-
7/31/2019 Antidiabetic Buccal Dosage Form
1/21
1. IntroductionBy, Vikram Viswajit Mishra,
M.Pharma
Jeypore College of Pharmacy
E-mail id [email protected]
The effect of new formulations can be enhanced by the
development of newer release
systems. The main controlled drug delivery systems currently
available include matrices,
pellets, floating systems, liposomes, microemulsions, liquid
crystals, solid dispersions,
nanosuspensions, transdermal systems, cyclodextrin inclusion
complexes, osmotic pumps and
bioadhesive systems. The potential use for mucoadhesive systems
as drug carriers lies in its
prolongation of the residence time at the absorption site,
allowing intensified contact with the
epithelial barrier. When adhesion is restricted to the mucosal
membrane it is called as
mucoadhesion. Mucous membrane is the main administration site
for bioadhesive systems.
Mucous membranes of human organism are relatively permeable and
allow fast drug
absorption. They are characterized by an epithelial layer whose
surface is covered by mucus.
This approach to confer bioadhesion properties has been widely
applied in the development
of a number of drug delivery systems.
[1-2]
The Mucosal Buccal Delivery has brought about a great change in
the pharmaceutical
arena. It produces a sustained release of drug over a prolonged
time, thereby reducing
frequent dosing. The area is well suited for a retentive device
and appears to be acceptable to
the patient. With the right dosage form design and formulation,
the permeability and the local
environment of the mucosa can be controlled and manipulated in
order to accommodate drug
permeation. Buccal drug delivery is a promising area for
continued research with the aim of
systemic delivery of orally inefficient drugs as well as a
feasible and attractive alternative for
non-invasive delivery of potent peptide and protein drug
molecules.[3- 4]
1.1 Diabetes
Diabetes is a group of metabolic diseases in which a person has
high blood sugar, either
because the body does not produce enough insulin, or because
cells do not respond to the
insulin that is produced. This high blood sugar produces the
classical symptoms of polyuria(frequent urination), polydipsia
(increased thirst) and polyphagia (increased hunger).
-
7/31/2019 Antidiabetic Buccal Dosage Form
2/21
Diabetes is a condition in which the quantity of glucose in the
blood is raised called
hyperglycemia. This happens when there is low or no insulin
production or improper use of
insulin.
Types of Diabetes
There are two major types of diabetes. They are as follows:
1. Type 1 DM: It results from the body's failure to produce
insulin, and presentlyrequires the person to inject insulin. (Also
referred to as insulin-dependent diabetes
mellitus (IDDM) or "juvenile" diabetes). Type 1 diabetes can
occur in an older
individual due to destruction of the pancreas by alcohol,
disease, or removal by
surgery.
2. Type 2 DM: It results from insulin resistance, a condition in
which cells fail to useinsulin properly, sometimes combined with an
absolute insulin deficiency. (Formerly
referred to as noninsulin-dependent diabetes mellitus (NIDDM) or
"adult-onset"
diabetes).
Epidemiology
Globally, as of 2010, an estimated 285 million people had
diabetes, with type 2 making up
about 90% of the cases. Its incidence is increasing rapidly, and
by 2030, this number is
estimated to almost double. Diabetes mellitus occurs throughout
the world, but is more
common (especially type 2) in the more developed countries. The
greatest increase in
prevalence is, however, expected to occur in Asia and Africa,
where most patients will
probably be found by 2030. The increase in incidence in
developing countries follows the
trend of urbanization and lifestyle changes, perhaps most
importantly a "Western-style" diet.
This has suggested an environmental (i.e., dietary) effect, but
there is little understanding of
the mechanism(s) at present, though there is much speculation,
some of it most compellingly
presented. India has more diabetics than any other country in
the world, according to the
International Diabetes Foundation, although more recent data
suggest that China has even
more. The disease affects more than 50 million Indians - 7.1% of
the nation's adults - and
kills about 1 million Indians a year. The average age on onset
is 42.5 years. The high
-
7/31/2019 Antidiabetic Buccal Dosage Form
3/21
incidence is attributed to a combination of genetic
susceptibility plus adoption of a high-
calorie, low-activity lifestyle by India's growing middle
class.[6-7]
Pathology of Diabetes
Diabetes (Hyperglycemia), which is defined as fasting plasma
glucose above 126 mg/dl &
oral glucose tolerance test (OGTT) above 200 mg/dl
Pre-Diabetes is defined as impaired fasting glucose (IFG) of
100-125 mg/dl & impaired
glucose tolerance (IGT) of 140-199 mg/dl
Acute Complications of Uncontrolled Diabetes (all directly
caused by hyperglycemia)
--Polyuria due to excess fluid intake and glucose-induced
osmotic diuresis --Weight loss due to calories lost as glucosuria,
leaving a negative calorie balance --Poor wound healing,
gingivitis, blurred vision
Chronic Complications of Uncontrolled Diabetes
Chronic complications may be due to mitochondrial superoxide
overproduction in response to
hyperglycemia.
Macro vascular Atherosclerosis: diabetics have a high incidence
of coronary, cerebral, and
peripheral artery diseases. Caused by dyslipidemias including
elevated LDL and triglycerides,
low HDL, and reduced fibrinolysis activity. Management includes
foot care.
Micro vascular Diseases of Diabetes
1. Diabetic Retinopathy has many manifestations, including micro
aneurysms, microhemorrhages, proliferative vessel changes, and
vitreous bleeds (cause blindness). Diabetic
retinopathy is caused by basement membrane deterioration and
ischemia.
2. Nephropathy progresses from micro albuminuria to proteinuria
to uremia to ESRD.
Nephropathy is caused by hyper filtration, increased glomerular
pressure, and BM thickening.
End stage Complications of Uncontrolled Diabetes
-
7/31/2019 Antidiabetic Buccal Dosage Form
4/21
-
7/31/2019 Antidiabetic Buccal Dosage Form
5/21
Sign and symptoms
In both types of diabetes, signs and symptoms are more likely to
be similar as the blood sugar
is high, either due to less or no production of insulin, or
insulin resistance. In any case, if
there is inadequate glucose in the cells, it is identifiable
through certain signs and symptoms.
These symptoms are quickly relieved once the Diabetes is treated
and also reduce the chances
of developing serious health problems .
DiabetesType1:
In type 1, the pancreas stop producing insulin due to autoimmune
response or possibly viral
attack on pancreas. In absence of insulin, body cells dont get
the required glucose forproducing ATP (Adenosin Triphosphate) units
which results into primary symptom in the
form of nausea and vomiting. In later stage, which leads to
ketoacidosis, the body starts
breaking down the muscle tissue and fat for producing energy
hence, causing fast weight loss.
Dehydration is also usually observed due to electrolyte
disturbance. In advanced stages, coma
and death is witnessed .
Diabetes Type 2:
Increased fatigue: Due to inefficiency of the cell to metabolize
glucose, reserve fat ofbody is metabolized to gain energy. When fat
is broken down in the body, it uses
more energy as compared to glucose, hence body goes in negative
calorie effect,
which results in fatigue.
Polydipsia: As the concentration of glucose increases in the
blood, brain receivessignal for diluting it and, in its
counteraction we feel thirsty.
http://diabetesinformationhub.com/SymptomsofDiabetes.phphttp://diabetesinformationhub.com/SymptomsofDiabetes.phphttp://diabetesinformationhub.com/SymptomsofDiabetes.phphttp://diabetesinformationhub.com/SymptomsofDiabetes.php
-
7/31/2019 Antidiabetic Buccal Dosage Form
6/21
Polyuria: Increase in urine production is due to excess glucose
present in body. Bodygets rid of the extra sugar in the blood by
excreting it through urine. This leads to
dehydration because along with the sugar, a large amount of
water is excreted out of
the body.
Polyphagia : The hormone insulin is also responsible for
stimulating hunger. In orderto cope up with high sugar levels in
blood, body produces insulin which leads to
increased hunger.
Blurry vision: Hyperosmolar hyperglycemia nonketotic syndrome is
the conditionwhen body fluid is pulled out of tissues including
lenses of the eye, which affects its
ability to focus, resulting blurry vision.
Poor wound healing : High blood sugar resists the flourishing of
WBC, (white bloodcell) which are responsible for body immune
system. When these cells do not function
accordingly, wound healing is not at good pace. Secondly, long
standing diabetes
leads to thickening of blood vessels which affect proper
circulation of blood in
different body parts.[8]
Treatment
The major goal in treating diabetes is to minimize any elevation
of blood sugar (glucose)without causing abnormally low levels of
blood sugar. Type 1 diabetes is treated with insulin,
exercise, and a diabetic diet. Type 2 diabetes is treated first
with weight reduction, a diabetic
diet, and exercise. When these measures fail to control the
elevated blood sugars, oral
medications are used. If oral medications are still
insufficient, treatment with insulin is
considered. Adherence to a diabetic diet is an important aspect
of controlling elevated blood
sugar in patients with diabetes.Weight reduction and exercise
increase the body's sensitivity
to insulin, thus helping to control blood sugar elevations.
Testosterone replacement therapy may improve glucose tolerance
and insulin sensitivity in
diabetic hypogonadal men. The mechanisms by which testosterone
decreases insulin
resistance is under study. Moreover testosterone may have a
protective effect on pancreatic
beta cells, which is possibly exerted by
androgen-receptor-mediated mechanisms and
influence of inflammatory cytokines. Recentlyit has been
suggested that a type ofgastric
bypass surgery may normalize blood glucose levels in 80-100% of
severely obese patients
with diabetes.. This approach may become a treatment for some
people with type 2 diabetes,
but has not yet been studied in prospective clinical
trials.[94]
This surgery may have the
http://www.medicinenet.com/script/main/art.asp?articlekey=47883http://en.wikipedia.org/wiki/Testosterone_replacement_therapyhttp://en.wikipedia.org/wiki/Testosteronehttp://en.wikipedia.org/wiki/Insulin_resistancehttp://en.wikipedia.org/wiki/Insulin_resistancehttp://en.wikipedia.org/wiki/Gastric_bypass_surgeryhttp://en.wikipedia.org/wiki/Gastric_bypass_surgeryhttp://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid12409659-93http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid12409659-93http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid12409659-93http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid12409659-93http://en.wikipedia.org/wiki/Gastric_bypass_surgeryhttp://en.wikipedia.org/wiki/Gastric_bypass_surgeryhttp://en.wikipedia.org/wiki/Insulin_resistancehttp://en.wikipedia.org/wiki/Insulin_resistancehttp://en.wikipedia.org/wiki/Testosteronehttp://en.wikipedia.org/wiki/Testosterone_replacement_therapyhttp://www.medicinenet.com/script/main/art.asp?articlekey=47883
-
7/31/2019 Antidiabetic Buccal Dosage Form
7/21
additional benefit of reducing the death rate from all causes by
up to 40% in severely obese
people.[95]
A small number of normal to moderately obese patients with type
2 diabetes have
successfully undergone similar operations.
MODY is another classification of diabetes and it can be treated
by early lifesyle
management and medical management. it has to be treated in the
early stage, so as to provide
a good health.[9]
1.2 Mucoadhesive Buccal Drug Delivery
Buccal drug delivery is a promising area for continued research
and attractive alternative for
non-invasive delivery of potent peptide and protein drug
molecules. Buccal administration of
drugs provides a convenient route of administration for both
systemic and local drug actions.
The need for safe and effective buccal permeation absorption
enhancers is a crucial
component for a prospective future in the area of buccal drug
delivery. Buccal nitroglycerin,
can use for acute therapy for an animal attack as well as for
chronic prophylaxis Novel liquid
aerosol formulation of insulin Development of suitable delivery
devices, permeation
enhancement, and Buccal delivery of drugs that undergo a
first-pass effect, such as
cardiovascular drugs, analgesics, and peptides Research yield
some successes Promote
further research; more companies Rest depend on delivery
technology.[10]
Buccal Route of Drug Absorption
There are two permeation pathways for passive drug transport
across the oral mucosa:
paracellular and transcellular routes. Permeants can use these
two routes simultaneously, but
one route is usually preferred over the other depending on the
physicochemical properties of
the diffusant. Since the intercellular spaces and cytoplasm are
hydrophilic in character,
lipophilic compounds would have low solubility in this
environment. The cell membrane,
however, is rather lipophilic in nature and hydrophilic solutes
will have difficulty permeating
through the cell membrane due to a low partition coefficient.
Therefore, the intercellular
spaces pose as the major barrier to permeation of lipophilic
compounds and the cell
membrane acts as the major transport barrier for hydrophilic
compounds. Since the oral
epithelium is stratified, solute permeation may involve a
combination of these two routes.
The route that predominates, however, is generally the one that
provides the least amount of
hindrance to passage.
http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid17715409-94http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid17715409-94http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid17715409-94http://en.wikipedia.org/wiki/Diabetes_management#cite_note-pmid17715409-94
-
7/31/2019 Antidiabetic Buccal Dosage Form
8/21
Buccal mucosa as a site for Drug Delivery
There are three different categories of drug delivery within the
oral cavity (i.e.,
Sublingual, buccal, and local drug delivery). Selecting one over
another is mainly based on
anatomical and permeability differences that exist among the
various oral mucosal sites. The
sublingual mucosa is relatively permeable, giving rapid
absorption and acceptable
bioavailability of many drugs, and is convenient, accessible,
and generally well accepted .The
sublingual route is by far the most widely studied of these
routes. Sublingual dosage forms
are of two different designs, those composed of rapidly
disintegrating tablets, and those
consisting of soft gelatin capsules filled with liquid drug.
Such systems create a very high
drug concentration in the sublingual region before they are
systemically absorbed across the
mucosa. Local delivery to tissues of the oral cavity has a
number of applications, including
the treatment of toothaches, periodontal disease, bacterial and
fungal infections, and dental
stomatitis, and in facilitating tooth movement with
prostaglandins. First difference being in
the permeability characteristics of the region, where the buccal
mucosa is less permeable and
is thus not able to give a rapid onset of absorption (i.e., more
suitable for a sustained release
formulation). Second being that, the buccal mucosa has an
expanse of smooth muscle andrelatively immobile mucosa which makes
it a more desirable region for retentive systems
used for oral transmucosal drug delivery. Thus the buccal mucosa
is more fitted for sustained
delivery applications, delivery of less permeable molecules, and
perhaps peptide drugs.
1.3 Advantages of Mucosal Buccal Drug Delivery
1. Bypass of the gastrointestinal tract and hepatic portal
system, increasing the bioavailability
of orally administered drugs that otherwise undergo hepatic
first-pass metabolism. In addition
the drug is protected from degradation due to pH and digestive
enzymes of the middle
gastrointestinal tract
2. Improved patient compliance due to the elimination of
associated pain with injections;
administration of drugs in unconscious or incapacitated
patients; convenience of
administration as compared to injections or oral
medications.
3. Sustained drug delivery.
-
7/31/2019 Antidiabetic Buccal Dosage Form
9/21
4. A relatively rapid onset of action can be achieved relative
to the oral route, and the
formulation can be removed if therapy is required to be
discontinued.
5. Increased ease of drug administration.
6. Though less permeable than the sublingual area, the buccal
mucosa is well vascularized,
and drugs can be rapidly absorbed into the venous system
underneath the oral mucosa.
7. In comparison to TDDS, mucosal surfaces do not have a stratum
corneum. Thus, the major
barrier layer to transdermal drug delivery is not a factor in
transmucosal routes of
administration. Hence transmucosal systems exhibit a faster
initiation and decline of delivery
than do transdermal patches.
8. Transmucosal delivery occurs is less variable between
patients, resulting in lower
intersubject variability as compared to transdermal
patches.[11-14]
1.4 Limitations of Mucosal Buccal Drug Delivery
1. For local action the rapid elimination of drugs due to the
flushing action of saliva or the
ingestion of foods stuffs may lead to the requirement for
frequent dosing. Depending on
whether local or systemic action is required the challenges
faced while delivering drug via
buccal drug delivery can be enumerated as follows.
2. The non-uniform distribution of drugs within saliva on
release from a solid or semisolid
delivery system could mean that some areas of the oral cavity
may not receive effective
levels.
3. For both local and systemic action, patient acceptability in
terms of taste, irritancy and
mouth feel is an issue.[11-14]
-
7/31/2019 Antidiabetic Buccal Dosage Form
10/21
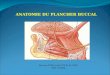
1.5 Overview of the Oral Mucosa
Structure
The oral mucosa is composed of outermost layer of stratified
epithelium.Below lies a
basement membrane, a lamina prairie followed by the submucosa as
the innermost layer. The
epithelium is similar to stratified squamous epithelia found in
the rest of the body in that it
has a mitotically active basal cell layer, advancing through a
number of differentiating
intermediate layers to the superficial layers, where cells are
shed from the surface of the
epithelium18. The epithelium of the buccal mucosa is about 40-50
cell layers thick, while that
of the sublingual epithelium contains somewhat fewer. The
epithelial cells increase in size
and become flatter as they travel from the basal layers to the
superficial layers. The turnover
time for the buccal epithelium.It has been estimated at 5-6
days, and this is probably
representative of the oral mucosa as a whole. The oral mucosal
thickness varies depending on
the site: the buccal mucosa measures at 500-800 m, while the
mucosal thickness of the hard
and soft palates, the floor of the mouth, the ventral tongue,
and the gingival measure at about
100-200 m.[15]
Fig 1.2. Section of buccal mucosal layer
-
7/31/2019 Antidiabetic Buccal Dosage Form
11/21
Permeability
The oral mucosa in general is a somewhat leaky epithelial
intermediate between that of the
epidermis and intestinal mucosa. It is estimated that the
permeability of the buccal mucosa is
4-4000 times greater than that of the skin . As indicative by
the wide range in this reported
value, there are considerable differences in permeability
between different regions of the oral
cavity because of the diverse structures and functions of the
different oral mucosae. In
general, the permeabilities of the oral mucosae decrease in the
order of sublingual greaterthan
buccal, and buccal greater than palatal. This rank order is
based on the relative thickness and
degree of keratinization of these tissues, with the sublingual
mucosa being relatively thin and
non-keratinized, the buccal thicker and non-keratinized, and the
palatal intermediate in
thickness but keratinized. The MCGs of keratinized epithelium
are composed of lamellar
lipid stacks, whereas the non-keratinized epithelium contains
MCGs that are non-lamellar.
The MCG lipids of keratinized epithelia include sphingomyelin,
glucosylceramides,
ceramides, and other nonpolar lipids, however for
non-keratinized epithelia, the major MCG
lipid components are cholesterol esters, cholesterol, and
glycosphingolipids Aside from the
MCGs, the basement membrane may present some resistance to
permeation as well,however
the outer epithelium is still considered to be the rate limiting
step to mucosal penetration. The
structure of the basement membrane is not dense enough to
exclude even relatively large
molecules.[16]
Environment
The cells of the oral epithelia are surrounded by an
intercellular ground substance, mucus, theprinciple components of
which are complexes made up of proteins and carbohydrates.
These
complexes may be free of association or some maybe attached to
certain regions on the cell
surfaces. This matrix may actually play a role in cell-cell
adhesion, as well as acting as a
lubricant, allowing cells to move relative to one another. Along
the same lines, the mucus is
also believed to play a role in bio adhesion of mucoadhesive
drug delivery systems. In
stratified squamous epithelia found elsewhere in the body, mucus
is synthesized by
specialized mucus secreting cells like the goblet cells, however
in the oral mucosa, mucus is
secreted by the major and minor salivary glands as part of
saliva . Up to 70% of the total
-
7/31/2019 Antidiabetic Buccal Dosage Form
12/21
mucin found in saliva is contributed by the minor salivary
glands . At physiological pH the
mucus network carries a negative charge (due to the sialic acid
and sulfate residues) which
may play a role inmucoadhesion. At this pH mucus can form a
strongly cohesive gel structure
that will bind to the epithelial cell surface as a gelatinous
layer.
1.6 Mechanism of Mucoadhesion
The mechanism of adhesion of certain macromolecules to the
surface of a mucous tissue is
not well understood yet. The mucoadhesive must spread over the
substrate to initiate close
contact and increase surface contact, promoting the diffusion of
its chains within the mucus.
Attraction and repulsion forces arise and, for a mucoadhesive to
be successful, the attraction
forces must dominate. Each step can be facilitated by the nature
of the dosage form and how
it is administered. For example, a partially hydrated polymer
can be adsorbed by the substrate
because of the attraction by the surface water. Thus, the
mechanism of mucoadhesion is
generally divided in two steps, the contact stage and the
consolidation stage (Figure1.3). The
first stage is characterized by Mucoadhesive drug delivery
systems 3 the contact between the
mucoadhesive and the mucous membrane, with spreading and
swelling of the formulation,
initiating its deep contact with the mucus layer .In some cases,
such as for ocular or vaginal
formulations, the delivery system is mechanically attached over
the membrane. In other
cases, the deposition is promoted by the aerodynamics of the
organ to which the system is
administered, such as for the nasal route. On the other hand, in
the gastrointestinal tract direct
formulation attachment over the mucous membrane is not feasible.
Peristaltic motions can
contribute to this contact, but there is little evidence in the
literature showing appropriate
adhesion. Additionally, an undesirable adhesion in the esophagus
can occur. In these cases,
mucoadhesion can be explained by peristalsis, the motion of
organic fluids in the organ
cavity, or by Brownian motion. If the particle approaches the
mucous surface, it will come
into contact with repulsive forces (osmotic pressure,
electrostatic repulsion, etc.) and
attractive forces (van der Waals forces and electrostatic
attraction). Therefore, the particle
must overcome this repulsive barrier. In the consolidation step
(Figure 1.3), the
mucoadhesive materials are activated by the presence of
moisture. Moisture plasticizes the
system, allowing the mucoadhesive molecules to break free and to
link up by weak van der
Waals and hydrogen bonds. Essentially, there are two theories
explaining the consolidation
step: the diffusion theory and the dehydration theory. According
to diffusion theory, the
mucoadhesive molecules and the glycoproteins of the mucus
mutually interact by means of
-
7/31/2019 Antidiabetic Buccal Dosage Form
13/21
interpenetration of their chains and the building of secondary
bonds .For this to take place the
mucoadhesive device has features favoring both chemical and
mechanical interactions. For
example, molecules with hydrogen bonds building groups (OH,
COOH), with an anionic
surface charge, high molecular weight, flexible chains and
surface-active properties, which
induct its spread throughout the mucus layer, can present
mucoadhesive properties.[17]
Fig 1.3 The two steps of mucoadhesive process
1.7 Mucoadhesive Theories
There are six classical theories adapted from studies on the
performance of several materials
and polymer-polymer adhesion which explain the phenomenon
Electronic theory
Electronic theory is based on the fact that both mucoadhesive
and biological materials
possess opposing electrical charges. Thus, when both materials
come into contact, they
transfer electrons leading to the building of a double
electronic layer at the interface, where
the attractive forces within this electronic double layer
determines the mucoadhesive strength.
Adsorption theory
According to the adsorption theory, the mucoadhesive device
adheres to the mucus by
secondary chemical interactions, such as in van der Waals and
hydrogen bonds, electrostatic
-
7/31/2019 Antidiabetic Buccal Dosage Form
14/21
attraction or hydrophobic interactions For example, hydrogen
bonds are the prevalent
interfacial forces in polymers containing carboxyl groups .Such
forces have been considered
the most important in the adhesive interaction phenomenon
because, although they are
individually weak, a great number of interactions can result in
an intense global adhesion
Wetting theory
The wetting theory applies to liquid systems which present
affinity to the surface in order to
spread over it. This affinity can be found by using measuring
techniques such as the contact
angle. The general rule states that the lower the contact angle
then the greater the affinity
(Figure 1.3). The contact angle should be equal or close to zero
to provide adequate spread
ability
Fig. 1.4 .Schematic diagram showing influence of contact angle
between device and
mucous membrane
Fracture theory
This is perhaps the most-used theory in studies on the
mechanical measurement of
mucoadhesion. It analyses the force required to separate two
surfaces after adhesion is
established
-
7/31/2019 Antidiabetic Buccal Dosage Form
15/21
Mechanical theory
Mechanical theory considers adhesion to be due to the filling of
the irregularities on a rough
surface by a mucoadhesive liquid. Moreover, such roughness
increases the interfacial area
available to interactions thereby aiding dissipating energy and
can be considered the most
important phenomenon of the process. It is unlikely that the
mucoadhesion process is the
same for all cases and therefore it cannot be described by
single theory. The mechanisms
governing mucoadhesion are also determined by the intrinsic
properties of the formulation
and by the environment in which it is applied. Intrinsic factors
of the polymer are related to
its molecular weight, concentration and chain flexibility. For
linear polymers, mucoadhesion
increases with molecular weight, but the same relationship does
not hold for nonlinear
polymers.[18]
1. 8 Factors Affecting Drug Delivery via Buccal Route
The rate of absorption of hydrophilic compounds is a function of
the molecular size. Smaller
molecules (75-100 Da) generally exhibit rapid transport across
the mucosa, with permeability
decreasing as molecular size increases. For hydrophilic
macromolecules such as peptides,
absorption enhancers have been used to successfully alter the
permeability of the buccal
epithelium, causing this route to be more suitable for the
delivery of larger molecules
1. 9 Methods to Increase Drug Delivery via Buccal Route
(1) Absorption enhancers:
Absorption enhancers have demonstrated their effectiveness in
delivering high molecular
weight compounds, such as peptides, that generally exhibit low
buccal absorption rates.[19]
-
7/31/2019 Antidiabetic Buccal Dosage Form
16/21
Table 1.1: List of Permeation Enhancers
Sr. no Permeation Enhancers Sr. no Permeation Enhancers
1 2,3-Lauryl ether 9 Phosphatidylcholine
2 Aprotinin 10 Polyoxyethylene
3 Azone 11 Polysorbate 80
4 Benzalkonium chloride 12 Polyoxyethylene
5 Cetylpyridinium chloride 13 Phosphatidylcholine
6 Cetyltrimethyl ammonium bromide 14 Sodium EDTA
7 Cyclodextrin 15 Sodium glycoholate
8 Dextran sulfate 16 Sodium glycodeoxycholate
(2) Prodrugs:
Hussein et al delivered opioid agonists and antagonists in
bitterness prodrug forms and found
that the drug exhibited low bioavailability as prodrug.
Nalbuphine and naloxone bitter drugs
when administered to dogs via the buccal mucosa, the caused
excess salivation and
swallowing. As a result, the drug exhibited low
bioavailability.[20]
(3) pH :
Shojaei et al evaluated permeability of acyclovir at pH ranges
of 3.3 to 8.8, and in the
presence of the absorption enhancer, sodium glycocholate. The in
vitro permeability of
acyclovir was found to be pH dependent with an increase in flux
and permeability coefficient
at both pH extremes (pH 3.3 and 8.8), as compared to the
mid-range values (pH 4.1, 5.8, and
7.0).
-
7/31/2019 Antidiabetic Buccal Dosage Form
17/21
(4) Patch design:
Several in vitro studies have been conducted regarding on the
type and amount of backing
materials and the drug release profile and it showed that both
are interrelated.
Also, the drug release pattern was different between
single-layered and multi-layered patches.
1.4 Classifications of buccal bioadhesive dosage forms
1. Buccal Bioadhesive Tablets.
2. Buccal Bioadhesive semisolids
3. Buccal Bioadhesive patch and films
4. Buccal Bioadhesive Powders
1. Buccal bioadhesive tablets
Buccal bioadhesive tablets are dry dosage forms that are to be
moistened prior to placing in
contact with buccal mucosa. Double and multilayered tablets are
already formulated using
bioadhesive polymers and excipients. The two buccal bioadhesive
tablets commercially
available buccoadhcsive tablets in UK are "Bucastem" and Suscard
buccaP'.
2. Buccal bioadhesivc semisolid dosage forms
Buccal bioadhesive semisolid dosage forms consists of finally
powdered natural or synthetic
polymer dispersed in a polyethylene or in aqueous solution,
Example: Arabase.21
3. Buccal bioadhesive patches and films
Buccal bioadhesive patches consists of two ply laminates or
multilayered thin film round or
oval as consisting of basically of bioadhesive polymeric layer
and impermeable backing layer
to provide unidirectional flow of drug across buccal mucosa.
Buccal bioadhesive films arc
formulated by incorporating the drug in alcohol solution of
bioadhesive polymer.
-
7/31/2019 Antidiabetic Buccal Dosage Form
18/21
4.Buccal bioadhesive powder dosage forms
Buccal bioadhesive powder dosage forms are a mixture of
Bioadhesive polymers and the
drug and are sprayed onto the buccal mucosa the reduction in
diastolic B.P after the
administration of buccal tablet and buccal film of
Nifedipine.
1.10 Basic Components of Buccal Bioadhesive Drug Delivery
The basic components of buccal bioadhesive drug delivery system
are
1. Drug substance2. Bioadhesive polymers3. Backing membrane4.
Penetration enhancers5. Adhesives
1. Drug substance:
Before formulating buccoadhcsive drug delivery systems, one has
to decide whether the
intended, action is for rapid release/prolonged release and for
local/systemic effect The drug
should have following characteristics.[21]
1. The conventional single dose of the drug should be small.
The drugs having biological half-life between 2-8 hours are good
candidates for controlled
drug delivery.
2. Tmax of the drug shows wider-fluctuations or higher values
when given orally.30
3. The drug absorption should be passive when given orally.
2. Bioadhesive polymers:
The first step in the development of buccoadhcsive dosage forms
is the selection and
characterization of appropriate bioadhesive polymers in the
formulation." Bioadhesive
polymers play a major role in buccoadhcsive drug delivery
systems of drugs. Polymers arc
also used in matrix devices in which the drug is embedded in the
polymer matrix, which
controls the duration of release of drugs
An ideal polymer for buccoadhcsive drug delivery systems should
have following
Characteristics:
-
7/31/2019 Antidiabetic Buccal Dosage Form
19/21
It should be inert and compatible with the environment The
polymer and its degradation products should be non-toxic absorbable
from the
Mucous layer.
It should adhere quickly to moist tissue surface and should
possess some sitespecificity.
The polymer must not decompose on storage or during the shelf
life of the dosageform.
The polymer should be easily available in the market and
economical.3. Backing membrane: Backing membrane plays a major role
in the attachment of
bioadhesive devices to the mucus membrane. The materials used as
backing membrane
should be inert, and impermeable to the drug and penetration
enhancer. The commonly used
materials in backing membrane include carbopol, magnesium
separate, HPMC, HPC, CMC,
polycarbophil etc.
4. Penetration enhancers: Penetration enhancers arc used in
buccoadhcsive formulations to
improve the release of the drug. They aid in the systemic
delivery of the drug by allowing the
drug to penetrate more readily into the viable tissues.
5. Bioadhesion: Bioadhesive are the substances that are capable
of interacting with the
biological material and being retained on them or holding them
together for extended periodof time.Bioadhesive can be used to
apply to any mucous or no mucous membranes and it also
increases intimacy and duration of contact of the drug with the
absorbing membrane. The
commonly used bioadhesive are sodium alginate, carbomers,
polycarbophil, HPMC, HPC,
gelatin etc.
-
7/31/2019 Antidiabetic Buccal Dosage Form
20/21
1.11 LIST OF DRUGS DELIVERED VIA BUCCAL ROUTE.
Table 1.2: List of drugs delivered via buccal route
Sr.No Active Ingredients
1 Acitretin
2 Acyclovir
3 Arecoline
4 Buprenorpine
5 Carbamazepine
6 Cetyl Pyridium Chloride
7 Chitosan
8 Chlorpheniramine Maleate
9 Cyanocobalamine
10 Danazol
11 Denbufylline
12 Diclofenac Sodium
13 Diltiazem Hydrochloride
14 Ergotamine Tartrate
15 Fluride
16 Metronidazole
17 Melatonin
18 Metoprolol
19 Morphine Sulphate
20 Nalbuphine
21 Nicotine
22 Nifedipine
23 Omeprazole
24 Oxytocin
25 Pindolol
-
7/31/2019 Antidiabetic Buccal Dosage Form
21/21
26 Propolis
1.12 Mucoadhesive Buccal Tablet
Mucoadhesive Buccal tablets comprising hydrogels can adhere to
the buccal mucosa. They
are similar to conventional tablets and are prepared by wet
granulation, dry granulation, or
direct compression processes. Drug is released upon the
hydration and adhesion of the
device. Buccal tablets should be fabricated and optimized for
swelling behavior and drug
release to ensure a prolonged period of bioadhesion and
sustained or controlled release.
Generally, the tablets are formulated with flat punches with
dimensions less than 10 mm in
diameter and 2 mm thick to aid in establishing intimate contact
with buccal mucosa and
reduce their interference with normal activities. In addition to
mucoadhesive components,
most of the tablets contained water-soluble excipients such as
high-molecular-weight
polyethylene glycols and mannitol.[22-24]



![Cronicon OPEN ACCESS PHARMACEUTICAL SCIENCE Research … · 2015-08-27 · interest in the development of novel mucoadhesive buccal dosage forms [6,7]. The buccal mucosa has been](https://img.pdfslide.net/doc/110x75/5e9b13a0512fa35fd3520480/cronicon-open-access-pharmaceutical-science-research-2015-08-27-interest-in-the.jpg)