Embed Size (px)
Citation preview

The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
2008;90:163-174. doi:10.2106/JBJS.H.00753 J Bone Joint Surg Am.Raghuram Thonse and Janet D. Conway
Nonunions and Segmental Bone DefectsAntibiotic Cement-Coated Nails for the Treatment of Infected
This information is current as of December 20, 2008
Reprints and Permissions
Permissions] link. and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery

COPYRIGHT © 2008 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
163
Antibiotic Cement-Coated Nails for the Treatment of Infected
Nonunions and Segmental Bone DefectsBy Raghuram Thonse, MS(Orth), DNB(Orth), FRCS(Glasg), FRCS(Ed), and Janet D. Conway, MD
Introductionreatment of infected nonunions is a challenge faced bymany orthopaedic surgeons. Traditionally, the treat-ment strategy has been control of the infection fol-
lowed by procedures to achieve osseous union. Débridement,antibiotic-impregnated cement beads, and intravenous antibi-otics have been used for the control of the infection1-3. Externalor internal fixation methods have been used to achieve stabil-ity to promote union. Antibiotic cement-coated intramedul-lary nails can be used to treat the infection with high doses oflocal antibiotics and to provide bone stability4. Use of thesedevices allows immediate weight-bearing and prevents manycomplications associated with external fixation, such as pin-track infections and joint stiffness. This novel approach to thetreatment of infected nonunions was developed to minimizethe number of additional surgical procedures required for in-fection control and to achieve bone union. We present our se-ries of fifty-two patients in whom an antibiotic cement-coatedintramedullary nail was inserted for the treatment of an in-fected nonunion or segmental bone defect.
Materials and MethodsPreoperative Planning
areful preoperative planning is essential. It is essential todetermine if the patient has a history of allergy to antibi-
otics so that those antibiotics are not used when mixing thebone cement. The evaluation of intraoperative culture andsensitivity results guides the selection of the appropriate post-operative intravenous antibiotics.
Preoperative radiographs, including anteroposteriorand lateral views of the involved bone and full-length standinganteroposterior views of both lower extremities made with a130-cm cassette, should be evaluated. This evaluation allowsthe surgeon to determine the size of the intramedullary nailthat should be used and also provides information regardingthe need for additional procedures (such as deformity correc-
tion). The length of the intramedullary nail is determinedwith the same standard method as is used to determine thelength of an interlocking nail. For example, when antegradenailing of the femur is performed, the nail’s length should bethe same as the distance from the piriformis fossa to the distalfemoral physeal scar.
Proper preoperative planning allows the surgeon to pre-pare the antibiotic cement-coated nail while the other mem-bers of the operating team prepare the patient for surgery. Thecement coating on the nail can then harden on the clean backtable while the surgeon performs a thorough débridement ofthe infected bone and the soft tissues followed by copious lav-age. Once débridement is complete, the instruments that wereused for the “dirty” portion of the procedure are removed andthe patient’s limb is prepared again and draped. The surgeonand the rest of the operating team change all gowns andgloves. The “clean” portion of the procedure then begins, usu-ally by the surgeon inserting the antibiotic cement-coated nail.
Two methods have been used to prepare the antibioticcement-coated intramedullary nails. Initially, the antibioticcement-coated nails were prepared with a reusable mold (themold technique, or Method 1). The second generation of anti-biotic cement-coated nails was prepared with use of dispos-able silicone tubing (the silicone tubing technique, or Method2). The intraoperative time required to prepare a nail with useof Method 2 is approximately ten minutes, which is substan-tially less than the time required to prepare a nail with Method1 (one hour). Additional advantages of Method 2 include theuniformity and improved reliability of the coating. There havebeen no instances of insertional debonding of nails made withMethod 2.
All antibiotic cement-coated nails were made with useof the same antibiotic combination of 3.6 g of tobramycin and1 g of vancomycin per 40-g package of cement, except for twopatients who had a history of allergy to vancomycin. Extramonomer (3 to 4 mL) was necessary for mixing the large
T
C
Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. One or more of the authors, or a member of his or her immediate family, received, in any one year, payments or other benefits of less than $10,000 or a commitment or agreement to provide such benefits from a commercial entity (Quantum Medical Concepts). No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, division, center, clinical practice, or other charitable or nonprofit organization with which the authors, or a member of their immediate families, are affiliated or associated.
J Bone Joint Surg Am. 2008;90 Suppl 4:163-74 • doi:10.2106/JBJS.H.00753
Thonse.fm Page 163 Wednesday, October 15, 2008 12:52 PM

164
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
Fig. 1-A Fig. 1-B
Fig. 1-C Fig. 1-D
Fig. 1-E Fig. 1-F
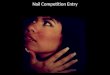
Figs. 1-A through 1-K The mold technique (Method 1). Figs. 1-A and 1-B Molds are coated with sterile ultrasound gel. Figs. 1-C and 1-D Cement powder is sprinkled over the ultrasound gel, and excess powder is removed. Figs. 1-E and 1-F Powdered antibiotics and cement powder are mixed with monomer in a cement gun until the mixture is homogeneous. The cement gun is used to apply the antibiotic-impregnated cement to both sides of the mold. The nail is then inserted into one of the molds.
Thonse.fm Page 164 Wednesday, October 15, 2008 12:52 PM

165
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
quantity of antibiotics with the cement. Commercially avail-able interlocking nails, including femoral (antegrade or retro-grade), knee arthrodesis, tibial, and ankle arthrodesis nails,were selected for the specific condition of each patient.
Molds were used to provide a uniform 1-mm-thick ce-ment mantle circumferentially around the intramedullarynail, starting from just distal to the proximal interlockingholes and extending to the tip of the nail. Molds composed en-tirely of stainless steel were obtained from Biomet (Warsaw,Indiana). All mold sizes accommodated an increase in nail di-ameter of 2 mm. The mold templates were 12 mm in width forthe knee arthrodesis, tibial, and ankle arthrodesis nails. Thefemoral mold was 14 mm in diameter to accommodate a 12-mm-diameter nail.
Method 1 (Mold Technique)The antibiotic cement-coated nail is prepared on a sterile table(Figs. 1-A through 1-K). A thin layer of sterile ultrasound gel(AQUAGEL; Parker Laboratories, Fairfield, New Jersey) issmeared on the mold. We used Surgilube (Fougera, Melville,New York) for the initial cases, but it caused pitting of the ce-ment surface. Dry cement powder is sprinkled over the coatedmold, and the excess cement powder is shaken off the mold.
In all cases in which Method 1 was used, a 12 by 36-cmmold was used to coat a 10-mm-diameter tibial nail, a 14 by42-cm mold was used to coat a 12-mm-diameter femoral nail(either antegrade or retrograde), a 12 by 75-cm mold was usedto coat a 10-mm-diameter knee arthrodesis nail, and a 12 by24-cm mold was used to coat a 10-mm-diameter ankle arthro-desis nail. All femoral nails and knee arthrodesis nails andsome tibial nails were manufactured by Biomet. TriGen in-tramedullary nails (Smith and Nephew, Memphis, Tennessee)were also coated with the use of the tibial mold. The decisionto use a TriGen intramedullary nail instead of a Biomet in-tramedullary nail was based on the proximal triplanar lockingpattern and matte finish of the TriGen nail.
Two packages of cement are required for ankle arthrod-esis, femoral, and tibial nails, whereas knee arthrodesis nailsrequire as many as three packages. The antibiotics are mixedwith the cement powder. The vacuum cement mixer is used tomix the cement powder containing antibiotics with the ce-ment liquid. Often, extra monomer (3 to 4 mL) is needed toallow adequate mixing of the Palacos bone cement (Zimmer,Warsaw, Indiana) with the antibiotic powder. The Palacos ce-ment is mixed in a standard fashion with use of a vacuummixing technique.
The nozzle of the cement gun is used to insert the anti-biotic-impregnated bone cement into the slots of the molds.The interlocking nail selected for the patient is carefullyplaced into one of the slots. The second mold is placed overthe first mold, and the two are gently pressed together while
Fig. 1-G
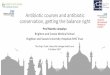
The mold is closed carefully while ensuring that the nail is still centered
in it. The insertion threads of the proximal part of the nail are kept free
of cement by placing the insertion bolt into the proximal nail threads.
Fig. 1-H
Figs. 1-H and 1-I The mold is opened carefully and excess cement is removed with an osteotome.
Fig. 1-I
Thonse.fm Page 165 Wednesday, October 15, 2008 12:52 PM

166
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
the cement is allowed to set. Before the nail is placed in themold, the threaded bolt of the interlocking nail insertion jigshould be inserted into the proximal end of the nail to pre-vent inadvertent coating of the threads on the inside of theproximal part of the intramedullary nail. In the initial cases,an attempt was made to keep the interlocking holes free ofcement by placing screw-sized pins into the holes andthrough the mold. It later became clear that this was not nec-essary and could affect the uniformity of the cement mantle.Currently, the cement is allowed to fill the interlocking holes,which are subsequently drilled during insertion of the lock-ing screws into the nail as if one were inserting a normallocking screw.
After the cement has set, the two parts of the moldand the antibiotic cement-coated nail are separated withthe gentle use of osteotomes. A file is used on the cement tocreate a bullet-shaped tip. If there is an area of spotty cov-erage, newly prepared antibiotic-impregnated cement isused to cover this area.
Method 2 (Silicone Tubing Technique)This method of preparation of the antibiotic cement-coatednail involves the use of disposable silicone tubing (QuantumMedical Concepts, Portland, Oregon). The antibiotic-impreg-nated cement is prepared as it is in Method 1. The nozzle ofthe cement gun is used to insert the cement into the siliconetubing (with a 12.5-mm inner diameter), filling its entirelength (Fig. 2-A). Then the interlocking nail is inserted intothe silicone tubing. The tube with the nail inside is gentlyrolled on the sterile preparation table to ensure a uniform ce-ment mantle (Fig. 2-B). After the cement has set, the siliconetube is split longitudinally with a sharp knife (Fig. 2-C), andthe antibiotic cement-coated nail is removed. Excess cementthat is present beyond the tip of the nail is removed with useof an osteotome, and the tip is filed to a smooth bullet shapeas it is in Method 1.
Insertion of the NailThe insertion technique is similar to that for an interlocking
Fig. 1-J
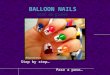
Figs. 1-J and 1-K The tip is filed to a bullet shape for ease of insertion, and the nail is mounted on the insertion jig. The antibiotic cement-coated
nail is ready for insertion.
Fig. 1-K
TABLE I Demographic Characteristics of Patients Treated with an Antibiotic Cement-Coated Nail
Mold Technique (Method 1)
Silicone Tubing Technique (Method 2)
No. of patients (M, F) 32 (23, 9) 20 (17, 3)
Mean age (range) (yr) 46.5 (16-86) 45.7 (19-80)
Host status5 (no. of patients)
A 8 6
B 24 14
Mean duration of follow-up (range) (mo) 22.5 (2-60) 4.5 (1-12)
Type of bone involvement (no.)
Nonunion 17 17
Segmental bone defect 15 (avg. size, 8.63 cm; range, 1-30 cm) 2 (sizes, 6 cm and 1.5 cm)
Acute fracture after external fixation 1
Thonse.fm Page 166 Wednesday, October 15, 2008 12:52 PM

167
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
nail. The medullary canal of the bone is reamed to a diameterthat is at least 2 mm greater than the diameter of the antibioticcement-coated nail. One millimeter of cement coating is pro-vided around the nail; therefore, the final diameter of the anti-biotic cement-coated nail is 2 mm larger than that of theintramedullary nail. For example, after a 10-mm-diameternail is coated with cement, it will have a total diameter of 12mm and the canal will be reamed to 14 mm.
The antibiotic cement-coated nail is mounted on theinsertion jig that is provided with the interlocking-nail in-strumentation. The guidewire used for reaming is removed.The antibiotic cement-coated nail is inserted in the samemanner as is employed for unreamed nailing. The cement oc-cludes the cannulated portion of the intramedullary nail, pre-venting its insertion over a guidewire, and it is inserted withuse of a combination of direct inspection, palpation, and in-traoperative fluoroscopy. Proximal locking is performed withthe help of the insertion guide of the interlocking nail. Distallocking is performed with a freehand technique and use ofimage intensification.
The cement might separate from the intramedullarynail (i.e., there might be cement-nail debonding) duringits insertion. Proper preparation of the canal, includingoverreaming, can prevent this. If debonding does occur, it canbe dealt with by removing the nail and the cement and prepar-ing a new antibiotic cement-coated nail.
Removal of the NailThe antibiotic cement-coated nail can remain in the medul-lary canal indefinitely after the dual goals of control of the in-fection and union have been achieved. If both infection andnonunion persist, the nail is exchanged for another antibioticcement-coated nail, generally six to eight weeks after the index
surgery. If removal of an antibiotic cement-coated nail is indi-cated, it is performed in a standard fashion with care taken toprevent cement-nail debonding. If debonding occurs, the ce-ment mantle can be removed with reasonable ease by using aJ-hook from the revision cemented total hip arthroplasty in-strument set (Moreland Cemented Instruments; DePuy Or-thopaedics, Warsaw, Indiana). Use of an image intensifiergreatly facilitates this process.
Tips for Preparation and Insertion of the Antibiotic Cement-Coated Nail1. Overream the medullary canal of the bone by 2 mm (the in-tramedullary nail diameter plus an additional 2 mm for thecement coating plus 2 mm) for ease of insertion.
Fig. 2-B
An intramedullary nail is inserted into the silicone tubing and rolled
carefully in the tubing to ensure a uniform coating.
Fig. 2-C
The silicone tubing is cut and peeled off. The antibiotic cement-coated
nail is mounted on the insertion jig and is ready for insertion.
Fig. 2-A
Figs. 2-A, 2-B, and 2-C The silicone tubing technique (Method 2).
Fig. 2-A After the cement is mixed as it is in Method 1, the cement gun
is used to insert the cement into silicone tubing that has a 12.5-mm in-
ner diameter.
Thonse.fm Page 167 Wednesday, October 15, 2008 12:52 PM

168
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
TABLE II Types of Intramedullary Nails Used to Create Antibiotic Cement-Coated Nails
Type of Intramedullary Nail
No. of Nails
Mold Technique (Method 1)
Silicone Tubing Technique (Method 2) Total
Ankle arthrodesis nail 7 9 16
Tibial nail 7 4 11
Femoral antegrade nail 7 3 10
Knee arthrodesis nail 9 3 12
Femoral retrograde nail 2 1 3
Fig. 3-B
Fig. 3-A
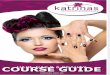
Fig. 3-A Anteroposterior radiograph of a twenty-five-year-old man who sustained a Grade-IIIB28 femoral fracture in a motor-vehicle collision. He was
treated with a rotational flap and split-thickness skin graft. Infection and nonunion of the left femur developed. Fig. 3-B Lateral (left) and antero-
posterior (right) radiographs made before the index operation.
Thonse.fm Page 168 Wednesday, October 15, 2008 12:52 PM

169
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
2. While preparing the antibiotic cement-coated nail,maintain a low room temperature to allow more workingtime.
3. Do not forget to add additional monomer when com-bining large quantities of antibiotic powder with cement.
4. Do not use Surgilube in place of ultrasound gel. Itcauses pitting in the cement coating.
5. Use the bolt from the insertion device while preparingthe antibiotic cement-coated nail to prevent cement fromclogging the insertion threads.
6. Do not ream out interlocking holes before insertionof the antibiotic cement-coated nail; the cement mantle might
fragment. This does not occur when the interlocking holes aredrilled after the insertion of the antibiotic cement-coated nailinside the bone.
Tips for Removal of the Antibiotic Cement-Coated Nail1. If cement debonds during removal, the J-hook from the ar-throplasty cement-removal set is the most effective instru-ment for removal of the cement.
2. If initial attempts to remove residual cement withthe arthroplasty cement-removal instruments have failed,the cement can be removed with sequential reaming and
Fig. 3-C
Anteroposterior (left) and lateral (right) radiographs made immediately after the surgery. At the time of surgery, the medial bridge had healed but tis-
sue suspicious for infection was noted. Before the surgical site was opened, a Reamer/Irrigator/Aspirator System (Synthes USA, West Chester,
Pennsylvania) was used to harvest bone graft. An antibiotic cement-coated nail was inserted, and antibiotics and bone morphogenetic protein-2
(BMP-2) were added to the bone graft.
Thonse.fm Page 169 Wednesday, October 15, 2008 12:52 PM

170
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
subsequent copious irrigation of the canal with use of canal-tip pulsed lavage.
3. A distal vent hole or channel is often necessary tocompletely remove all retained cement if one must resort toreaming the cement coating.
Resultsfter receiving approval by our institutional review board,we performed a retrospective study of fifty-two (twelve fe-
male and forty male) patients who had undergone treatmentwith an antibiotic cement-coated nail between 2002 and 2007.Thirty-four infected nonunions or arthrodesis sites and seven-teen infected segmental bone defects were treated. One patienthad an acute fracture that was initially treated with externalfixation. The initial cause of the nonunion and infection inthese patients was trauma (Figs. 3-A through 3-D), chronicosteomyelitis, chronic infection after total knee arthroplasty,
and infection in an ankle with Charcot arthropathy. The aver-age patient age was 46.2 years (range, sixteen to eighty-sixyears). According to the clinical staging system described byCierny et al.5, fourteen patients had a host status of A andthirty-eight patients had a host status of B. The demographiccharacteristics of the patients treated by the two methods areshown in Table I. The average duration of follow-up was 22.5months for the patients treated with Method 1, 4.5 months forthose treated with Method 2, and 15.6 months (range, one tosixty months) for the combined groups.
The interlocking nail that was used depended on theanatomic site. The types used most often were ankle andknee arthrodesis nails (Table II). The most common isolatedorganism was methicillin-resistant Staphylococcus aureus.Multiple organisms were isolated from a large number of pa-tients (Table III).
Two of the fifty-two patients were lost to follow-up, and
A
Fig. 3-D
Postoperative anteroposterior (left) and lateral (right) radiographs. The infection was eradicated, and the bone has healed.
Thonse.fm Page 170 Wednesday, October 15, 2008 12:52 PM

171
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
one who had had a cement spacer inserted in situ was ex-cluded from some of the analyses. Osseous union wasachieved in 84% (forty-one) of the forty-nine remaining pa-tients. Eight patients had a nonunion; three of these patients
had a stable nonunion, two had a pending union, two under-went above-the-knee amputation, and one had an unstablenonunion. Including those with a stable nonunion, 90%(forty-four) of the forty-nine patients were able to walk on the
TABLE V Additional Procedures to Treat Infection
Procedure
No. of Procedures
Mold Technique (Method 1) (N = 32)
Silicone Tubing Technique (Method 2) (N = 20) Total
Nail removal 3 0 3
Débridement 2 1 3
Exchange to an antibiotic cement-coated nail 5 2 7
Above-the-knee amputation 2 0 2
TABLE IV Results
Percent of Patients (No./Total No. in Group)
Entire Series(Methods 1 and 2)
Mold Technique (Method 1)
Silicone Tubing Technique (Method 2)
Bone union achieved* 84% (41/49) 86% (25/29) 95% (19/20)
Infection eradicated 85% (44/52) 78% (25/32) 80% (16/20)
Additional procedure needed to treat infection or nonunion
27% (14/52) 38% (12/32) 15% (3/20)
Only index antibiotic-coated nail required 73% (38/52) 63% (20/32) 85% (17/20)
*Two patients were lost to follow-up, and one patient with a cement spacer was excluded.
TABLE III Isolated Organisms
Isolated Organism
No. of Organisms
Mold Technique (Method 1) (N = 32)
Silicone Tubing Technique (Method 2) (N = 20)
Multiple organisms 11 4
Methicillin-resistant Staphylococcus aureus 17 13
Pseudomonas 1 2
Enterobacter 4 1
Escherichia coli 3 0
Serratia marcescens 3 0
Acinetobacter 1 2
Group-B Streptococcus 3 0
Enterococcus 2 0
Coagulase-negative Staphylococcus 2 3
Staphylococcus aureus 3 0
Streptococcus viridans 1 0
Morganella 1 0
Corynebacterium 2 0
Micrococcus 1 0
Proteus 0 2
Citrobacter 1 0
Klebsiella 0 1
Thonse.fm Page 171 Wednesday, October 15, 2008 12:52 PM

172
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
operatively treated extremity. The infection was controlled in85% (forty-four) of the fifty-two patients (Table IV). The in-dex surgery with the antibiotic cement-coated nail was theonly procedure required in 73% (thirty-eight) of the fifty-twopatients.
Additional procedures for the treatment of infectionand/or nonunion were required in 27% (fourteen) of thefifty-two patients. These additional procedures included ex-change to a new antibiotic cement-coated nail, additionaldébridement, and removal of the intramedullary nail (TableV). Bone graft was used to hasten union after control of theinfection in some cases (Table VI). Two patients underwentabove-the-knee amputation because the infection was onlypartially controlled. The overall limb salvage rate was 96%(fifty of fifty-two).
More patients treated with Method 1 (the mold tech-nique) underwent additional procedures to control the infec-tion. Twelve procedures were performed in the thirty-twopatients who had been treated with Method 1 compared withthree procedures in the twenty patients who had been treatedwith Method 2. We believe that this difference is due to thegreater number of patients in the Method-1 group who hadbone defects as well as infections with multiple organisms.
ComplicationsThe most common complication associated with both meth-ods was cement-nail debonding during the removal of the an-tibiotic cement-coated nail (nine cases) (Table VII). There wasretention of cement in two patients after nail removal. The ce-ment in these patients was removed with sequential reaming
and subsequent copious irrigation of the canal with use ofcanal-tip pulsed lavage. A distal vent hole or channel was nec-essary in these cases to facilitate complete removal of all re-tained cement. Incarceration of the antibiotic cement-coatednail during insertion occurred in one patient because ofimproper reaming. This was treated by splitting the anteriorfemoral cortex, removing the antibiotic cement-coated nail(without debonding), overreaming the canal, and reinsertingthe nail. This patient had not required any additional surgeryby the time of writing. Twenty-five percent (thirteen) of thefifty-two patients had complications specific to the antibioticcement-coated nail.
Discussionnfected nonunions require procedures to control the infec-tion, to provide stability, and to achieve union. Surgical dé-
bridement and delivery of antibiotics locally and systemicallyare used to control the infection. Local antibiotic therapy re-sults in high local concentrations of antibiotics with minimalsystemic levels2. Antibiotic-impregnated polymethylmethac-rylate beads are used in the treatment of osteomyelitis andopen fractures3,6. However, a second procedure is required toremove the beads. Other methods of local antibiotic deliveryinclude use of bioabsorbable delivery vehicles such as calciumsulfate and synthetic polymers2,7. New synthetic bioabsorb-able delivery vehicles are being developed to avoid the need fora second surgical procedure and, in some cases, to promoteosseous union8-14.
At present, cement containing sufficient concentrationsof antibiotics to achieve local control of infection is not com-mercially available. If antibiotic-impregnated bone cement isneeded to treat infection, the surgeon must prepare the ce-ment by using high doses of various antibiotics.
Aminoglycosides and vancomycin are common choicesfor local delivery because of their broad spectrum of activity,heat stability, and low allergenicity2. Palacos bone cement(Zimmer) has been found to elute antibiotics more effectivelythan Simplex bone cement (Howmedica-Stryker, Rutherford,New Jersey)15. Antibiotic elution from the polymethyl-methacrylate beads follows a biphasic pattern, with an initialrapid phase followed by a secondary phase after five to tendays16. The safety of local antibiotic therapy has been docu-mented in clinical studies. Both animal and clinical studies
I
TABLE VI Additional Procedures (Bone-Grafting with or without Additional Fixation) to Achieve Union
Percent of Patients (No./Total No. in Group)*
Mold technique (Method 1) 21% (6/29)
Silicone tubing technique (Method 2)
20% (4/20)
Entire Series (Methods 1 and 2) 20% (10/49)
*Two patients were lost to follow-up, and one patient with a ce-ment spacer was excluded.
TABLE VII Types of Complications Encountered with Antibiotic Cement-Coated Nails
Mold Technique (Method 1)
Silicone Tubing Technique (Method 2)
Percent of patients with a complication (no./total no. in group)
31% (10/32) 15% (3/20)
No. of complications
Cement-nail debonding with nail removal 7 2
Debonding with nail insertion 1 0
Retained cement 2 0
Nail incarceration with insertion 0 1
Thonse.fm Page 172 Wednesday, October 15, 2008 12:52 PM

173
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
have shown high local concentrations and undetectable orvery low serum levels of the locally delivered antibiotics with-out systemic toxicity2,12.
Vancomycin and tobramycin are effective against manyof the bacteria that were generally found in our patients (TableIII). These antibiotics have been shown to be heat stable, withgood elution properties from bone cement, and to have fewadverse effects on bone-healing1,2,7,15,17,18. In addition, we ad-minister cefazolin intravenously during the immediate post-operative period until we receive the results of culture andsensitivity testing of the samples sent at the time of surgery.The systemic antibiotics are then changed as necessary, in con-sultation with an infectious disease specialist. In general, thesystemic antibiotics are administered for six weeks or untilthere is a reduction in the levels of inflammatory markers suchas C-reactive protein. Further treatment with oral antibioticsis given if recommended by the infectious disease specialist.
Infected nonunions have traditionally been treatedwith external or internal fixation19. However, a high preva-lence of pin-site infections, muscle contractures, and jointstiffness has been observed in association with externalfixation20–22. Some patients might not consent to the use of ex-ternal fixators, while others might not be ideal candidates forexternal fixation because of obesity or an expectation of poorcompliance. The use of antibiotic cement-coated nails bene-fits these patients.
Use of an intramedullary nail with antibiotic-impreg-nated cement beads has been reported for the treatment of in-fected nonunions23,24. This method entails a second procedurefor removal of the beads or spacer. Antibiotic-impregnatedcement-coated guide rods made with use of a chest tube as atemplate allow control of infection25. However, a second surgi-cal procedure is necessary to remove the guide rod and insertthe intramedullary nail to provide adequate stability for heal-
ing of the nonunion. The use of an Ender or Küntscher nailcoated with antibiotic-impregnated cement has also beenreported26,27. However, these nails do not provide adequate sta-bility for healing of the nonunion in all cases.
Both methods used to prepare the antibiotic cement-coated intramedullary nails in the present study are effective;however, the silicone tubing method produces a more reliablecoating, is associated with fewer complications related to in-sertion, and requires less intraoperative time to prepare (tenminutes instead of one hour with the mold technique). It iscurrently our method of choice.
Overall, the antibiotic cement-coated intramedullarynails are very effective for treating infected nonunions andsegmental bone defects. These conditions would normally re-quire long periods of external fixation and often bone trans-port. Our method is associated with a 27% risk that anadditional procedure will be needed to treat the infection ornonunion. This is an acceptable risk given the difficult natureof the initial problem and the higher risk of complications andadditional surgical procedures associated with circular exter-nal fixators22. The only disadvantage of the antibiotic cement-coated nail appears to be cement-nail debonding during nailremoval. The arthroplasty cement-removal instruments havebeen very effective for removal of cement. Future endeavorsare being directed at improving the cement-nail interface.
Raghuram Thonse, MS(Orth), DNB(Orth), FRCS(Glasg), FRCS(Ed)Musgrave Park Hospital, Belfast BT9 7JB, United Kingdom. E-mail address: [email protected]
Janet D. Conway, MDRubin Institute for Advanced Orthopedics, Sinai Hospital, 2401 West Belvedere Avenue, Baltimore, MD 21215. E-mail address: [email protected]
References
1. Patzakis MJ, Zalavras CG. Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: current management concepts. J Am Acad Orthop Surg. 2005;13:417-27.
2. Zalavras CG, Patzakis MJ, Holtom P. Local antibiotic therapy in the treatment of open fractures and osteomyelitis. Clin Orthop Relat Res. 2004;427:86-93.
3. Beals RK, Bryant RE. The treatment of chronic open osteomyelitis of the tibia in adults. Clin Orthop Relat Res. 2005;433:212-7.
4. Thonse R, Conway J. Antibiotic cement-coated interlocking nail for the treat-ment of infected nonunions and segmental bone defects. J Orthop Trauma. 2007;21:258-68.
5. Cierny G 3rd, Mader JT, Penninck JJ. A clinical staging system for adult osteo-myelitis. Contemp Orthop. 1985;10:17-37.
6. Henry SL, Ostermann PA, Seligson D. The prophylactic use of antibiotic impreg-nated beads in open fractures. J Trauma. 1990;30:1231-8.
7. Hanssen AD. Local antibiotic delivery vehicles in the treatment of musculoskel-etal infection. Clin Orthop Relat Res. 2005;437:91-6.
8. Hendricks KJ, Lane D, Burd TA, Lowry KJ, Day D, Phaup JG, Anglen JO. Elution characteristics of tobramycin from polycaprolactone in a rabbit model. Clin Or-thop Relat Res. 2001;392:418-26.
9. Rutledge B, Huyette D, Day D, Anglen J. Treatment of osteomyelitis with local antibiotics delivered via bioabsorbable polymer. Clin Orthop Relat Res. 2003;411:280-7.
10. Gürsel I, Korkusuz F, Türesin F, Alaeddinoglu NG, Hasirci V. In vivo application of biodegradable controlled antibiotic release systems for the treatment of im-plant-related osteomyelitis. Biomaterials. 2001;22:73-80.
11. Shirtliff ME, Calhoun JH, Mader JT. Experimental osteomyelitis treatment with antibiotic-impregnated hydroxyapatite. Clin Orthop Relat Res. 2002;401:239-47.
12. Mader JT, Stevens CM, Stevens JH, Ruble R, Lathrop JT, Calhoun JH. Treat-ment of experimental osteomyelitis with a fibrin sealant antibiotic implant. Clin Orthop Relat Res. 220;403:58-72.
13. Ambrose CG, Clyburn TA, Louden K, Joseph J, Wright J, Gulati P, Gogola GR, Mikos AG. Effective treatment of osteomyelitis with biodegradable microspheres in a rabbit model. Clin Orthop Relat Res. 2004;421:293-9.
14. Türesin F, Gürsel I, Hasirci V. Biodegradable polyhydroxyalkanoate implants for osteomyelitis therapy: in vitro antibiotic release. J Biomater Sci Polym Ed. 2001;12:195-207.
15. van Raaij TM, Visser LE, Vulto AG, Verhaar JA. Acute renal failure after local gentamicin treatment in an infected total knee arthroplasty. J Arthroplasty. 2002;17:948-50.
16. Nelson CL, Griffin FM, Harrison BH, Cooper RE. In vitro elution characteristics of commercially and noncommercially prepared antibiotic PMMA beads. Clin Or-thop Relat Res. 1992;284:303-9.
17. Perry AC, Prpa B, Rouse MS, Piper KE, Hanssen AD, Steckelberg JM, Patel R. Levofloxacin and trovafloxacin inhibition of experimental fracture-healing. Clin Or-thop Relat Res. 2003;414:95-100.
Thonse.fm Page 173 Wednesday, October 15, 2008 12:52 PM

174
THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 90-A · SU P P L E M E N T 4 · 2008AN T I B I O T I C CE M EN T-CO ATE D NA IL S F O R TH E TRE A T M E N T OF IN FE C TE D NO NU N ION S A N D SE G M EN T A L BO N E DEF E C T S
18. Lindsey RW, Probe R, Miclau T, Alexander JW, Perren SM. The effects of antibiotic-impregnated autogeneic cancellous bone graft on bone healing. Clin Orthop Relat Res. 1993;291:303-12.
19. Bose WJ, Gearen PF, Randall JC, Petty W. Long-term outcome of 42 knees with chronic infection after total knee arthroplasty. Clin Orthop Relat Res. 1995;319:285-96.
20. Green SA. Complications of external skeletal fixation. Clin Orthop Relat Res. 1983;180:109-16.
21. Herzenberg JE, Scheufele LL, Paley D, Bechtel R, Tepper S. Knee range of motion in isolated femoral lengthening. Clin Orthop Relat Res. 1994;301:49-54.
22. Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res. 1990;250:81-104.
23. Tandon SC, Thomas PB. Persistent osteomyelitis of the femur—2 cases of exchange intramedullary nailing with gentamicin beads in the nail. Acta
Orthop Scand. 1996;67:620-2.
24. Sundgren K. Cemented modular intramedullary nail in failed knee arthro-plasty—a report of 2 cases. Acta Orthop Scand. 1999;70:305-7.
25. Paley D, Herzenberg JE. Intramedullary infections treated with antibiotic cement rods: preliminary results in nine cases. J Orthop Trauma. 2002;16:723-9.
26. Ohtsuka H, Yokoyama K, Higashi K, Tsutsaumi A, Fukushima N, Noumi T, Ito-man M. Use of antibiotic-impregnated bone cement nail to treat septic nonunion after open tibial fracture. J Trauma. 2002;52:364-6.
27. Grimer RJ, Belthur M, Chandrasekar C, Carter SR, Tillman RM. Two-stage revi-sion for infected endoprostheses used in tumor surgery. Clin Orthop Relat Res. 2002;395:193-203.
28. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24:742-6.
Thonse.fm Page 174 Wednesday, October 15, 2008 12:52 PM