Embed Size (px)
Citation preview

Anticoagulation Using new anticoagulants in AF, VTE
and PE
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group
Dr Matthew Fay GP Principal The Willows Medical Practice:-Queensbury
GPwSI and Co-Founder Westcliffe Cardiology Service Clinical Partner The Westcliffe Medical Group

Declaration of interests
• The practice has received funding from: Abbott, Bayer, Boehringer-Ingelheim, Bristol Myers Squibb, Dawn, INRStar, Medtronic, Oberoi Consulting, Pfizer, Roche, Sanofi-Aventis, Servier.
• An advisor to: AF Association, Anticoagulation Europe, Arrhythmia Alliance, Heart Valve Voice, National Stroke Association, Syncope Trust
• A trustee of Thrombosis UK



Learning Points
• Thrombosis • DVT • AF • NOACs • Food for thought

Thrombosis

Haemostasis
Successful haemostasis depends on • vessel wall • coagulation system • fibrinolytic system
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Blood Vessels
• constrict to limit blood loss • arteries, veins, capillaries • mechanism not fully understood
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

9
PLATELETS
On contact with fibrin or collagen platelets release granules which promote aggregation of adjacent platelets to form a mass which covers, for example, an endothelial defect.
Contact with Fibrin or Collagen
Release Granules
Aggregate to form a mass E.g. Covering Endothelial
Defect
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

10
PLATELETS
Platelet aggregation in this way is a normal phenomenon, and occurs continuously in the body to repair minor endothelial injury.
In excess, a mass is formed in a vessel: THROMBOSIS
Contact with Fibrin or Collagen
Release Granules
Aggregate to form a mass E.g. Covering Endothelial
Defect
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Coagulation System
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Coagulation
• Cascade • Series of inactive components converted to
active components Coagulation
Cascade
Fibrinogen Fibrin
Soluble Solid
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Coagulation
• 1 ml of blood can generate enough thrombin to convert all the fibrinogen in the body to fibrin
• Tight regulation therefore required • Balance of procoagulant and anticoagulant
forces
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Control of Coagulation
• Thrombin destroys factors V and VIII • Thrombin inhibitors
– anti-thrombin III* – alpha 1 anti-trypsin – alpha 2 macroglobulin – protein C and S* * inherited deficiency may predispose to thrombosis
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Fibrinolysis
• Breakdown of fibrin • Plasminogen Plasmin Plasminogen activators • Fibrinolytic therapy widely used
– streptokinase – tPA
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Endothelium
• Anti-thrombotic – plasminogen activators – prostacyclin – nitric oxide – thrombomodulin
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

What is a Thrombosis
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

What is a Thrombosis?
• Solid mass of blood constituents
• Formed within the vascular system
• In life
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Thrombosis is different to Clot!
• Clotting means coagulation which can occur within or outside the vascular system in life or post mortem.
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Why does thrombosis occur?
• Abnormalities of the vessel wall
– atheroma – direct injury – inflammation
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Why does thrombosis occur?
• Abnormalities of blood flow – stagnation – turbulence
• Abnormalities of blood components – smokers – post-partum – post-op
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

24
PREDISPOSING FACTORS FOR THROMBOSIS
Factors which promote thrombosis can be found in the blood vessel wall, or be concerned with the flow of blood or its constituents.
This group of three factors is known as Virchow’s triad.
WALL
FLOW BLOOD CONSTITUENTS
Virchow’s Triad
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

25
TYPES OF THROMBI
Thrombi can occlude a vessel which may result in necrosis of the part served (infarction).
Mural thrombus can release fragments (emboli) which can travel in the bloodstream to block distal vessels.
Thrombus on heart valves due to infection can also embolise.
Occlusive
Mural
Vegetation
Infarction
Embolism
Embolism
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

26
OUTCOMES OF THROMBOSIS
Lysis Fibrosis
Recanalisation Embolism
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Thrombosis-DVT

Deep Vein Thrombosis • DVT is the formation of a thrombus in a
deep vein. • Usually in the legs; partially or completely
obstructs blood flow. • Annual incidence is about 1 in 1000
people. • The most serious complication is
pulmonary embolism. • Only about a third of people with a clinical
suspicion of DVT have the condition.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Risk factors for DVT • Risk factors include:
– Previous venous thromboembolism. – Cancer (known or undiagnosed). – Increasing age. – Being overweight or obese. – Male sex. – Heart failure. – Acquired or familial thrombophilia. – Chronic low-grade injury to the vascular wall (for
example vasculitis, hypoxia from venous stasis, or chemotherapy).
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Temporary risk factors • Risk factors that temporarily raise the
likelihood of DVT: – Immobility, significant trauma, or direct trauma
to a vein. – Hormone treatment (for example oestrogen-
containing contraception or hormone replacement therapy).
– Pregnancy and the postpartum period. – Dehydration.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Differential Diagnosis?
• Physical trauma: – Calf muscle tear or strain. – Haematoma (collection of blood) in the
muscle. – Sprain or rupture of the Achilles tendon. – Fracture.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Differential Diagnosis? • Cardiovascular disorders:
– Superficial thrombophlebitis. – Post-thrombotic syndrome. – Venous obstruction or insufficiency, or external
compression of major veins (for example by a fetus during pregnancy, or cancer).
– Arteriovenous fistula and congenital vascular abnormalities.
– Acute limb ischaemia. – Vasculitis. – Heart failure.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

• Other conditions including: – Ruptured Baker's cyst. – Cellulitis (commonly mistaken as DVT). – Dependent (stasis) oedema. – Lymphatic obstruction. – Septic arthritis. – Cirrhosis. – Nephrotic syndrome. – Compartment syndrome.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.
Differential Diagnosis?

When to suspect a DVT • Suspect a DVT if the person has:
– Signs or symptoms of a DVT: • Pain and swelling in one leg, although both legs
may be affected. • Tenderness, changes to skin colour and
temperature, and vein distension. – A risk factor for DVT
• previous VTE • Immobility
• To exclude an alternative cause:
– Carry out a physical examination. – Review the person's general medical history.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Managing a suspected DVT
• Refer immediately if pregnant or given birth within the past 6 weeks. – Requires same-day assessment and management as it is not possible to
accurately assess the risk of DVT in primary care.
• For everyone else, use the two-level DVT Wells score to assess likelihood of DVT and inform further management.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Using the two-level DVT Wells score
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.
Criteria Score
Active cancer (treatment ongoing, within the last 6 months, or palliative). 1
Paralysis, paresis, or recent plaster immobilization of the legs 1
Recently bedridden for 3 days or more, or major surgery within the last 12 weeks requiring general or local anaesthetics
1
Localized tenderness along the distribution of the deep venous system (such as the back of the calf)
1
Entire leg is swollen. 1
Calf swelling by more than 3 cm compared with the asymptomatic leg (measured 10 cm below the tibial tuberosity).
1
Pitting oedema (greater than on the asymptomatic leg) 1
Collateral superficial veins (non-varicose). 1
Previously documented DVT 1
If an alternative cause is considered more likely than DVT. -2

Two-level DVT Wells score
• Validated, simple scoring system that takes into account previous DVT.
oDVT is likely if the score is two points or more. oDVT is unlikely if the score is one point or
less.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Other methods of assessment • Do not use:
– Individual symptoms and signs on their own. • On their own they are poor predictors of the
presence or absence of DVT. – A positive Homans' sign (pain in the calf or
popliteal region on passive, abrupt, forceful dorsiflexion of the ankle with the knee in a flexed position):
• Is insensitive and nonspecific. • Can be painful, and there is a theoretical possibility
of dislodging a thrombus.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

If DVT likely (>2 points) • Refer for a proximal leg vein ultrasound scan to
be carried out within 4 hours. • If a proximal leg vein ultrasound scan cannot be
carried out within 4 hours of being requested: – Take a blood sample for D-dimer testing. – Give an interim 24-hour dose of a anticoagulant
• Ensure a proximal leg vein ultrasound scan is carried out within 24 hours of being requested.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Which anticoagulant? • Offer a choice of low molecular weight
heparin (LMWH) – Licensed LMWHs for DVT treatment include
dalteparin, enoxaparin, and tinzaparin. • Offer a choice of Xa Inhibitor
– Apixaban and Rivaroxaban – Fondaparinux is a synthetic pentasaccharide that
inhibits activated factor X but is parentral • Choice of anticoagulant depends on:
– Comorbidities – Contraindications – Cost
• Local policy may also influence choice.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

If DVT unlikely (< 1point) • Offer D-dimer testing. • If negative D-dimer test - consider an alternative
diagnosis to explain symptoms. • If positive D-dimer test - refer for a proximal leg
vein ultrasound scan to be carried out within 4 hours.
• If a proximal leg vein ultrasound scan cannot be carried out within 4 hours of being requested: – Give an interim 24-hour dose anticoagulant
• Ensure a proximal leg vein ultrasound scan is carried out within 24 hours of being requested.
Based on the CKS topic DVT (April 2013) and NICE guidance (2012a); Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing.

Thrombosis-AF

Personalised package of care and information
Diagnosis of AF
Stroke prevention
Rate control strategies
Ablation strategies
Nice AF Guideline DRAFT: January 2014
Symptomatic Asymptomatic
Symptomatic
Rhythm Control Strategy
On-going annual assessment NICE AF Guideline June 2014

Stroke Risk

Stroke risk in AF: CHADS2
CHADS2 risk criteria Score
Cardiac failure 1
Hypertension 1
Age >75 yrs 1
Diabetes mellitus 1
Stroke or TIA (previous history) 2

Stroke risk in AF: CHA2DS2VASc CHA2DS2VASc risk criteria Score
Cardiac failure 1
Hypertension 1
Age >75 yrs 2
Diabetes mellitus 1
Stroke or TIA (previous history) 2
Vascular disease (IHD, PAD) 1
Age >75 yrs 1
Sex Category 1

AF PIE: PAST
Fuster V. Circulation 2012; epubl April 18
AF PIE: FUTURE

AVERROES
Apixaban (%)
Aspirin (%)
Assessment that INR could be maintained in therapeutic range
17 17 X
Assessment that INR could not or was unlikely to be measured at requested intervals
43 43 X
Uncertainty about patients ability to adhere to instructions regarding VKA Therapy 16 15 X
CHADS2 score of 1 and VKA therapy not recommended by physician 21 22 X
Patients refusal to take VKA 38 37
Multiple reasons for unsuitability of VKA therapy 51 52 X

Cum
ulat
ive
Risk
0.
0 0.
01
0.03
0.
05
0 3 6 9 12 18 21
ASA 81-324 mg/d
Apixaban 2.5-5 mg bd
No. at Risk ASA Apix
2791 2720 2541 2124 1541 626 329 2809 2761 2567 2127 1523 617 353
Months
RR= 0.46 95%CI= 0.33-0.64 p<0.001
AVERROES: Stroke or SEE 5600 patients, 36 countries, 522 centres

Cum
ulat
ive
Risk
0.
0 0.
005
0.01
0 0.
015
0.02
0
0 3 6 9 12 18 21
ASA
Apixaban
No. at Risk ASA Apix
2791 2744 2572 2152 1570 642 340 2809 2763 2567 2123 1521 622 357
Months
RR= 1.14 95%CI= 0.74-1.75 P= 0.56
AVERROES - Major Bleeding
N Engl J Med. 2011;364:806-817

Bleeding Risk

HAS-BLED risk criteria Points awarded
Hypertension (i.e. Uncontrolled BP) 1
Abnormal renal and liver function (1 point each) 1 or 2
Stroke 1
Bleeding 1
Labile INRs 1
Elderly (e.g. age >65 years, frail condition) 1
Drugs or alcohol (1 point each) 1 or 2
Maximum 9 points
Bleeding risk in AF: HAS-BLED
NICE AF Guideline June 2014

Antiplatelet Use for Stroke Prevention in AF

Aspirin vs Placebo in Stroke Prevention in AF
Favors Placebo/ Control
Antiplatelet therapy reduces incidence of stroke by about 22%
Hart R, et al. Ann Intern Med. 2007;146:857-867.
All Trials
100% 50% 0% -50% -100%
AFASAK-1 SPAF I EAFT ESPS-II LASAF, daily
UK-TIA, 300 mg daily
Favors Antiplatelet
LASAF, alternate day
UK-TIA, 1200 mg daily JAST Aspirin Trials SAFT ESPS II, Dipyridamole ESPS II, Combination

Vitamin K Oral Anticoagulant Use for Stroke Prevention in AF

Warfarin vs Placebo in Stroke Prevention in AF
100% 50% 0% -50% -100%
AFASAK-1
SPAF BAATAF
CAFA
SPINAF
EAFT
ALL Trials
Favors Warfarin Favors Placebo/ Control
Hart R, et al. Ann Intern Med. 2007;146:857-867.
Warfarin reduces incidence of stroke by about 64%

Time in therapeutic range (TTR) matters
0 500 1000 1500 2000
Survival to stroke (days)
0.6
0.7
0.8
0.9
1.0
Cum
ulat
ive
surv
ival
71–100%
Warfarin group
61–70% 51–60% 41–50% 31–40% <30% Non warfarin
Morgan CL et al. Thrombosis Research 2009;124:37–41.

- 58 -

Non Vitamin K Oral Anticoagulant Use for
Stroke Prevention in AF

The perfect anticoagulant • Effective • Oral • Fast onset of action • Short half life • Predictable pharmacokinetics • No drug/food interactions • Fully reversible • Do the NOACs fulfill these criteria?

Indications and Dosing
Dabigatran Apixaban Edoxaban Rivaroxaban
Prevention of VTE post THR/TKR
110mg bd 2.5mg bd 10mg od
Prevention of CVA in AF
150mg bd (110mg bd)
5mg bd (2.5mg bd)
60mg od 20mg od
Treatment of acute VTE 150mg bd
10mg bd for 7/7
5mg bd 60mg od
15mg bd for 3/52 20mg od
SPC Dabigatran, Rivaroxaban, Apixaban

Renal function
Anticoagulant Creatinine clearance (ml/min) 30-50 30-15 <15
Apixaban 5mg bd 2.5mg bd AVOID Dabigatran 150mg bd (110mg bd) AVOID Edoxaban 60mg 30mg AVOID Rivaroxaban 15mg od 15mg od AVOID

How do NOACs affect the coagulation screen?

Coagulation tests with Anticoagulant Drugs
Test UFH LMWH Warfarin Rivaroxaban Apixaban Dabigatran PT - - ↑↑↑ ↑/- -/↑ -/↑ APTT ↑↑↑ -/↑ ↑ -/↑ -/↑ ↑↑↑ Fibrinogen - - - - - - Thrombin Time
↑↑↑
↑
- - - ↑↑↑
Anti-Xa ↑
↑↑↑ - ↑↑↑
↑↑↑
-
Haemoclot ↑↑ ↑ - - - ↑↑↑
Rivaroxaban and Apixaban: The PT and APTT cannot be used to determine whether anticoagulant drug present

Switching from one anticoagulant to another

Switching from warfarin to NOAC
• Apixaban – Wait till INR < 2.0
• Dabigatran – Wait till INR < 2.0
• Edoxaban – Wait till INR < 2.5
• Rivaroxaban – Wait till INR < 3.0 AF – Wait till INR < 2.5 DVT, PE

ESC Practical Guide on the use of NOAC 2013
What to do if a dose of a NOAC is missed?
• Once daily regimens – Take the forgotten dose up to 12hrs after time
of usual intake • Twice daily regimens
– Take the forgotten dose up till 6hrs after time of usual intake

Bleeding
• Local measures • Stop NOAC temporarily • Tranexamic acid • Coagulation screen • Renal function • Discuss with haematologist if ongoing issue

Elective minor (when warfarin would not be stopped)
Dabigatran Rivaroxaban Apixaban
Minor dental work 12 hours post dose 18-24 hours post dose
>24 hours post dose
Major dental work 24 hours post dose Next dose > 4 hours post procedure
24 hours post dose Next dose > 4 hours post procedure
24-48 hours post dose Next dose > 4 hours post procedure
Upper/lower Endoscopy + simple biopsy Cataract removal Joint injection
24 hours post dose Next dose > 4 hours post procedure
24 hours post dose Next dose > 4 hours post procedure
24-48 hours post dose Next dose > 4 hours post procedure
NHS GGC Guidance based on SPC Dabigatran, Rivaroxaban, Apixaban

Emergency Surgery and Bleeding

Warfarin
• Vitamin K – IV 6 hours – PO 24 hours
• Prothrombin complex concentrates (PCCs) – Factors II, VII, IX, X – Reversal within 30 minutes
• Can assess INR for effectiveness/safety

NOACs • No specific reversal agent • Well-adsorbed to activated charcoal
– give within two hour of swallowing • Dialysis
– Dabigatran – yes – Rivaroxaban, apixaban – no
• General principles – Check coagulation screen
• Assess effect – Check renal function
• Assess half life • Products
– largely speculation/ based on non-clinical data – off-licence use; safety issues (thrombosis)

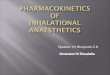
Vitamin K - no Immediate Effect on INR • Schematic diagram showing effect of vitamin K on INR • Vitamin K has a slow onset (>24 hours)1
– Vitamin K supports generation of normal, functioning clotting factors in the liver – Effectivity of INR normalization depending on VKA used (different half-lifes; (from
9–11 hours for acenocoumarol, to 90–140 hours for phenprocoumon)1,2
1. Heidbuchel et al, 2013; 2. Scharf et al, 2009
Day 1 Day 2
PD profile (INR) of VKA t½ of VKA ~4–5 days
INR
PD profile (INR) after administration of vitamin K 3
2
Vitamin K injection
4

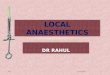
Emergencies in Anticoagulated Patients
• Schematic diagram showing PK/PD characteristics of VKA and rivaroxaban – Reversal strategies may be required if action of drug is long and needs to be antagonized
in emergency situations
1. Makris et al, 2012; 2. Kubitza et al, 2005; 3. Kubitza et al, 2008
Day 1 Day 2
PD profile (INR) of VKA
PK/PD profile of rivaroxaban
t½ of VKA ~4–5 days
t½ of rivaroxaban 5–9 hours (young) or 11–13 hours (elderly)
Sche
mat
ic d
iagr
am
PD, pharmacodynamic; PK, pharmacokinetic; t½, half-life

Rivaroxaban-Induced Anticoagulation Reversal with PCC
• 20 mg rivaroxaban was administered bid for 2.5 days followed by PCC (Prothrombin Complex Concentrate - Cofact®, 50 U/kg body weight)
• Prolongation of PT was reversed completely by PCC
• ETP was reversed by PCC with an overshoot in effects
• Limitation – PT agent used showed low sensitivity
to rivaroxaban – Prolongation of PT in this study was
approximately 4 seconds at maximum
18 −
16 −
14 −
12 −
10 −
Time
PT in
seco
nds
Placebo
PCC
Eerenberg et al. Circulation 2011;124:1573–1579
Rivaroxaban (2.5 days)
PCC

Specific Reversal Agents for Non-VKA Oral Anticoagulants
Company Compound Reversal for:
Status Factor Xa inhibitor
Factor IIa inhibitor
LMWH/ fondaparinux
Portola Pharma-ceuticals
PRT064445/ (andexanet alfa) Universal No
Yes (antithrombin-
mediated Factor Xa inhibition)
Phase II completed One phase III with
apixaban completed; rivaroxaban and
edoxaban - onngoing
Boehringer Ingelheim
BI 655075 (idarucizumab) No Specific for
dabigatran No Phase I completed;3
phase III started4
Perosphere, Inc.
PER977 (aripazine) Universal Universal Universal Phase I completed5

Dabigatran antidote: idarucizumab
Disclaimer: idarucizumab is not currently licensed for use Date of prep: March 2015 UK/CVS-141014b

Idarucizumab development process
Monoclonal mouse antibody developed with high dabigatran binding affinity Monoclonal antibody was then humanized and directly
expressed as a Fab fragment in mammalian cells
Humanized Fab
Chimeric Fab
Human
Mouse
Mouse antibody
Fab region
Fc region
Disclaimer: idarucizumab is not currently licensed for use Date of prep: March 2015 UK/CVS-141014b
van Ryn J. Presented at the AHA Congress, Los Angeles, USA. 5 November 2012. Presentation 9928; van Ryn J et al. Circulation 2012;126:A9928

Idarucizumab characteristics
Fully humanized antibody fragment (Fab)
Potently binds dabigatran
No prothrombotic or antithrombotic effects
Short half-life
No endogenous targets
Intravenous administration
van Ryn J. Presented at the AHA Congress, Los Angeles, USA. 5 November 2012. Presentation 9928;
van Ryn J et al. Circulation 2012;126:A9928
Disclaimer: idarucizumab is not currently licensed for use Date of prep: March 2015 UK/CVS-141014b

Idarucizumab mode of action
Disclaimer: idarucizumab is not currently licensed for use
Idarucizumab rapidly binds to dabigatran in the plasma Idarucizumab alters the
equilibrium – dabigatran dissociates from thrombin
Antidote (idarucizumab)
Thrombin
Dabigatran molecule
Dabigatran inhibiting thrombin
Dabigatran bound to plasma proteins
Unbound dabigatran
Date of prep: March 2015 UK/CVS-141014b


Practical Considerations
Created 2/1/2016 Dr. Matthew Fay: Westcliffe Medical Group

Starting a patient on a NOAC
• Check patient is not taking interacting drugs • Counsel patient: it is an anticoagulant
– Head injury, trauma, melaena, significant GI bleed, prolonged epistaxis, large ecchymoses/ haematoma
• Compliance- important to take as advised (od Rivaroxaban, bd Apixaban, bd Dabigatran)
• Baseline FBC, renal and liver function


Summary of use of NOACs • Benefits of novel anticoagulants
– Non inferior/superior to warfarin – More stable anticoagulation (in patients poorly controlled
on warfarin) – Shorter half life – No requirement for anticoagulant monitoring – Fewer drug-drug interactions – No food-drug interactions – Less intracranial bleeding
• But – Limited reversal options – Increased drug costs compared to warfarin – Current lack of familiarity


Fig 2 Cumulative incidences for major adverse cardiovascular event during two year follow-up for patients receiving warfarin versus no oral anticoagulant .
Ying Xian et al. BMJ 2015;351:bmj.h3786
©2015 by British Medical Journal Publishing Group

Fig 3 Major adverse cardiovascular event (MACE) and home time according to warfarin treatment at discharge, overall and in clinically relevant subgroups.
Ying Xian et al. BMJ 2015;351:bmj.h3786
©2015 by British Medical Journal Publishing Group

Learning Points
• Thrombosis • DVT • AF • NOACs • Food for thought