Embed Size (px)
Citation preview
Antimicrobial Resistance (AMR) Systems MapOverview of the factors influencing the development of AMR and the interactions between them
Departmentfor EnvironmentFood & Rural Affairs
Departmentof Health
Public HealthEngland
VeterinaryMedicinesDirectorate
December 2014
2 Antimicrobial Resistance (AMR) Systems Map
Description
Purpose
The aim of producing an antimicrobial resistance (AMR) systems map is to provide a broad overview of the factors influencing the development of antimicrobial resistance and the interactions between them rather than detailed consideration of individual factors or infectious agents. We hope this will increase awareness of the diverse factors that influence AMR, aid research groups in identifying issues for investigation and aid in policy development.
We recognise that the map would benefit from further development. By publishing our first iteration of this map we hope that others can suggest improvements and/or develop particular aspects in more detail, either independently or in collaboration with us.
Description
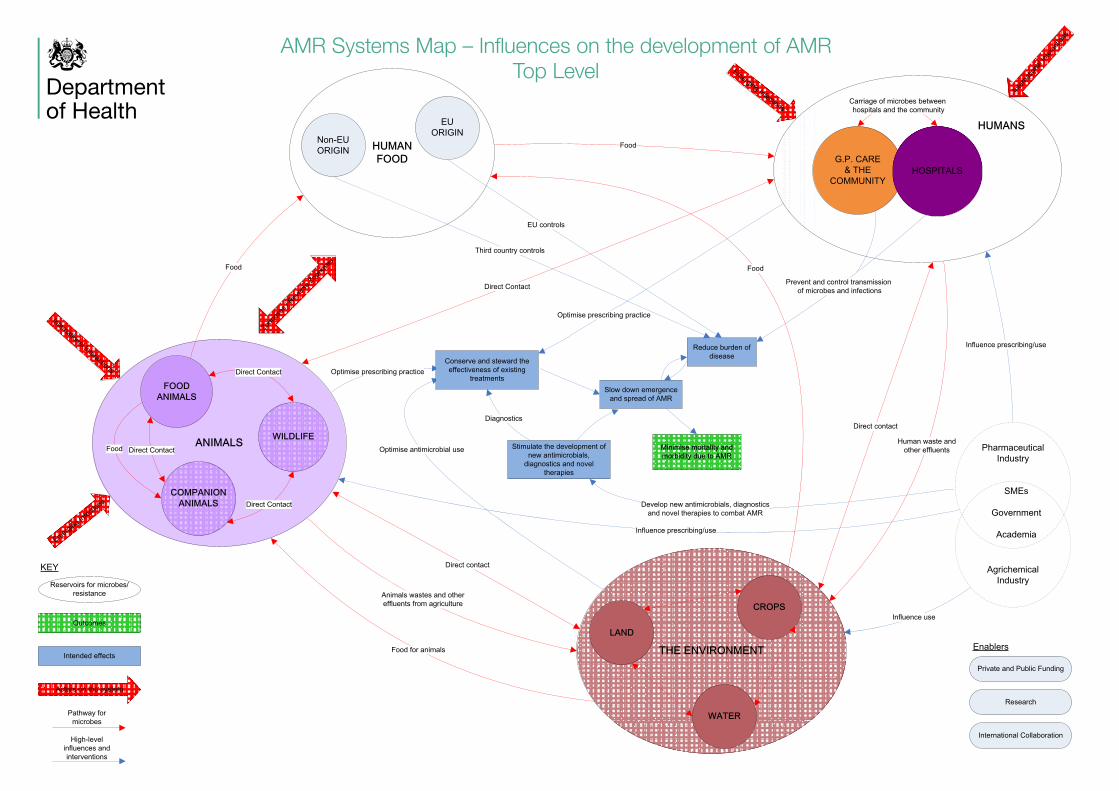
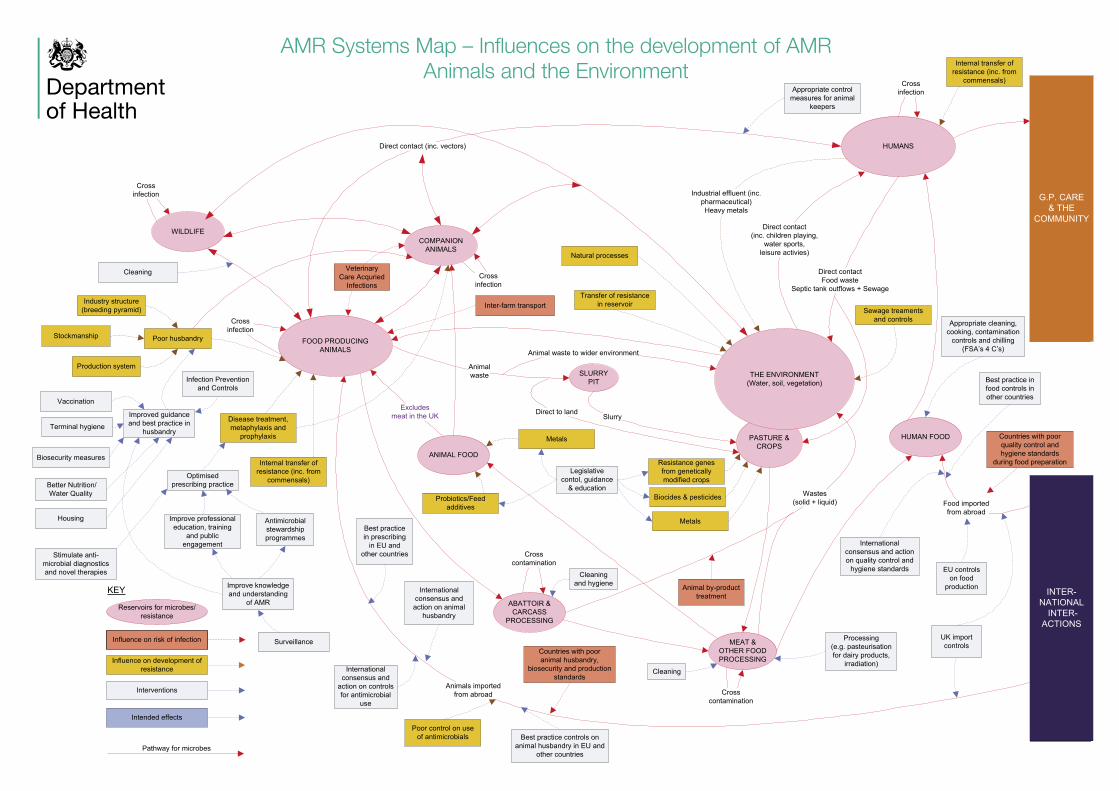
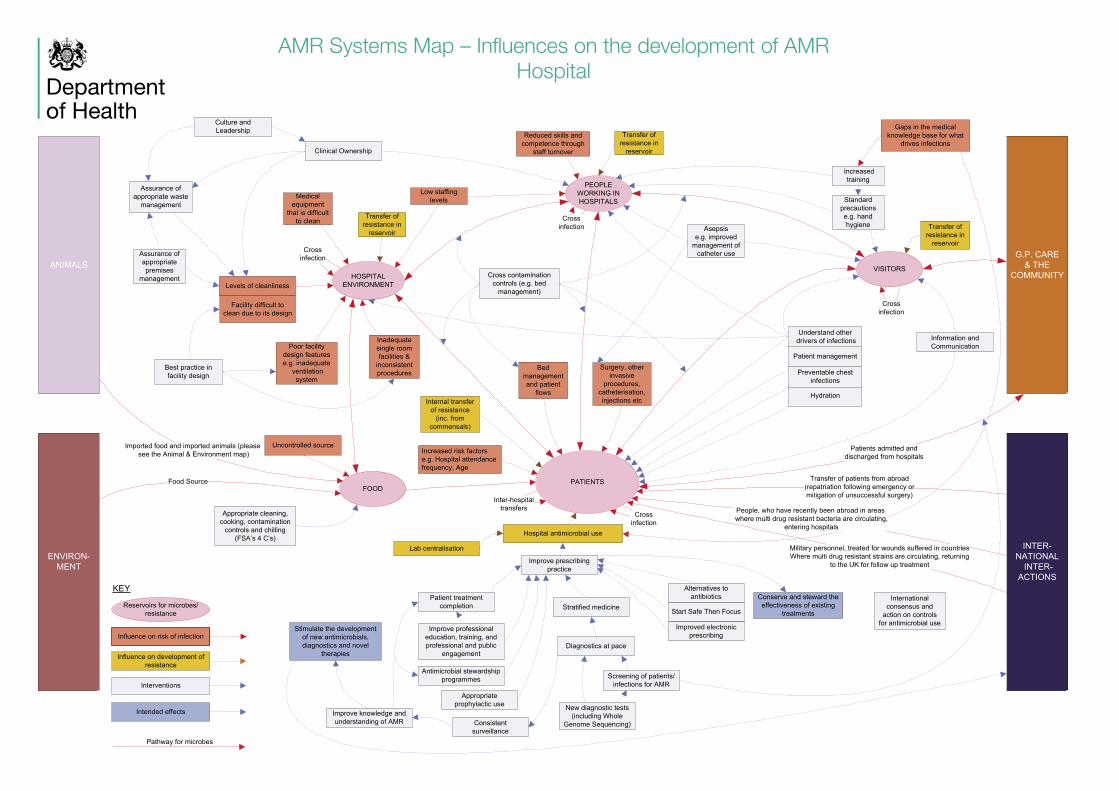
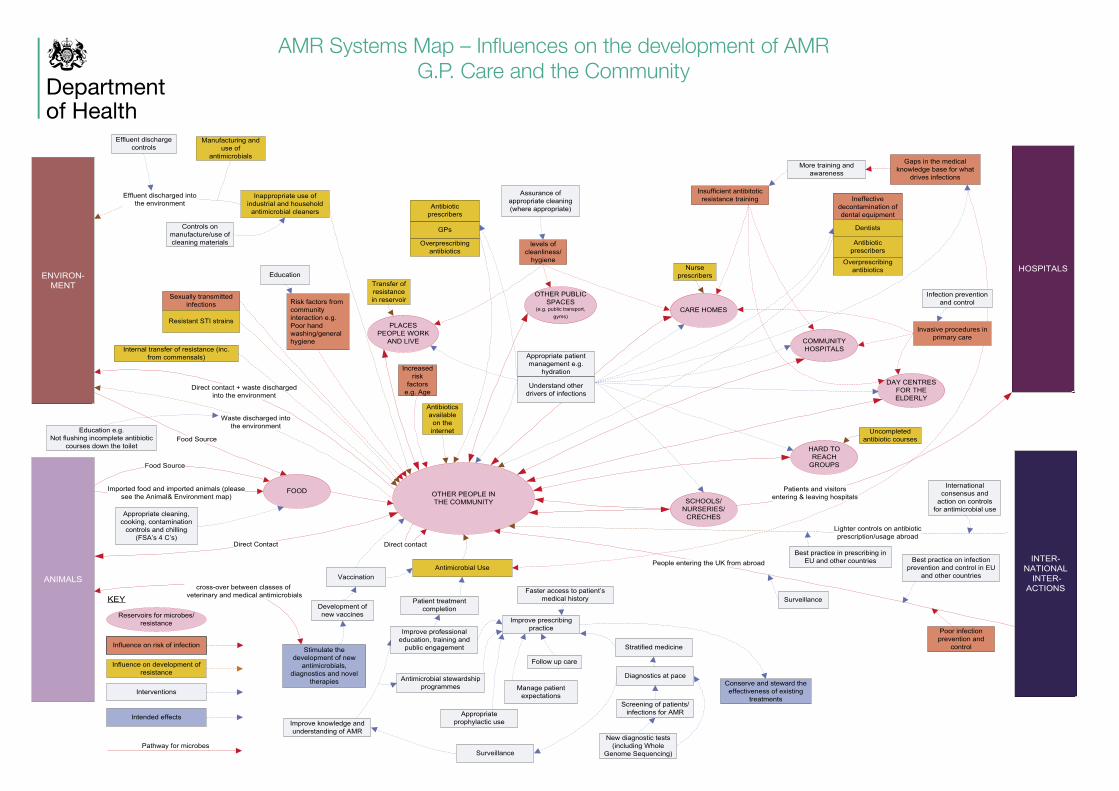
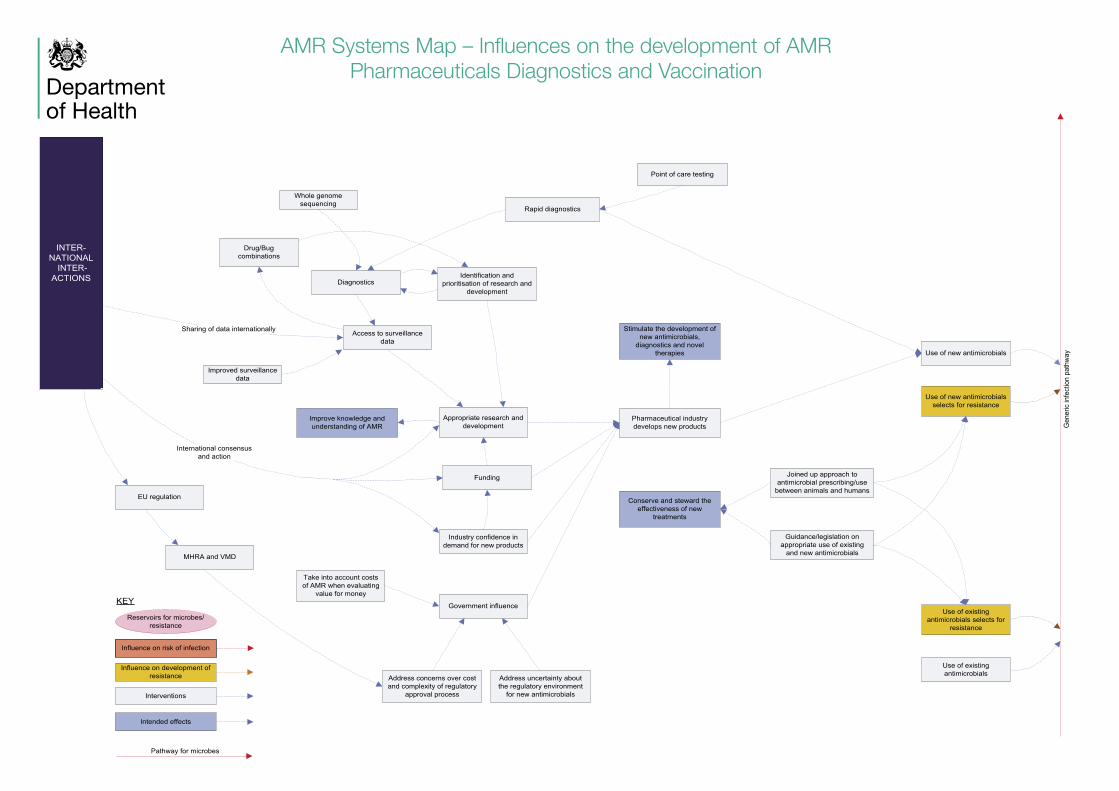
The systems map provides a visual representation of the various influences on the development of AMR and the interaction between them. The aim is to provide a qualitative insight into the issues around antimicrobial resistance from a United Kingdom perspective. This includes both understanding the pathways that spread infection and resistance that could cause increased mortality and morbidity and identifying interventions (e.g. antibiotic stewardship programmes, behaviour change, infection control measures, etc.) that may impact on these pathways. This has been done by identifying reservoirs of infection and the pathways that link these reservoirs. By reservoirs of infection we mean any person, animal, plant, soil, substance or place in which an infectious agent normally lives and multiplies. The reservoir may harbour the infectious agent without injury to itself and serves as a source from which other individuals can be infected.
Please note that the map adopts a generic approach; it does not represent pathways for a particular infectious agent. The particular pathways which are applicable will depend on the infectious agent. There is no attempt, at this stage, to identify the relative importance of different pathways or prioritise the interventions. Interventions will require investigation of their impact, associated risk:benefit, and cost effectiveness. The size of boxes in the map does not reflect scale or significance.
Structure of the map and sub maps
A top level map shows the high level pathways that infections may take between animals, the environment and humans. High level interventions and influences act on these pathways to have four key outcomes:
1. Reduce burden of disease2. Conserve and steward the effectiveness of existing outcomes3. Slow down the emergence and spread of AMR4. Stimulate the development of new antimicrobials, diagnostics and novel therapies
These in turn drive the ultimate desired outcome of minimising mortality and morbidity due to AMR which sits at the centre of the map.
Antimicrobial Resistance (AMR) Systems Map
AMR Systems Map – Influences on the development of AMR 3
From the top level map more detailed sub maps are layered. These more detailed sub maps cover:
1. Animals & Environment2. Hospital3. G.P. Care & the Community4. Pharmaceuticals, diagnostics and vaccinations
These seek to show the interventions and actions within each of these areas which can influence the key outcomes (these are the same as those shown in the Top Level map). Relevant links are also made between the different areas (e.g. the influence of transmission of infections between humans and animals) through the rectangular boxes on the side of each sub map. The elements within each of maps are:
1. Reservoirs for microbes/infection2. Influences on risk of infection3. Influences on development of resistance4. Interventions (that either impact the reservoirs or the influences)5. Outcomes.
Across all the maps, mentions are made of the potential international interactions that may influence the development of AMR.
Methodology
The systems mapping approach itself is described below. The map and sub maps were developed in a series of facilitated workshops through a process of first identifying the reservoirs, then the pathways linking them and finally the interventions. The maps were then constructed on Visio. Some individual contributions were received after the workshops and have been incorporated.
The Top Level map and the Animals & Environment sub map were developed in joint workshops involving participants from DEFRA, DH and Public Health England. The Hospital and the G.P. Care & the Community sub-maps were developed in a workshop of invited experts. A list of participants is at the end of this document.
Systems Mapping
Systems mapping is the process of conceptually representing a system (a set of elements and the relationships between them) and illustrating how events in one part of it affect other parts. Whole systems generally exhibit properties or behaviours that cannot be predicted from the properties of the individual parts.
A key purpose in building systems maps is to gain insight in the underlying structure of a messy, complex situation. A systems map shows how the elements interrelate and where there are opportunities to intervene in the modelled system to influence its behaviour. The essential contribution of systems maps is to summarise and communicate current trends, relationships and constraints that may influence the future behaviour of a system.
Systems mapping is a precursor to more detailed modelling. The map can be used to identify feedback effects, as a structure for the evidence base and in the longer term provide a basis for quantitative systems modelling.
Further Development
We intend to establish a panel to review and update the map on an (at least) annual basis. If you wish the panel to consider any additions or changes to the map please submit your suggestions to [email protected].
Departmentof Health
AMR Systems Map – Influences on the development of AMR Top Level
Departmentof Health
Pathway for microbes
KEY
Interventions
Influence on risk of infection
Influence on development of resistance
Reservoirs for microbes/resistance
Intended effects
FOOD PRODUCING ANIMALS
INTER-NATIONAL
INTER-ACTIONS
WILDLIFE
ANIMAL FOOD
COMPANION ANIMALS
HUMANS
HUMAN FOODPASTURE & CROPS
THE ENVIRONMENT(Water, soil, vegetation)
ABATTOIR & CARCASS
PROCESSING
MEAT & OTHER FOOD PROCESSING
SLURRY PIT
Animals importedfrom abroad
Food importedfrom abroad
Excludesmeat in the UK
Animal waste
Animal waste to wider environment
SlurryDirect to land
Direct contact(inc. children playing,
water sports,leisure activies)
Direct contactFood waste
Septic tank outflows + Sewage
Wastes(solid + liquid)
Appropriate cleaning, cooking, contamination
controls and chilling (FSA’s 4 C’s)
Metals
Internal transfer of resistance (inc. from
commensals)
Probiotics/Feed additives
Cleaning
Disease treatment, metaphylaxis and
prophylaxis
Resistance genes from genetically modified crops
Biocides & pesticides
Poor husbandry
Industry structure (breeding pyramid)
Production system
Vaccination
Terminal hygiene
Industrial effluent (inc.pharmaceutical)Heavy metals
Metals
Natural processes
Crosscontamination
Crosscontamination
Processing (e.g. pasteurisation for dairy products,
irradiation)Cleaning
Cleaning and hygiene
Crossinfection
Crossinfection
Crossinfection
Inter-farm transport
Veterinary Care Acquried
Infections
Appropriate control measures for animal
keepers
Legislative contol, guidance
& education
Optimised prescribing practice
G.P. CARE & THE
COMMUNITY
Surveillance
Antimicrobial stewardship programmes
Improve professional education, training
and public engagement
Improve knowledge and understanding
of AMR
Crossinfection
Improved guidance and best practice in
husbandry
Internal transfer of resistance (inc. from
commensals)
Transfer of resistance in reservoir
Countries with poor quality control and hygiene standards
during food preparation
UK import controls
Countries with poor animal husbandry,
biosecurity and production standards
Poor control on use of antimicrobials
International consensus and
action on controls for antimicrobial
use
International consensus and action on animal
husbandry
International consensus and action on quality control and
hygiene standards
Best practice in food controls in other countries
EU controls on food
production
Best practice in prescribing
in EU and other countries
Best practice controls on animal husbandry in EU and
other countries
Stockmanship
Infection Prevention and Controls
Biosecurity measures
Better Nutrition/Water Quality
Housing
Stimulate anti-microbial diagnostics and novel therapies
Sewage treaments and controls
Animal by-product treatment
Direct contact (inc. vectors)
AMR Systems Map – Influences on the development of AMR Animals and the Environment
Departmentof Health
Pathway for microbes
KEY
Interventions
Influence on risk of infection
Influence on development of resistance
Reservoirs for microbes/resistance
Intended effects
People, who have recently been abroad in areas where multi drug resistant bacteria are circulating,
entering hospitals
PATIENTS
HOSPITAL ENVIRONMENT
FOOD
G.P. CARE & THE
COMMUNITYVISITORSANIMALS
ENVIRON-MENT
Imported food and imported animals (please see the Animal & Environment map)
Food Source
Crossinfection
Transfer of resistance in
reservoir
Appropriate cleaning, cooking, contamination
controls and chilling (FSA’s 4 C’s)
Cross contamination controls (e.g. bed
management)
Stratified medicine
Diagnostics at pace
Screening of patients/ infections for AMR
New diagnostic tests (including Whole
Genome Sequencing)Consistent surveillance
Hospital antimicrobial use
Appropriate prophylactic use
Antimicrobial stewardship programmes
Improve professional education, training, and professional and public
engagement
Patient treatment completion
Levels of cleanliness
Surgery, other invasive
procedures, catheterisation, injections etc
Best practice in facility design
Improve knowledge and understanding of AMR
Crossinfection
Crossinfection
Transfer of resistance in
reservoir
Transfer of resistance in
reservoir
Standard precautions e.g. hand hygiene
INTER-NATIONAL
INTER-ACTIONS
Transfer of patients from abroad(repatriation following emergency or mitigation of unsuccessful surgery)
Inter-hospitaltransfers
Poor facility design features e.g. inadequate
ventilation system
Low staffing levels
Reduced skills and competence through
staff turnover
Increased training
Culture and Leadership
PEOPLE WORKING IN HOSPITALS
Crossinfection
Clinical Ownership
Information and Communication
Uncontrolled source
Assurance of appropriate premises
management
Gaps in the medical knowledge base for what
drives infections
Inadequate single room facilities &
inconsistent procedures
Asepsis e.g. improved
management of catheter use
Bed management and patient
flows
Start Safe Then Focus
Alternatives to antibiotics
Lab centralisation
Stimulate the development of new antimicrobials, diagnostics and novel
therapies
Improve prescribing practice
Improved electronic prescribing
Assurance of appropriate waste
management
Patients admitted and discharged from hospitals
Internal transfer of resistance
(inc. from commensals)
Understand other drivers of infections
Hydration
Patient management
Preventable chest infections
Medical equipment
that is difficult to clean
Facility difficult to clean due to its design
Increased risk factorse.g. Hospital attendance frequency, Age
Military personnel, treated for wounds suffered in countries Where multi drug resistant strains are circulating, returning
to the UK for follow up treatment
Conserve and steward the effectiveness of existing
treatments
International consensus and
action on controls for antimicrobial use
AMR Systems Map – Influences on the development of AMR Hospital
Departmentof Health
Pathway for microbes
KEY
Interventions
Influence on risk of infection
Influence on development of resistance
Reservoirs for microbes/resistance
Intended effects
OTHER PEOPLE IN THE COMMUNITY
FOOD
ANIMALS
ENVIRON-MENT
Food Source
Food Source
Appropriate cleaning, cooking, contamination
controls and chilling (FSA’s 4 C’s)
Increased risk
factors e.g. Age
HOSPITALS
PLACES PEOPLE WORK
AND LIVE
Inappropriate use of industrial and household
antimicrobial cleaners
Effluent discharged intothe environment
Waste discharged intothe environment
levels of cleanliness/
hygiene
Transfer of resistance in reservoir
Assurance of appropriate cleaning (where appropriate)
Controls on manufacture/use of cleaning materials
Effluent discharge controls
Manufacturing and use of
antimicrobials
Infection prevention and control
Invasive procedures in primary care
INTER-NATIONAL
INTER-ACTIONS
Lighter controls on antibioticprescription/usage abroad
Direct contact + waste discharged into the environment
Direct contact
Education e.g.Not flushing incomplete antibiotic
courses down the toilet
Internal transfer of resistance (inc. from commensals)
Risk factors from community interaction e.g.Poor hand washing/general hygiene
Antibiotics available
on the internet
CARE HOMES
HARD TO REACH
GROUPS
Appropriate patient management e.g.
hydration
Insufficient antibitotic resistance training
More training and awareness
Uncompleted antibiotic courses
Gaps in the medical knowledge base for what
drives infections
OTHER PUBLIC SPACES
(e.g. public transport, gyms)
COMMUNITY HOSPITALS
Nurse prescribers Education
Understand other factors driving
Understand other drivers of infections
DAY CENTRES FOR THE ELDERLY
Sexually transmitted infections
Ineffective decontamination of dental equipment
Antibiotic prescribers
Dentists
Overprescribing antibiotics
GPs
Antibiotic prescribers
Overprescribing antibiotics
Resistant STI strains
Patients and visitorsentering & leaving hospitalsSCHOOLS/
NURSERIES/CRECHES
International consensus and
action on controls for antimicrobial use
People entering the UK from abroad
Poor infection prevention and
control
Best practice in prescribing in EU and other countries
Surveillance
Best practice on infection prevention and control in EU
and other countries
Imported food and imported animals (please see the Animal& Environment map)
Improve professional education, training and
public engagement
Direct Contact
Antimicrobial Use
Screening of patients/ infections for AMR
Development of new vaccines
Vaccinationcross-over between classes of
veterinary and medical antimicrobials
Conserve and steward the effectiveness of existing
treatments
Stimulate the development of new
antimicrobials, diagnostics and novel
therapies
Improve knowledge and understanding of AMR
Antimicrobial stewardship programmes
Patient treatment completion
Surveillance
Improve prescribing practice
Manage patient expectations
Appropriate prophylactic use
Follow up care
Stratified medicine
Diagnostics at pace
New diagnostic tests (including Whole
Genome Sequencing)
Faster access to patient’s medical history
AMR Systems Map – Influences on the development of AMR G.P. Care and the Community
Departmentof Health
AMR Systems Map – Influences on the development of AMR Pharmaceuticals Diagnostics and Vaccination
Pathway for microbes
KEY
Interventions
Influence on risk of infection
Influence on development of resistance
Reservoirs for microbes/resistance
Intended effects
Use of existing antimicrobials selects for
resistance
Use of new antimicrobials selects for resistance
Gen
eric
infe
ctio
n pa
thw
ay
Stimulate the development of new antimicrobials,
diagnostics and novel therapies
Diagnostics
Access to surveillance data
Identification and prioritisation of research and
development
Appropriate research and development
Funding
Industry confidence in demand for new products
Government influence
Take into account costs of AMR when evaluating
value for money
Address concerns over cost and complexity of regulatory
approval process
Address uncertainty about the regulatory environment
for new antimicrobials
Pharmaceutical industry develops new products
Joined up approach to antimicrobial prescribing/use
between animals and humans
Guidance/legislation on appropriate use of existing
and new antimicrobials
Use of new antimicrobials
Use of existing antimicrobials
Conserve and steward the effectiveness of new
treatments
INTER-NATIONAL
INTER-ACTIONS
International consensusand action
Sharing of data internationally
EU regulation
MHRA and VMD
Rapid diagnostics
Drug/Bug combinations
Improved surveillance data
Improve knowledge and understanding of AMR
Whole genome sequencing
Point of care testing
Acknowledgements 9
AcknowledgementsAMR Systems Map Design
Stephen Dobra & Peter Johnston – Department of Health
Further developed by:
Matthew Baugh, Christina Barfoot, Peter Bennett, Stephen Dobra – Department of Health Suzanne Eckford – DEFRA
Created on Microsoft Visio 2010 by Peter Johnston, Matthew Baugh & George Chappelle
Thank you to the following for participation in workshops developing the initial map and the Animals & the Environment Map sub map:
From DEFRA:
Suzanne Eckford Head of Antimicrobial Resistance Team, Veterinary Medicines Directorate (VMD)
Helen Jukes Head of General Assessment and Research Team, VMDKen Stapleton Human and Environmental Safety Assessor, VMDChris Teale Head of AMR, Animal Health and Veterinary Laboratories Agency
(AHVLA)Emma Snary Head of Risk Analysis, AHVLA
From DH:
Dr Peter Bennett Head of Analysis, Health Protection, Public and International Health Directorate (PIHD)
Stephen Dobra Analytical Programme Manager, PIHDMichael Fleming Analytical Programme Manager, PIHDPeter Johnston Operational Research Analyst, PIHDRoss Leach Economic Advisor: Medicine, Pharmacy and IndustrySally Wellsteed Antimicrobial Resistance and HCAI Team Leader, PIHD
From Public Health England:
Dr Andre Charlett Head of Statistics, Modelling and Economics Department
Professor Alan Johnson Head, Department of Healthcare Associated Infection and Antimicrobial Resistance
Dr Julie Robotham Mathematical Modeller/Health Economist
Facilitated by: Dr Peter Bennett, Stephen Dobra & Peter Johnston – DH

10 Antimicrobial Resistance (AMR) Systems Map
© Crown copyright 2014 2902838 Produced by Williams Lea for the Department of Health
Departmentof Health
Thank you to the following for participation in a workshop that developed the G.P. Care & the Community and Hospital sub maps:
Isabel Boyer – Lay Member, Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection (ARHAI)
Dr Ceire Costelloe – Lecturer in Medical Statistics, Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London
Dr Nicholas Brown – Consultant Medical Microbiologist at Addenbrooke’s Hospital in Cambridge and Clinical Services Director. President of the British Society for Antimicrobial Chemotherapy (BSAC)
Dr Kumara Dharmasena – Consultant Microbiologist, Walsall Hospitals NHS Trust
Rosie Dixon – Senior Nurse, Infection Prevention and Control at Sheffield Health and Social Care NHS FT
Michael Fleming – Analytical Programme Manager, Department of Health
Dr Nick Francis – Senior Clinical Research Fellow, Cardiff University
Martin Kiernan – Nurse Consultant – Southport & Ormskirk NHS Trust & member of ARHAI
Dr Chris Settle – Consultant Microbiologist, City Hospitals Sunderland
Facilitated by Peter Bennett, Stephen Dobra & Carole Fry – DH
Reporting by Christina Barfoot & Matthew Baugh
Thank you to Dr Elizabeth Jones – Head of Patient Environment, Department of Health for contributing on Estates issues.
Thank you to:
Richard Carter – DH Life Sciences, Office for Life SciencesRoss Leach for reviewing the Pharmaceutical sub map





























