Embed Size (px)
Citation preview
Antimicrobial stewarship in different scenarios
Programy Optimalizacepoužívání Antibiotik (PROA)
Juan Pablo Horcajada
Service of Infectious Diseases
Hospital del Mar, Barcelona, Spain

Summary
1. Introduction
2. Current concerns on antimicrobial resistance
3. Antimicrobial stewardship programs
4. AMS in different scenarios including ICU
5. Implementation strategies
6. Conclusions

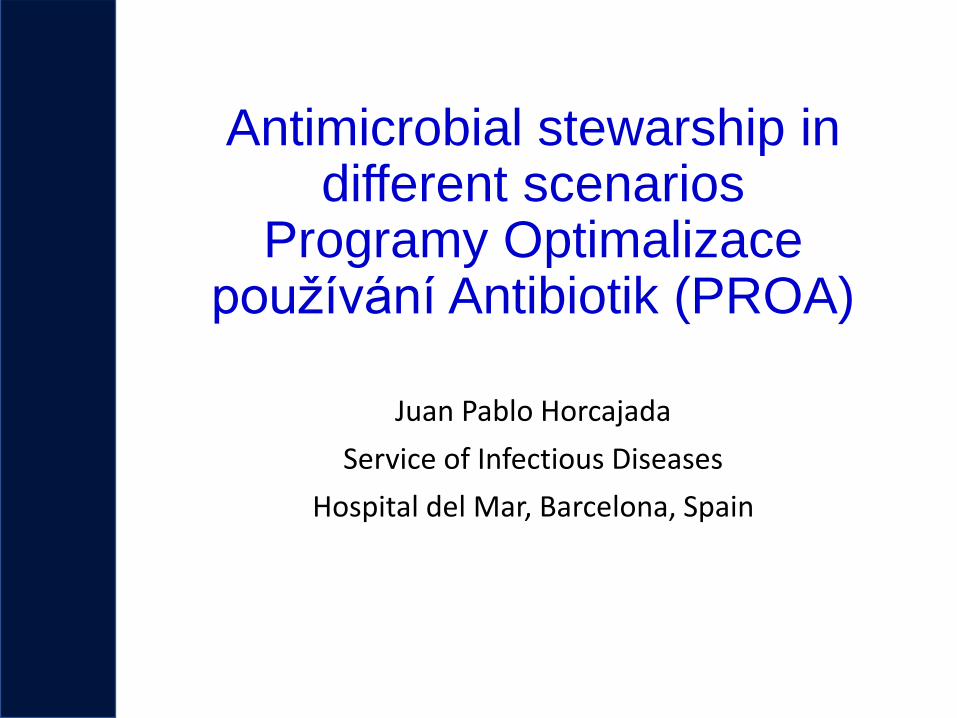
Introduction
• Antimicrobials: one of the biggest advances in medicine
• Since their introduction resistances are developed
• One of the main public health menaces
• 3 Solutions: new drugs, better infection control and optimizing antimicrobial use.
Rodríguez-Baño et al. SEIMC Enferm Infecc Microbiol Clin. 2012 Jan;30(1):22.e1
Introduction
• Los antibióticos: uno de los mayores
avances en la medicina.Mortality rates from all causes, non-infectious causesand for infectious diseases during the period 1900-1996
Armstrong GL et al, JAMA 1999;281(1):61-66
“The antibioticMiracle“

Antimicrobial resistance: future landscape
Projection of deaths attributed to multidrug resistance in
2050 in comparison with those attributed to other causes.
Jim O’Neill. Antimicrobial Resistance: Tackling a crisis for the health and wealth of nations. Dec 2014

Antimicrobials are different
• High cure rate, and (relatively) safe
• Any doctor can prescribe them: risk of overuse
or inappropriate use.
• Between 25-50% of hospital prescriptions are inadequate
• Peculiarity: the choice directed to a patient can have an
ecological impact:
• compromises the evolution of another patient
• enviroma
Goff DA. Curr Opin Infect Dis 2011; 24 (Suppl 1): S11

Charani et al. JAC 2010
Antimicrobial prescription
• Antimicrobial prescription is very difficult
• Currently there is a high demand due to multidrug resistanceand complexity of infections and patients
• Prescriptors we need:
- A cultural context priorizing the adequate use of antimicrobials
- Insitutional support, training and tools

Clinical outcomeHealthcare quality
Collateral damage:- Resistances- Adverse events- Costs
Looking for equilibrium

Programas de Optimización del uso de Antimicrobianos (PROA)
Programy Optimalizace používání Antibiotik
- Institutional multidisciplinary programs that intend to improve
clinical responses through appropriate use of antimicrobials
- Objectives: To optimize the choice, dose, route and duration
of antibiotic treatment
- These programs along with infection control and surveillance
programs play a crucial role in reducing the selection and
transmission of resistant pathogens.
- Cost-effectiveness

Spanish PROA Guidelines

PROA: Institutional Frame
• Institutional initiative, emanated from the Infection
Committee
• Multidisciplinary teams integrating the main specialties
in the field of diagnosis and treatment of infectious
diseases and use of antimicrobials
• Support from the Hospital Director or Manager

PROA: Services portfolio
• Monitoring
• Antimicrobial use and expenses,
• Prescription quality
• Results: indicators and resistances
• Antimicrobial therapy guidelines: gold standard
• Audits / advice
• Education and comunication

• Creation and dissemination of training materials on AMS
Programs / Teams
• AMS training accreditation system
• Training actions directed to AMS teams and professionals
• Activities included in the time of training of professionals
from Hospital Manager
• Training and activities of scientific societies
PROA: Education

Infectious Diseases Specialist (coordinator)
Antimicrobial expert Pharmacist
Microbiologist expert in antimicrobial resistance
Intensive care physician (if ICU)
PROA TÝM

Effects
• Better antimicrobial use
• Adequate therapy
• Safety and efficacy
• Reduce spectrum or duration
• atb load and resistences
• Hospital stay Saving €
• Re-admissions
Activities
• Education
• Optimizing indication
• Dose adjustment (PK/PD)
• Rapid diagnosis
• De-escalation
• Shorten duration
• Assesment at discharge
Activities and effects PROA
➔

• Monitoring resistances
• Monitoring antimicrobial use
• Indicators: performance and results
• Antimicrobial therapy guidelines: gold standard
• Audits and interventions
• Education and comunication
Antimicrobial stewardship essentials

• Monitoring resistances
• Monitoring antimicrobial use
• Indicators: performance and results
• Antimicrobial therapy guidelines: gold standard
• Audits and interventions
• Education and comunication
Antimicrobial stewardship essentials

Epidemiologic mapsHOSPITAL DEL MAR. URINE CULTURES. E. COLI. 2012-2018

Epidemiologic mapsHOSPITAL DEL MAR. URINE CULTURES. E. COLI. 2012-2018

• Monitoring resistances
• Monitoring antimicrobial use
• Indicators: performance and results
• Antimicrobial therapy guidelines: gold standard
• Audits and interventions
• Education and comunication
Antimicrobial stewardship essentials

Monitoring antimicrobial use

Monitoring antimicrobial use

• Monitoring resistances
• Monitoring antimicrobial use
• Indicators: performance and results
• Antimicrobial therapy guidelines: gold standard
• Audits and interventions
• Education and comunication
Antimicrobial stewardship essentials

Indicators: adequacy of therapy
Adquisition
Total
N=720
Community
N=463
Nosocomial
N=71
HCA
N=186
p
Inadequate to
guidelines
203 (28%) 106 (23%) 33 (47%) 64 (34%) <0.01
“In vitro”
inadequate
90 (13%) 53 (11%) 9 (13%) 28 (15%) 0.454
Catalan AMS Program. PROA VINCAT 2017
Bacteremic UTI due to E. coli.
Data from 39 Hospitals. Catalunya 2017-2018
Place of acquisition
TotalN=1976
CommunityN=1260
HospitalN=189
Ambulatory Healthcare system
N=527
p
Inadequate to guidelines 557 (28.2%) 307 (24.4%) 82 (43.4%) 168 (31.9%) <0.001
Inadequate “in vitro” 264 (13.4%) 135 (10.7%) 34 (18%) 95 (18%) <0.001
Fluorquinolone R 719 (36.4%) 351 (27.9%) 74 (39.2%) 294 (55.8%) <0.001
ESBL 337 (17.1%) 131 (10.4%) 41 (21.7%) 165 (31.3%) <0.001
Carbapenem R 16 (0.8%) 6 (0.5%) 2 (1.1%) 8 (1.5%) 0.07

• Monitoring resistances
• Monitoring antimicrobial use
• Indicators: performance and results
• Antimicrobial therapy guidelines: gold standard
• Audits and interventions
• Education and comunication
Antimicrobial stewardship essentials

European UTI guidelines
Uncomplicated UTI
Grabe et al. Guidelines of Urological Infections. EUA 2015NB: International Guidelines may not reflect
local AUS guidelines. See. www.tg.org.au.
• Monitoring resistances
• Monitoring antimicrobial use
• Indicators: performance and results
• Antimicrobial therapy guidelines: gold standard
• Audits and interventions
• Education and comunication
Antimicrobial stewardship essentials
0,00
20 000,00
40 000,00
60 000,00
80 000,00
100 000,00
120 000,00
140 000,00
160 000,00
180 000,00
200 000,00
I.15 II.15III.15IV.15V.15VI.15VII.15VIII.15IX.15X.15XI.15XII.15I.16 II.16III.16IV.16V.16VI.16VII.16VIII.16
Co
ste
n €
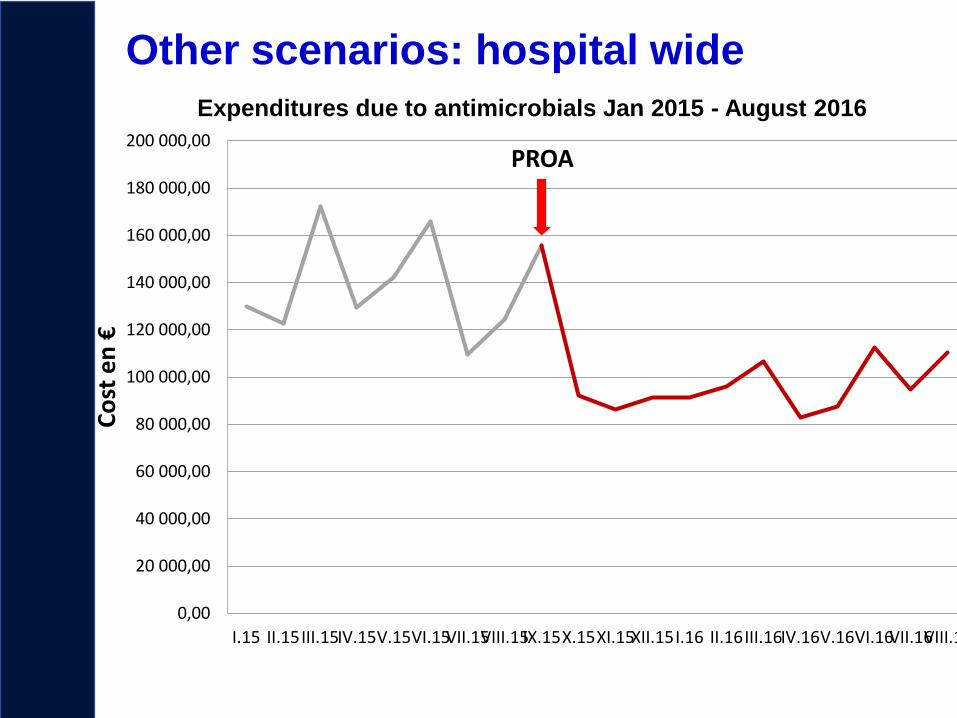
Expenditures due to antimicrobials Jan 2015 - August 2016
PROA
Other scenarios: hospital wide

Between october 2015 and october 2016 a reduction of costs
from 1.299.219 to 782.434 euros, saving:
516.785 euros (39,7% ).
13,299,441 Kc !
Our experience
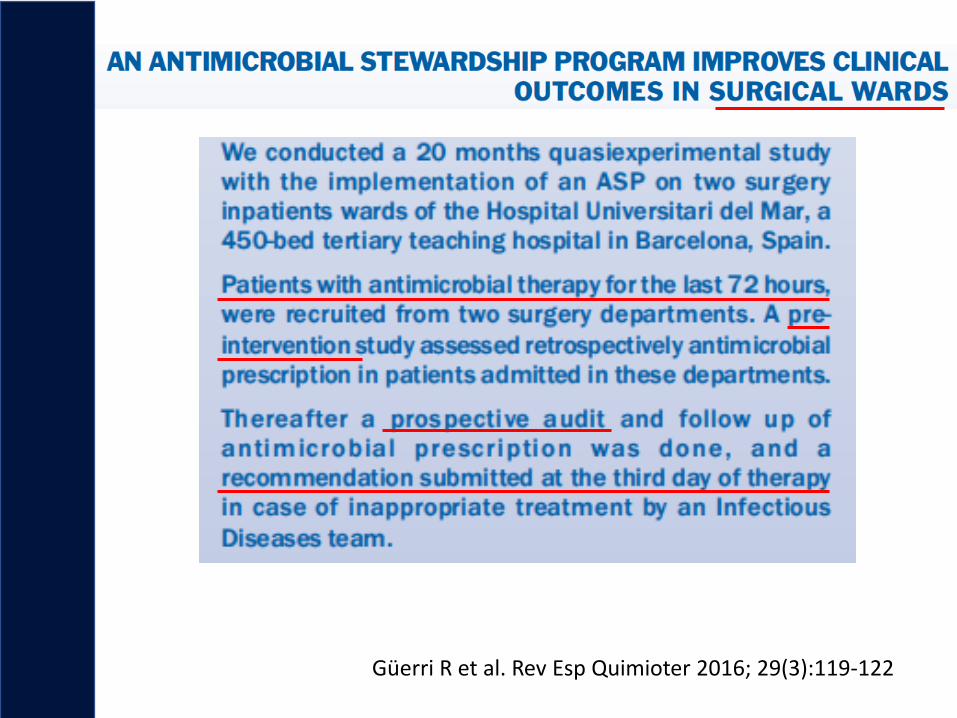
Güerri R et al. Rev Esp Quimioter 2016; 29(3):119-122

Güerri R et al. Rev Esp Quimioter 2016; 29(3):119-122

Güerri R et al. Rev Esp Quimioter 2016; 29(3):119-122
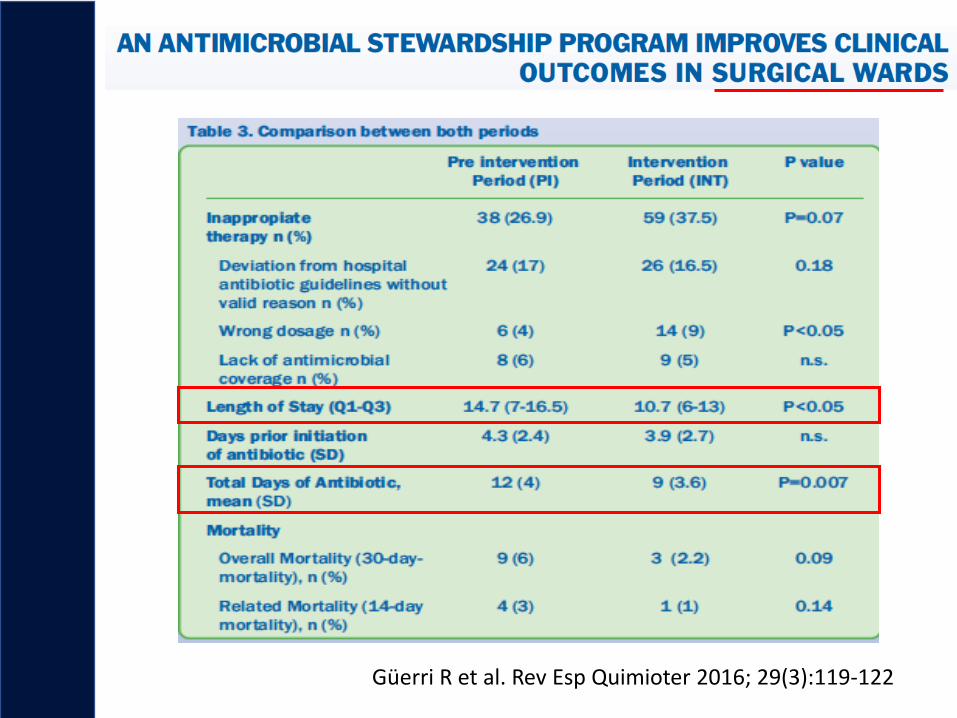
Güerri R et al. Rev Esp Quimioter 2016; 29(3):119-122

AMS Program in the ICU. Hospital del Mar. Barcelona
Alvarez Lerma et al. Antimicrobial Agents Chemother 2018;62:e01825-17.

AMS Program in the ICU. Barcelona• Multidisciplinary group with specialists in infectious diseases, pharmacy,
microbiology, and intensive care medicine responsible for the design and implementation of the AMS program
• Computer application for prescription of antimicrobials
• Selection of 10 antimicrobial agents due to their greater environmental and economic impact, for special control measures:
• to justify their indications in writing through the computer application form
• compulsory information of the duration of treatment,
• immediate information of the cost of prescription
• automatic discontinuation of drug administration on the day set by the prescriber physician,
• reassessment of indications during the next 24 to 72 h by a member of the working group.
• Daily review of antibiotics regimens of all patients during the shift change (8:00 a.m., 3:00 p.m., and 9:00 p.m.),
• Dose adjustment, de-escalation, or withdrawal in the daily clinical sessions of the ICU staff (2:00 to 3:30 p.m.).
• Decisions taken by consensus of the ICU team.
• Support from de Medical Director
Alvarez Lerma et al. Antimicrobial Agents Chemother 2018;62:e01825-17.


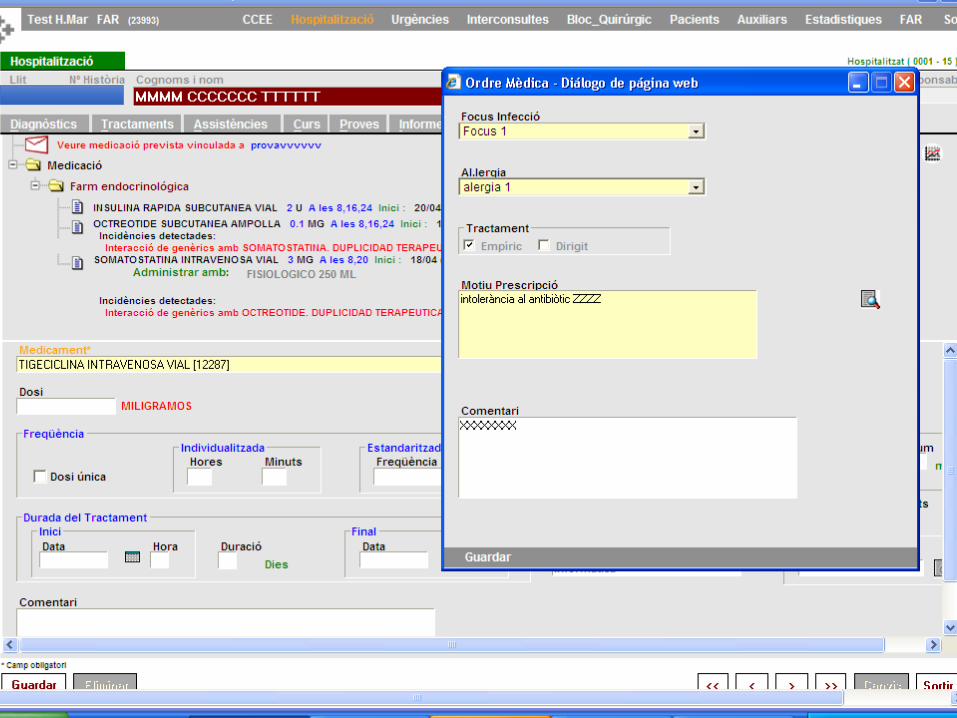


Circuit
• When finishing the prescription
• Information about the cost of therapy appears
• Automatic query to AMS team


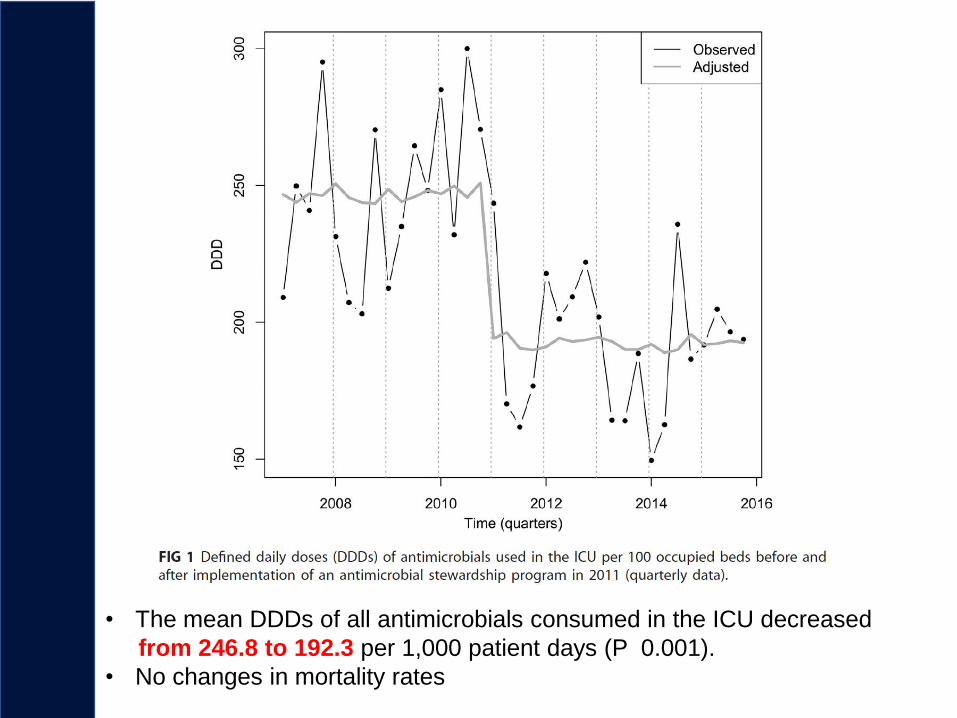
• The mean DDDs of all antimicrobials consumed in the ICU decreased
from 246.8 to 192.3 per 1,000 patient days (P 0.001).
• No changes in mortality rates
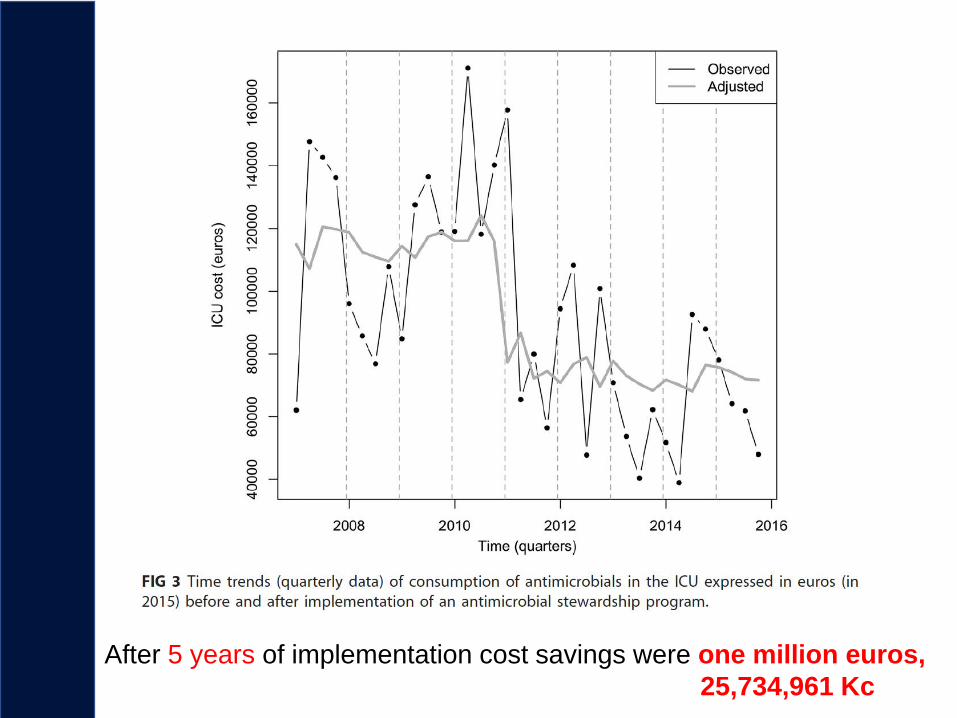
After 5 years of implementation cost savings were one million euros,
25,734,961 Kc

Conclusions
• Antimicrobial resistance threat
• Antibiotics are more difficult to use in the era of AMR
• Antimicrobial stewarship is one important tool
against AMR
• Therapy is influenced by AMR = less options
• Monitoring AMR and antibiotic use
• Indicators and interventions