Embed Size (px)
Citation preview

Antimicrobial Stewardship
St. Mary’s Hospital Infection Control Committee

What is Antimicrobial Stewardship
• An interdisciplinary team dedicated to practices that improve appropriate selection, dosing, route, and duration of antimicrobial therapy
• The ultimate goal of antimicrobial stewardship is to improve patient care and health care outcomes
Antimicrobial Stewardship Team• Infectious Disease Physician• Clinical Pharmacist• Clinical microbiologist• Information System
Specialist• Infection control
professional• Hospital epidemiologist• Leadership support
Elements of an Antimicrobial Stewardship Team
• A comprehensive program will include:– Active monitoring of resistance– Fostering of appropriate antimicrobial use– Collaboration with an effective infection control
program to minimize secondary spread of resistance is considered optimal

Elements of an Antimicrobial Stewardship Program
• Prospective audit with intervention and feedback
• Formulary restriction and preauthorization
• Guidelines and clinical pathways
• Antimicrobial cycling• Antimicrobial Order Forms• Monitoring of progress and
outcome measures
• Education• De-escalation of therapy• Dose optimization• Conversion from parenteral
to oral• Computer
Surveillance/Decision Support
• Microbiology Laboratory
Prospective audit,intervention,and feedback
• Have the clinical pharmacist on the floor making recommendations about appropriate antibiotic, route, length of therapy
• Probiotic Protocol to prevent C. Diff
• Focus on one floor for recommendations
• Up to a 37% reduction in the number of days of inappropriate antibiotic use.Approx. $400.00 cost savings per patient
• While assessing patients for probiotics look at de-escalating of antibiotics
• Decrease rate of C. Diff
Formulary restriction and preauthorization requirements for specific agents
• Control of certain antibiotic use through Pharmacy and Therapeutics Committee can be very effective
• Control of Cleocin use has led to prompt cessation of nosocomial outbreak of C. Diff
• Restriction of Vancomycin and third generation cephalosporins in response to VRE has demonstrated mixed results
Education• Conference Presentations • Student teaching• E-mail alerts• Provision of written
guidelines• Peri-operative area order
forms• Share results of audits
Guidelines and Clinical Pathways• Implementation of guidelines
incorporating local microbiology and resistance patterns
• Balance antibiotics in HAP and VAP patients
• Use algorithms incorporating the clinical pulmonary infection score
• Leads to decreased duration of therapy,decreased VAP recurrence, decrease of multi-drug resistance patterns

Antimicrobial Cycling• Slows spread of
resistance• Most popular is
Gentamicin to Amikacin• Ceftazadime for
Ciprofloxacin lead to a decreased incidence of VAP
Antimicrobial Order Forms• Use of Peri-operative
prophylactic order forms with automatic stop at 2 days (SCIP Guidelines)
• Pneumonia Order set (Pneumonia core measures) with 6 different pneumonia indications and drugs
• Order forms facilitate implementation of practice guidelines
Streamlining or De-Escalation of therapy• Continuing excessive broad therapy contributes to the selection of
antimicrobial resistant pathogens• When culture results become available we can streamline or de-
escalate antimicrobial therapy to more targeted therapy that decreases antimicrobial exposure and contains cost
• This can also lead to avoidance of redundant inpatient antibiotic- days

Dose Optimization• Dosing that accounts for
individual patient characteristics (age,weight,renal function)
• Site of infection• Pharmacokinetics -Vancomycin
and aminoglycosides• Optimize antimicrobial
pharmacodynamics of the drugs B-lactams and fluoroquinolones

Conversion from parenteral to oral therapy
• Having a systematic plan for switching from parenteral to oral treatment may have an added benefit of aiding in early hospital discharge planning
• Development of clinical criteria and guidelines allowing conversion can facilitate implementation.
Computer Surveillance / Microbiology
• Add cost codes to antimicrobial susceptibility data
• Antimicrobial report to pharmacy
• Vancomycin dosing/utilization sheet
• Review antimicrobial errors• Leap frog to CPOE
• Actively involved in resistance surveillance
• Update antibiogram annually
• Make easily accessible to physicians
St.Mary’s Antibiotic Stewardship Efforts to Date
• Probiotic Protocol• Antibiogram on line• Pneumonia Order sets• Pharmacokinetics• Peri-op Area Guidelines• IV to PO conversion• Culture results from lab• Pharmacy/IS generated
pneumonia vaccine program
What does our future hold for Antibiotic Stewardship
• Assign antibiotic rounds to new pharmacy school professor ( de-escalating and streamlining)
• Follow culture results from lab
• Approve IV to PO conversion automatic by pharmacist
• Finish 6 month Probiotic study
• Work on Vancomycin Order form

Antibiotic Stewardship 2013
0
20
40
60
80
100
120
140
Jan-1
4
Mar
-14
May
-14
Jul-1
4
Sep-1
4
Nov-14
#Interventions
% Acceptance
15.5
16
16.5
17
17.5
18
18.5
1stQtr 2ndQtr 3rd Qtr 4th Qtr
TARGETAthens cost per dischargeTotal Savings 2013 $15,458

Change Dose
Change Antibiotic
IV to PO conversion
DiscontinueTherapy
Add an antibiotic
Renal dosing
Streamline Other: Probiotic
Accepted 1
10 21 28 1 15 2 8
Not accepted
5
6 3 1
Total 1 15 27 31 2 15 2 8
Documentation of Interventions by type
MONTH : SEPTEMBER 2013Total Antibiotic Interventions:100
Percent Accepted: 85%
• April Ecker and Gin Fleming (Antibiotic Pharmacist)

C.H.E. Act Initiatives Thru September 2013
0
5
10
15
20
25
2011-2013 Target
Cost peradjusteddischarge
0
1
2
3
4
5
6
7
8
9
Mar
-12
May
-12
Jul-1
2
Sep-1
2
Nov-12
Jan-
13
Mar
-13
May
-13
Jul-1
3
Sep-1
3
Target
Asthma Drugs Cost peradjusted discharge
0.7
0.75
0.8
0.85
0.9
0.95
1
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
TARGET
PPI COST PER ADJUSTEDDISCHARGE
0
1
2
3
4
5
6
7
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Target
Anticoag cost peradjusted discharge
Anti-infectives (Antibiotics)
Anticoagulants
Asthma Drugs Proton Pump Inhibitors
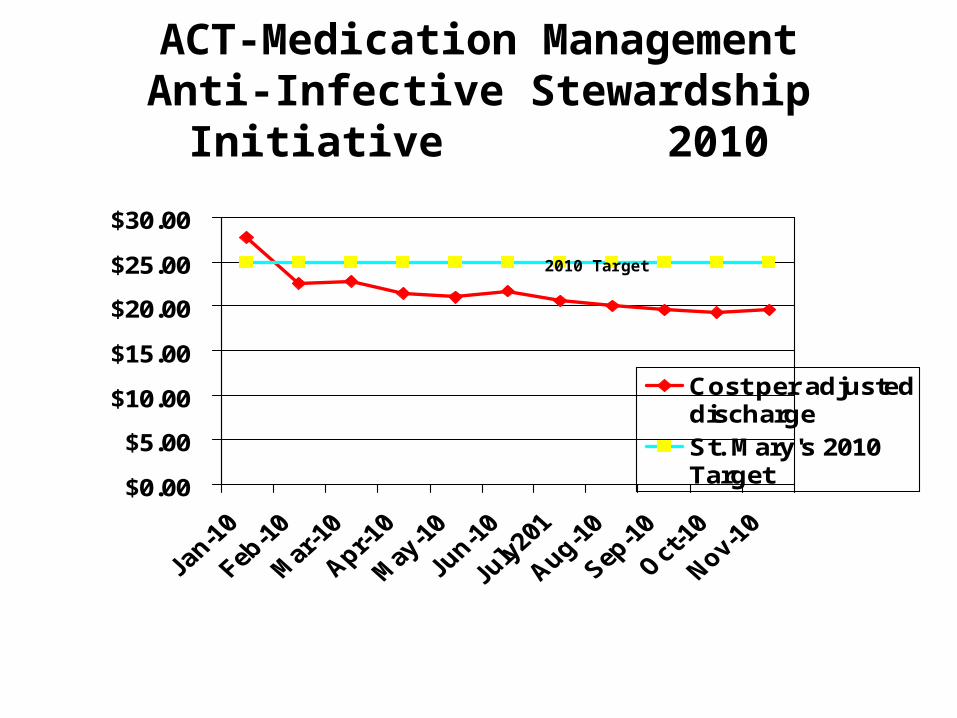
ACT-Medication ManagementAnti-Infective Stewardship Initiative
2010
$0.00
$5.00
$10.00
$15.00
$20.00
$25.00
$30.00
Cost per adjusteddischargeSt. Mary's 2010Target
2010 Target