Embed Size (px)
Citation preview

1
Antibodies are not the only standard part of first relapse management in myeloma
Jonathan L. Kaufman, MDAssociate ProfessorDepartment of Hematology and Medical OncologyWinship Cancer InstituteEmory University School of Medicine

2Winship Cancer Institute | Emory University
Considerations for using antibodies in myeloma• When
• Smoldering: Dara as single agent: Nooka PI• Induction: Elo RVD: Nooka PI• Consolidation/Maintenance: Elo Len: Nooka PI• First Relapse• Later relapse• Retreatment with pom/dara: Nooka PI
• Applicability of clinical trial data to our patients
• Non antibody based treatment options
• Optimal partner

3Winship Cancer Institute | Emory University
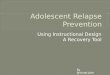
TOURMALINE-MM1: Phase 3 Study of Weekly Oral Ixazomib Plus Lenalidomide-dexamethasone
Ran
dom
izat
ion
Ixazomib + Lenalidomide + DexamethasoneIxazomib: 4 mg on days 1, 8, and 15Lenalidomide: 25 mg* on days 1-21
Dexamethasone: 40 mg on days 1, 8, 15, 22
N=722
1:1
Placebo + Lenalidomide + DexamethasonePlacebo: on days 1, 8, and 15
Lenalidomide: 25 mg* on days 1-21Dexamethasone: 40 mg on days 1, 8, 15, 22
Repeat every 28 days until progression, or unacceptable toxicity
Stratification:• Prior therapy: 1 vs 2 or 3• ISS: I or II vs III• PI exposure: yes vs no
Global, double-blind, randomized, placebo-controlled study design
Response and progression (IMWG 2011 criteria1) assessed by an independent review committee (IRC) blinded to both treatment and investigator assessment
Primary endpoint: • PFSKey secondary endpoints: • OS • OS in patients with del(17p)
Moreau P, et al. N Engl Med. 2016;374(17):1621-1634.

Outcomes by cytogenetic risk group
Median OS could not be estimated
In the IRd arm, median PFS in high-risk patients was similar to that in the overall patient population and in patients with standard-risk cytogenetics
ORR, % ≥VGPR, % ≥CR, % Median PFS, months
IRd Placebo-Rd IRd Placebo-Rd IRd Placebo-Rd IRd Placebo-RdHR
All patients 78.3* 71.5 48.1* 39 11.7* 6.6 20.6 14.7 0.742*
Standard-risk patients 80 73 51 44 12 7 20.6 15.6 0.640*
All high-risk patients 79* 60 45* 21 12* 2 21.4 9.7 0.543
Patients with del(17p)† 72 48 39 15 11* 0 21.4 9.7 0.596
Patients with t(4;14) alone 89 76 53 28 14 4 18.5 12.0 0.645
*p<0.05 for comparison between regimens. †Alone or in combination with t(4;14 or t(14;16). Data not included on patients with t(14:16) alone due to small numbers (n=7).
Moreau P, et al. N Engl Med. 2016;374(17):1621-1634.

5Winship Cancer Institute | Emory University
PFS results based on different cut-offs for del(17p)
Cut-off for del(17p)
Number of patients Median PFS, mos IRd vs placebo-Rd
HR p-value
5% 69 21.4 vs 9.7 0.596 0.162
20% 59 21.4 vs 6.7 0.611 0.2049
60% 33 15.7 vs 5.1 0.49 0.2481
10% of patients had tumors harboring the del(17p) abnormality The outcomes for del17-positive patients, in the control arm (Rd), were
similar to what has been reported for Rd therapy in different trialsMoreau P, et al. N Engl Med. 2016;374(17):1621-1634.

6Winship Cancer Institute | Emory University
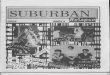
Final PFS analysis: A significant, 35% improvement in PFS with IRd vs placebo-Rd
Number of patients at risk:
IRdPlacebo-Rd
360 345 332 315 298 283 270 248 233 224 206 182 145 119 111 95 72 58 44 34 26 14 9 1 0
362 340 325 308 288 274 254 237 218 208 188 157 130 101 85 71 58 46 31 22 15 5 3 0 0
1.0
0.8
0.6
0.4
0.2
0.00 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Prob
abili
ty o
f pro
gres
sion
-fr
ee s
urvi
val
Time from randomization (months)
Log-rank test p=0.012Hazard ratio (95% CI): 0.742 (0.587, 0.939)Number of events: IRd 129; placebo-Rd 157
Median PFS:IRd: 20.6 monthsPlacebo-Rd: 14.7 months
Median follow-up: ~15 monthsMoreau P, et al. N Engl Med. 2016;374(17):1621-1634.

7Winship Cancer Institute | Emory University
ASPIRE Study Design
IV, intravenous; KRd, carfilzomib, lenalidomide, and dexamethasone; Rd, lenalidomide and dexamethasone.
RdLenalidomide 25 mg days 1–21
Dexamethasone 40 mg days 1, 8, 15, 22
KRdCarfilzomib 27 mg/m2 IV (10 min)
Days 1, 2, 8, 9, 15, 16 (20 mg/m2 days 1, 2, cycle 1 only)
Lenalidomide 25 mg days 1–21Dexamethasone 40 mg days 1, 8, 15, 22
Randomization(1:1)
N=792
Stratification:
• β2-microglobulin
• Prior bortezomib
• Prior lenalidomide
28-day cycles
After cycle 12, carfilzomib given on days 1, 2, 15, 16After cycle 18, carfilzomib discontinued
Stewart AK, et al. N Engl J Med. 2015;372(2):142-152.

8Winship Cancer Institute | Emory University
Progression-Free Survival Intent-to-Treat Population (n=792)
8
1.0
0.8
0.6
0.4
0.2
0.0
Pro
porti
onSu
rviv
ing
With
out P
rogr
essi
on
KRdRd
0 6 12 18 24 30 36 42 48
Months Since RandomizationNo. at Risk:
KRdRd
396 332 279 222 179 112 24 1396 287 206 151 117 72 18 1
CI, confidence interval; KRd, carfilzomib, lenalidomide, and dexamethasone; Rd, lenalidomide and dexamethasone.
KRdN=396
RdN=396
PFS, median months 26.3 17.6
Hazard ratio (KRd/Rd) (95% CI)
0.69 (0.57-0.83)
P value (one-sided) <.0001
Stewart AK, et al. N Engl J Med. 2015;372(2):142-152.

9Winship Cancer Institute | Emory University
PFS by Cytogenetic Risk Status at Baseline (continued)
KRd, carfilzomib, lenalidomide, and dexamethasone; PFS, progression-free survival; Rd, lenalidomide and dexamethasone.
Pro
porti
on S
urvi
ving
W
ithou
t Pro
gres
sion
0.2
Months Since Randomization
6 12 18 24 30 36 48
KRd HighRd HighKRd StandardRd Standard
420
0
0.4
0.6
0.8
1.0
Stewart AK, et al. N Engl J Med. 2015;372(2):142-152.

10Winship Cancer Institute | Emory University
Eligibility
• Relapsed/refractory MM
• 1-3 prior lines of therapy
• PR to at least 1 line of therapy
Carfilzomib 30-min infusion + Low-dose dexamethasone
RBortezomib IV or SC
+ Low-dose dexamethasone
ENDEAVOR: A Phase III Study of Cd versus Vd
Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.

11Winship Cancer Institute | Emory University
ENDEAVOR: A Phase III Study of Cd versus Vd
Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.

12Winship Cancer Institute | Emory University
ENDEAVOR: A Phase III Study of Cd versus Vd
Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.

13Winship Cancer Institute | Emory University
ENDEAVOR: A Phase III Study of Cd versus Vd
HTN: 16/9; Dyspnea; 23/5
Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.

14Winship Cancer Institute | Emory University
CHAMPION-1 Study Design
Carfilzomib (mg/m2)a Dexamethasone (mg)Phase 1 (3+3 dose-escalation schema)
Dose level 1 45 40Dose level 2 56 40Dose level 3 70 40Dose level 4 88 40
Phase 2 MTD from phase 1 40aCarfilzomib 20 mg/m2 was administered to all patients on only cycle 1 day 1.
CarfilzomibDays 1, 8, and 15
Duration of infusion: 30 minutesand
Dexamethasone IV or PODays 1, 8, 15, and 22 (day 22 omitted for cycles 9+)Both drugs given until PD or unacceptable toxicity
IV, intravenous; MTD, maximum tolerated dose; PD, progressive disease: PO, per oral.
Treatment Schedule (Phase 1 and 2)
Dosing28 day cycles:
Berenson JR, et al. Blood. 2016;127(26):3360-3368.

15Winship Cancer Institute | Emory University
Response Rates
15
CBR, clinical benefit rate; CI, confidence interval; DOR, duration of response; NA, not available; ORR, overall response rate; PR, partial response; TTR, time to response; VGPR, very good partial response.
Phase 1–270 mg/m2
(N=104)Best overall response, n (%)
Stringent complete response 5 (5)Complete response 13 (13)Very good partial response (VGPR) 31 (30)Partial response 31 (30)Minimal response 7 (7)Stable disease 12 (12)Progressive disease 2 (2)Not evaluable 3 (3)
ORR, % (95% CI) 77 (68–85)CBR, % (95% CI) 84 (75–90)DOR (≥PR), median months (95% CI) 16.3 (12.7–NA)TTR (≥PR), median months (range) 1.6 (0.7–7.2)
≥VGPR=47%
Berenson JR, et al. Blood. 2016;127(26):3360-3368.

16Winship Cancer Institute | Emory University
AEs of Any Grade Occurring in ≥ 20% of PatientsAE, n (%) Patients
(N=104)Fatigue 55 (53)Nausea 41 (39)Diarrhea 34 (33)Insomnia 33 (32)Upper respiratory tract infection 33 (32)Headache 31 (30)Anemia 29 (28)Cough 29 (28)Pyrexia 29 (28)Dyspnea 28 (27)Thrombocytopenia 25 (24)Peripheral edema 25 (24)Back pain 22 (21)
16
AE, adverse event
Berenson JR, et al. Blood. 2016;127(26):3360-3368.

17Winship Cancer Institute | Emory University
ENDEAVOR: A Phase III Study of Cd versus Vd
Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.

18Winship Cancer Institute | Emory University
DVd vs Vd: Efficacy: 1-3 Prior Lines

19Winship Cancer Institute | Emory University
POLLUX: Study Design
Cycles: 28 days
DRd (n = 286)Daratumumab 16 mg/kg IV
• Qw in Cycles 1 to 2, q2w in Cycles 3 to 6, then q4w until PD
R 25 mg PO• Days 1 to 21 of each cycle until PD
d 40 mg PO• 40 mg weekly until PDRd (n = 283)
R 25 mg PO• Days 1 to 21 of each cycle until PD
d 40 mg PO • 40 mg weekly until PD
Primary endpoint• PFS
Secondary endpoints• TTP
• OS
• ORR, VGPR, CR
• MRD
• Time to response
• Duration of response
Key eligibility criteria• RRMM
• ≥1 prior line of therapy
• Prior lenalidomide exposure, but not refractory
• Creatinine clearance ≥30 mL/min
Multicenter, randomized (1:1), open-label, active-controlled, phase 3 study
Stratification factors• No. of prior lines of therapy
• ISS stage at study entry
• Prior lenalidomide
RANDOMIZE
1:1
Statistical analyses• Primary analysis:
~177 PFS eventsISS, International Staging System; DRd, daratumumab/lenalidomide/dexamethasone; IV, intravenous; qw, weekly; q2w, every 2 weeks; q4w, every 4 weeks; R, lenalidomide; PO, oral; PD, progressive disease; d, dexamethasone; Rd, lenalidomide/dexamethasone; TTP, time to progression; OS, overall survival; MRD, minimal residual disease.
Dimopoulos MA, et al. N Engl J Med. 2016;375(14):1319-1331.

20Winship Cancer Institute | Emory UniversityDimopoulos MA, et al. N Engl J Med. 2016;375(14):1319-1331.

21Winship Cancer Institute | Emory UniversityDimopoulos MA, et al. N Engl J Med. 2016;375(14):1319-1331.

Differential Effects the Same Target
Myeloma Cell Death
T-cellsNK-cells
T-Cell and NK cell
activation
IMID AgentPom>Len>Thal
IKZF1/3
↓ IRF4↓ MYC
IKZF1/3↑ IL-2↓ TNF

ORRa: DARA + POM-D

ORR Subgroup Analysis: DARA + POM-D

Emory (Nooka) Approach to Early Relapse
Slow indolent relapse Aggressive relapse+ Len maintenance - Len maintenance + Len maintenance - Len maintenance
Consider adding Ixazomib/Dex*
Consider Adding Elo/Dex*
* Increase len dose
Consider Dara/Len/Dex
Consider Elo/Len/Dex
Consider Car/Len/Dex
Consider Dara/Pom/Dex
Consider Car/Pom/Dex
Consider Dara/Len/Dex
Consider Dara/Vel/Dex
Consider Car/Pom/Dex

Emory (exanded)Approach to Early Relapse
Slow indolent relapse Aggressive relapse+ Len maintenance - Len maintenance + Len maintenance - Len maintenance
Consider adding Ixazomib/Dex*
Consider Adding Elo/Dex*
Car/dex
Consider Dara/Vel/Dex
Consider Dara/Len/Dex
Consider Elo/Len/Dex
Car/dex
Consider Car/Len/Dex
Consider Dara/Pom/Dex
Consider Car/Pom/Dex
Consider Car/Len/Dex
Consider Dara/Vel/Dex
Consider Dara/Len/Dex
Consider Dara/Vel/Dex
Consider Car/Pom/Dex
Consider Car/Len/Dex