Upload
others
View
11
Download
0
Embed Size (px)
Citation preview
ANTEPARTAL AND INTRAPARTAL FETAL
MONITORING3rd Edition
By MICHELLE L. MURRAY, PhD, RNC
New York
“But many do not know that they do not know, and many think they know when they know nothing.”
Balthasar GraciánOriginally written in 1637 in SpanishTranslated by Joseph JacobThe Art of Worldly Wisdom© 1993 Shambhala Publications, Inc.
Copyright © 2007 Springer Publishing Company, LLC
All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system, or transmitted inany form or by any means, electronic, mechanical, photocopying, recording, or otherwise, with-out the prior permission of Springer Publishing Company, LLC.
Springer Publishing Company, LLC11 West 42nd StreetNew York, NY 10036www.springerpub.com
Acquisitions Editor: James CostelloProduction Editor: Rose Mary PiscitelliComposition: International Graphic Services
07 08 09 10 / 5 4 3 2 1––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Library of Congress Cataloging-in-Publication Data
Antepartal and intrapartal fetal monitoring / [edited] by Michelle L. Murray.–3rd ed.p. ; cm.
Includes bibliographical references and index.ISBN 0-8261-3262-61. Fetal monitoring. I. Murray, Michelle (Michelle L.)[DNLM: 1. Fetal Monitoring. 2. Heart Rate, Fetal. WQ 209
A6271 2007]RG628.A574 2007618.3’2075--dc22
2006028397––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Printed in the United States of America by Bang Printing
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
ii
www.springerpub.com
ANTEPARTAL AND INTRAPARTAL FETAL MONITORINGThird Edition
Michelle L. Murray, PhD, RNCAuthor and Editor
Kenneth J. Moise, Jr., MDGary Joffe, MDSherrill L. Tillger, RN, MAContributing Editors
Contributions By:
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
iii
Chapter 1 Penny Peterson, RNC, MSNCorporate Sponsors
Chapter 2 Deborah J. Eganhouse, PhD, RNCSherrill L. Tillger, RN, MAJean Marie Yackey, RNC, MSN
Chapters 3 & 4 Tracey A. Kasnic, RNC, BSN, MBA
Chapter 5 Katherine W. O’Connell, RN, MN
Chapter 6 Linda Chagnon, RNC, MBA, MNJulia M. B. Fine, PhD, RNJoyce Vogler, DrPH, RN
Chapter 7 Kathy W. O’Connell, RN, MN
Chapter 8Linda A. Petersen, RNC, BSNCheryl Wallerstedt, RNC, MS
Chapter 9 Carolyn L. Gegor, CNM, MS, RDMS
Chapter 10 Carolyn L. Gegor, CNM, MS, RDMSSusan Nelson, RN
PrefaceThe dawn of a new era in treating the fetus as a patient arrived in 1958 when Dr. Edward Hon reported the capabili-ty to continuously assess the fetal heart rate by means of a fetal EKG monitor on the maternal abdomen.Commercial devices for bedside fetal heart rate monitoring were introduced in the late 1960s, and by the mid-1980sthe great majority of laboring women in the United States underwent electronic fetal monitoring.
Our forefathers were so convinced that such surveillance would reduce the incidence of cerebral palsy and peri-natal asphyxia that clinical trials were omitted before widespread implementation of fetal monitoring. Some 40years later, we know this not to be the case. Clearly, a large percentage of perinatal asphyxia occurs prior to theonset of labor. Recent randomized trials have even questioned the validity of continuous electronic monitoring inany low-risk obstetrical patient. In addition, several authorities have concluded that monitoring has contributed tothe disturbing rise in the rate of cesarean delivery.
Minimal advances have been achieved in monitoring techniques. Computer technology has brought us autocor-relation to improve our ability to assess fetal heart rate variability with external monitoring. Electronic sensors inspecialized intrauterine pressure catheters with amnioinfusion ports have improved our capability to accuratelyassess intrauterine pressure and replace amniotic fluid volume in cases of variable decelerations. Yet in an era whenspace shuttle missions are so commonplace that they rarely receive prime time television coverage, we must stillrely on the interaction between the fetal central nervous system and the fetal heart to establish in utero well-being.Perhaps the newest technology of fetal pulse oximetry, now in clinical trials, will aid us in accurately interpretingthe fetal heart rate tracing. More likely, a continuous assessment of the fetal acid-base status will transform the art ofevaluating fetal monitoring tracings into a true science.
Although the accurate interpretation of a fetal heart rate tracing is paramount to the care of the laboring patient,it remains one of the more difficult skills to master. One must learn to appreciate subtle changes in the baseline rate,short-term variability, and patterns of decelerations to determine that the tracing is nonreassuring. In her secondedition of Antepartal and Intrapartal Fetal Monitoring, Michelle Murray, PhD, RNC, has provided us with an excellenttool to begin the process of understanding the basics as well as the more advanced aspects of fetal heart rate moni-toring. The book has more than doubled in size since the publication of the first edition in 1988. Sections on mater-nal and fetal physiology have been added to describe the wealth of knowledge that has been acquired in these areasin the last decade. Dr. Murray has chosen to include a section on fetal pulse oximetry, a clear reflection of the con-temporaneous nature of this book. Beginners will find this work extremely useful to master the endless patterns offetal heart rate tracings. This book also deserves a special place on the front shelf of the seasoned practitioner as auseful reference text.
Kenneth J. Moise, Jr., MDUpJohn Distinguished Professor of Obstetrics and Gynecology
Director, Division of Maternal-Fetal MedicineUniversity of North CarolinaChapel Hill, North Carolina
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
iv
PrefaceIn 1988, Michelle Murray’s text, Antepartal and Intrapartal Fetal Monitoring, was published by the Nurses’ Associationof the American College of Obstetricians and Gynecologists (NAACOG). NAACOG is now known as theAssociation of Women’s Health, Obstetric, and Neonatal Nurses (AWHONN). Antepartal and Intrapartal FetalMonitoring has been referred to as “The Bible.” It was updated in 1989, and has sold over 10,000 copies. In this newedition, Dr. Murray has expanded the depth and breadth of the original text. The second edition provides practition-ers with the needed references and resources they need to provide quality care to women and their fetuses. It is acutting edge resource for a practice-based discipline, with details and references that are specific and clear. In addi-tion, the protocols and procedures found in the appendix are applicable to clinical practices that include fetal monitors.
The leadership role in fetal monitoring education for nurses came from AWHONN. AWHONN demonstratedtheir commitment to fetal monitoring by publishing the first edition of this text. AWHONN continues to take a lead-ership role in fetal monitoring education through their fetal monitoring courses and videotapes. AWHONN is to becommended in these endeavors.
Building on the traditions of AWHONN, Dr. Murray selected a broad base team of contributors and editors whorepresent every aspect of perinatal nursing and medicine from practice, research, business, industry, education,management, and academia. The educational preparation of this team is vast, representing the baccalaureate to thedoctorate. All contributors have expertise in one or more aspects of fetal monitoring. Many are fetal monitoringinstructors or instructor-trainers for AWHONN.
As with any book, there are people who help turn dreams into reality. One is Elaine Smiel who, during the preg-nancy of her fourth child, undertook the task of typing this text. Indeed, it was a birthing process. Dr. Murray’s sons,Sean and David, have been an inspiration and a grounding force for their mother. They have allowed her the oppor-tunity to grow and create this new book for all of us to use in our practice settings. Most of all, this book is for you.To the nurses who care for mothers, babies, and families, may this text be the foundation for your excellence in prac-tice, education, and research. To the physicians who read this text, our teamwork and common knowledge are anasset to the quality care families deserve.
Patricia Grant Higgins, PhD, RNProfessor of Parent-Child Nursing, retired
University of New Mexico Health Sciences CenterCollege of Nursing, Albuquerque, New Mexico
AWHONN Director-at-Large
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
v
AcknowledgmentsThe Decade of the 1970sIn the 1970s, when I became a labor and delivery staff nurse, the vast majority of nurses and physicians learned to usefetal monitors “on the job.” A few books were available to help us learn basic fetal monitoring concepts. Journal arti-cles started to appear that enhanced our understanding of the fetus. For example, the first case report on fetal seizuresthat included a fetal heart rate pattern was published in 1978 in the American Journal of Obstetrics and Gynecology.
The Decade of the 1980sIn 1980, I became an instructor in a 2 year associate degree program. My MSN was completed in May, 1981. TheADN curriculum included only 1/2 hour on fetal monitoring concepts. Student nurses were rarely allowed to partici-pate in the care of a woman during labor and delivery, other than to witness a delivery. Just as I had learned fetalmonitoring, graduates of our program were expected to learn fetal monitoring “on the job.”
In 1984, I became the Ob/Gyn Nursing Education Coordinator for a 9 hospital system in New Mexico. I wastasked with developing a fetal monitoring education program for nurses. By 1986, I had taught 500 nurses fetalmonitoring. The handout materials for that program grew into a book which later became the first edition of thistext. The entire process of creating the first edition of Antepartal and Intrapartal Fetal Monitoring took 3 years. In 1985,I began my doctoral studies. Antepartal and Intrapartal Fetal Monitoring was published in 1988. I completed my doctoral studies in 1992.
The 1990sBetween 1986 and 1996, over 50,000 people from all 50 states and at least 7 foreign countries had attended my cours-es on fetal monitoring. The excellence of these courses is due, in part, to the dedicated staff at ProfessionalEducation Center in Chico, California. My participants have included student nurses, OB techs, licensed practicalnurses, registered nurses, certified nurse midwives, residents, family practice physicians, obstetricians, chiefs ofobstetrics, paralegals, insurance company employees, and lawyers. They have been my teachers and have generous-ly shared their most interesting tracings and experiences with me. Many of their tracings are included in this text. Ithank each and every one of them for their generous contributions and support.
I wish to thank everyone who helped me finish the second edition, which was completed in 1 1/2 years. The reference librarians and employees at the New Mexico Health Sciences Center Library, especially Becca, Judy, andTim, always maintained a pleasant attitude in spite of our pressures and deadlines. Whatever we needed, theyhelped us get. The quality of the reference lists reflects their excellence and the work of Elaine Smiel, who spentcountless hours on the telephone with the librarians, or copying articles for me to read, or typing.
My contributors are all very busy, talented, and dedicated people. Each offered as much support as they could so that this text could be revised. Some critiqued a chapter and made suggestions for additions. Others rewrote sections of the old edition. Some wrote sections of the new edition and even edited a chapter. Corporate sponsorsoffered support so that the text could be completed in as short a time as possible.
It is with deep pride and intense love that I thank my sons, Sean and David, for their continued tolerance of mywork to educate users of the fetal monitor. I wish to acknowledge my mother, Emma Sarah Angel Moise, whotaught me, “If there’s a will, there’s a way.” I had the will, I found the way. Now, Springer Publishing will help mereach more readers of this book. I am grateful for their dedication to excellence!
Michelle L. Murray, PhD, RNC
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
vi
Table of Contents
Contributors and Corporate Sponsors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iiiPreface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ivAcknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . viChapter 1 Fetal and Maternal Monitoring Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Chapter 2 The Baseline, Accelerations, and Decelerations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59 Chapter 3 Intrinsic Factors that Affect the Fetal Heart Rate. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163 Chapter 4 Extrinsic Factors that Affect Oxygen Delivery and the FHR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197Chapter 5 Acid-Base Balance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241 Chapter 6 Prediction and Prevention of Intrapartal Fetal Asphyxia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305 Chapter 7 Hemodynamic and Biochemical Fetal Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 341 Chapter 8 Variations of the Fetal Heart Rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 391 Chapter 9 Antepartal Fetal Monitoring. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 455 Chapter 10 Biophysical Fetal Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 489 Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 507 Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 517
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
vii
This page intentionally left blank
Advances in fetal monitor development have paralleled computer and ultrasound development.First generation fetal monitors, from the 1960s and1970s, were equipped with ultrasound technologythat poorly detected the fetal heart rate. In fact, 40 to 45 percent of the signals were missed which created gaps in thetracing (1). Experienced clinicians knew internal devices,such as the spiral electrode and intrauterine pressurecatheter, provided better signal transmission than externaldevices such as the ultrasound transducer and tocotransducer.
A goal of the 1970s was to improve ultrasound (US) technology (2). Advanced microprocessors, wider beam USdevices, and autocorrelation enhanced the signal to noiseratio resulting in a higher quality fetal heart rate (FHR) tracing. Second generation monitors, introduced in the 1980s,had this advanced technology (3-4). Their US signal loss wasless than 20 percent in the less than 25 week gestation andless than 10 percent in the 25 or greater week gestation (5).
A goal of the 1980s was to reduce inconsistent tracinginterpretations. Software programs were developed and tested in both antepartal and intrapartal settings (6-8). Thegoal of the next century is to improve these software programs, incorporating artificial intelligence so that management strategies can be recommended.
The value of electronic fetal monitors depends on thedepth and breath of the user ’s knowledge of fetal and maternal physiology and technology. Chapter 2 examinedfetal and maternal physiology related to regulation of theFHR. This chapter includes strengths and limitations of continuous electronic fetal monitoring (EFM), fetal monitorfeatures, computer applications related to fetal monitoring,
external and internal monitoring devices, and the assessmentand analysis of uterine activity (UA).
BENEFITS AND LIMITATIONS OF CONTINUOUS EFMThe application of a fetal monitor throughout labor with frequent evaluation of the FHR and UA pattern is known ascontinuous EFM. On the positive side, continuous EFM wasassociated with a decrease in fetal and neonatal death rates(0.05 percent vs. 0.43 percent) (9-13). However, controversyabout the benefits of continuous EFM persist due to studiesthat found no relationship between EFM use and fetal death(14-17).
Continuous EFM has been associated with an increase inthe cesarean section and post partum endometritis rates (9).However, EFM studies rarely examine other factors related toan abnormal FHR pattern or the decision to perform a cesareansection. Continuous EFM, in conjunction with fetal scalp pHsampling, was associated with a lower cesarean section ratethan EFM use alone, but a higher cesarean section rate thanintermittent auscultation (18). This finding implies scalp pHresults support a decision to wait for a vaginal birth.
A fetus at high risk for intrapartal asphyxia, such as theintrauterine growth restricted (IUGR) fetus who has limitedoxygen reserves, benefits the most from continuous surveillance.Benefits of continuous EFM must be weighed with its limitations (see Tables 1 and 2). Although there are more limitations than benefits, the impact of each point on thefetus, mother, and her support network should be considered.
Clinicians who overuse EFM may be fearful that laborincreases the risk of fetal or neonatal neurologic injury. But,
Fetal and MaternalMonitoring Equipment
1
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
labor events are rarely the primary cause of cerebral palsy(12, 16, 19-22). Fear may precede “over monitoring,” resulting in millions of monitor tracings for analysis by clinicians with differing educational backgrounds and
interpretation skills. Thus, over monitoring may result inmisinterpretation of FHR and UA patterns, conflicting interpretations, and unnecessary interventions (6-7).
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
2
Table 1: Benefits of Continuous EFM
1. Reliably identifies the healthy fetus (23-25).2. Provides a means of antepartum fetal surveillance in high risk pregnancies (26).3. Less labor intensive than auscultation (23).4. External monitoring, like auscultation, is noninvasive.5. Records FHR variability (23, 25).6. Expedites twin and triplet monitoring.7. Provides a continuous printout of the FHR and UA for evaluation by health care providers who may not be present at the
bedside 100 percent of the time.8. Enhances the woman’s awareness of the onset of contractions so she can begin relaxation techniques (27-28).9. Reassures women when they hear a normal FHR (27-28). 10. Less intrusive than auscultation with less interruption of maternal concentration than intermittent auscultation (27-28).11. Preferred by obese women, high risk women, and women with a history of stillbirth (29).
Table 2: Limitations of Continuous EFM
1. EFM equipment is expensive (30).2. The FHR pattern is not diagnostic, it does not quantitate hypoxia, and a hypoxic fetus may be missed (16, 23-26). Auscultation
may also fail to identify a hypoxic fetus.3. Fetal and maternal benefits are controversial (31-33).4. May increase forceps and cesarean section deliveries (31-33).5. Encourages other obstetric interventions (15, 31-33).6. Subjective analysis of the tracing results in interpretation discrepancies and unnecessary operative interventions (6-7, 26).7. Similar patterns of the FHR or UA have different causes.8. Increased maternal or fetal risk of complications when internal monitoring devices are used, e.g., the spiral
electrode (SE) may be dangerous in the very small preterm fetus (26, 34-35).9. The tocotransducer (toco) may not detect contractions well in preterm, obese, or restless women (36-37).10. The monitor medicalizes labor, may interfere with relaxation, and increases maternal immobility which may affect labor
progress or precede weak and more painful contractions (26, 28, 30, 38).11. Lack of knowledge of FHR and UA patterns may increase anxiety of the woman and her support network (28, 38).12. Perpetuates the misconception that monitors replace nurses (28).13. Places a barrier between the care giver and the laboring woman (28, 38).14. The monitor can become the focal point in the room, distracting attention away from the laboring woman (28, 38).15. The SE may transmit the maternal ECG (MECG) in a case of fetal demise. The maternal heart rate (MHR) will be printed on
the tracing (39). The US may detect maternal aortic wall movement and the MHR will be printed. A failure to recognize thelack of a FHR may delay appropriate management.
EQUIPMENT: FETAL MONITOR FEATURESFetal monitors are capable of detecting, analyzing, and displaying fetal movement, the fetal ECG (FECG), and UA(40). Monitor features include: 1. On/off recorder button: Turns the paper recorder on or off.
2. Paper and Paper tray: Paper is heat sensitive with two distinct sections or channels. The top is referred to as theFHR channel and the bottom is the UA channel. Somemonitors also record fetal movement in the UA channel.The FHR channel may be printed in 5 or 10 beats perminute (bpm) increments on the vertical scale. USA scaledpaper has 10 bpm increments with 30 bpm per
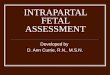
centimeter (cm) on the vertical scale (30 to 240 bpmrange). European scaled paper is printed in 5 bpm increments with 20 bpm/cm on the vertical scale, usuallywith a range of 50 to 210 bpm (2) (see Figure 1.1). Mostmonitors sold in the United States are preset for USAscaled paper. If European scaled paper is used, monitorscan be adjusted to print on this paper. Once the monitor isset to print on European scaled paper, only Europeanscaled paper should be used. Otherwise, if USA scaledpaper is used, the FHR pattern would be misinterpreted.European scaled paper (5 bpm increments) widens theFHR baseline, and increases the height of accelerationsand the depth of decelerations.
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
3
Figure 1.1 USA scaled paper on the left with 30 bpm/cm in the FHR channel. European scaled paper on the right with 20 bpm/cm. Note the uterine activitychannel is similar, usually rising from 0 to 100 mm Hg in 5 to 10 mm Hg increments. Fetal monitor paper may be printed in 10 or 20 second increments.Uterine activity may be denoted in 0 to 13.3 kilopascal (kPa) units (1 kPa = 7.5 mm Hg). At 1, 2 or 3 cm/minute, both USA and European paper roll out of thefetal monitor at the same speed. At 3 cm/minute, 10 seconds = 0.5 cm, and 1 minute includes six 10 second boxes or three 20 second boxes. Paper may beprinted with dark vertical lines 3 cm apart (1 minute) at 3 cm/minute speed.
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
4
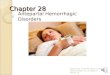
Figure 1.2: With a spiral electrode on the fetus and logic off, PVCs are represented by lines above and below the FHR baselinelevel. With logic on, PVC lines are deleted. The upward deflections reflect the rate calculated from the pulse interval between thenormal R wave and the premature R wave. The downward deflections reflect the slower rate calculated using the pulse intervalbetween the premature R wave and the R wave following a compensatory pause.
3. Paper speed switch: Fetal monitors may be set at 1, 2 or 3cm/minute. However, fetal monitors used in the USA must beset at 3 cm/minute. Anything less would be below thenational standard of practice (41). The standard may varyin other countries where paper speed may be 1, 2 or 3cm/minute. The paper speed is often printed between theFHR and UA channels of the paper. The images at 1 or 2cm/minute will be more compressed than those at 3cm/minute and may be misinterpreted by people whoare unfamiliar with the significance of those images.
4. Printer: Most fetal monitors have a heated thermal arrayprinter, which is necessary when twins are monitored sothat the FHR tracings can overlap. Some fetal monitorshave thermal pens. The width of the printed dot (resolu-tion) affects the accuracy of the printout when there arevery small differences between consecutive calculatedrates. Resolution is usually one bpm, but some monitorshave a 1/2 bpm resolution. Date, time, monitoring mode,
and paper speed may be automatically printed at inter-vals on the paper. When the monitor is started, check theaccuracy of this information.
5. Logic or ECG artifact elimination switch: Logic algorithms inthe monitor software prevent the recording of extraneousnoise and consecutive heart rates that are outside of pre-defined parameters. It is best to leave logic off. When the USis used, most second generation fetal monitors will notprint consecutive rates that differ more than 25 bpm.When the SE is used and logic is ON, consecutive ratesthat differ more than 28 bpm will NOT be printed. Whenlogic is OFF with SE use, all FHRs will be printed.Premature ventricular contractions will appear as longlines of similar length (see Figure 1.2).
6. FECG plot: Monitors that print the FECG on the paper havean ECG plot switch, not a logic switch. At the time of thiswriting, the AMS IM-76® and IM-77® (Advanced Medical
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
5
Figure 1.3: Fetal ECG printout automatically recorded at top of FHR channel if ECG plot is on (tracing provided by Advanced Medical Systems, Hamden, CT).
Systems, Hamden, CT) automatically plotted an FECG for4 seconds at 25 mm/second on the top of the FHR channelif a SE were in use and the consecutive FHRs differed bymore than 20 bpm (see Figure 1.3). This feature can bemanually activated or deactivated. The SonicaidMeridian® intrapartum fetal monitor (Oxford Instruments)also prints the FECG when the SE is used and the ECG plotis activated. Corometrics and Hewlett-Packard monitorsdo not print the FECG on the paper. To see the FECG,Corometrics monitors require a cable and ECG recorder.
7. Test button: Can be activated to check the internal circuitryof the monitor, the printer and paper feed. The digital displays of the FHR and UA are illuminated with a standard set of numbers. When the test button is pressed,the paper rolls out of the machine as the printer printslines and/or words on the paper. The monitor circuitrycan be tested with FHR and UA cables plugged in or out.When the monitor is first plugged in, it may run a selftest. The monitor test may be manually activated.
8. Uterine activity button: Most monitors have a UA button tomove the UA baseline to zero when an intrauterine pressure catheter (IUPC) is used. If a toco is used, thisbutton or dial is used to return the UA baseline to a predetermined level such as 10 units.
9. Fetal heart rate volume: Used to increase or decrease thevolume of the monitor’s speaker.
10. Loudspeaker: The fetal monitor produces sounds. Thesesounds are not actual heart sounds. Therefore, it is inappropriate to inform women that the sound they hearis their baby’s heart beat. If the transducer should slipand no sound is heard, she might think her baby is injeopardy. Therefore, she needs to be informed that thesound is machine generated. Different sounds are produced by the Doppler shift when the US is used. If thesound is not manipulated by the equipment, the differ-ences in the sounds reflected by different moving objectsmay be useful. Different sounds may also be heard when
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
6
Figure 1.4: Maternal heart rate detected by ultrasound transducer during the second stage of labor. Suspect the fetus is not being recorded when there is astable rate with uniform accelerations during times of maternal pain. This is entirely the MHR.
a hand-held Doppler is used. For example, cardiac wallmotion produces a low pulsing sound, valve closure produces a clicking sound, umbilical or placental bloodflow produces a swishing sound, and maternal arteriesproduce a whispered rumble. Since the actual heart soundis not heard, it is NOT appropriate to document “heartrate audible” when a fetal monitor is used. To hear thefetal heart beating (the ventricular rate), fetal heartsounds should be assessed by auscultation with a fetoscope or stethoscope. Fetal movement is not audible,but artificial sounds created by the monitor are oftenheard. However, rhythmic sounds in response to detecteddiaphragm movement may be heard when the fetus hashiccups.
11. Automatic gain control: Amplifies signals, increasing the sig-nal to noise ratio which improves signal detection. The USplaced over the maternal aorta detects maternal blood flowand aortic wall movement. Automatic gain control increas-es the strength of this weak signal and the MHR will be
recorded on the tracing. This has occurred in cases of fetaldemise when an US or SE was used. For example, theweak MECG signal passes through the fetal body, is ampli-fied by automatic gain control, and the MHR is printed.
Prior to application of the fetal monitor, the MHRshould be assessed and a fetal movement history shouldbe obtained. If there is a question regarding fetal life, theFHR should be determined. The FHR is best assessed byhearing the heart beat (fetoscope or stethoscope) or seeingit beat (real-time ultrasound). If a hand-held Doppler isused, the rate should be distinct from the MHR (7, 36, 42-43). If the maternal apical or radial pulse coincide withthe rate printed on the tracing, the fetus is not beingrecorded (44-45).
Fetal death should be suspected if there is no fetal movement (FM), no fetal heart tones, the recorded base-line may be less than 100 bpm, uniform accelerationsoccur with contractions (the maternal pain response) (seeFigure 1.4), and there is no acceleration following fetalscalp stimulation (45). In addition, the maternal heart rate
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
7
Figure 1.5: Maternal heart rate decelerations during contractions in a confirmed case of fetal demise.
can decelerate, and may be mistaken for a FHR pattern(see Figure 1.5). Loss of the FHR signal, e.g., the US wasover the maternal aorta, might create a small gap in thetracing, then MHR accelerations with a low baselinemight be misinterpreted as FHR decelerations (46).
12. Artifact: When US is used, gaps and dots on the tracingmay appear when the cardiac signal is undetected or tooweak to be continuously recorded. When the SE is used,artifact includes irregular lines with varying lengths, unlikethe regular lines of PVCs (see Figure 1.6). To improve sig-nal transmission, the US transducer should be reposi-tioned, coupling gel may be added or a SE may need tobe applied. Signal interference when the SE wires bumpthe vaginal wall cause artifact. This “cervical interfer-ence” may also occur when the SE is first applied or thewires are touched during a vaginal examination.
13. Monitor clock: Clocks are battery-backed. If the printoutreads “set time/date” when the monitor is plugged inand turned on, backup batteries need replacement. Reset the
clock if necessary, but consider replacing the back-up batteries as soon as possible. If each monitor’s clock isreset to the nurse’s watch, all the monitors will be set atdifferent times. Then, events noted in the nurses’ notesmay not be timed to correspond with monitor times. Thiscould create confusion as to the actual time of events. Toavoid this confusion, it is better to set one’s watch to themonitor then the monitor to one’s watch.
14. Monitoring ports: Monitors may have two or three cardioports. When only two cardio ports exist, one twin is mon-itored by US and the other by SE. If three cardio portsexist, twins may be simultaneously monitored by US.When the US and SE ports are used simultaneously, theUS tracing is often darker than the SE tracing. When twoUS ports are used, the rate detected by US 2 often printsdarker than the rate detected by US 1.
15. Maternal ECG (MECG) cable: The MHR may be calculatedwhen the MECG is detected by a two lead or three leadECG device adapted for the fetal monitor (see Figures 1.7
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
8
Figure 1.6: Artifact produced by signal loss or interference when the spiral electrode was in place. If artifact persists, it may be helpful to apply the ultrasound transducer and determine the cause of the artifact (see Table 5).
and 1.8). The MECG may be detected when a US or SE isin use in some monitors. In other monitors, the MECGcan only be detected when an US is used as the MECGcable is inserted in the SE port. Dual maternal and fetalmonitoring may be helpful when β-sympathomimetics,such as intravenous terbutaline, are administered orwhen a fetal demise is suspected. The MHR, not theMECG, and the FHR will be printed. In the case of fetaldemise, the two rates will be nearly identical (47). Whendemise is suspected, the absence of fetal cardiac motionshould be confirmed by real-time ultrasound.
Cross-channel verification™ (Hewlett-PackardM1350A®) helps identify maternal monitoring in the caseof fetal demise or dual monitoring of one twin. Cross-channel verification triggers the printing of a questionmark at the top of the FHR channel when more than onedevice, such as the MECG transducer, SE, or US detect asignal from the same source.
Figure 1.7: The maternal ECG cable detects the maternal ECG and trans-mits it to fetal monitor for analysis. The MHR will be printed on tracing.(Photographed by Barbara Gibson, Gibson Graphics, Albuquerque, NM)
Figure 1.8: Suggested placement location for three lead maternal ECGcable. The electrodes are attached and the cable is plugged into the cardioor SE port on the fetal monitor. The two active electrodes may be placed anywhere on the upper thorax. The reference electrode (ground) should beat least 12 inches from the active electrodes.
16. Twin baseline offset: Some monitors print twin heart rateson two different numeric grids. Others have a baseline offset feature that adds 20 or 30 bpm to the twinmonitored with US 1. Consult the manufacturer ’s guidelines for activation of this feature.
17. Fetal Actocardiograph: Some fetal monitors print fetalmovement on the UA channel of the paper. For example,the Toitu Fetal Actocardiograph® detects and prints fetalmovement as well as the FHR and UA (see book cover).Fetal movement is recorded as spikes at the bottom of theUA channel of the tracing. Dot marks also appearbetween the FHR and UA channels when FM speedexceeds a preset threshold.
18. Data entry devices: A keypad, keyboard, touch screen,light pen, or barcode reader have been used to enter comments on the tracing and in the nurses’ notes. Entriesappear between the FHR and UA channels on the fetalmonitor paper.
19. Peripheral equipment: An automated noninvasive bloodpressure cuff and SpO2 monitor can be built in or connected via cables to the fetal monitor. After usingthese peripheral devices, blood pressure and SpO2 shouldbe printed on the strip. If they are not printed, additionalhardware may need installation or adjustments, such asequalizing the baud rate of the fetal monitor and theperipheral equipment.
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
9
G
- +
Fetal monitors can be connected by means of cables tocomputers for data storage. When a computer system isinstalled, the tracing and documentation may be stored onoptical laser disks and the hard drive. Dual back-up disks areessential. As many as 10,000 records may be stored on a 20megabyte hard drive (48). It is important to confirm thewoman’s tracing is actually stored as loose cable connectionsmay result in storage of another woman’s data. When tracings are stored on disk, all entries must be made usingthe data entry system as handwritten remarks are not stored.
Fetal monitors may store FHR and UA information. TheAMS IM-77® (Advanced Medical Systems, Hamden, CT)stores approximately 60 minutes of strip data in its memoryif the paper ends (out of paper memory™). Once new paperis placed in the paper tray, the stored information should beprinted at a rapid rate until the strip catches up with the current data.
Data from fetal monitors may also be transmitted by amodem or telemetry (49). Modems utilize telephone lines totransmit data to a personal computer (PC) or a fax machine.Data can be stored for later transmission. For example, 100minutes of stored data can be transferred in 10 minutes. Or,real-time data can be transmitted. Some receivers can accommodate multiple transmissions.
Telemetry is a wireless system that transmits data fromone location to another. In 1979, telemetry was being createdand was considered a promising line of development in 1987(24, 50). A telemetry unit which transmits radio waves maybe carried like a shoulder bag by the pregnant woman.Transducer cables are plugged into this unit. Its receiver isplugged into the back of the fetal monitor. Telemetry allowscontinuous recording of FHR and UA data when the womanis out of bed away from the monitor. In the future, fetal monitors may have different forms of telemetry. For example,Advanced Medical Systems (Hamden, CT) is seeking FDAapproval for a fetal monitor with cableless toco and US transducers that transmit signals to the fetal monitor by electromagnetic waves.
COMPUTER APPLICATIONS IN OBSTETRICSInitially, computers were used in hospitals for patient admis-sions, billing, and management reporting. The first computersystems designed for obstetrics were introduced in the mid-1980s. These systems were PC based and capable of transmis-sion, archival and retrieval of maternal and fetal data.Electronic fetal monitor signals were captured, digitized, and stored within the computer’s memory. Thebest computer systems can simultaneously record FHR andUA information and:• display the tracing on a computer screen• send it to another PC via modem • print the tracing on a computer printer and• store the information on a hard drive and laser optical
disks. Some computer systems are capable of:• central display at the nurses’ station
• remote display in hospital rooms, hallways, and lounges• central and remote alarm systems• electronic point-of-care charting • interconnections to other biomedical devices such as a
blood pressure monitor• data retrieval and statistical report generation, and• networking with other computer systems such as the
“housewide” financial system.
Central and Remote Display FunctionsBusy units may benefit from access to all fetal monitor tracings on one or more computer screens located at the nurses’ station. The charge nurse’s accountability expands asthe number of displayed tracings increases.
Optical Disk ArchivingStorage of UA and FHR data on a computer disk should savespace and time. Fetal monitor strips may be discarded andretrieval of tracings from the computer is faster than searching for microfilm in the medical records department.Some hospitals continue to microfilm the tracing prior to discard. This provides an exact copy of the tracing.
Computer-generated tracings are close facsimiles, notexact copies. In 1990, computerized systems were consideredinvestigational and no final legal status of computer-archivedtracings existed (51). Since 1990, however, they appear tohave been accepted in medical malpractice cases.
To safeguard against loss or damage to one optical diskcartridge, dual optical disk storage should be installed.Computer systems can be installed with an electronicallycontrolled security system to protect data from tampering orremoval. Risk managers may prefer an optical disk storagesystem in which the strip is automatically archived and nostrip review is allowed.
Point-of-Care DocumentationComputer systems have been designed to eliminate redundant charting. One entry can be sent to multiple places,a “single entry-multiple result” design. Documentation speedmay be enhanced by use of a pen light and software with aGraphical User Interface (GUI) capable of point and clickdata entry. Data entry options may include a keyboard,mouse, trackball, touch screen, and light pen.
Computer software documentation programs shouldreflect expert clinician input and provide data entry optionsin all areas health care providers currently chart. For example, they should allow entries that reflect assessmentssuch as the FHR baseline, short-term variability (STV), long-term variability (LTV), accelerations, decelerations, uterinecontraction frequency, duration, intensity, peak intrauterinepressure (IUP), and relaxation or resting tone. The number ofcomputers should be adequate to meet personnel needs andprevent documentation delays. Computer-generated documents should be easy to retrieve and read.
When changing from a paper documentation system to acomputerized system, success depends on having enough
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
10
computer workstations at each charting location. Success alsorequires the nurse manager’s commitment to the change.User comfort with technology and a positive approach tochange will increase acceptance of the new computerizedsystem. Change requires a clear implementation plan and aquality assurance process that provides continuous feedbackto staff. Everyone involved in the change should be patient,persistent, and open-minded. No other major changes should becompeting for attention.
Data Retrieval: Reports and StatisticsThe quantity and quality of retrieved data depends on thequantity and quality of data entered. If data entry is deficient,some say, “Garbage in, garbage out.” Therefore, to ensureexcellent reports, it is critical to determine who will enterdata prior to purchase of a point-of-care charting module.Data entry tasks will be a major part of their job. Data may becollected for unit statistics, patient reports, and customizablereports. Reports that once took several days or weeks to gen-erate can be generated in a few minutes. Some vendors donot offer a customizable report option.
Remote Access, Communications, and NetworkingData from the strip alone or the entire chart may be retrievedby midwives or physicians in their offices or homes or sentfrom community-based hospitals to tertiary centers. The
physician or clinic may purchase a system by which the prenatal record is computerized and transmitted to labor anddelivery or the antepartal unit via a modem.
Purchase of a Computer SystemMany options are available for a comprehensive obstetricalinformation management system (see Figure 1.9). One ormore of these options can be purchased. Some central displaysystems are not expandable. In other words, the central system “black box” technology is not upgradable or capableof being connected to other computer systems. Therefore,prior to purchase, costs and benefits as well as enhancementcapabilities of each component of the system should be considered.
Prior to purchase, a computer system selection committeeshould perform a needs assessment. The committee shouldconsist of the following people: the medical and nursingdirectors of perinatal services, antenatal and intrapartal unitnurse managers, clinical nurse specialists, the medicalrecords department director, an information systems representative, and the risk manager. Issues to be discussedby the sales representative and this committee should includethe computer system’s ease of use, system flexibility, documentation capabilities, future software developmentplans, and configuration requirements to meet everyone’sneeds.
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
11
Figure 1.9: The steps to successful obstetrical information management (©1995 Peritronics Medical, Inc., reproduced with permission). The bottom two stepsare the basic requirements of an obstetric computer system.
CCOOMMPPLLEETTEELLYY EELLEECCTTRROONNIICCPPAATTIIEENNTT CCHHAARRTT
NNEETTWWOORRKKIINNGG WWIITTHH HHOOSSPPIITTAALLCCOOMMPPUUTTEERR SSYYSSTTEEMMSS
PPAATTIIEENNTT RREEPPOORRTTSS//SSTTAATTIISSTTIICCSS
AARRCCHHIIVVIINNGG SSTTRRIIPPSS WWIITTHH NNOOTTEESS
AARRCCHHIIVVIINNGG FFEETTAALL MMOONNIITTOORR SSTTRRIIPPSS
CCEENNTTRRAALL SSUURRVVEEIILLLLAANNCCEE,, RREEMMOOTTEE DDIISSPPLLAAYY AANNDD AALLEERRTTSS
Prior to purchase of a computer system, the committeeshould answer the following questions:1. Is a central display system critical?2. Are remote display functions needed and if so, to what
extent?3. Is bed to bed surveillance needed?4. Is an alert/alarm function needed and if so, is it
customizable for each patient?5. Is optical disk archiving a significant advantage or is the
current EFM strip storage system adequate?6. Is the system sold by a stable company who has been in
business for some time?7. Who will perform data entry?8. Which data entry tasks would provide the greatest return
on the investment?9. What peripheral devices for data collection will be
connected to the system?10. Does the system support connection to different fetal
monitors?11. What data needs to be stored, reviewed, and retrieved?12. Does the system support user-configurable report
writing?13. What technology standards does the system have?14. Is the system’s technology compatible with the hospital’s
strategic plan and future?15. Does the system allow for growth and flexibility as future
needs change?16. Does the vendor have experience implementing a
successful computerized documentation system?17. Can you interview others who have succeeded in the
areas you are interested in?18. What support will be required to implement the system?19. What support will be needed on an ongoing basis?20. What support/training services does the company offer
after installation? 21. Will the vendor provide training and support, and if so,
at what cost?22. What level of customization will be needed and who will
be responsible for customization, the hospital or the vendor?
23. Will it be necessary to hire or train a full time specialistfor internal support and training of the personnel whowill use the computer system?
If all these issues are considered prior to purchase, computer systems should not be a source of frustration ordisappointment. The budget should be adequate to cover theentire system required, including an adequate warranty provision and support services such as training of employeesin the use of the system. Software may be very minimal andrequire extensive set-up and customization prior to use. Or,the data storage procedures will require tedious manualprocesses for backup and quality control. These indirect costscould be the burden of the obstetric department. Therefore,to avoid indirect costs, a realistic budget should be determined with the vendor prior to purchase.
Implementation of a Comprehensive OB Computer SystemChanging to a computer-based documentation system from apaper system is a major event. The process may take morethan a year. Adaptation to this change may be slow.
If the hospital wishes to change to bedside/point-of-carecharting, staff may find it difficult to change if they are notaccustomed to documenting at the bedside. Hospitals shouldlook for a vendor that develops a long term partnership towork with the staff to facilitate this change.
Each component of the computer system should beimplemented, evaluated, and deemed successful prior toinstallation of the next component. A quality assuranceprocess should be in place to identify problems and areas forfurther training or system modifications. A forced or rapidchange may create resentment or antagonism towards theprocess, and the project could fail. The department managerwill need to be a coach and a leader with the patience to dealwith minor and major obstacles in the change process.Commitment is required for success.
ANALYSIS OF THE FHRVisual Analysis of the FHR PatternAgreement between nurses and physicians in the meaning ofFHR and UA patterns is critical when the fetus is sufferingfrom hypoxia, acidosis, or asphyxia or the woman has abnormal uterine activity as the result of a placental abrup-tion or uterine rupture. If the fetus is healthy, disagreements areof little consequence. However, if the fetus is not, disagreementsmay result in a treatment delay, fetal damage, fetal death, or mater-nal death. Fortunately, nurses have a high rate of agreement intheir interpretations of nonstress tests (NST) as reactive or nonreactive. Four hundred and twelve nurses agreed 84 to 98percent of the time when they reviewed 5 NST strips (52). Afailure to agree that the NST is nonreactive could precedeinaction and fetal demise or the birth of a neonate with a sig-nificant risk for low Apgar scores, neonatal intensive careunit admission, or death (53). Physicians and nurses rarely experience total agreement with themselves when they take asecond or third look at a tracing (intraobserver agreement) orwhen their interpretations are compared to each others’ interpretations (interobserver agreement). Disagreementslimit the predictive value of fetal monitoring and reflect different training and experiences (54-55).
Nurses and physicians may agree more often with theirown interpretation than the interpretation of others (56).Some people agree with themselves less then they agree withothers. For example, agreement with oneself occurred 22 percent of the time when obstetricians, perinatologists, andnurses took a second look at NST and labor strips. But, theyagreed with each others’ interpretation 42 to 55 percent of thetime (57-58). Scoring systems may heighten agreement, buttheir use assumes the definitions and descriptions of FHRcomponents are understood and accepted by the individualsusing the system (59). One would think attendance by physicians and nurses at the same fetal monitoring
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
12
educational seminars would heighten agreement. Yet, evenwhen fetal monitoring education occurred within one hospital, differences in opinions persisted (56).
Even nurses and physicians, who considered themselvesexperts in fetal monitor strip interpretation, disagreed witheach other’s pattern interpretation. When 5 obstetriciansreviewed 150 labor strips, all 5 only agreed on 44 of 150 tracings (29 percent) (60). When 8 nurse experts reviewed 45FHR patterns, they only agreed on 25 of the 45 tracings (56percent). Agreement was defined as consensus between 3 ormore nurses. When 20 of 25 agreed upon tracings were randomly selected for review, the 8 nurse experts agreed 100percent of the time on some, but not all, of the FHR patterncomponents. In one strip, there was only 54 percent agreement on the type of deceleration that was present (61-62). In Denmark, physician residents agreed the decelerationwas a late deceleration or a variable deceleration less than 56percent of the time (63).
Barriers to deceleration recognition include insufficient orerroneous recognition criteria or a limited mental image tocompare with newly encountered examples (61).Recognition criteria help people see an image imbedded in afield. The field is the grid on the fetal monitor paper. Theimage may be the FHR baseline, STV, LTV, accelerations, ordecelerations. A failure to learn appropriate recognition criteria could limit recognition skills.
Images in one’s mind are called prototypes. Limitedexposure to the various deceleration types and multipleexamples of each type of deceleration limits the recognitionof other decelerations in that category. Variable decelerationsoccur more often than late decelerations. Therefore, some latedecelerations may not be recognized if there is limited prototype development. As more images are recognized,based on recognition criteria, prototypes become moreabstract. A highly abstracted prototype increases imagerecognition.
Interpretation accuracy increases when the number ofexamples on a tracing increases and the number of peopleexamining the tracing increases. For example, accuracy interpreting a 55 to 70 minute UA strip generated by a tocodecreased when contractions lasted less than 40 seconds andwere fewer than 4 per hour. One observer was only accuratein their assessment 70 percent of the time, 2 were accurate 82percent of the time, and 3 were accurate 88 percent of thetime (55).
Appropriate actions should be the response to accurateinterpretation. Computer analysis of FHR data should diminish incorrect and inconsistent interpretations. But, clinical judgment will still be required to determine management strategies. The product of computer analysis is asummary of FHR and UA data, not a conclusion or plan ofaction. Many physicians have been working to refine softwareprograms for FHR and UA pattern analysis. They believe FHRpatterns are too complex for some users to interpret in a reli-able, consistent or accurate way and that computer softwareincreases the accuracy of FHR pattern analysis (40, 54, 64-66).
Computer Analysis of FHR Patterns The fetal monitor transmits its data via a digital parallel portand cable to a PC for analysis (64). Software programs havebeen developed to identify components of the FHR patternand UA. When a SE is on the fetus, the FECG is transmitted intothe fetal monitor and transferred to the PC. R waves on theFECG waveform reflect the heart beat or systole. The computer determines a bpm rate based on one R to R orpulse interval. For example, if the pulse interval were ¹⁄₂second or 500 milliseconds (msec), the minute rate would be120 bpm.
The computer calculates STV by identifying the msec differences between two consecutive pulse intervals. LTV iscalculated by adding 30 to 60 seconds of pulse intervals (67-68). The baseline rate is computed after 5 minutes of pulseintervals are analyzed (69). When a computer was used toanalyze the FHR pattern, benefits included:
1. constant fetal surveillance2. assistance in interpretation for inexperienced staff 3. multiple variables that set off an alarm 4. standardized interpretation5. data storage, analysis, interpretation, recall, and
display at any time and 6. data retrieval for research or legal purposes (48, 51, 69).
Researchers developed an experimental program withartificial intelligence that analyzed the FHR and UA patternsduring antepartal testing and labor. The program made adiagnosis, prognosis, and recommended actions based on thefindings, such as “repeat the test in standard conditions…”.Prior to labor, the program was used to determine theBishop’s score and labor favorability. The program also predicted morbidity. During labor, the program evaluatedFHR and UA patterns, and labor progress. Diagnoses weremade as well as suggestions for management, such as achange in maternal position, fetal blood sampling, or maternal oxygen administration. The application of artificialintelligence techniques used in this program depended ondata entry and the procedural and informational knowledgeprogrammed into the software. While this type of programmight be helpful to retrospectively evaluate antepartal tests orlabor tracings and management, its applicability in a clinicalsetting may be hampered by a lack of data entry personneland high speed computers. In addition, physicians did notalways agree with the computer analysis of the tracing.Agreement between physician analysis and management andcomputer analysis and management varied between 71 to 85percent (70).
Preliminary research in 1976 compared physician andcomputer analyses of tracings generated by a SE. There was91 percent agreement between physician interpretation andcomputer analysis (69). Early problems with computer analysis included the lack of a precise formula to recognizecontractions or to identify deceleration types. Plus, therewere faulty alarms and a failure to evaluate some decelerations. The analysis of FHR data has challenged
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
13
software developers (51). By 1990, software algorithms weremore consistent in how the FHR was calculated but someresearchers were still developing algorithms (64). Today,computer software analyzes the FHR and UA patternswhether or not external (US and toco) or internal (IUPC and SE)devices are used. Computer analysis of the FHR pattern generated by US yielded similar results as the computeranalysis of the tracing generated by SE, except in the measurement of STV.
The Sonicaid system 8000® is a PC-based computer program that was developed in the United Kingdom to analyze the FHR and UA. Once analyzed, the following variables were printed:• baseline or basal (BL) FHR • variation of the baseline• time spent in high variation (24 or more msec)• time spent in low variation (less than 24 msec)• fetal movement (FM) recorded by the woman or her
nurse• uterine contractions (UCs)• accelerations that lasted more than 15 seconds and
peaked 10 or more bpm above the baseline and• decelerations dropping 10 or more bpm below the base-
line lasting 1 or more minutes or dropping 20 bpm belowthe baseline lasting more than 30 seconds (1, 51).
This automated FHR and UA analysis works best with anear term fetus when the woman is not in labor. Duringlabor, signal loss limits data acquisition. Software was programmed based on known changes in the FHR duringdifferent fetal behavioral states. A minimum of 45 minutes ofmonitoring is required if there are no episodes of high variation or accelerations (71).
Both LTV and STV are determined after each minute ofpulse intervals is analyzed for a minimum of five minutes(48). The minimum and maximum pulse intervals determined during the five minutes become the bottom andtop of the FHR baseline range.
Long-term variation is determined each minute by addingthat minute’s pulse interval differences. The lower normal limitfor LTV is 30 msec/minute (72-73). Twenty to 30 msec/minute isquestionable. Less than 20 msec/minute is considered abnormal (72).“Decreased variation” best predicted acidemia, acidosis, and deathin the post-term fetus (6, 74). Nine of 10 fetuses withdecreased variation during antepartal testing had “fetal dis-tress” during labor. Seven of 12 with decreased variation dur-ing labor had acidemic cord artery pH values (74).
STV is calculated as the average pulse interval over a1/16 minute (3.75 seconds) epoch. After each epoch, it wasexpected that the average pulse interval would vary slightlyand create a small difference in each consecutive calculatedrate. Fifty percent of consecutive rate differences wereapproximately 1 bpm when an abdominal FECG was used tocalculate the FHR (75).
STV was determined with an US transducer in place. FHRpatterns when an US is used to detect the FHR may look
smoother than FHR patterns when a SE is used because autocorrelation averages pulse intervals over 0.5 to 1.2 sec-onds (3, 27, 76-79). Using US technology, pulse interval differences for normoxic fetuses were 3 or more msec. A pulseinterval difference of 4.17 msec creates one bpm changebetween consecutive rates. Pulse interval differences less than2.6 msec were associated with acidemia, and less than 2 msec wereassociated with fetal death in less than 24 hours in 7 fetuses.Decelerations detected by computer analysis were also a warning ofimpending death (6).
Bernardes and Pereira (65) hoped both visual and com-puter analysis would be complementary and enhance thedetection of acidotic fetuses during labor. Unfortunately,labor was associated with FHR signal loss where no validpulse intervals could be obtained for analysis (66). Signal losswas also more common in premature gestations and obesewomen (36).
Computer analysis of FHR patterns and FM yielded newdata about variation, accelerations, and fetal behavior. Forexample, the average baseline FHR at 20 weeks was 149 bpmand 134 bpm at term (5). This indicates the vagus becomesmore dominant as gestation advances. The baseline slowlydrops between 24 and 30 weeks’ gestation (68).
Low variation lasted up to 40 minutes near term and wasoften associated with a quiescent fetal sleep state (5, 68, 80).The amount of time spent in high variation increased as gestation progressed. The number of accelerations significantly increased between 20 to 41 weeks’ gestation (5,81-82). Thirteen percent of 20 to 30 week fetuses did notaccelerate within a 60 minute observation period. “One bigdeceleration” occurred in 7 percent of fetuses 20 to 37 weeks’gestation. Between 30 and 41 weeks, fetal rest and activityepisodes lengthened and became more distinct (5).
Visual and Computer AnalysisVisual interpretation of the FHR pattern is subjective andrequires identification of the FHR baseline, its variability(STV and LTV), accelerations, decelerations, arrhythmias,and artifact. The UA pattern may be analyzed for frequency,duration, intensity, peak IUP, and relaxation or resting tone.Pattern analysis is coupled with clinical observations or teststo determine the meaning of the pattern.
Computer software programs that analyze tracings havebeen developed in countries such as the United Kingdom,Portugal, Italy, and the United States of America (26, 64, 83-84). Computer analysis of the FHR and UA is objective butlimited as it does not factor in clinical observations (68, 73).Therefore, computer analysis is best used as an adjunct toclinical observations and decision making.
Visual analysis is qualitative; computer analysis is quantitative (85-86). Some felt the computer was “superior” inits analysis (87). Computer analysis is different than visualanalysis. Therefore, comparing computer and visual analysisis synonymous with comparing apples to oranges. Therefore,any research that does so is open to criticism. It would be better to compare fetal outcomes, not tracing interpretations.
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
14
Humans and computers are similar in their ability toidentify well fetuses who have normal birth outcomes (87).Sometimes the computer was more sensitive than humans to abnormal findings, but predicted well babies the same. Forexample, in a 1993 study, 93 percent of reactive tracings byvisual analysis met the computer’s requirements for reactive(88). The computer found 13 abnormal results that thereviewers felt were normal (73). This suggested visual analysis might miss an abnormal FHR pattern. On the otherhand, the FHR pattern may have had low LTV and representeda fetus in a quiet sleep state rather than a hypoxic fetus.
Sometimes physicians were more sensitive than the computer toabnormal findings. When three physicians evaluated 148 NSTstrips, they found 17 to 19 were nonreactive. The computerfound 14 were nonreactive. For the computer to identify thetracing as reactive, there had to be at least one FM or threeaccelerations and five of six minutes had to have high FHRvariation and no large deceleration (72). The difference in“reactive” criteria partially explains different interpretationsby the physicians and the computer.
Perinatal nurses and perinatologists reviewed NST strips,
and for the most part they agreed with the computer ’s determination of the baseline rate (89). In another study,there was 82 percent agreement between visual and computeranalysis of the baseline of 158 tracings, but less agreementwith the number and duration of contractions, the number ofaccelerations, the number of decelerations, and the timebetween contractions and decelerations (83). Escarena (90)found physicians and the computer had poor agreement onSTV. However, the computer used different criteria to assessSTV than the physicians.
MONITOR START-UP and DISCONTINUANCEPrior to using the electronic fetal monitor, inspect the powercord. If it is damaged, don’t use it. Inspect the transducercables for missing pins or loose wires. The lack of pins orloose wires may interrupt or diminish signal transmission.Damaged cables should not be used.
In case of an electrical outage, the fetal monitor should bedisconnected from its power source until power is restored.However, even if a fetus were attached to a SE and the monitorwere plugged in when power was restored, it is not possible that a
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
15
Figure 1.10: Some monitors run an automatic test of the electronic circuitry, printer, and paper feed. If a gap exists between the printed line and the papergrid line, the paper may need to be adjusted in the paper tray or the printer may need to be adjusted by a skilled technician.
power surge would override the surge protector in the fetalmonitor, travel down the SE cable, through the SE wires to thefetus resulting in electrocution because the manufacturers havetaken all precautions necessay to prevent direct current transferto the fetus.
Equipment should be working properly prior to its use.When the monitor is plugged in, it may automatically gothrough an electronic test. A manual test of the fetal monitorcircuitry could be performed at any time during monitor useby pressing the test button. Some monitors require transducersand the telemetry receiver be unplugged from the monitor when it is undergoing the initial self test. It is a goodhabit to test the monitor and its transducers prior to use. If atest strip is generated, it should remain part of the permanent medical record.
To test the connection between the fetal monitor and itscomponent devices, e.g., the toco and the US, turn the monitor on after transducers are connected. If two ultrasounds are to be used for monitoring twins, plug in oneUS at a time. Press the test button. A digital readout on thefetal monitor FHR and UA screens should appear while the printer prints lines on the UA and FHR channels. Anauditory signal should be heard at the same rate as thatprinted in the FHR channel. Examine the lines of the test pat-tern to ensure the printing is clear and consistent (see Figure1.10). If there are gaps between the printed lines and thepaper grid, reposition the paper in the paper tray and retest.If the gaps persist or the lines contain gaps or are too dark ortoo light, the monitor should be sent for printer repair oradjustment. Some monitors display an error message on thedigital readout when equipment malfunctions. Peripheraldevices, such as a barcode reader, may be tested using a bar-code sheet.
A continuous line or squares printed on the paper indicates the paper end is approaching, often with less than30 minutes remaining when a 3 cm/minute paper speed isused. If these lines are present prior to beginning monitoring,remove the old paper and add new paper to the tray.
THE TOCOTRANSDUCER: INDIRECT/EXTERNAL UTERINE MONITORINGThe most common external monitoring devices are the uter-ine tocodynamometer or tocotransducer (toco) and the ultra-sound transducer (US). “Toco” is similar to the Greek word“tokos” meaning childbirth. Uterine activity will be recordedon the lower portion of the tracing in the UA channel. Sincethis is an external device that rests on the abdomen, mm Hgor kPa units are not used in the analysis of the UA pattern.Instead, the waveform is examined for its shape.
The Tocodynamometer Mechanism In the near term woman, the toco should be placed on theupper third of the abdomen. In the preterm gestation, itshould be placed below the umbilicus (91). During a uterinecontraction (UC), the uterus becomes more convex androtates to the anterior abdominal wall. The traditional
guard-ring tocos contain a strain gauge in the form of a piston held in place by a metal ring. Pressure from theabdomen is exerted on the piston. The piston bends a metalstrip which activates a Wheatstone bridge that convertsmechanical energy to electrical energy for transmission intothe fetal monitor (91). Another type of toco contains a pressure-sensitive piezoelectric computer chip connected to aWheatstone bridge. Voltage transmitted from the Wheatstonebridge into the fetal monitor is amplified by automatic gaincontrol prior to determination of the relative frequency, duration, intensity, and relaxation of contractions. A UAwaveform will be printed on the tracing (92, 93).
Guard-ring tocos have been used for ambulatory pretermUA monitoring (94). Some home UA monitors store up to aweek of UA data (95). Tocos used in the hospital may beinsensitive to preterm UA. Other tocos may be set at differentsensitivities for the preterm and term woman. If the tocotransducer is not highly sensitive, preterm labor contractions may not be recorded. To improve recognition ofpreterm UA, a highly sensitive toco should be used, and thefeelings and complaints of women should be consideredwhen the nurse or physician palpates the abdomen.
Some women complained they were in preterm labor, butwere not contracting at all! Contractions appeared to berecorded on the paper, but they were created by the womanwhen she pressed on the toco or pushed out her abdomen(96). Woman-made UA patterns have UC waveforms thatlook more square then curved. Women who feign labor mayhave Munchausen Syndrome. In the case of suspectedMunchausen Syndrome, a hand should be placed under thewoman’s lower back with another hand near the toco on theabdomen to prevent touching of the toco by the woman. UAis palpated while a psychosocial history is obtained. The trac-ing should be evaluated during the woman’s sleep times.Women with Munchausen Syndrome cannot push the toco toregister false contractions when they sleep.
Testing the TocotransducerTo test the tocotransducer, plug the cable into its port on thefetal monitor, turn on the monitor, then press the toco’s pressure-sensitive surface. Observe the digital readout on themonitor screen. The pressure should increase and be recorded at the top of the UA channel.
Setting the UA BaselineSome tocos automatically set the UA baseline at zero, whileothers need to be manually set to a UA level of 10 units. Aslong as UA is recorded in the UA channel, and the beginningand end of the UA waveform are visible, the toco baselinecan be placed at any level. Of course, it is preferable to seethe entire UA waveform which is most common when the baseline is set near 10 units.
Analysis of UAContractions look like hills that last 30 or more seconds in theUA channel. Each contraction has an ascending limb, acme or
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
16
peak, and descending limb or decrement reflecting the relative onset, peak, and offset of the contraction. When thetoco is used, the recorded waveform reflects pressure exerted bythe abdomen in the area under the toco which can be altered bythe location of the toco, maternal activity such as turning tothe side, or by adjusting the UA dial or button.
External UA monitoring with a toco provides qualitative notquantitative information. The assessment of UA by a toco wasfairly reliable for UC frequency, less reliable for UC duration, andnot reliable for peak pressures and resting tone (97). The recordedUC peaks depend upon the thickness of subcutaneous tissue,belt tightness, position of the toco on the abdomen, andmaternal position.
Maternal position is an important assessment that shouldbe recorded in the nurses’ notes. A supine position might create supine hypotension and reduce uterine blood flow dueto compression of the great vessels. The resulting uterinehypoxemia may precede weak, frequent contractions. Alateral position increases uterine blood flow, and may reduceUC frequency, but increase contraction duration and intensity (98).
When women bear down or hold their breath, theirabdomen becomes distended and the contraction waveformextends past the actual contraction duration. This false duration may prevent some physicians and nurses fromacknowledging the presence of late decelerations. Whilelate decelerations return to the baseline after contractionsend, when a toco is used, the exact end of a UC is unknown.Therefore, this recognition criteria for a late deceleration isthe least significant when a toco is in place. Decelerationsare identified first by their shape, then by their timing inrelation to contractions. The timing alone does not deter-mine the name given to the observed deceleration. If clarifi-cation of the deceleration pattern is needed, exactmeasurements of IUP can be obtained after an IUPC isinserted into the uterus (92-93).
Contractions are usually palpable and will be recordedprior to the woman’s awareness of the onset of the contraction.The woman’s coach can be instructed to identify the ascendinglimb of the contraction to help prepare the woman to copewith the contraction. Recorded UA is relative when a toco is used,therefore it is essential to palpate the woman’s abdomen andlisten to her subjective viewpoint to confirm UC duration,intensity, and relaxation. The uterus should be soft betweencontractions for at least 60 seconds. Women’s subjective complaints, coupled with a review of the UA pattern, maysuggest placental abruption. For example, contractions every 1 ¹⁄₂ to 2 minutes experienced by a restless and screamingwoman who is requesting removal of transducer belts hasbeen associated with abruption of the placenta.
EXTERNAL FHR MONITORING DEVICESFour devices detect the FHR: the phonocardiotransducer, anabdominal wall electrocardiogram (indirect FECG), the ultra-sound transducer, and the SE (direct FECG) (see Figure 1.11).
PhonocardiographyPhonocardiography was first used in 1908, and was availablewith the first clinically useful fetal monitor. However, it israrely used in clinical practice. A microphone placed on theabdomen detects harmonic content of fetal heart soundsbetween 75 and 107 Hz. It also detects ambient noises. Soundtriggers a cardiotachometer for determination of the FHR.Detection of heart sounds is hampered by excessive abdominal wall movement during contractions (99-100).Signal clarity is also affected by abdominal wall thickness,the quantity of amniotic fluid, and maternal and fetal position (2, 100). Because the actual beat of the heart duringsystole is determined, this device can be used to measureSTV (2,99).
Abdominal Wall Fetal ECG (aFECG)The fetal ECG (FECG) may be transmitted into the fetal monitor by a spiral electrode applied directly under the fetalskin. This is a direct ECG assessment and is abbreviatedDECG. The FECG may also be detected by electrodes appliedto the maternal abdomen, an indirect assessment of both thematernal and fetal ECGs. This indirect FECG assessment isabbreviated aFECG.
The first recorded aFECG occurred in 1906. Abdominalelectrodes were placed over the uterine fundus and an electrode was placed in the vagina. This technique has beenused to diagnose twins, fetal life, fetal position, and congenitalheart defects (99). The technique is rarely used in clinicalpractice (101). Abdominal FECG electrodes may be noninvasiveor invasive, i.e., three to six electrodes have been appliedmidline on the abdomen or three platinum electrodes havebeen inserted subcutaneously in the anterior abdominal wall(102-103). The FECG is analyzed by an abdominal electrocar-diogram processor. The FHR can be calculated by a computerand printed on a computer screen.
The aFECG detects the FECG and MECG complexes andtransmits them into the processor. The FECG is hidden in asea of electrical noise. To extract the signal, a filter and averaging and subtraction of the MECG or substitution of theFECG have been used (2, 100, 104). The FECG is difficult todetect because it is often distorted and 2 to 10 times smallerthan the MECG (99, 105-106). In addition, maternal skin has ahigh impedance, which diminishes signal detection (106).
When the MECG and FECG coincide, an averaging orsubstitution technique can be used to detect or replace theundetected FECG complex (107-108). If an averaging technique is used, an averaged MECG waveform is subtractedfrom the entire signal (109). This enables detection of all fetalQRS complexes, even if they coincide with MECG complexes.With pulse substitution, a FECG complex is entered when itshould have occurred. This artificial signal reconstructionmay lose any ectopic beats, such as premature ventricularcontractions. Actual and substituted pulse intervals havebeen compared and were within 0 to 10 msec 98.5 percent of the time (101).
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
17
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
18
Figure 1.11: Techniques for fetal heart rate measurement. (Reproduced with permission of Marshall Klavan, MD: Clinical Concepts of Fetal Heart RateMonitoring. Hewlett-Packard Company, 1977).
Automatic gain control constantly searches for a fetal signal to amplify. Automatic gain control increases instrength until it finds a signal and it shuts down when excessive electrical noise exists. In the absence of fetal life, itwill amplify the MECG. Since R waves trigger the cardiota-chometer, absence of a FECG would allow the MECG to trigger the cardiotachometer (97).
Once the FECG is detected and amplified, it is filteredand converted to a digital signal. The digital signal is filtered,and might be modified by averaging or substitution. Then,the refined ECG waveform is stored in memory, a rate is calculated, and the ECG may be plotted on ECG paper mov-ing at 25 mm/second or the FECG and FHR may appear on acomputer screen (101, 105-106, 110).
aFECG Reliability In 1994, researchers reported as many as 35 percent of FECGsignals were weak, not detected, or unsuitable for analysis(103). Signal strength varies with different electrodes anddecreases during contractions and pushing. While phonocar-diography provides a reliable signal to detect STV, aFECGmay be less reliable due to signal averaging and/or substitution. When the FECG was substituted, STV was notexactly the same as when the FECG was transmitted by theSE. However, STV calculated by aFECG versus a SE was verysimilar (r = 0.83 ± 0.08). LTV was also similar between theaFECG and SE (r = 0.95 ± 0.02) (111). In spite of this limitation, STV calculated by aFECG predicted 12 of 17 casesof “fetal distress” (112). As technology advances, and software improves, it may be possible to use aFECG to detectSTV during labor (78). Until then, the US and SE will continueto be the most common devices used to detect the FHR.
Gestational Age. Gestational age and position of thefetus, placenta, and woman decrease FECG transmission andresult in a 35 percent or greater signal loss (99, 103). TheFECG was detected only 50 to 80 percent of the time between28 and 34 weeks’ gestation, possibly due to the thick vernixcaseosa on the fetus (1, 101). The best signals, and thereforethe most accurate tracings, were obtained antepartally fromfetuses 36 or more weeks’ gestation who were in a cephalicpresentation with electrodes placed midline above the symphysis pubis over the uterus and at the height of theuterine fundus (103,107).
Electrical Noise. The use of an aFECG during labor isnearly nonexistent, as an accurate, clear tracing is difficult toobtain (99, 107). The best results are obtained after epiduralanesthesia (107). Maternal exertion during labor generateselectromyographic interference or noise. In addition, electrical “noise” is created by the MECG, the abdominalmuscles, the uterus, and equipment (100, 106).
Fetal and Maternal Position. Fetal postural changes alterthe FECG configuration (99). The best FECG signal wasobtained with the woman supine or at a 15 degree lateral tilt.
A dry cup electrode poorly transmitted the FECG signal; anelectrode moistened with ECG paste was better (113).
T/QRS RatioIn 1969, Dr. Edward Hon suggested changes in the P waveand ST segment duration in the FECG waveform mightreflect asphyxia (99). Some believe the ST segment and T wave change prior to heart failure (114). To study FECGchanges related to myocardial hypoxia and acidemia,researchers have developed equipment that analyzes theFECG, the ST segment, and the T/QRS ratio. The FECG isaltered when the fetus becomes metabolically acidotic andthe heart becomes depleted of glycogen and creatine-phos-phate, plasma lactate, and epinephrine (from the adrenalglands) increase (103). As the pH drops, the PR interval decreas-es and the pulse interval increases resulting in a decreased FHR.The fetal T/QRS ratio is fairly stable during labor. Withacidemia and a drop in the pH, the T wave increases and theT/QRS ratio increases.
Figure 1.12: ECG schematic indicating T and QRS height used to calculateT/QRS ratio.
Researchers hoped the fetal T/QRS ratio could be used torule out metabolic acidosis and reduce unnecessary cesareansections or forceps without adversely affecting neonatal outcome (103). The STAN® fetal monitor (ST Analyzer,Cinventa AB, Sweden) is a conventional fetal monitor thatplots the ST analysis alongside the FHR pattern. The STAN®monitor also prints a representation of an averaged FECGevery two minutes on the fetal monitor paper. AdvancedMedical Systems (Hamden, CT) monitors plot the ST segment or a FECG above the FHR pattern when the ECGplot is activated. In Figure 1.13, the tocotransducer is off (UA:out). The FHR is being monitored by a spiral electrode (HR1:ECG). The monitor has another cardio port (HR2: US) whichis not in use.
Occasionally the S wave, not the R wave, becomes thecounting trigger which creates a false high T/QRS ratio. Ahigh T/QRS ratio is greater than 0.28 or 28 percent. In onestudy, a high T/QRS ratio predicted a low umbilical cord pH(< 7.12) twice as often as an abnormal FHR pattern (103).Conversely, a high T/QRS ratio detected fewer acidemic
Fetal and Maternal Monitoring Equipment
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
19
P
QRS Height
QS
TT Wave height
R
Isoelectric line
fetuses than an abnormal FHR pattern (115). Others found norelationship between the T/QRS ratio and an abnormal FHRpattern (116). So far it appears that the relationship betweenthe fetal ST waveform, T/QRS ratio, the FHR pattern, andApgar scores is unclear (103). Additional prospective ran-domized controlled trials are needed before the T/QRS ratiobecomes useful information in clinical practice.
THE ULTRASOUND TRANSDUCER:INDIRECT/EXTERNAL FHR and FM MONITORING Ultrasound was created for submarine detection (117).Ultrasonography was first used in obstetrics in Scotland inthe 1950s. By 1964, the first inexpensive Doppler instrumentfor detecting the human FHR was described (99). In 1968,fetal monitors with US transducers were available for purchase. US was used for over two decades when the firstclinical study of obstetric ultrasound was published in 1980(118). By 1987, US was used in as many as 40 percent of antenatal tests (117). Today, US use is common in antenataland intrapartal settings.
Testing and Cleaning the Ultrasound TransducerTo test this component, plug the transducer cable into themonitor, turn on the power, and turn up the sound volume.Apply ultrasonic (coupling) gel or water to the transducer
face. Gently rub the transducer face in small circles, movingin a clockwise or counterclockwise direction. Where ever thetransducer face is rubbed, static should be heard if the crystals inside the transducer are functioning. Another wayto test the transducer is to hold it in one hand while movingthe other hand toward and away from the transmitting surface. If the monitor produces a noise as the hand movestowards the transducer, the transducer is working.
Be gentle with US transducers to avoid damage of the delicate piezoelectric crystals inside (2). Usually, transducersand their cables should not be immersed in water. However,some manufacturers make immersible transducers.Transducers should be cleaned after use with a disinfectantsolution, thoroughly rinsed with water, and dried with aclean cloth.
The Doppler Principle Ultrasound devices, such as a hand-held Doppler, have oneor more piezoelectric crystals inside which transmit high frequency US waves and receive reflected waves (see Figure1.14). Ultrasounds are motion detectors. The Doppler Principlestates that ultrahigh frequency sound wave echoes reflectedfrom moving objects differ from those reflected from nonmoving objects. The difference in the frequency of thereturn waves is called the Doppler shift.
Ultrasound devices send US waves into the abdomen and
ANTEPARTAL AND INTRAPARTAL FETAL MONITORING
20
Figure 1.13: Segments of the fetal ECG (ST segments) are plotted above the FHR pattern. The dark line at the bottom of the paper indicates the end of paperis near.
uterus which are reflected back by moving objects, similar toa ping pong ball (US waves) and a ping pong paddle (moving object). The reflected beam may be increased ordecreased in frequency based on the direction of motion.Movement perpendicular to and towards the face of the UStransducer increases sound wave frequency. Movement awayfrom the transducer decreases sound wave frequency (108).
“Moving objects” include maternal abdominal muscles,maternal blood flow through the aorta, the aortic wall, maternal bowel, fetal limbs, the umbilical cord, fetal atria andventricles, and fetal heart valves (2-3). Movement that createsa signal for detection may not be from the fetus or thewoman. A tracing has been generated when the US was unattached to the woman but was sitting on top of the fetalmonitor. A tachycardic rate was recorded.
Since maternal aortic movement can reflect US waveswhich will be amplified and counted, the maternal pulseshould be assessed and recorded prior to US application. Therecorded rate should differ from the MHR. The MHR andfetal heart sounds or fetal movement should be confirmedand documented when the signal source of the tracing isunclear.
Confirmation of the FHR is also important when β-sympathomimetics are used for tocolysis or when fetaldemise is suspected. (36-37, 44). To confirm fetal life, a fetoscope or stethoscope should be used to hear fetal ventricular heart sounds, or the fetus should be scanned by areal-time ultrasound to visualize cardiac motion. The MECGcable could be applied to distinguish the MHR from the
printed rate. A hand-held Doppler device could be used atthe same time the MHR is assessed. The Doppler rate and theMHR should differ.
The US detects mechanical activity, not electrical energy orsound. Systole and diastole, with the respective valvular closures (closure of