Embed Size (px)
Citation preview

13.5 0. ROSS BEIRNE
References Ramstrom (;. Sintlct-l’cdcrxn 5. Hall G. et al: Prc-vcntion of postsurgic;?l hlccding in oral surgrr) using trancsamic acid without dose moditication of or.ll anticoagulants. J Oral hlnsillo- f;ic Surg i I : 12 11, 1993 13ow;1 (;. Monte-hugnoli L. Capuzzi I’. ct al: Trancsamic acid as ;I mouthn-ash in ;Inticoaaul:lnt-treated patients undergoing 0rA surge?: An alternative method to discontinuing anticoagulant therapy Oral Surg Oral >MMed OrA Pathol ‘5:29. 1993 Souto JCL Oliver A. Zuazu-Jausoro I. et al: OrA surgcy in anticoagulated patients without reducing the dose of oral anticoagulant: A prospective randomized study. J Oral ~Masillo- fat Surg i4:2-. 1996 (discussion 32-j) Beirne OK. K;oehkr JR: Surgical management of patients on warfarin sodium. J OrA hlaxillofac Surg ii: 1 1 15. 1996 Saour JN. Ali Hr\. Matnmo L4. et al: Dental procedures in patients receiving oml anticoagulation therapy. J Heart Valve Dis 3.315. 1994 . Zusman SP, Lustig JP. Bin Nun G: Cost c-valuation of t\vo methods of post tooth extmction hrmostasis in patients on anticoagulant therap! Community Dental Health 10: 16’. 1993 Dcvani P. Lava-rhy M, Howell (IJT: Dental extractions in patients on warfarin: Is alteration of the anticoagulant regime ncccssary? BrJ Oral Masillofac Surg 36: IO’. 1998 Kurvandl SK. Balm K. Gostout <:I: The risli of withdrawing chronic anticoagulation hccausc- of acute GI bleeding. Am J Gastroenterol 92:361. 199’
9
IO
II
I2
15
I-1
Ii
16
I’
Polk I.. Thomson J. Evidcncc for “rchound” hypcrcoagulahil- ity after stopping anticoagulants. knee-t 2:62. 196-t Palarrti (;. Lrgnani (:. (;uazzaloca G. et al: Acti\;nion of blood coagulation after abrupt or stcpwk withdrawal of oral antictr agulants: A prospcctivc study. Thrombosis & Hnemostasis ‘2:222. 19% Grip 1.. Blomb;ick Xl. Schulman S: Hypercoagukthlc state and thromhoc-mholisnl following warfarin withdrawal in post- m!ocardi;ll-inf;lrction patirnts. Eur Hrart J 12: 1225. 1991 Cenrwc-in li. Haehcrli A. Strnth PW. et al: Kc-hound after cessation l,f oral anticoagulant thcmpy: The biochemical evi- dence. BrJ Haematol 92:-1’9. 1996 Tardy B. Tardy-Poncct B. l;cporte-Simitsidis S. et al: Evolution of blood coagulation and lihrinolysis pdramcters after abrupt vc’rsus gmdual withdra~val of acc.nocoumarol in patients with vc’noub thromhoemholisni: A double-blind mndomized study. BrJ Haematol 96: 1’4. 199’ Woltcrs H. trn Catc H. Thomas LLXI. et al: Low-intrnsiy oral anticoagulation in sickle-cell discasc rcvc’rses the prethrom- hotic state: Promises for trcatmcnt? BrJ Hacm~tol9O:‘li. 1995 Ezcko\vitz MD. Bridgcrs SL. James KE. et al: Warbrin in the prrvcntion of btrokcr associated with nonrheumatic atrial fihril- Mon. N En@ J Sled 32’: 146. 1992 The- Boston Arca Anticoagulation Trial for htrial Fibrillation Investigators: The effect of lo\v-dosc- warfarin on the risk of strok in patients with nonrheumatic atrial fibrillation. N Engl J Xlc-d 523: 1 iOi. 1990 KistlerJP. Singer DE. Millenson MM. c’t al: Efkct of low-intensit) \varfarin anticoagulation on kvc-I of activiq of the hemostatic system in patients with atrial tihrillation. Stroke 2-k: 1360. 1993
J Oral Monlllofa; swg 58 135-l 36 2000
Discussion
Anticoagulation and Minor Oral Surgery: Should the Anticoagulation Regimen Be Altered?
0. Ross Beime, DMD, PIJD Professor and Choir, Unlverslty of WashIngton, Department of Oral and Mox~llofoc~al Surgery. Seattle, Woshlngton, emall slsbQu washington edu
The or4 and maxillofacial surgeon is frequently asked to manage patients who are chronically anticoagulated with Coumadin (DuPont, Wilmington, DE) derivatives. The aim of treatment is to minimize the risli of hemorrhage while continuing to protect the patient against thromboembolism formation. However, the management of these patients is controversial.’
Coumadin derivatives alter clotting by competitively inbib iting vitamin K activation by vitamin K epoxide reductase.’ Active vitamin K is needed for carboxylation of the gluta- mate residues in factors II, VII. IX. and X. Inhibition of this posttranslational modification makes die clotting factors biologically inactive. Factors with the shortest half-life are affected first. and factors with the longest half-life recover last. Because Coumadin derivatives affect the synthesis of active clotting factors, changing the dose of these anticoagu- lates does not have an immediate effect on c0ilglkltiOtl.
Recovery is not only dependent on the distribution and elimination of the drugs, but also on the synthesis of active clotting factors.
Because Coumadin anticoagulation cannot be reversed rapidly. clinicians have suggested several different protocols for managing patients taking Coumadin derivatives.3 The risk of bemorrbage can be reduced by decreasing the dose of Coumadin derivatives before surgery. Coumadin therap) can be stopped for severzl days before extracting the teeth and anticoagulation therapy begun immediately after sur- gery. Coumadin tbempy can be stopped, the patient admit- ted to the hospital. and intravenous bepatin used to adjust anticoagulation because its effects are reversed must faster than the effects of the Coumadin derivatives. Sometimes extractions can be done without changing a patient’s anticoagulation therapy. However, any time that Coumadin therapy is stopped or altered. the patient is at increased risk for developing a life-threatening thrombus.
Because of the risks associated with stopping Coumadin therapy. the preferred treatment for patients needing oral and maxillofacial surgery is to continue such therapy..’ Even though many reports recommend continuing Coumadin therapy, few controlled clinical trials have examined this issue. After an exhaustive search of the literature, Wahl’ concluded that the risk for hemorrhage was minimal and anticoagulation thempy should not be altered before dental
136 DISCIISSION
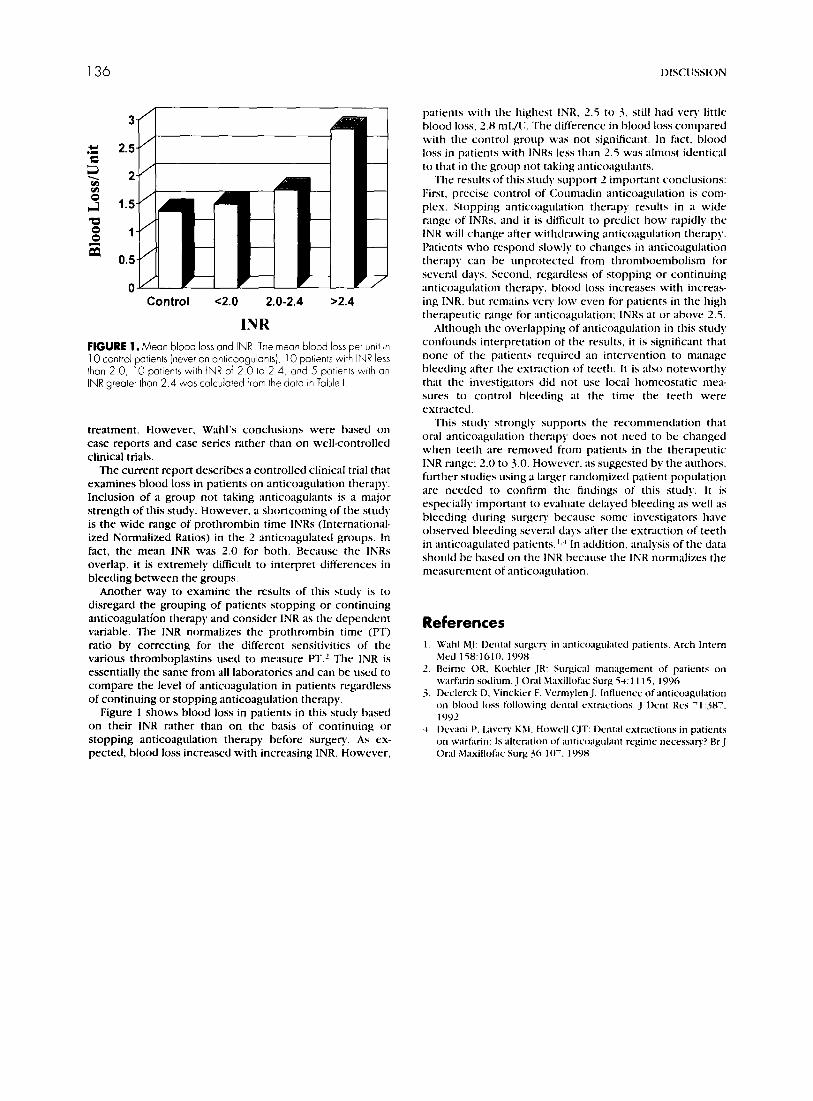
Control e2.0 2.0-2.4 >2.4
INR FIGURE 1. Mean blood loss ond INR The mean blood loss per unit in 10 control patients (never on anticoagulants), IO patients with INR less than 2 0, IO patients with INR of 2 0 to 2 4, and 5 potlents with an INR greater than 2 4 was calculated from the data In Table I
treatment. However, Wahl’s conclusions were based on case reports and case series rather than on well-controlled clinical trials.
The current report describes a controlled clinical trial that examines blood loss in patients on anticoagulation therapy. Inclusion of a group not taking anticoagulants is a major strength of this study. However. a shortcoming of the stud) is the wide range of prothrombin time INRs (Intemational- ized Normalized Ratios) in the 2 anticoagulated groups. In fact, the mean INR was 2.0 for both. Because the INRs overlap, it is extremely difficult to interpret differences in bleeding between the groups.
Another way to examine the results of this study is to disregard the grouping of patients stopping or continuing anticoagulation therapy and consider INR as the dependent variable. The INR normalizes the prothrombin time (PT) ratio by correcting for the d8erent sensitivities of the various thromboplastins used to measure FT.l The INR is essentially the same from all laboratories and can be used to compare the level of anticoagulation in patients regardless of continuing or stopping anticoagulation therapy.
Figure 1 shows blood loss in patients in this study based on their INR rather than on the basis of continuing or stopping anticoagulation therapy before surgery. As cx- petted. blood loss increased with increasing INR. However,
patients with the highest INR. 2.5 to 3. still had very little blood loss. 2.8 ml./ll. The difference in blood loss compared with the control group was not significant. In fact, blood loss in patients with INRs less than 2.5 was almost identical to that in the group not taking anticoagulants.
The results of this study support 2 important conclusions: First, precise control of Coumadin anticoagulation is com- plex. Stopping anticoagulation thempy results in a wide range of INRs, and it is difficult to predict how rapidly the INR will change after withdrawing anticoagulation therapy. Patients who respond slowly to changes in anticoagulation therapy can he unprotected from thromhoenlbolism for several days. Second, regardless of stopping or continuing anticoagulation therapy. blood loss increases with increas- ing INR, hut remains very low even for patients in the high therapeutic range for ;InticoagLll;ltit,n: INRs at or above 2.5.
Although the overlapping of anticoagulation in this stud! confounds interpretation of the results, it is significant that none of the patients required an intervention to manage hleeding after the extraction of teeth. It is also noteworthy that the investigators did not use local homeostatic mea- sures to control bleeding at the time the teeth were extracted.
This study strongly supports the recommendation that orA anticoagulation therapy does not need to be changed when teeth are removed from patients in the therapeutic INR range; 2.0 to 3.0. However, as suggested by the authors. huther studies using a larger randomized patient population are needed to confirm the Iindings of this study. It is especially important to evaluate delayed bleeding as well as bleeding during surgev because some investigators have observed bleeding several days after the extraction of teeth in anticoagulated patients. I.’ In addition, analysis of the data should he based on the INK because the INR normalizes the measurement of anticoagLll;ltion.
References
L. Deimc OR. Ko~hlc-r JR: Surgical management of pdric-nts on warfarin sodium. J Oral Maxillofac Surg 5-1: 1 I 15. 1996
3. Dc-ckrck D, Vinckicr f:. V~rnmylen J: Intlurncc of anticoagulation on blood loss following drntal CstrJctions. J lknt RCS 7 I :38’. 1992
1. Dc-vani I’. L;lvrry Kbl. Howe-II CJT: tkntal extractions in patknts on warfarin: Is alttmtion of antic‘oa@int rqimr neccssaq? Ur J Oral Masillofac Surg 36: IO’. 1998