Embed Size (px)
Citation preview

Anaerobe 10 (2004) 155–164
ARTICLE IN PRESS
*Correspondi
7113918.
E-mail addre
1075-9964/$ - see
doi:10.1016/j.an
Clinical microbiology
Antibiotic-resistant Propionibacterium acnes on the skin of patientswith moderate to severe acne in Stockholm
Cristina Opricaa,b, Lennart Emtestamb, Jan Lapinsb, Erik Borglundc, Filippa Nybergc,Kajsa Stenlundd, Lena Lundeberge, Eva Sillerstr .oma, Carl Erik Norda,*
aDivision of Clinical Bacteriology, Department of Laboratory Medicine, Karolinska Institutet, Karolinska University Hospital Huddinge,
SE-14186 Stockholm, SwedenbDivision of Dermatology and Venereology, Department of Medicine, Karolinska Institutet, Karolinska University Hospital Huddinge,
Stockholm, SwedencV .allingby Medical Centre, Stockholm, Sweden
dDepartment of Medicine, Betania Foundation Hospital, Stockholm, SwedeneDivision of Dermatology and Venereology, Karolinska Institutet, Karolinska University Hospital Solna, Stockholm, Sweden
Received 21 August 2003; received in revised form 11 February 2004; accepted 13 February 2004
Abstract
The objective was to study the prevalence and antibiotic susceptibility patterns of Propionibacterium acnes strains isolated from
patients with moderate to severe acne in Stockholm, Sweden and to determine the diversity of pulsed-field gel electrophoresis types
among resistant P. acnes strains. One hundred antibiotic-treated patients and 30 non-antibiotic-treated patients with moderate to
severe acne participated in the investigation. Facial, neck and trunk skin samples were taken with the agar gel technique. The
susceptibility of P. acnes strains to tetracycline, erythromycin, clindamycin and trimethoprim-sulfamethoxazole was determined by
the agar dilution method. The genomic profiles of the resistant strains were determined by pulsed-field gel electrophoresis. In the
group of patients treated with antibiotics, resistant P. acnes strains were recovered in 37%, while in the non-antibiotic group of
patients the incidence of resistant strains was 13%. Thus antibiotic-resistant P. acnes strains were significantly more often isolated
from antibiotic-treated patients with moderate to severe acne than from non-antibiotic-treated patients (odds ratio, 3.8; P ¼ 0:01).There was a genetic diversity among the P. acnes strains. Forty-four different patterns of SpeI DNA digests were detected and two
predominant clones were found. P. acnes strains exhibited different antibiotic susceptibility patterns and identical genotypes or vice
versa. A person can be colonized with different strains with varying degrees of antibiotic resistance. The risk of increased resistance
of P. acnes must be considered when treating acne patients with antibiotics, and especially long-term therapy should be avoided.
r 2004 Elsevier Ltd. All rights reserved.
Keywords: Propionibacterium acnes; Resistance; Acne; Pulsed-field gel electrophoresis
1. Introduction
Acne vulgaris is a multifactorial disease in whichpropionibacteria, i.e. Propionibacterium acnes, whichform part of the resident cutaneous micro-flora, arethought to play an important role in the pathogenesis ofinflamed lesions [1]. Acne is a disorder of the pilosebac-eous follicle characterized by non-inflammatory (come-dones) and inflammatory lesions (papules, pustules and
ng author. Tel.: +46-8-58587838; fax: +46-8-
ss: [email protected] (C.E. Nord).
front matter r 2004 Elsevier Ltd. All rights reserved.
aerobe.2004.02.002
nodulocystic lesions). Epidemiological studies haveshown that up to 70–87% of the adolescents experienceacne vulgaris [2] but also adults and especially femalepatients [3,4]. 15–30% of acne patients need treatmentbecause of the severity of the disease and only in USA,between 1996 and 1998 the patients received 6.5 millionnew prescriptions for acne vulgaris with a total cost ofmore than USD 1 billion [5,6].Acne treatments, which act by interfering with the
growth and/or metabolism of propionibacteria, fall intotwo main categories: antibiotics and non-antibioticdrugs. Antibiotics have been used for over 40 yearsand are still widely prescribed. Until the late 1970s the

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164156
propionibacteria were uniformly susceptible to thera-peutically useful antibiotics [7]. Since then a relationshiphas been found between the carriage of resistant strainsand failure to respond to the treatment with thecorresponding antibiotic [8–10]. Poor clinical responsecan be also the result of poor compliance, inadequateduration of therapy, development of Gram-negativefolliculitis, resistance or a high sebum excretion rate.Studies since early 1980 from the Netherlands, UK,
USA, New Zealand and Japan have suggested a clearassociation between the emergence of resistance toclindamycin, tetracyclines, erythromycin and trimetho-prim–sulfamethoxazole in P. acnes and the therapeuticuse of these antibiotics [8–14]. It has been reported thatthe incidence of antibiotic resistance of P. acnes wasgradually increasing from 35% in 1991 to 60% in 1996,with a peak of 64% in 1997 [15,16]. A recent Europeanstudy shows that prescribing practices for acne affectresistant rates especially to the tetracyclines. Also,topical formulations of erythromycin and clindamycinused for acne treatment will induce a significantdissemination of cross-resistant P. acnes strains. Highestresistant rates have been found in Spain (94%), andlowest in Hungary (51%) [17]. The likelihood ofovergrowth of antibiotic-resistant strains of propioni-bacteria increases with the duration of therapy. Acnetreatments last several months, so the pressure on thenormal flora will be high. It is not uncommon to changethe first antibiotic after several weeks to another one, orto use concomitant oral and topical antibiotics [18]. Allthese practices will increase the number of multiresistantstrains. A good clinical effect of oral antibiotic can beobtained not earlier than after 4–8 weeks [19].Besides from a small study from the 1980s [20], little is
known about the situation in Scandinavia.The first objective of this study was to document the
prevalence of antibiotic resistance (tetracycline, erythro-mycin, clindamycin and trimethoprim–sulfamethoxa-zole) among isolates of P. acnes in patients from theStockholm area with moderate to severe acne who werecurrently being treated with systemic antibiotics duringthe last 2–6 months.The second objective was to determine the genomic
diversity and the epidemiological relatedness amongresistant P. acnes strains using pulsed-field gel electro-phoresis (PFGE).
2. Materials and methods
The study was conducted exclusively in the Stockholmarea. Patients were recruited at two open care units (theDermatology Clinics at V.allingby Medical Centre and atBetania Foundation Hospital) and at one universityhospital (the Division of Dermatology and Venereology
at the Karolinska University Hospital). The local ethicscommittee approved the study.
2.1. Patient selection for the study
All male and female patients enrolled into the study
* had to be 12–45 years of age,* had moderate to severe inflammatory acne (papulo-
pustular acne and nodular lesions),* had been on oral antibiotic therapy during the last
2–6 months,* were not allowed to use topical benzoyl peroxide or
topical antibiotic treatment.
The patients were informed orally and in writing andthey or their parents gave their oral and writteninformed consent to participate in the study.A control group of acne patients with the same
characteristics as above but without systemic/localantibiotics for the last 2 months was also enrolled.From March 1999 to May 2000, every patient with
acne visiting the participating centres was evaluated forthe study. The most common reason not to be enrolledinto the study was the use of topical antibacterial agents,especially the use of benzoyl peroxide. The total studypopulation during the period was estimated to 400patients with the diagnosis of acne.
2.2. Bacterial sampling
Sampling kits were provided to all investigators alongwith instructions of the appropriate sampling technique.Before the study, every nurse who was to be involved inthe sampling was personally instructed in the samplingtechnique.Three samples, from the facial, neck or trunk areas,
per patient were taken for the isolation of P. acnes. Thesites were recorded in the case record form. Whensampling for culture, a soft agar gel, with a cross-sectional area of approximately 2 cm2 was pressedagainst the skin surface for 10 s without rotation. Thena slice of the soft agar with the bacterial bearing surfacewas cut off, put into a sterile glass tube with prereducedbroth and immediately transported to the microbiolo-gical laboratory for bacterial cultivation. From theDermatology Clinics at V.allingby, Betania andKarolinska University Hospital Solna, the laboratorywas informed that a sample was on its way and thesamples reached the laboratory by a transport car onthe same day and were immediately processed. From theDivision of Dermatology at Karolinska UniversityHospital Huddinge, the samples were immediatelycarried by the research staff to the laboratory formicrobial analysis.

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164 157
2.3. Microbiological procedures
The prereduced broth carrying the bacterial load (3samples for each patient) was used to inoculate bloodagar plates (5% horse blood) for anaerobic cultivation(37�C, 7 days) of P. acnes. Then, from each plate strainswith different morphologies were identified [21]. Onecolony from each different strain was picked up andsubcultured. From each sample one or more strains wereisolated. P. acnes strains were identified by Gramstaining, catalase test, indole test, gas–liquid chromato-graphic analysis of metabolic end products and bio-chemical tests (Rapid-Ana II system, REMEL Inc.,Lenexa, KS, USA).After the identification and quantification, the iso-
lated strains were frozen (–70�C) and the susceptibilitytesting was done on all isolated strains at the same time.Thereby the minimum inhibitory concentration (MIC)of each antibiotic was determined by the agar dilutionmethod with PDM Antibiotic Sensitivity Medium agar(Biodisk, Solna, Sweden) and 5% defibrinated horseblood. Different antimicrobial concentrations wereobtained by incorporating each substance when prepar-ing the agar plates. The inocula consisted of 105CFU/mL applied to the agar plates with a modified Steersreplicator. An agar plate without antimicrobial agentwas used as a growth control. Agar plates wereincubated in anaerobic jars (GasPak; BBLMicrobiologySystem, Baltimore, MD, USA) for 48 h at 37�C [22].The MIC was determined as the lowest concentration ofthe antibiotic that inhibited bacterial growth completelyas judged by the eye. For quality control of theantibiotic tests the following strains were used: Clos-
tridium perfringens ATCC 13124, Bacteroides fragilis
ATCC 25285 and P. acnes ATCC 6919. The breakpointsused to define susceptibility or resistance followed therecommendations given by the European Committee onAntibiotic Susceptibility Testing (EUCAST) [23]. Re-sistance to tetracycline was defined at MIC X2mg/L, toclindamycin at MIC X0.25mg/L, erythromycin at MICX0.5mg/L and to trimethoprim/sulfamethoxazole atMIC X1mg/L.
2.4. Genotypic analyses with pulsed-field gel
electrophoresis
All the resistant strains (n ¼ 69) were molecular typedby pulsed-field gel electrophoresis [24].
2.5. DNA preparation
Cells of pure cultures were grown on sheep-bloodagar plates with glucose 5.8 g/L. Cells were takendirectly from the plates and suspended in EET buffer(100mM Na2EDTA, 10mM EGTA and 10mM Tris–HCl ) to 3–4� 109CFU/mL. The suspension was then
mixed with an equal volume of 2% low melting pointagarose (Sea Plaque GTC agarose, Bio WhittakerMolecular Application, Rockland, ME) and the mixturewas used for plugs preparation (20 mL mixture/disk).After chilling to 4�C for 15min, the solidified plugs weretransferred into 1mL lysis buffer (6mM Tris pH 7.5,0.5% lauroyl sarcosyn, 1% polyethylenglycol, 0.5% brii,0.2% deoxycholate) containing 625U/mL of mutanoly-sin (Sigma-Aldrich, Inc., St. Louis, MO) and 12.5mg/mL of lysozyme (Sigma-Aldrich, Inc., St. Louis, MO)and incubated for 6 h at 37�C. Mutanolysin in mixturewith lysozyme was necessary for inducing lysis [25]. Inthe lysis buffer polyethylene glycol was used that servesas an osmotic stabilizer and as an enhancer of the lysisprocess [26]. Lysis buffer was then replaced byproteolysis buffer: 1% SDS, 1mg/mL Protease (Sigma,St. Louis, MO). The proteolysis step was carried out at37�C for 12 h. The agarose plugs were washed four timeswith 10 mL T10E1 buffer (10mM Tris–HCl, 1mMNa2EDTA [pH 8]) at room temperature with gentleshaking. Plugs were stored at 4�C in 1mL fresh T10E1
buffer until use.
2.6. Restriction and gel electrophoresis
The DNA containing disks were digested 3 h with20U of SpeI (Promega, Madison, WI) at 37�C. Theplugs were loaded in a 1% agarose gel (SeaKemR GTGagarose, FMC BioProducts, Rockland, ME) dissolvedin 0.5�TBE buffer (130mM/L Tris, 45mM/L boricacid, 2.5mM/L EDTA) using a contour-clampedhomogenous electric field apparatus (Gene PathTM
System, Bio-Rad Laboratories, Hercules, CA). Therunning conditions were as follows: voltage gradient6V/cm, ramped with an initial switching time of 0.5 sand a final switching time 5 s for 16 h at 14�C, 120�
angle. The gels were stained with ethidium bromide(1 mg/mL) for 30min, destained in tap water (15min)and photographed under ultra-violet irradiation.
2.7. Computerized numerical analyses of PFGE data
Calculation of similarity matrices and creation ofdendrograms was done by aid of a Molecular AnalystSoftware program (Bio-Rad Laboratories) using theunweighted pair group method with arithmetic averages(UPGMA). The similarity coefficients were calculatedaccording to the method of Dice [27]. The isolates werealso visually inspected. P. acnes ATCC 6919 was used ascontrol for each gel experiment to allow comparisonsusing the Molecular Analyst Software program. Theclonal group level was set at X80% similarity. Capitalletters (A–H) were used to designate the main geneticlineages of P. acnes. The preparation and digestion ofDNA strains randomly chosen was repeated under thesame conditions to assess the reproducibility of the

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164158
method and identical results were obtained at the sametime.
2.8. Data analysis
Fisher exact test was used to compare the prevalenceof resistant strains between the two groups. Odds ratiofor these data was calculated from standard contingencytable with 95% confidence interval. Fisher’s exact testwas also used to compare the antibiotic resistancepattern of strains collected from treated and non-treatedpatients. w2 analysis was used to compare the carriage ofresistant strains in different age groups.Analysis was performed through the help of computer
software program Statistica version 6.0.
3. Results
General characteristics of the patients from bothgroups are shown in Table 1. Both males and femalepatients were evaluated.For both groups, acne lesions were most commonly
found only on the face (73% non-treated group/69%treated group) and both the face and back (16% non-treated group/13% treated group).Altogether 100 patients in the antibiotic-treated group
were evaluable; P. acnes was isolated in 82 of thesepatients (82%) and in 46% of the patients P. acnes wasisolated in all three samples. For the susceptibilitytesting, 201 strains of P. acnes were investigated.The most common antibiotic used was tetracycline
(97% patients). 2% of patients were treated witherythromycin and 1% with both antibiotics. Seventy-seven percent had only oral therapy, but 23% were alsotreated with topically retinoids.Thirty patients from the non-antibiotic treated group
were evaluable; P. acnes was isolated from 28 of themand in 22 of these patients in all three samples. Fromthis group of non-treated patients, 79 strains of P. acnes
were available for the susceptibility testing.
Table 1
Patient characteristics
Evaluable patients Antibiotic-treated
group
Non-treated
group
Gender
Male 42 12
Female 58 18
Age (yr)
Mean7SD 20.576.3 20.274.4
Range 13–49 13–29
Treatment duration (weeks)
Mean7SD 16.3711.7
3.1. Antimicrobial susceptibility
The range for the sensitivity of the four testedantibiotics and the MIC50 and MIC90 values of the201 strains isolated from the antibiotic-treated acnepatients and of the 79 strains isolated from the non-treated acne patients are shown in Table 2 and 3.As can be seen, there are strains highly resistant to
erythromycin and clindamycin but also to tetracycline inthe treated group of patients. No resistance againsttrimethoprim–sulfamethoxazole was detected. The fre-quency distribution of erythromycin MICs was bimodel0.032mg/L for sensitive strains and >128mg/L forresistant strains. For clindamycin: 0.032mg/L forsensitive strains and 0.25mg/L for resistant strains.Table 4 shows the number of isolates examined and theresistance profiles. Of the 201 isolates, 11 were resistantonly to clindamycin, three were resistant to erythromy-cin, five were resistant to tetracycline, 19 were resistantto clindamycin and erythromycin, and 18 were resistantto all three antibiotics.For the group of non-treated patients, MIC50 and
MIC90 were below the breakpoints for all testedantibiotics. In this group, there were six resistant strainsand the resistance profile is shown in Table 4. Threestrains were highly resistant both to clindamycin (MICsof 16mg/L) and to erythromycin (MICs>128mg/L);two strains had low resistance to clindamycin(MICs=0.25mg/L) and one strain was resistant totetracycline (MIC of 4mg/L) and trimethoprim-sulfa-methoxazole (MIC>2mg/L).Comparing the two groups, it can be noticed that in
the treated group there were strains with higher MICsfor clindamycin (64mg/L comparative with 16mg/L)and tetracycline (32mg/L comparative with 4mg/L): forerythromycin the range of sensitivity was the same(p0:0082 > 128mg/L) and for trimethoprim–sulfa-methoxazole the range was higher for the non-treatedgroup (4mg/L comparative with 0.5mg/L).Altogether, 37 of the antibiotic-treated 100 patients
(37%) were colonized by resistant strains of P. acnes andonly four of 30 of the non-treated patients (13%). Thus,a significant number of patients carried resistant strainsin the treated group (P ¼ 0:01). We calculated the oddsratio for these data at 3.8 (95% confidence inter-val=2:126:7). Of the 37 individuals, two harbouredmultiple resistant strains with different resistancepatterns (Table 5). The resistance profile for antibiotictreated patients showed that 14 patients carried resistantstrains to one antibiotic, 15 patients carried resistantstrains to two antibiotics and 10 patients to threeantibiotics. By comparison, no patient from the non-treated group carried strains resistant to all threeantibiotics (Table 5). There was no significant differencebetween the groups with regard to resistant pattern fordifferent antibiotics (P>0.05 using Fisher’s exact test).

ARTICLE IN PRESS
Table 2
Susceptibility against four antibiotics in 201 P. acnes strains isolated from 100 acne patients treated with systemic antibiotics for 2–6 months and in
79 strains of P. acnes isolated from 30 non-treated acne patients (in italics). The chosen breakpoints are according to the European Committee on
Antibiotic Susceptibility Testing (EUCAST)
Antibiotic Breakpoints Minimum Inhibitory Concentration (mg/L) MIC range
MIC 50 treated
group
MIC 50 non-
treated
MIC 90 treated
group
MIC 90 non
treated
Treated group Non-treated
CL 0.25 0.032 0.032 4 0.064 p0.008–64 p0.008–16
EM 0.5 0.032 0.032 >128 0.032 p0:0082 >128
p0.008 – >128
TCY 2 0.5 0.25 4 0.5 0.064–32 0.064–4
T/S 1 0.125 0.064 0.25 0.125 0.016–0.5 0.064 – >2
CL=clindamycin; EM=erythromycin; TCY=tetracycline; T/S=trimethoprim-sulfamethoxazole.
Table 3
Minimum inhibitory concentrations of four antibiotics against 201 isolates of P. acnes strains from treated patients and against 79 isolates of P. acnes
strains from non-treated patients (in parenthesis)
Numbers of isolates inhibited at MIC (mg/L) of
p0.008 0.008 0.016 0.032 0.064 0.125 0.25 0.5 1 2 4 8 16 32 64 128 >128
CLa 20 4 102 13 7 13b 11 6 3 6 7 8 1
(4) (67) (2) (1) (2) (3)
EMa 5 19 27 104 5 1 8 1 1 2 6 1 21
(14) (4) (1) (55) (2) (3)
TCYa 4 1 63 66 37 6 4 19 1
(10) (2) (42) (24) (1)
T/Sa 2 17 74 72 32 4 (1)
(46) (31) (1)
aCL=clindamycin; EM=erythromycin; TCY=tetracycline; T/S=trimethoprim-sulfamethoxazole.bResistant strains in italics.
Table 4
Resistance profile for P. acnes resistant strains in antibiotic-treated/
non-treated acne patients
Antibiotica Number of P.acnes
strains in antibiotic-
treated patients
(n ¼ 201)
Number of P.acnes
strains in non-
treated patients
(n ¼ 79)
Susceptible 138 73
CL 11 2
EM 3 —
TCY 5 —
CL; EM 19 3
CL; TCY 7 —
TCY; T/S — 1
CL; EM; TCY 18 —
aCL=clindamycin; EM=erythromycin; TCY=tetracycline; T/S=
trimethoprim-sulfamethoxazole.
Table 5
Number of patients colonized with antibiotic-resistant strains of P.
acnes in 100 antibiotic-treated acne patients and in 30 non-treated acne
patients
Antibiotica Antibiotic-treated
group (no. patients)
Non-treated group
(no.patients)
CL 8 2
EM 3b —
TCY 3 —
CL; EM 11c 1
CL; TCY 4 —
TCY; T/S — 1
CL; EM; TCY 10b,c —
aCL=clindamycin; EM=erythromycin; TCY=tetracycline;
T/S=trimethoprim-sulfamethoxazole.bOne patient was colonized by strains with different resistance
patterns: EM and CL, EM, TCY.cOne patient was colonized by strains with different resistance
patterns: CL, EM and CL, EM, TCY.
C. Oprica et al. / Anaerobe 10 (2004) 155–164 159
Resistant propionibacteria were isolated in 18 of 37patients (49%) at multiple sites.In the treated group of patients, both female and male
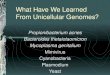
patients were colonized by resistant strains (Fig. 1).Logistic regression analysis for age and gender showedthat there was no significant difference between maleand female patients with regard to carriage of resistantstrains.
Young patients were more likely than other agegroups to carry resistant strains (50% of patientsyounger than 15 years old, 35.5% of patients 16–20years old, and 37% of patients older than 21 years werefound to be colonized with resistant strains), but thedifference was not statistically significant (P >0.05).

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164160
Of the four patients from the non-treated group, twopatients carried resistant strains to one antibiotic andtwo patients carried resistant strains to two antibiotics.One patient was colonized by resistant strains atmultiple sites. One patient in this group was colonizedwith a strain resistant to tetracycline and trimethoprim–sulfamethoxazole. In the treated group, no strainsresistant to trimethoprim–sulfamethoxazole were iden-tified (Table 5).
0
10
20
30
40
50
60
70
≤ 15 16-20 ≥ 21
Age (years)
% p
atie
nts
with
res
ista
nt is
olat
es
FemalesMales
Fig. 1. Age distribution of skin colonization by antibiotic resistant
P. acnes strains in male and female acne patients from the treated group.
Fig. 2. Diversity of Spe I digests of chromosomal DNA of P. acnes resistant i
four different patterns of DNA digests grouped in eight main genetic lineages
represented a strain isolated from one patient excepting isolates from three d
right side of the dendrogram (see text for details). The clonal group level wa
3.2. PFGE typing
All resistant strains were distinguishable by PFGE.Forty-four different patterns of SpeI DNA digests weredetected (Fig. 2). A band-based cluster analysis (Mole-cular Analyst, Bio-Rad), in which band similarity thatexceeds 80% was used as the criterion of clusterformation, revealed eight pattern clusters, from A toH. Also the visual analysis showed that strains from thesame cluster rendered less than three bands differenceand the number of bands difference between strainsbelonging to different clusters was more than fourbands. According to Tenover et al. [28] the first group iscomposed of strains closely related and the second onefrom possibly related or genetically unrelated strains.From the final analysis strains belonging to the samepatient were excluded if they exhibited the same patternof resistance, the same MIC values and identical bands.These isolates were considered representing the samestrain, and only one strain from each group wasanalysed. The number of DNA fragments observed inPFGE patterns after SpeI restriction digestion of theisolates varied from 15–25 (Fig. 2).The similarity between major PFGE types ranged from
58% to 98%. A relative tight clustering was observed.Each cluster included between one and 23 isolates. Themajority of isolates (n ¼ 34; 77%) were grouped into twotypes: C (n ¼ 23; 52%) and A (n ¼ 11; 25%). Twoisolates with unique pattern form type H clustered with
solates displayed as a dendrogram of Dice similarity coefficients. Forty-
of P. acnes (A–H) isolated from 41 patients were detected. Each pattern
ifferent patients and their resistance pattern that are represented on the
s set at X80% similarity (dotted line).

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164 161
other strains at 58% similarity (Fig. 2). These two strainsbelonged to different patients and were both resistant forclindamycin and erythromycin. Four PFGE types (B, D,E, G) were composed by single isolates. There were sevenresistance phenotypes; the most frequent was found forclindamycin and clindamycin/erythromycin (12 strainseach), and for the combination clindamycin/erythromy-cin/tetracycline (11 strains). One single strain was resistantfor tetracycline and trimethoprim–sulfamethoxazolebelonging to clone D (Table 6).
3.3. Concordance between PFGE analysis and resistance
pattern
Eighty-three percent of clindamycin resistant strains(10/12) belonged to the same clone C (Fig. 3; Table 6).
Fig. 3. Dendrogram showing the relationship of eight representative finge
resistance patterns and clonal types (dendrogram and graph). The clonal gr
Table 6
Antimicrobial resistance patterns of resistant P. acnes strains and
PFGE types
Antibiotic resistant patterna
(no of strains)
PFGE type (no of strains)
CL (12) A (2); C (10)
TCY (3) A (1), B (1); C (1)
EM (2) C (1); F (1)
CL, EM (12) A (4); C (4); E (1); F (1); H (2)
CL, TCY (3) A (1); C (1); G (1)
CL, EM, TCY (11) A (3); C (6); F (2)
TCY, T/S (1) D (1)
aCL=clindamycin; EM=erythromycin; TCY=tetracycline; T/S=
trimethoprim-sulfamethoxazole.
4. Discussion
Resistance to antibiotics in P. acnes has not beforebeen carefully studied in Swedish patients with acne.There is only one small previous double-blind study on20 patients with acne vulgaris, in which 10 patients weretreated with topical clindamycin and 10 patients withoral tetracycline for 8 weeks [20]. The skin and colonmicro-flora were determined before, during and up to 8weeks after treatment. All patients improved markedlyto the same extent. In patients receiving tetracycline,40% of the skin bacteria became resistant duringtherapy, while the corresponding figure for clindamycinwas 60%. The skin flora was normalized in mostpatients after the treatment had stopped.The present and other studies have indicated that the
resistance problem of P. acnes will increase. In thepresent study, evidence was found for resistance toP. acnes to tetracycline, erythromycin and clindamycin.Compared to the non-treated controls, with lownumbers of resistance, the patients with moderate tosevere acne vulgaris treated at least for 2 months withantibiotics (tetracycline and/or erythromycin) showedincreased numbers of resistant P. acnes strains. InSweden tetracycline is much more prescribed for acnecompared to erythromycin or clindamycin but yet, theprevalence of tetracycline resistant strains is lower.From 98 patients treated with tetracycline, 81 patientswere not colonized with strains resistant to thisantibiotic. This situation is perhaps due to the fact thatoral tetracycline is less selective as far as bacterial
rprints of P. acnes strains (A–H) and correlations between different
oup level was set at X80% similarity.

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164162
resistance is concerned. Another explanation would bethe reduced fitness of tetracycline resistant strains andthe disadvantage of in vitro activity compared tosusceptible strains [15]. Strains resistant both toerythromycin and clindamycin were most common,followed by strains resistant to tetracycline, erythromy-cin and clindamycin. Only a few strains resistant toerythromycin alone were isolated but this antibiotic isseldom prescribed for acne therapy in Sweden. Patients’history could not be consistently ascertained for longerperiods. Some patients may have been treated withantibiotics belonging to the MLS class for otherdiseases, and these could be the explanation for theskin colonization with clindamycin/erythromycin resis-tant strains in patients who have received tetracyclinefor acne treatment. Also, the possibility of transfer ofresistant P. acnes isolates between patients and theirclose contacts should not be overlooked [17].One single strain was found resistant for trimetho-
prim–sulfamethoxazole and tetracycline. Resistance totrimethoprim–sulfamethoxazole has been reported be-fore [12,14] and this may indicate that new mechanismsof resistance may appear.Colonization rates with resistant isolates showed
higher prevalence in younger patients. Dermatologistsdo prescribe antibiotics as the first choice of treatmentfor younger patients. For older patients who have beenalready treated with several antibiotics, other therapiesare preferred.In the present study, only patients treated with oral
antibiotic therapy were included because this is therecommendation of treatment for moderate and severeforms of acne [6]. The intention was also to have ahomogenous group of treated patients. This homogene-ity is better in orally treated patients, due to thedifficulties in application of the topical treatment oncertain affected areas. Patients treated with benzoylperoxide were also excluded due to the fact that thisagent has an antibacterial effect by suppressing thefollicular population of P. acnes [29].Pulsed-field gel electrophoresis is considered as a
standard among epidemiological typing methods. It hasfull typability, good reproducibility and high discrimi-natory power. This molecular method is based on thesimilarities in the digested DNA electrophoretic pat-terns. Until now, this method has never been used forlarge epidemiological studies regarding P. acnes andacne patients. A reliable typing method can respond tomany questions regarding appearance and dissemina-tion of resistant strains. PFGE profiles can establishstrain relatedness among bacteria with the same patternof multiple antibiotic resistances. It can detect if acertain clone is more prone of becoming resistant or ifthe patients colonized with this clone respond less wellto therapy. For follow-up studies, PFGE can detect ifthe appearance of a resistant strain is due to anti-
microbial resistance development during therapy, or dueto acquisition of other resistant strains [30]. Cell wallskeleton of P. acnes contains glucosamine with freeamino acid groups, which are responsible for theresistance of lysozyme [31]. We have therefore used themethod described by Chassy and Giuffrida [26]. Thismethod is specifically adapted for the lysis of the cellwall of Gram-positive bacteria. The method useslysozyme suspended in a buffer containing polyethyleneglycol that serves as an osmotic stabilizer and enhancerof the lysis. Mutanolysin is splitting the beta-1-4-N-acetylmuramyl-N-acetylglucosamine linkage ofpeptidoglycan-polysaccharide cell-wall polymer, a link-age highly conserved among bacterial species. Thismuralytic enzyme has a wide range of activity againstbacterial strains resistant to lysozyme [32]. Differentconcentrations of both mutanolysin and lysozyme weretested and with this combination all strains werecompletely lysed.The presented data showed that strains with the same
antibiotic susceptibility pattern can be of differentPFGE types. For example if the strains were resistantto clindamycin and erythromycin, five PFGE wereobserved (Fig. 3; Table 6). Also, P. acnes resistantstrains of the same PFGE type were found to havedifferent resistant patterns.One patient (P 129) was colonized with strains with
different resistance patterns: clindamycin (MIC 4mg/L),erythromycin (MIC >128mg/L) and clindamycin (MIC32mg/L), erythromycin (MIC >128mg/L), tetracycline(MIC 4mg/L) belonging to the same clone C (Fig. 2). Itwill be interesting to study the possibility of the firststrain to become resistant to tetracycline in the future.Another patient (P 429) was colonized with strainsbelonging to different clones (A and C) harbouringdifferent patterns of resistance: clindamycin (MIC=0.5mg/L), erythromycin (MIC=0.5mg/L), tetracycline(MIC=8mg/L) and erythromycin (MIC=4mg/L)(Fig. 2). Both strains were exposed to the sameantibiotic pressure, so it could be possible that certainclones are more prone of becoming resistant to someantibiotics. Another patient (P 115) was also colonizedwith two different strains (one type A and the other typeC), with different degrees of resistance for clindamycin:MIC=0.25mg/L for the first strain and 0.5mg/L for thesecond strain (Fig. 2).These data proved that an individual might harbour
different strains of P. acnes with various degreesof resistance. Looking for an association betweenantibiotic susceptibilities and genotypes, it was foundthat 83% of clindamycin resistant strains (10/12)belonged to the clonal type C.The results indicated a relationship between the
isolates, but also showed that there was a genomicdiversity among P. acnes strains. It has been shown thatSpeI restriction is well adapted to PFGE.

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164 163
To validate the clonal analyses, PFGE analyses werecarried out with more than one restriction enzyme (SpeIand NotI). No differences regarding to the discrimina-tory power were found. There are two studies publishedusing this method for typing of P. acnes strains [33,34].In the first study, all three analysed strains were shownto be identical, and in the second study there was verylittle difference among nine P. acnes strains.With one exception represented by clone H, it was a
tight clustering around 70%. The relative homogeneitycould be explained by a triple selection, which gave riseto a selected population. First, the strains have beencollected from the same geographical region and at thesame time; second, they were from acne patients, agroup exposed to the pressure of topical/oral antibac-terial drugs; third, they were all resistant strains.It is possible that epidemiological unrelated isolates
may have similar genotypes, and methicillin-resistant S.
aureus represents a classical example. The epidemiolo-gical situation is limited to genetic diversity and most ofthe resistant strains derive from a small number ofancestral clones [28,35]. However, P. acnes resistantstrains from different geographical regions are genoty-pically different but there are some P. acnes clonesspread over different areas.Antibiotic resistance in P. acnes presents a worldwide
problem for the treatment of acne. Sweden is wellknown for a very restrictive policy regarding prescrip-tion of antibiotics, but still P. acnes resistance hasemerged. Thirty-seven percent of the patients receivingantibiotics were colonized with resistant strains.At a time when dermatologists are advised to reduce
antibiotic prescribing in an attempt to limit theincreasing risk of resistance in the hospitals and thecommunity, it seems more difficult to defend the oftenlong-term use of antibiotics for acne, because of thehigher pressure on the micro-organisms to developresistance. Unfortunately, until effective new non-antibiotic treatments for acne with acceptable sideeffects are available, antibiotics will remain the first linetreatment over the next coming years. Certain precau-tions are advocated in order to minimize the resistanceproblem: avoid antibiotics for milder forms of acne untilit is really necessary and using antibiotics in combina-tion with topical retinoids or benzoyl peroxide ifantibiotics must be administrated for longer than 2months [36,37]. Only retinaldehyde is antibacterial dueto its chemical structure, but all other topical retinoidshave an indirect mechanism on bacteria by modifyingthe skin lipids and drying effect [38]. It seems wise tolimit the use of antibiotics for the treatment of acne,both systemically and locally and seek other treatmentmodalities and not to use them as a maintenancetherapy [36].The concept of biofilms has recently been introduced
as a possible important pathogenic factor in acne
vulgaris [39]. This is a very interesting field for newapproaches of acne treatment, but antibacterial resis-tance should not be neglected. It was proved thatpatients colonized with strains resistant to erythromycinresponded poorly to therapy [9]. There is a certainability of the antibiotic to penetrate the biofilm andthere are reports showing an important reduction inviable propionibacteria after antibiotic treatment [40].The results presented suggest that the P. acnes
resistant population is polyclonal. There is genomicdiversity among the resistant isolates and PFGE allowsdifferentiation of P. acnes strains and could be a usefultechnique for epidemiological studies. It would beinteresting to analyse clinical isolates from differentgeographical areas and from different infections in orderto extend the observations. P. acnes colonizes other sitesthan skin, such as the nares, and the intestinal tract. It isnot known yet if these isolates represent a distinctpopulation, and in the future PFGE analysis may givemore information about the epidemiology of P. acnes
infections.
References
[1] Eady EA, Ingham E. Propionibacterium acnes—friend or foe? Rev
Med Microbiol 1994;5:163–73.
[2] Dreno B, Poli F. Epidemiology of acne. Dermatology 2003;206:
7–10.
[3] Goulden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in
adults. J Am Acad Dermatol 1999;41:577–80.
[4] Plunkett A, Merlin K, Gill D, Zuo Y, Jolley D, Marks R. The
frequency of common nonmalignant skin conditions in adults in
central Victoria, Australia. Int J Dermatol 1999;38:901–8.
[5] Stern RS. Medication and medical service utilization for acne
1995–1998. J Am Acad Dermatol 2000;43:1042–8.
[6] Zouboulis CC, Piquero-Martin J. Update and future of systemic
acne treatment. Dermatology 2003;206:37–53.
[7] Leyden JJ. Antibiotic resistant acne. Cutis 1976;17:593–6.
[8] Eady EA, Cove JH, Blake J, Holland KT, Cunliffe WJ.
Recalcitrant acne vulgaris. Clinical, biochemical and microbiolo-
gical investigation of patients not responding to antibiotic
treatment. Br J Dermatol 1988;118:415–23.
[9] Eady EA, Cove JH, Holland KT, Cunliffe WJ. Erythromycin
resistant propionibacteria in antibiotic treated acne patients:
association with therapeutic failure. Br J Dermatol 1989;121:51–7.
[10] Leyden JJ, McGinley KJ, Cavalieri S, Webster GF, Mills OH,
Kligman AM. Propionibacterium acnes resistance to antibiotics in
acne patients. J Am Acad Dermatol 1983;8:41–5.
[11] Cunliffe W. Propionibacterium acnes resistance and its clinical
relevance. J Dermatol Treatment 1995;6(Suppl 1):S3–4.
[12] Eady EA, Jones CE, Tipper JL, Cove JH, Cunliffe WJ, Layton
AM. Antibiotic resistant propionibacteria in acne: need for
policies to modify antibiotic usage. Br Med J 1993;306:555–6.
[13] Kurokawa I, Nishijima S, Asada Y. The antibiotic susceptibility
of Propionibacterium acnes: a 15-year bacteriological study and
retrospective evaluation. J Dermatol 1988;15:149–54.
[14] Ross JI, Snelling AM, Eady EA, Cove JH, Cunliffe WJ, Leyden
JJ, Collignon P, Dreno B, Reynaud A, Fluhr J, Oshima S.
Phenotypic and genotypic characterization of antibiotic-resistant
Propionibacterium acnes isolated from acne patients attending

ARTICLE IN PRESSC. Oprica et al. / Anaerobe 10 (2004) 155–164164
dermatology clinics in Europe, the USA, Japan and Australia. Br
J Dermatol 2001;144:339–46.
[15] Coates P, Vyakrnam S, Eady EA, Jones CE, Cove JH, Cunliffe
WJ. Prevalence of antibiotic-resistant propionibacteria on the
skin of acne patients: 10–year surveillance data and snapshot
distribution study. Br J Dermatol 2002;146:840–8.
[16] Eady EA. Bacterial resistance in acne. Dermatology 1998;196:
59–66.
[17] Ross JI, Snelling AM, Carnegie E, Coates P, Cunliffe WJ, Bettoli
V, Tosti G, Katsambas A, Galvan Perez Del Pulgar JI, Rollman
O, Torok L, Eady EA, Cove JH. Antibiotic-resistant acne: lessons
from Europe. Br J Dermatol 2003;148:467–78.
[18] Berson DS, Shalita AR. The treatment of acne: the role of
combination therapies. J Am Acad Dermatol 1995;32:S31–41.
[19] Krowchuk DP. Treating acne. A practical guide. Med Clin North
Am 2000;84:811–28.
[20] Borglund E, Hagermark O, Nord CE. Impact of topical
clindamycin and systemic tetracycline on the skin and colon
microflora in patients with acne vulgaris. Scand J Infect Dis
1984;43(Suppl):76–81.
[21] Rodloff AC, Hillier SL, Moncla BJ. Peptostreptococcus, Propio-
nibacterium, Lactobacillus, Actinomycetes and other non-spore-
forming anaerobic Gram-positive bacteria. In: Murray PR, Baron
EJ, Pfaller MA, Tenover FC, Yolken RH, editors. Manual of
clinical microbiology. Washington, DC: American Society for
Microbiology; 1999. p. 672–89.
[22] National Committee for Clinical Laboratory Standards. Methods
for antimicrobial susceptibility testing of anaerobic bacteria.
Approved standard M11-A5, 5th ed. Villanova, PA: NCCLS; 2001.
[23] European Committee on Antimicrobial Susceptibility Testing
(EUCAST). Business Meeting 13th European Congress of
Clinical Microbiology and Infectious Diseases, Glasgow, UK,
May 12, 2003.
[24] Maslow JN, Slutsky AM, Arbeit RD. Application of pulsed-field
gel electrophoresis to molecular epidemiology. In: Persing DH,
Smith TF, Tenover FC, White TJ, editors. Diagnostic molecular
microbiology: principles and applications. Washington, DC:
American Society for Microbiology; 1993. p. 563–72.
[25] Fliss I, Emond E, Simard RE, Pandian S. A rapid and efficient
method of lysis of Listeria and other gram-positive bacteria using
mutanolysin. Biotechniques 1991;11:453,456–7.
[26] Chassy BM, Giuffrida A. Method for the lysis of Gram-positive,
asporogenous bacteria with lysozyme. Appl Environ Microbiol
1980;39:153–8.
[27] Dice LR. Measures of the amount of ecological association
between species. J Ecol 1945;26:297–302.
[28] Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray
BE, Persing DH, Swaminathan B. Interpreting chromosomal
DNA restriction patterns produced by pulsed-field gel electro-
phoresis: criteria for bacterial strain typing. J Clin Microbiol
1995;33:2233–9.
[29] Kligman AM, Leyden JJ, Stewart R. New uses for benzoyl
peroxide: a broad-spectrum antimicrobial agent. Int J Dermatol
1977;16:413–7.
[30] Sahm DF. Molecular Typing of bacteria using pulsed-field gel
electrophoresis (PFGE). Lab Med Newslett 1996;4.
[31] Kamisango K, Saiki I, Tanio Y, Okumura H, Araki Y, Sekikawa
I, Azuma I, Yamamura Y. Structures and biological activities of
peptidoglycans of Listeria monocytogenes and Propionibacterium
acnes. J Biochem (Tokyo) 1982;92:23–33.
[32] Lichtman SN, Okoruwa EE, Keku J, Schwab JH, Sartor RB.
Degradation of endogenous bacterial cell wall polymers by the
muralytic enzyme mutanolysin prevents hepatobiliary injury in
genetically susceptible rats with experimental intestinal bacterial
overgrowth. J Clin Invest 1992;90:1313–22.
[33] Jallo GI, Koslow M, Hanna BA, Carson LA. Propionibacterium
as a cause of postneurosurgical infection in patients with dural
allografts: report of three cases. Neurosurgery 1999;44:1138–41.
[34] Ting DT, Chern KC, Meisler DM, Hall GS, Knapp CC,
Doyle LJ, Ludwig M, Tuohy M, Foster RE, Lowder CY.
Evaluation of Propionibacterium acnes isolates using contour-
clamped homogeneous electric field gel electrophoresis. Anaerobe
1999;5:579–82.
[35] Kreiswirth B, Kornblum J, Arbeit RD, Eisner W, Maslow JN,
McGeer A, Low DE, Novick RP. Evidence for a clonal origin of
methicillin resistance in Staphylococcus aureus. Science
1993;259:227–30.
[36] Gollnick H, Cunliffe W, Berson D, Dreno B, Finlay A, Leyden JJ,
Shalita AR, Thiboutot D. Management of acne: a report from a
global alliance to improve outcomes in acne. J Am Acad
Dermatol 2003;49(Suppl 1):S1–2.
[37] Eady EA, Gloor M, Leyden JJ. Propionibacterium acnes
resistance: a worldwide problem. Dermatology 2003;206:54–6.
[38] Pechere M, Germanier L, Siegenthaler G, Pechere JC, Saurat JH.
The antibacterial activity of topical retinoids: the case of
retinaldehyde. Dermatology 2002;205:153–8.
[39] Burkhart CN, Burkhart CG. Microbiology’s principle of biofilms
as a major factor in the pathogenesis of acne vulgaris. Int J
Dermatol 2003;42:925–7.
[40] Gloor M, Kraft H, Franke M. Effectiveness of topically applied
antibiotics on anaerobic bacteria in the pilo-sebaceous duct.
Dermatologica 1978;157:96–104.