate the standards for the use of electronic devices during clinical experiences in the healthcare facilities and within patient care areas subject themselves to HIPAA violation claims which could result in legal actions. I have read the Antelope Valley College Associate Degree Nursing Electronic Devices Policy. I understand the contents and I agree to comply with the said policy. _________________________________ _________________________________ Student’s Name (Please Print) Student’s Signature ________________________________ Date

31
ANTELOPE VALLEY COLLEGE Health Sciences Division
(661) 722-6300, Ext. 6402 • Fax (661) 722-6403
ASSOCIATE DEGREE NURSING PROGRAM
I received, viewed or printed a copy of the 2014-15 Mandatory Student Resource Manual. The Associate Degree Nursing Program policies in the manual were explained, and I had an opportunity to ask questions about the policies.
If I fail or withdraw from any nursing science course (NS 110/111, 120/121/122, 200, 230/231/232 or 240/241), I must apply for re-admission. If I fail or withdraw from NS 110/111, I must submit a new application, updated education plan, current transcript, and an attrition assessment form. I will be placed on the list for admission based on the date of my application. If I fail or withdraw from any other nursing science course, I must write a letter of intent to re-enter and complete an attrition assessment form. If the number of students who wish to re-enter the course that I want to enter exceeds the number of spaces available in the course, there will be a lottery for the spaces.
If I fail or withdraw from any nursing science course a total of two times (including NS 200), I will no longer be eligible to re-enter the Antelope Valley College Associate Degree Nursing Program.
I understand that I must have all immunizations up-to-date in order to register for the next nursing science class in the program. I must have a TB test (or chest x-ray, if TB test is positive) and physical examination annually. Background screening, urine drug testing, and personal liability insurance are required. If I do not meet clinical agency health and background requirements, I will not be permitted to attend clinic.
I understand that I must surrender my hospital photo identification badge to my instructor if I fail a course, withdraw from a course, or when the instructor or program administration requests the badge.
I understand the policies for:
Uniforms
Absence from a scheduled examination
Health requirements and personal liability insurance
Grades needed to progress in the program
Withdrawal
Repeating Nursing Science courses
Photo identification badges
Electronic Devices
Simulation
Attendance
______________________________ ______________________________ Print name Signature ______________________________ Date
32
NAME BADGE REQUISITION
DATE:
L A S T
F I R S T
LINE ONE:
(Name and Certification, if appropriate)
LINE TWO: S T U D E N T N U R S E
(Job Title)
LINE THREE A V C O L L E G E
(Department)
Y N
IDENTIFICATION
STUDENT'S SIGNATURE
(VERIFY STATE ISSUED ID …)
SUPERVISOR'S SIGNATURE
EMPLOYEE
EMPLOYEE #
REGISTRY
REASON FOR REQUEST
CHAPLAIN
NEW HIRE
SCRIBE
NAME CHANGE
CONSULTANT
TITLE CHANGE
INSTRUCTOR
PROMOTION
VOLUNTEER
LOST OR DAMAGED
TEMPORARY
RESIDENT
If "PINK BOX" is requested Director signature authorizing must be on line below.
STUDENT X
AVOIC
______________________________________________________
PINK BOX
Signature and Date
END DATE:
DIRECTOR J A C K B U R K E , R N, C O O/ C N
O
or contact person
Phone Number 9 4 9 - 5 5 1 4

33
ANTELOPE VALLEY HOSPITAL PARKING
(UPDATED FALL 2011)
Instructor and
student parking

34
PALMDALE REGIONAL HOSPITAL PARKING (UPDATED FALL 2012)
AVC, UAV and other schools must park in the NW corner of the campus across from the drive which is your designated spot.
REMEMBER: PRMC is a NO SMOKING campus and facility, which is clearly outlined in your hospital orientation packet, please do not smoke ANYWHERE on the grounds, including in your vehicles.

35
MODULE 3
NURSING THEORY

36
NURSING THEORY: SELF-CARE
THE FOLLOWING ARE SOME QUOTATIONS ABOUT NURSING THAT WE WOULD LIKE TO SHARE WITH YOU. "Nursing puts us in touch with being human ... Without even asking, nurses are invited into the inner spaces of other people's existence for where there is suffering, loneliness, the tolerable pain of cure or the solitary pain of permanent change, there is a need for the kind of human service we call nursing."
Donna Diers "The new professionalism calls for us to have a clear sense of direction, to be well focused in our priorities and to be unified in their pursuit ... We must assert a distinct, sharp image, developing and brandishing our highest profile in what we do and what we are."
Margretta M. Styles "Patients have a right to freedom of choice. They have a right to participate in their treatment, to be well informed and allowed to use free will ... We must endeavor, at the local, national and international level, to let it be known that we nurses are united in our thinking and in our actions to work for freedom for all."
Olive Anstey "To the nurse ... in touch with the fundamentals of human experience, is given a unique opportunity to relate the adventure of thought to the adventure of action."
Annie W. Goodrich "A renewed consciousness is emerging in nursing today. It brings with it a gentle power, a sense of autonomy and a commitment to facilitate health. In particular, it brings a renewed awareness of the special way in which human caring is intrinsic in nursing practice."
Marie-Therese Connell "The true measure of the value of nursing rests in the degree to which it modifies the health behavior of others."
R.B. Freeman "Nursing requires an effort of considerable intellectual acuity - which looks to an outsider like intuition - to thread one's way through all the knowledge, technique and tenderness one has and to come out with the right action to serve the patient's particular needs."
Donna Diers
37
QUOTATIONS (CONTINUED) "... so finally we have learned that health really does lie in restoring independence, not merely ministering to illness."
Leah Curtin "Nursing is the appraisal and enhancement of the health status, health assets, and health potentials of human beings, and the preservation of dignity appropriate to their humanity."
Rozella M. Schlotfeldt
"To nurse is to tend the flow of life in ways that facilitate growth in the direction of wholeness and health."
Marie Therese Connell "There are three major features of a fully human way of being: being aware, being willing to act and being responsible. These ideas about what it means to be human can find expression in what is the most meaningful of professions, the practice of nursing."
Susan L. Carter "No matter where care is delivered, no matter what the pathophysiologic process, no matter how many lines, medications, or pieces of equipment are involved, nursing's unique role is to care for the person."
Sarah Sanford
38
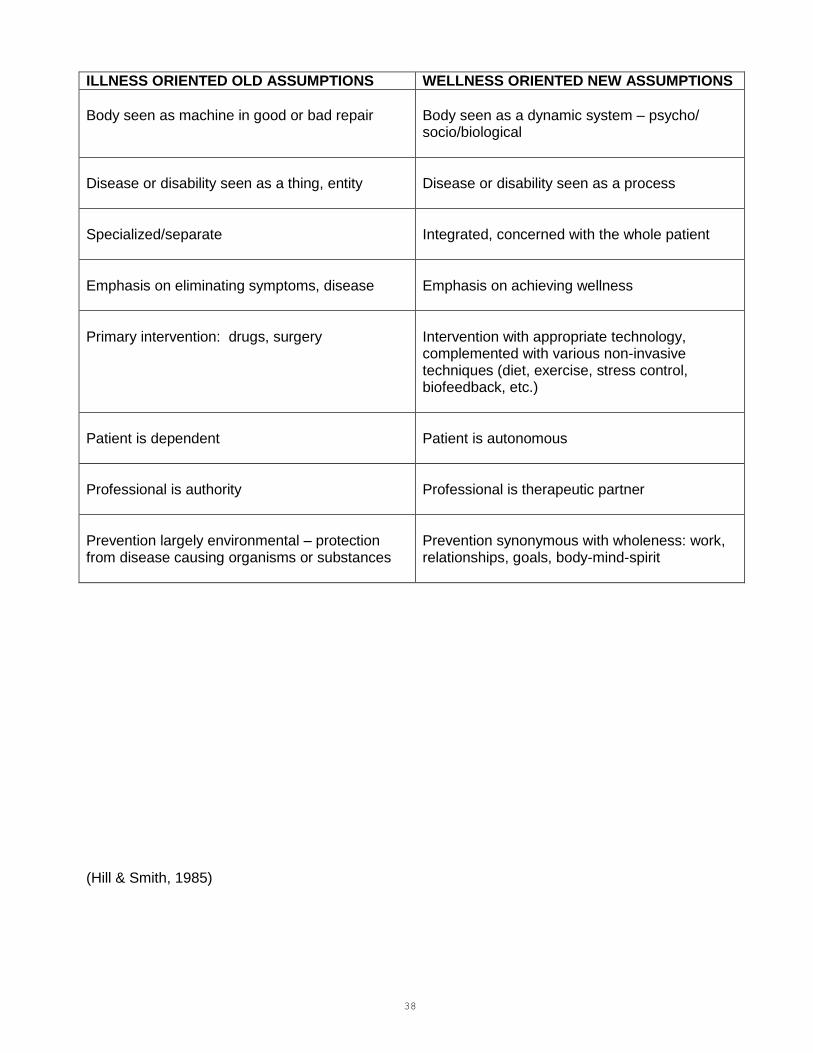
ILLNESS ORIENTED OLD ASSUMPTIONS WELLNESS ORIENTED NEW ASSUMPTIONS
Body seen as machine in good or bad repair
Body seen as a dynamic system – psycho/ socio/biological
Disease or disability seen as a thing, entity
Disease or disability seen as a process
Specialized/separate
Integrated, concerned with the whole patient
Emphasis on eliminating symptoms, disease
Emphasis on achieving wellness
Primary intervention: drugs, surgery
Intervention with appropriate technology, complemented with various non-invasive techniques (diet, exercise, stress control, biofeedback, etc.)
Patient is dependent
Patient is autonomous
Professional is authority
Professional is therapeutic partner
Prevention largely environmental – protection from disease causing organisms or substances
Prevention synonymous with wholeness: work, relationships, goals, body-mind-spirit
(Hill & Smith, 1985)
39
BASIC ASSUMPTIONS UNDERLYING SELF-CARE THEORY
1. Each individual is a psycho-socio-biological being who is rational and responsible for himself/herself. 2. Each individual exists in an environment that contains biological, physical, psychological and social components. Each individual is constantly in interaction with his/her environment. 3. Health is a dynamic state of wholeness or integrity of the individual. 4. All persons must meet certain conditions to maintain life and well-being. Human beings
require continuous inputs to themselves and their environment to remain alive and functioning.
5. Individuals act deliberately in performing care for themselves and others in identifying needs
for input and making needed inputs. 6. Human beings experience limitations in ability to engage in the inputs for self and others for sustaining life and regulating function. 7. Individuals, families and groups discover, develop and transmit to others ways and means to identify needs for and make inputs to self and others. (Orem, 1985)

40
NURSING THEORY: SELF-CARE
VOCABULARY ______________________________________________________________________________________________________________________________________________
TERM DEFINITION BY OREM EXAMPLE/DISCUSSION
______________________________________________________________________________________________________________________________________________ Self-Care The practice of activities that individuals initiate and As a child, Mary learned to feed herself. This is a self-care behavior practiced perform on their own behalf to maintain life, health by adults and children. Self-care actions are deliberate actions that when and well-being. continuously and effectively engaged in, regulate structural integrity, physio- psycho-social functioning and human development.
Self-Care Agency (SCA) The ability of an individual to initiate and perform The ability to engage in self-care involves motivation, knowledge and skill. When activities for himself/herself to maintain life, health Mary was 3 months old she may have had some motivation but not the knowledge and well-being. (Human agency is the power to act or skills to meet her need for nutrition. She lacks self-care agency. deliberately.)
Self-Care Agent The person providing the self-care. When Mary is 2 years old she can physically feed herself. She is the self-care agent.
Dependent-Care Agent The provider of infant care, child care or dependent At this age, however, Mary does not have the knowledge to choose a balanced adult care. diet or the ability to prepare her meals. Her mother acts as a dependent-care agent for her. If Mary were hospitalized a nurse could be the dependent-care agent.
Power Components Specific abilities required to engage in self-care. As Mary develops physically and mentally she acquires the abilities needed to engage in her own self-care.
Self-Care Requisites (SCR) Purposes or goals to be attained through the practice Mary's basic needs or requisites are met through the practice of self-care. of self-care. Three types of requisites are identified: Universal, Developmental and Health-Deviation. Universal requisites include air, water, food, rest/activity, elimination, safety, solitude
and social interaction and a realistic self-concept.
Developmental requisites are those associated with the developmental process and events occurring throughout the life cycle. Mary needs an environment that encourages her success in the use of a spoon and a glass in order to develop skills to feed herself.
Health-deviation requisites are those associated with structural and functional defects or deviations and their effects. If Mary were to severely sprain her ankle a health-deviation requisite would be the prevention of weight bearing on her injured ankle.
41
VOCABULARY (CONTINUED) ____________________________________________________________________________________________________________________________________________
TERM DEFINITION BY OREM EXAMPLE/DISCUSSION
____________________________________________________________________________________________________________________________________________
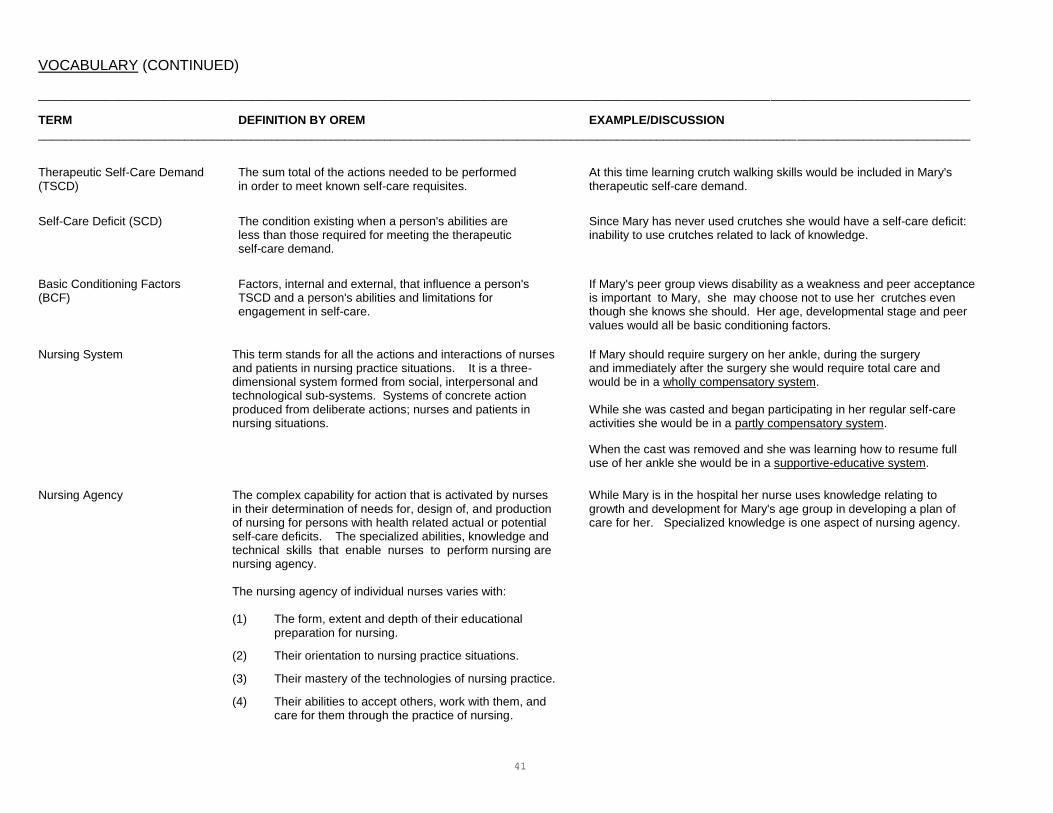
Therapeutic Self-Care Demand The sum total of the actions needed to be performed At this time learning crutch walking skills would be included in Mary's (TSCD) in order to meet known self-care requisites. therapeutic self-care demand.
Self-Care Deficit (SCD) The condition existing when a person's abilities are Since Mary has never used crutches she would have a self-care deficit: less than those required for meeting the therapeutic inability to use crutches related to lack of knowledge. self-care demand.
Basic Conditioning Factors Factors, internal and external, that influence a person's If Mary's peer group views disability as a weakness and peer acceptance (BCF) TSCD and a person's abilities and limitations for is important to Mary, she may choose not to use her crutches even engagement in self-care. though she knows she should. Her age, developmental stage and peer values would all be basic conditioning factors.
Nursing System This term stands for all the actions and interactions of nurses If Mary should require surgery on her ankle, during the surgery and patients in nursing practice situations. It is a three- and immediately after the surgery she would require total care and dimensional system formed from social, interpersonal and would be in a wholly compensatory system. technological sub-systems. Systems of concrete action produced from deliberate actions; nurses and patients in While she was casted and began participating in her regular self-care nursing situations. activities she would be in a partly compensatory system.
When the cast was removed and she was learning how to resume full use of her ankle she would be in a supportive-educative system.
Nursing Agency The complex capability for action that is activated by nurses While Mary is in the hospital her nurse uses knowledge relating to in their determination of needs for, design of, and production growth and development for Mary's age group in developing a plan of of nursing for persons with health related actual or potential care for her. Specialized knowledge is one aspect of nursing agency. self-care deficits. The specialized abilities, knowledge and technical skills that enable nurses to perform nursing are nursing agency.
The nursing agency of individual nurses varies with:
(1) The form, extent and depth of their educational
preparation for nursing.
(2) Their orientation to nursing practice situations.
(3) Their mastery of the technologies of nursing practice.
(4) Their abilities to accept others, work with them, and care for them through the practice of nursing.

42
VOCABULARY (CONTINUED) ____________________________________________________________________________________________________________________________________________
TERM DEFINITION BY OREM EXAMPLE/DISCUSSION
____________________________________________________________________________________________________________________________________________
METHODS OF ASSISTANCE
1. Acting for or doing for another A helping method that requires that the helper use developed Giving Mary a bed bath is acting for, doing for. abilities toward achieving specific results for persons in need
of help.
2. Guiding another This method is valid in situations in which persons must: Discussing with Mary why using her crutches is important (1) make choices, or is guiding her. (2) pursue a course of action, but not without direction or
supervision. The one being guided must be motivated and able to perform the activities required. In turn, the guidance given must be appropriate, whether in the form of suggestions, instructions, directions, or supervision.
3. Supporting another To support another person means to "sustain an effort" and Providing crutches for Mary is support. Also encouraging thereby prevent the person from failing or from avoiding an her as she crutch walks is support. unpleasant situation or decision. It also may enable the person in need of support to do something without undue stress because of the sustaining influence of the helper.
4. Providing a developmental This method of assistance requires the helper to provide or Keeping the floor clear of debris for Mary is a means to environment help to provide environmental conditions that motivate the provide a developmental environment. Providing privacy
person being helped to establish appropriate goals and when her friends visit is another method of providing for adjust behavior to achieve results specified by the goals. a developmental environment. The needed environmental conditions may be psychosocial or physical.
5. Teaching another This is a method of helping a person or a patient who needs Providing literature on crutch walking and teaching crutch instruction in order to develop knowledge or particular skills. walking techniques to Mary is providing the methods of
The nurse must consider the patient's background and assisting and teaching. experience, lifestyle and habits of daily living, modes of perceiving and thinking, and self-care requisites in order to be able to impart knowledge to the patient.
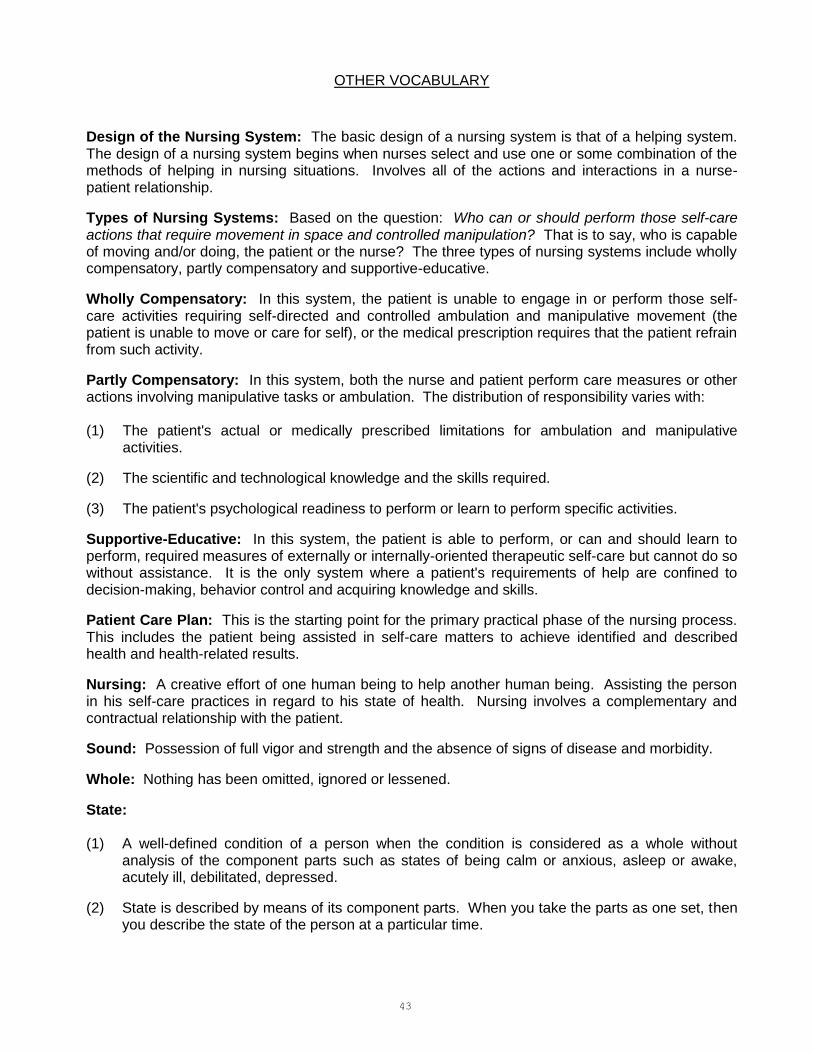
43
OTHER VOCABULARY
Design of the Nursing System: The basic design of a nursing system is that of a helping system. The design of a nursing system begins when nurses select and use one or some combination of the methods of helping in nursing situations. Involves all of the actions and interactions in a nurse-patient relationship.
Types of Nursing Systems: Based on the question: Who can or should perform those self-care actions that require movement in space and controlled manipulation? That is to say, who is capable of moving and/or doing, the patient or the nurse? The three types of nursing systems include wholly compensatory, partly compensatory and supportive-educative.
Wholly Compensatory: In this system, the patient is unable to engage in or perform those self-care activities requiring self-directed and controlled ambulation and manipulative movement (the patient is unable to move or care for self), or the medical prescription requires that the patient refrain from such activity.
Partly Compensatory: In this system, both the nurse and patient perform care measures or other actions involving manipulative tasks or ambulation. The distribution of responsibility varies with: (1) The patient's actual or medically prescribed limitations for ambulation and manipulative
activities.
(2) The scientific and technological knowledge and the skills required.
(3) The patient's psychological readiness to perform or learn to perform specific activities.
Supportive-Educative: In this system, the patient is able to perform, or can and should learn to perform, required measures of externally or internally-oriented therapeutic self-care but cannot do so without assistance. It is the only system where a patient's requirements of help are confined to decision-making, behavior control and acquiring knowledge and skills.
Patient Care Plan: This is the starting point for the primary practical phase of the nursing process. This includes the patient being assisted in self-care matters to achieve identified and described health and health-related results.
Nursing: A creative effort of one human being to help another human being. Assisting the person in his self-care practices in regard to his state of health. Nursing involves a complementary and contractual relationship with the patient.
Sound: Possession of full vigor and strength and the absence of signs of disease and morbidity.
Whole: Nothing has been omitted, ignored or lessened.
State: (1) A well-defined condition of a person when the condition is considered as a whole without
analysis of the component parts such as states of being calm or anxious, asleep or awake, acutely ill, debilitated, depressed.
(2) State is described by means of its component parts. When you take the parts as one set, then you describe the state of the person at a particular time.

44
OTHER VOCABULARY (CONTINUED) Well-Being: A subjective feeling; how the person perceives or understands his/her condition as being. Help: To give or provide what is necessary to accomplish a task or satisfy a need; contribute strength or means to; render assistance; cooperative effectively with; aid/assist; to make easier or less difficult; contribute to, facilitate. Promote: To help or encourage to exist or flourish further; advance, assist, help, support. Foster: To promote the growth and development of; further; encourage; to care for or cherish; forward; advance; nurse; sustain; support; maintain. ANA Definition of Nursing: The diagnosis and treatment of human responses to health and illness. Theory: A theory attempts to describe a particular phenomena. It isolates or pulls out the important/critical parts or components of the phenomena. It goes on to describe how the parts relate to each other. These relationships can then be tested and if they are always true, they can predict what will happen.

45
HEALTH FOCUS PERSPECTIVES
PATIENT
Patient’s State of Health
1. Present abilities to engage in self-care
2. Health-related disabilities in giving self-care
Health results sought for patient
1. Life
2. Normal or near normal functioning
3. Effective living despite disability
Patient’s requirements for therapeutic self-care to meet
1. Universal requisites
2. Developmental requisites
3. Health-deviation requisites
Physician’s perspective of the patient’s health situation
Patient’s perspective of the health situation
Nurse’s perspective of the health care situation
(Orem, 1991)
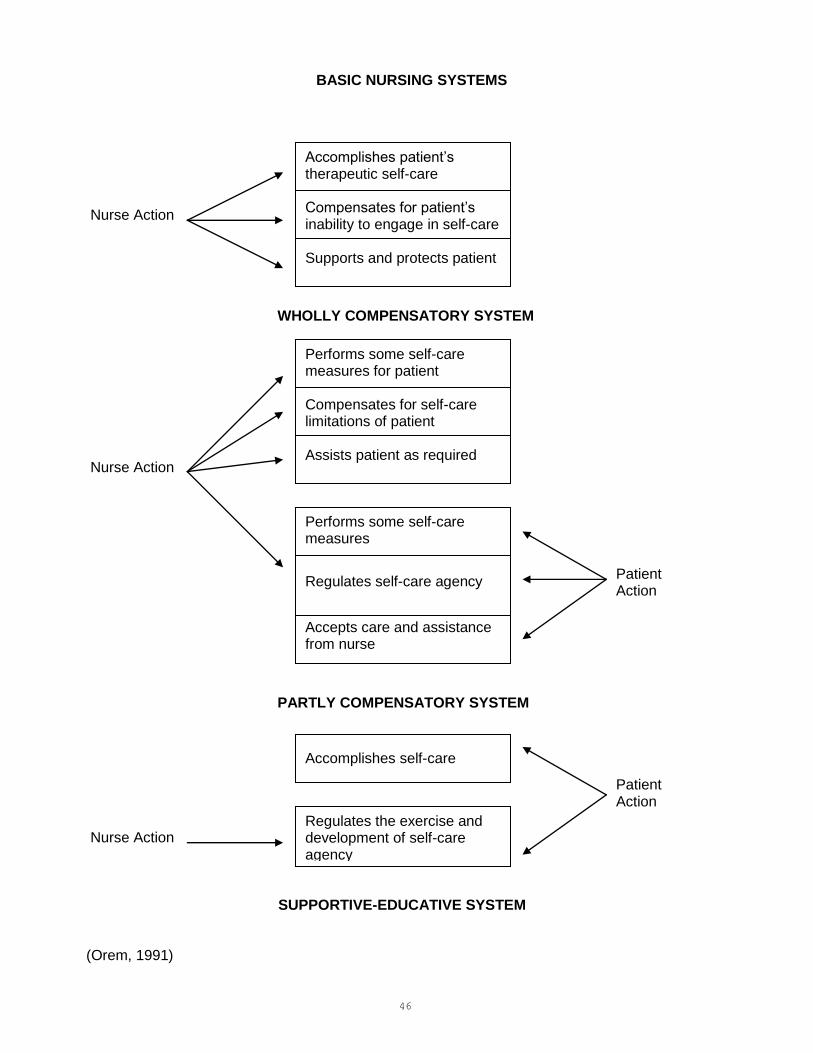
46
BASIC NURSING SYSTEMS
Nurse Action WHOLLY COMPENSATORY SYSTEM Nurse Action PARTLY COMPENSATORY SYSTEM Nurse Action (Orem, 1991)
Accomplishes patient’s therapeutic self-care Compensates for patient’s inability to engage in self-care Supports and protects patient
Performs some self-care measures for patient Compensates for self-care limitations of patient Assists patient as required
Performs some self-care measures
Regulates self-care agency
Accepts care and assistance from nurse
Accomplishes self-care
Regulates the exercise and development of self-care agency
SUPPORTIVE-EDUCATIVE SYSTEM
Patient Action
Patient Action

47
RELATIONSHIP OF THE TERMS OF SELF-CARE THEORY (Jewish Hospital of St. Louis)
UNIVERSAL SELF- DEVELOPMENTAL HEALTH-DEVIATION CARE REQUISITES SELF-CARE REQUISITES SELF-CARE REQUISITES Individualized by Basic Conditioning Factors Result in THERAPEUTIC SELF-CARE DEMANDS Which if not met by SELF-CARE AGENCY Result in SELF-CARE DEFICIT Determines NURSING SYSTEM Implemented by means of METHODS OF ASSISTING NURSING ACTION Effectiveness Determined by EVALUATION
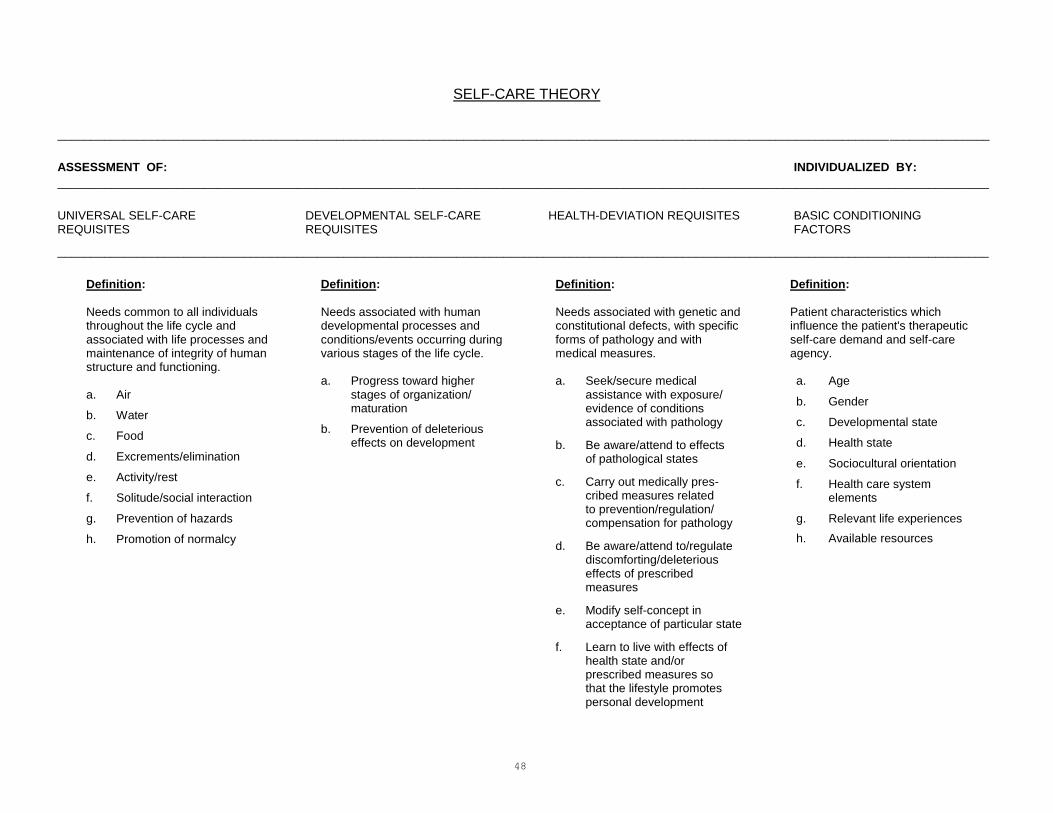
48
SELF-CARE THEORY ____________________________________________________________________________________________________________________________________________ ASSESSMENT OF: INDIVIDUALIZED BY: ____________________________________________________________________________________________________________________________________________ UNIVERSAL SELF-CARE DEVELOPMENTAL SELF-CARE HEALTH-DEVIATION REQUISITES BASIC CONDITIONING REQUISITES REQUISITES FACTORS ____________________________________________________________________________________________________________________________________________
Definition:
Needs common to all individuals throughout the life cycle and associated with life processes and maintenance of integrity of human structure and functioning. a. Air
b. Water
c. Food
d. Excrements/elimination
e. Activity/rest
f. Solitude/social interaction
g. Prevention of hazards
h. Promotion of normalcy
Definition:
Needs associated with human developmental processes and conditions/events occurring during various stages of the life cycle. a. Progress toward higher stages of organization/ maturation b. Prevention of deleterious effects on development
Definition:
Needs associated with genetic and constitutional defects, with specific forms of pathology and with medical measures. a. Seek/secure medical assistance with exposure/ evidence of conditions associated with pathology
b. Be aware/attend to effects of pathological states
c. Carry out medically pres- cribed measures related to prevention/regulation/
compensation for pathology
d. Be aware/attend to/regulate discomforting/deleterious effects of prescribed measures
e. Modify self-concept in acceptance of particular state
f. Learn to live with effects of health state and/or prescribed measures so that the lifestyle promotes personal development
Definition:
Patient characteristics which influence the patient's therapeutic self-care demand and self-care agency. a. Age
b. Gender
c. Developmental state
d. Health state
e. Sociocultural orientation
f. Health care system elements
g. Relevant life experiences
h. Available resources

49
SELF-CARE THEORY _______________________________________________________________________________________________________________________________________________ RESULTS IN: MINUS: EQUALS:
_______________________________________________________________________________________________________________________________________________ THERAPEUTIC SELF-CARE DEMANDS SELF-CARE AGENCY SELF-CARE DEFICIT/PROBLEM _______________________________________________________________________________________________________________________________________________ Definition:
A prescription for continuous self-care action through which identified self-care requisites can be met with stipulated degrees of effectiveness.
Definition:
The ability of an individual to initiate and perform activities essential for self-care. These abilities are the power components and include: 1. Awareness of self and surroundings
2. Physical energy to carry out self-care actions
3. Ability to control body position, movements
4. Ability to reason
5. Motivation
6. Ability to make and implement decisions
7. Ability to acquire, retain and use technical knowledge
8. Skills necessary to perform self-care actions
9. Ability to order self-care
10. Ability to perform self-care actions consistently and to fit them into personal, family and community life
Definition:
Self-care actions that the individual cannot carry out alone at this time due to limitation in self-care agency. SCA < TSCD = SCD When Self-Care Agency is less than Therapeutic Self- Care Demand then a Self-Care Deficit exits.
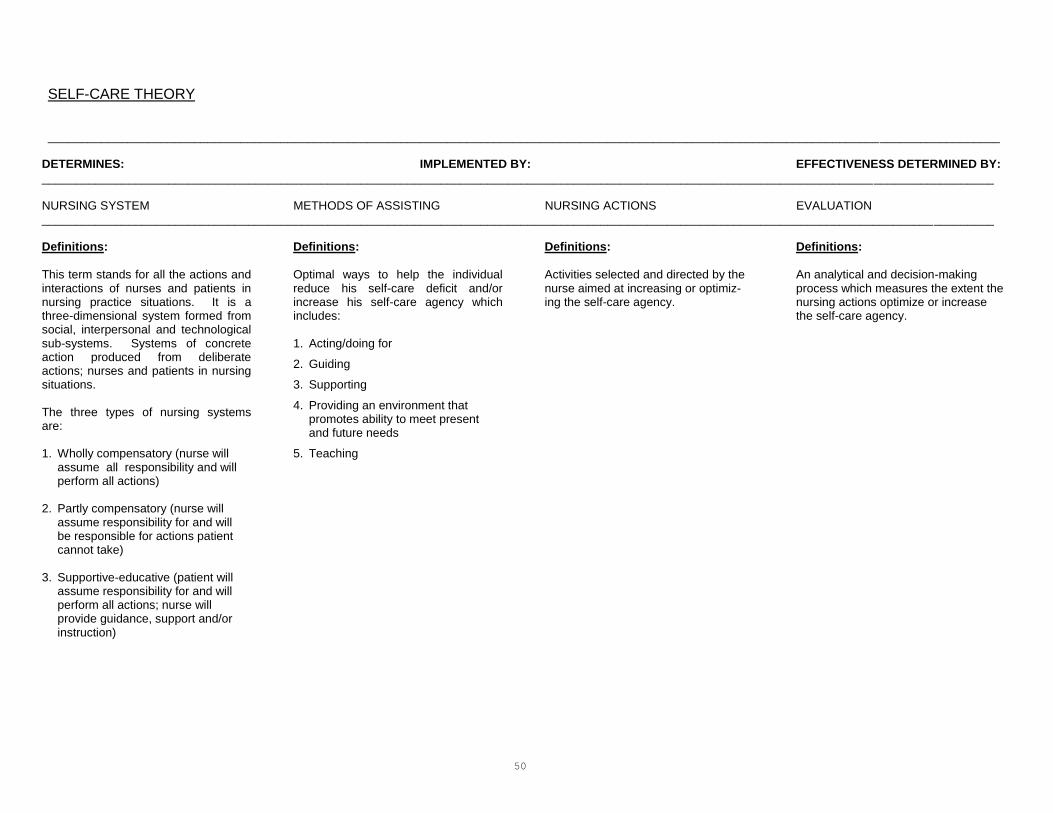
50
SELF-CARE THEORY _______________________________________________________________________________________________________________________________________________
DETERMINES: IMPLEMENTED BY: EFFECTIVENESS DETERMINED BY:
_______________________________________________________________________________________________________________________________________________ NURSING SYSTEM METHODS OF ASSISTING NURSING ACTIONS EVALUATION _______________________________________________________________________________________________________________________________________________
Definitions:
This term stands for all the actions and interactions of nurses and patients in nursing practice situations. It is a three-dimensional system formed from social, interpersonal and technological sub-systems. Systems of concrete action produced from deliberate actions; nurses and patients in nursing situations. The three types of nursing systems are: 1. Wholly compensatory (nurse will assume all responsibility and will perform all actions) 2. Partly compensatory (nurse will assume responsibility for and will be responsible for actions patient cannot take) 3. Supportive-educative (patient will assume responsibility for and will perform all actions; nurse will provide guidance, support and/or instruction)
Definitions:
Optimal ways to help the individual reduce his self-care deficit and/or increase his self-care agency which includes: 1. Acting/doing for
2. Guiding
3. Supporting
4. Providing an environment that promotes ability to meet present and future needs
5. Teaching
Definitions:
Activities selected and directed by the nurse aimed at increasing or optimiz- ing the self-care agency.
Definitions:
An analytical and decision-making process which measures the extent the nursing actions optimize or increase the self-care agency.

51
BASIC CONDITIONING FACTORS ASSESSMENT GUIDE Patient characteristics which influence the patient's therapeutic self-care demand to be met and self-care agency. These characteristics are:
1. Age.
2. Gender.
(Chronological age and gender relate to status within a family, i.e., status and roles of husband and wife, mother and father, son and daughter. They define duties and
responsibilities of the person toward other family members depending upon socio-cultural setting.)
3. Developmental State:
a. Psychological -
(1) Developmental task according to Erickson. (2) Self-image and concept, philosophy, intimacy, social relationships, etc.
b. Cognitive -
(1) Orientation. (2) Memory. (3) Concentration and calculation. (4) Knowledge. (5) Judgment. (6) Thought processes.
c. Physical -
(1) Weight and height. (2) Muscle mass and adipose tissue distribution.
4. Relevant Life Experience:
a. How patient has reacted in stress-producing situations.
b. How patient has reacted to similar situations with his friends and family, i.e., illness and hospitalization.
c. Reaction to and perception of illness.
d. Perception of health care, attitudes about wellness/illness.
e. Level of stress and anxiety. 5. Health Care System:
a. Present (diagnosis, date admitted, signs and symptoms of present illness, date of surgery/significant examinations and procedures).
b. Past medical history.
52
BASIC CONDITIONING FACTORS ASSESSMENT GUIDE (CONTINUED) 6. Health State:
Information about aspects of human structure and functioning at moments in time (reason for seeking treatment, signs and symptoms, vital signs, physical assessment). 7. Socio-Cultural Orientation:
a. Role in family/marital status.
b. Ethnic background.
c. Religion/church affiliation.
d. Educational/intellectual level.
e. Occupation.
f. Recreational/diversional activities; hobbies, social and leisure activities. 8. Available Resources:
a. Financial status.
b. Insurance.
c. Social security and other benefits.
d. Support systems.
e. Time.
f. Other.
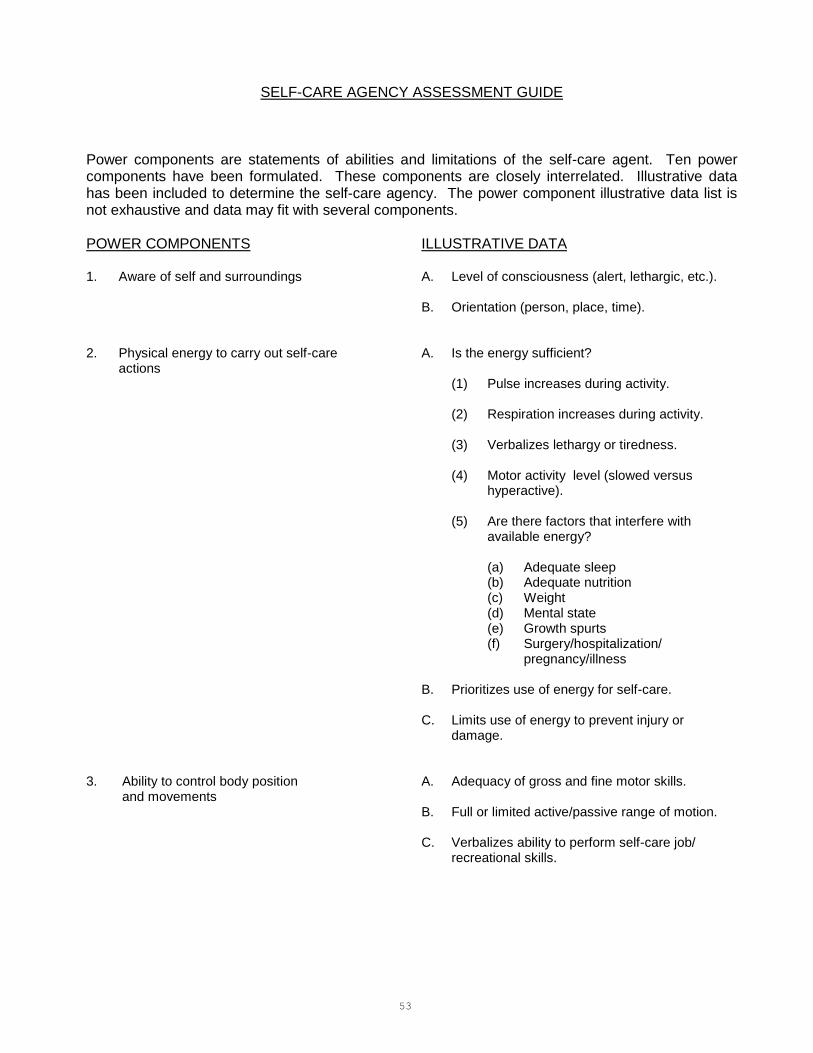
53
SELF-CARE AGENCY ASSESSMENT GUIDE
Power components are statements of abilities and limitations of the self-care agent. Ten power components have been formulated. These components are closely interrelated. Illustrative data has been included to determine the self-care agency. The power component illustrative data list is not exhaustive and data may fit with several components. POWER COMPONENTS ILLUSTRATIVE DATA 1. Aware of self and surroundings A. Level of consciousness (alert, lethargic, etc.).
B. Orientation (person, place, time). 2. Physical energy to carry out self-care A. Is the energy sufficient?
actions (1) Pulse increases during activity.
(2) Respiration increases during activity.
(3) Verbalizes lethargy or tiredness.
(4) Motor activity level (slowed versus hyperactive).
(5) Are there factors that interfere with available energy?
(a) Adequate sleep (b) Adequate nutrition (c) Weight (d) Mental state (e) Growth spurts (f) Surgery/hospitalization/
pregnancy/illness
B. Prioritizes use of energy for self-care.
C. Limits use of energy to prevent injury or damage. 3. Ability to control body position A. Adequacy of gross and fine motor skills.
and movements B. Full or limited active/passive range of motion.
C. Verbalizes ability to perform self-care job/
recreational skills.

54
SELF-CARE AGENCY ASSESSMENT GUIDE (CONTINUED) POWER COMPONENTS ILLUSTRATIVE DATA 4. Ability to reason A. Reasons without interferences from defensive
functioning (denial, projection, etc.).
B. Identifies cause/effect relationships.
C. Associates own needs and related self-care actions.
D. Responds consistently and congruently to questions. 5. Motivation A. Values self-care and health.
B. Explains significance of self-care activities.
C. Initiates and follows through with good health care goals.
6. Ability to make and implement A. Recognizes problems without someone else
decisions regarding self-care calling attention to them.
B. Recognizes responsibility for actions.
C. States goals and describes plan, implementa- tion, and evaluation.
D. Identifies supports, constraints, and conflicts in attaining goals.
7. Ability to acquire, retain and utilize A. Adequate length of attention span.
knowledge B. Adequate short-term (accurate) memory.
C. Adequate long-term memory.
D. Verbalizes knowledge pertinent to own health
state.
E. Demonstrates utilization of this knowledge.
F. Utilizes community resources and health care professionals as sources of knowledge.
8. Repertoire of skills A. Self-care actions that are carried out.

55
SELF-CARE AGENCY ASSESSMENT GUIDE (CONTINUED) POWER COMPONENTS ILLUSTRATIVE DATA 9. Ability to order self-care actions A. Establishes priorities.
B. Organizes actions to meet priorities. 10. Ability to perform self-care actions A. Maintains self-care regimen on a regular basis.
consistently and to fit them into personal, family and community life. B. Integrates self-care regimen into patterns of
living.
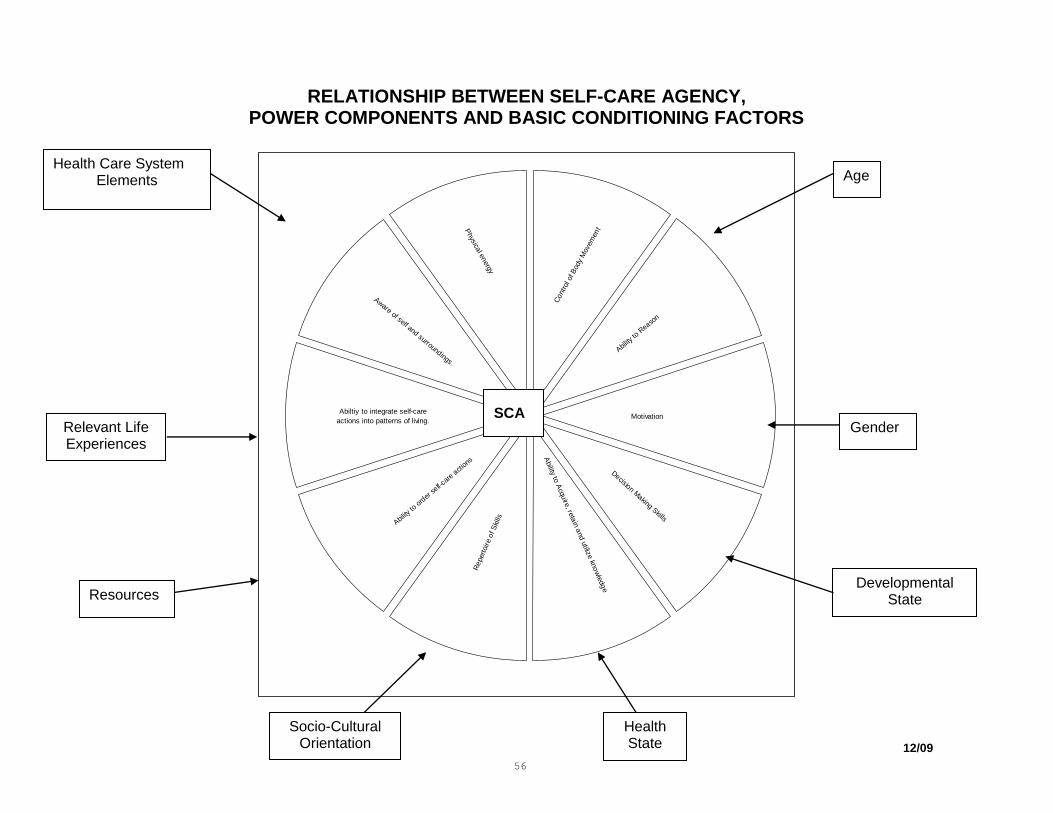
56
RELATIONSHIP BETWEEN SELF-CARE AGENCY, POWER COMPONENTS AND BASIC CONDITIONING FACTORS
Ability
to A
cqu
ire, re
tain
and u
tilize kn
ow
ledg
e
Re
pert
oir
e o
f S
kills
Ability
to o
rder
self-
care
act
ions
Abiltiy to integrate self-care
actions into patterns of living.
Aware of self and surroundings.
Physica
l energy
Decision Making Skills
Ability
to R
easo
n
Motivation
Cont
rol o
f Bod
y M
ovem
ent
SCA
Health Care System Elements
Age
Gender
Developmental State
Health State
Socio-Cultural Orientation
Resources
Relevant Life Experiences
12/09
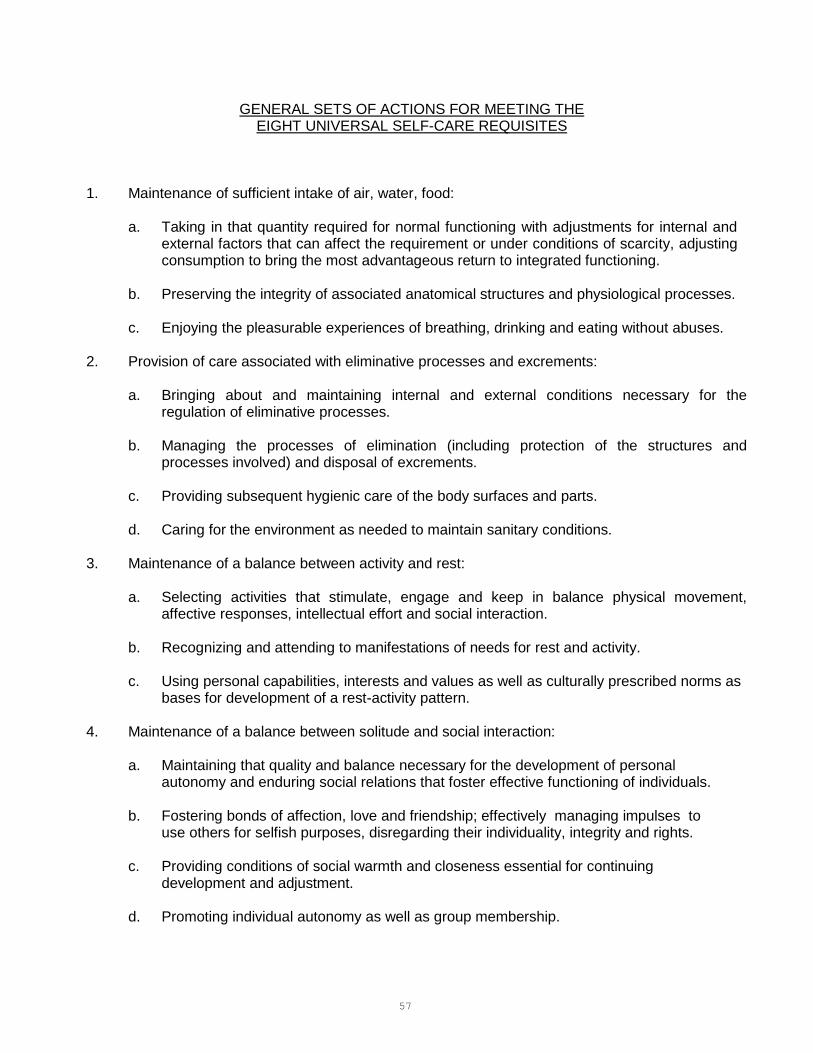
57
GENERAL SETS OF ACTIONS FOR MEETING THE EIGHT UNIVERSAL SELF-CARE REQUISITES
1. Maintenance of sufficient intake of air, water, food:
a. Taking in that quantity required for normal functioning with adjustments for internal and external factors that can affect the requirement or under conditions of scarcity, adjusting consumption to bring the most advantageous return to integrated functioning.
b. Preserving the integrity of associated anatomical structures and physiological processes.
c. Enjoying the pleasurable experiences of breathing, drinking and eating without abuses. 2. Provision of care associated with eliminative processes and excrements:
a. Bringing about and maintaining internal and external conditions necessary for the regulation of eliminative processes.
b. Managing the processes of elimination (including protection of the structures and
processes involved) and disposal of excrements.
c. Providing subsequent hygienic care of the body surfaces and parts.
d. Caring for the environment as needed to maintain sanitary conditions. 3. Maintenance of a balance between activity and rest:
a. Selecting activities that stimulate, engage and keep in balance physical movement, affective responses, intellectual effort and social interaction.
b. Recognizing and attending to manifestations of needs for rest and activity.
c. Using personal capabilities, interests and values as well as culturally prescribed norms as
bases for development of a rest-activity pattern. 4. Maintenance of a balance between solitude and social interaction:
a. Maintaining that quality and balance necessary for the development of personal autonomy and enduring social relations that foster effective functioning of individuals.
b. Fostering bonds of affection, love and friendship; effectively managing impulses to use others for selfish purposes, disregarding their individuality, integrity and rights.
c. Providing conditions of social warmth and closeness essential for continuing development and adjustment.
d. Promoting individual autonomy as well as group membership.
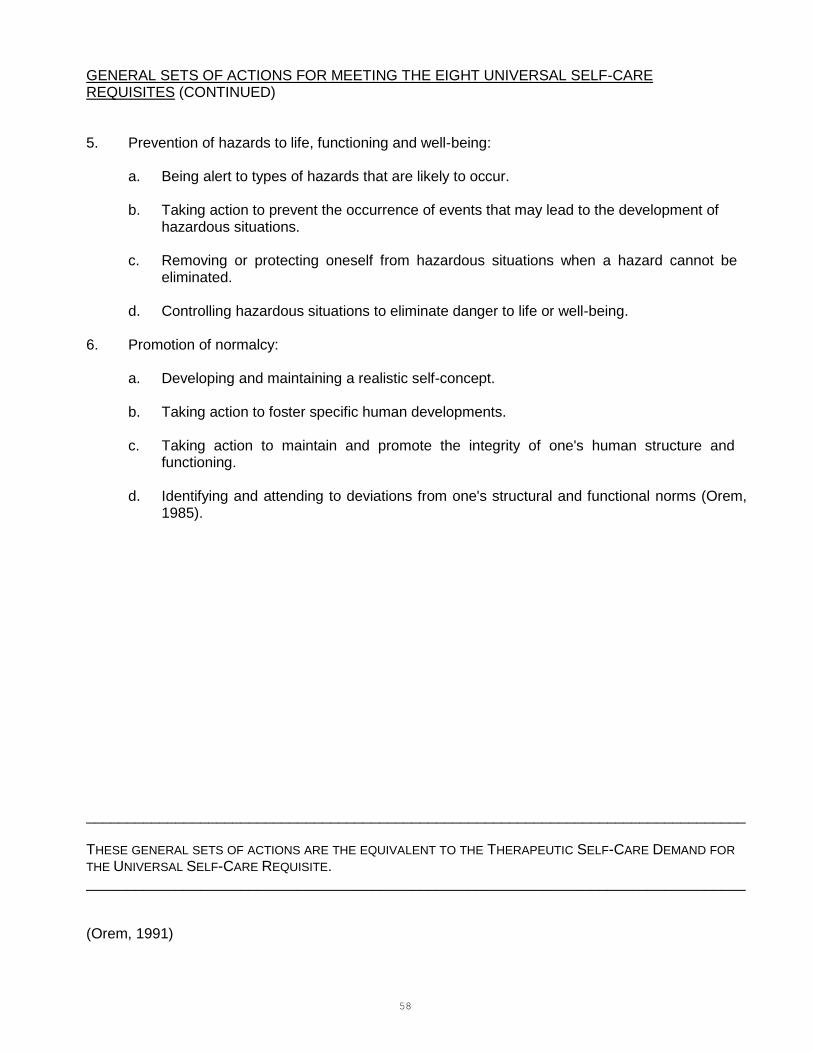
58
GENERAL SETS OF ACTIONS FOR MEETING THE EIGHT UNIVERSAL SELF-CARE REQUISITES (CONTINUED) 5. Prevention of hazards to life, functioning and well-being:
a. Being alert to types of hazards that are likely to occur.
b. Taking action to prevent the occurrence of events that may lead to the development of hazardous situations.
c. Removing or protecting oneself from hazardous situations when a hazard cannot be
eliminated.
d. Controlling hazardous situations to eliminate danger to life or well-being. 6. Promotion of normalcy:
a. Developing and maintaining a realistic self-concept.
b. Taking action to foster specific human developments.
c. Taking action to maintain and promote the integrity of one's human structure and functioning.
d. Identifying and attending to deviations from one's structural and functional norms (Orem,
1985). _________________________________________________________________________________ THESE GENERAL SETS OF ACTIONS ARE THE EQUIVALENT TO THE THERAPEUTIC SELF-CARE DEMAND FOR
THE UNIVERSAL SELF-CARE REQUISITE. _________________________________________________________________________________ (Orem, 1991)
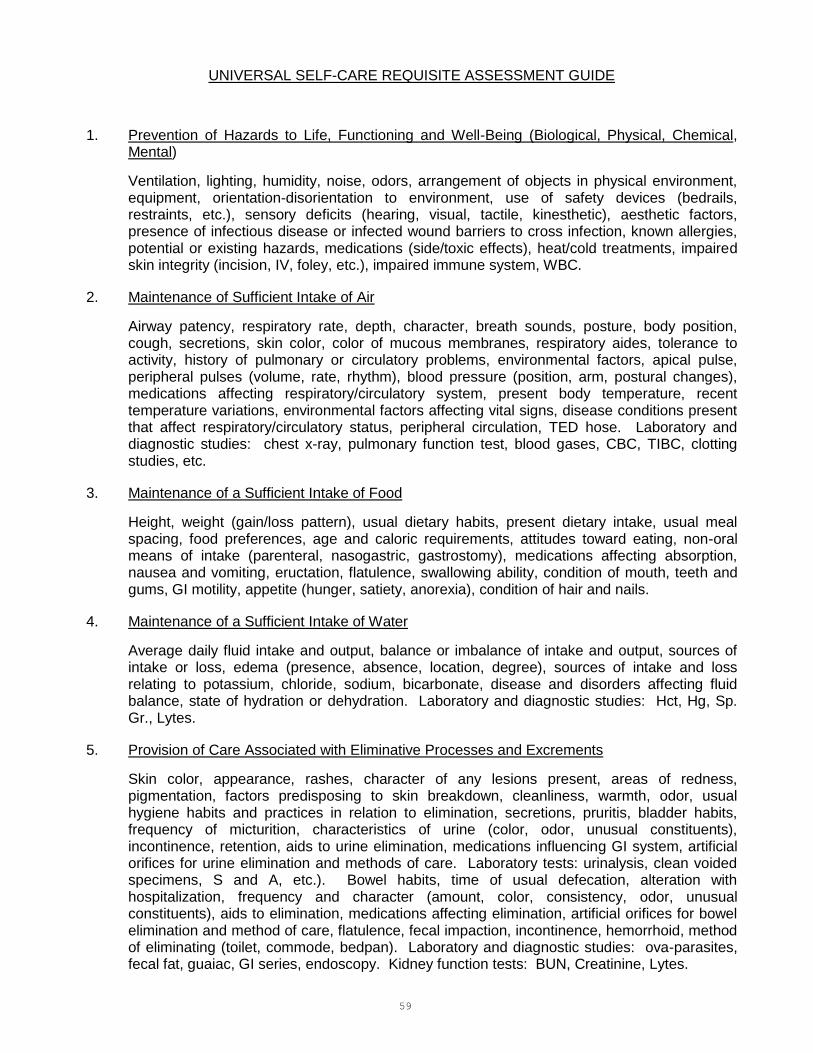
59
UNIVERSAL SELF-CARE REQUISITE ASSESSMENT GUIDE
1. Prevention of Hazards to Life, Functioning and Well-Being (Biological, Physical, Chemical, Mental)
Ventilation, lighting, humidity, noise, odors, arrangement of objects in physical environment, equipment, orientation-disorientation to environment, use of safety devices (bedrails, restraints, etc.), sensory deficits (hearing, visual, tactile, kinesthetic), aesthetic factors, presence of infectious disease or infected wound barriers to cross infection, known allergies, potential or existing hazards, medications (side/toxic effects), heat/cold treatments, impaired skin integrity (incision, IV, foley, etc.), impaired immune system, WBC.
2. Maintenance of Sufficient Intake of Air
Airway patency, respiratory rate, depth, character, breath sounds, posture, body position, cough, secretions, skin color, color of mucous membranes, respiratory aides, tolerance to activity, history of pulmonary or circulatory problems, environmental factors, apical pulse, peripheral pulses (volume, rate, rhythm), blood pressure (position, arm, postural changes), medications affecting respiratory/circulatory system, present body temperature, recent temperature variations, environmental factors affecting vital signs, disease conditions present that affect respiratory/circulatory status, peripheral circulation, TED hose. Laboratory and diagnostic studies: chest x-ray, pulmonary function test, blood gases, CBC, TIBC, clotting studies, etc.
3. Maintenance of a Sufficient Intake of Food
Height, weight (gain/loss pattern), usual dietary habits, present dietary intake, usual meal spacing, food preferences, age and caloric requirements, attitudes toward eating, non-oral means of intake (parenteral, nasogastric, gastrostomy), medications affecting absorption, nausea and vomiting, eructation, flatulence, swallowing ability, condition of mouth, teeth and gums, GI motility, appetite (hunger, satiety, anorexia), condition of hair and nails.
4. Maintenance of a Sufficient Intake of Water
Average daily fluid intake and output, balance or imbalance of intake and output, sources of intake or loss, edema (presence, absence, location, degree), sources of intake and loss relating to potassium, chloride, sodium, bicarbonate, disease and disorders affecting fluid balance, state of hydration or dehydration. Laboratory and diagnostic studies: Hct, Hg, Sp. Gr., Lytes.
5. Provision of Care Associated with Eliminative Processes and Excrements
Skin color, appearance, rashes, character of any lesions present, areas of redness, pigmentation, factors predisposing to skin breakdown, cleanliness, warmth, odor, usual hygiene habits and practices in relation to elimination, secretions, pruritis, bladder habits, frequency of micturition, characteristics of urine (color, odor, unusual constituents), incontinence, retention, aids to urine elimination, medications influencing GI system, artificial orifices for urine elimination and methods of care. Laboratory tests: urinalysis, clean voided specimens, S and A, etc.). Bowel habits, time of usual defecation, alteration with hospitalization, frequency and character (amount, color, consistency, odor, unusual constituents), aids to elimination, medications affecting elimination, artificial orifices for bowel elimination and method of care, flatulence, fecal impaction, incontinence, hemorrhoid, method of eliminating (toilet, commode, bedpan). Laboratory and diagnostic studies: ova-parasites, fecal fat, guaiac, GI series, endoscopy. Kidney function tests: BUN, Creatinine, Lytes.

60
UNIVERSAL SELF-CARE REQUISITE ASSESSMENT GUIDE (CONTINUED) 6. Maintenance of a Balance Between Activity and Rest
Condition of skin at pressure points, activity restrictions/limitations, mechanical devices for assistance, gait endurance, general movement (coordination, stability), muscle strength, tone and mass, range of motion, posture, handedness, deformities, paralysis, weakness, rehabilitative measures, usual sleep patterns, alterations due to hospitalization, medications affecting sleep, usual bedtime and arising time, number of arousals, position for sleep, measures to induce sleep (drinks, reading, bath, medications), environmental conditions, number and length of naps, exercise, type of activity, frequency, duration, presence of pain or discomfort (location, duration, degree, extent, character, precipitating factors), use of aids to relieve pain and discomfort (medications, comfort measures), response to medications or comfort measures, conditions lessening ability to tolerate pain, pain threshold.
7. Maintenance of a Balance Between Solitude and Social Interaction
Presence/absence of roommate, solitary and social activities, visitors (who, when, how many), phone calls, flowers, gifts, presence of television/phone/radio, depression, withdrawn, anxious, isolates self, ability/inability to leave hospital room including isolation requirements, arrangement of environment conducive for visitors, presence/absence of uninterrupted time for visitors, level of consciousness, ability to verbalize, communication skills, living arrangements at home, spiritual assessment, medications altering mood or emotional response, awareness of reality, presence/absence of privacy.
8. Promotion of Normalcy
Threats to biological integrity or self esteem, actual or potential, interference with necessary satisfaction of basic needs, loss of control related to decisions and choices affecting one's self, loss of identity, changes in body image, loss of personal space, effects of health status on sexuality, effects of health status on role with family and significant others, presence/absence of pain, modification of life style or self concept due to illness, possession/lack of self esteem including feelings of dependence/independence, desire, knowledge, and ability to engage in self-care.
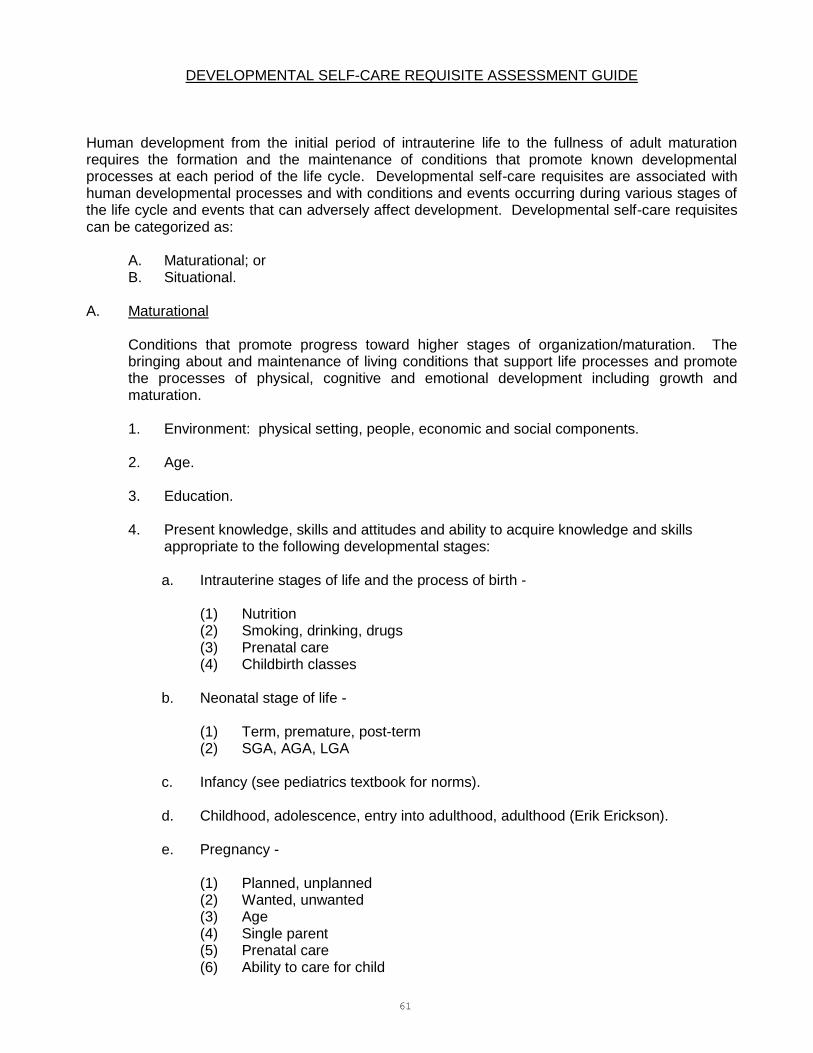
61
DEVELOPMENTAL SELF-CARE REQUISITE ASSESSMENT GUIDE Human development from the initial period of intrauterine life to the fullness of adult maturation requires the formation and the maintenance of conditions that promote known developmental processes at each period of the life cycle. Developmental self-care requisites are associated with human developmental processes and with conditions and events occurring during various stages of the life cycle and events that can adversely affect development. Developmental self-care requisites can be categorized as:
A. Maturational; or B. Situational.
A. Maturational
Conditions that promote progress toward higher stages of organization/maturation. The bringing about and maintenance of living conditions that support life processes and promote the processes of physical, cognitive and emotional development including growth and maturation.
1. Environment: physical setting, people, economic and social components.
2. Age.
3. Education.
4. Present knowledge, skills and attitudes and ability to acquire knowledge and skills appropriate to the following developmental stages:
a. Intrauterine stages of life and the process of birth -
(1) Nutrition (2) Smoking, drinking, drugs (3) Prenatal care (4) Childbirth classes
b. Neonatal stage of life -
(1) Term, premature, post-term (2) SGA, AGA, LGA
c. Infancy (see pediatrics textbook for norms).
d. Childhood, adolescence, entry into adulthood, adulthood (Erik Erickson).
e. Pregnancy -
(1) Planned, unplanned (2) Wanted, unwanted (3) Age (4) Single parent (5) Prenatal care (6) Ability to care for child

62
DEVELOPMENTAL SELF-CARE REQUISITE ASSESSMENT GUIDE (CONTINUED) B. Situational
Prevention of deleterious effects on development/situation. Provision of care either to prevent the occurrence of deleterious effects of conditions that can affect human development or to
decrease or overcome these effects from conditions such as the following:
1. Educational deprivation -
a. Lack of knowledge. b. Ability to learn. c. Past learning experiences.
2. Problems of social adaptation.
3. Failure of individuation -
a. Erickson's developmental stages/signs of failure to attain.
4. Loss of relatives, friends, associates -
a. When did loss occur? b. Why and how did loss occur? c. Who was lost and what was the meaning of the loss to the person? d. Is the loss potential, temporary or permanent?
5. Loss of occupational security and/or possessions -
a. When, why and how did loss occur? b. Is loss potential, temporary or permanent?
6. Abrupt change of residence to an unfamiliar environment -
a. Why, how and when did change occur? b. Is it potential, temporary or permanent?
7. Status-associated problems -
a. Will patient status be affected by condition? b. Will it be readily observable or able to be concealed? c. Is it potential, temporary or permanent?
8. Poor health or disability -
a. How does it affect ADL? b. How does it affect ability for growth, development and maturation? c. Is it potential, temporary or permanent?

63
DEVELOPMENTAL SELF-CARE REQUISITE ASSESSMENT GUIDE (CONTINUED) 9. Oppressive living conditions -
a. How do they affect ability to deal with condition? b. How long have they been this way? c. What is the potential for change?
10. Terminal illness and impending death -
a. Patient and family awareness. b. Stage of death and dying (Kubler-Ross). c. Support systems available. d. Cause of illness.

64
HEALTH DEVIATION SELF-CARE REQUISITE ASSESSMENT GUIDE
A. Basic Conditioning Factor Information Required
1. Diagnosis.
2. Treatment:
a. Procedures. b. Medications. c. Self-care requisites: activities of daily living which must be modified because of
diagnosis. B. Health Deviation Self-Care Requisites Assessment
1. Seek/secure medical assistance with exposure/evidence of conditions associated with pathology:
a. Knowledge of cause and effects of pathological state. b. Knowledge of signs and symptoms of pathological state. c. Willingness to seek and secure medical assistance. d. Ability and resources to seek and secure medical assistance.
2. Be aware/attend to effects of pathological state:
a. Knowledge of effects and signs and symptoms. b. Effects, signs and symptoms of treatment procedures and medications. c. Ability to gain the above knowledge. d. Alertness, awareness. e. Ability to take action for untoward effects.
3. Carry out medically prescribed measures related to prevention/regulation/
compensation for pathology:
a. Knowledge of medically prescribed measures. b. Ability or willingness to learn. c. Motivation to carry out measures. d. Mental and physical abilities to carry out the measures.
4. Be aware/attend to/regulate discomforting/deleterious effects of prescribed measures:
a. Knowledge of the effects and their signs and symptoms. b. Knowledge of means to control these effects. c. Ability to learn. d. Ability to be aware of and attend to the effects. e. Physical ability to carry out control measures. f. Willingness to be aware of and take care of the effects.
65
HEALTH DEVIATION SELF-CARE REQUISITE ASSESSMENT GUIDE (CONTINUED)
5. Modify self-concept in acceptance of particular state:
a. Self-esteem, self-concept. b. Behavior as it relates to the particular state (verbal/nonverbal). c. Changes in body image, loss of control, identity, status and satisfaction of basic
needs as they relate to health state. d. Meaning of above changes to individual.
6. Learn to live with effects of health state and/or prescribed measures so that the life-style
promotes personal development:
a. Knowledge of the health state and prescribed measures. b. Past history of self-care as it relates to the health state and prescribed measures. c. Ability to learn. d. Willingness to alter life-style. e. Resources and support system necessary to assist person to alter life-style. f. Meaning of changes in life-style to individual.

66
NURSING THEORY: SELF-CARE DEFICIT
SELF-CARE LIMITATIONS: Limitations that restrict individuals in providing the amount and kind of self-care required. 1. Limitation of knowing about one's own functioning, needed self-care and the methods through
which self-care is accomplished. These limitations are associated with past experience (or lack of it) and with what is being experienced in the present.
a. New requirements for knowledge related to new health deviations, diagnostic measures
and treatments.
b. Impaired sensory or cognitive function that impairs the ability to either perceive or under- stand what is occurring in one's environment or within oneself. This would include impaired perception, memory, consciousness, or rationality.
c. Inappropriate mental functioning. Psychic and cognitional limitations for developing
insights about situations, for seeking to acquire knowledge and for the "knowing" that is basic to "doing". This includes giving meaning to situations that is not in accord with reality and denial of the meaning of a situation. Limitations in this group impair an individual's ability to know when action needs to be taken, to adjust or adapt actions to changing situations, to know when to stop actions and the ability to organize actions into meaningful sequences.
2. Limitations for making judgments and decisions
a. Lack of learning skills or skills for seeking and acquiring knowledge and lack of ability to reflect and reason.
b. Inability to direct and maintain attention necessary to investigate situations from the
stand-point of self-care.
c. Lack of motivation and decision making skills. Avoidance of decision-making. 3. Limitations for engagement in result achieving courses of action
a. Lack of knowledge or resources.
b. Limitations related to energy and control of body movements and being able to attend to or monitor oneself.
c. Lack of motivation: lack of interest, lack of feeling want or desire to meet perceived
needs, inadequate goal orientation, low value placed on self-care (or on "self"). d. External interferences such as deliberate interference by family or others, patterns of
living, lack of support system, and crisis or disaster situations (Orem, 1985).
67
EXAMPLES OF NURSING DIAGNOSES REFLECTING THE DIFFERENT FOCI MEDICAL MODEL Impaired physical mobility related to amputation of left lower
extremity below knee. SELF-CARE MODEL Impaired physical mobility: unable to compensate for altered
mobility related to lack of knowledge and required skills. MEDICAL MODEL Alteration in peripheral tissue perfusion related to surgical
intervention and trauma. SELF-CARE MODEL Alteration in comfort, pain, related to inability to control
physiological responses. SELF-CARE MODEL Alteration in comfort, pain: unable to maintain pain control related to lack of repertoire skills (and hospital policy). The Self-Care Model moves the focus of attention from the patient's body part to the total patient. Goals: (1) Continuous, ongoing self-care.
(2) Increased self-care agency.
68
REFERENCES
Antelope Valley College Associate Degree Nursing Program. (2009). Mandatory Resource Manual. Hill, L. & Smith, N.L. (1985). Self-Care Nursing: Promotion of Health. Norwalk, Connecticut: Appleton-Century-Crofts. Jewish Hospital of St. Louis School of Nursing (material adapted and used with their permission). Orem, D. E. (1985). Nursing: Concepts of Practice, New York: McGraw-Hill Book Co.
69
MODULE 4 NURSING PROCESS
AND
NURSING CARE PLANS

70
RECOMMENDED TEXTS For all courses except NS 121 Gulanick, M. and Myers, J.L. Nursing Care Plans: Nursing Diagnosis and Intervention, 7th Edition,
2011: Mosby, St. Louis. (ISBN: 0-323-03954-5)
For NS 121 Ladwig, G.G. and Ackley, B.J. Guide to Nursing Diagnosis, 3rd Edition, 2010: Mosby, St. Louis. (ISBN: 0-323-07172-4)
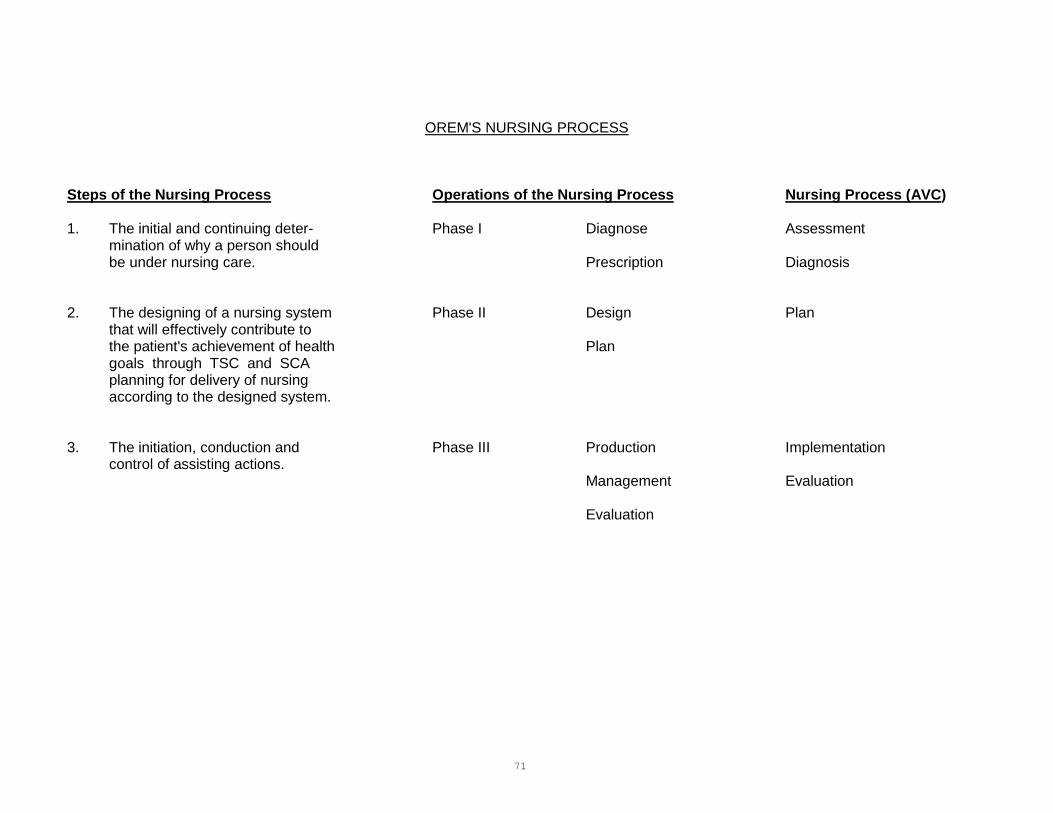
71
OREM'S NURSING PROCESS
Steps of the Nursing Process Operations of the Nursing Process Nursing Process (AVC) 1. The initial and continuing deter- Phase I Diagnose Assessment
mination of why a person should be under nursing care. Prescription Diagnosis
2. The designing of a nursing system Phase II Design Plan
that will effectively contribute to the patient's achievement of health Plan goals through TSC and SCA planning for delivery of nursing according to the designed system.
3. The initiation, conduction and Phase III Production Implementation
control of assisting actions. Management Evaluation
Evaluation

72
DEFINITIONS OF NURSING PROCESS NURSING PROCESS The process of determining why a person needs nursing, designing a system of nursing assistance, planning for the delivery of the specified nursing assistance, and providing and controlling the delivery of nursing assistance in the nursing process. Antelope Valley College’s nursing process is listed first with correlating Orem’s Nursing process in parenthesis. ASSESSMENT (DIAGNOSIS) This is an investigative operation that enables nurses to make judgments about the existing health care situation and decisions about what can and should be done. It focuses on the question "What is?" and "Why?" Nurses in this operation of the nursing process are looking for the answers to five questions: (1) What is the patient's Therapeutic Self-Care Demands (TSCD) now? At a future time? (2) Does the patient have a deficit for engaging in self-care to meet the TSCD? (3) If so, what is its nature and the reasons for its being there? (4) Should the patient be helped to refrain from engaging in self-care or to protect already developed self-care capabilities for therapeutic purposes? (5) What is the patient's potential for engaging in self-care at a future time period? Increasing
self-care knowledge and skills? Motivation to engage in self-care? DIAGNOSIS (PRESCRIPTION) Prescription gives direction. It identifies the self-care deficit, either existing or projected. In relation to the question of Diagnosis, "What is?" and "Why?" it focuses on the questions "What should be?" and "What can be?". This is the goal setting operation. PLAN (DESIGNING) This operation prioritizes the patient's TSCD and selects the methods of assisting that will be effective and efficient in compensating for or overcoming a patient's self-care deficits. Design also specifies who and to what degree nurses and patients will be involved in the production of the patient's self-care.
73
DEFINITIONS FOR NURSING PROCESS (CONTINUED) PLAN (PLANNING) This operation is the movement from the design of the nursing systems to ways and means for their production. This sets forth the organization and timing of essential tasks to be performed. It allocates their performance to nurse or patients and designates how patients are to be helped by nurses in task performance. IMPLEMENTATION (PRODUCTION) This operation involves the actual performance of the planned activities. EVALUATION (EVALUATION) This operation involves looking at the goals to determine if the goal has or has not been met and if so, to what extent it has been met. EVALUATION (MANAGEMENT) This operation involves making adjustments in patient care based upon the results of the evaluation. This is a continuous ongoing process.

74
SUGGESTED NURSING DIAGNOSES UNIVERSAL SELF-CARE REQUISITES Hazards Health maintenance, alteration in Risk for infection Risk for injury (potential for poisoning; for suffocation; for trauma) Skin integrity, impaired (allergies) Violence, risk for: self-directed or other-directed Food Breastfeeding, effective Breastfeeding, ineffective Breastfeeding, interrupted Impaired swallowing Infant feeding pattern, ineffective Nutrition, alteration in: more than body requirements Nutrition, alteration in: less than body requirements Nutrition, alteration in: actual Nutrition, alteration in: risk Oral mucous membrane, alteration in Risk for aspiration Self-care deficit (less able to feed self) Water Fluid volume deficit, actual Fluid volume deficit, risk Fluid volume excess Oral mucous membrane, alteration in Air Airway clearance, ineffective Breathing pattern, ineffective Cardiac output, alteration in: decreased Gas exchange, impaired Peripheral neurovascular dysfunction, high risk for Risk for suffocation Tissue perfusion, alteration in: cerebral, cardiopulmonary, renal, gastrointestinal, peripheral Ventilation, inability to sustain spontaneous Ventilatory weaning response, dysfunctional
75
SUGGESTED NURSING DIAGNOSES (CONTINUED) Rest/Activity Activity intolerance, actual Activity intolerance, risk for Disuse syndrome, high risk for Dysrefleria Impaired physical mobility Impaired tissue integrity Self-care deficit Skin integrity impairment, actual Skin integrity impairment, high risk for impaired Sleep pattern disturbance Elimination Bowel elimination, alteration in: constipation Bowel elimination, alteration in: diarrhea Constipation, colonic Constipation, perceived Functional incontinence Incontinence, bowel Reflex incontinence Self-care deficit Skin integrity impairment, actual Skin integrity impairment, risk for Stress incontinence Total incontinence Urinary elimination, alteration in patterns Urinary retention Solitude/Social Interaction Social isolation Impaired verbal communication Spiritual distress (inability to carry out rituals) Social interaction, impaired Diversional activity deficit Normalcy Altered sexuality patterns Alteration in comfort, chronic pain Alteration in comfort, pain Anxiety, fear Caregiver role strain Caregiver role strain, high risk Coping, defensive Coping: ineffective individual Decisional conflict Hopelessness Knowledge deficit

76
SUGGESTED NURSING DIAGNOSES (CONTINUED) Normalcy Parental role conflict Personal identity disturbance Post-trauma response Powerlessness Rape/trauma syndrome Role performance, altered Self-esteem, chronic low Self-esteem, disturbance Self-esteem, situational low Self-mutilation, high risk for Sensory perceptions, alteration in: visual, auditory, kinesthetic, gustatory, tactile, olfactory Sexual dysfunction Spiritual distress Thought processes, alteration in Unilateral neglect

77
SUGGESTED NURSING DIAGNOSES DEVELOPMENTAL REQUISITES Maturation: Progress toward higher stages of organization
Altered growth and development Altered sexuality patterns Body image disturbance Caregiver role strain Caregiver role strain, high risk Coping: ineffective family, compromised Coping: ineffective family, disabling Coping: potential for family growth Diversional activity deficit Family process, alteration in Impaired social interaction Impaired verbal communication Ineffective family coping Ineffective breastfeeding Ineffective infant feeding patterns Knowledge deficit Parental role conflict Parenting, alteration in Risk for injury Protection, altered Role performance, altered Sensory/perceptual alteration Sexual dysfunction Spiritual distress Violence, risk for Situational: Prevention of deleterious effects on development
Altered sexuality patterns Anxiety Body image disturbance Coping, effective, individual Diversional activity deficit Grieving, anticipatory Grieving, dysfunctional Hopelessness Impaired adjustment Impaired social interaction Impaired verbal communication Knowledge deficit Post trauma response Powerlessness Rape trauma syndrome Relocation stress syndrome Self-concept, disturbance in Sleep pattern disturbance Social isolation

78
SUGGESTED NURSING DIAGNOSES
HEALTH-DEVIATION REQUISITES Seek/secure medical assistance with exposure/evidence of conditions associated with pathology Health seeking behaviors (specify) Noncompliance Knowledge deficit Be aware/attend to effects of pathological states Health maintenance, alteration in Hyperthermia Hypothermia Impaired gas exchange Ineffective airway clearance Ineffective breathing patterns Ineffective thermoregulation Knowledge deficit Noncompliance Risk alteration in body temperature Risk for infection Risk for injury Unilateral neglect Carry out medically prescribed measures related to prevention/regulation/compensation for pathology Activity intolerance Altered nutrition: more than body requirements Altered nutrition: less than body requirements Fatigue Fluid volume deficit Fluid volume excess Health maintenance, alteration in Impaired physical mobility Impaired skin integrity Infection transmission, high risk for Knowledge deficit Noncompliance Risk for infection Risk for injury Self-care deficit Unilateral neglect
79
HEALTH DEVIATION REQUISITES (CONTINUED) Be aware/attend to/regulate discomforting/deleterious effects of prescribed measures Altered sexuality patterns Disuse syndrome, high risk for Diversional activity deficit Dysfunction, high risk for Dysrefleria Fatigue Health maintenance, alteration in Impaired communication Impaired physical mobility Ineffective management of therapeutic regimen Knowledge deficit Noncompliance Peripheral neurovascular Risk for injury Social isolation Unilateral neglect Ventilation, inability to sustain spontaneous Ventilatory weaning response, dysfunctional Modify self-concept in acceptance of particular states Altered sexuality patterns Anxiety Coping, impaired individual Fear Health seeking behavior (specify) Hopelessness Impaired adjustment Noncompliance Personal identity disturbance Post trauma response Powerlessness Self-concept, disturbance in Social isolation Spiritual distress Learn to live with effects of health state and/or prescribed measures so that the life-style promotes personal development Altered sexuality patterns Coping, impaired individual Health maintenance, alteration in Health seeking behavior (specify) Hopelessness Impaired adjustment Post trauma response Therapeutic regimen, ineffective management of Unilateral neglect

80
ASSOCIATE DEGREE NURSING PATIENT CARE PLAN GUIDELINE
Name: _______________________________________ Date: ______________________________ Patient’s Initials: _______ Primary Medical Diagnosis: _________________________________________________________________________________________________
BCF and PC
Universal Self-Care
Developmental Self-Care
Health Deviations
Self-Care Deficits
BCF Age, gender, developmental state, relevant life experiences, health care system, health state, socio-cultural orientation, available resources PC Awareness of self and surroundings, physical energy, control body positions and movements, reason, motivation, make and implement decisions of self-care, acquire, retain and utilize knowledge, repertoire of skills, order self-care actions, perform self-care actions
Air
Water
Food
Rest and Activity
Hazards
Elimination
Solitude/Social Interaction
Normalcy
Maturation: Progress toward higher stages of organization/maturation Situational: Prevention of deleterious effects on development
Seek/secure medical assistance with exposure/evidence of conditions associated with pathology Be aware/attend to effects of pathological states Carry out medically prescribed measures related to prevention/ regulation/compensation for pathology Be aware/attend to/regulate discomforting/deleterious effects of prescribed measures Modify self-concept in acceptance of particular states Learn to live with effects of health state and/or prescribed measures so that the life-style promotes personal development
Difference between self-care needs and self-care capabilities

81
NURSING SYSTEM: Only one system may be selected. The selection depends upon the amount of input the self-care agent can provide.
Nursing Diagnosis
Goals
Intervention with Rationale
Evaluation
North American Nursing Diagnosis Association (NANDA) related to factors in assessment data and related factors in nursing diagnosis book.
Goals need to be tailored to a particular individual’s needs, since illness affects each individual in a unique way. Refer back to nursing diagnosis. Goals can be short term or long term. Goals must: (1) Be specific and objective. (2) Include a subject, action verb, performance criteria, special conditions, target time. (3) Be realistic and achievable. (4) Have the patient as subject. (5) Be mutually agreed upon with the patient. (6) Include a date for evaluation.
Patient interventions are planned and carried out to optimize or increase the self-care agency.
Within the chosen nursing system, the nurse selects methods of assistance that are appropriate for the system. These are:
Acting/doing for
Guiding
Supporting – (a) physically (b) psychologically
Providing an environment that promotes personal development
Teaching
1. Interventions should be specific and individualized. For example:
a. Patient-teaching; list specifically what will be taught, not just “patient teaching of wound care,” etc.
b. Use of communications; state specifically what technique you will use, with an example.
c. If a specific teaching activity or consultant is to be called, the person responsible, (i.e., PCG), the shift and date the activity is to occur must be included.
2. If a dependent nursing function is included, it must be based on an independent nursing judgment. For example: “Give prn medication for pain 30 minutes before dressing change.” 3. If a Nursing Assessment is included it must state parameters and what intervention will be taken if the findings are outside the parameters.
4. The intervention should NOT be simply following a doctor’s
order. It must indicate independent nursing judgment.
5. Rationales are statements which reflect the scientific basis for the nursing intervention. A rationale should answer the question why an intervention is important to do so.
6. Each intervention must be supported with a rationale. Each rationale should be referenced with the author, year, and page number.
The patient’s response in relation to the goal should be stated, along with supporting evidence. Include date of evaluation. Adjustments made in patient care based upon results of the evaluation.

82
Associate Degree Nursing Major Care Plan
Name: Date: Patient Initials: Chief Complaint: Primary Medical Diagnosis:
Assessment
Basic Conditioning Factors And Power Components
Universal Self-Care
Developmental Self-Care
Health Deviations
Self-Care Deficits
BCF: Age, gender, developmental state, relevant life experiences, health care system, health state, socio-cultural orientation, available resources PC: Awareness of self and surroundings, physical energy, control body positions and movements, reason, motivation, make and implement decisions of self-care, acquire, retain and utilize knowledge, repertoire of skills, order self-care actions, perform self-care actions
1. Prevention of hazards to life, functioning and well-being:
2. Maintenance of sufficient intake of air: 3. Maintenance of sufficient intake of
food: 4. Maintenance of a sufficient intake of
water: 5. Provision of care associated with
eliminative processes & excrements: 6. Maintenance of a balance between
activity and rest: 7. Maintenance of a balance between
solitude and social interaction: 8. Promotion of normalcy:
Maturational:
Situational:
1. Seek/secure medical assistance:
2. Be aware of pathological state:
3. Carry out medically prescribed measures:
4. Be aware of effaces of prescribed measures:
5. Modify self-concept in acceptance of particular state:
6. Learn to live with health state and prescribed measures:
Unwilling or unable to:

83
Nursing Diagnosis
NANDA terms and related to deficit or limitation (R/T)
Goals
Short-term with time and date and long term with date
Intervention Measurable, independent, and
dependent nursing interventions.
Rationale for Intervention with citation
Evaluation
Explain what worked what did not work, and
how goal was met
1. NANDA:
1. Nursing System (if partly compensatory there must be a patient action):
1. New plan if ineffective:

84
Student Name _________________________________ Date __________________
Nursing Science Major Care Plan Grading Rubric for a 20 Point Care Plan
Criteria Excellent Satisfactory Unsatisfactory
Demographic Sub/Obj Data
Patient name
Age & gender
Chief complaint, subjective
Medical Diagnosis, objective
Points 0.25
Missing information
Points 0
Basic Conditioning
Factors & Power
Components
All 8 BCF’s are fully assessed
All 10 Power Components are fully assessed
Nursing physical assessment is organized and complete
Points 2.5
6-7 BCFs are assessed
8-9 PCs’ are assessed
Nursing physical assessment is complete, but not organized
Points 2
Less then 6 BCFs are assessed, or not fully assessed
Less the 8 PCs are assessed, or not fully assessed
The nursing physical is not complete
Points 0
Universal Requisites
All 8 requisites are completely assessed
Medications are listed under all appropriate requisites
Points 3
All requisites are assessed, but incomplete
Points 2
Less than 8 requisites are assessed
Points 0
Developmental Requisite
Both requisites are fully assessed and clarified
Points 0.5
One requisite is fully assess and clarified
Points 0.25
Neither requisite is fully assess or clarified
Points 0
Health Deviation Requisites
All 6 requisites are fully assessed
Points 0.5
4-5 requisites are fully assessed
Points 0.25
Fewer then 4 requisites are fully assessed
Points 0
Priority Self Care Deficit
Identifies the two priority Self Care Deficits
Points 1
Identifies one priority Self Care Deficit
Points 0.5
Does not identifies either priority Self Care Deficits
Points 0
Self Care Deficit
Both Self Care Deficits are correctly worded and well supported in the preceding assessment
Points 2
One Self Care Deficits is correctly worded and well supported in the preceding assessment
Points 1.5
Neither Self Care Deficits is worded correctly or well supported in the preceding assessment
Points 0
Nursing Diagnosis
Both nursing diagnoses are correctly worded
Both diagnoses correlate with the Self Care Deficit
Points 2
One nursing diagnosis is not correctly worded or
One diagnosis does not correlate with the Self Care Deficit
Points 1.5
The nursing diagnoses are not correctly worded
The diagnoses are not reflected in the Self Care Deficit
Points 0
Goal Goals correlate with the Self Care
Deficit and nursing diagnosis
Goals are patient (not student nurse) oriented
Goals have a timeframe
Goals are measurable and realistic Points 2
Goals correlate with the Self Care Deficit and nursing diagnosis
Goals are patient oriented
Goals have a poorly defined timeframe
Goal is measurable Points 1.25
Goals do not correlate with the Self Care Deficit or nursing diagnosis
Goals have a poor timeframe
Goals are not measurable Points 0
Interventions
12 (3 for each goal) interventions for each goal stated correctly
Points 4
At least 9 interventions stated correctly
Points 3
Fewer then 9 interventions stated correctly
Points 0
Rationales
12 rationales stated correctly
Points 1
At least 9 rationales stated correctly
Points 0.5
Less than 9 rationales stated correctly
Points 0
Evaluation
Correctly stated evaluation for each goal
Points 1
Correctly stated evaluation for 3 goals
Points 0.75
Correctly stated evaluation for less than 3 goals
Points 0
Nursing System
The nursing system for the most dependent intervention is indicated
Points 0.25
The nursing system is not correctly indicated
Points 0
Based on Orem Assessment guidelines in the Resource Manual _______ Total 08/13/09
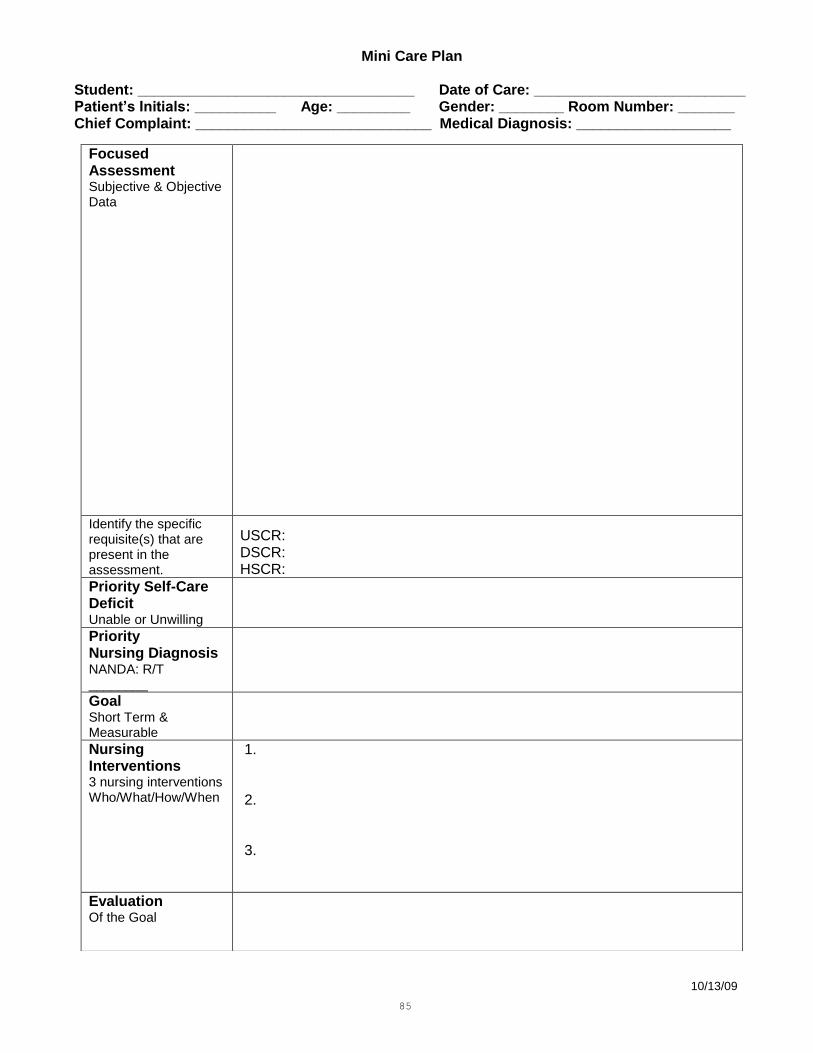
85
Mini Care Plan
Student: __________________________________ Date of Care: __________________________ Patient’s Initials: __________ Age: _________ Gender: ________ Room Number: _______ Chief Complaint: _____________________________ Medical Diagnosis: ___________________
10/13/09
Focused Assessment Subjective & Objective Data
Identify the specific requisite(s) that are present in the assessment.
USCR: DSCR: HSCR:
Priority Self-Care Deficit Unable or Unwilling
Priority Nursing Diagnosis NANDA: R/T ________
Goal Short Term & Measurable
Nursing Interventions 3 nursing interventions Who/What/How/When
1. 2. 3.
Evaluation Of the Goal

86
Name ___________________________________ Date _______________
Nursing Science
Mini Care Plan Grading Rubric (5 points)
Criteria
Excellent
Satisfactory
Unsatisfactory
Demographic Chief complaint/ medical diagnosis
Patient name
Age & gender
Chief complaint,
Medical Diagnosis
Points: 0.25
Missing more than 1 piece of information
Points: 0
Focused Assessment supporting a Self Care Deficit/diagnosis Universal/Developmental/ Health Deviation Requisites
Only data pertinent to the identified Self Care Deficit is recorded.
Includes all relevant subjective/objective data
Selects the requisite that correlates with the Self Care Deficit.
Points: 1.5
Includes data not relevant to Self Care Deficit
Selects the requisite that correlates with the Self Care Deficit
Missing one or more important pieces of assessment data
Points: 1
Includes data not relevant to Self Care Deficit and/or does not include all subjective/objective data
Does not identify requisite.
Points: 0
Priority Self Care Deficit
The priority Self Care Deficit is correctly worded and well supported in the preceding assessment
Points: 0.25
The Self Care Deficit is not well supported in the preceding assessment.
The Self Care Deficit is worded incorrectly.
Points: 0
Priority Nursing Diagnosis
The nursing diagnosis is correctly worded and reflects the Self Care Deficit.
The diagnosis is a priority concern
Points: 0.5
The nursing diagnosis is not correctly worded and does not reflect a priority concern.
Points: 0
Goal
Goal correlates with the Self Care Deficit and nursing diagnosis
Goal is patient/Caregiver oriented
Goal has a time frame.
Goal is measurable and realistic
Points: 0.5
Goal addresses either the Self Care Deficit or nursing diagnosis
Goal is not patient/Caregiver oriented
Goal has no a time frame
Goal is not measurable
Points: 0
Interventions
3 appropriate active interventions for the stated goal that you (student) could carry out independently
All interventions are correctly stated and have a timeframe
Points 1.5
2 appropriate active interventions for the stated goal that you (student) could carry out independently
One or more interventions is not correctly stated or timed
Points: 1
Less than 2 appropriate active interventions for the stated goal that you (student) could carry out independently
Points: 0
Evaluation
Clearly stated evaluation for the goal.
Points: 0.5
Does not clearly state evaluation for the goal.
Evaluates interventions instead of goal.
Points: 0
Based on Orem assessment guidelines in the Resource Manual ____________ Total 10/23/09

87
Physical Assessment Worksheet
Criteria Findings Comments
Vital Signs T_____P_____R_____BP__________Pain_____ Location:
General Appearance Hygiene: BB/PB/Shower/Oral Care/Pericare Posture: Erect/Slumped Gait:____________ HT___________WT__________
Activity:
Neuromuscular LOC: Alert/Oriented (Time/Place/Person/Situation) Confused/Lethargic/Unresponsive PERRL_____/Size_____ Extremities: RU_____LU_____RL_____LL_____ (Use S-strong, W-weak, A-absent)
Describe Deficits
Pulmonary Breath Sounds: Clear/Rales/Rhonchi/Wheezing Diminished Respirations: Labored_______Unlabored________ Mucous Membranes: Pink/Pale/Moist/Dry Oxygen:_______________________ Pulse Ox:_____________________
Treatments:
Cardiac Apical Pulse________ Rhythm: Reg/Irreg Peripheral Pulses: Radial- R/L Pedal- R/L Capillary Refill: R______L______ Edema: Location/ Depth________________________ Homan’s R______L______
Gastrointestinal Appearance: flat/distended/soft/firm Tenderness: _________________________________ Bowel Sounds: ______________________________ % Meals Taken:______________________________ Date of Last BM:_____________________________ Bowel Habits: _______________________________ Intake:_____________Output:___________
Genitourinary Voiding/Ostomy/Foley: Size____________________ Urine Color & Appearance :____________________ Continent/Incontinent
Integumentary Appearance: Warm/Dry/Cool/Cold/Diaphoretic Color: Pink/Pale/Jaundiced/Cyanotic Braden Score:______________________ Pressure Ulcers: Location______________ Stage ___________Size ________________ Dressings:____________________________________
Treatments:
Equipment IV site_________ Appearance_______________ Insertion Date_____________ Tubes: NG/ GT/ Other______________________
Pertinent Lab Data Date/Test/Result___________________________ Date/Test/Result___________________________ Date/Test/Result___________________________
Social/Family Assessment
Developmental Level:__________________________ Family Support:______________________________ Living Situation:_____________________________
Medications Allergies:_________ _________________
Name/Indications/Side Effects for each

88
NURSING PROCESS GOAL STATEMENT SHEET
GOALS MUST:
Be specific, objective and measurable.
Include a subject, action verb, performance criteria, special conditions, target time.
Be realistic and achievable.
Have the patient as the subject.
Be mutually agreed upon with the patient.
Include a date for evaluation.
Indicate that the problem is solved. DO NOT USE DO USE Normal Temperature less than 996 More 80% of meal Less Pain remains less than 3 Satisfactory Will nurse 5 minutes each breast Patient will walk length of hallway with use of Feels walker 3 x day by 10/18. Understands Output greater than 1500 ml Fluid volume deficit Urine light yellow Drinks 8 glasses of water Mucus membranes moist and pink
CAUTION: You must state goals according to our criteria.

89
CARE PLAN CRITERIA REFER TO COURSE SYLLABUS FOR SPECIFIC CRITERIA FOR EACH COURSE.
Complete assessment includes data for BCF power components, universal, developmental and health deviation requisites.
State self-care deficit (with "Unable" or "Unwilling").
Stated nursing diagnosis utilizing NANDA and related factors.
Goal: (1) Include date for evaluation.
(2) Must match diagnosis.
(3) Stated in measurable terms:
a. Teaching/consulting must have date and shift.
b. Pain medication must be specific; use pain scale.
c. Teaching must be specific and measurable.
(4) Must be reasonable and individualized to the patient.
(5) Must start with “Patient will …”
Interventions must be specific and appropriate.
Rationale from the appropriate text must be provided.
Nursing system must be appropriate to patient.
Evaluation – explain whether or not the patient’s goal was met.
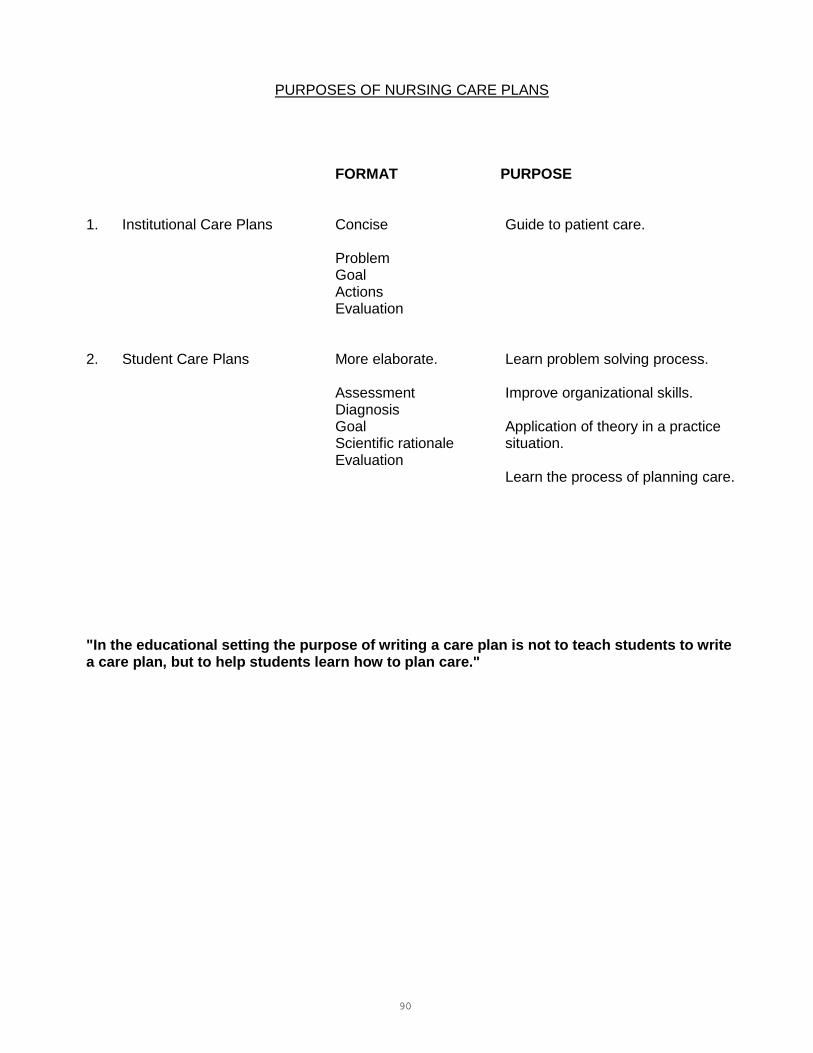
90
PURPOSES OF NURSING CARE PLANS
FORMAT PURPOSE 1. Institutional Care Plans Concise Guide to patient care.
Problem Goal Actions Evaluation
2. Student Care Plans More elaborate. Learn problem solving process.
Assessment Improve organizational skills. Diagnosis Goal Application of theory in a practice Scientific rationale situation. Evaluation
Learn the process of planning care. "In the educational setting the purpose of writing a care plan is not to teach students to write a care plan, but to help students learn how to plan care."
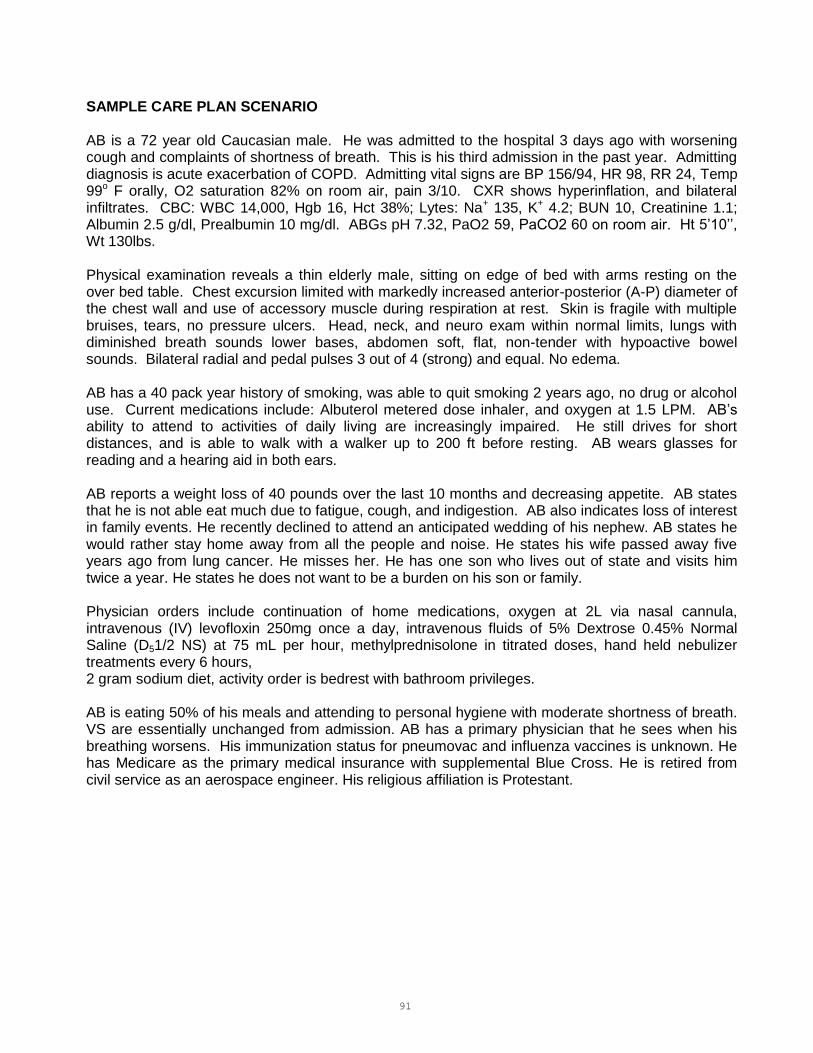
91
SAMPLE CARE PLAN SCENARIO AB is a 72 year old Caucasian male. He was admitted to the hospital 3 days ago with worsening cough and complaints of shortness of breath. This is his third admission in the past year. Admitting diagnosis is acute exacerbation of COPD. Admitting vital signs are BP 156/94, HR 98, RR 24, Temp 99o F orally, O2 saturation 82% on room air, pain 3/10. CXR shows hyperinflation, and bilateral infiltrates. CBC: WBC 14,000, Hgb 16, Hct 38%; Lytes: Na+ 135, K+ 4.2; BUN 10, Creatinine 1.1; Albumin 2.5 g/dl, Prealbumin 10 mg/dl. ABGs pH 7.32, PaO2 59, PaCO2 60 on room air. Ht 5’10’’, Wt 130lbs. Physical examination reveals a thin elderly male, sitting on edge of bed with arms resting on the over bed table. Chest excursion limited with markedly increased anterior-posterior (A-P) diameter of the chest wall and use of accessory muscle during respiration at rest. Skin is fragile with multiple bruises, tears, no pressure ulcers. Head, neck, and neuro exam within normal limits, lungs with diminished breath sounds lower bases, abdomen soft, flat, non-tender with hypoactive bowel sounds. Bilateral radial and pedal pulses 3 out of 4 (strong) and equal. No edema. AB has a 40 pack year history of smoking, was able to quit smoking 2 years ago, no drug or alcohol use. Current medications include: Albuterol metered dose inhaler, and oxygen at 1.5 LPM. AB’s ability to attend to activities of daily living are increasingly impaired. He still drives for short distances, and is able to walk with a walker up to 200 ft before resting. AB wears glasses for reading and a hearing aid in both ears. AB reports a weight loss of 40 pounds over the last 10 months and decreasing appetite. AB states that he is not able eat much due to fatigue, cough, and indigestion. AB also indicates loss of interest in family events. He recently declined to attend an anticipated wedding of his nephew. AB states he would rather stay home away from all the people and noise. He states his wife passed away five years ago from lung cancer. He misses her. He has one son who lives out of state and visits him twice a year. He states he does not want to be a burden on his son or family. Physician orders include continuation of home medications, oxygen at 2L via nasal cannula, intravenous (IV) levofloxin 250mg once a day, intravenous fluids of 5% Dextrose 0.45% Normal Saline (D51/2 NS) at 75 mL per hour, methylprednisolone in titrated doses, hand held nebulizer treatments every 6 hours, 2 gram sodium diet, activity order is bedrest with bathroom privileges. AB is eating 50% of his meals and attending to personal hygiene with moderate shortness of breath. VS are essentially unchanged from admission. AB has a primary physician that he sees when his breathing worsens. His immunization status for pneumovac and influenza vaccines is unknown. He has Medicare as the primary medical insurance with supplemental Blue Cross. He is retired from civil service as an aerospace engineer. His religious affiliation is Protestant.
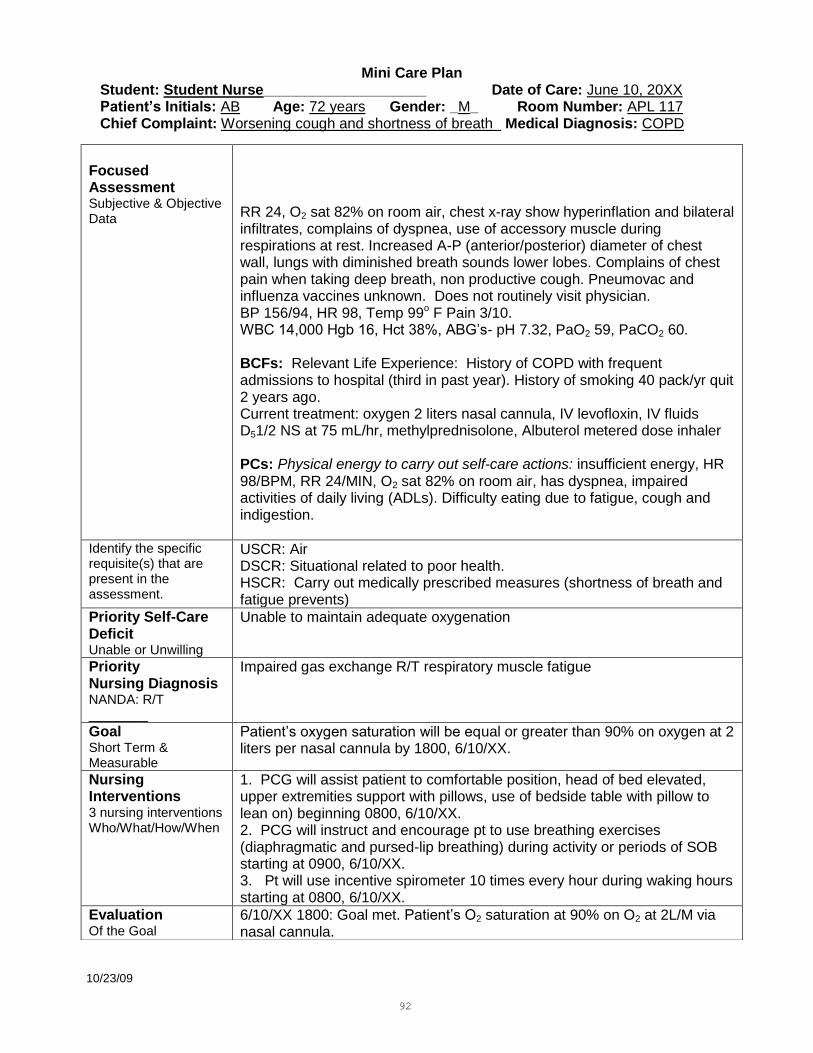
92
Mini Care Plan
Student: Student Nurse____________________ Date of Care: June 10, 20XX Patient’s Initials: AB Age: 72 years Gender: _M_ Room Number: APL 117 Chief Complaint: Worsening cough and shortness of breath Medical Diagnosis: COPD
10/23/09
Focused Assessment Subjective & Objective Data
RR 24, O2 sat 82% on room air, chest x-ray show hyperinflation and bilateral infiltrates, complains of dyspnea, use of accessory muscle during respirations at rest. Increased A-P (anterior/posterior) diameter of chest wall, lungs with diminished breath sounds lower lobes. Complains of chest pain when taking deep breath, non productive cough. Pneumovac and influenza vaccines unknown. Does not routinely visit physician. BP 156/94, HR 98, Temp 99o F Pain 3/10. WBC 14,000 Hgb 16, Hct 38%, ABG’s- pH 7.32, PaO2 59, PaCO2 60. BCFs: Relevant Life Experience: History of COPD with frequent admissions to hospital (third in past year). History of smoking 40 pack/yr quit 2 years ago. Current treatment: oxygen 2 liters nasal cannula, IV levofloxin, IV fluids D51/2 NS at 75 mL/hr, methylprednisolone, Albuterol metered dose inhaler PCs: Physical energy to carry out self-care actions: insufficient energy, HR 98/BPM, RR 24/MIN, O2 sat 82% on room air, has dyspnea, impaired activities of daily living (ADLs). Difficulty eating due to fatigue, cough and indigestion.
Identify the specific requisite(s) that are present in the assessment.
USCR: Air DSCR: Situational related to poor health. HSCR: Carry out medically prescribed measures (shortness of breath and fatigue prevents)
Priority Self-Care Deficit Unable or Unwilling
Unable to maintain adequate oxygenation
Priority Nursing Diagnosis NANDA: R/T ________
Impaired gas exchange R/T respiratory muscle fatigue
Goal Short Term & Measurable
Patient’s oxygen saturation will be equal or greater than 90% on oxygen at 2 liters per nasal cannula by 1800, 6/10/XX.
Nursing Interventions 3 nursing interventions Who/What/How/When
1. PCG will assist patient to comfortable position, head of bed elevated, upper extremities support with pillows, use of bedside table with pillow to lean on) beginning 0800, 6/10/XX. 2. PCG will instruct and encourage pt to use breathing exercises (diaphragmatic and pursed-lip breathing) during activity or periods of SOB starting at 0900, 6/10/XX. 3. Pt will use incentive spirometer 10 times every hour during waking hours starting at 0800, 6/10/XX.
Evaluation Of the Goal
6/10/XX 1800: Goal met. Patient’s O2 saturation at 90% on O2 at 2L/M via nasal cannula.
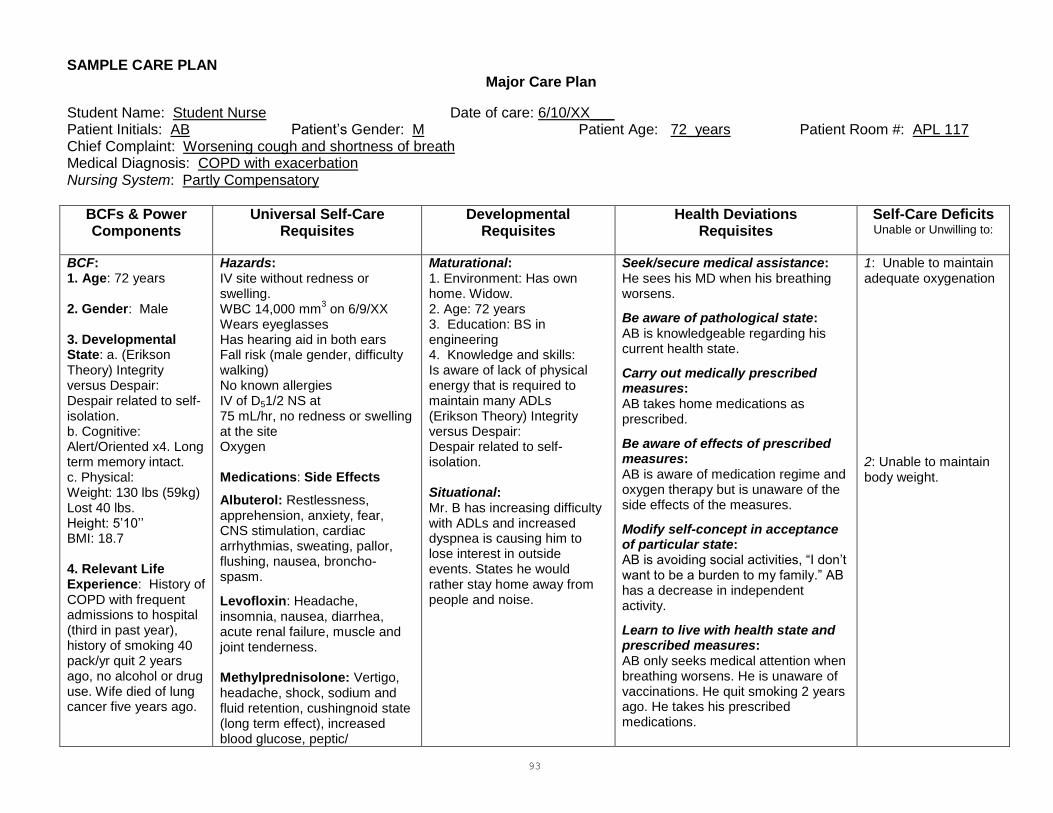
93
SAMPLE CARE PLAN Major Care Plan
Student Name: Student Nurse Date of care: 6/10/XX___ Patient Initials: AB Patient’s Gender: M Patient Age: 72_years Patient Room #: APL 117 Chief Complaint: Worsening cough and shortness of breath Medical Diagnosis: COPD with exacerbation Nursing System: Partly Compensatory
BCFs & Power Components
Universal Self-Care Requisites
Developmental Requisites
Health Deviations Requisites
Self-Care Deficits Unable or Unwilling to:
BCF: 1. Age: 72 years 2. Gender: Male 3. Developmental State: a. (Erikson Theory) Integrity versus Despair: Despair related to self-isolation. b. Cognitive: Alert/Oriented x4. Long term memory intact. c. Physical: Weight: 130 lbs (59kg) Lost 40 lbs. Height: 5’10’’ BMI: 18.7 4. Relevant Life Experience: History of COPD with frequent admissions to hospital (third in past year), history of smoking 40 pack/yr quit 2 years ago, no alcohol or drug use. Wife died of lung cancer five years ago.
Hazards: IV site without redness or swelling. WBC 14,000 mm
3 on 6/9/XX
Wears eyeglasses Has hearing aid in both ears Fall risk (male gender, difficulty walking) No known allergies IV of D51/2 NS at 75 mL/hr, no redness or swelling at the site Oxygen Medications: Side Effects
Albuterol: Restlessness, apprehension, anxiety, fear, CNS stimulation, cardiac arrhythmias, sweating, pallor, flushing, nausea, broncho-spasm.
Levofloxin: Headache, insomnia, nausea, diarrhea, acute renal failure, muscle and joint tenderness. Methylprednisolone: Vertigo, headache, shock, sodium and fluid retention, cushingnoid state (long term effect), increased blood glucose, peptic/
Maturational: 1. Environment: Has own home. Widow. 2. Age: 72 years 3. Education: BS in engineering 4. Knowledge and skills: Is aware of lack of physical energy that is required to maintain many ADLs (Erikson Theory) Integrity versus Despair: Despair related to self-isolation. Situational: Mr. B has increasing difficulty with ADLs and increased dyspnea is causing him to lose interest in outside events. States he would rather stay home away from people and noise.
Seek/secure medical assistance: He sees his MD when his breathing worsens.
Be aware of pathological state: AB is knowledgeable regarding his current health state.
Carry out medically prescribed measures: AB takes home medications as prescribed.
Be aware of effects of prescribed measures: AB is aware of medication regime and oxygen therapy but is unaware of the side effects of the measures.
Modify self-concept in acceptance of particular state: AB is avoiding social activities, “I don’t want to be a burden to my family.” AB has a decrease in independent activity.
Learn to live with health state and prescribed measures: AB only seeks medical attention when breathing worsens. He is unaware of vaccinations. He quit smoking 2 years ago. He takes his prescribed medications.
1: Unable to maintain adequate oxygenation 2: Unable to maintain body weight.
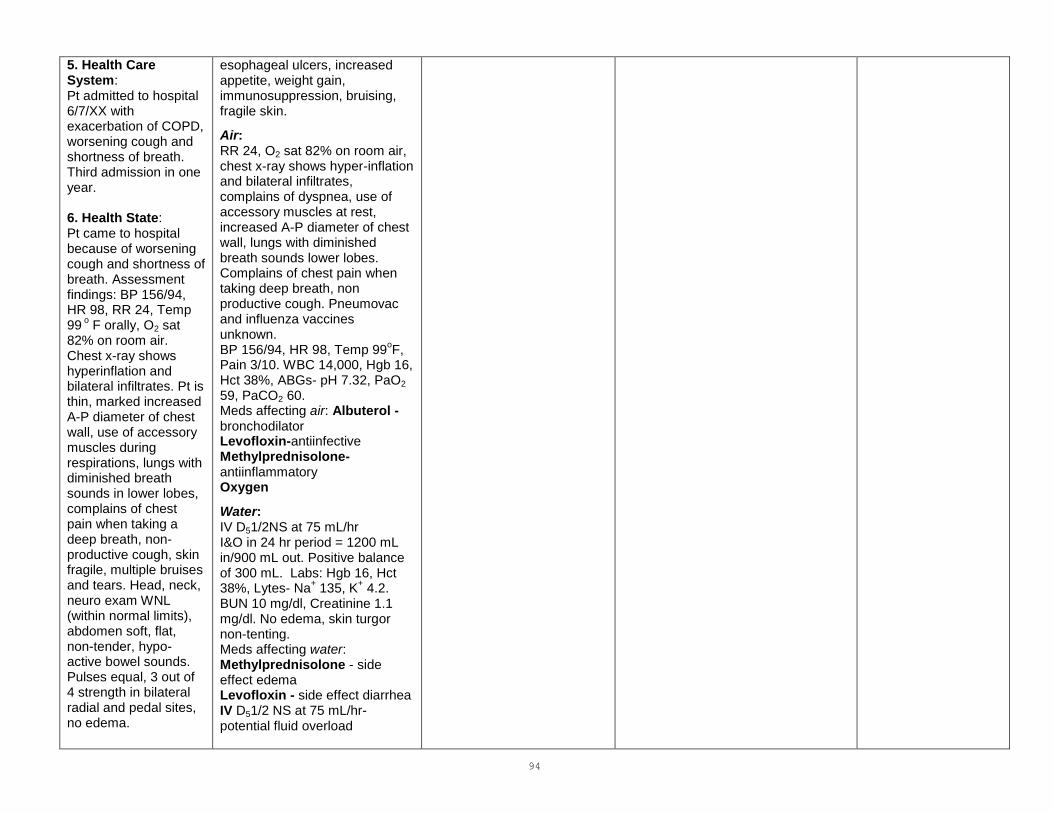
94
5. Health Care System: Pt admitted to hospital 6/7/XX with exacerbation of COPD, worsening cough and shortness of breath. Third admission in one year. 6. Health State: Pt came to hospital because of worsening cough and shortness of breath. Assessment findings: BP 156/94, HR 98, RR 24, Temp 99
o F orally, O2 sat
82% on room air. Chest x-ray shows hyperinflation and bilateral infiltrates. Pt is thin, marked increased A-P diameter of chest wall, use of accessory muscles during respirations, lungs with diminished breath sounds in lower lobes, complains of chest pain when taking a deep breath, non-productive cough, skin fragile, multiple bruises and tears. Head, neck, neuro exam WNL (within normal limits), abdomen soft, flat, non-tender, hypo-active bowel sounds. Pulses equal, 3 out of 4 strength in bilateral radial and pedal sites, no edema.
esophageal ulcers, increased appetite, weight gain, immunosuppression, bruising, fragile skin.
Air: RR 24, O2 sat 82% on room air, chest x-ray shows hyper-inflation and bilateral infiltrates, complains of dyspnea, use of accessory muscles at rest, increased A-P diameter of chest wall, lungs with diminished breath sounds lower lobes. Complains of chest pain when taking deep breath, non productive cough. Pneumovac and influenza vaccines unknown. BP 156/94, HR 98, Temp 99
oF,
Pain 3/10. WBC 14,000, Hgb 16, Hct 38%, ABGs- pH 7.32, PaO2 59, PaCO2 60. Meds affecting air: Albuterol -bronchodilator Levofloxin-antiinfective Methylprednisolone-antiinflammatory Oxygen
Water: IV D51/2NS at 75 mL/hr I&O in 24 hr period = 1200 mL in/900 mL out. Positive balance of 300 mL. Labs: Hgb 16, Hct 38%, Lytes- Na
+ 135, K
+ 4.2.
BUN 10 mg/dl, Creatinine 1.1 mg/dl. No edema, skin turgor non-tenting. Meds affecting water: Methylprednisolone - side effect edema Levofloxin - side effect diarrhea IV D51/2 NS at 75 mL/hr- potential fluid overload

95
Has 40 lb weight loss past 10 months. Expresses loss of interest in family events. Current treatment: oxygen 2L nasal cannula, IV levofloxin, IV fluids D51/2 NS at 75 mL/hr, Methylprednisolone, Albuterol metered dose inhaler. Labs: 6/7/XX (admission) CBC-WBC 14,000, Hgb 16, Hct 38%, Lytes- Na
+ 135,
K+ 4.2. BUN 10,
Creatinine 1.1; Albumin 2.5 g/dl, prealbumin 10 g/dl, ABGs - pH 7.32, PaO2 59, PaCO2 60. 7. Socio-Cultural AB is a Caucasian male, widowed five years ago, has one son who lives out of state, reports loss of interest in family events, states rather stay home away from people. He misses his deceased wife. He is retired. Religious affiliation is Protestant. 8. Available Resources: AB has Medicare for his primary insurance with supplemental Blue Cross. He has an attending physician.
Food: Height 5’10’’ Weight: 130 lbs (59 kg) BMI: 18.7 Albumin 2.5 g/dl (normal 3.4-4.8g/dL), Prealbumin 10 mg/dl (normal 23-45). 2 gm sodium diet, but because of dyspnea, fatigue and cough has not been able to eat. 50% meals eaten. 40 lb weight loss in 10 months. Elimination: Urine 900 mL in 24 hr period. Continent of bowel and bladder. Urine is clear, yellow. Last BM today. Abdomen soft, flat, non-tender with hypoactive bowel sounds. Lytes- Na
+ 135, K
+ 4.2
BUN 10, Creatinine 1.1 Meds affecting elimination: Levofloxin - side effect diarrhea Activity/Rest: Skin fragile with multiple bruises, tears, no pressure ulcers. Ambulates with walker 200 feet then must rest. Sleeps 4 to 6 hours throughout night. Braden Scale 15 (high risk for skin integrity) Meds affecting skin: Methylprednisolone- side effects bruising, fragile skin. Social/Solitude: Loss of interest in family events. Spoke briefly with son on phone from hospital.
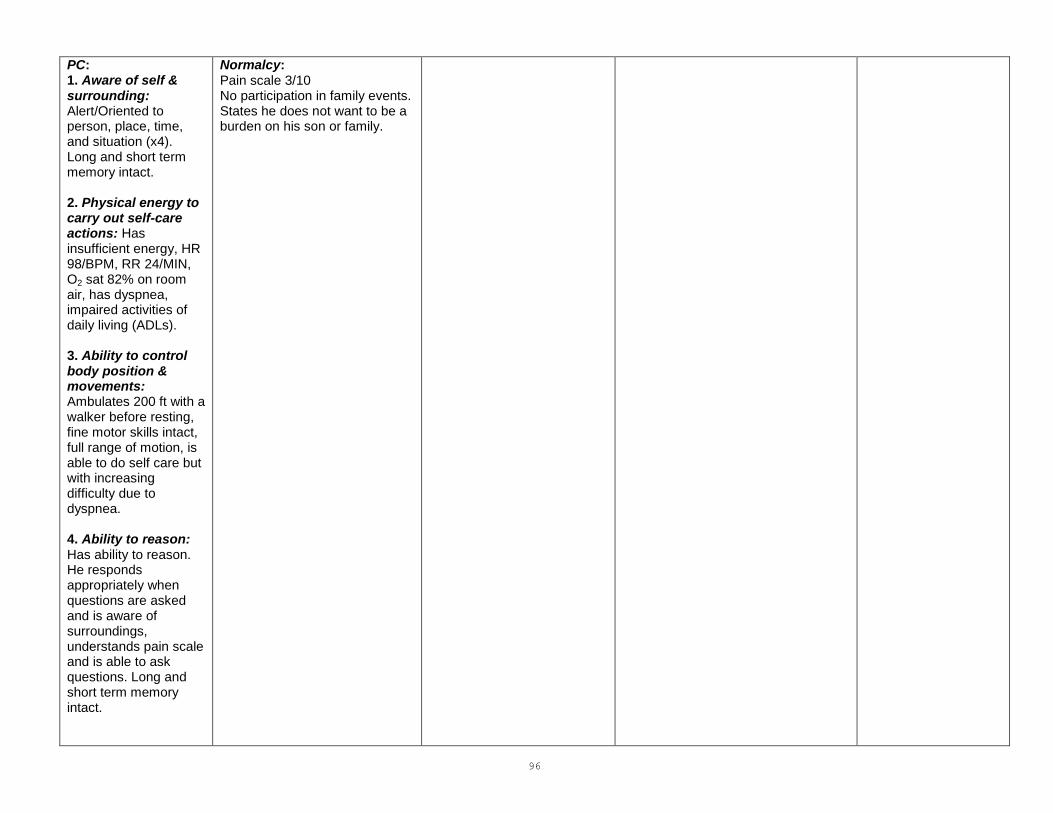
96
PC: 1. Aware of self & surrounding: Alert/Oriented to person, place, time, and situation (x4). Long and short term memory intact. 2. Physical energy to carry out self-care actions: Has insufficient energy, HR 98/BPM, RR 24/MIN, O2 sat 82% on room air, has dyspnea, impaired activities of daily living (ADLs). 3. Ability to control body position & movements: Ambulates 200 ft with a walker before resting, fine motor skills intact, full range of motion, is able to do self care but with increasing difficulty due to dyspnea. 4. Ability to reason: Has ability to reason. He responds appropriately when questions are asked and is aware of surroundings, understands pain scale and is able to ask questions. Long and short term memory intact.
Normalcy: Pain scale 3/10 No participation in family events. States he does not want to be a burden on his son or family.
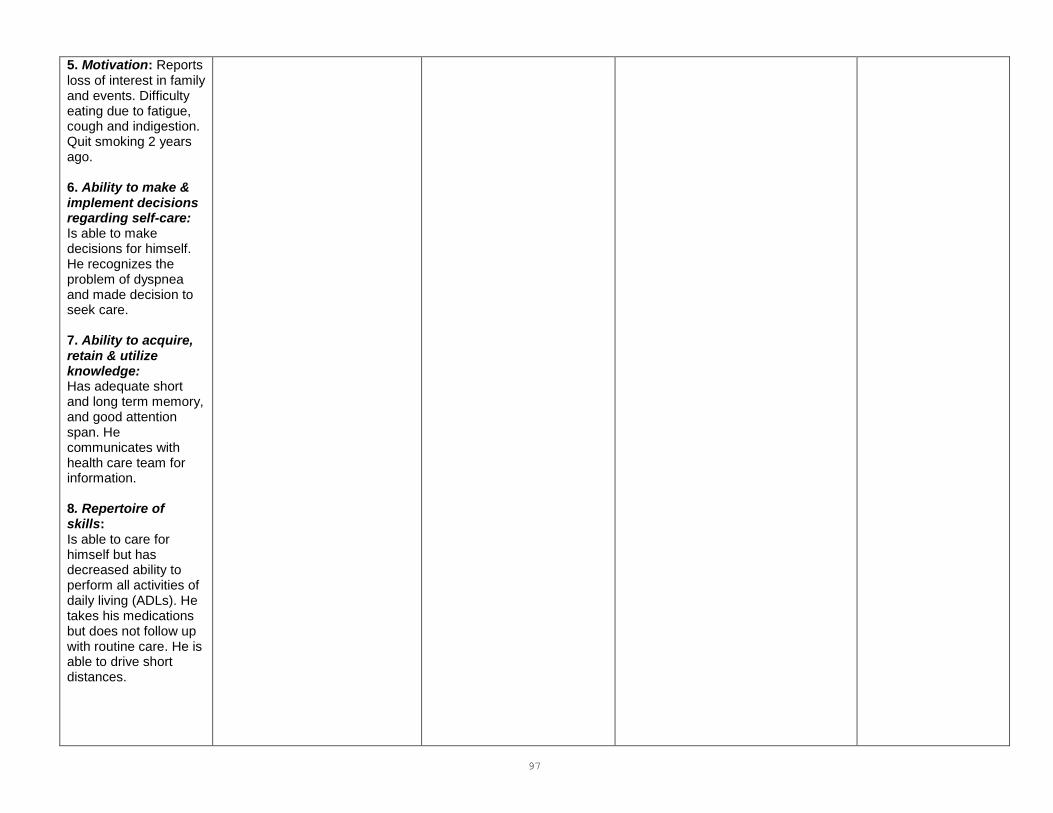
97
5. Motivation: Reports loss of interest in family and events. Difficulty eating due to fatigue, cough and indigestion. Quit smoking 2 years ago. 6. Ability to make & implement decisions regarding self-care: Is able to make decisions for himself. He recognizes the problem of dyspnea and made decision to seek care. 7. Ability to acquire, retain & utilize knowledge: Has adequate short and long term memory, and good attention span. He communicates with health care team for information. 8. Repertoire of skills: Is able to care for himself but has decreased ability to perform all activities of daily living (ADLs). He takes his medications but does not follow up with routine care. He is able to drive short distances.

98
9. Ability to order self care actions: Is able to prioritize self care actions. He takes his medications but does not follow up with routine care. 10. Ability to perform self care actions consistently & to fit them into personal, family & community life: Shows loss of interest in family and outside events. He quit smoking 2 years ago.
10/23/09
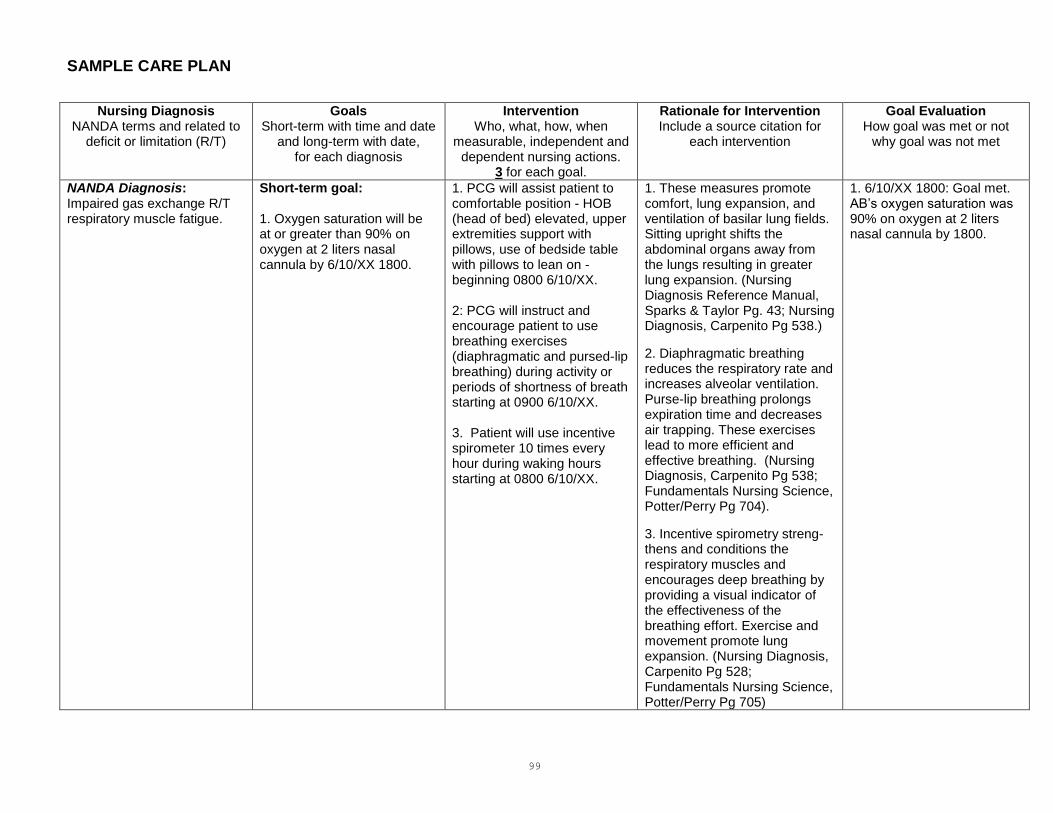
99
SAMPLE CARE PLAN
Nursing Diagnosis NANDA terms and related to
deficit or limitation (R/T)
Goals Short-term with time and date
and long-term with date, for each diagnosis
Intervention Who, what, how, when
measurable, independent and dependent nursing actions.
3 for each goal.
Rationale for Intervention Include a source citation for
each intervention
Goal Evaluation How goal was met or not
why goal was not met
NANDA Diagnosis: Impaired gas exchange R/T respiratory muscle fatigue.
Short-term goal: 1. Oxygen saturation will be at or greater than 90% on oxygen at 2 liters nasal cannula by 6/10/XX 1800.
1. PCG will assist patient to comfortable position - HOB (head of bed) elevated, upper extremities support with pillows, use of bedside table with pillows to lean on - beginning 0800 6/10/XX. 2: PCG will instruct and encourage patient to use breathing exercises (diaphragmatic and pursed-lip breathing) during activity or periods of shortness of breath starting at 0900 6/10/XX. 3. Patient will use incentive spirometer 10 times every hour during waking hours starting at 0800 6/10/XX.
1. These measures promote comfort, lung expansion, and ventilation of basilar lung fields. Sitting upright shifts the abdominal organs away from the lungs resulting in greater lung expansion. (Nursing Diagnosis Reference Manual, Sparks & Taylor Pg. 43; Nursing Diagnosis, Carpenito Pg 538.)
2. Diaphragmatic breathing reduces the respiratory rate and increases alveolar ventilation. Purse-lip breathing prolongs expiration time and decreases air trapping. These exercises lead to more efficient and effective breathing. (Nursing Diagnosis, Carpenito Pg 538; Fundamentals Nursing Science, Potter/Perry Pg 704).
3. Incentive spirometry streng-thens and conditions the respiratory muscles and encourages deep breathing by providing a visual indicator of the effectiveness of the breathing effort. Exercise and movement promote lung expansion. (Nursing Diagnosis, Carpenito Pg 528; Fundamentals Nursing Science, Potter/Perry Pg 705)
1. 6/10/XX 1800: Goal met. AB’s oxygen saturation was 90% on oxygen at 2 liters nasal cannula by 1800.
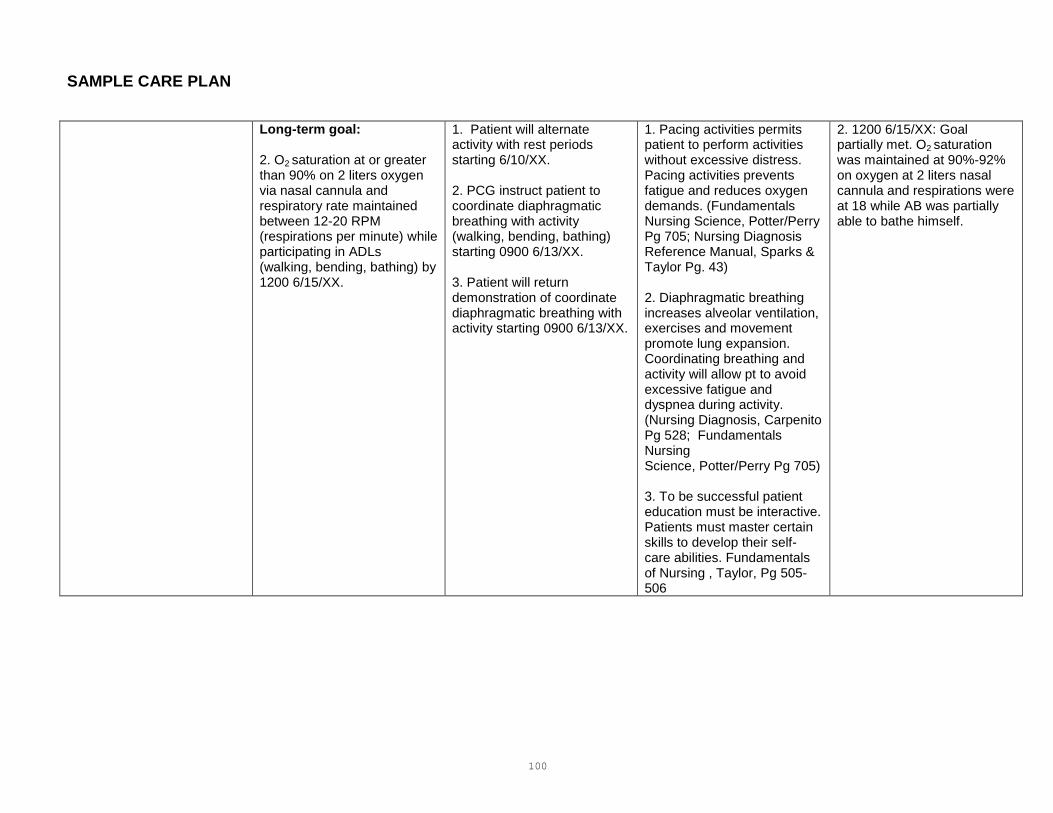
100
SAMPLE CARE PLAN
Long-term goal: 2. O2 saturation at or greater than 90% on 2 liters oxygen via nasal cannula and respiratory rate maintained between 12-20 RPM (respirations per minute) while participating in ADLs (walking, bending, bathing) by 1200 6/15/XX.
1. Patient will alternate activity with rest periods starting 6/10/XX. 2. PCG instruct patient to coordinate diaphragmatic breathing with activity (walking, bending, bathing) starting 0900 6/13/XX. 3. Patient will return demonstration of coordinate diaphragmatic breathing with activity starting 0900 6/13/XX.
1. Pacing activities permits patient to perform activities without excessive distress. Pacing activities prevents fatigue and reduces oxygen demands. (Fundamentals Nursing Science, Potter/Perry Pg 705; Nursing Diagnosis Reference Manual, Sparks & Taylor Pg. 43) 2. Diaphragmatic breathing increases alveolar ventilation, exercises and movement promote lung expansion. Coordinating breathing and activity will allow pt to avoid excessive fatigue and dyspnea during activity. (Nursing Diagnosis, Carpenito Pg 528; Fundamentals Nursing Science, Potter/Perry Pg 705) 3. To be successful patient education must be interactive. Patients must master certain skills to develop their self-care abilities. Fundamentals of Nursing , Taylor, Pg 505-506
2. 1200 6/15/XX: Goal partially met. O2 saturation was maintained at 90%-92% on oxygen at 2 liters nasal cannula and respirations were at 18 while AB was partially able to bathe himself.
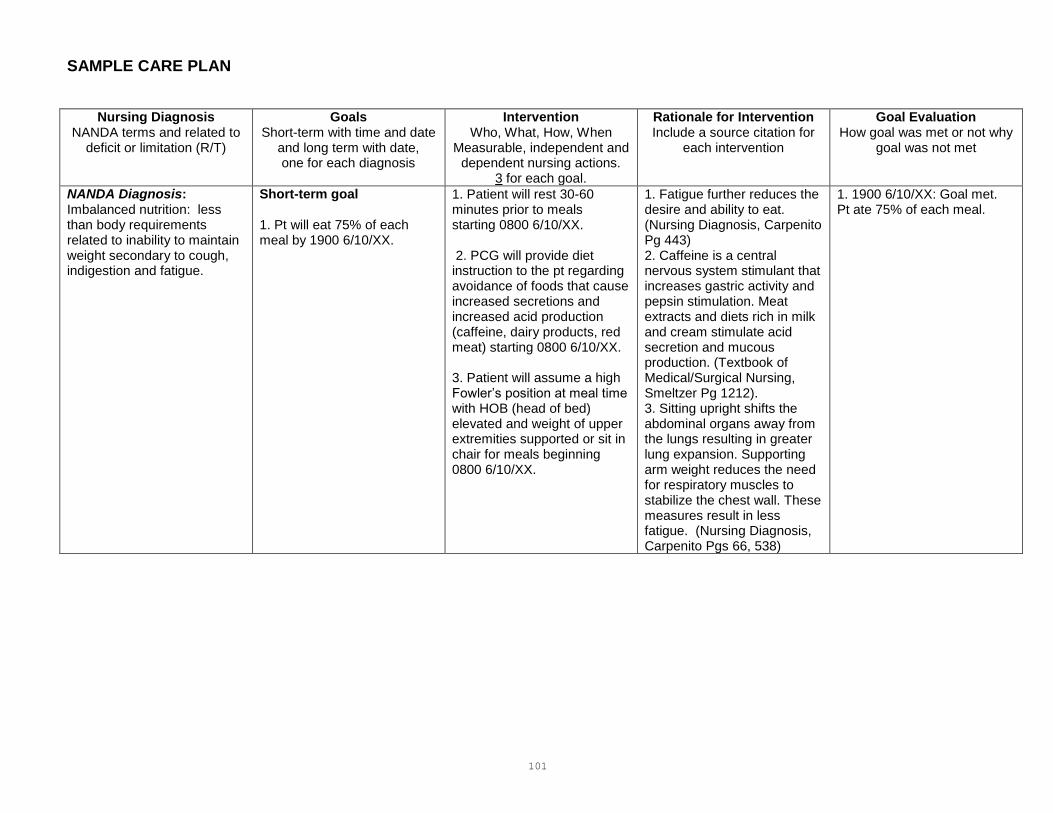
101
SAMPLE CARE PLAN
Nursing Diagnosis NANDA terms and related to
deficit or limitation (R/T)
Goals Short-term with time and date
and long term with date, one for each diagnosis
Intervention Who, What, How, When
Measurable, independent and dependent nursing actions.
3 for each goal.
Rationale for Intervention Include a source citation for
each intervention
Goal Evaluation How goal was met or not why
goal was not met
NANDA Diagnosis: Imbalanced nutrition: less than body requirements related to inability to maintain weight secondary to cough, indigestion and fatigue.
Short-term goal 1. Pt will eat 75% of each meal by 1900 6/10/XX.
1. Patient will rest 30-60 minutes prior to meals starting 0800 6/10/XX. 2. PCG will provide diet instruction to the pt regarding avoidance of foods that cause increased secretions and increased acid production (caffeine, dairy products, red meat) starting 0800 6/10/XX. 3. Patient will assume a high Fowler’s position at meal time with HOB (head of bed) elevated and weight of upper extremities supported or sit in chair for meals beginning 0800 6/10/XX.
1. Fatigue further reduces the desire and ability to eat. (Nursing Diagnosis, Carpenito Pg 443) 2. Caffeine is a central nervous system stimulant that increases gastric activity and pepsin stimulation. Meat extracts and diets rich in milk and cream stimulate acid secretion and mucous production. (Textbook of Medical/Surgical Nursing, Smeltzer Pg 1212). 3. Sitting upright shifts the abdominal organs away from the lungs resulting in greater lung expansion. Supporting arm weight reduces the need for respiratory muscles to stabilize the chest wall. These measures result in less fatigue. (Nursing Diagnosis, Carpenito Pgs 66, 538)
1. 1900 6/10/XX: Goal met. Pt ate 75% of each meal.

102
Long term goal: 2. Pt will maintain current weight of 66.28 Kg by 0800 6/15/XX.
1. PCG will obtain and record weight at the same time every day starting at 0700 6/11/XX. 2. PCG will assist patient to set a target weight and have patient record daily weight starting 6/13/XX. 3. PCG to refer patient to dietician for consult by 1200 6/10/XX.
1. Weighing at the same time every day yields accurate data and gives pt some control over foods eaten and rewards gained. Weight gain should be slow and progressive. (Nursing Diagnosis Reference Manual, Sparks & Taylor Pg. 231; Fundamentals Nursing Science, P&P Pg 1107). 2. Involvement in the nursing care plan improves compliance. (Nursing Diagnosis Reference Manual, Sparks & Taylor Pg. 235). 3. Consultation with a dietician or nutritionist can help ensure a person is following a diet that provides optimal caloric and nutrient intake. (Nursing Diagnosis, Carpenito Pg 443).
2. 0800 6/15/XX: Goal met. AB’s weight is maintained at 66.28 Kg.
10/23/09

103
MODULE 5
SURVIVAL SKILLS FOR
ADN STUDENTS

104
ORIENTATION TO THE MULTIMEDIA TEACHING APPROACH Our nursing science classes are built on a multimedia approach. Our emphasis is on learning rather than on teaching. In order for the student to succeed with the multimedia approach to learning, he/she should: 1. Read the objectives for each module. Determine the application of the objection to the different steps of the nursing process. 2. Read ALL of the required readings. Create a reading schedule to stay on track, it is very possible. Read the content before the lecture. Develop questions to be answered while reading the text. 3. Read the required lecture notes. PowerPoint notes are often available prior to the lecture and should be reviewed. 4. Supplement the above by utilizing the computer software, audio-visual materials and
laboratory practice to meet the objectives, and NCLEX CD review. 5. Seek help from the instructor and skills lab coordinator when needed.
WHAT SHOULD YOU STUDY? 1. Buy all the required reading texts before class starts and begin reading now. 2. Do all the reading, make a schedule. Get it done. 3. Define key terms and make up a good example of the use of each one. 4. Practice critical thinking exercises in textbooks, study guides, accompanying CDs, and the textbook websites. These are best done when first reading the content. 5. Points emphasized in class or text or lecture notes: If the instructor repeated anything or
drew attention to it by writing it on the board, or used emphasis words like "most significant," "the chief cause," etc., take special note of that point.
6. Study the objectives for each module, do this after completing the reading to test your comprehension. 7. Make practice questions using the nursing process to frame them.

105
SUGGESTIONS FOR STRESS MANAGEMENT
1. Find support systems and study groups. 2. Remember the value of exercise. Find the type of exercise that appeals to you on a daily
basis, whether it is walking, jogging, or an aerobic dance class. 3. Find a hobby, something you truly enjoy, and one in which you can forget the tensions of the day. 4. Sleep is important. Give yourself a wind-down time that is non-school related before going
to bed. (Reading a light novel, listening to music; whatever works for you!) 5. Provide yourself with leisure time. Don’t laugh, we mean it, do something fun. 6. Be realistic and flexible when setting your personal goals. 7. Consider seeking outside help when you feel that you are experiencing overwhelming stress.
Use your ASO card for free psychological counseling. 8. Attitude does make a difference! Minimize problems by emphasizing a positive attitude. 9. Remember the value of good nutrition. A person who eats wisely is better able to deal with
stress. Also, cut down or eliminate caffeinated beverages - coffee, tea, cola, or diet beverages. Try herb teas or bottled waters. Minimize sweets and junk foods. Emphasize foods you like that are good for you.
10. Use relaxation techniques or tapes when needed, you will learn some in class. 11. Have a family meeting to gain support for your efforts. 12 Make some new friends in your courses, you have a lot in common with each other; don’t think you are the only one. 13. Make a study plan/schedule and stick to it.
106
STRATEGIES FOR ANSWERING MULTIPLE CHOICE QUESTIONS
107
CHARACTERISTICS OF MULTIPLE CHOICE QUESTIONS
The first part of a multiple choice question is called the stem and the choices that are given for answers are called options. Both of these questions have four options: a, b, c and d. Also, they both illustrate two important characteristics of multiple choice questions: (1) they should be clearly stated; and (2) there should be only one correct answer. 1. Which of the following is the most common cause of death among Americans? a. Cancer of the lungs. b. Coronary heart disease. c. Stroke. d. Hypertension. The correct answer to the question is option b. Many times you will be asked to determine the best right answer, or the first of four reasonable actions you need to take in response to the question being asked. These questions are used to determine your understanding and use of the content. 1. Which of the following actions best represent an elderly patient who is demonstrating compliance in supporting bone health? a. Assures daily sun exposure of a minimum of one hour daily after eating leafy green vegetables. b. Daily walks, supplements diet with calcium and vitamin D capsules. c. Drinks a glass of whole milk with each meal. d. Walks weekly at a moderate pace, eats leafy green vegetables twice a week. The correct answer to the question is option d.
Multiple choice questions can also be either incomplete statements followed by possible ways the statements may be completed, or they are questions followed by possible answers. This example is a question followed by possible answers to it. It is a simple question/answer to determine recall of material. 2. Which of the following medications is in the pharmacological category of ‘antihypertensive’? a. Allopurinol. b. Biaxin. c. Lotensin. d. Roxinol. The correct answer to the question is option b.
108
BASIC STRATEGY FOR MULTIPLE CHOICE QUESTIONS
Multiple choice questions provide one option which is the correct answer and the other options which are distracters. The theory is that correct answers should be selected only by students who know correct answers and other students should be "distracted" and select one of the other options/distracters. Therefore, the strategy to use when answering a multiple choice question is to decide which options are distracters and to select as the correct answer the option that is not a distracter. One way to identify distracters is to analyze a multiple choice question as though it is a series of true/false questions. The following question may be analyzed in this way.
1. Reduced urine production can result from:
a. Diuretic drug effect. b. Improved renal flow. c. Increased cardiac output. d. Reduced fluid intake.
This question, like most multiple choice questions, is actually a series of true/false questions, only one of which is "true". Reduced urine production results from a diuretic drug effect (F) Reduced urine production results from improved renal flow (F) Reduced urine production results from increased cardiac output (F) Reduced urine production results from reduced fluid intake (T) When you answer multiple choice questions, cross out each option that you decide is a distracter. For example:
a. Diuretic drug effect. b. Improved renal flow. c. Increased cardiac output. d. Reduced fluid intake.
In this example, a student has decided that reduced urine production results not from, improved renal flow or increased cardiac output. She has decided the correct answer must be either drug effect or reduced fluid intake, and eventually she will decide that one of these options is a distracter and cross it out too, then select as the correct answer, the option she has decided is not a distracter. The correct answer is option d.

109
SELECT THE ANSWER YOU LEARNED
The questions on college tests are based on application of the information that is printed in course reading material or that is stated during class lectures or discussions. Keep this in mind and you will avoid making unnecessary errors when you answer multiple choice questions. For example, students in a course on diabetes learn that obese people have an increased incidence of insulin resistant diabetes. Some of the students become confused when asked to answer the following question:
1. The incidence of diabetes in obese persons is:
a. Increased. b. Parallel. c. Unchanged. d. Unknown.
The correct answer is increased, but some students are confused by the option parallel and select it. This is an example of an extremely poor test-taking strategy. Since test questions are almost always based on information presented in a course, it is irrational to select an answer because it is not known. The only time an unfamiliar term or phrase should be selected as the correct answer to a question is when it has been determined that all of the other options are distracters.
UNDERLINE NOT, EXCEPT, INCORRECT AND FALSE Many multiple choice questions are answered incorrectly because students fail to observe the words not, except, incorrect and false. It is absolutely essential for you to find not, except, incorrect and false in stems because if you do not find them you may select incorrect answers.
DON'T BE CONFUSED BY EXAMPLES Sometimes multiple choice questions have an example in the stem or a series of examples for options. The following question might appear on a test regarding the planning of patient care.
1. The very experienced nurse wishes to have a written plan of care for an elderly post operative patient. The plan needs to include goals for resumption of walking and eating. Which of the following diagnosis will best serve this patient in achieving the goal?
a. Acute pain, related to surgical incision. b. Risk of immobility related to pain. c. Risk of infection related to surgical incision. d. Risk of injury related fall after opioid administration.
Some students are unnecessarily confused by questions such as this one. They worry, for example, what the importance of the nurse’s experience is and what it was they were supposed to have learned about being experienced in prioritizing nursing diagnoses.

110
DON'T BE CONFUSED BY EXAMPLES (CONTINUED) The question, though, is not about experience or prioritizing, it is about a diagnosis for walking and eating. It could have been written this way:
2. Which of the following nursing diagnoses would address the need for a patient to walk?
a. Acute pain, related to surgical incision. b. Risk of immobility related to pain. c. Risk of infection related to surgical incision. d. Risk of injury related fall after opioid administration.
Option b is the correct answer to both questions. Do not be distracted by the examples in the stems of multiple choice questions. Instead, try to imagine how the stem would be worded if it did not include an example.
DON'T BE CONFUSED BY SEQUENCES
Multiple choice questions about sequences also often cause unnecessary difficulty for some students. The following question might appear on a test for a psychology, sociology, or health education course.
1. Which of the following is the correct sequence of developmental stages for Erickson?
a. Trust versus Mistrust, Autonomy Vs Shame, Doubt. b. Industry versus Inferiority, Trust Vs Mistrust. c. Generative versus Self Absorption and Stagnation, Industry Vs Inferiority. d. Integrity versus Despair, Trust Vs Mistrust.
Students who study sequences will know that the Trust Vs Mistrust stage comes first and that options b and d are, therefore, distracters. They will draw lines through these two options and examine options b and c to decide which of them lists the sequence they studied. The correct answer is a.
ABSOLUTE STATEMENTS MAY BE INCORRECT ANSWERS Absolute statements exclude all possibilities except the one they state. For example:
All patients hate hospital food.
There is no student who enjoys taking tests.
If there is one patient who likes hospital food or one student who enjoys taking tests, these statements are false. Absolute statements often include words such as every, all, always, invariably, best, no, none, never, and worst. These and similar words in the options of multiple choice questions are clues that the options may be distracters. On the other hand, words such as many, most, usually, generally, frequently, often, seldom, and some tend to appear in correct answers. For example:
Many patients do not like hospital food.
Students generally do not enjoy taking tests.
111
ABSOLUTE STATEMENTS MAY BE INCORRECT ANSWERS (CONTINUED) These statements are probably true. When you have difficulty selecting the correct answer to a multiple choice question, you will sometimes find help by remembering that statements are probably incorrect when they include words such as all or never, and they are probably correct when they include words such as some or seldom.
HIGH OR LOW NUMBERS MAY BE INCORRECT ANSWERS Some multiple choice questions have options that are a series of numbers. For example:
1. The oxygen flow rate to a nasal cannula should not exceed:
a. 1 LPM. b. 3 LPM. c. 5 LPM. d. 7 LPM.
When you must guess at a correct number to questions of this type, you are likely to increase your chance of selecting the correct answer if you eliminate the lowest and highest numbers and select from the other options. The correct answer is option c. Of course, you should always answer test questions using information you have learned. However, studies of multiple choice questions have found that when options are a series of numbers, chances are that the correct answer is not the highest or lowest number in the series.
ALL OF THE ABOVE MAY BE THE CORRECT ANSWER While rarely used the following example may be helpful. There is a definite tendency for the option all of the above to be the correct answer to multiple choice questions. All of the above often serves the same function as a more complete answer. Compare the following questions:
1. Nursing assessment of pain reported by a patient should include:
a. Effect on ADLs. b. Location, radiation. c. Quantity, quality. d. All of the above.
Also, when you know that two options are correct and a third option is all of the above, you know that all of the above is the correct answer.
112
ONE OF TWO SIMILAR LOOKING ANSWERS MAY BE CORRECT
When two options for a multiple choice question are similar looking, the correct answer is likely to be one of the two similar looking options. For example: 1. The loss of all sensation in your hand would most likely result from: a. Aphasia. b. Hallucinations. c. Damage to afferent spinal nerves. d. Damage to efferent spinal nerves. Options c and d are very similar looking; the correct answer is option c. Experienced question writers usually write multiple choice questions so that test-takers will not be able to use this clue to correct answers.
MULTIPLE ANSWER TYPE QUESTIONS These questions can occur in 3 different formats and are as follows: A patient had a posterolateral total hip replacement 2 days ago. What should the nurse include in the patient's plan of care? Select all that apply. 1. When using a walker, encourage the patient to point the toes inward. 2. Position a pillow between the legs to maintain abduction. 3. Allow the patient to be in the supine position or in the lateral position on the unoperated side. 4. So not allow the patient to bend down to tie or slip on shoes. 5. Place ice on the incision after physical therapy. (2 , 3, 4, 5) You are required to indicate all that are correct for the question without prioritizing the response. The nurse is monitoring a patient with increased intracranial pressure. What indicators are the most critical for the nurse to monitor? 1. Systolic blood pressure. 2. Urine output. 3. Breath sounds. 4. Cerebral perfusion pressure. 5. Level of pain. a. 1, 3, 4 b. 2, 4, 5 c. 1, 2 d. 1, 4 (correct answer) e. 2, 4, 5 Again the term most is used in the stem and indicates that some of the responses will not be correct.

113
MULTIPLE ANSWER TYPE QUESTIONS (CONTINUED) The nurse must begin teaching a newly diagnosed type I diabetic self-care. In what order should the information be presented to the patient? a. Activity planning. b. Pathophysiology of diabetes. c. When to call the physician. d. Diet. (b, c, e, a) Unless you are told that you will be severely penalized for incorrect answers, always select an answer for every multiple choice question, even if you must guess at some answers. When you guess at any answer to a multiple choice question with four options (a, b, c, and d) you have a 25 percent chance of guessing the correct answer. When you guess at an answer to a multiple choice question that has five options (a, b, c, d and e) you have a 20 percent chance of guessing the correct answer.

114
STUDENT GUIDE
TEST TAKING STRATEGIES
115
PART 1: STRATEGIES TO USE DURING THE TEST A. Read the Question Carefully
1. Keys in the question:
a. Who? b. What? c. When? d. What for?
Question #1 To prevent respiratory complications in the patient who has had abdominal surgery, what nursing actions are of highest priority in the postoperative period?
a. Monitor vital signs every hour until stable. b. Encourage coughing and deep breathing every two hours. c. Apply anti-embolism stockings. d. Administer pain medications as ordered. Who? What? When? What for?
Question #2 To prevent circulatory complications in the patient who has had abdominal surgery, what nursing actions are of highest priority in the postoperative period? a. Monitor vital signs every hour until stable.
b. Encourage coughing and deep breathing every two hours. c. Apply anti-embolism stockings. d. Administer pain medications as ordered. Who? What? When? What for?
116
TEST TAKING STRATEGIES (CONTINUED) Question #3
A 38 year old woman had an abdominal hysterectomy. The nurse is giving preoperative instructions to the woman and her husband. Which statement by the husband indicates to the nurse that more instruction is needed?
a. "My wife will need extra rest for a while when she comes home from the hospital." b. "I will do the grocery shopping for two weeks after she comes home from the hospital." c. "I will call the doctor if there is a lot of bleeding." d. "We will wait a few months before trying to have another baby."
Who? What? When? What for?
Question #4
Which statement indicates the best understanding by the nurse regarding range of motion exercises?
a. All hospitalized persons should have passive range of motion exercises performed. b. Active range of motion exercises should not be performed by persons who have had joint replacement surgery. c. Range of motion exercises are usually appropriate for immobilized patients. d. The nurse should never perform passive range of motion exercises without a written order from the physician.
Who? What? When? What for?
Question #5 The nurse is caring for a newly admitted patient who is in danger of going into shock. While assessing the patient, the nurse should understand which of the following about shock?
a. Blood loss is always present. b. Respirations will decrease. c. Blood pressure rises. d. Respirations may increase.
Who? What? When? What for?

117
TEST TAKING STRATEGIES (CONTINUED) Question #6 The patient is receiving Thorazine. What side effect must the nurse assess the patient for because he is taking Thorazine?
a. Hypertension. b. Elevated blood pressure. c. Orthostatic hypotension. d. Increased vital signs.
Who? What? When? What for?
Question #7
Before taking vital signs, the nurse must:
a. Count the pulse for 30 seconds and multiply by 2. b. Count respirations for one full minute. c. Pump the blood pressure cuff higher than the patient's usual systolic pressure. d. Wash hands.
Who? What? When? What for?
Question #8
The nurse is teaching the patient dietary sources of iron. Which answer the patient gives indicates a need for more instruction?
a. Spinach. b. Broccoli. c. Collard greens. d. Yogurt.
Who? What? When? What for?

118
TEST TAKING STRATEGIES (CONTINUED) Question #9
The nurse is caring for a three-year-old child with a congenital heart defect. The child has a low tolerance for frustration and always wants to have his way immediately. The nurse understands that the primary reason the child with a congenital heart defect has difficulty dealing with frustration is that children with heart defects:
a. Are frequently tired. b. Have had little chance to learn to deal with frustrations. c. Have usually been "spoiled" by their families. d. Are emotionally immature.
Who? What? When? What for?

119
MAKE NOTES FOR STUDYING

120
MAKE NOTES FOR STUDYING 1. Preview before you read and prepare critical thinking questions to be answered. 2. Skim sections of chapters. 3. Read and underline with a purpose. 4. Decide what you want to study. 5. Make notes for studying. Keep notes as simple as possible. Use outline form. Keep words to a minimum. 6. Recite information you want to learn, use flashcards and taped information when you have time. Such as during haircuts and waiting in the HMO clinic urgent care. THE IMPORTANCE OF NOTES There are three reasons it is important for you to make notes for the things you want to learn in your books. 1. The simple act of writing information in notes will often help you learn it
When you make notes, you process information in your mind to state ideas in your words. 2. Written notes reduce the amount of information you need to Learn When you make notes, you are forced to decide what you will and will not learn; the notes for a book do not include all the information in the book. Also, good notes condense information by summarizing it in fewer words than are used in books. 3. Your notes are organized in ways that make it easier for you to learn information
Textbooks are organized to make information understandable to most college students; they are not written with the intention that you will study directly from them. But the notes you make are organized to make it possible for you to learn information in ways that are most efficient and meaningful to you. Notes for books may be written on notebook paper or on 3 x 5 index cards. After underlining or highlighting a chapter of a book and deciding what information you will study in it, use the following guidelines to write notes on paper or cards: 1. Write titles for notes that describe exactly what you want to learn. 2. List the information about topics in your notes in ways that will help you to learn it. 3. Include examples in your notes. Imagine this information applying to or coming from a patient or patient situation.
121
THE IMPORTANCE OF NOTES (CONTINUED) Headings in textbooks will often give you all the help you need to write descriptive titles for notes. When headings for sections of chapters are not very descriptive of the information they explain, rewrite the titles to make them more descriptive. Use words such as method, types, comparison, benefits, characteristics and sequence to write descriptive titles for your notes. Descriptive titles will help you remember information correctly and recall it accurately. List information in notes so it will be easy for you to learn. Examples are included in notes because they aid in understanding the meanings of terms and the explanations of concepts. If you do not have the habit of using examples to help you in understanding and remembering terms and concepts, you are likely to be pleased when you start using them. Students often report that their ability to remember and recall increases dramatically as a result of studying examples in books and thinking of their own examples.

122
STUDY GROUPS
123
STUDY GROUPS If you are not already in a study group, shop around for one. If you can't find one, start one. If you are hesitant just try it out and see how you like it. For example, organize a temporary group to prepare for one event such as a major exam or a massive project. If you like studying and working together, you can meet on a more permanent basis. Your schedule is most likely to mesh with those of other students in your clinical rotation. See if you can interest a half dozen of them in joining you. Successful study groups have certain ground rules. For the group to be effective, every nursing student in it must agree to the following: 1. Understand and accept the group purpose or mission.
2. Contribute ideas, information, opinions, and feelings.
3. Invite and encourage other members to do the same.
4. Listen intently.
5. Demonstrate respect and support for other members.
6. Help keep the discussion relevant.
7. Periodically help summarize the major points.
8. Give examples and share pertinent clinical experiences.
9. Refrain from eating, smoking, or knitting during the session.
HOW TO MAKE A GOOD STUDY GROUP BETTER Time Always meet at the same time. Place Always meet at the same place. Begin Always begin on time. Monitor Appoint a monitor to keep the group on target and the discussion moving. Focus on the here and now. Don't let the group spend too much time dwelling in the past or fretting about the future. Goal At the beginning of the session, state the goal. "Today we will discuss Chapters 4 and 5,” or "This group is reviewing for the anatomy midterm."

124
STUDY GROUPS (CONTINUED) Discuss
Allow free-flowing of discussion anything relevant to the group's goal. Identify major concepts, clarify discrepancies between text and lecture, share examples from clinical experience, and relate theory to practice. If questions arise that cannot be quickly and accurately answered, don't waste time pooling ignorance. Appoint one member to check with the instructor and report back to the group. Review
Review lecture notes, highlights of outside readings, films, class objectives, lists to be memorized, etc. Quiz
Drill each other. Use test questions at the end of the chapter or, better yet, construct your own.
"Lately we've each been bringing two `trivia' questions to group. It's not only fun, it also forces each member to read and review before the study session. Constructing questions has helped me think the way instructors think when they're making up tests."
Summarize
Periodically pause and recap the major points under discussion. At the end of the session, summarize what you have accomplished and list the things that still need to be done. Divide
Whenever possible, divide tasks and activities.
"We split up the objectives, with each member being responsible for just a few. That person gathers the information and brings copies for everyone to the next meeting. It saves so much time!"
Assign
Assign individuals or sub-groups to tasks, and be sure to specify dates for completion. End
Always end on time. When students form study groups or support groups, they are "networking". You may be interested to learn that student networks reach far beyond your own campus. They operate on a national and an international level. If you would like to extend your network log onto:
http://www.ncsbn.org OR http://www.nsna.org Registered nurses band together in groups for the same reason students do – to survive; and for one even better reason – to thrive.
125
MODULE 6
MATH FOR NURSES
126
LEARNING ACTIVITIES
1. The unit method of working problems (dimensional analysis) will be taught in class. 2. Work all problems in the syllabus. Check your answers against the answer key. Please see the instructor about any problems you cannot work. Additional problems can be obtained from the instructor. 3. Take the Review Test in the syllabus. If you score 90 percent or above on it, you are ready for the math examination. (Time allowed is 1 hour, 40 minutes.)
INCLUSIONS 1. Math Guide. 2. Weights and Measures 3. The Dimensional Analysis Method. 4. Practice Problems. 5. Review Test. 6. Review Test - Answer Key. .

127
MATH GUIDE
1. Round the following values to hundredths:
a. mg b. mcg c. kg d. units e. g f. gr
2. Round mL to tenths if more than 1 mL; to hundredths if less than 1 mL. 3. Tablets are usually given as whole numbers. If a tablet is scored, it may be split in half. 4. A suppository can only be cut in half lengthwise. If greater than 0.5 use entire suppository (Pediatrics). 5. Drops (gtts) should be in whole numbers. 6. Round a number up if number to the right of it is 5 or above; the number stays the same if the number to the right of it is 4 or below. 7. Do not convert fractions to decimals within the problem, unless it is an even fraction. 8. Use the closest equivalent; use of multiple equivalents increases inaccuracy of result. 9. Intravenous fluids calculated in mL per hour may be rounded to tenths. 10. Round pounds to tenths.
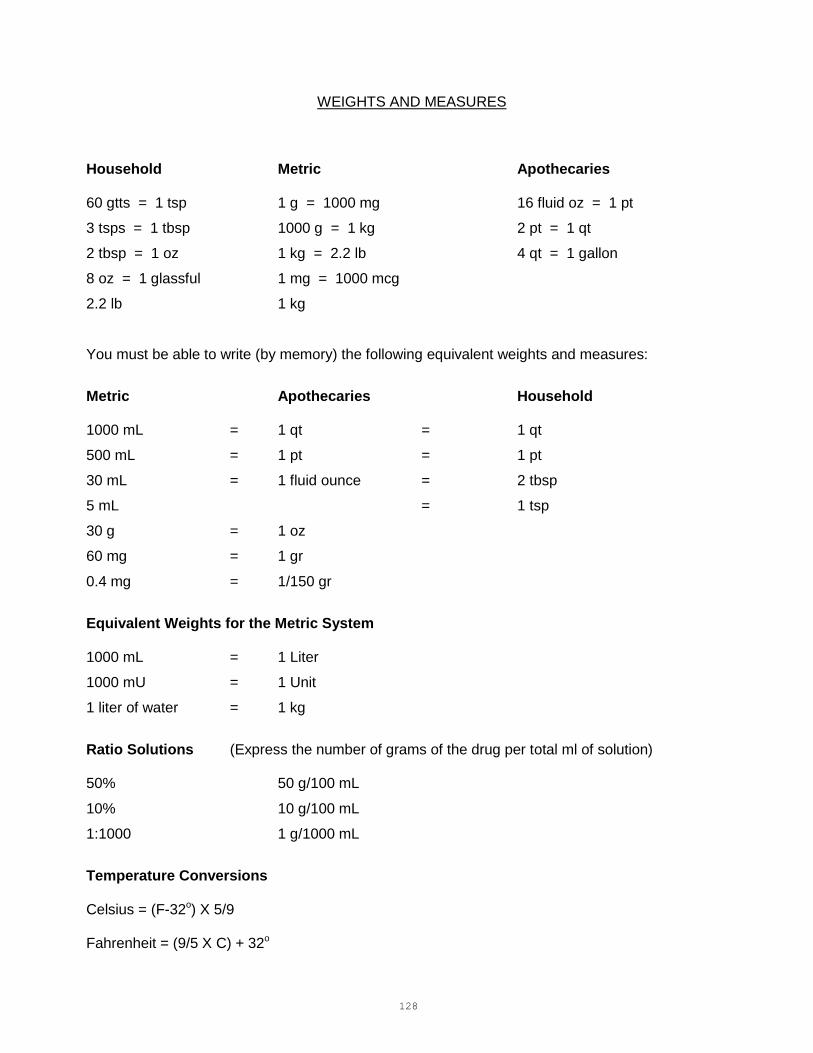
128
WEIGHTS AND MEASURES
Household Metric Apothecaries 60 gtts = 1 tsp 1 g = 1000 mg 16 fluid oz = 1 pt
3 tsps = 1 tbsp 1000 g = 1 kg 2 pt = 1 qt
2 tbsp = 1 oz 1 kg = 2.2 lb 4 qt = 1 gallon
8 oz = 1 glassful 1 mg = 1000 mcg
2.2 lb 1 kg
You must be able to write (by memory) the following equivalent weights and measures:
Metric Apothecaries Household 1000 mL = 1 qt = 1 qt
500 mL = 1 pt = 1 pt
30 mL = 1 fluid ounce = 2 tbsp
5 mL = 1 tsp
30 g = 1 oz
60 mg = 1 gr
0.4 mg = 1/150 gr
Equivalent Weights for the Metric System 1000 mL = 1 Liter
1000 mU = 1 Unit
1 liter of water = 1 kg
Ratio Solutions (Express the number of grams of the drug per total ml of solution) 50% 50 g/100 mL
10% 10 g/100 mL
1:1000 1 g/1000 mL
Temperature Conversions Celsius = (F-32o) X 5/9 Fahrenheit = (9/5 X C) + 32o

129
MATHEMATICAL PROBLEM SOLVING
Dimensional Analysis/Unit Method
Dimensional analysis or the unit method is a method of solving mathematical problems that has been used by engineers, physicists, and chemists for many years. It has, however, only recently been applied to mathematical problem solving in nursing. It is a method that involves no memorization of formulas, no understanding of ratio and proportion, and no algebra. What the unit method does involve is an open mind and a willingness to give up traditional methods of problem solving that have been used in nursing for years. This method can be used for determining IV rates, doing conversions, calculating dosages ... almost any mathematical problem you will encounter in nursing. As with any method of mathematical problem solving, a basic understanding of the units of measurement for the apothecary, a metric and household system is necessary. When you have acquired this basic knowledge, you can then use the four steps in the method as presented in this program to solve any and almost all of your mathematical problems. DEFINITION OF TERMS Unit A unit is a word that represents a standardized quantity. For example, a minute is a unit of time. A gram is a unit of weight. EXAMPLE #1
How many pounds of sugar can you buy for 2 dollars if sugar is 79 cents for 1 pound?
The units are: (1) dollars (2) cents (3) pounds EXAMPLE #2
Give 1000 mg of Gantrisin. You have tablets of 500 mg each.
The units are: (1) mg (2) tablet (3) mg EXAMPLE #3
You are to give 1000 mL 5% D/W in 8 hours. The drip factor is 15 gtts per mL. At how many drops per minute will you infuse the IV?
The units are: (1) mL (2) hours (3) gtts (4) mL

130
Factor A factor is a single, given item in a problem. Each factor consists of a number and a unit.
EXAMPLE #1: How many pounds of sugar can you buy for 2 dollars if sugar is 79 cents for 1 pound?
The factors in this problem are:
1. 2 dollars
2. 79 cents
3. 1 pound (of sugar)
EXAMPLE #2: Give 1000 mg of Gantrisin. You have tablets of 500 mg each.
The factors here are:
1. 1000 mg
2. 1 tablet
3. 500 mg
EXAMPLE #3 You are to give 1000 mL 5% D/W in 8 hours. The drip factor is 15 gtts per mL.
At how many drops per minute will you infuse the IV?
The factors in this problem are:
1. 1000 mL
2. 8 hours
3. 15 gtts
4. 1 mL
Set
Two factors which are equivalent to each other make up a set. Problems are set up in the following way:
A C E
__ __ __ = Quantity Desired B D F
The boxes represent the individual factors in the problem. Each pair of factors, i.e., A is a set.
B
EACH FACTOR USED MUST INCLUDE ITS UNIT. THE FACTORS IN EACH SET MUST BE EQUAL.
HINT: The words “per” and “in” are verbal equal signs.
Let's identify the sets in the examples.
131
EXAMPLE #1, the sets are: (1) 1 pound
79 cents
It is helpful if you read the set as "A equals B" or "1 pound equals 79 cents".
There is also an implied set in the problem. This is 2 dollars equals 1 purchase. Most people using this method simply use the digit "1" in this set rather than using the implied unit. For clarity in this program I have put the implied unit in parentheses, but it is not necessary to do this in your problem.
(2) 2 dollars
1 (purchase) EXAMPLE #2, the sets are: (1) 500 mg
1 tablet (2) 1000 mg
1 (dose) EXAMPLE #3, the sets are: (1) 1000 mL
8 hours (2) 15 gtts
1 mL Using the dimensional analysis method, you may add to a problem any equivalent factors needed to solve a problem. You could, for example, use the following sets:
1 grain 60 mg
1 hour 60 minutes
1 pound 16 ounces

132
These sets could also be reversed and they would still be equivalent or equal:
60 mg 1 grain
60 minutes 1 hour
16 ounces 1 pound
Equivalent factors can be added to a problem because they do not change the value of the answer. Multiplying a number by 1 does not change the number.
6/10 x 1/2 = 6/20
6/10 x 1/2 x 1/1 = 6/20
6/10 x 1/2 x 3/3 = 18/60 or 6/20
In each of the above problems, adding a fraction equal to 1 did not change the answer.
SOLVING PROBLEMS STEP ONE
In space A start with a factor that has the unit that you need for your answer.
Problem You have an order for Drug X gr 1. You have on hand Drug X 30 mg per tablet. How many tablets will you give? The factors in the problem are: (1) 1 gr.
(2) 30 mg
(3) 1 tablet
The answer will be a number of tablets. Therefore, in space A we want the unit tablets. From
the problem we take the factor "1" tablet.
1 tablet = To complete this set an equivalent for 1 tablet must be used. We are given the information in the problem that 30 mg (Drug X) equals 1 tablet. We now have: 1 tablet = 30 mg
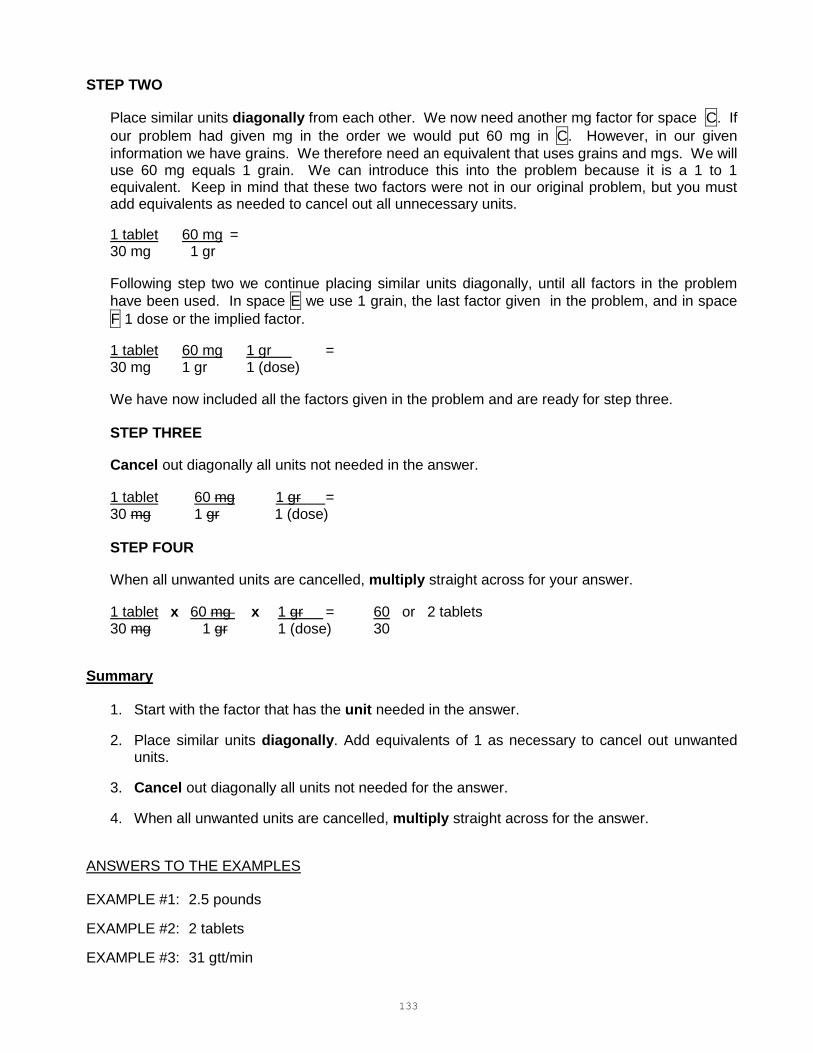
133
STEP TWO
Place similar units diagonally from each other. We now need another mg factor for space C. If
our problem had given mg in the order we would put 60 mg in C. However, in our given
information we have grains. We therefore need an equivalent that uses grains and mgs. We will use 60 mg equals 1 grain. We can introduce this into the problem because it is a 1 to 1 equivalent. Keep in mind that these two factors were not in our original problem, but you must add equivalents as needed to cancel out all unnecessary units.
1 tablet 60 mg = 30 mg 1 gr
Following step two we continue placing similar units diagonally, until all factors in the problem
have been used. In space E we use 1 grain, the last factor given in the problem, and in space
F 1 dose or the implied factor.
1 tablet 60 mg 1 gr = 30 mg 1 gr 1 (dose)
We have now included all the factors given in the problem and are ready for step three.
STEP THREE
Cancel out diagonally all units not needed in the answer.
1 tablet 60 mg 1 gr = 30 mg 1 gr 1 (dose) STEP FOUR
When all unwanted units are cancelled, multiply straight across for your answer.
1 tablet x 60 mg x 1 gr = 60 or 2 tablets 30 mg 1 gr 1 (dose) 30
Summary
1. Start with the factor that has the unit needed in the answer.
2. Place similar units diagonally. Add equivalents of 1 as necessary to cancel out unwanted units.
3. Cancel out diagonally all units not needed for the answer.
4. When all unwanted units are cancelled, multiply straight across for the answer.
ANSWERS TO THE EXAMPLES EXAMPLE #1: 2.5 pounds
EXAMPLE #2: 2 tablets
EXAMPLE #3: 31 gtt/min

134
SAMPLE PROBLEMS
1. Give Drug X 100 mg. You have Drug X 50 mg per mL vials. How many mLs will you give?
STEP ONE - You need to know how many mLs to give, start with the mL factor and its equivalent.
1 mL 50 mg
STEP TWO - Place similar factors diagonally.
1 mL x 100 mg 50 mg 1 (dose)
All factors have been used.
STEP THREE - Cancel all unwanted units.
1 mL x 100 mg = 50 mg 1 (dose)
Looking only at the units remaining we have "mL" per "dose".
STEP FOUR - Multiply straight across.
1 mL x 100 mg = 100 or 2 mL 50 mg 1 (dose) 50
2. Give Drug X 1/200 gr. You have a vial marked Drug X 1 mL = 0.4 mg. How many mLs will
you give?
STEP ONE
1 mL 0.4 mg
STEP TWO 1 mL x 60 mg x 1/200 gr = 0.4 mg 1 gr 1 (dose)
The 60 mg equals 1 gr. Equivalency was added to allow us to cancel out the mg and the gr units.
STEP THREE
1 mL x 60 mg x 1/200 gr = 0.4 mg 1 gr 1 (dose)
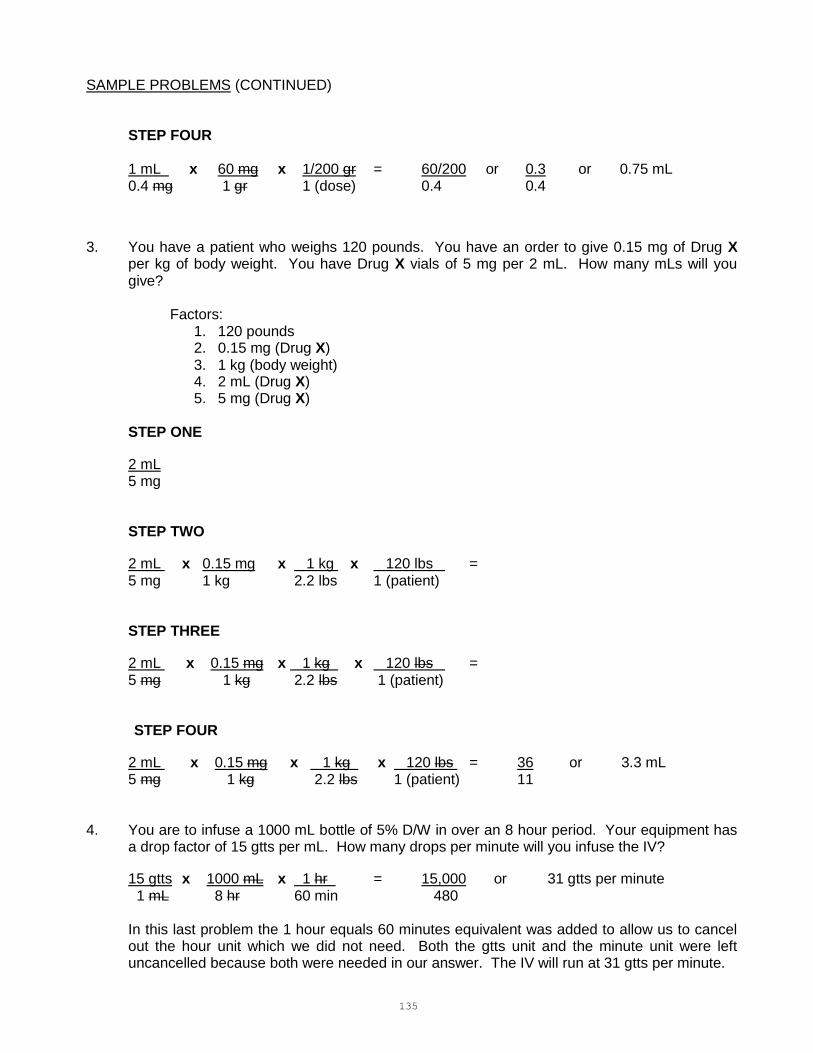
135
SAMPLE PROBLEMS (CONTINUED) STEP FOUR
1 mL x 60 mg x 1/200 gr = 60/200 or 0.3 or 0.75 mL 0.4 mg 1 gr 1 (dose) 0.4 0.4
3. You have a patient who weighs 120 pounds. You have an order to give 0.15 mg of Drug X per kg of body weight. You have Drug X vials of 5 mg per 2 mL. How many mLs will you give?
Factors:
1. 120 pounds 2. 0.15 mg (Drug X) 3. 1 kg (body weight) 4. 2 mL (Drug X) 5. 5 mg (Drug X)
STEP ONE
2 mL 5 mg
STEP TWO
2 mL x 0.15 mg x 1 kg x 120 lbs = 5 mg 1 kg 2.2 lbs 1 (patient)
STEP THREE
2 mL x 0.15 mg x 1 kg x 120 lbs = 5 mg 1 kg 2.2 lbs 1 (patient)
STEP FOUR
2 mL x 0.15 mg x 1 kg x 120 lbs = 36 or 3.3 mL 5 mg 1 kg 2.2 lbs 1 (patient) 11
4. You are to infuse a 1000 mL bottle of 5% D/W in over an 8 hour period. Your equipment has
a drop factor of 15 gtts per mL. How many drops per minute will you infuse the IV?
15 gtts x 1000 mL x 1 hr = 15,000 or 31 gtts per minute 1 mL 8 hr 60 min 480
In this last problem the 1 hour equals 60 minutes equivalent was added to allow us to cancel out the hour unit which we did not need. Both the gtts unit and the minute unit were left uncancelled because both were needed in our answer. The IV will run at 31 gtts per minute.

136
PHARMACOLOGY WORK PROBLEMS
CONVERSIONS
1. 110 lb = ________ kg
2. 60 mL = ________ oz
3. 1 pt = ________ mL
4. 30 mg = ________ gr
5. 1 g = ________ gr
6. 2 qt = ________ mL
7. 3.5 g = ________ mg
8. 15 kg = ________ g
9. 33 mg = ________ g
10. 1000 mL = ________ L
11. 1 oz= ________ g
12. 60 mg = __________ gr
13. 1mg = __________ mcg
14. 1g = __________ mg
15. 8 oz = __________glassful(s)
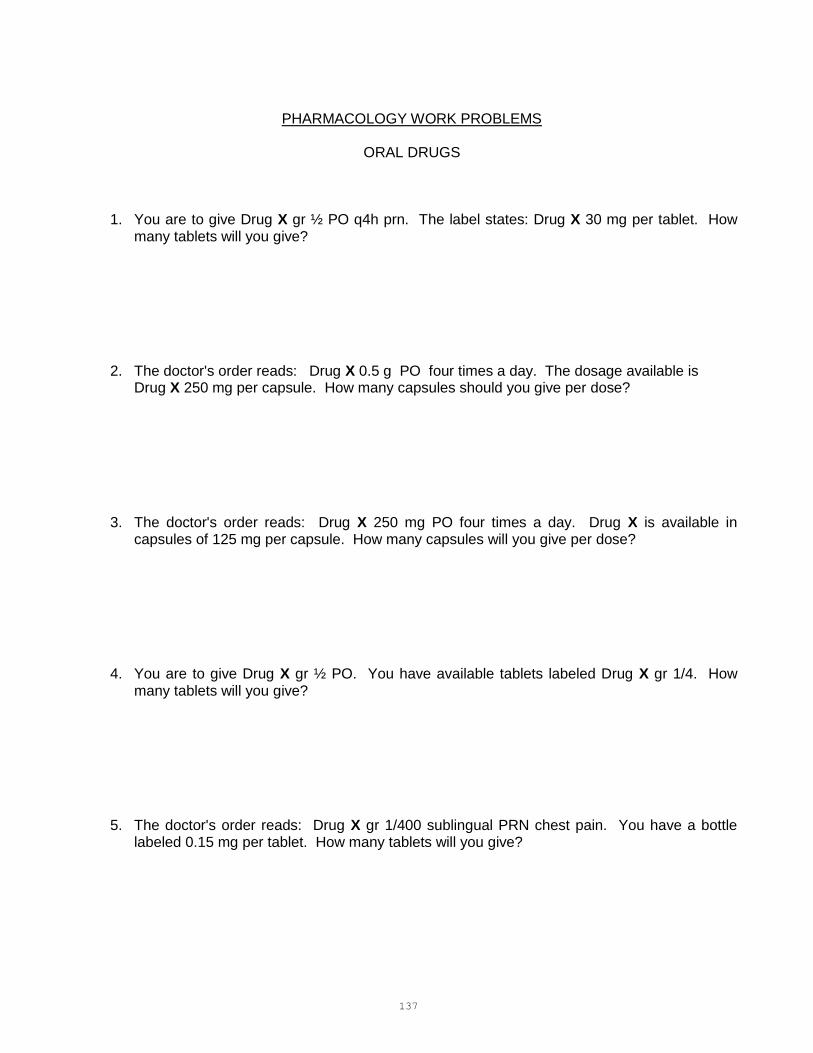
137
PHARMACOLOGY WORK PROBLEMS
ORAL DRUGS
1. You are to give Drug X gr ½ PO q4h prn. The label states: Drug X 30 mg per tablet. How many tablets will you give?
2. The doctor's order reads: Drug X 0.5 g PO four times a day. The dosage available is Drug X 250 mg per capsule. How many capsules should you give per dose?
3. The doctor's order reads: Drug X 250 mg PO four times a day. Drug X is available in capsules of 125 mg per capsule. How many capsules will you give per dose?
4. You are to give Drug X gr ½ PO. You have available tablets labeled Drug X gr 1/4. How many tablets will you give?
5. The doctor's order reads: Drug X gr 1/400 sublingual PRN chest pain. You have a bottle labeled 0.15 mg per tablet. How many tablets will you give?

138
PHARMACOLOGY WORK PROBLEMS – ORAL (CONTINUED)
6. The doctor's order reads: Drug X 12.5 mg PO. You have Drug X 25 mg per tablet. How many tablets will you give?
7. You have an order for Drug X 625 mcg PO. Tablets are labeled 0.625 mg. How many
tablets will you give? 8. The order is Drug X 3.75 mg PO. Drug X 2.5 mg tablets are available. How many tablets
will you give? 9. The order is for Drug X 0.125 mg PO. The bottle is labeled Drug X 0.25 mg. How many
tablets will you give? 10. You are to give Drug X 0.05 mg PO. The bottle is labeled Drug X 50 mcg. How many
tablets will you give? 11. The doctor's order reads Drug X gr 1/6 PO. You have Drug X 10 mg tablets. How many
tablets will you give?

139
PHARMACOLOGY WORK PROBLEMS – ORAL (CONTINUED)
12. You have an order for Drug X 0.06 g per kg of body weight per day to be divided into four equal doses. Drug X is available in tablets of 0.5 g. Your patient weighs 145 pounds. How many tablets will you give for one dose?
13. The doctor's order reads Drug X 40 mEq PO. The label reads Drug X oral solution 20 mEq
in 15 mL. How many mL will you give? 14. You are to give Drug X 10 mg PO tid. You have Drug X elixir 20 mg per 5 mL. How many
mL will you give for one dose? 15. Give Drug X oral suspension 0.2 g PO. The bottle is labeled 400 mg per 5 mL. How many
mL will you give?
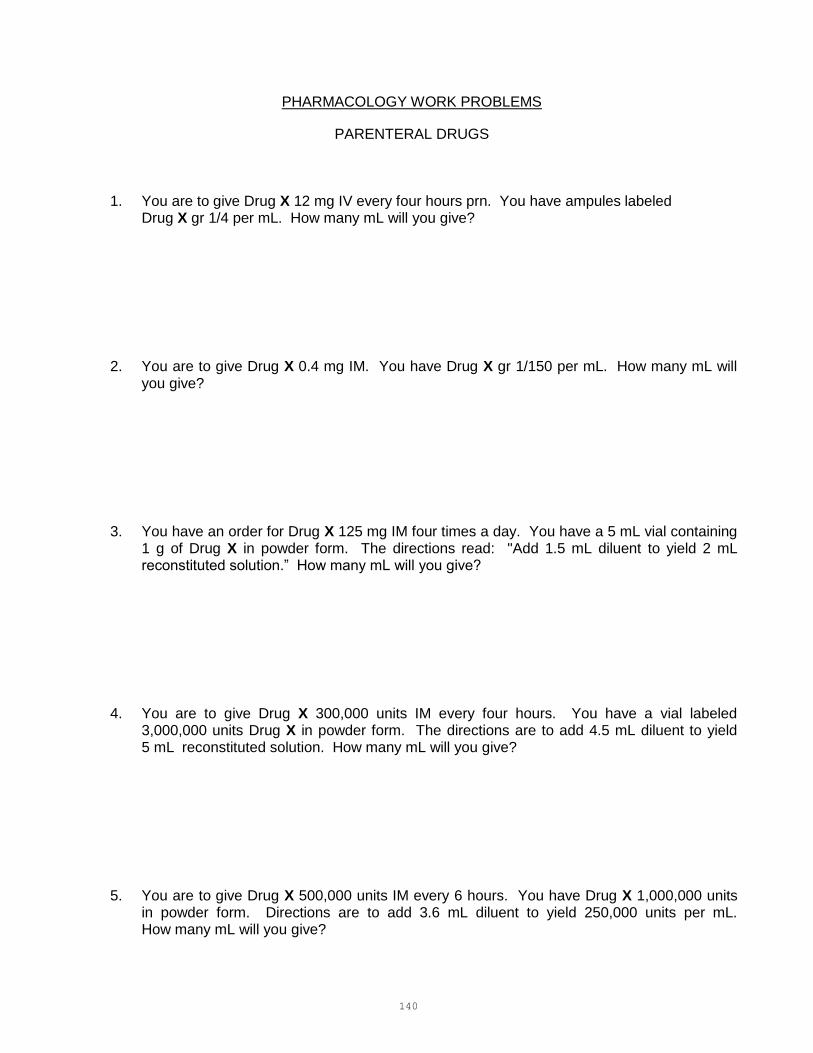
140
PHARMACOLOGY WORK PROBLEMS
PARENTERAL DRUGS
1. You are to give Drug X 12 mg IV every four hours prn. You have ampules labeled
Drug X gr 1/4 per mL. How many mL will you give?
2. You are to give Drug X 0.4 mg IM. You have Drug X gr 1/150 per mL. How many mL will you give?
3. You have an order for Drug X 125 mg IM four times a day. You have a 5 mL vial containing 1 g of Drug X in powder form. The directions read: "Add 1.5 mL diluent to yield 2 mL reconstituted solution.” How many mL will you give?
4. You are to give Drug X 300,000 units IM every four hours. You have a vial labeled 3,000,000 units Drug X in powder form. The directions are to add 4.5 mL diluent to yield 5 mL reconstituted solution. How many mL will you give?
5. You are to give Drug X 500,000 units IM every 6 hours. You have Drug X 1,000,000 units in powder form. Directions are to add 3.6 mL diluent to yield 250,000 units per mL. How many mL will you give?
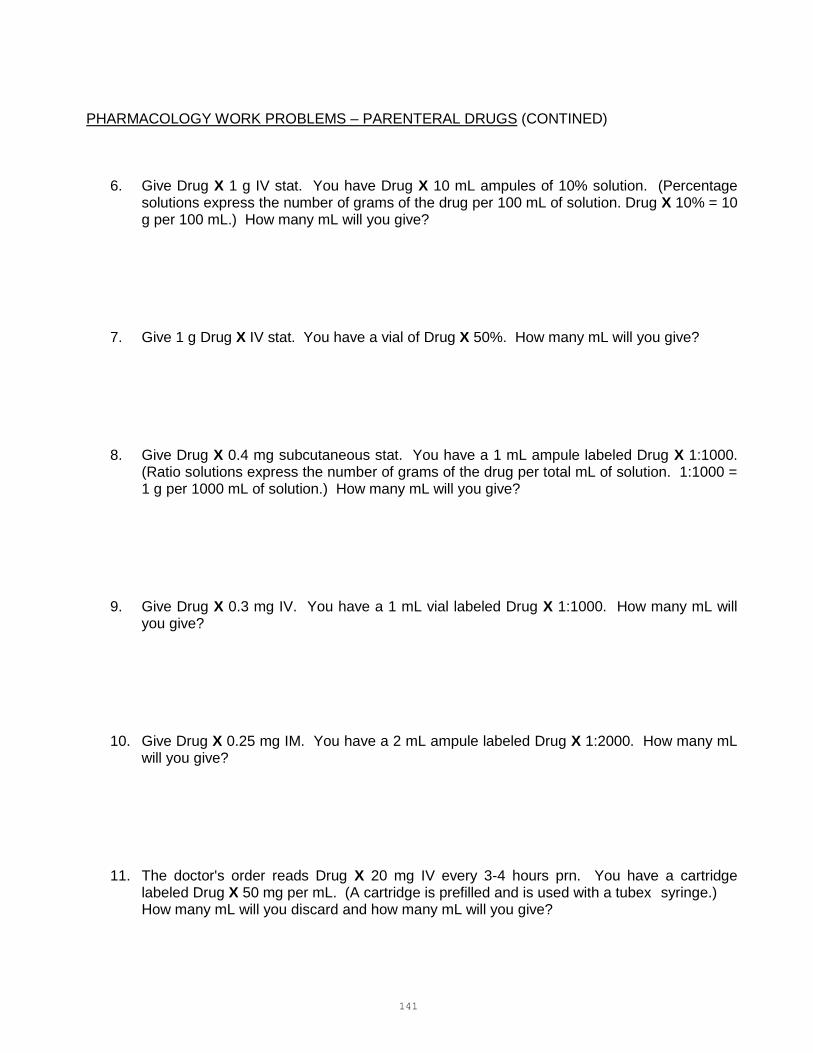
141
PHARMACOLOGY WORK PROBLEMS – PARENTERAL DRUGS (CONTINED)
6. Give Drug X 1 g IV stat. You have Drug X 10 mL ampules of 10% solution. (Percentage solutions express the number of grams of the drug per 100 mL of solution. Drug X 10% = 10 g per 100 mL.) How many mL will you give?
7. Give 1 g Drug X IV stat. You have a vial of Drug X 50%. How many mL will you give?
8. Give Drug X 0.4 mg subcutaneous stat. You have a 1 mL ampule labeled Drug X 1:1000. (Ratio solutions express the number of grams of the drug per total mL of solution. 1:1000 = 1 g per 1000 mL of solution.) How many mL will you give?
9. Give Drug X 0.3 mg IV. You have a 1 mL vial labeled Drug X 1:1000. How many mL will you give?
10. Give Drug X 0.25 mg IM. You have a 2 mL ampule labeled Drug X 1:2000. How many mL will you give?
11. The doctor's order reads Drug X 20 mg IV every 3-4 hours prn. You have a cartridge labeled Drug X 50 mg per mL. (A cartridge is prefilled and is used with a tubex syringe.) How many mL will you discard and how many mL will you give?

142
PHARMACOLOGY WORK PROBLEMS – PARENTERAL DRUGS (CONTINED)
12. Give Drug X 6,000,000 units IM bid. You have available a 10 mL vial labeled Drug X 5,000,000 units per mL. How many mL will you give?
13. You are to give Drug X 0.15 mg subcutaneous to a child. You have a 20 mL vial labeled Drug X 0.4 mg per mL. How many mL will you give? 14. Give Drug X gr ¼ IM. You have a vial labeled Drug X 15 mg per mL. How many mL will
you give? 15. Give Drug X gr 1/6 IM. You have a vial labeled Drug X gr 1/4 per mL. How many mL will
you give?
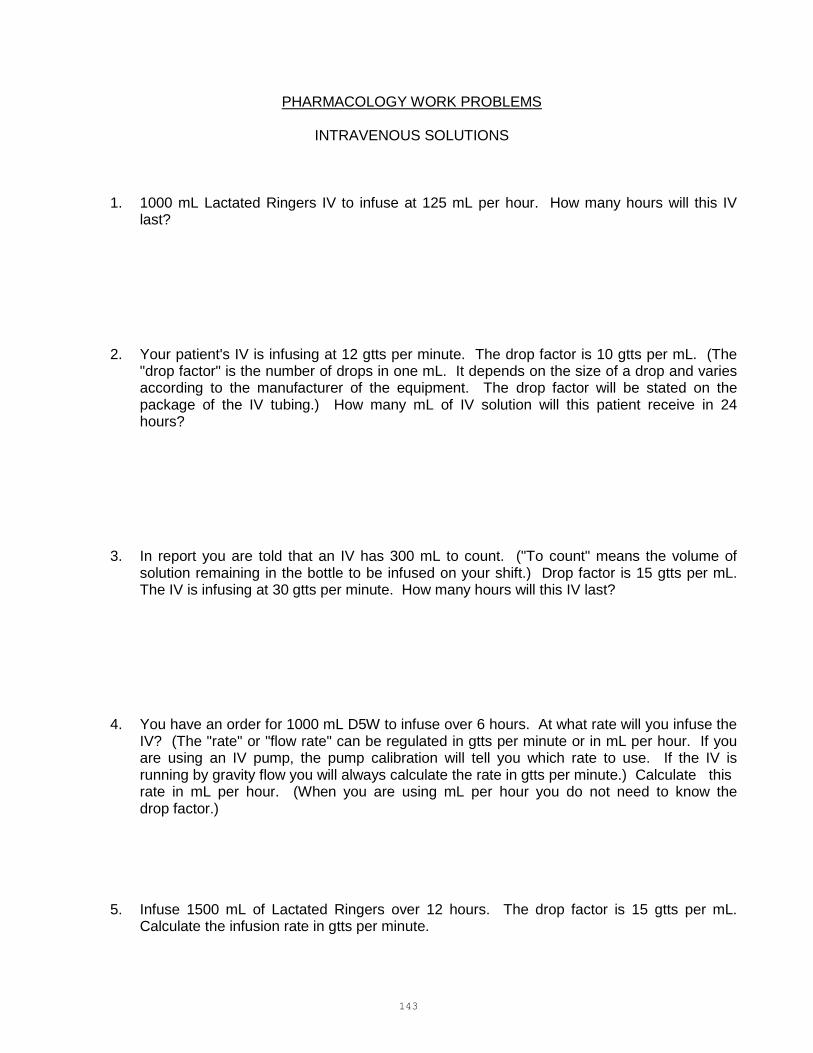
143
PHARMACOLOGY WORK PROBLEMS
INTRAVENOUS SOLUTIONS
1. 1000 mL Lactated Ringers IV to infuse at 125 mL per hour. How many hours will this IV last?
2. Your patient's IV is infusing at 12 gtts per minute. The drop factor is 10 gtts per mL. (The "drop factor" is the number of drops in one mL. It depends on the size of a drop and varies according to the manufacturer of the equipment. The drop factor will be stated on the package of the IV tubing.) How many mL of IV solution will this patient receive in 24 hours?
3. In report you are told that an IV has 300 mL to count. ("To count" means the volume of solution remaining in the bottle to be infused on your shift.) Drop factor is 15 gtts per mL. The IV is infusing at 30 gtts per minute. How many hours will this IV last?
4. You have an order for 1000 mL D5W to infuse over 6 hours. At what rate will you infuse the IV? (The "rate" or "flow rate" can be regulated in gtts per minute or in mL per hour. If you are using an IV pump, the pump calibration will tell you which rate to use. If the IV is running by gravity flow you will always calculate the rate in gtts per minute.) Calculate this rate in mL per hour. (When you are using mL per hour you do not need to know the drop factor.)
5. Infuse 1500 mL of Lactated Ringers over 12 hours. The drop factor is 15 gtts per mL. Calculate the infusion rate in gtts per minute.
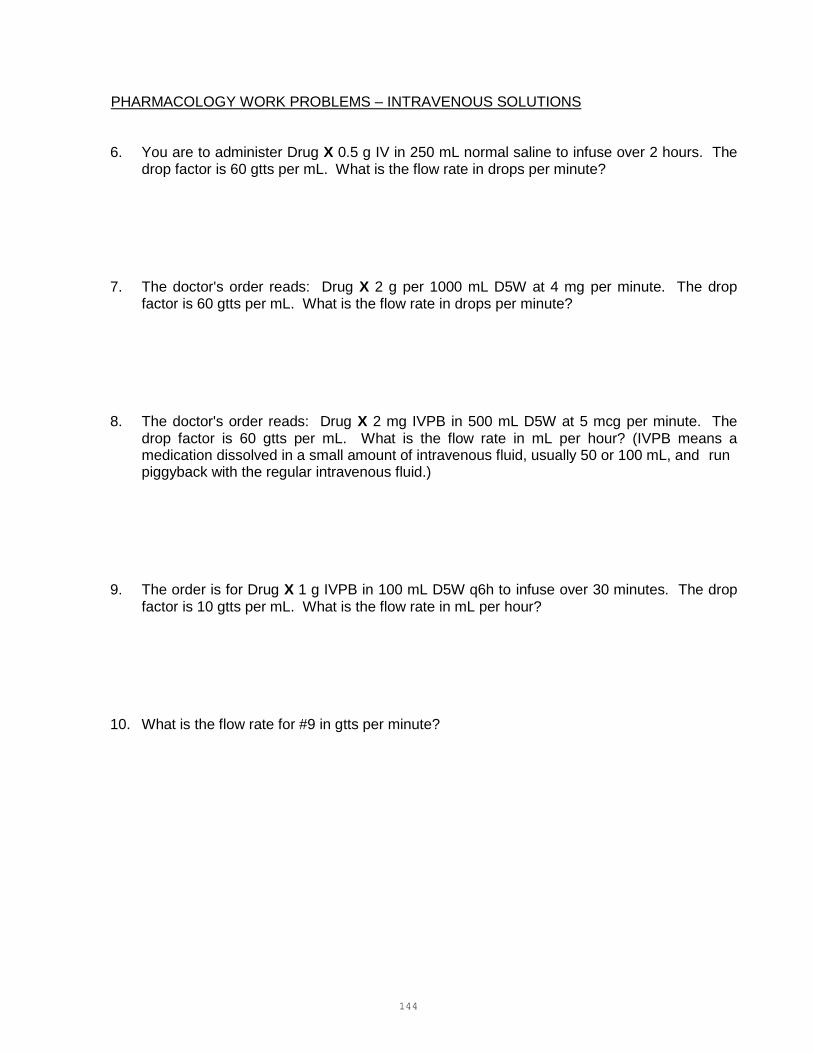
144
PHARMACOLOGY WORK PROBLEMS – INTRAVENOUS SOLUTIONS
6. You are to administer Drug X 0.5 g IV in 250 mL normal saline to infuse over 2 hours. The drop factor is 60 gtts per mL. What is the flow rate in drops per minute?
7. The doctor's order reads: Drug X 2 g per 1000 mL D5W at 4 mg per minute. The drop factor is 60 gtts per mL. What is the flow rate in drops per minute?
8. The doctor's order reads: Drug X 2 mg IVPB in 500 mL D5W at 5 mcg per minute. The drop factor is 60 gtts per mL. What is the flow rate in mL per hour? (IVPB means a medication dissolved in a small amount of intravenous fluid, usually 50 or 100 mL, and run piggyback with the regular intravenous fluid.)
9. The order is for Drug X 1 g IVPB in 100 mL D5W q6h to infuse over 30 minutes. The drop factor is 10 gtts per mL. What is the flow rate in mL per hour?
10. What is the flow rate for #9 in gtts per minute?
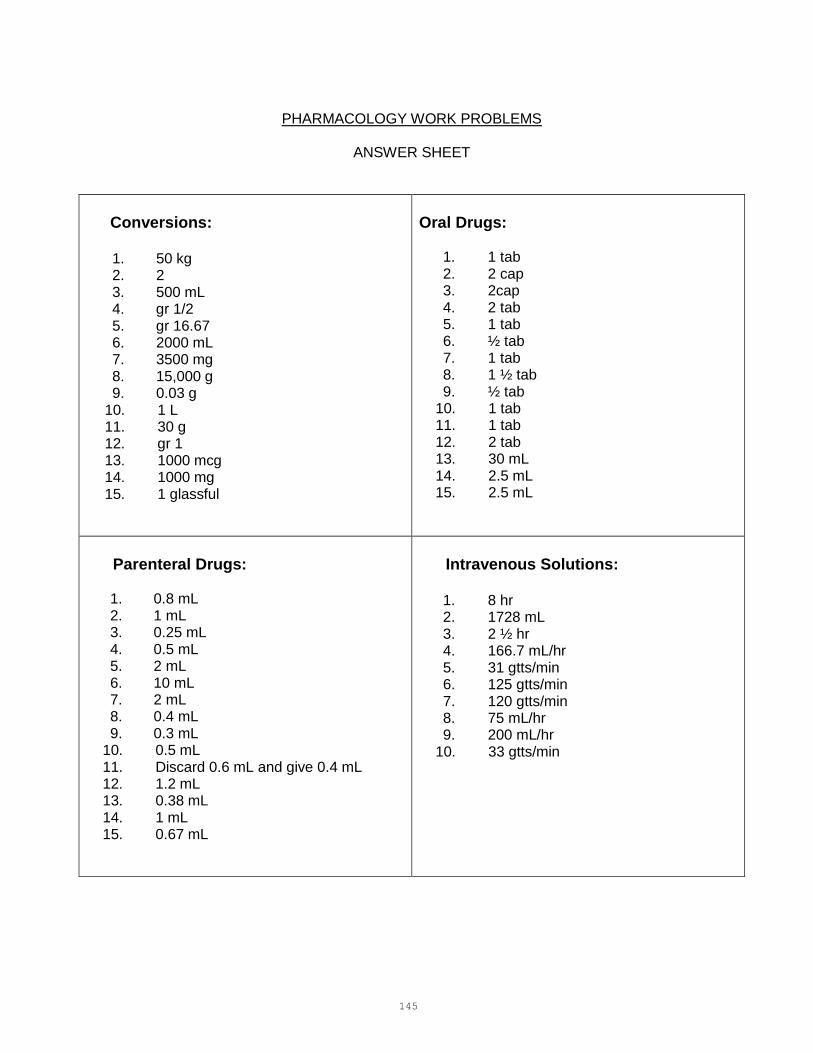
145
PHARMACOLOGY WORK PROBLEMS
ANSWER SHEET
Conversions: 1. 50 kg 2. 2 3. 500 mL 4. gr 1/2 5. gr 16.67 6. 2000 mL 7. 3500 mg 8. 15,000 g 9. 0.03 g
10. 1 L 11. 30 g 12. gr 1 13. 1000 mcg 14. 1000 mg 15. 1 glassful
Oral Drugs:
1. 1 tab 2. 2 cap 3. 2cap 4. 2 tab 5. 1 tab 6. ½ tab 7. 1 tab 8. 1 ½ tab 9. ½ tab
10. 1 tab 11. 1 tab 12. 2 tab 13. 30 mL 14. 2.5 mL 15. 2.5 mL
Parenteral Drugs:
1. 0.8 mL 2. 1 mL 3. 0.25 mL 4. 0.5 mL 5. 2 mL 6. 10 mL 7. 2 mL 8. 0.4 mL 9. 0.3 mL
10. 0.5 mL 11. Discard 0.6 mL and give 0.4 mL 12. 1.2 mL 13. 0.38 mL 14. 1 mL 15. 0.67 mL
Intravenous Solutions:
1. 8 hr 2. 1728 mL 3. 2 ½ hr 4. 166.7 mL/hr 5. 31 gtts/min 6. 125 gtts/min 7. 120 gtts/min 8. 75 mL/hr 9. 200 mL/hr
10. 33 gtts/min
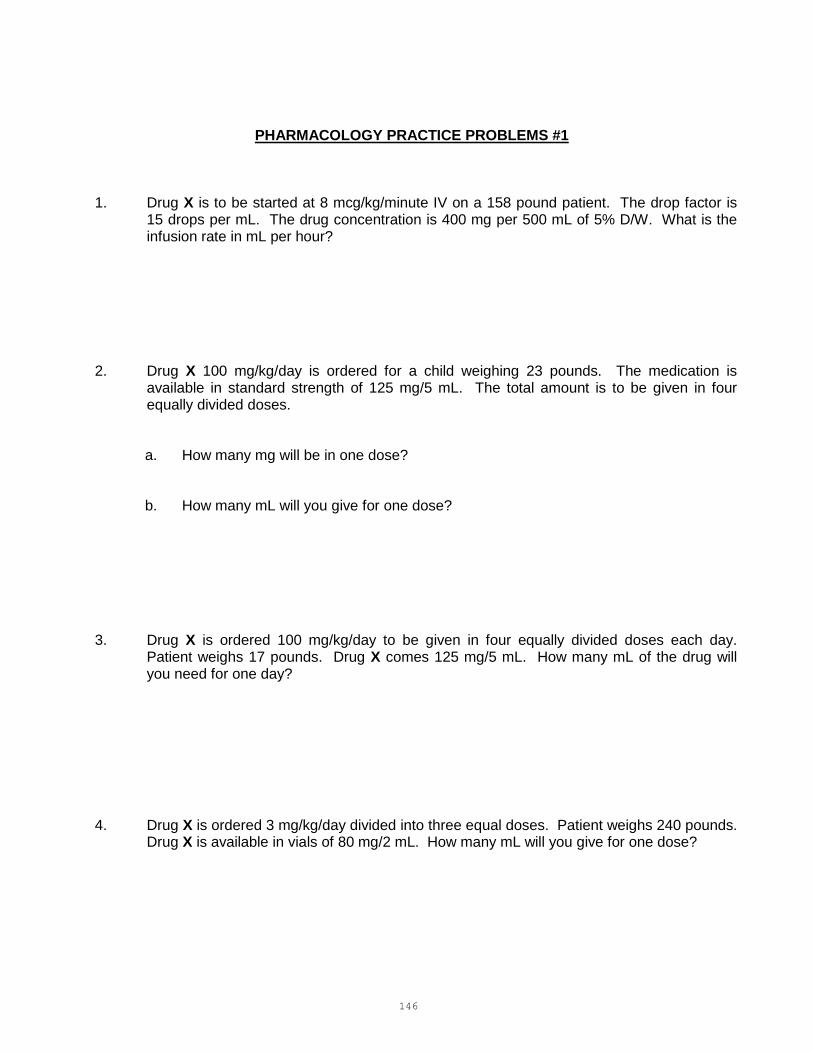
146
PHARMACOLOGY PRACTICE PROBLEMS #1
1. Drug X is to be started at 8 mcg/kg/minute IV on a 158 pound patient. The drop factor is 15 drops per mL. The drug concentration is 400 mg per 500 mL of 5% D/W. What is the infusion rate in mL per hour?
2. Drug X 100 mg/kg/day is ordered for a child weighing 23 pounds. The medication is
available in standard strength of 125 mg/5 mL. The total amount is to be given in four equally divided doses.
a. How many mg will be in one dose? b. How many mL will you give for one dose? 3. Drug X is ordered 100 mg/kg/day to be given in four equally divided doses each day.
Patient weighs 17 pounds. Drug X comes 125 mg/5 mL. How many mL of the drug will you need for one day?
4. Drug X is ordered 3 mg/kg/day divided into three equal doses. Patient weighs 240 pounds.
Drug X is available in vials of 80 mg/2 mL. How many mL will you give for one dose?

147
PHARMACOLOGY PRACTICE PROBLEMS #1 (CONTINUED)
5. You are to give Drug X 25,000 units/kg/24 hours in six equally divided doses. The medication comes in powder form 1,000,000 units per vial. When dissolved in 9.6 mL of diluent, the concentration is 100,000 units/mL. Patient weighs 100 pounds. How many mL will you give for one dose?
6. You are to add 5 mL diluent to a 2 g vial of Drug X. The final concentration will be 330 mg
per mL. How many mLs will you administer when the order is for 500 mg per dose? 7. You are to give Drug X in liquid form. The ordered first dose is 100 mg/kg to be followed
by 50 mg/kg/day in three equally divided doses. Drug X comes 250 mg/5 mL. Patient weighs 38 pounds.
a. How many mL will you give for the first dose?
b. How many mL in each following dose? 8. Drug X is to be started at 3 mcg/kg/minute. Drop factor is 60 gtts/mL. Patient weighs
234 pounds. Concentration of drug is 500 mg per 1000 mL.
a. At what rate in mL/hour will you infuse the IV? b. How many mg of the drug will the patient receive in one hour?
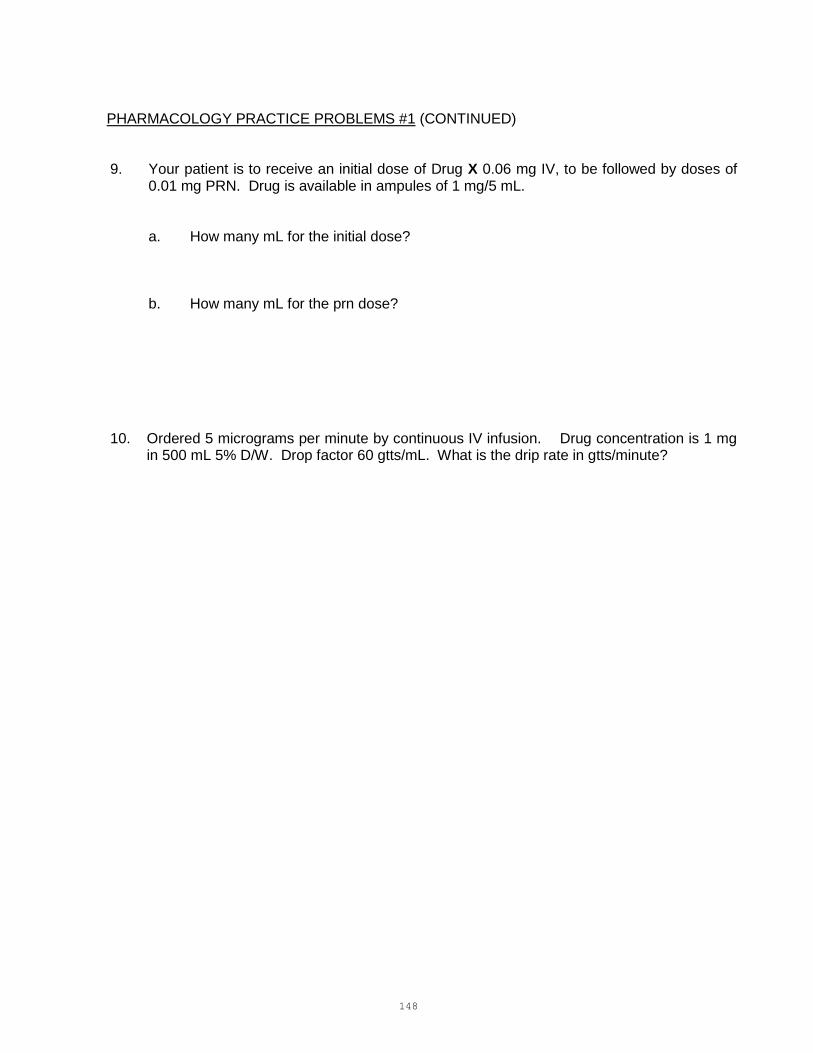
148
PHARMACOLOGY PRACTICE PROBLEMS #1 (CONTINUED)
9. Your patient is to receive an initial dose of Drug X 0.06 mg IV, to be followed by doses of 0.01 mg PRN. Drug is available in ampules of 1 mg/5 mL.
a. How many mL for the initial dose? b. How many mL for the prn dose?
10. Ordered 5 micrograms per minute by continuous IV infusion. Drug concentration is 1 mg in 500 mL 5% D/W. Drop factor 60 gtts/mL. What is the drip rate in gtts/minute?

149
PHARMACOLOGY PRACTICE PROBLEMS #1
ANSWERS
1. 43.1 mL/hour 2. a. 261.36 mg b. 10.5 mL 3. 30.9 mL 4. 2.7 mL 5. 1.9 mL 6. 1.5 mL 7. a. 34.5 mL b. 5.8 mL 8. a. 38.3 mL/hour b. 19.15 mg in 1 hour 9. a. 0.3 mL b. 0.05 mL 10. 150 gtts/minute
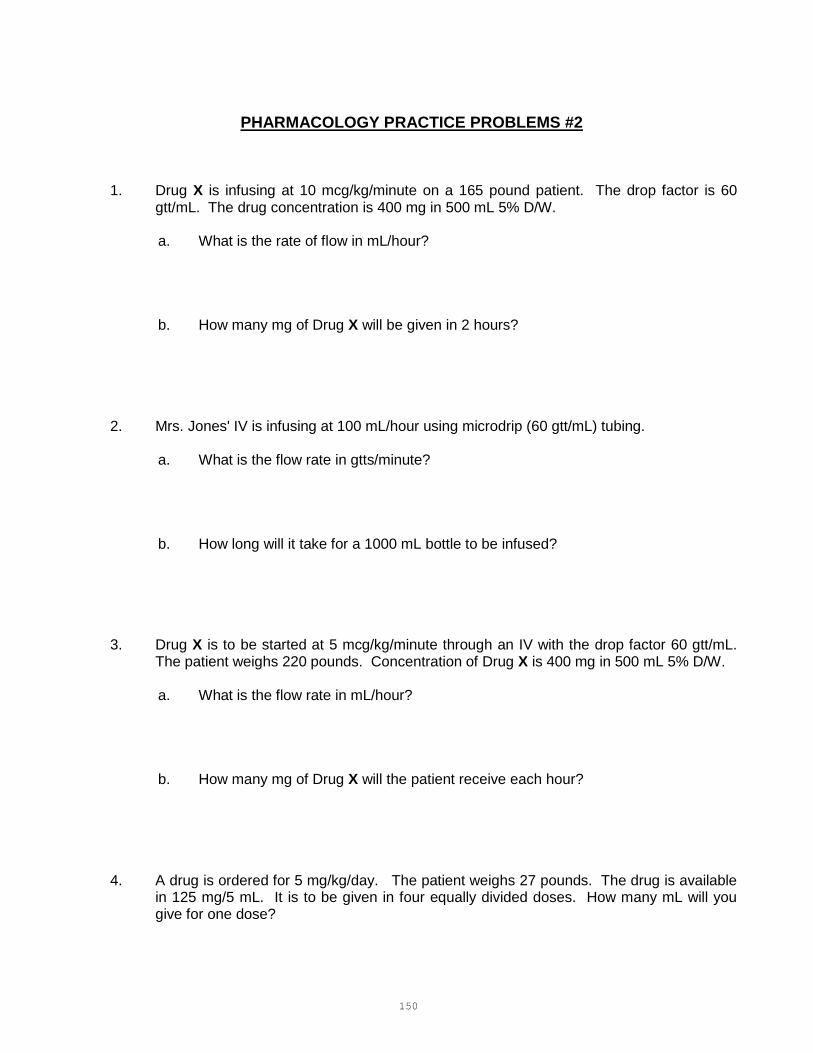
150
PHARMACOLOGY PRACTICE PROBLEMS #2
1. Drug X is infusing at 10 mcg/kg/minute on a 165 pound patient. The drop factor is 60 gtt/mL. The drug concentration is 400 mg in 500 mL 5% D/W.
a. What is the rate of flow in mL/hour?
b. How many mg of Drug X will be given in 2 hours?
2. Mrs. Jones' IV is infusing at 100 mL/hour using microdrip (60 gtt/mL) tubing.
a. What is the flow rate in gtts/minute?
b. How long will it take for a 1000 mL bottle to be infused?
3. Drug X is to be started at 5 mcg/kg/minute through an IV with the drop factor 60 gtt/mL. The patient weighs 220 pounds. Concentration of Drug X is 400 mg in 500 mL 5% D/W.
a. What is the flow rate in mL/hour?
b. How many mg of Drug X will the patient receive each hour?
4. A drug is ordered for 5 mg/kg/day. The patient weighs 27 pounds. The drug is available in 125 mg/5 mL. It is to be given in four equally divided doses. How many mL will you give for one dose?
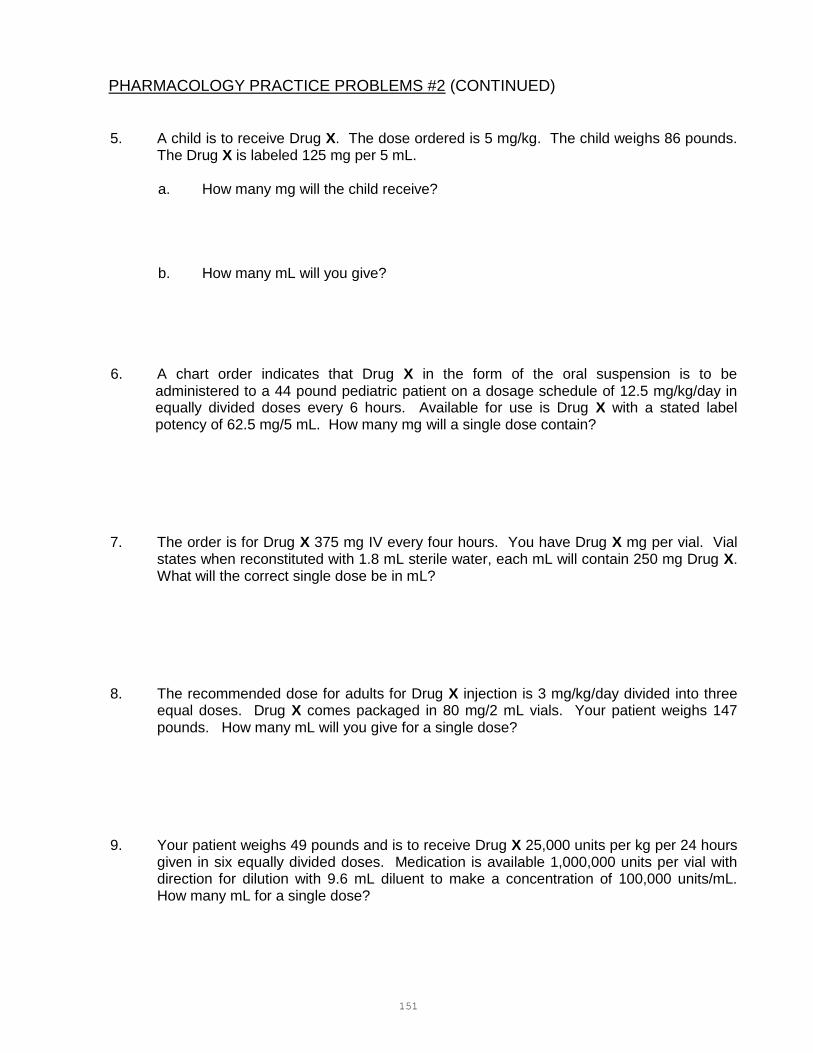
151
PHARMACOLOGY PRACTICE PROBLEMS #2 (CONTINUED)
5. A child is to receive Drug X. The dose ordered is 5 mg/kg. The child weighs 86 pounds. The Drug X is labeled 125 mg per 5 mL.
a. How many mg will the child receive?
b. How many mL will you give?
6. A chart order indicates that Drug X in the form of the oral suspension is to be administered to a 44 pound pediatric patient on a dosage schedule of 12.5 mg/kg/day in equally divided doses every 6 hours. Available for use is Drug X with a stated label potency of 62.5 mg/5 mL. How many mg will a single dose contain?
7. The order is for Drug X 375 mg IV every four hours. You have Drug X mg per vial. Vial states when reconstituted with 1.8 mL sterile water, each mL will contain 250 mg Drug X. What will the correct single dose be in mL?
8. The recommended dose for adults for Drug X injection is 3 mg/kg/day divided into three equal doses. Drug X comes packaged in 80 mg/2 mL vials. Your patient weighs 147 pounds. How many mL will you give for a single dose?
9. Your patient weighs 49 pounds and is to receive Drug X 25,000 units per kg per 24 hours given in six equally divided doses. Medication is available 1,000,000 units per vial with direction for dilution with 9.6 mL diluent to make a concentration of 100,000 units/mL. How many mL for a single dose?

152
PHARMACOLOGY PRACTICE PROBLEMS #2 (CONTINUED)
10. The recommended dosage for Drug X liquid for children weighing 20 kg or less is 100 mg/kg/day to be given in four equally divided doses. Your patient weighs 17 pounds. The medication comes in standard strength of 125 mg/5 mL.
a. How many mg will your patient receive in 24 hours?
b. How many mL per dose?
11. You are to give: Drug X 50 mg } Drug Y gr 1/150 } IM Drug Z 25 mg }
You have: Drug X 100 mg per 2 mL
Drug Y 0.4 mg per mL Drug Z 100 mg per 2 mL
What is the total amount in mL you will administer?
12. Your patient has an IV infusing at 25 gtt/minute. Drop factor is 10 gtt/mL. How many mL will your patient receive in 8 hours?
13. Drug X 1000 mg is added to a 500 mL of 5% Dextrose/Water. It is to be given IV at a rate of 20 mg/hour. The drop factor is 20 gtts/mL. How many mL/hour should the IV infuse?

153
PHARMACOLOGY PRACTICE PROBLEMS #2 (CONTINUED)
14. Administer Drug X 0.5 mcg/Kg/min IV for a hypertensive crisis. On hand is Drug X 50 mg in 500mL of normal saline. The patient weighs 140 lbs. Calculate the mL/hour rate for the infusion pump.
15. You have a multiple dose vial of Drug X labeled 5,000,000 units. The directions read "add
3.2 mL diluent to make 1,000,000 units per mL.” If the patient receives 1.7 mL of this solution, how many units will he receive?
16. Drug X is ordered at 5 mg/kg four times a day for an 86 pound patient. The medication
comes in a vial containing 75 mg/2 mL. a. How many mL per dose? b. How many mg per day? 17. Add 25,000 units of Drug X to 250 mL of D5W. Infuse at 1200 units/ hour. The drip factor
is 10 gtts/mL. Calculate the mL/hour rate for the infusion pump.

154
PHARMACOLOGY PRACTICE PROBLEMS #2 (CONTINUED)
18. Patient is to receive Drug X 4 mcg/kg/minute IVPB. Drop factor is 15 gtt/mL. Patient's weight is 375 pounds. Drug concentration is 500 mg/500 mL. What is the flow rate in mL/hour?
19. Patient is to receive IV Drug X 15,000 units/day. Vial is labeled 40,000 units per 2 mL. Drug X is to be added to a 500 mL bottle of 5% D/W for 24 hours.
a. How many mL of Drug X will you add?
b. What will the flow rate be in mL/hour?
20. You are to add 10 g of Drug X to 1000 mL of D5W. You have a 10 mL vial of 50% solutions of Drug X. How many mL will you add?
21. The patient is receiving TPN (40% Dextrose 500 mLs with 8.25% FreAmine 500 mLs) at 80 mLs per hour. The patient also receives 500 mLs 10% lipids daily. Approximately how many calories does the patient receive daily from these IV fluids?
22. The patient is receiving SPN (20% Dextrose 500 mLs with 5.25% Nephramine 500 mLs) at
75 mLs per hour. The patient also receives 250 mLs 20% lipids daily. Approximately how many calories does the patient receive daily from these IV fluids?

155
PHARMACOLOGY PRACTICE PROBLEMS #2
ANSWERS
1. a. 56.3 mL/hour b. 90.08 mg/dose (90 mg/dose if start with 10 mcg/kg/min)
2. a. 100 gtt/minute b. 10 hours
3. a. 37.5 mL/hour b. 30 mg/hour
4. 0.61 mL
5. a. 195.45 mg b. 7.8 mL
6. 62.5 mg
7. 1.5 mL
8. 1.7 mL
9. 0.93 mL
10. a. 772.73 mg b. 7.7 mL
11. 2.5 mL
12. 1200 mL
13. 10 mL/hour
14. 19.1 mL/hour
15. 1,700,000 units
16. a. 5.2 mL b. 781.82 mg/day
17. 12 mL/hour
18. 40.9 mL/hour
19. a. 0.75 mL b. 20.8 mL/hour
20. 20 mL
21. 2303 calories
22. 1359 calories
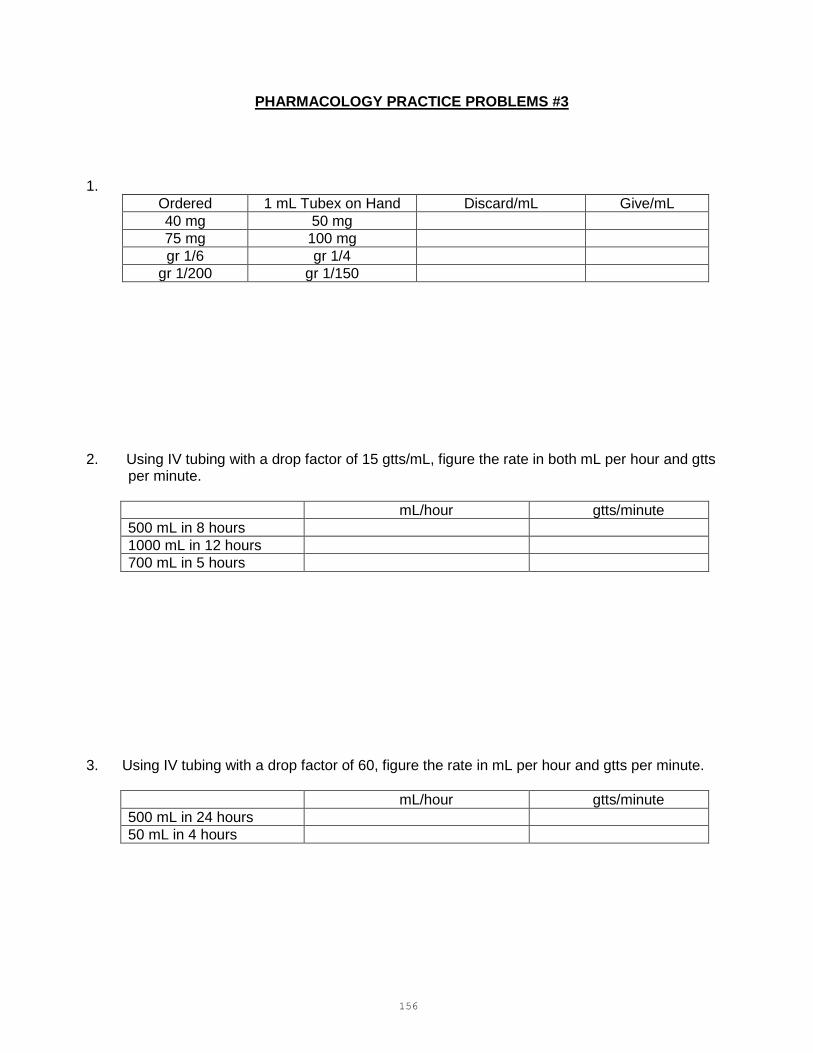
156
PHARMACOLOGY PRACTICE PROBLEMS #3
1.
Ordered 1 mL Tubex on Hand Discard/mL Give/mL
40 mg 50 mg
75 mg 100 mg
gr 1/6 gr 1/4
gr 1/200 gr 1/150
2. Using IV tubing with a drop factor of 15 gtts/mL, figure the rate in both mL per hour and gtts
per minute.
mL/hour gtts/minute
500 mL in 8 hours
1000 mL in 12 hours
700 mL in 5 hours
3. Using IV tubing with a drop factor of 60, figure the rate in mL per hour and gtts per minute.
mL/hour gtts/minute
500 mL in 24 hours
50 mL in 4 hours
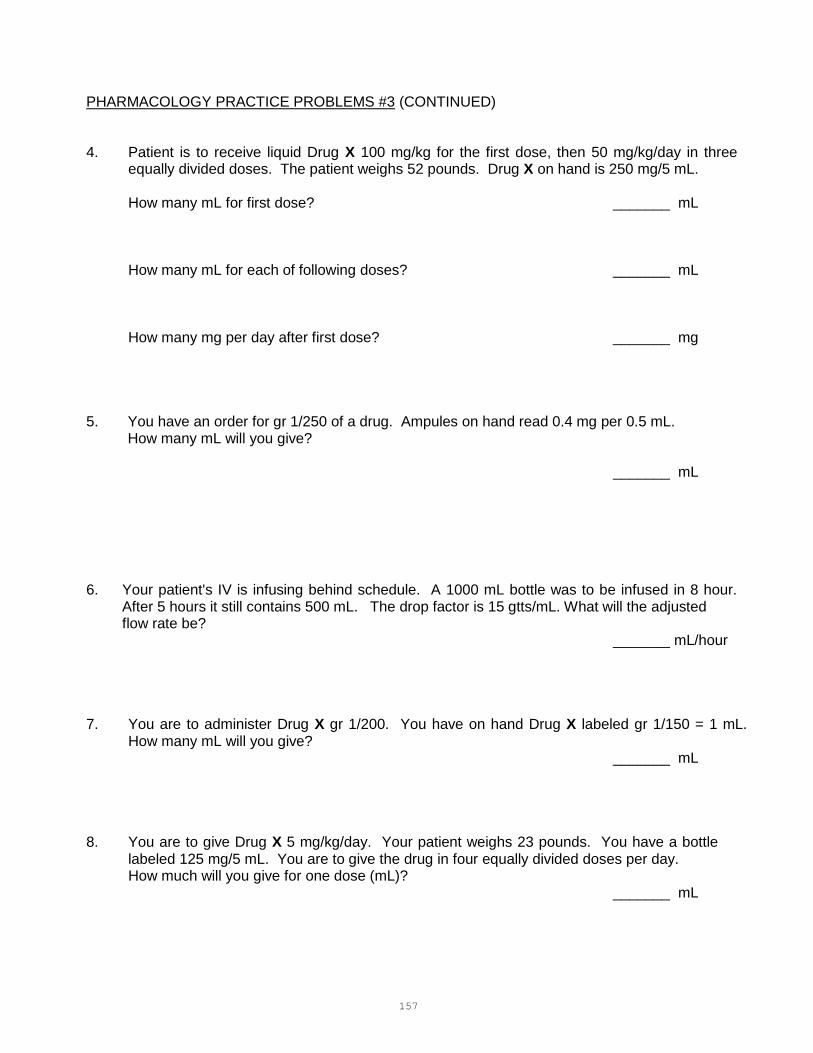
157
PHARMACOLOGY PRACTICE PROBLEMS #3 (CONTINUED) 4. Patient is to receive liquid Drug X 100 mg/kg for the first dose, then 50 mg/kg/day in three
equally divided doses. The patient weighs 52 pounds. Drug X on hand is 250 mg/5 mL.
How many mL for first dose? _______ mL
How many mL for each of following doses? _______ mL
How many mg per day after first dose? _______ mg 5. You have an order for gr 1/250 of a drug. Ampules on hand read 0.4 mg per 0.5 mL. How many mL will you give?
_______ mL
6. Your patient's IV is infusing behind schedule. A 1000 mL bottle was to be infused in 8 hour.
After 5 hours it still contains 500 mL. The drop factor is 15 gtts/mL. What will the adjusted flow rate be? _______ mL/hour
7. You are to administer Drug X gr 1/200. You have on hand Drug X labeled gr 1/150 = 1 mL.
How many mL will you give? _______ mL
8. You are to give Drug X 5 mg/kg/day. Your patient weighs 23 pounds. You have a bottle
labeled 125 mg/5 mL. You are to give the drug in four equally divided doses per day. How much will you give for one dose (mL)?
_______ mL

158
PHARMACOLOGY PRACTICE PROBLEMS #3 (CONTINUED) 9. You are to give Drug X 1 g IVPB in 100 mL every 6 hours. You are to infuse it in over a 30
minute period. Drop factor is 10. You have 1 g of Drug X in 100 mL 5% D/W.
At what rate will you infuse it in mL per hour? _______ mL/hr
At what rate will you infuse it in gtts per minute? _______ gtts/min
10. The patient is to receive 100 mg of Drug X at bedtime to be administered via the feeding
tube. The concentration of the medications is 20 mg/5 mL. How many mL should be administered via the feeding tube?
_______ mL 11. You are to add 12 mEq of Drug X to an IV. You have a vial of Drug X labeled 20 mEq in 10
mL. How many mL will you add to the IV? _______ mL
12. You have been given an order to begin infusing Drug X at 10 mcg/minute. You are to add 10
mg to 500mL of D5/LR. Drug X vials are labeled 10 mg/mL. What is the concentration of the solution? _______ mcg/mL What is the infusion rate? _______ mL/hr

159
PHARMACOLOGY PRACTICE PROBLEMS #3 (CONTINUED) 13. You are to run an infusion of Drug X, starting with a bolus dose of 4 g over 30 minutes and then a maintenance rate of 2 g/hr. (Drug X comes in a 50% solution in 20 mL vials and the standard mixture is 40 g in 1000 mL of D5RL.) What is the rate of infusion for the bolus dose? _______ mL/hr What will the maintenance rate be set at on the IV pump? _______ mL/hr

160
PHARMACOLOGY PRACTICE PROBLEMS #3
ANSWERS
1.
Discard Give
0.2 mL 0.8 mL
0.25 mL 0.75 mL
0.33 mL 0.67 mL
0.25 mL 0.75 mL
2.
mL/hour gtt/minute
62.5 mL 16 gtts
83.3 mL 21 gtts
140 mL 35 gtts
3.
mL/hour gtts/minute
20.8 mL 21 gtts
12.5 mL 13 gtts
4. 47.3 mL
7.9 mL 1181.82 mg
5. 0.3 mL
6. 166.7 mL/hr
7. 0.75 mL
8. 0.52 mL
9. a. 200 mL/hour b. 33 gtts/minute
10. 25 mL
11. 6 mL
12. a. 20 mcg/mL b. 30 mL/hour
13. a. 200 mL/hour b. 50 mL/hour

161
REVIEW TEST
TIME LIMIT: 1 HOUR 40 MINUTES
1. The physician has ordered 400 mg of a drug. The label reads as follows: Add 3.6 mL sterile water to make 150 mg/mL. How many mL will you give?
_______ mL
2. A label reads 8 mg per 4 mL. You are to give 20 mg. How many mL will you give?
_______ mL
3. You have an order for 500,000 units Drug X. The label reads: Add 8.2 mL to make 1 mL = 300,000 units. How many mL will you give?
_______ mL
4. Give 0.2 g Drug X from a 5 mL vial labeled 100 mg per mL. How many mL will you give?
_______ mL
5. You are to give 0.1 mg of a drug. You have tablets labeled 100 mcg each. How many tablets will you give?
______ tabs
6. The physician has ordered 100 mg of Drug X PO. You have tablets of 0.05 g each. How many tablets will you give?
_______ tabs

162
REVIEW TEST (CONTINUED)
7. You are to give gr 1/300 of Drug X from a vial labeled 1 mL = 0.2 mg. How many mL will you give?
_______ mL
8. You have an order for 80 mg of Drug X PO. The tablets contain gr 1/3 per tablet. How many tablets will you give?
_______ tabs
9. You are to give Drug X gr 1/600 from a vial which reads 0.15 mg per mL. How many mL will you give?
_______ mL
10. Ordered: Drug X 20 mg. Label reads: 120 mg = 5 mL. How many mL will you give?
_______ mL
11. Administer Drug X 15 mg from a vial labeled: 1 mL = gr 1/8. How many mL will you give?
_______ mL
12. You are to administer Drug X to a child weighing 86 pounds. The order is for 5 mg per kg. You have a bottle labeled: Drug X 125 mg per 5 mL. How many mL will you give?
_______ mL
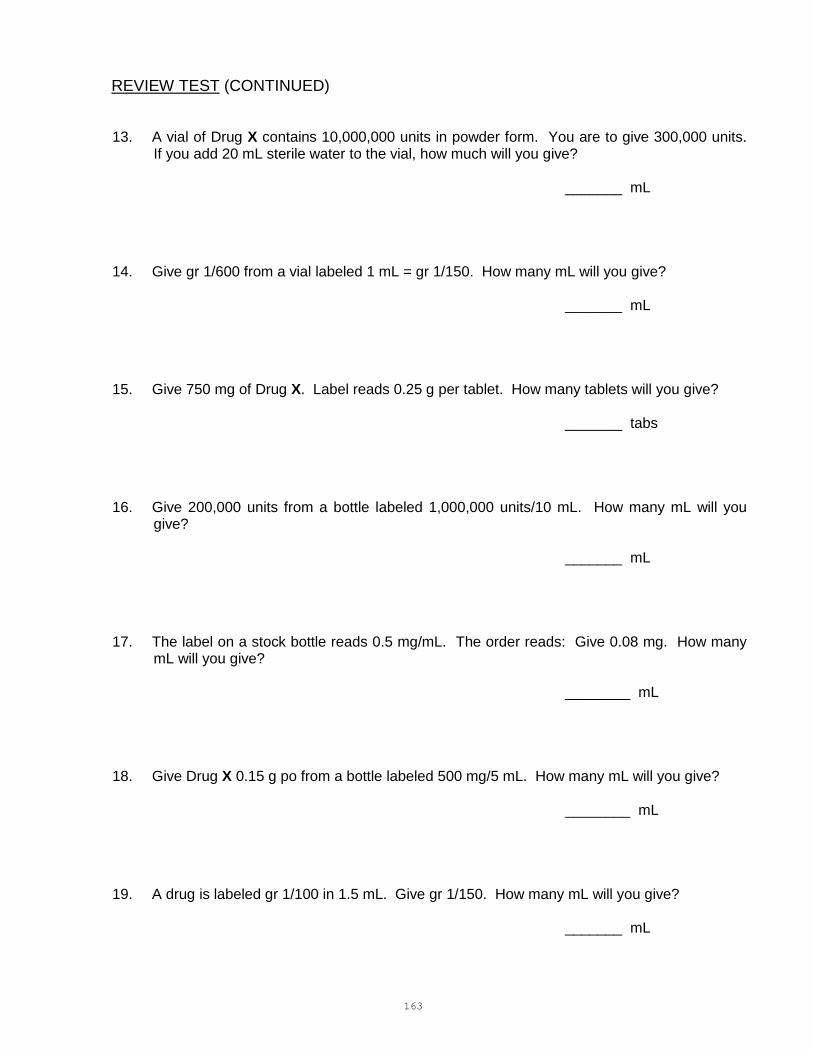
163
REVIEW TEST (CONTINUED)
13. A vial of Drug X contains 10,000,000 units in powder form. You are to give 300,000 units. If you add 20 mL sterile water to the vial, how much will you give?
_______ mL 14. Give gr 1/600 from a vial labeled 1 mL = gr 1/150. How many mL will you give? _______ mL 15. Give 750 mg of Drug X. Label reads 0.25 g per tablet. How many tablets will you give? _______ tabs 16. Give 200,000 units from a bottle labeled 1,000,000 units/10 mL. How many mL will you
give? _______ mL 17. The label on a stock bottle reads 0.5 mg/mL. The order reads: Give 0.08 mg. How many
mL will you give? ________ mL 18. Give Drug X 0.15 g po from a bottle labeled 500 mg/5 mL. How many mL will you give? ________ mL 19. A drug is labeled gr 1/100 in 1.5 mL. Give gr 1/150. How many mL will you give? _______ mL
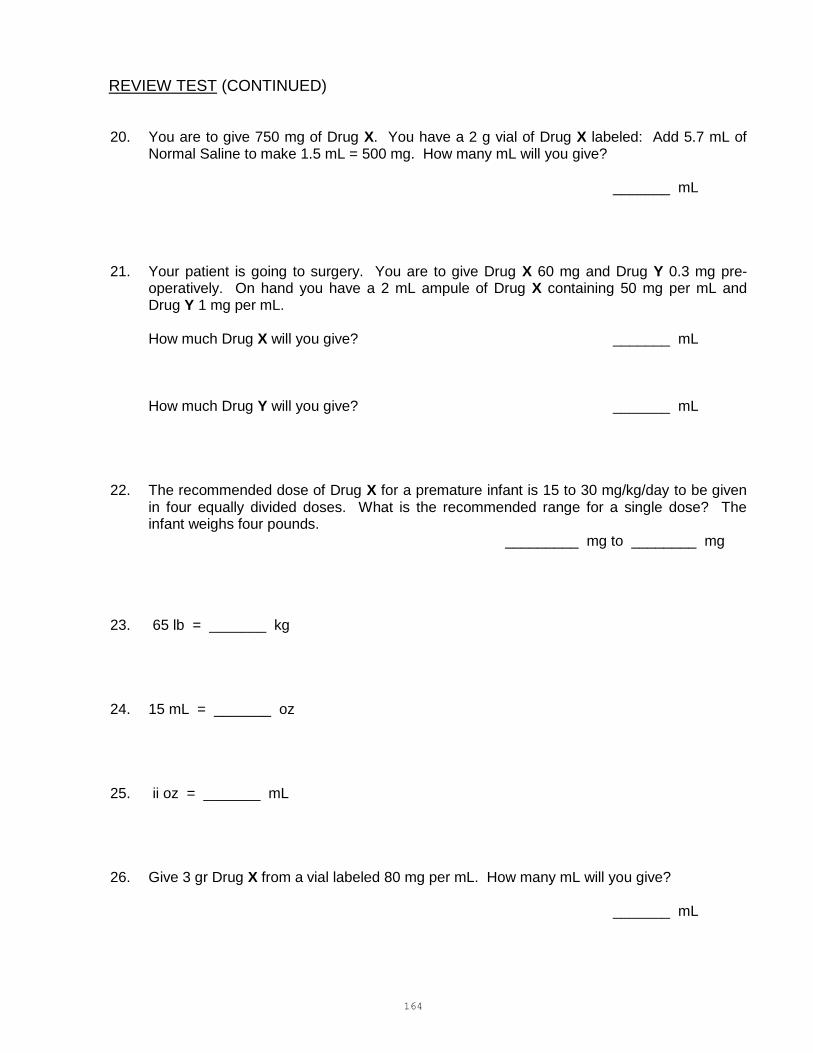
164
REVIEW TEST (CONTINUED)
20. You are to give 750 mg of Drug X. You have a 2 g vial of Drug X labeled: Add 5.7 mL of Normal Saline to make 1.5 mL = 500 mg. How many mL will you give?
_______ mL
21. Your patient is going to surgery. You are to give Drug X 60 mg and Drug Y 0.3 mg pre- operatively. On hand you have a 2 mL ampule of Drug X containing 50 mg per mL and Drug Y 1 mg per mL.
How much Drug X will you give? _______ mL
How much Drug Y will you give? _______ mL
22. The recommended dose of Drug X for a premature infant is 15 to 30 mg/kg/day to be given in four equally divided doses. What is the recommended range for a single dose? The infant weighs four pounds.
_________ mg to ________ mg
23. 65 lb = _______ kg
24. 15 mL = _______ oz
25. ii oz = _______ mL
26. Give 3 gr Drug X from a vial labeled 80 mg per mL. How many mL will you give?
_______ mL
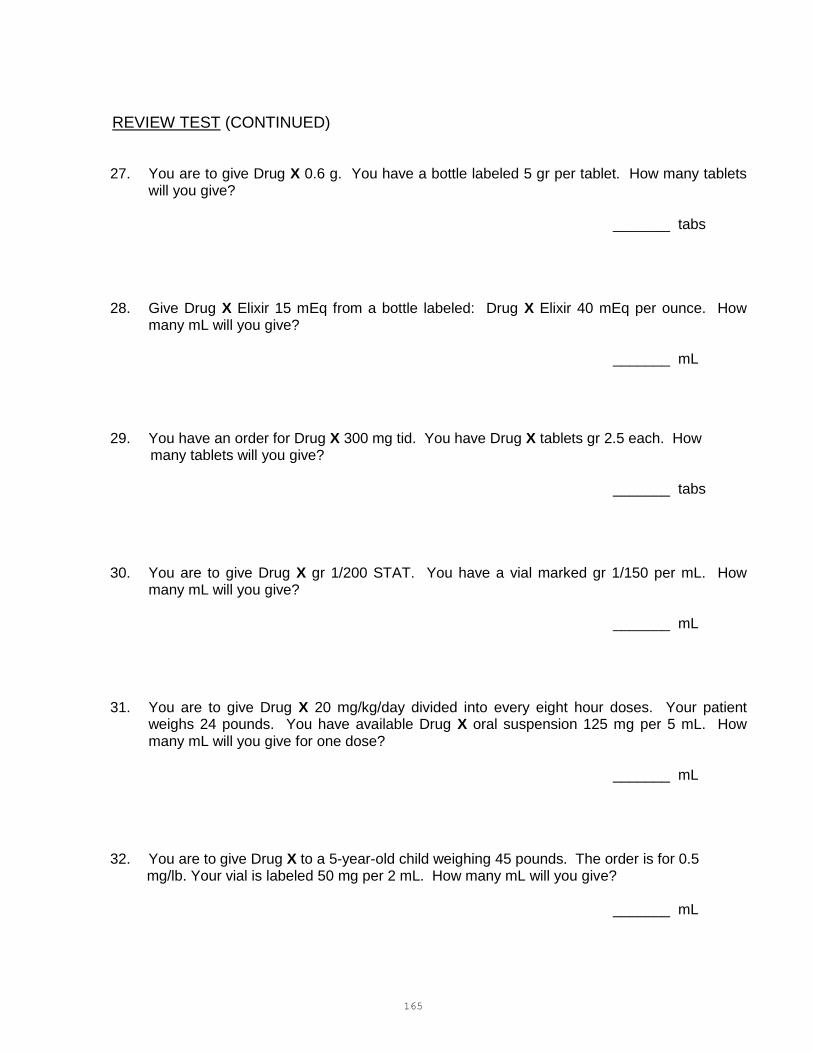
165
REVIEW TEST (CONTINUED)
27. You are to give Drug X 0.6 g. You have a bottle labeled 5 gr per tablet. How many tablets will you give?
_______ tabs
28. Give Drug X Elixir 15 mEq from a bottle labeled: Drug X Elixir 40 mEq per ounce. How many mL will you give?
_______ mL
29. You have an order for Drug X 300 mg tid. You have Drug X tablets gr 2.5 each. How many tablets will you give?
_______ tabs
30. You are to give Drug X gr 1/200 STAT. You have a vial marked gr 1/150 per mL. How many mL will you give?
_______ mL
31. You are to give Drug X 20 mg/kg/day divided into every eight hour doses. Your patient weighs 24 pounds. You have available Drug X oral suspension 125 mg per 5 mL. How many mL will you give for one dose?
_______ mL
32. You are to give Drug X to a 5-year-old child weighing 45 pounds. The order is for 0.5 mg/lb. Your vial is labeled 50 mg per 2 mL. How many mL will you give?
_______ mL

166
REVIEW TEST (CONTINUED)
33. You are to give Drug X 1/4 gr IM. Your ampule is labeled 1/8 gr per mL. How many Ml will you give?
_______ mL
34. 0.6 g = gr ________
35. 100 mg = gr ________
36. You are to give Drug X gr 1/8. Your bottle is labeled 2 mg per mL. How many mL will you administer?
_______ mL
37. You are to give Drug X 400,000 units bid. You have a 10 mL vial labeled 300,000 units per mL. How many mL will you give?
_______ mL
38. You are to give Drug X 1 g IV STAT. You have a 10 mL ampule of Drug X 10%. How many mL will you give?
_______ mL
39. You are to give Drug X subcutaneously STAT according to the pediatric emergency room's dosage guideline of 0.01 mL/kg/dose of 1:1000 solution. You are to administer Drug X to
an 11 pound infant. How many mL will you give?
_______ mL

167
REVIEW TEST (CONTINUED)
40. How many mg will you give in Problem #39?
_______ mg
41. You are to give Drug X 10,000 units every eight hours. You have a vial marked 40,000 units per mL. How many mL will you give?
_______ mL
42. You are to give Drug X 0.5 mg. You have an ampule labeled 0.5 mL = 1 mg. How many mL will you give?
_______ mL
43. Drug X is ordered 0.01 mg/kg/dose. You are to administer this to an 8 1/4 pound infant. Your ampule is labeled: 1 mL of Epinephrine 1:10,000. How many mL will you give?
_______ mL
44. 300 mg = gr _______
45. gr 15 = ________ g
46. 4 tbsp = ________ oz.
47. You have an order for 40 mg of a drug. Available is a vial with 50 mg/mL. How many mL are needed for one dose?
_______ mL

168
REVIEW TEST (CONTINUED)
48. You are to give 0.016 g of Drug X. On hand is a bottle labeled 4 mg=1 mL. How many mL will you give?
_______ mL
49. A continuous infusion of Drug X is ordered for a newly admitted patient in Cardiogenic shock. The concentration is 2 mg in 500 mL D5W, and the rate of infusion is 40 mL/hour. Calculate the mcg/min infusing.
_______ mcg/min
50. A patient is to receive 3000 mL of D5W over 20 hours. The drop factor is 20 gtts/mL. Calculate the flow rate in gtts/minute.
________ gtts/minute
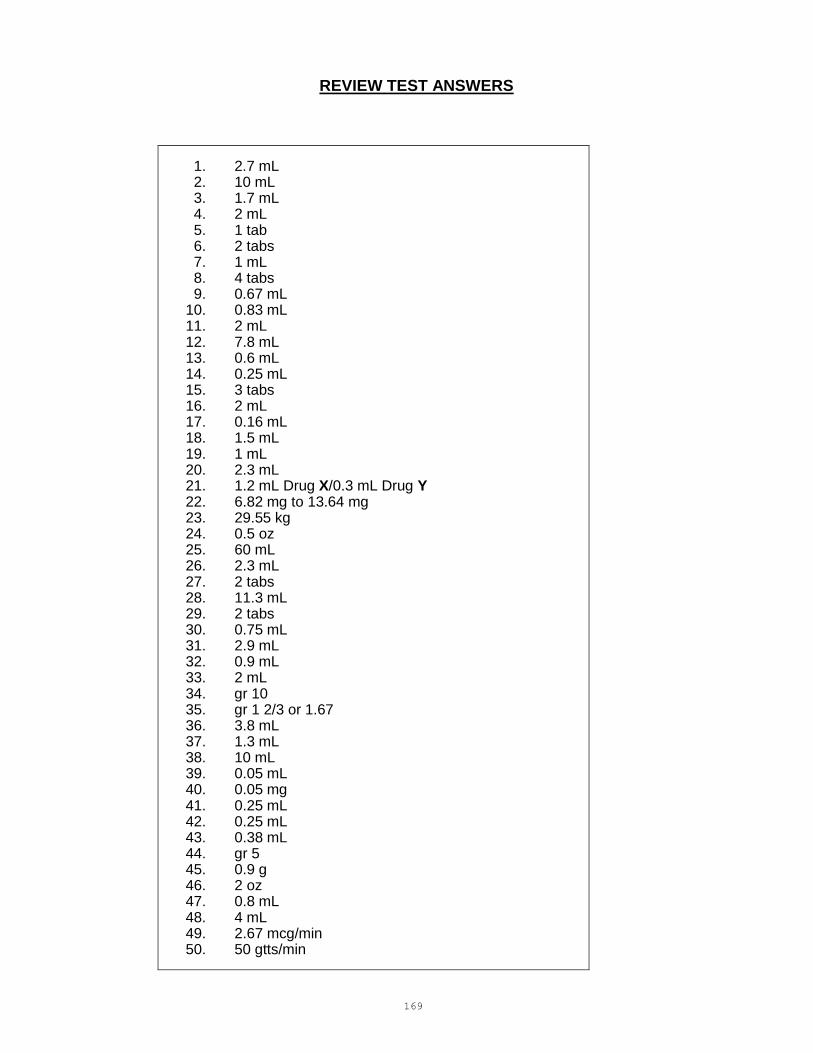
169
REVIEW TEST ANSWERS
1. 2.7 mL 2. 10 mL 3. 1.7 mL 4. 2 mL 5. 1 tab 6. 2 tabs 7. 1 mL 8. 4 tabs 9. 0.67 mL 10. 0.83 mL 11. 2 mL 12. 7.8 mL 13. 0.6 mL 14. 0.25 mL 15. 3 tabs 16. 2 mL 17. 0.16 mL 18. 1.5 mL 19. 1 mL 20. 2.3 mL 21. 1.2 mL Drug X/0.3 mL Drug Y 22. 6.82 mg to 13.64 mg 23. 29.55 kg 24. 0.5 oz 25. 60 mL 26. 2.3 mL 27. 2 tabs 28. 11.3 mL 29. 2 tabs 30. 0.75 mL 31. 2.9 mL 32. 0.9 mL 33. 2 mL 34. gr 10 35. gr 1 2/3 or 1.67 36. 3.8 mL 37. 1.3 mL 38. 10 mL 39. 0.05 mL 40. 0.05 mg 41. 0.25 mL 42. 0.25 mL 43. 0.38 mL 44. gr 5 45. 0.9 g 46. 2 oz 47. 0.8 mL 48. 4 mL 49. 2.67 mcg/min 50. 50 gtts/min
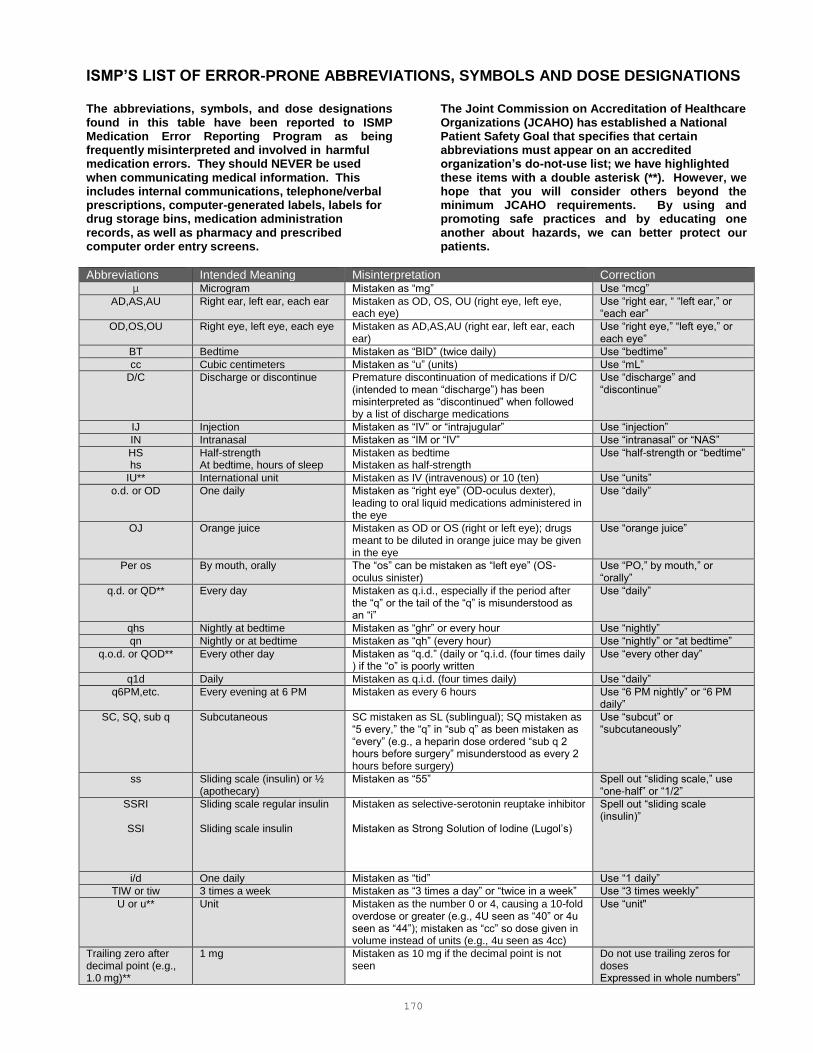
170
ISMP’S LIST OF ERROR-PRONE ABBREVIATIONS, SYMBOLS AND DOSE DESIGNATIONS The abbreviations, symbols, and dose designations found in this table have been reported to ISMP Medication Error Reporting Program as being frequently misinterpreted and involved in harmful medication errors. They should NEVER be used when communicating medical information. This includes internal communications, telephone/verbal prescriptions, computer-generated labels, labels for drug storage bins, medication administration records, as well as pharmacy and prescribed computer order entry screens.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has established a National Patient Safety Goal that specifies that certain abbreviations must appear on an accredited organization’s do-not-use list; we have highlighted these items with a double asterisk (**). However, we hope that you will consider others beyond the minimum JCAHO requirements. By using and promoting safe practices and by educating one another about hazards, we can better protect our patients.
Abbreviations Intended Meaning Misinterpretation Correction µ Microgram Mistaken as “mg” Use “mcg”
AD,AS,AU Right ear, left ear, each ear Mistaken as OD, OS, OU (right eye, left eye, each eye)
Use “right ear, “ “left ear,” or “each ear”
OD,OS,OU Right eye, left eye, each eye Mistaken as AD,AS,AU (right ear, left ear, each ear)
Use “right eye,” “left eye,” or each eye”
BT Bedtime Mistaken as “BID” (twice daily) Use “bedtime”
cc Cubic centimeters Mistaken as “u” (units) Use “mL”
D/C Discharge or discontinue Premature discontinuation of medications if D/C (intended to mean “discharge”) has been misinterpreted as “discontinued” when followed by a list of discharge medications
Use “discharge” and “discontinue”
IJ Injection Mistaken as “IV” or “intrajugular” Use “injection”
IN Intranasal Mistaken as “IM or “IV” Use “intranasal” or “NAS”
HS hs
Half-strength At bedtime, hours of sleep
Mistaken as bedtime Mistaken as half-strength
Use “half-strength or “bedtime”
IU** International unit Mistaken as IV (intravenous) or 10 (ten) Use “units”
o.d. or OD One daily Mistaken as “right eye” (OD-oculus dexter), leading to oral liquid medications administered in the eye
Use “daily”
OJ Orange juice Mistaken as OD or OS (right or left eye); drugs meant to be diluted in orange juice may be given in the eye
Use “orange juice”
Per os By mouth, orally The “os” can be mistaken as “left eye” (OS-oculus sinister)
Use “PO,” by mouth,” or “orally”
q.d. or QD** Every day Mistaken as q.i.d., especially if the period after the “q” or the tail of the “q” is misunderstood as an “i”
Use “daily”
qhs Nightly at bedtime Mistaken as “ghr” or every hour Use “nightly”
qn Nightly or at bedtime Mistaken as “qh” (every hour) Use “nightly” or “at bedtime”
q.o.d. or QOD** Every other day Mistaken as “q.d.” (daily or “q.i.d. (four times daily ) if the “o” is poorly written
Use “every other day”
q1d Daily Mistaken as q.i.d. (four times daily) Use “daily”
q6PM,etc. Every evening at 6 PM Mistaken as every 6 hours Use “6 PM nightly” or “6 PM daily”
SC, SQ, sub q Subcutaneous SC mistaken as SL (sublingual); SQ mistaken as “5 every,” the “q” in “sub q” as been mistaken as “every” (e.g., a heparin dose ordered “sub q 2 hours before surgery” misunderstood as every 2 hours before surgery)
Use “subcut” or “subcutaneously”
ss Sliding scale (insulin) or ½ (apothecary)
Mistaken as “55” Spell out “sliding scale,” use “one-half” or “1/2”
SSRI
SSI
Sliding scale regular insulin Sliding scale insulin
Mistaken as selective-serotonin reuptake inhibitor Mistaken as Strong Solution of Iodine (Lugol’s)
Spell out “sliding scale (insulin)”
i/d One daily Mistaken as “tid” Use “1 daily”
TIW or tiw 3 times a week Mistaken as “3 times a day” or “twice in a week” Use “3 times weekly”
U or u** Unit Mistaken as the number 0 or 4, causing a 10-fold overdose or greater (e.g., 4U seen as “40” or 4u seen as “44”); mistaken as “cc” so dose given in volume instead of units (e.g., 4u seen as 4cc)
Use “unit"
Trailing zero after decimal point (e.g., 1.0 mg)**
1 mg Mistaken as 10 mg if the decimal point is not seen
Do not use trailing zeros for doses Expressed in whole numbers”
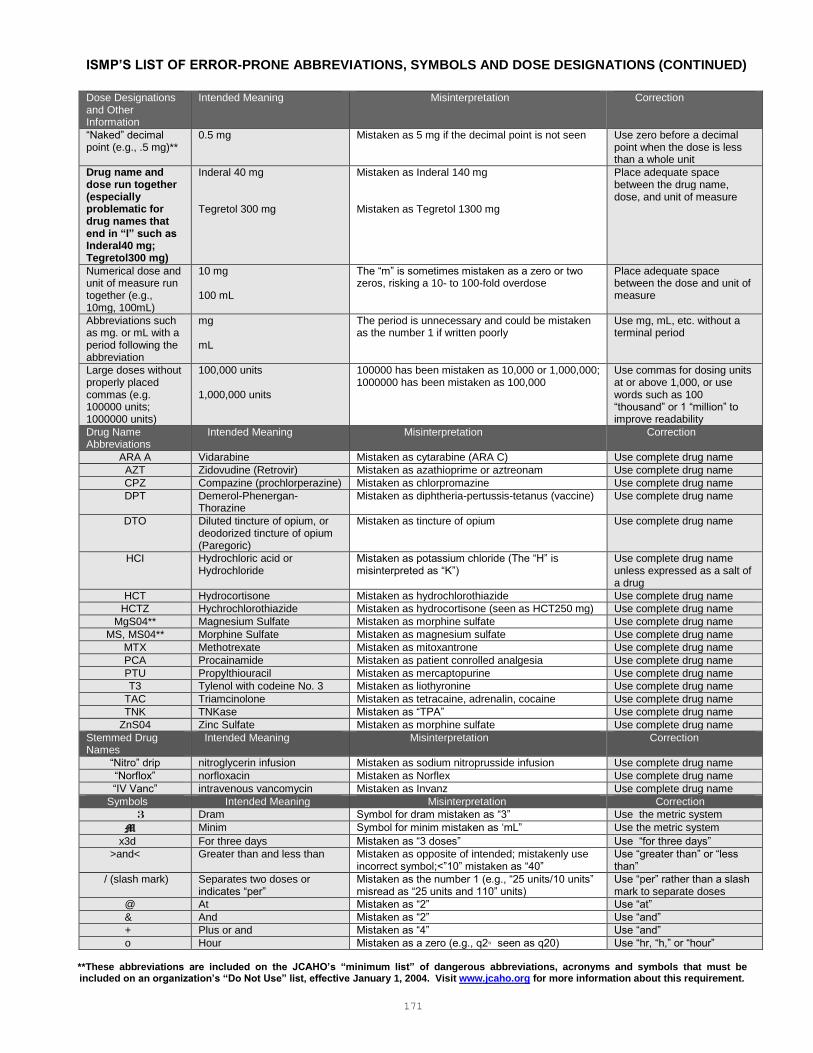
171
ISMP’S LIST OF ERROR-PRONE ABBREVIATIONS, SYMBOLS AND DOSE DESIGNATIONS (CONTINUED)
Dose Designations and Other Information
Intended Meaning Misinterpretation Correction
“Naked” decimal point (e.g., .5 mg)**
0.5 mg Mistaken as 5 mg if the decimal point is not seen Use zero before a decimal point when the dose is less than a whole unit
Drug name and dose run together (especially problematic for drug names that end in “l” such as Inderal40 mg; Tegretol300 mg)
Inderal 40 mg Tegretol 300 mg
Mistaken as Inderal 140 mg Mistaken as Tegretol 1300 mg
Place adequate space between the drug name, dose, and unit of measure
Numerical dose and unit of measure run together (e.g., 10mg, 100mL)
10 mg 100 mL
The “m” is sometimes mistaken as a zero or two zeros, risking a 10- to 100-fold overdose
Place adequate space between the dose and unit of measure
Abbreviations such as mg. or mL with a period following the abbreviation
mg mL
The period is unnecessary and could be mistaken as the number 1 if written poorly
Use mg, mL, etc. without a terminal period
Large doses without properly placed commas (e.g. 100000 units; 1000000 units)
100,000 units 1,000,000 units
100000 has been mistaken as 10,000 or 1,000,000; 1000000 has been mistaken as 100,000
Use commas for dosing units at or above 1,000, or use words such as 100 “thousand” or 1 “million” to improve readability
Drug Name Abbreviations
Intended Meaning Misinterpretation Correction
ARA A Vidarabine Mistaken as cytarabine (ARA C) Use complete drug name
AZT Zidovudine (Retrovir) Mistaken as azathioprime or aztreonam Use complete drug name
CPZ Compazine (prochlorperazine) Mistaken as chlorpromazine Use complete drug name
DPT Demerol-Phenergan-Thorazine
Mistaken as diphtheria-pertussis-tetanus (vaccine) Use complete drug name
DTO Diluted tincture of opium, or deodorized tincture of opium (Paregoric)
Mistaken as tincture of opium Use complete drug name
HCI Hydrochloric acid or Hydrochloride
Mistaken as potassium chloride (The “H” is misinterpreted as “K”)
Use complete drug name unless expressed as a salt of a drug
HCT Hydrocortisone Mistaken as hydrochlorothiazide Use complete drug name
HCTZ Hychrochlorothiazide Mistaken as hydrocortisone (seen as HCT250 mg) Use complete drug name
MgS04** Magnesium Sulfate Mistaken as morphine sulfate Use complete drug name
MS, MS04** Morphine Sulfate Mistaken as magnesium sulfate Use complete drug name
MTX Methotrexate Mistaken as mitoxantrone Use complete drug name
PCA Procainamide Mistaken as patient conrolled analgesia Use complete drug name
PTU Propylthiouracil Mistaken as mercaptopurine Use complete drug name
T3 Tylenol with codeine No. 3 Mistaken as liothyronine Use complete drug name
TAC Triamcinolone Mistaken as tetracaine, adrenalin, cocaine Use complete drug name
TNK TNKase Mistaken as “TPA” Use complete drug name
ZnS04 Zinc Sulfate Mistaken as morphine sulfate Use complete drug name
Stemmed Drug Names
Intended Meaning Misinterpretation Correction
“Nitro” drip nitroglycerin infusion Mistaken as sodium nitroprusside infusion Use complete drug name
“Norflox” norfloxacin Mistaken as Norflex Use complete drug name
“IV Vanc” intravenous vancomycin Mistaken as Invanz Use complete drug name
Symbols Intended Meaning Misinterpretation Correction
3 Dram Symbol for dram mistaken as “3” Use the metric system
M Minim Symbol for minim mistaken as ‘mL” Use the metric system
x3d For three days Mistaken as “3 doses” Use “for three days”
>and< Greater than and less than Mistaken as opposite of intended; mistakenly use incorrect symbol;<”10” mistaken as “40”
Use “greater than” or “less than”
/ (slash mark) Separates two doses or indicates “per”
Mistaken as the number 1 (e.g., “25 units/10 units” misread as “25 units and 110” units)
Use “per” rather than a slash mark to separate doses
@ At Mistaken as “2” Use “at”
& And Mistaken as “2” Use “and”
+ Plus or and Mistaken as “4” Use “and”
o Hour Mistaken as a zero (e.g., q2◦ seen as q20) Use “hr, “h,” or “hour” **These abbreviations are included on the JCAHO’s “minimum list” of dangerous abbreviations, acronyms and symbols that must be included on an organization’s “Do Not Use” list, effective January 1, 2004. Visit www.jcaho.org for more information about this requirement.





























