Embed Size (px)
Citation preview

The different stories:a historical perspective
Georges M. Halpern, MD, PhDDistinguished Professor of Pharmaceutical Sciences
Hong Kong Polytechnic University
Are all Antihistamines the same ?

General History of Antihistamines
1910 Histamine discovered
1937 First antihistamines (AHs) synthesized
1942 Antihistamines introduced for clinical use
1943 First CNS effects of AHs reported
1955 Antiallergic effects of AHs described
1981 2nd generation AHs introduced
1986 Cardiotoxic effects of AHs reported
1991 Human H2 receptor cloned
1993 Human H1 receptor cloned
1998 H1 receptor polymorphism described
1999 Human H3 receptor cloned
2000 Human H4 receptor cloned
Modified from Simons FER. Antihistamines, Chapter 51, in Middleton's Allergy: Principles and Practice, Mosby, 6th Edition, 2003

1910-1911: Discovery of Histamine
Henry Dale and Patrick Laidlaw identified and described the properties of histamine (from: histos = tissue, with an amine constituent).

1937: First Animal Studies
Etienne Fourneau synthesized the 1st AH (thymo-ethyl-diethylamine); Daniel Bovet, assisted by Anne-Marie Staub studied it.
It was found to be too weakly active, and too toxic for clinical use.
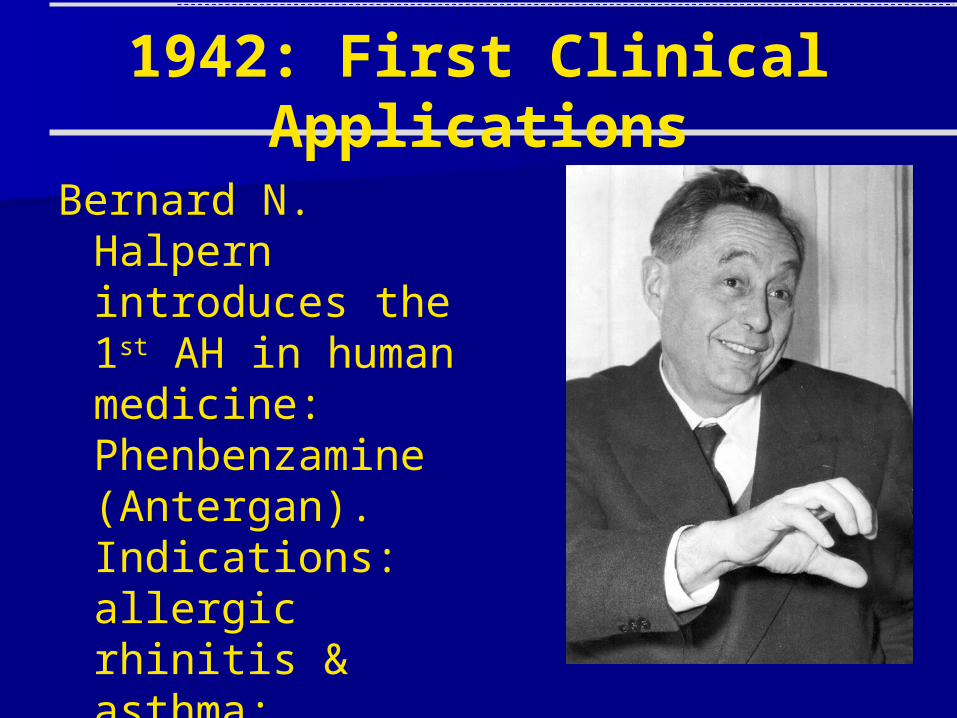
1942: First Clinical Applications
Bernard N. Halpern introduces the 1st AH in human medicine: Phenbenzamine (Antergan). Indications: allergic rhinitis & asthma; urticaria; blood conservation.

Next Steps Marked by intensive and diversified research
leading to notable differences between commercially available antihistamines – different synthesis pathways, hence different classes– different chemical structures– different indications/uses in various diseases– different development objectives– different generations– different safety features– different antihistamine performance and efficacy
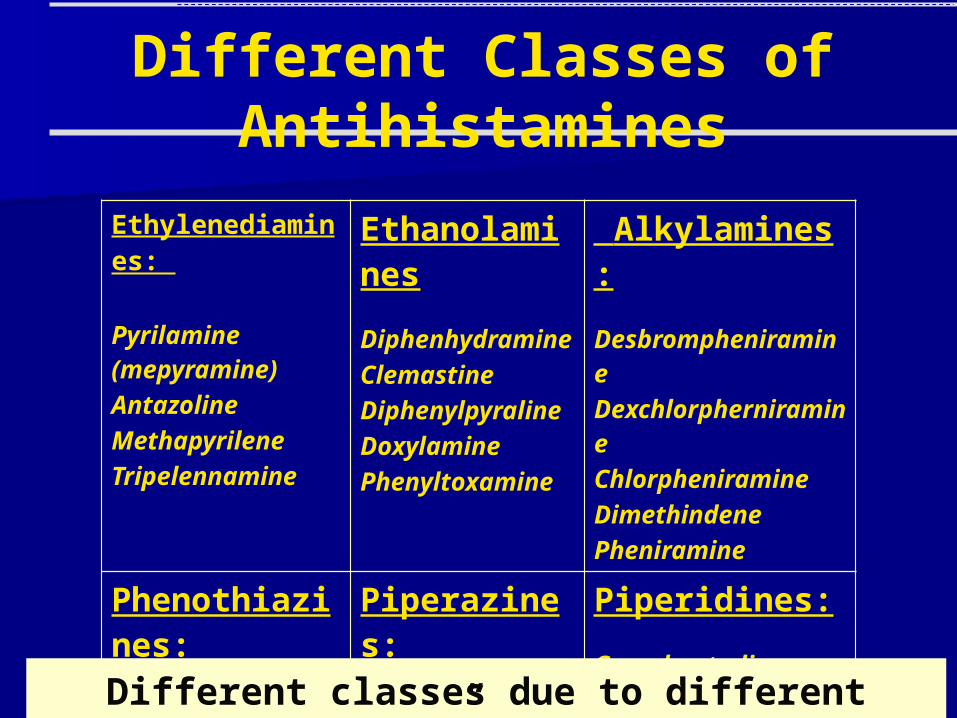
Different Classes of Antihistamines
Ethylenediamines:
Pyrilamine (mepyramine) Antazoline Methapyrilene Tripelennamine
Ethanolamines
Diphenhydramine Clemastine Diphenylpyraline Doxylamine Phenyltoxamine
Alkylamines:
Desbrompheniramine Dexchlorpherniramine Chlorpheniramine Dimethindene Pheniramine
Phenothiazines:
Promethazine Methdilazine Trimeprazine
Piperazines:
Cyclizine Buclizine Hydroxyzine Meclizine
Piperidines:
Cyproheptadine Azatadine Loratadine
Different classes due to different “mother” molecules

Different Chemical Structures

Different Applications of Antihistamines Allergy:
– 1st & 2nd generation H1-antihistamines (chlorpheniramine, diphenylhydramine, hydroxyzine, astemizole, terfenadine, cetirizine, fexofenadine, loratadine, desloratadine, levocetirizine)
Anti-Migraine: – cyproheptadine, ergotamine + diphenydramine,
pizotifen Cough, Cold and Pain relief:
– diphenhydramine, doxylamine

Different Applications of Antihistamines
Motion Sickness: – dimenhydrinate, hydroxyzine, promethazine
theoclate Sedatives:
– doxylamine succinate, diphenhydramine, pyrilamine, promethazine hydrochloride, mepyramine maleate, trimeprazine
Different uses due to different properties and different development objectives

PK, lower drug-drug interactions
Receptor affinity and selectivity,
efficacySafety, lower cardiotoxicity
Different Development Objectives General trend: improve tolerability and safety (less to
no sedation; reduce the cholinergic effects)
Targeted Molecules for improvement
Type of Improvement
Loratadine
Hydroxyzine
Terfenadine
Astemizole
ObjectiveClass
Piperidine
Piperazine
Piperidine
Piperidine
Isomer Purification
Levocetirizine
Active metabolite
Desloratadine
Cetirizine
FexofenadineNo possible improvement
not even designed as an antihistamine; discovered during research of calcium channel-blocking agents

Different Generation of Antihistamines
Antergan and Neo-Antergan
1st Generation:pyrilamine, antazoline, tripelennamine, diphenhydramine, clemastine, chlorpheniramine, triprolidine, promethazine,
mequitazine, hydroxyzine, cyclizine, azatadine, cyproheptadine
2nd Generation:terfenadine, astemizole, cetirizine, acrivastine, ebastine,
levocabastine, loratadine, mizolastine
New or 3rd Generation:levocetirizine, carebastine, desloratadine, fexofenadine

Different Safety Profiles
0
0.2
0.4
0.6
0.8
1
1.2
1.4N
um
be
r o
f v
iab
le c
ells
(a
bs
orb
an
ce
)
withdrawn from the market due to cardiotoxicity
A set of AHs tested for toxicity (inhibition of cellular proliferation) by the MTS assay (Sussman NL et al. Cell Notes, Issue 3, 2002: 7-10). All drugs tested in quadruplicate at 80m and all assays performed at 72 hrs.
Still on the market

Different Destinies Some withdrawn from the market:
– astemizole, terfenadine Some failed to reach enough patients:
– ebastine, levocabastine Some quickly falling out of favour:
– loratadine Some are still going strong:
– fexofenadine, cetirizine, desloratadine, levocetirizine

Are all antihistamines the same ?
Apparently, they are NOT– Different synthesis pathways– Different development objectives– The uncertainty of whether a 3rd generation exists
or not is also related to the different development histories and product characteristics
The diverse pharmacology, efficacy and safety characteristics will be featured in
the presentations that follow mine