Embed Size (px)
Citation preview

Antibiotics and Duration
James A. McKinnell, M. D.
David Geffen School of Medicine UCLA
Los Angeles County Department of Public Health
Acute Communicable Disease Control Unit

Appreciation
• Brad Spellberg
• Phil Robinson
2

Disclosures
• I have received Government Research Funding from NIH,
AHRQ, CDC, and CTSI
• I have served as a consultant for Achaogen, Allergan,
Cempra, Science 37, Theravance, and ThermoFisher
• I have no commercial/financial relationships related to
decolonization, CHG, mupirocin, or iodophor products
3

Disclosures
One Third of What you Learned in Medical School and
Residency is Wrong .... The Trick is Learning Which Third!!
4

Objectives
• Understand the Value of Antibiotics
• Understand Where Current Durations of Antibiotics were
developed
• Review Current Indications of Antibiotic Duration
5

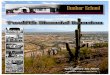
Value of Antibiotics6
Disease Pre-Antibiotic Death Rate
Death With Antibiotics
Change in Death
Community Pneumonia1 35% 10% -25%
Hospital Pneumonia2 60% 30% -30%
Heart Infection3 100% 25% -75%
Brain Infection4 >80% <20% -60%
Skin Infection5 11% <0.5% -10%
By comparison…treatment of myocardial infarction with aspirin or fibrinolytic drugs6
-3%
1IDSA Position Paper ’08 Clin Infect Dis 47(S3):S249-65; 2IDSA/ACCP/ATS/SCCM Position Paper ’10 Clin Infect Dis 51(S1):S150-70; 3Kerr AJ. Subacute Bacterial Endocarditis. Springfield IL: Charles C. Thomas, 1955 & Lancet 1935 226:383-4; 4Lancet ’38 231:733-4 & Waring et al. ’48 Am J Med 5:402-18; 5Spellberg et al. ’09 Clin Infect Dis 49:383-91 & Madsen ’73 Infection 1:76-81; 6’88 Lancet 2:349-60

7
52.1%
12.2%
42.0%
17.7%
P < 0.001
P < 0.001
Hospital
Mortality
(%)
All-Cause Mortality Infection-Related Mortality
Inadequate antimicrobial therapy associated with
higher mortality
Prospective study (n=2000: 655 with infections)
Kollef MH., et al. Chest. 1999;115:462-474.
25% of patients received inadequate treatment

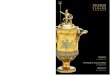
Relationship between survival and time to effective antimicrobial
treatment among patients with septic shock
Kumar A, et al. Crit Care Med 2006; 1589-1596 (June)
Time from hypotension onset (hours)
Fra
ction o
f to
tal patients
1.0
0.8
0.6
0.4
0.2
0.0
0-0.49 0/5-0.99 1-1.99 2-2,99 3-3.99 4-4.99 5-5.99 6-8.99 9-11.99 12-12.99 24-35.99 >36
Retrospective multi-center study (n=2731)

“The more we use them, the more we lose them…”
By courtesy of Dr. Liselotte Diaz Högberg

10
“Make sure you take every dose of your prescribed antibiotic, even after you feel better.”

Antibiotic Duration as Football Scores
• Community Associated Pneumonia 7-10
• HAP/VAP 10-14
• Pyelonephritis 10-14
• Cellulitis 7-10
• Bacteremia 14-42
11

12
Standard Abx durations: 1-2 Constantine
units—based on 1695 year old decree

Short Course Therapy!!!!
13
Diagnosis Short (d) Long (d) Result
CAP 3 or 5 7, 8, or 10 Equal
HAP 7 10-15 Equal
VAP 8 15 Equal
Pyelo 7 or 5 14 or 10 Equal
Intra-abd 4 10 Equal
AECB <5 >7 Equal
Cellulitis 5-6 10 Equal
Osteo 42 84 Equal

Community Associated Pneumonia
3-5 Days
14
• Multiple RCT showing 3-5 days NI to 7 - 10 days
• Includes pts with PORT IV and V
(Uranga et al. JAMA IM)
• Reduced emergence of resistance
Singh et al. Am J Respir Crit Care Med 2000;162:505-11; Dunbar et al. Clin Infect Dis 2003;37:752-60; Zhao X et al. Diagn Microbiol Infect Dis 2014;80:141-7; Pakistan Multicentre Amoxycillin Short Course Therapy pneumonia study group. Lancet 2002;360:835-41; Greenberg et al. The Pediatric infectious disease journal 2014;33:136-42; Dunbar et al. Current medical research and opinion 2004;20:555-63; el Moussaoui et al. Bmj 2006;332:1355; Uranga et al. JAMA IM 2016 176:1257-65.

• Several RCTs 7-8 days equal to 10-15 days
• Reduced emergence of resistance
• MRSA and Pseudomonas infections may
require longer therapy
Capellier et al. PLoS One 2012:7:e41290; Chastre et al. JAMA 2003
290:2588-98; Kalil et al. CID 2016 63:e61-e111
15
HCAP/VAP7 DAYS

• Several RCTs 5-7 days equal to 10-14 days
• Short course effective despite diabetes and
GNB bacteremia
Jernelius et al. Acta Med Scand 1988;223:469-77; de Gier R, Karperien
A, Bouter K, et al. 1995. Int J Antimicrob Agents 6:27-30; Talan
DA, Stamm WE, Hooton TM, et al. 2000 JAMA 283:1583-90;
Sandberg et al. 2012 Lancet 380:484-90; Peterson et al. 2008
Urology 71:17-22; Klausner et al. 2007. Current medical research
and opinion 23:2637-45.
16
PYELONEPHRITIS5-7 DAYS

• Recent Trial 4 Days Equal to 10 days
• Assuming Adequate Source Control
Sawyer et al. 2015 NEJM 372:1996-2005.
17
INTRA-ABDOMINAL INFECTION4-5 DAYS

• Dozens of Studies
• Meta-analysis show that 3-5 days of therapy
equal to 7 or more days.
El Moussaoui 2008 Thorax 68:415-22
18
AECB/COPD3-5 DAYS

• Numerous trials show that 5-7 equal to 10-14
days
• Drainage of abscess is key
• When you drain and abscess, treat especially
if surrounding cellulitis.
Hepburn 2004 Arch Int Med 164:1669-74; Prokocimer 2013 JAMA
309:559-69; Moran 2014 Lancet ID 14:696-705.
19
CELLULITIS/ABSCESS3-5 DAYS

• Short Course TB trials underway
• Chronic infections still require prolonged therapy – e.g. prosthetic hip infections
• Data on Endocarditis is evolving
• Rheumatic fever may require 5 days of cephalosporins but 10 days of penicillin – data
not clear
20
EXCEPTIONS

Short Course Therapy!!!!
21
Diagnosis Short (d) Long (d) Result
CAP 3 or 5 7, 8, or 10 Equal
HAP 7 10-15 Equal
VAP 8 15 Equal
Pyelo 7 or 5 14 or 10 Equal
Intra-abd 4 10 Equal
AECB <5 >7 Equal
Cellulitis 5-6 10 Equal
Osteo 42 84 Equal

22
“The most viable strategy for reducing antimicrobial selective
pressure is to treat infections only for as long as is necessary.”
Dr. Lou Rice, Executive Chair of Medicine, Warren Alpert School of Medicine of Brown University. 2008 Maxwell Finland Lecture at IDSA Annual Meeting

Longer Therapy Actually Hurts the Patient
23
• Longer therapy causes more selective pressure—off-target in microbiome and in the environment
• Even at the site of infection, studies of short vs. long-course therapy have found greater emergence of resistance with longer therapy (Chastre ‘03 JAMA 290:2588-9; Singh ‘00 Am J
Resp Crit Care Med 162:505-11)

Fight the Errors of our Forebarers
24
• Stop telling patients to complete course of Abx even if their symptoms are gone
• Taking antibiotics after symptom resolution provides no efficacy but selects for resistant among microbiome
• If patients feel better, they should call their doctor to ask to stop earlyy

LAC – DPH to the Rescue
Healthcare Associated Infection Antibiotic Resistance
Control Task Force
Epidemiology, Infectious Disease Physicians, Infectious
Disease Pharmacists, Microbiologists, Infection Prevention
Specialists, and Others
25

CDC (http://www.cdc.gov/media/releases/2015/p0915-nursing-home-antibiotics.html)

• “By the end of 2017, CMS and CA require long-term care
and nursing home facilities to develop and implement
robust ASPs that adhere to best practices”
New Requirements27

Basic ASP Tier Elements for SNFs:
Less Challenging Components1. Antimicrobial stewardship (AS) policy/procedure
2. Written statement in support of ASP with evidence for
necessary budget/staffing
3. AS activities reported to facility’s Quality Assurance-
Performance Improvement (QAPI) program.
4. Establish physician-supervised, multidisciplinary
antimicrobial stewardship committee
28

Basic ASP Tier Elements for SNF:
More Challenging Components4. Program support from a physician or pharmacist with
specific training on antimicrobial stewardship
5. AS education provided to nursing staff, medical staff,
residents, and visitors
29

LA County Antimicrobial Resistance Network (ARN)
• Support acute care hospitals (ACHs) in engaging their
network SNFs to meet upcoming ASP requirements
• Improve inter-facility communication to reduce spread of
multidrug-resistant organisms (MDROs)
30

31
LA County Department of Public Health Antibiotic Resistance Network

UTI
Estimates for Outpatient UTI in the US in 1995:
• 11.3 million Rx with $1.6 Billion in costs
Foxman B et al. Ann Epidemiol 2000;10:509-15

US Expenditures
Griebling, Journal of Urology 173:1281,8 (2005)
Women
($2.5B)
Men
($1B)

UTI
25-35% women 20-40 y/o have had a UTI
• 1.8 - 6.1 days of symptoms
• 0.6 - 1.2 days of missed work or classes
• 0.4 - 0.6 days in bed
Foxman B et al. Ann Epidemiol 2000;10:509-15
Foxman B et al. Am J Public Health 1985;75:1308-13
Schappert SM; Vital Health Stat 1994; 13:1-110.

GN Resistance
• Fluroquinolone Resistance was High
Among E. Coli it was 32%
TMP/SMX resistance not included
Nitrofurantoin resistance not included
35

36
McKinnell et al. Mayo Clinic 2011

37
McKinnell et al. Mayo Clinic 2011

LAC DPH Outpatient Stewardship Project
• LAC DPH Healthcare Outreach Unit is planning a multi-
faceted intervention to improve provider prescribing in
outpatient settings
• Intervention includes a core package:
• Poster commitment
• Treatment guidelines
• Communication skills training
• Additional strategies tailored to facility’s needs
38

LAC DPH Outpatient Stewardship Project,
cont.• Benefits to participation:
• Tailored assistance in implementation of CDC Core Elements
• Improved provider knowledge of resistance and appropriate
prescribing for upper respiratory infections
• Free resources to support providers in improving antibiotic
prescribing
• Increased coordination and exchange of antibiotic stewardship best
practices
39

LAC DPH Outpatient Stewardship Project,
cont.• Seeking volunteer primary care clinics to participate
• Ability to collect/ report prescribing data
• Identify stewardship champion in facility
40
For more information, contact Kelsey OYong:[email protected]
(213) 240-7941