Embed Size (px)
Citation preview

ANTIAGGREGANTI, TAO E ENDOSCOPIA
GIUSEPPE ARENACARDIOLOGIA – UTICUSL1 MASSA CARRARA



Heart Disease and Stroke Statistics—2013 Update
by Alan S. Go, Dariush Mozaffarian, Véronique L. Roger, Emelia J. Benjamin, Jarett D. Berry, William B. Borden, Dawn M. Bravata, Shifan Dai, Earl S. Ford, Caroline S. Fox, Sheila Franco, Heather J. Fullerton, Cathleen Gillespie, Susan M. Hailpern, John A. Heit, Virginia J. Howard, Mark D. Huffman, Brett M. Kissela, Steven J. Kittner, Daniel
T. Lackland, Judith H. Lichtman, Lynda D. Lisabeth, David Magid, Gregory M. Marcus, Ariane Marelli, David B. Matchar, Darren K. McGuire, Emile R. Mohler, Claudia S. Moy, Michael E. Mussolino, Graham Nichol, Nina P. Paynter, Pamela J. Schreiner, Paul D. Sorlie, Joel Stein, Tanya N. Turan, Salim S. Virani, Nathan D. Wong, Daniel Woo, and
Melanie B. Turner
CirculationVolume 127(1):e6-e245
January 1, 2013
Copyright © American Heart Association
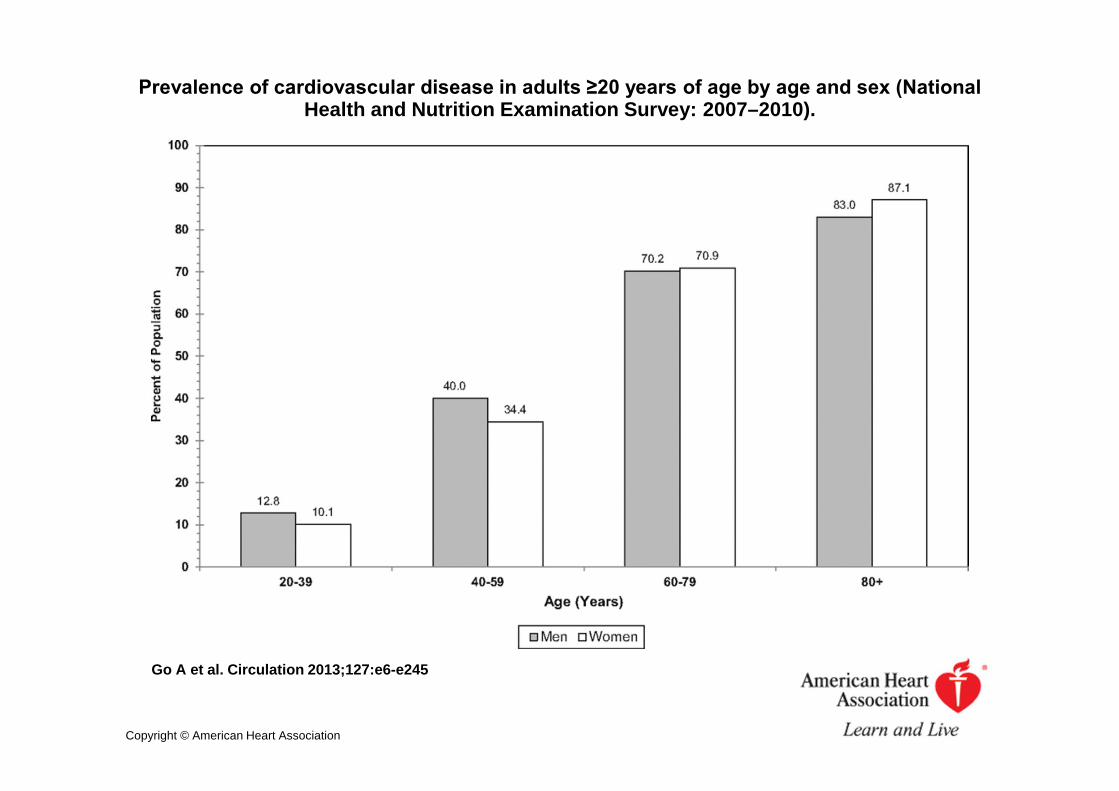
Prevalence of cardiovascular disease in adults ≥20 years of age by age and sex (National Health and Nutrition Examination Survey: 2007–2010).
Go A et al. Circulation 2013;127:e6-e245
Copyright © American Heart Association
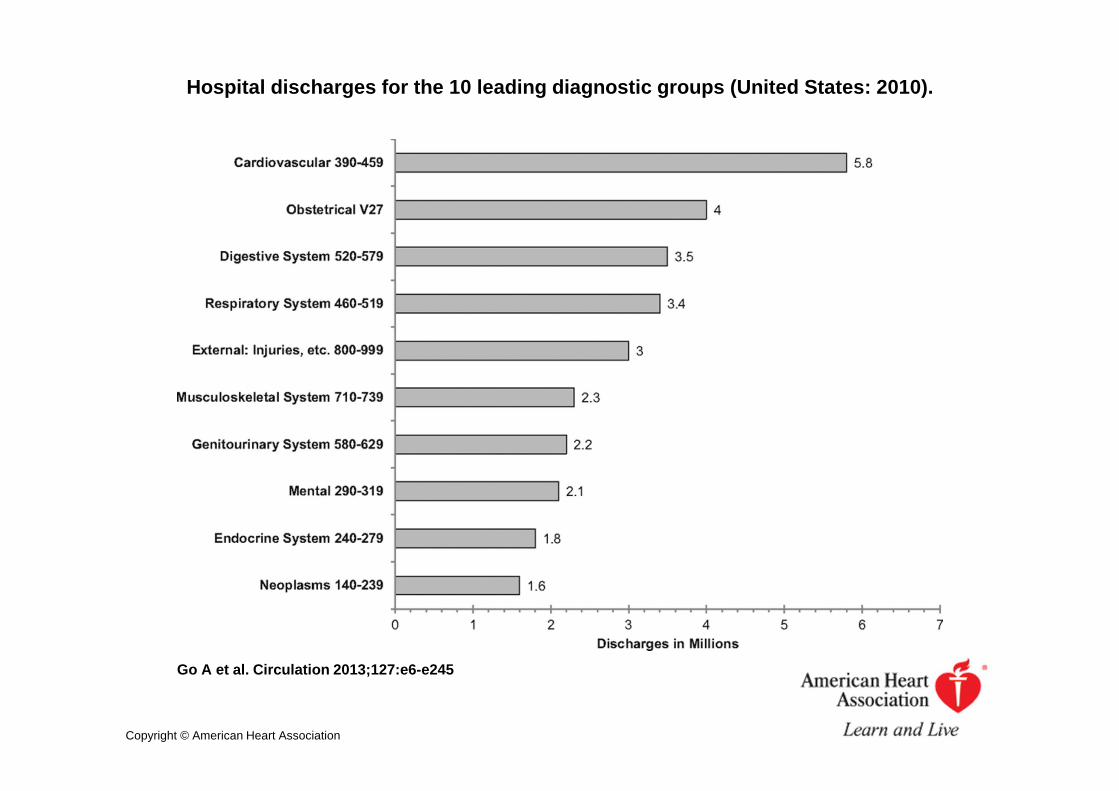
Hospital discharges for the 10 leading diagnostic groups (United States: 2010).
Go A et al. Circulation 2013;127:e6-e245
Copyright © American Heart Association
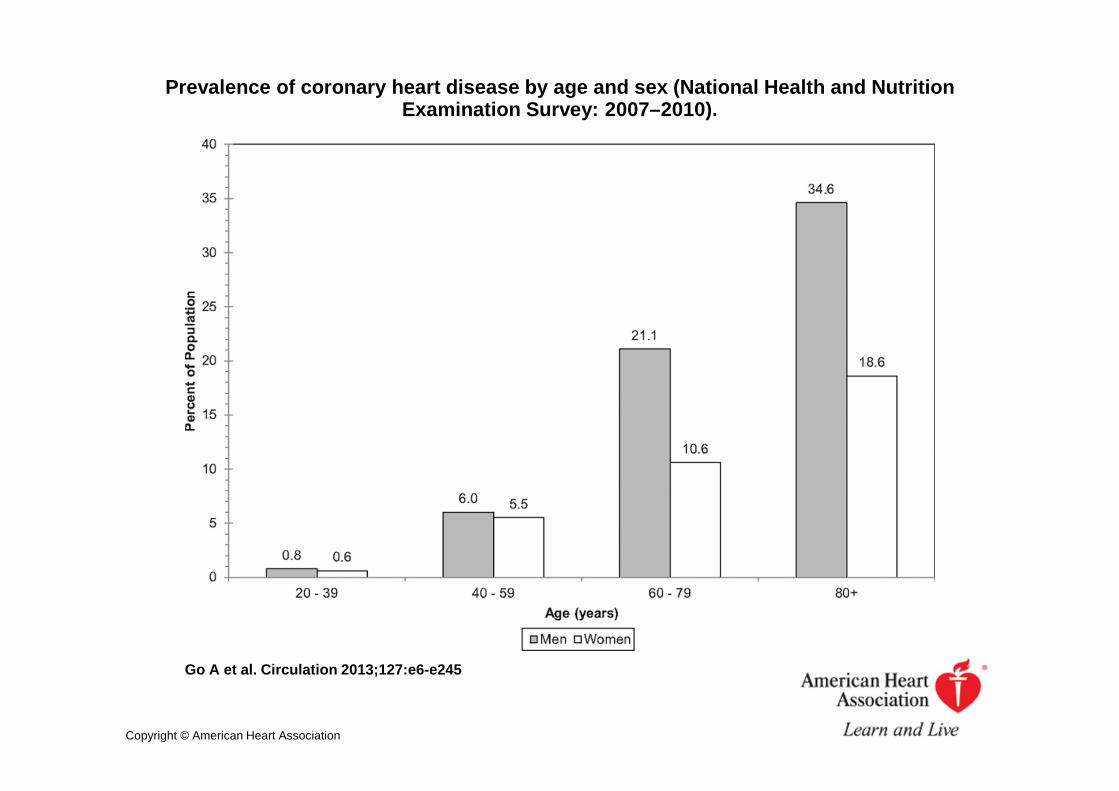
Prevalence of coronary heart disease by age and sex (National Health and Nutrition Examination Survey: 2007–2010).
Go A et al. Circulation 2013;127:e6-e245
Copyright © American Heart Association

Prevalence of stroke by age and sex (National Health and Nutrition Examination Survey: 2007–2010).
Go A et al. Circulation 2013;127:e6-e245
Copyright © American Heart Association

SOCIETY GUIDELINESAmerican Society for Gastrointestinal Endoscopy (ASGE)
Management of antithrombotic agents for endoscopic procedures. AndersonMA, et al. Gastrointest Endosc. 2009;70(6):1060
American College of GastroenterologyManagement of anticoagulation before and after gastrointestinal endoscopy.Kwok A, Faigel DO. Am J Gastroenterol. 2009;104(12):3085.
American College of CardiologyManagement of platelet-directed pharmacotherapy in patients withatherosclerotic coronary artery disease undergoing elective endoscopicgastrointestinal procedures. Becker RC, et al. J Am Coll Cardiol.2009;54(24):2261.
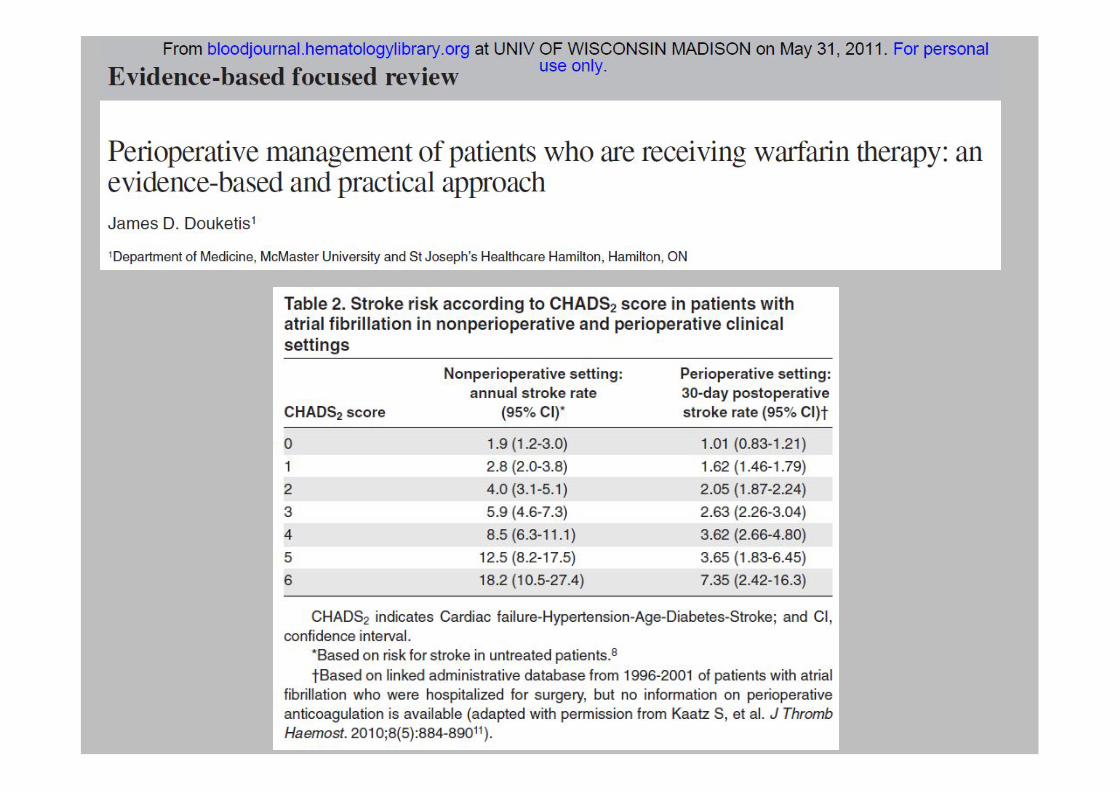
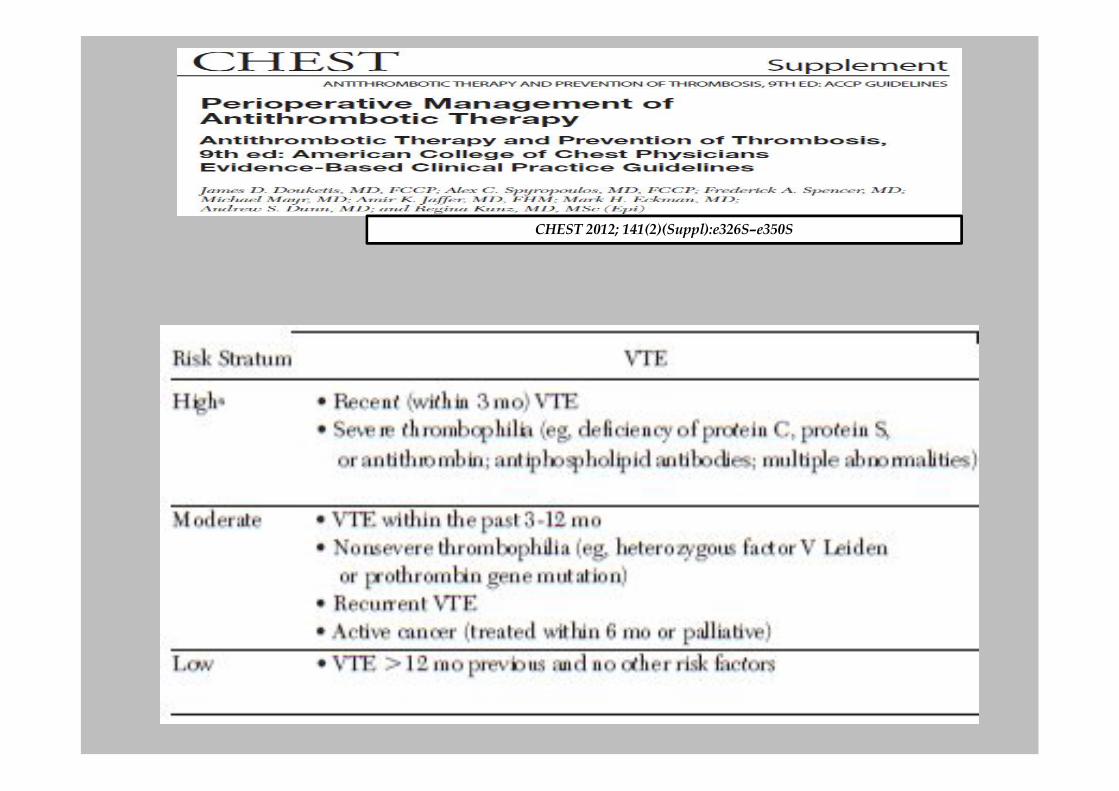
American College of Chest PhysiciansPerioperative management of antithrombotic therapy: AntithromboticTherapy and Prevention of Thrombosis, 9th ed. Douketis JD, et al. Chest.2012;141(2 Suppl):e326S.
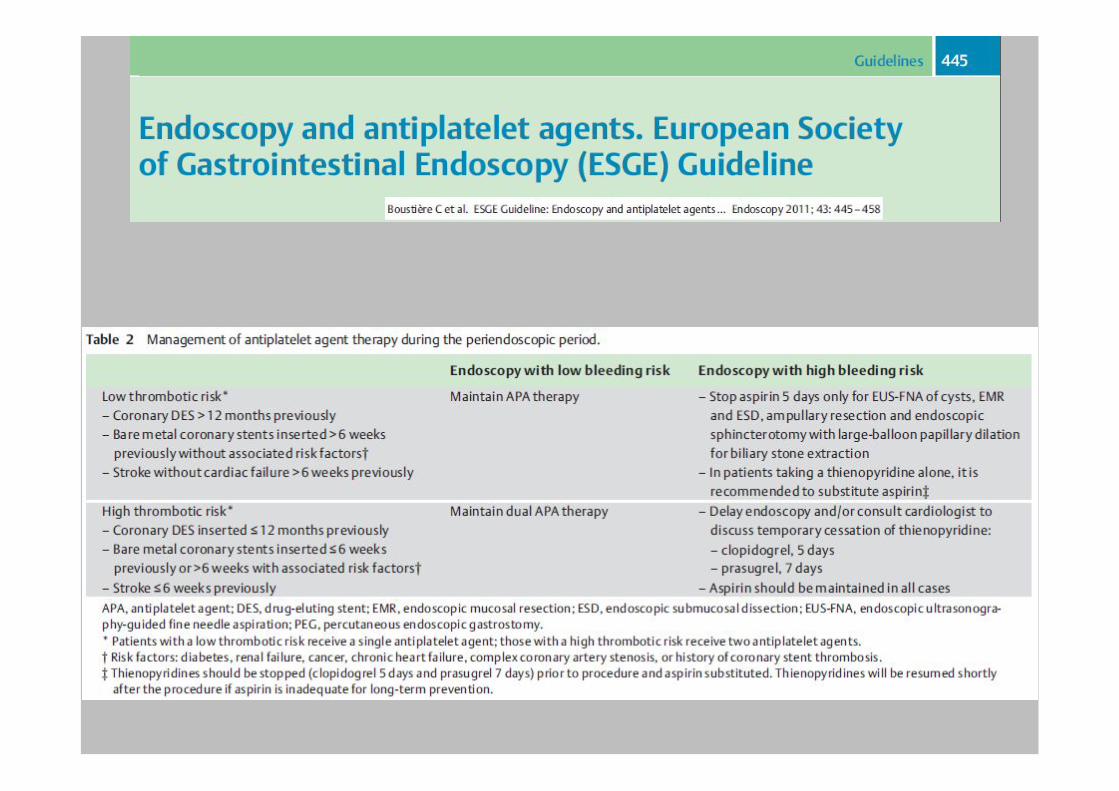
European Society of Gastrointestinal Endoscopy (ESGE)Endoscopy and antiplatelet agents. C. Boustière, et al. Endoscopy 2011; 43:445–458

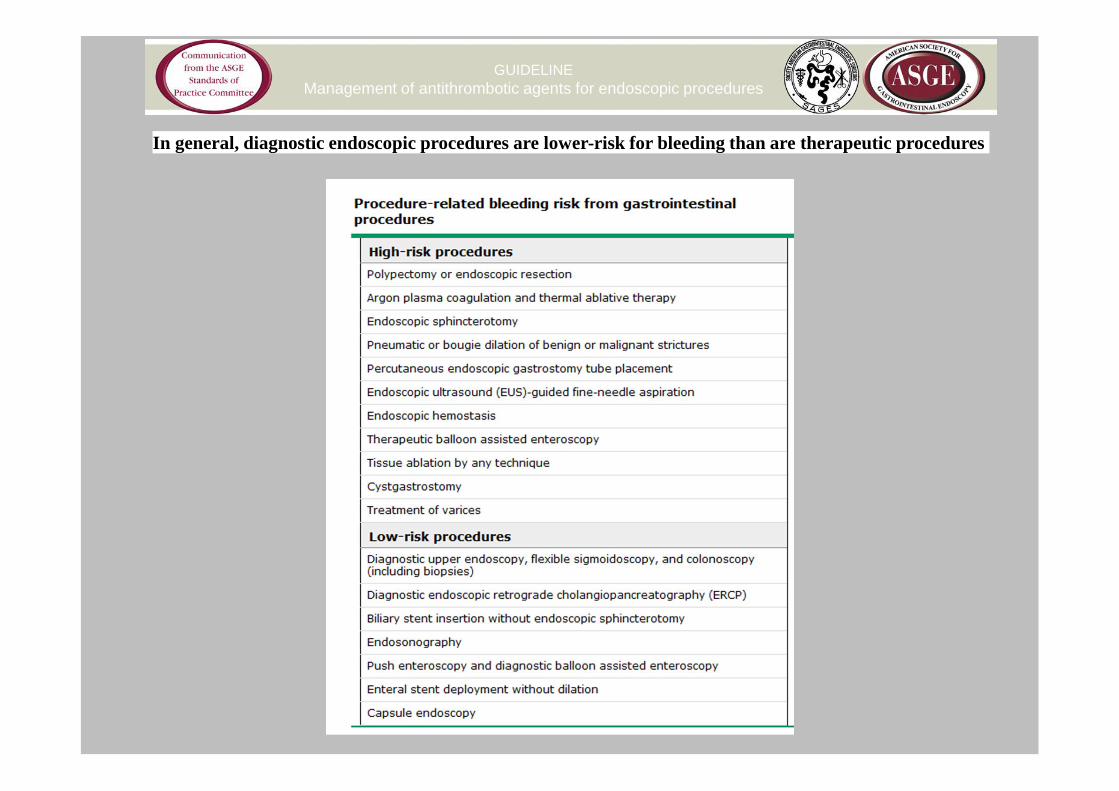
In general, diagnostic endoscopic procedures are lower-risk for bleeding than are therapeutic procedures
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
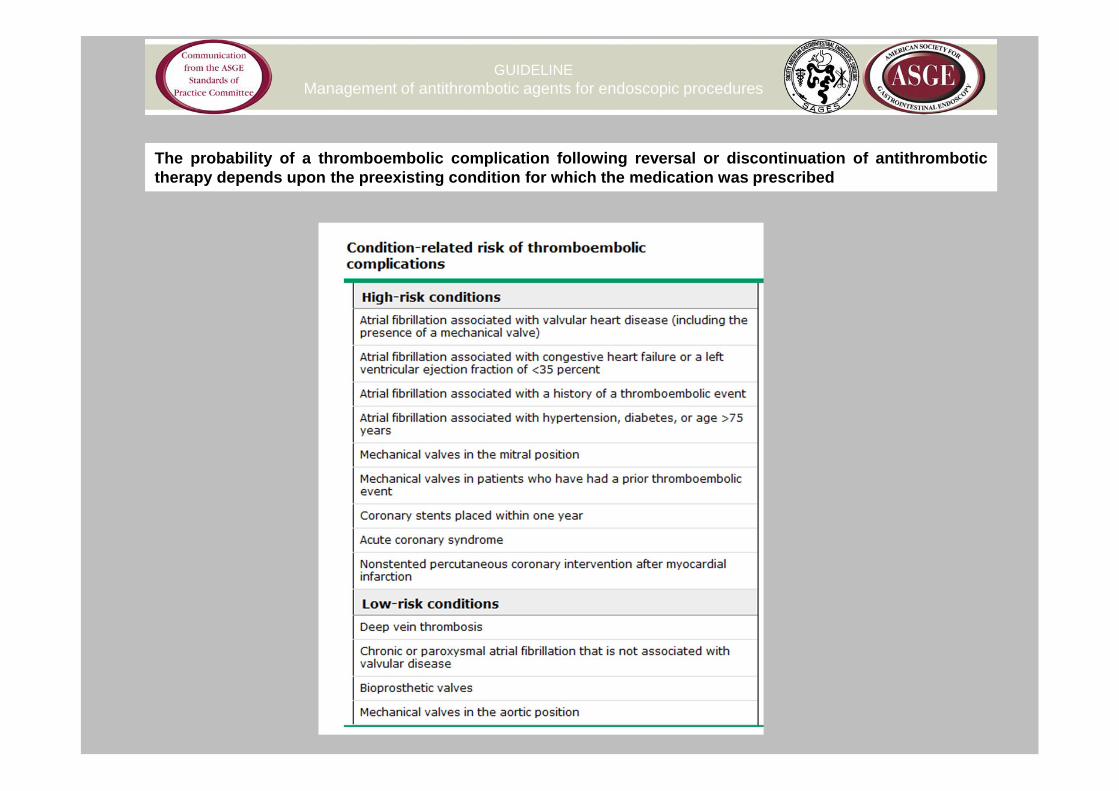
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
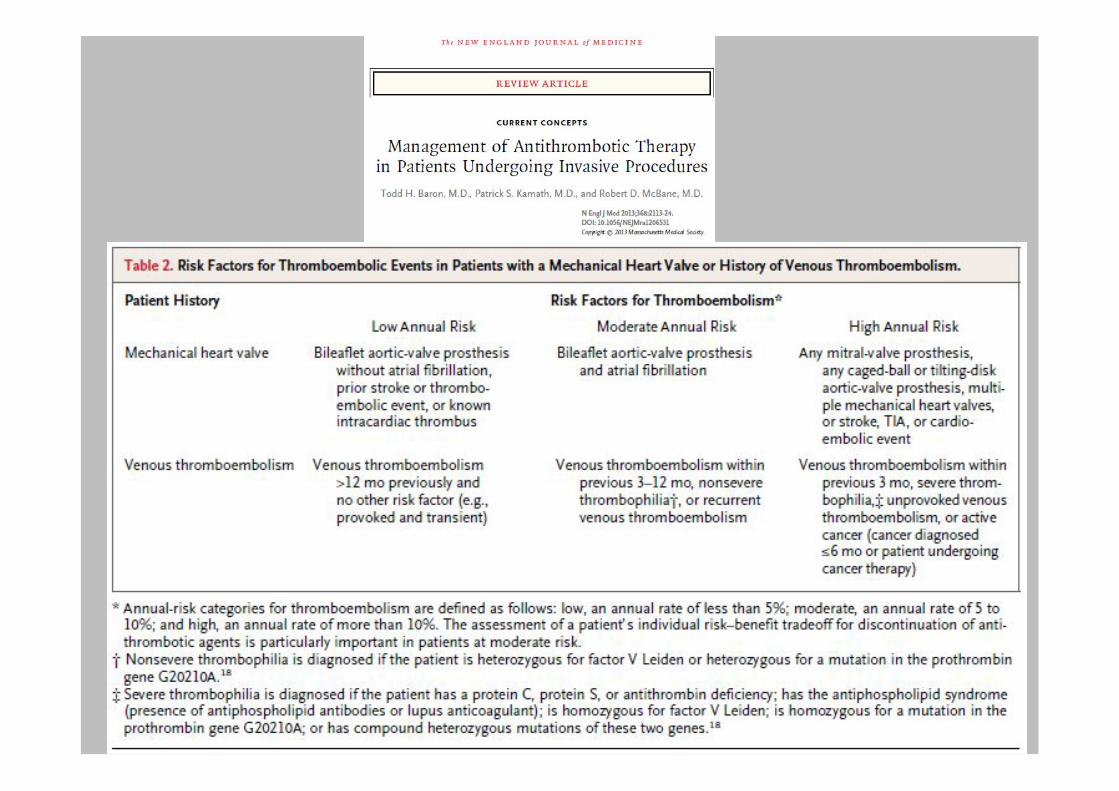
The probability of a thromboembolic complication following reversal or discontinuation of antithrombotictherapy depends upon the preexisting condition for which the medication was prescribed
www.escardio.org/guidelines
www.escardio.org/guidelines

www.escardio.org/guidelines
www.escardio.org/guidelines
www.escardio.org/guidelines
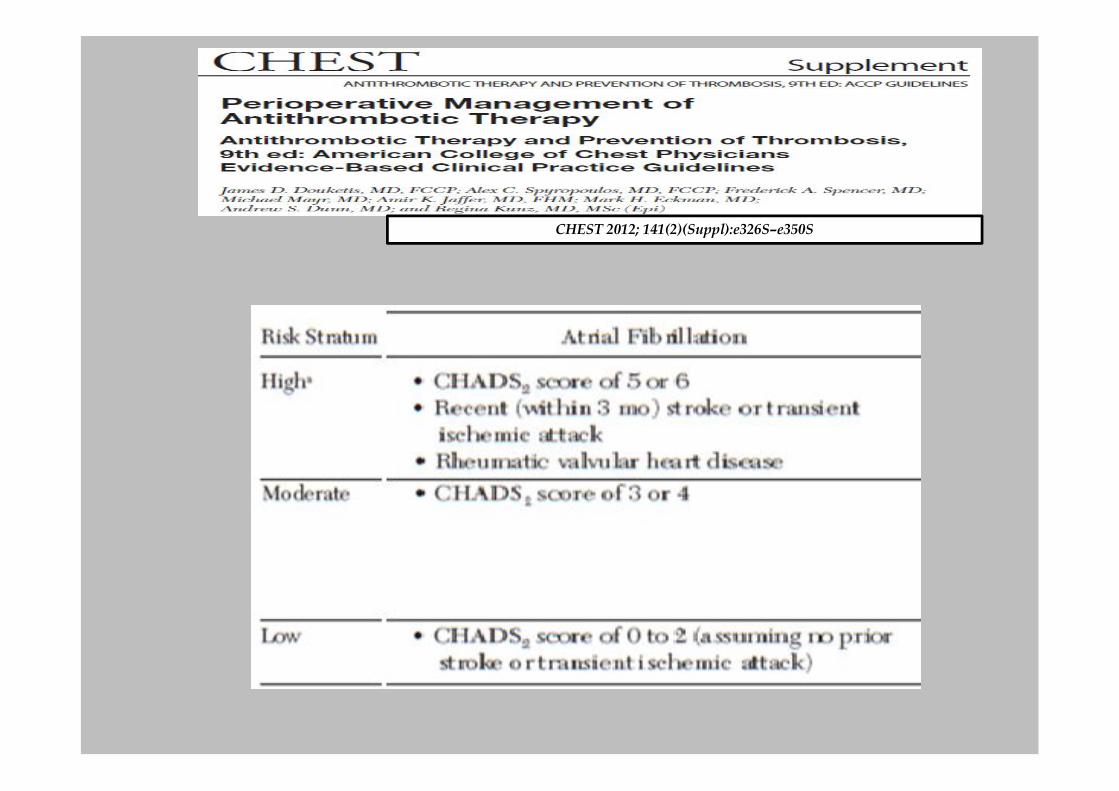
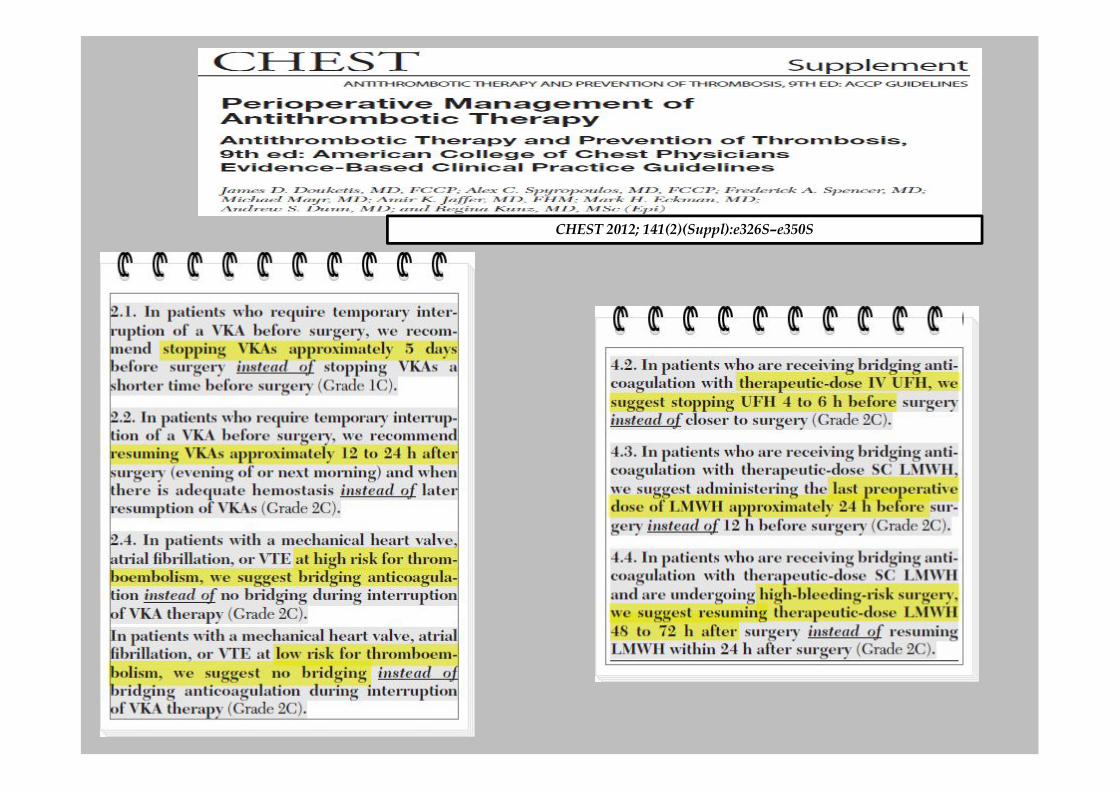
CHEST 2012; 141(2)(Suppl):e326S–e350S

CHEST 2012; 141(2)(Suppl):e326S–e350S
CHEST 2012; 141(2)(Suppl):e326S–e350S

Low-risk procedures, high or low-risk conditions
• No change in anticoagulation is recommended for low-riskprocedures
• Elective procedures should be delayed in patients taking warfarin ifthe INR or prothrombin time is in the supratherapeutic range (INR> 2,5)
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
ELECTIVE PROCEDURES IN ANTICOAGULATED PATIENTS
The guidelines recommend that elective procedures be delayed whenpossible if the indication for anticoagulation is temporary
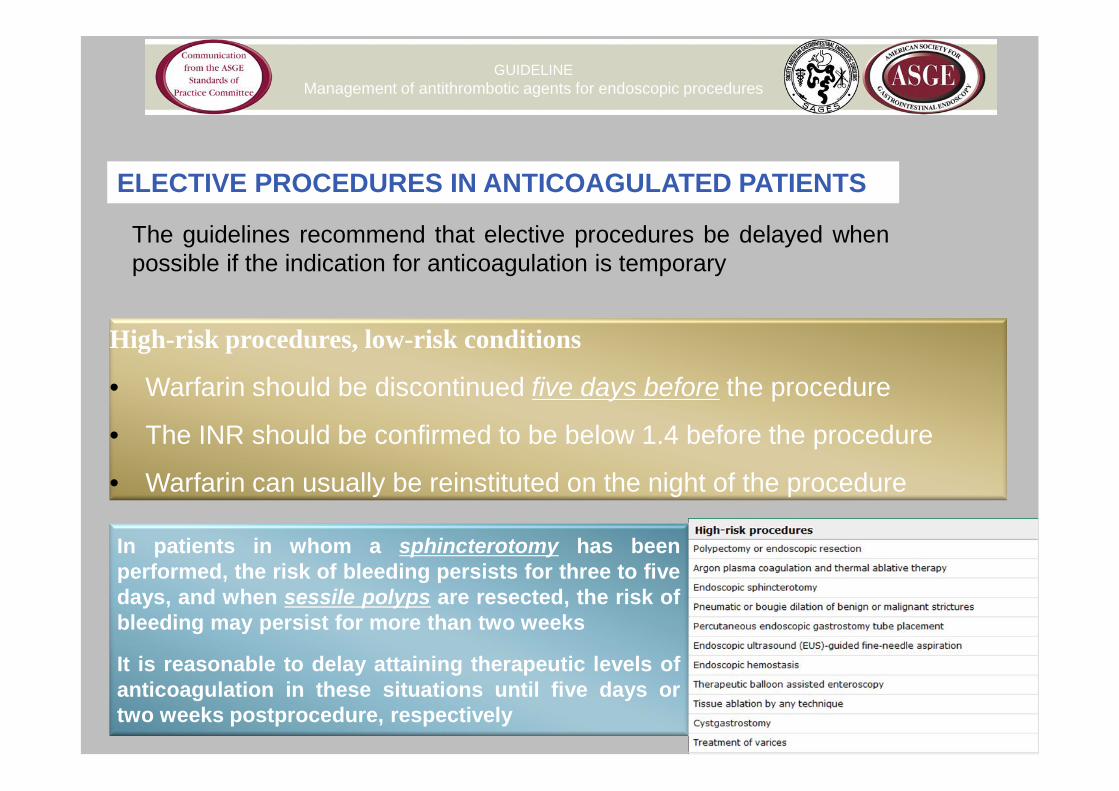
High-risk procedures, low-risk conditions
• Warfarin should be discontinued five days before the procedure
• The INR should be confirmed to be below 1.4 before the procedure
• Warfarin can usually be reinstituted on the night of the procedure
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
ELECTIVE PROCEDURES IN ANTICOAGULATED PATIENTS
The guidelines recommend that elective procedures be delayed whenpossible if the indication for anticoagulation is temporary
In patients in whom a sphincterotomy has beenperformed, the risk of bleeding persists for three to fivedays, and when sessile polyps are resected, the risk ofbleeding may persist for more than two weeks
It is reasonable to delay attaining therapeutic levels ofanticoagulation in these situations until five days ortwo weeks postprocedure, respectively
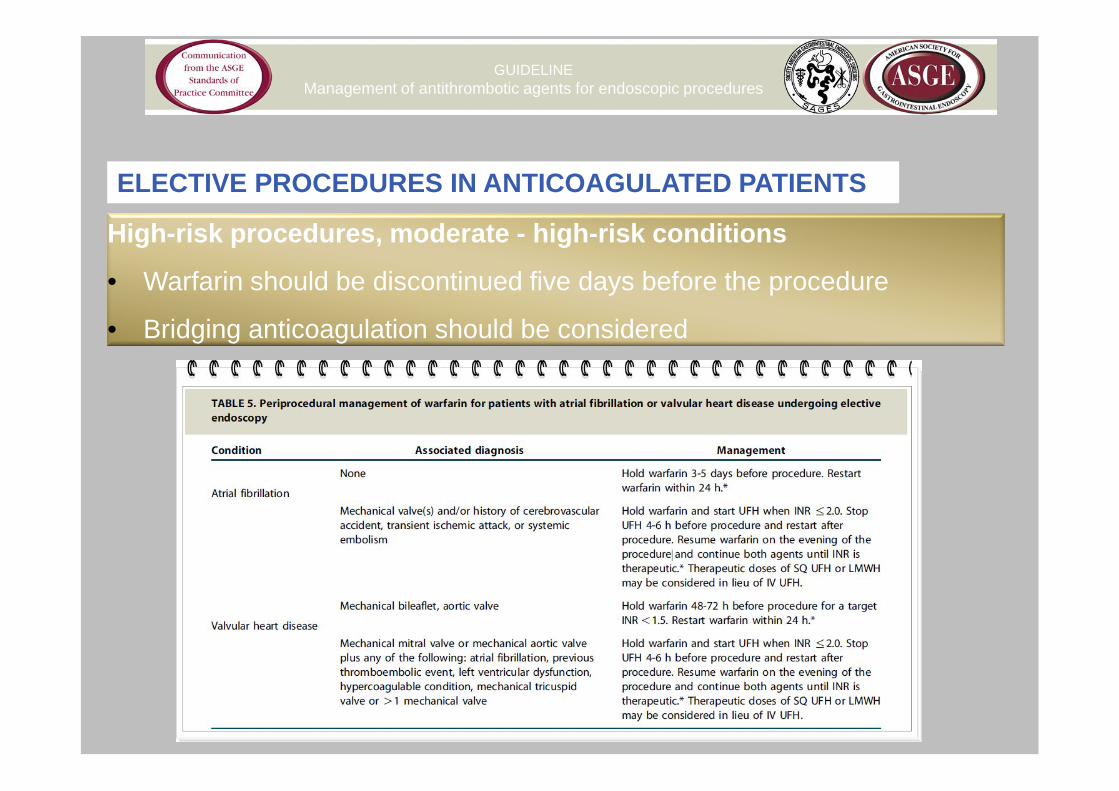
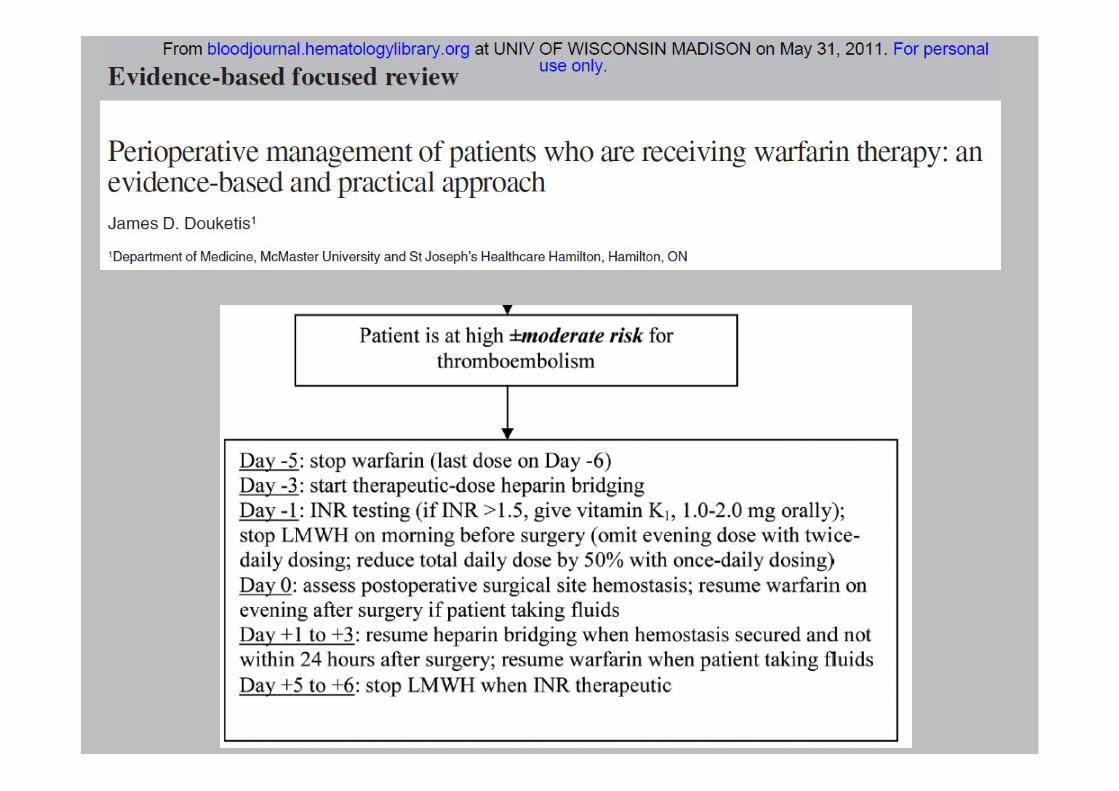
High-risk procedures, moderate - high-risk conditions
• Warfarin should be discontinued five days before the procedure
• Bridging anticoagulation should be considered
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
ELECTIVE PROCEDURES IN ANTICOAGULATED PATIENTS

STOP WARFARIN
INR < 2
START UFH
STOP 4 – 6 HRS
BEFORE
ENDOSCOPY
2 – 6 HRS AFTER
RESUME UFH
IN THE EVENING
RESUME WARFARIN
INR > 2
STOP UFH
BRIDGING ANTICOAGULATION
An advantage of standard heparin is its short half-life, which permits temporary discontinuation should patients develop a bleeding complication
BRIDGING ANTICOAGULATION
Low molecular weight heparin vs unfractionated heparin
• greater bioavailability
• longer duration of action
• can be given in a fixed dose based upon body weight
• outpatient treatment
• at least as effective as unfractionated heparin
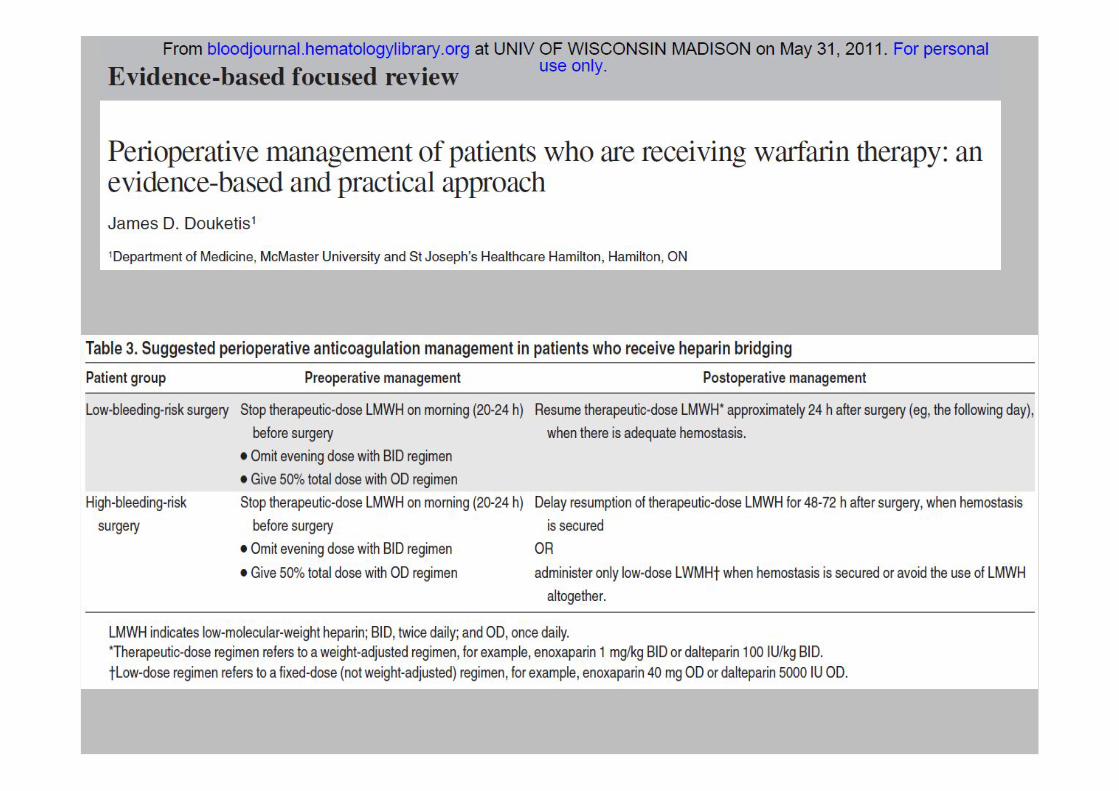
CHEST 2012; 141(2)(Suppl):e326S–e350S

LOW-RISK HIGH-RISK
LOW-RISK CONTINUE CONTINUE
HIGH-RISK STOPSTOP
+BRIDGING
CONDITIONS(thrombotic risk)
PR
OC
ED
UR
ES
(ble
edin
gri
sk)
ANTICOAGULATION THERAPY

INTERAZIONI FARMACOLOGICHE INTERAZIONI ALIMENTARI
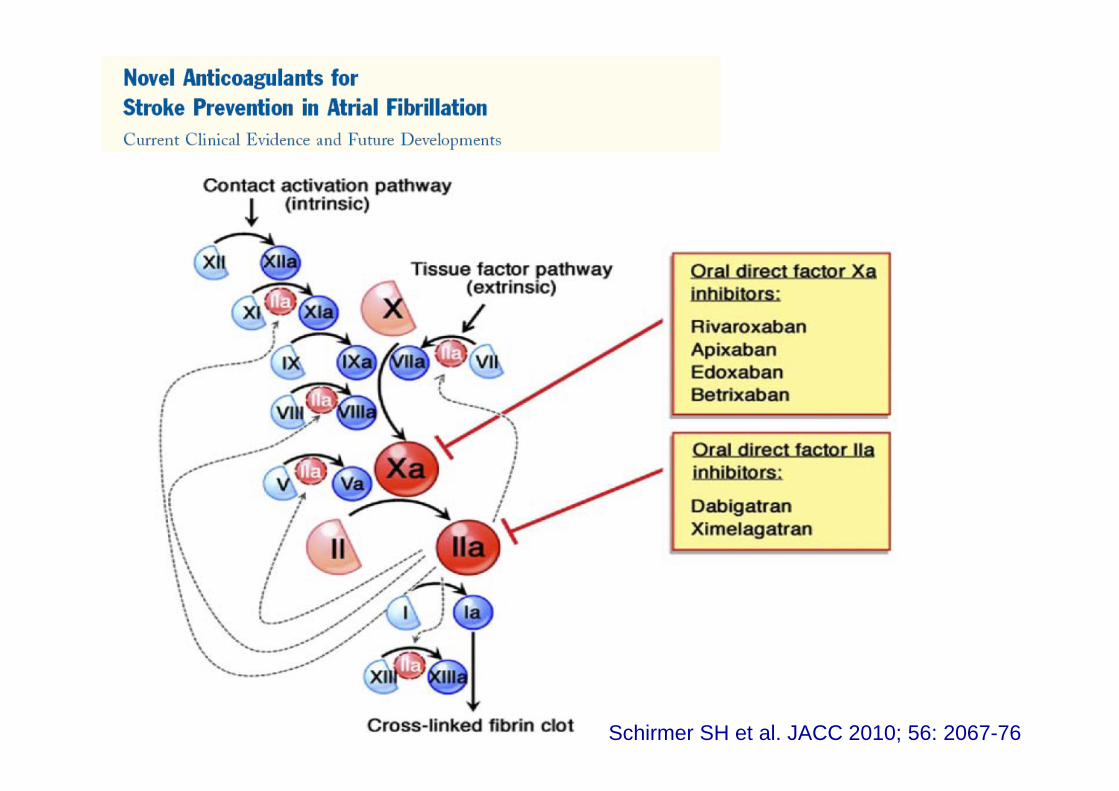
Schirmer SH et al. JACC 2010; 56: 2067-76

DABIGATRAN RIVAROXABAN APIXABAN
Meccanismo d’azione Inibitore diretto
TROMBINA
Inibitore diretto
FXa
Inibitore diretto
FXa
Biodisponibilità 6.5% 80% 50%
Via di somministrazione Orale Orale Orale
Pro-farmaco SI NO NO
Interazioni alimentari NO NO NO
Clearance renale 85% 66% (36% immodif.) 27%
Emivita (T1/2) 14-17 h 7-11 12 h
T max 0.5-2 h 2-4 h 3 h
Interazioni farmacologiche
P-gp inhibitors
P-gp inducers(Es: amiodarone)
CYP3A4 inhibitors
CYP3A4 inducers
P-gp inhibitors
CYP3A4 inhibitors
CYP3A4 inducers P-gp inhibitors
Ansell J. Haematology 2010; 2010: 221-228
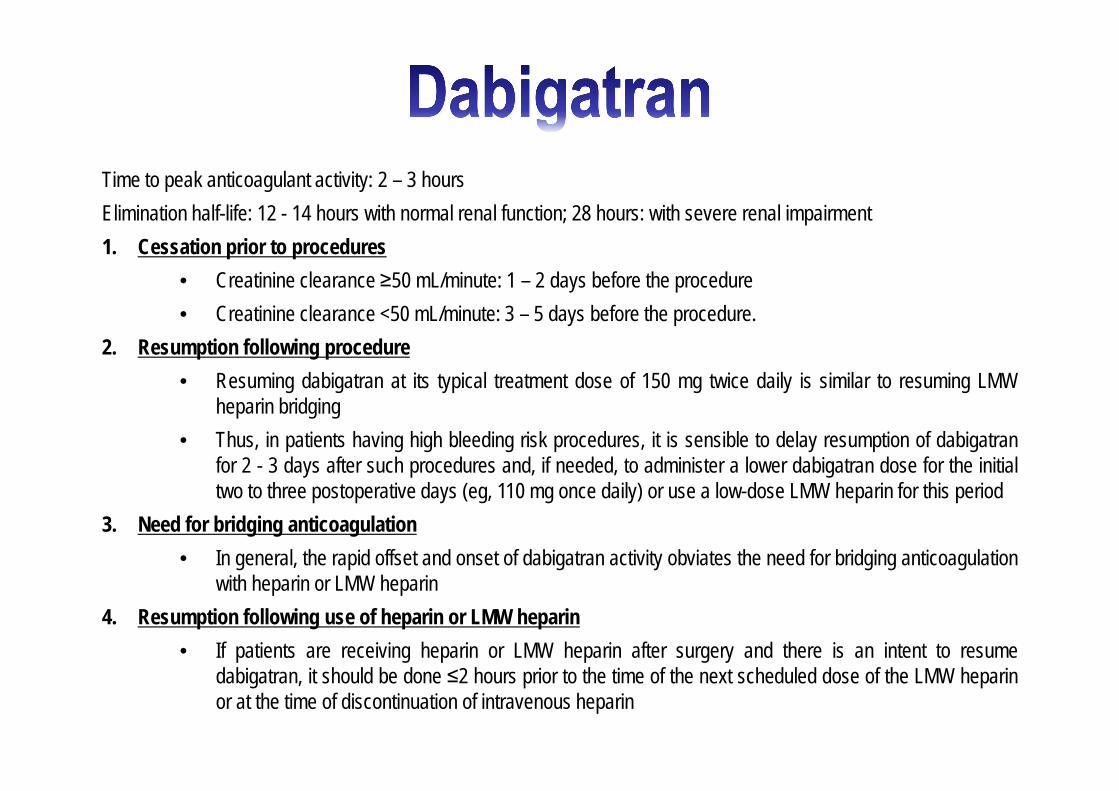
Time to peak anticoagulant activity: 2 – 3 hours
Elimination half-life: 12 - 14 hours with normal renal function; 28 hours: with severe renal impairment
1. Cessation prior to procedures
• Creatinine clearance ≥50 mL/minute: 1 – 2 days before the procedure
• Creatinine clearance <50 mL/minute: 3 – 5 days before the procedure.
2. Resumption following procedure
• Resuming dabigatran at its typical treatment dose of 150 mg twice daily is similar to resuming LMWheparin bridging
• Thus, in patients having high bleeding risk procedures, it is sensible to delay resumption of dabigatranfor 2 - 3 days after such procedures and, if needed, to administer a lower dabigatran dose for the initialtwo to three postoperative days (eg, 110 mg once daily) or use a low-dose LMW heparin for this period
3. Need for bridging anticoagulation
• In general, the rapid offset and onset of dabigatran activity obviates the need for bridging anticoagulationwith heparin or LMW heparin
4. Resumption following use of heparin or LMW heparin
• If patients are receiving heparin or LMW heparin after surgery and there is an intent to resumedabigatran, it should be done ≤2 hours prior to the time of the next scheduled dose of the LMW heparinor at the time of discontinuation of intravenous heparin
Oral direct factor Xa inhibitors
Rapid onset of action (peak activity after 2 – 3 hours)
Elimination half-life of 9 to 12 hours
Unlike dabigatran, are less dependent on renal clearance (eg, 25 to 33 percent
instead of 80 percent)
In countries where these drugs are approved for long-term use and patients may
require perioperative management, the same approach should be used as with
dabigatran-treated patients
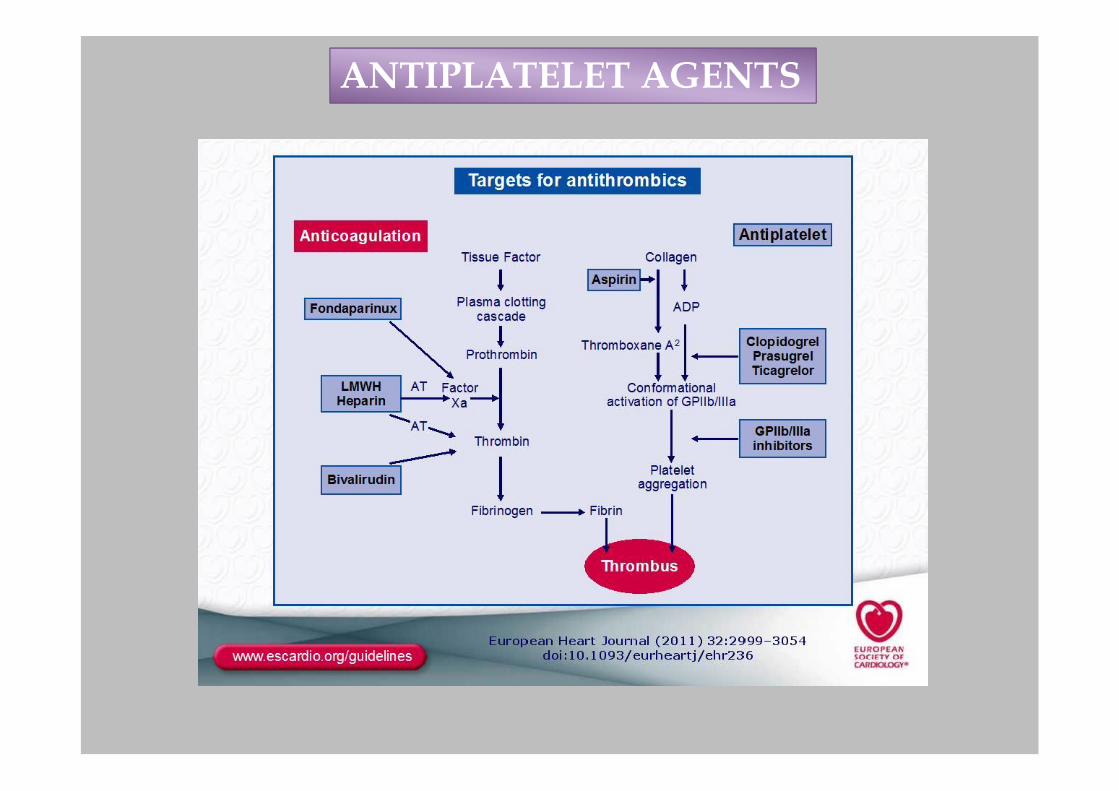
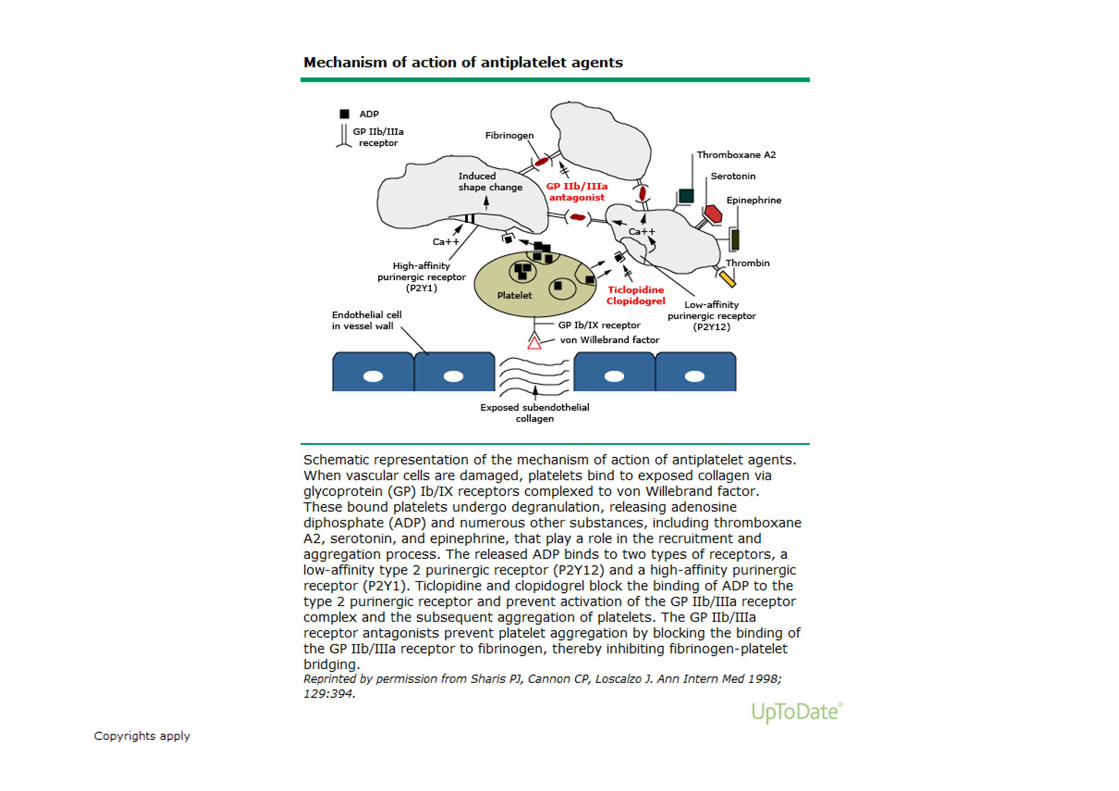
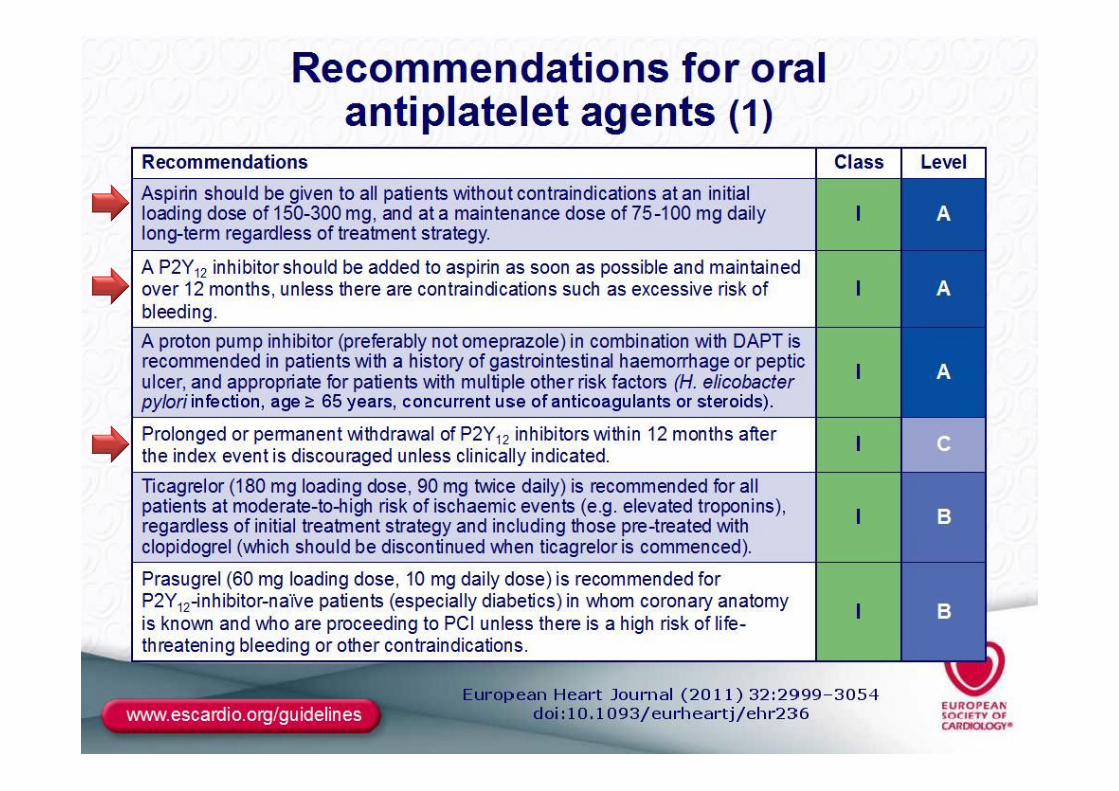
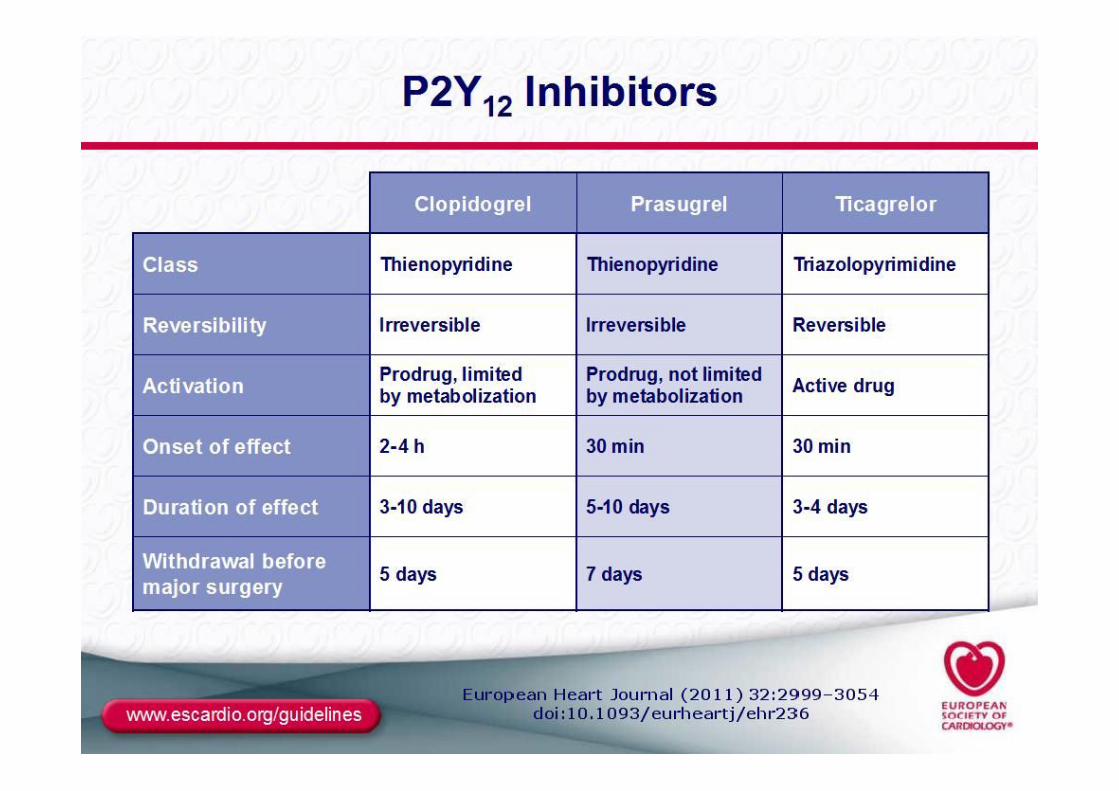
ANTIPLATELET AGENTS
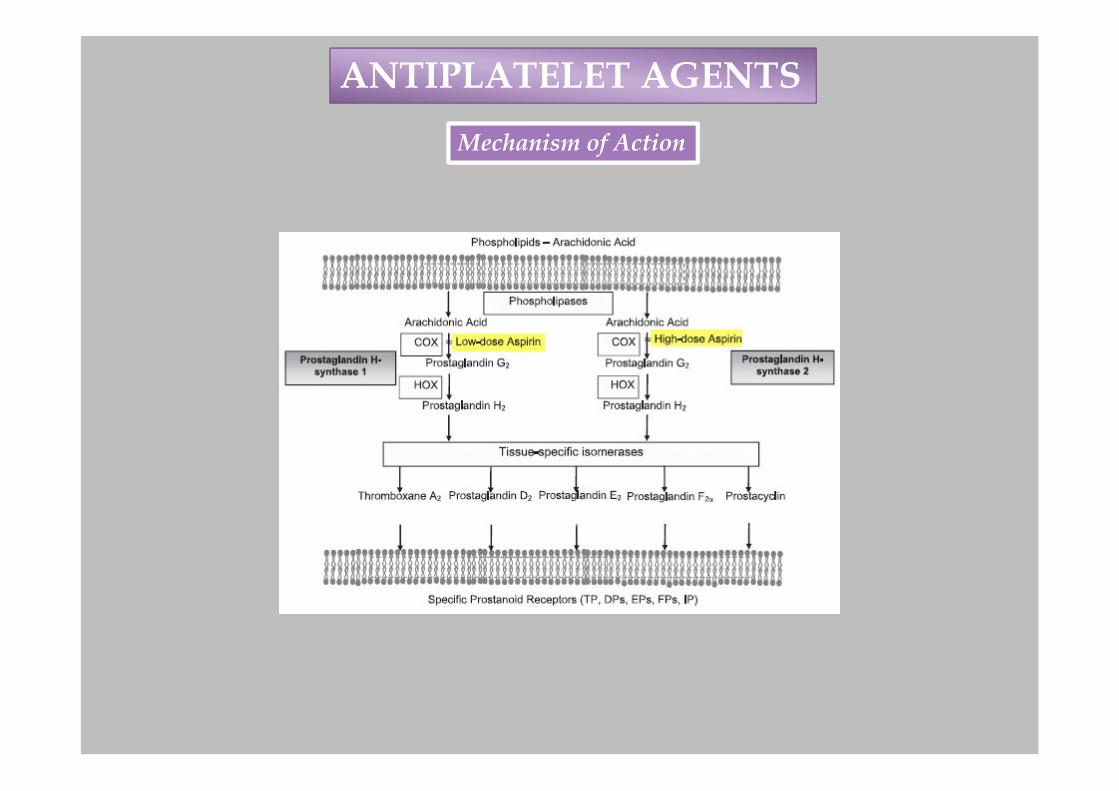
ANTIPLATELET AGENTS
Mechanism of Action

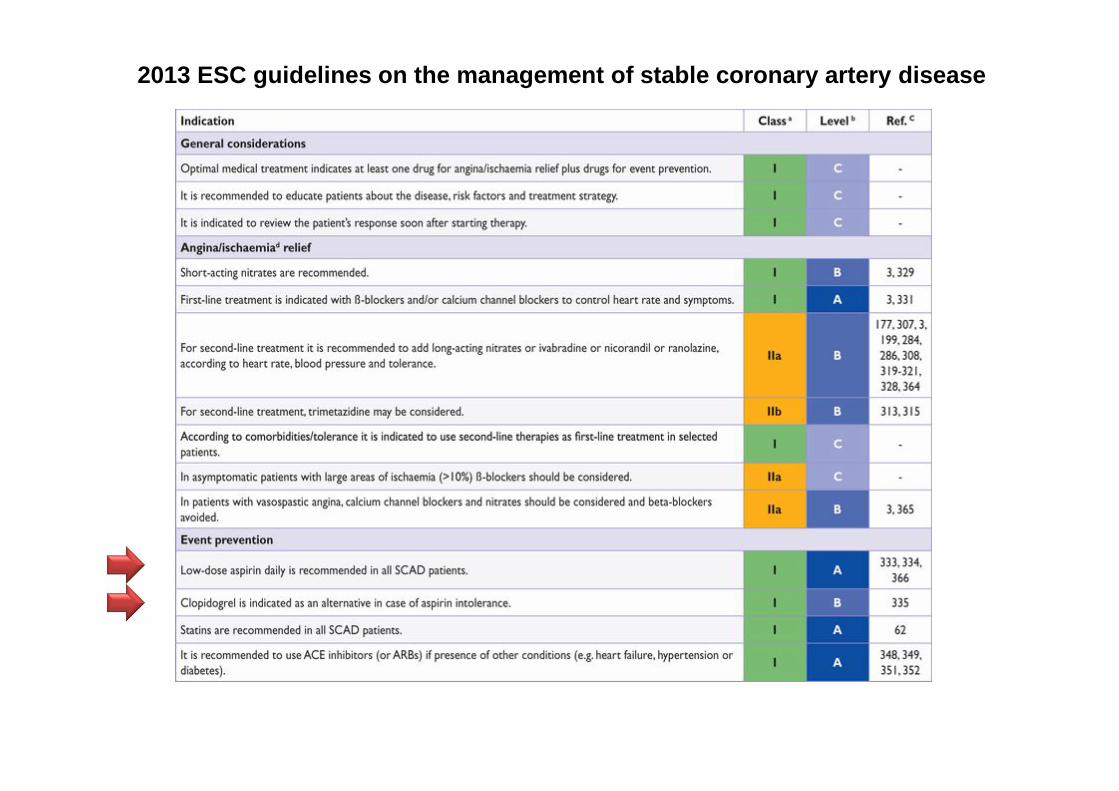
2013 ESC guidelines on the management of stable coronary artery disease
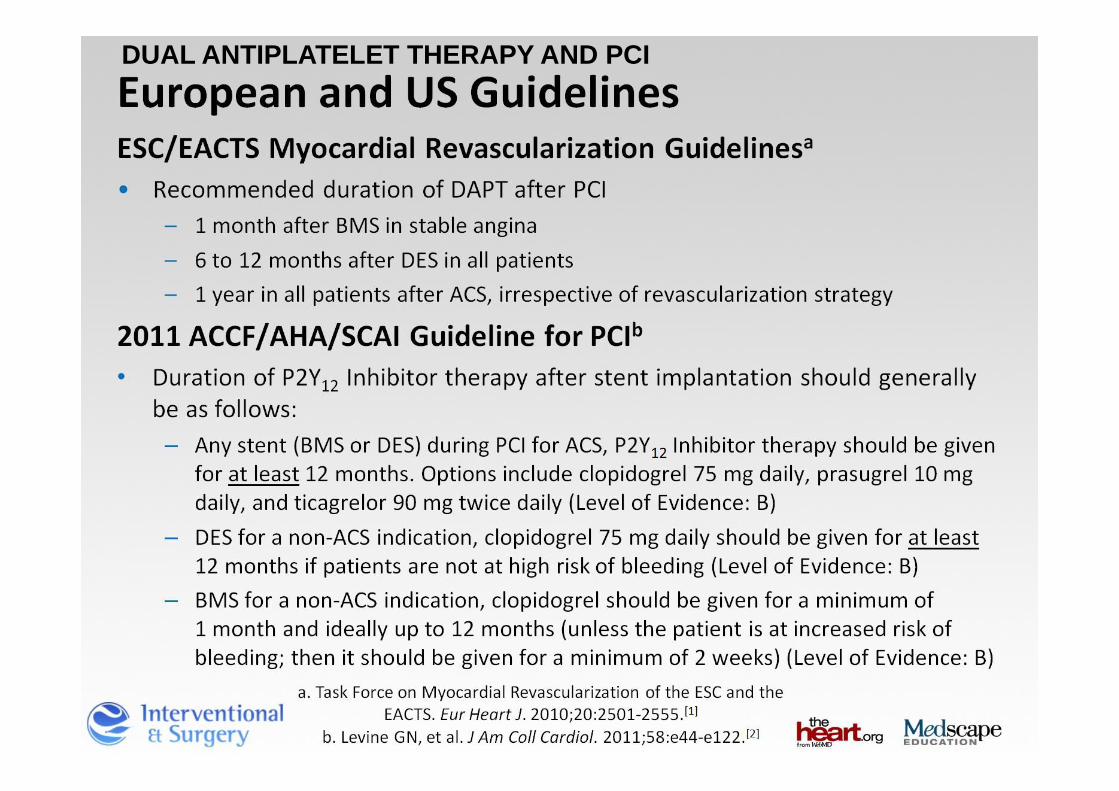
DUAL ANTIPLATELET THERAPY AND PCI
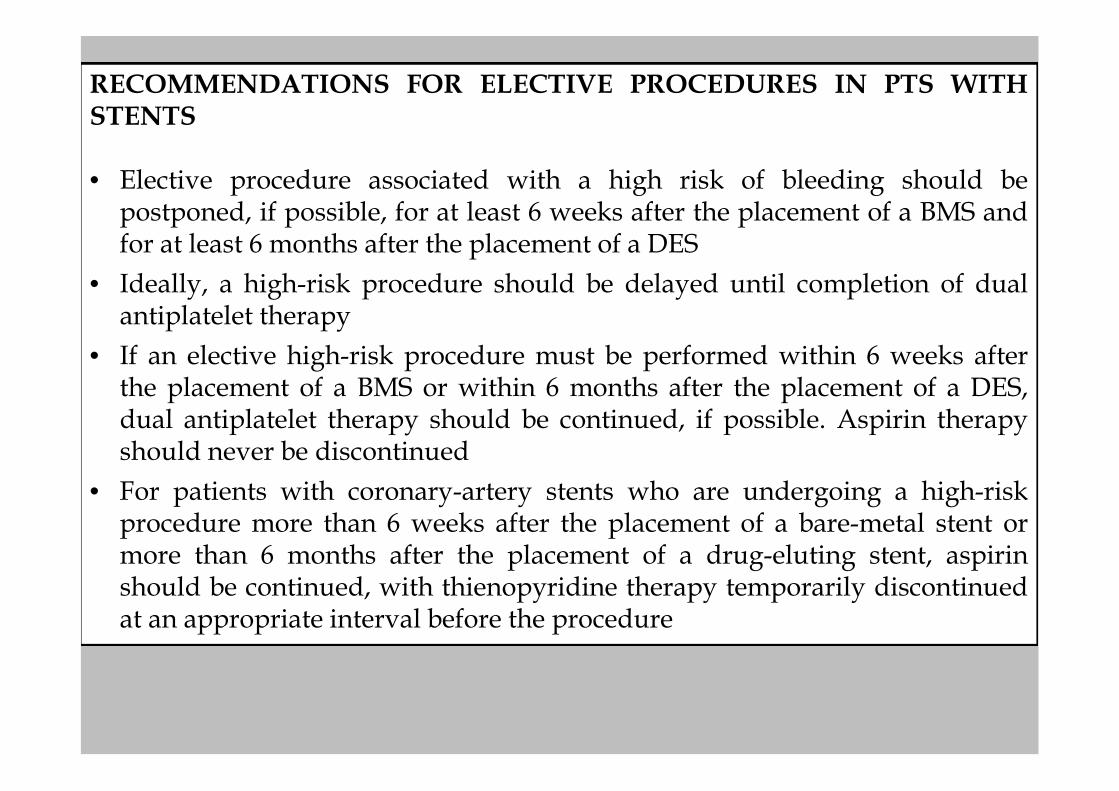
RECOMMENDATIONS FOR ELECTIVE PROCEDURES IN PTS WITHSTENTS
• Elective procedure associated with a high risk of bleeding should bepostponed, if possible, for at least 6 weeks after the placement of a BMS andfor at least 6 months after the placement of a DES
• Ideally, a high-risk procedure should be delayed until completion of dualantiplatelet therapy
• If an elective high-risk procedure must be performed within 6 weeks afterthe placement of a BMS or within 6 months after the placement of a DES,dual antiplatelet therapy should be continued, if possible. Aspirin therapyshould never be discontinued
• For patients with coronary-artery stents who are undergoing a high-riskprocedure more than 6 weeks after the placement of a bare-metal stent ormore than 6 months after the placement of a drug-eluting stent, aspirinshould be continued, with thienopyridine therapy temporarily discontinuedat an appropriate interval before the procedure
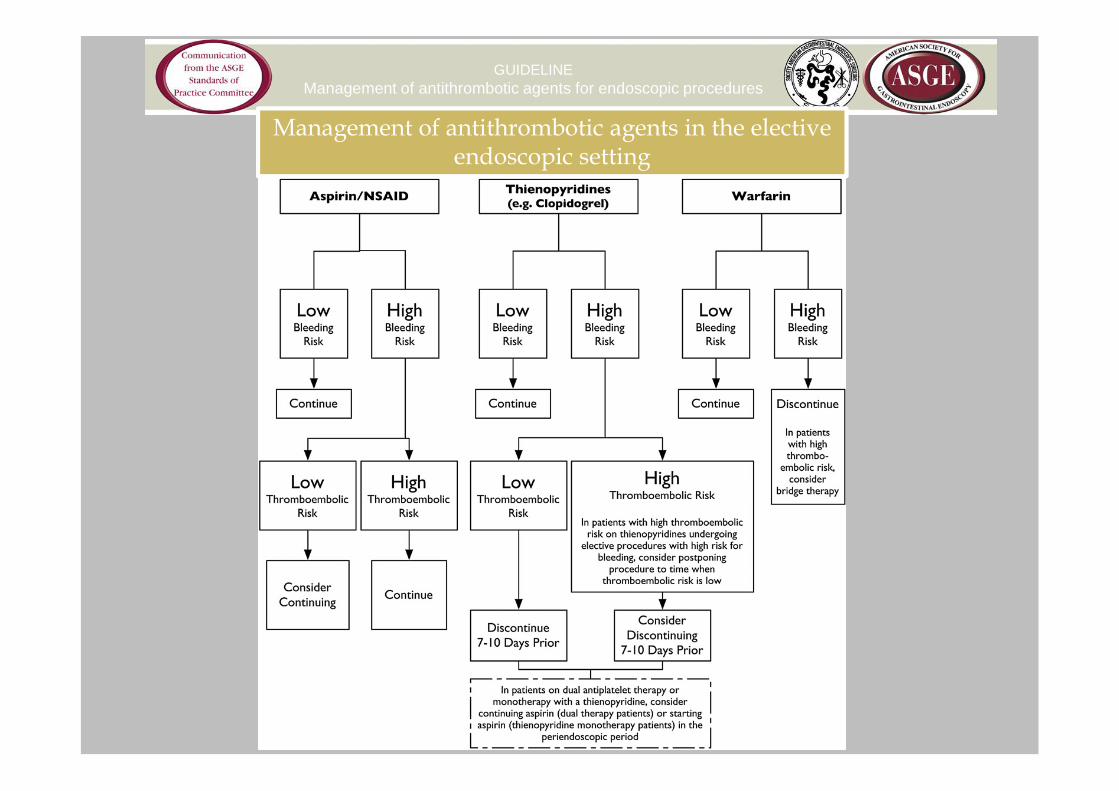
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
Management of antithrombotic agents in the elective endoscopic setting

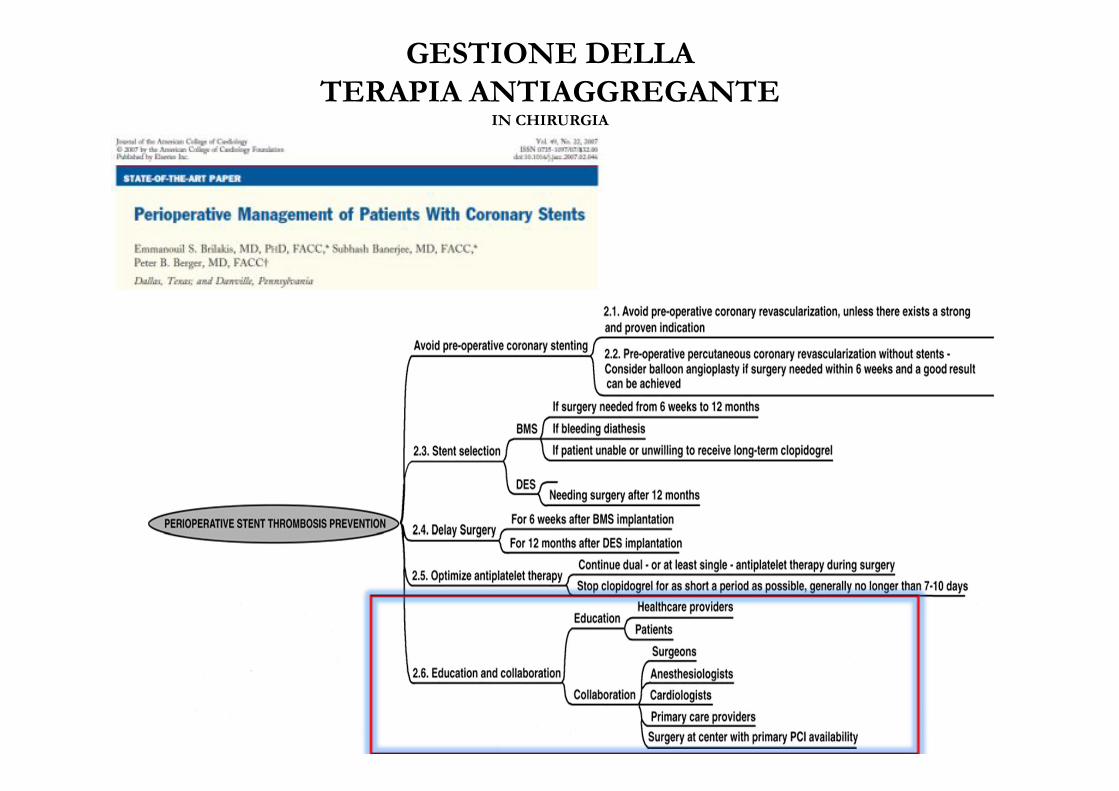
GESTIONE DELLATERAPIA ANTIAGGREGANTE
IN CHIRURGIA
G ITAL CARDIOL | VOL 13 | LUGLIO-AGOSTO 2012
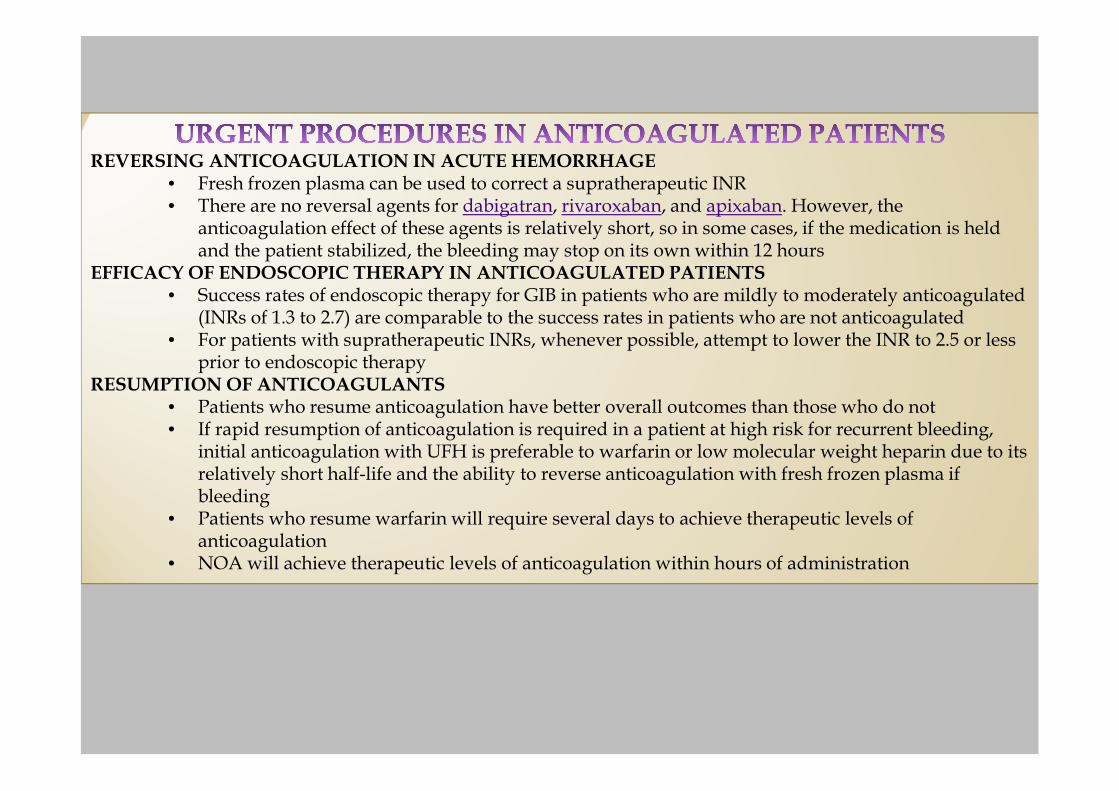
REVERSING ANTICOAGULATION IN ACUTE HEMORRHAGE• Fresh frozen plasma can be used to correct a supratherapeutic INR• There are no reversal agents for dabigatran, rivaroxaban, and apixaban. However, the
anticoagulation effect of these agents is relatively short, so in some cases, if the medication is held and the patient stabilized, the bleeding may stop on its own within 12 hours
EFFICACY OF ENDOSCOPIC THERAPY IN ANTICOAGULATED PATIENTS• Success rates of endoscopic therapy for GIB in patients who are mildly to moderately anticoagulated
(INRs of 1.3 to 2.7) are comparable to the success rates in patients who are not anticoagulated• For patients with supratherapeutic INRs, whenever possible, attempt to lower the INR to 2.5 or less
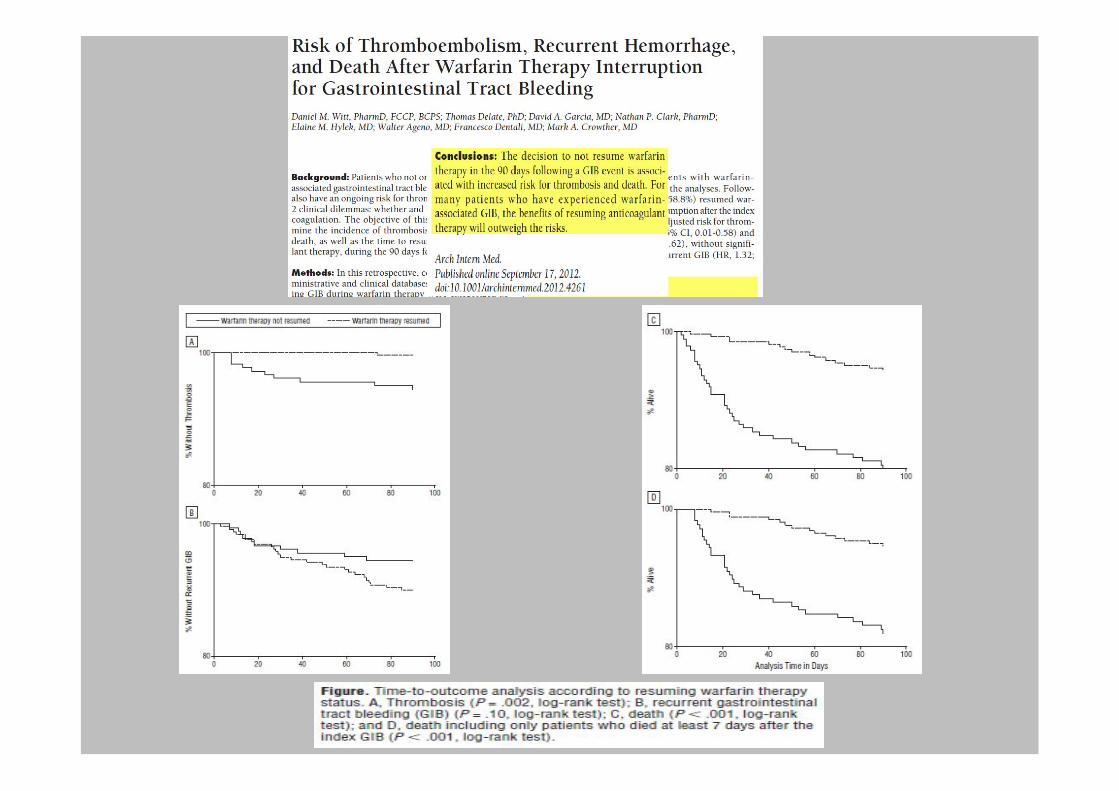
prior to endoscopic therapyRESUMPTION OF ANTICOAGULANTS
• Patients who resume anticoagulation have better overall outcomes than those who do not• If rapid resumption of anticoagulation is required in a patient at high risk for recurrent bleeding,
initial anticoagulation with UFH is preferable to warfarin or low molecular weight heparin due to its relatively short half-life and the ability to reverse anticoagulation with fresh frozen plasma if bleeding
• Patients who resume warfarin will require several days to achieve therapeutic levels of anticoagulation
• NOA will achieve therapeutic levels of anticoagulation within hours of administration

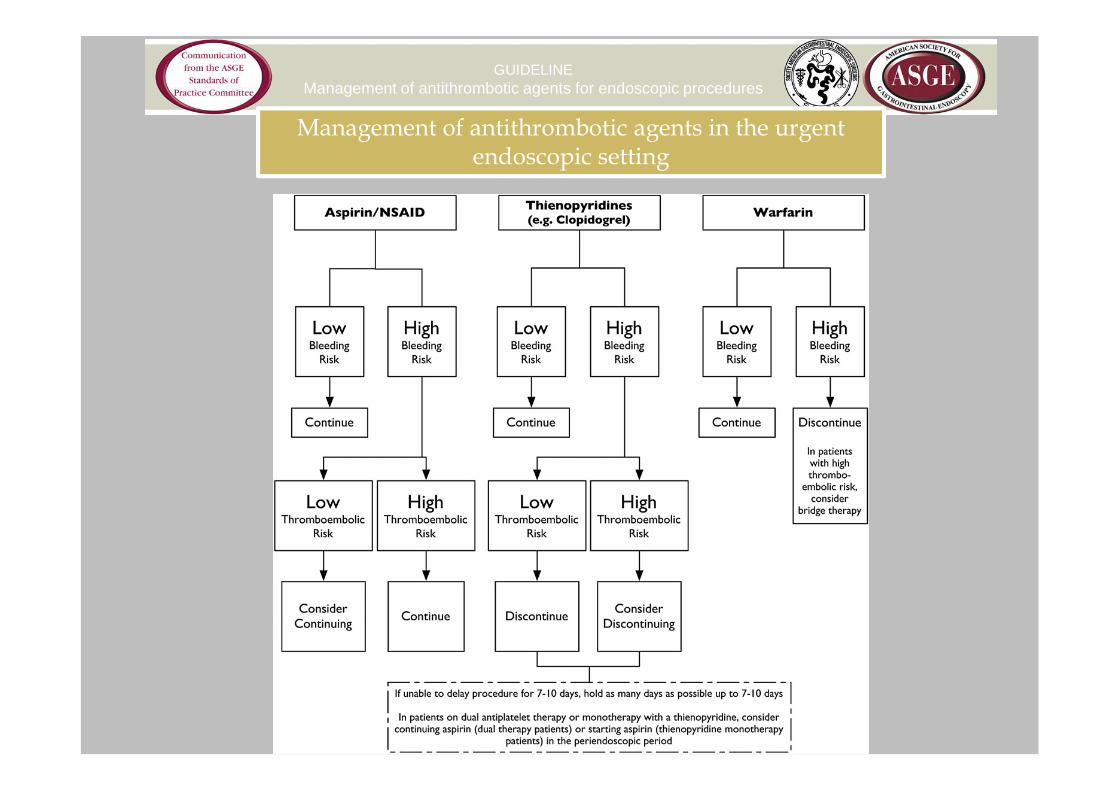
GUIDELINEManagement of antithrombotic agents for endoscopic procedures
Management of antithrombotic agents in the urgent endoscopic setting

• The risk of bleeding from endoscopic procedures can be classified as high orlow
• In general, diagnostic procedures are low-risk, whereas therapeuticprocedures are high-risk
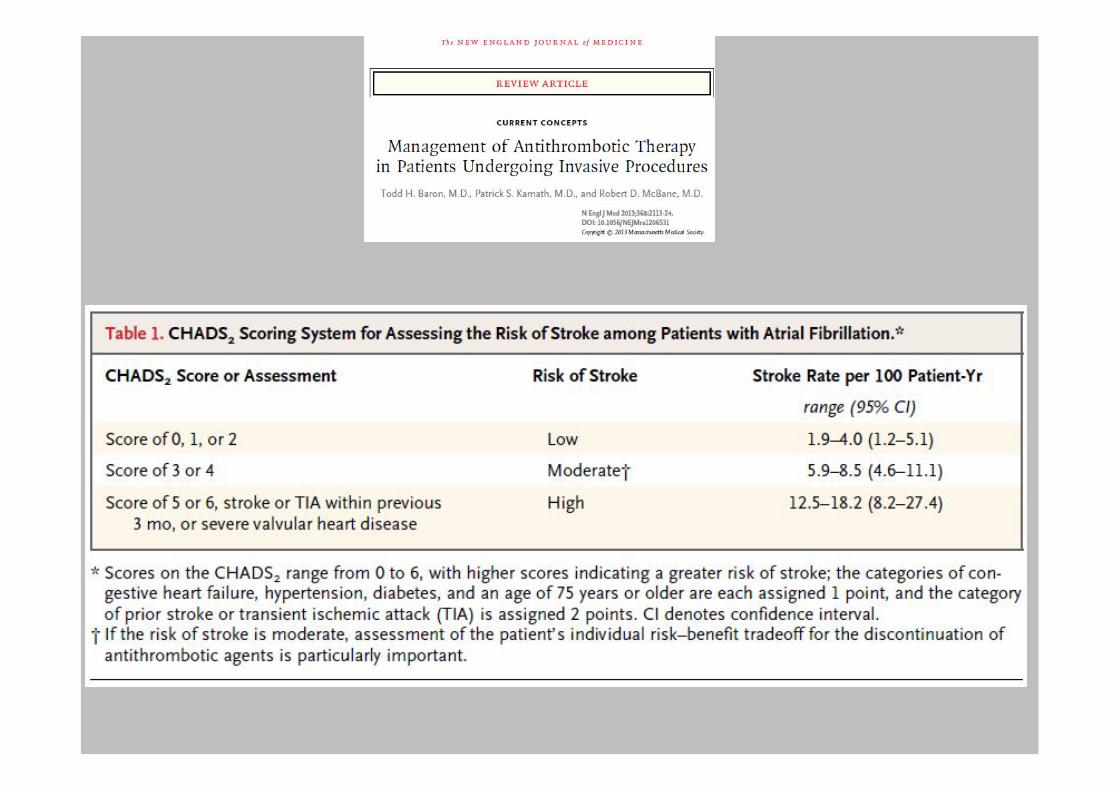
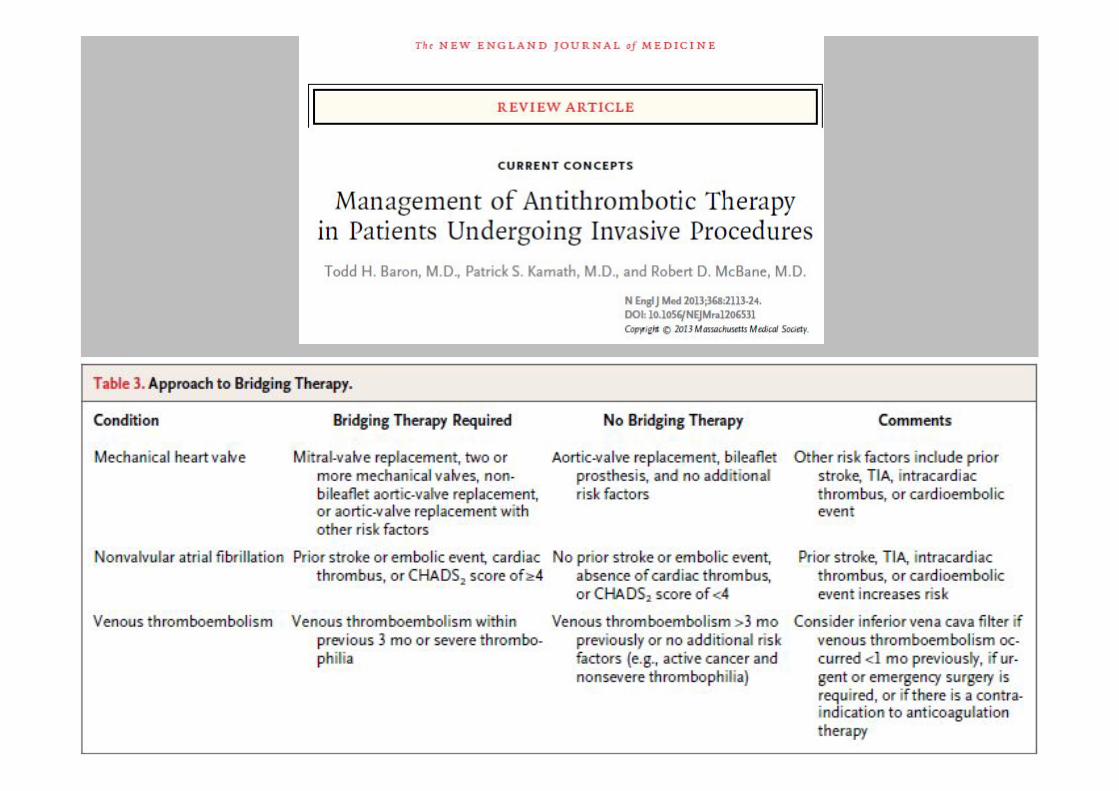
• The thromboembolic complication depends upon the preexisting condition
• For low-risk procedures no changes in anticoagulation but electiveprocedures be delayed if the INR is in the supratherapeutic range
• For high-risk procedures discontinue warfarin 5 days before and NOA 1 - 2days before the procedure in patients with normal renal function
• Bridge therapy is not required for patients at low-risk for thromboembolism
• For patients at high-risk for thromboembolism, bridge therapy is suggested

• Aspirin and NSAIDs may be continued for elective endoscopic procedures
• Stop of a thienopyridine need consultation with a cardiologist
• If a thienopyridine is going to be held for a procedure, it should be stopped7 to 10 days prior to the procedure
• For patients on dual antiplatelet therapy with a thienopyridine and aspirinundergoing high-risk procedures, if the thienopyridine is going to be held,it is suggested continuing the patient on aspirin
• Following the procedure, the thienopyridine should be restarted as soon asit is deemed safe