Embed Size (px)
Citation preview

Clinical Research
Antimicrobial Susceptibility and Characterizationof Virulence Genes of Enterococcus faecalisIsolates from Teeth with Failureof the Endodontic Treatment
Marlos Barbosa-Ribeiro, DDS, MSc, Adriana De-Jesus-Soares, DDS, Msc, PhD,Alexandre A. Zaia, DDS, MSc, PhD, Caio C.R. Ferraz, DDS, MSc, PhD,Jos�e F.A. Almeida, DDS, MSc, PhD, and Brenda P.F.A. Gomes, DDS, MS, PhDAbstract
SignificanceEnterococcus faecalis is a Gram-positive bacte-rium that has different mechanisms of virulenceand resistance that make it difficult to be eradi-cated from the root canals. Its increasing resis-tance to antimicrobial agents is a concern asit can have a negative effect on treatment effective-ness. E. faecalis isolates from persistent endo-dontic infections showed varied degrees ofsusceptibility to several antimicrobial agents, be-ing amoxicillin + clavulanate the most effectiveagent. Moreover, the strains showed differentexpression profile of virulence factors.
Introduction: The aim of this study was to investigatethe prevalence of virulence factors and the antimicrobialresistance of Enterococcus faecalis isolates of teethwith failure of the endodontic treatment. Methods:Twenty root canal samples were collected from teethwith apical periodontitis. E. faecalis was firstly identi-fied based on phenotypic features and then by 16Sribosomal RNA gene sequencing. The antimicrobial sus-ceptibility was determined by the minimum inhibitoryconcentration (MIC) of amoxicillin, amoxicillin + clavula-nate, azithromycin, benzylpenicillin, ciprofloxacin, clin-damycin, chloramphenicol, doxycycline, erythromycin,gentamicin, metronidazole, moxifloxacin, rifampicin,tetracycline, and vancomycin using the E test method.Virulence factors (ace, asa, asa373, cylA, efaA,esp, and gelE) were detected by polymerase chain reac-tion assay. Results: Amoxicillin + clavulanate was effec-tive against all strains. Intermediate and total resistancewas found against the majority of the tested antimicro-bials. The susceptibility of some microorganisms tosome antimicrobial agents changed according to the eval-uation time. MIC50 and MIC90 also varied according tothe evaluation time. In relation to the virulence factorsof the E faecalis isolates, ace was detected in 100%of the strains, asa (60%), asa373 (15%), efaA (95%),esp (70%), and gelE (75%), whereas cylA was notdetected. Conclusions: It was concluded that E. faeca-lis isolates from persistent endodontic infections showedvaried degrees of intermediate/total resistance to severalantimicrobial agents, with amoxicillin + clavulanate beingthe most effective agent. Moreover, the strains showeddifferent patterns for virulence gene detection. (J Endod2016;42:1022–1028)
From the Department of Restorative Dentistry, Endodontic DivisAddress request for reprints to Dr Brenda P.F.A. Gomes, Depar
Campinas–UNICAMP, Av Limeira, 901, Bairro Are~ao, Piracicaba, SP0099-2399/$ - see front matter
Copyright ª 2016 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2016.03.015
1022 Barbosa-Ribeiro et al.
Key WordsBacteria, Enterococcus faecalis, microbial sensitivity tests, virulence factor
Bacteria and their viru-lence factors are the
main agents for the emer-gence of post-treatmentapical periodontitis. Theymay have survived thechemomechanical proce-dures or invaded the canalvia coronal leakage ofthe root filling. Bacterialcultures and molecularstudies have confirmedthat Enterococcus faeca-lis is one of the most prev-alent bacteria found in the
root canal after endodontic treatment (1, 2). Enterococci are gram-positive cocci,and because of their morphologic and genetic characteristics, they can resist intracanalprocedures and systemic antibiotics, even in ecologic conditions of stress (3).The resistance mechanisms of E. faecalis result from physiological or structuralchanges in the bacterial cell, which is a survival strategy to abusive attack by antimicrobialagents (2). Enterococcus spp. has acquired genetic determinants conferring resistanceto several classes of antibiotics, including clindamycin, erythromycin, tetracycline, chlor-amphenicol, and, more recently, vancomycin (2, 4–6). Although the incidence ofresistant strains is more pronounced in hospital or systemic infections, studies usingbacterial isolates of endodontic infections have shown the emergence of bacterialresistance, especially at conventional regimens used in dental procedures (6).
Although systemic antibiotics are not commonly used in the treatment of intracanalinfections associated with chronic periapical lesions, in cases of patients with flare-upor at risk of bacterial endocarditis development, these become an important adjunct toendodontic treatment, being used in prophylactic regimens (2). Systemic antibiotics actas an adjunct to the conventional surgical methods and should be used with restraintbecause of the possibility of allergic reactions, toxicity, side effects, and development of
ion, Piracicaba Dental School, State University of Campinas, Piracicaba, S~ao Paulo, Brazil.tment of Restorative Dentistry, Endodontic Division, Piracicaba Dental School, State University of, Brazil, 13414-903. E-mail address: [email protected]
JOE — Volume 42, Number 7, July 2016

Clinical Research
resistant strains of microbes (2, 6). Therefore, it is imperative tomonitor E. faecalis resistance against the main antibiotics used inendodontics in order to provide updated data to guide physicians forthe most effective therapy (6). Periodic and accurate antimicrobial sus-ceptibility information is necessary to guide therapy and to call attentionto the problem of antimicrobial resistance.The epsilometer test (E test; BioM�erieux SA, Marcy-l’Etoile, France),an agar diffusion susceptibility test, holds the promise of being accurateand flexible enough to be performed in most clinical laboratories (7)and was thus used in several studies (1, 6, 8).
Virulence factors are means that microorganisms have to facilitateadherence, colonization, resistance, pathogenicity, and evasion of thehost immune response (3). The role of virulence factors of Entero-coccus spp. has not been fully elucidated and has attracted attentionbecause of its ability to enhance the infection and to generate exacerbatedresponses. These strains, even in the presence of a restricted nutritionalenvironment, can possess diversified mechanisms of virulence depen-dent on the genetic exchange process among them during the infectioncourse (9). The virulence factors that are more often related to E. fae-calis are the following: ace (collagen binding protein), asa and asa373(aggregation substance), cylA (hemolysin activator), efaA (antigen en-docarditis), esp (protein surface), and gelE (gelatinase). The expressionof these genes into endodontic biofilm can enable or exacerbate distincttissue responses at the periapical region, so it is imperative to understand
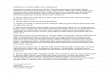
Figure 1. Culture plates and Gram staining of E. faecalis. (A) Colonies growing(C) m-Enterococcus agar plates. (D) Gram staining showing gram-positive cocci.
JOE — Volume 42, Number 7, July 2016
the specific role of each in the pathogenicity of the infectious contents ofthe root canals.
Therefore, the purpose of this study was to analyze the antimicro-bial susceptibility against antibiotics prescribed in endodontics by usingthe E test and to determine the prevalence of virulence factors of strainsof E. faecalis isolates from post-treatment apical periodontitis.
Materials and MethodsPatient Selection
Twenty patients were selected from those who attended thePiracicaba Dental School of the State University of Campinas, S~ao Paulo,Brazil, for nonsurgical endodontic retreatment.
The Human Research Ethics Committee of the Piracicaba DentalSchool approved a protocol (#018/2014) describing the specimencollection for this investigation, and all the patients signed an informedconsent form to participate in this research. The age of the patientsranged from 30–60 years old. All the specimens selected were root-filled teeth and showed radiographic evidence of apical periodontitis.
Failure of root canal treatment was determined based on clinicaland radiographic examinations. The presence of persistent periapicalradiolucent lesions; voids in or around the root canal filling; and persis-tent symptoms such as pain on palpation, discomfort to percussion, andpersistent sinus tract were considered reasons for retreatment (1).
on 5% defibrinated sheep blood–FAA agar. (B) Mitis salivarius agar plates.
Resistance and Virulence of Enterococcus faecalis 1023

Figure 2. The E test method. Plate with bacterial growth of E. faecalis andvancomycin strip after 48 hours of incubation. The arrow shows the intersec-tion point between the inhibition halo and the E test strip.
Clinical Research
Exclusion criteria were as follows: subjects who had received anti-biotic treatment within the preceding 3 months, subjects presentingwith reported systemic disease classified as American Society of Anes-thesiologists 3, teeth that could not be isolated with a rubber dam,and teeth with periodontal pockets deeper than 3 mm.
Endodontic Sample Collection and Clinical ProceduresDisinfection procedures, access to the pulp cavity, and sampling
were performed according to Endo et al (2) and Martinho and Gomes(10). Root filling materials were removed by using Reciproc R25 files(VDW, Munich, Germany) with no chemical solvent along the workinglength, which was radiographically obtained before surgery andcomplemented with the use of an apex locator (Novapex; Forum Tech-nologies, Rishon le-Zion, Israel). Next, 3 sterile paper points (Dents-ply Maillefer, Ballaigues, Switzerland) were consecutively introducedinto the full length of the canal and retained in position for 60 seconds.The paper points were then placed in a sterile tube containing 1 mLViability Medium G€oteborg Agar III (VGMA III) transport medium(11) for microbial culture; they were transported within 15 minutesto an anaerobic workstation (Don Whitley Scientific, Bradford, UK)for bacterial culture analysis.
Root canals were prepared with 2% chlorhexidine gel or 6%sodium hypochlorite using Reciproc R40 files (VDW) according to themanufacturer’s instructions in a reciprocating workingmotion generatedby themotor. Both instrumentation and irrigation were repeated until theReciproc file reached the working length (0 point on the display of theapex locator). A close inspection at high magnification with a dentaloperating microscope (DF Vasconcelos S/A, S~ao Paulo, Brazil) showedcomplete removal of gutta-percha, with the root canal walls being smoothand free of visible debris.
A final irrigation with 3 mL 17% EDTA was applied continuouslyfor 3 minutes under stirring, and ultrasound (Advanced SE; Micro-dont, S~ao Paulo, SP, Brazil) was used with tip ET40 (Satelec/Acteon,Mount Laurel, NJ) for 60 seconds alternately followed by 5 mL sterilesaline. Finally, all teeth were dried and filled with a single gutta-perchacone (Dentsply Maillefer) and Endom�ethasone sealer (Septodont,Saint-Maur-des-Foss�es, France). Access cavities were restored withColtosol (Coltene Whaledent Inc, Cuyahoga Falls, OH) at a thicknessof at least 2 mm, and a second layer of composite material (FiltekZ250; 3M ESPE, St Paul, MN) was applied in combination with a singlebond adhesive.
Microbial Culturing and Molecular Identificationof E. faecalis Isolates by 16S RibosomalRNA Gene Sequencing
Microbial sampling, isolation, and speciation were performed byusing advanced microbiological techniques for anaerobic species.Inside the anaerobic workstation, the tubes containing the transportmedium were shaken in a mixer for 60 seconds. Serial 10-fold dilu-tions were made up to 1/104 in prereduced Fastidious AnaerobeBroth (FAB; Laboratory M, Bury, UK), and 50 mL of each serial dilu-tion was plated onto several media as follows: 5% defibrinated sheepblood–Fastidious Anaerobe Agar (FAA, Laboratory M) alone and sup-plemented with 600 mL hemin and 600 mL menadione. The plateswere incubated at 37�C in an anaerobic atmosphere for up to 48 hoursto allow anaerobic or facultative microorganism growth. In addition,50 mL of the initial sample was plated onto m-Enterococcus agar(Difco, Sparks, MD) and Mitis salivarius agar (Difco) to increasethe chance of finding E. faecalis (Fig. 1A–C).
The preliminary characterization of microbial species was basedon the features of the colonies (ie, size, color, shape, height, rim, sur-
1024 Barbosa-Ribeiro et al.
face, texture, consistency, brightness, and hemolysis) through visualiza-tion with a stereoscopic lens (Lambda Let 2; Atto Instruments Co, HongKong, China) at 16�magnification. Isolates were then purified by sub-culture, Gram stained, tested for catalase production, and their gaseousrequirements were established by incubation for 2 days aerobically andanaerobically. Based on this information, it was possible to presumablyidentify E. faecalis (gram-positive cocci, catalase negative) (Fig. 1D).
The DNA frommicroorganisms presumably identified as E. faeca-lis was extracted and purified by using the QIAamp DNA Mini Kit (Qia-gen, Hilden, Germany) according to the manufacturer’s instructions.DNA concentration (absorbance at 260 nm) was determined with aspectrophotometer (Nanodrop 2000; Thermo Fisher Scientific, Wil-mington, DE). After amplification of the 16S ribonucleic RNA gene (for-ward primer: 50-GAG AGT TTG ATY MTG GCT CAG-3’; reverse primer:5’-GAA GGA GGT GWT CCA RCC GCA-30) (Invitrogen, S~ao Paulo, SP,Brazil) in the thermocycler (GenePro Thermal Cycler; Bioer Technol-ogy, Hangzhou, China), the purified product (QIAquick Gel Extraction,Qiagen) at a concentration of 40 ng/mL was submitted to sequencingusing the BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Bio-systems, Carlsbad, CA) according to the manufacturer’s recommenda-tions. The sequences obtained were first analyzed for quality andsimilarity of nucleotides by using the CLC Genomics Workbench soft-ware v6.5 (Qiagen). Those considered of good quality were alignedusing the Molecular Evolutionary Genetics Analysis version 6.0(MEGA 6) software (www.megasoftware.net) before comparison withthe sequences deposited in GenBank by using the basic local alignmenttool program for nucleotides (BLASTn; National Center for Biotech-nology Information National Library of Medicine, Bethesda, MD). Fora high level of quality of the sequences, a confidence level of 99%–100% similarity to E. faecalis was established (12).
Antimicrobial Susceptibility TestThe susceptibility of E. faecalis isolates was determined by the
minimum inhibitory concentration (MIC) of different antibiotics usingthe E test method (BioM�erieux SA, Marcy-l’Etoile, France).
JOE — Volume 42, Number 7, July 2016

TABLE 1. Range of Concentration of Antibiotics in the E Test Strip and Interpretive Cutoff Values Equivalent to the Minimum Inhibitory Concentration (mg/mL) ofAntimicrobial Bacteria Evaluated in the Enterococcus faecalis Tests
Antimicrobial agents Range (mg/mL) Susceptible Intermediate Resistant
Amoxicillin (AC) (256–0.016) #2 4 $8Amoxicillin + clavulanate (XL) (256–0.016) #4 8 $16Azithromycin (AZ) (256–0.016) #2 4 $8Benzylpenicillin (PGL) (256–0.016) #8 12 $16Ciprofloxacin (CI) (32–0.002) #1 2 $4Clindamycin (CM) (256–0.016) #2 4 $8Chloramphenicol (CL) (256–0.016) #8 16 $32Doxycycline (DC) (256–0.016) #4 8 $16Erythromycin (EM) (256–0.016) #0.5 1–4 $8Gentamicin (GM) (256–0.016) #4 8 $16Metronidazole (MZ) (256–0.016) #8 16 $32Moxifloxacin (MX) (32–0.002) #2 4 $8Rifampicin (RI) (32–0.002) #1 2 $4Tetracycline (TC) (256–0.016) #4 8 $16Vancomycin (VA) (256–0.016) #4 8-16 $32
Data from Clinical Laboratory Standard Institute [14].
Clinical Research
Colonies were suspended in Brucella broth (Laboratory M) toachieve a density corresponding to 1.0 McFarland turbidity standard.A cotton wool swab soaked in the inoculum was used to inoculatethe surface of the plates containing Brucella agar (Laboratory M).The E test strip was applied separately to the center of the plate withthe high MIC end toward the edge of the plate. The plates were thenimmediately incubated in an anaerobic chamber (Don Whitley Scienti-fic, Bradford, UK) for 24–48 hours. After growth, an ellipse of inhibitionwas seen around the strip. At the point of intersection of the ellipse withthe strip, the MIC was read from a rating scale (BioM�erieux SA) (Fig. 2).
Strains with an MIC less than or equal to the break points recom-mended by the Clinical Laboratory Standard Institute (CLSI, 2013) wereconsidered susceptible; those higher than the break points wereconsidered resistant. The reference values are shown at http://www.sciencedirect.com/science/article/pii/S0099239911006091 (Table 1).The MICs of antibiotics that inhibited 50% and 90% of the isolateswere calculated and expressed as MIC50 and MIC90, respectively.
Polymerase Chain Reaction Assayfor Virulence Gene Detection
Polymerase chain reactions (PCRs) for the detection of virulencegenes of E. faecalis were performed in a thermocycler (GenePro Ther-mal Cycler) according to Sedgley et al (13). A total volume of 30 mLcontaining 3 mL 10� PCR buffer (Invitrogen), 100 mmol/L deoxyribo-nucleotides (dNTP) mix (Invitrogen), 2.4mL 25 mmol/L MgCl2, 6 pmol
TABLE 2. Pair of Oligonucleotides (forward and reverse) Used in the PolymeraseIsolated from Teeth with Post-treatment Apical Periodontitis
Gene Primer
ace (collagen-binding protein) F: GGAATGAR: GCTTGATG
asa (aggregation substances) F: CCAGCCAAR: CTGGGTGT
cylA (hemolysin activator) F: GACTCGGGR: GCTGCTAA
efaA (endocarditis antigen) F: GCCAATTGR: CGCCTTCT
esp (surface protein) F: TTGCTAATR: GCGTCAA
gelE (gelatinase) F: ACCCCGTAR: ACGCATTG
JOE — Volume 42, Number 7, July 2016
of each respective primer (Invitrogen), 100–200 ng total DNA template,2 U Platinum Taq DNA polymerase (Invitrogen), and nuclease-free wa-ter was used. The PCR conditions were as follows: 15-minute initialenzyme activation/DNA denaturation step at 95�C followed by 35consecutive cycles at 94�C for 20 seconds, 58�C for 45 seconds, and72�C for 60 seconds. The primer sequences are listed in Table 2.
The PCR products were analyzed by electrophoresis using 1%agarose gel (containing ethidium bromide) in Tris/Borato/EDTA(TBE) buffer, with gels being analyzed under ultraviolet light. Thesize of the fragments generated by PCR was compared with the 1-KbPlus ladder (Invitrogen). The detection of target genes was consideredwhen there was a presence of positive bands.
ResultsE. faecalis was present in 100% of the root canals investigated.
One strain per canal was selected for this study, totaling 20 isolates.Different susceptibility patterns were found for the E. faecalis iso-
lates. All strains were susceptible to amoxicillin + clavulanate. Somestrains showed intermediary susceptibility to amoxicillin (5%), azithro-mycin (20%), benzylpenicillin (5%), ciprofloxacin (15%), doxycycline(5%), erythromycin (75%), tetracycline (10%), and vancomycin(15%). The other antibiotics had less favorable results, including clin-damycin (60%), chloramphenicol (5), gentamicin (65%), metronida-zole (95%), moxifloxacin (5%), and rifampicin (10%), because strainsexhibited resistance. The MIC50 and MIC90 values are listed in Table 3.
Chain Reaction for the Detection of Virulence Genes of Enterococcus faecalis
s pairs (50- 30) Amplicon size (bp)
CCGAGAACGATGGC 616TTGGCCTGCTTCCGCTATGGCGGACTAC 619GATTCCGCTGTTAGATTGATAGGC 688AGCTGCGCTTACGGACAGACCCTC 688GTTCCTTCTTTGGCGCTAGTCCACGACC 932CACTTGCATTGCCGATCATTGGTTT 405CTTTTCCATC
Resistance and Virulence of Enterococcus faecalis 1025

TABLE 3. Antimicrobial Activities of Various Antimicrobial Agents (mg/mL)against Enterococcus faecalis Isolates (N = 20) of Teeth with EndodonticTreatment Failure
Antimicrobialagents
MICSusceptibility
rate (%)
Range MIC50 MIC90 S I R
AC 0.13–5.33 0.38 0.5 95 5 —XL 0.09–2.67 0.4 0.88 100 — —AZ 0.48–14.67 2.67 13.3 80 20 —PGL 0–9.33 0.92 2.17 95 5 —CI 0.007–2 0.63 1.83 85 15 —CM 0.01–64 29.3 64 30 10 60CL 0.19–14.67 4 7.33 95 — 5DC 0.02–6 0.25 0.71 95 5 —EM 0.02–6.7 0.92 3 25 75 —GM 0.02–18.67 4 18.67 25 10 65MZ 0.05–1.83 1.83 1.83 5 — 95MX 0.04–12 0.21 0.42 95 — 5RI 0.01–3.3 1.5 3.33 25 65 10TC 0.03–14.67 0.63 1 90 10 —VA 1.25–6 2.33 5.33 85 15 —
AC, amoxicillin; AZ, azithromycin; CI, ciprofloxacin; CL, chloramphenicol; CM, clindamcyin; DC,
doxycycline; EM, erythromycin; GM, gentamicin; I, intermediate; MIC, minimum inhibitory concen-
tration; MIC50, MIC for 50% of the strains; MIC90, MIC for 90% of the strains; MX, moxifloxacin; MZ,
metronidazole; PGL, benzylpenicillin; R, resistant; RI, rifampicin; S, susceptible; TC, tetracycline; VA,
vancomycin; XL, amoxicillin + clavulanate.
Clinical Research
In relation to the virulence factors of the E. faecalis isolates, acewas detected in 100% of the strains, asa in 60%, asa373 in 15%, esp in70%, efaA in 95%, and gelE in 75%, whereas the cylA gene was not de-tected. The results found for the virulence genes are listed in Table 4.
Table 4 also shows the raw data for virulence genes and the anti-microbial susceptibility of the E. faecalis strains investigated. Strainsshowing a high prevalence of virulence genes (5/7) are bold in thetable, showing intermediate or resistant resistance to azithromycin,ciprofloxacin, clindamycin, doxycycline, erythromycin, gentamicin,metronidazole, moxifloxacin, rifampicin, tetracycline, and vancomycin.Note that the isolate #13 was positive for almost all virulence genes
TABLE 4. Correlation between Positivity for the Virulence Genes and EnterococcuAntibiotics
Strain
Virulence genes
ace asa asa373 esp efaA gelE AC XL AZ
Isolate 1 + � � + + � S S IIsolate 2 + � � + + � I S SIsolate 3 + � � + + � S S IIsolate 4 + � � + + � S S SIsolate 5 + + � + + + S S SIsolate 6 + � � + + + S S SIsolate 7 + + � + + + S S SIsolate 8 + + � + + + S S SIsolate 9 + + � + + + S S IIsolate 10 + + � + + + S S IIsolate 11 + � � + + + S S SIsolate 12 + � � � + + S S SIsolate 13 + + + + + + S S SIsolate 14 + + + � + + S S SIsolate 15 + + � � + + S S SIsolate 16 + + � + � � S S SIsolate 17 + + + � + + S S SIsolate 18 + + � � + + S S SIsolate 19 + + � + + + S S SIsolate 20 + � � � + + S S S
+, positive;�, negative; AC, amoxicillin; AZ, azithromycin; CI, ciprofloxacin; CL, chloramphenicol; CM, clin
metronidazole; PGL, benzylpenicillin; R, resistant; RI, rifampicin; S, susceptible; TC, tetracycline; VA, vanc
1026 Barbosa-Ribeiro et al.
(6/7) and showed intermediate resistance to rifampicin and totalresistance to clindamycin, gentamicin, and metronidazole.
DiscussionAntimicrobial Susceptibility
E. faecalis is a gram-positive bacterium that has different mecha-nisms of virulence and resistance, which makes its eradication from theroot canals difficult. One of the objectives of this study was to evaluatethe susceptibility of E. faecalis strains against several antimicrobialagents in order to monitor their susceptibility/resistance over time.Gomes et al (6) monitored primary endodontic infections and foundthat some bacteria increased their resistance against the antibioticstested over time. Our study, involving E. faecalis isolates from second-ary/persistent endodontic infections, has also shown different profilesof susceptibility.
The E test, recommended by the CLSI, is a standard methodbroadly used in medical microbiology that is easy to use and interpret,in addition to being safe for testing antimicrobial susceptibility of bac-teria involved in endodontic infections (6, 8, 14–16). The CLSIperiodically revises and determines the standards for both testingand interpretation of the results, allowing the determination of theMIC for the tested strains. The method can also provide data forcomparison in longitudinal studies assessing changes in thebacterial susceptibility profiles over time (6, 8).
In the present work, amoxicillin + clavulanate was effective againstall tested isolates followed by amoxicillin and benzylpenicillin, whichwere effective against the majority of the strains. These results arecorroborated by other studies in the literature (1, 17, 18). However,the presence of enterococcal strains resistant to penicillin has beenreported in endodontic infections (19), which underlines the need toperform periodical susceptibility tests of these isolates.
Because of the predominance of E. faecalis in root-filled teeth withperiapical lesions, alternative drugs should be considered for prophy-laxis in individuals at risk for endocarditis during endodontic retreat-ment or with flare-up (20). In cases of patients allergic to penicillinand its derivatives, clindamycin is the antibiotic most commonly
s faecalis Strains that Showed Total or Intermediate Resistance to the Tested
Antibiotics
PGL CI CM CL DC EM GM MZ MX RI TC VA
S S R S S I R R S I S SS S S S S I S R S R I IS S R S S I R R S I S SI S R S S I I R S I S SS S R S S I R R S I S SS I R S S I R R S S S SS S S S S S I R R R S SS I R S S I R R S S S SS I R S S I R R S I S IS S I S S I S R S I S SS S S S S S S S S I S SS S S R S I S R S S S IS S R S S S R R S I S SS S R S I I R R S S I SS S R S S I R R S I S SS S S S S S R R S S S SS S R S S I R R S I S SS S R S S I R R S I S SS S I S S S S R S I S SS S S S S I R R S I S S
damcyin; DC, doxycycline; EM, erythromycin; GM, gentamicin; I, intermediate; MX, moxifloxacin; MZ,
omycin; XL, amoxicillin + clavulanate.
JOE — Volume 42, Number 7, July 2016

Clinical Research
prescribed. However, clindamycin is not an alternative drug to treat E.faecalis infections in patients allergic to penicillin and its derivatives.According to the CLSI, aminoglycosides (eg, gentamicin) (except athigh concentrations), cephalosporins, clindamycin, and trimetho-prim/sulfamethoxazole may appear active in vitro, but they are not clin-ically effective and should not be reported as sensitive. We found thatgentamicin and clindamycin were not effective against E. faecalis,thus agreeing with the findings of several authors (5, 20).We have found a high rate of resistance to clindamycin, genta-micin, and metronidazole and a lower rate of resistance to rifampicin,which was corroborated by Zhu et al (21) and Sun et al (22), despitesome discrepant results by other studies (13, 23). This fact may suggestthe development of resistance among these bacteria over the years (6).
With regard to both azithromycin and erythromycin, we havefound percentages of intermediate resistance of 25% and 75%,respectively, thus agreeing with the findings of Endo et al (2), whofound very similar values (33.3% and 75%, respectively). Pinheiroet al (20) reported that 14.2% and 28.5% of E. faecalis strainswere susceptible to azithromycin and erythromycin, respectively.Nevertheless, in the present study, none of the E. faecalis strainswere shown to be susceptible to both antibiotics. Emerging antibioticresistance in Enterococcus spp. has been shown in recent studies(24). Enterococci have acquired genetic determinants conferringintrinsic resistance to many classes of antimicrobials, including tetra-cycline, erythromycin, and chloramphenicol (4).
Chloramphenicol showed a good antimicrobial activity againstE. faecalis (95%), agreeing with the findings of other studies(25, 26) and showing that this antibiotic can be an alternative drugin cases in which the derivatives of penicillin failed.
Doxycycline, moxifloxacin, tetracycline, and vancomycin alsoshowed a good action against E. faecalis, which may suggest the useof these drugs as an alternative therapy. However, the use of these sub-stances should be undertaken with caution in order to avoid bacterialresistance development (20, 26).
As an alternative therapy for patients allergic to penicillin, someauthors (1, 2) suggested the use of moxifloxacin because they foundthat E. faecalis was susceptible to this antibiotic in 100% of the cases.However, our study has shown that there is already a change in thepattern of susceptibility over time because the susceptibility ratehad already dropped to 95% and one strain showed total resistanceto moxifloxacin. Moreover, our study indicates the use ofdoxycycline for patients allergic to penicillin because this antibioticshowed antimicrobial activity for 95% of the strains and only onestrain showed intermediate resistance.
In relation to the antibiotic therapy, an endodontic infectionmust be persistent or systemic to justify the need for antibiotics (ie,fever, swelling, lymphadenopathy, trismus, or malaise) in a healthypatient (27). Antibiotics are also more likely to be needed in animmunocompromised (28) patient or a patient in poor health. Theincreasing resistance to antimicrobial agents is a concern becauseit can have a negative effect on treatment effectiveness, thus increasingthe risk of super infections.
E. faecalis Virulence FactorsThis study has found distinct prevalence patterns of virulence
genes of Enterococcus spp. isolates from root canals of teeth with end-odontic treatment failure. The ace gene was detected in all clinicalisolates. Ace is an adhesin to collagen from E. faecalis expressed condi-tionally after growth in serum or in the presence of collagen. It is animportant factor for the establishment of these bacteria in the dentinof infected root canals (29).
JOE — Volume 42, Number 7, July 2016
The endocarditis antigen (efaA) is an important virulence gene ofE. faecalis. This gene was previously identified with the use of an anti-serum from a patient with E. faecalis endocarditis (30). The amino acidsequence of the associated protein, efaA, revealed a 55%–60% homol-ogy to a group of proteins known as streptococcal adhesins. Thus, it washypothesized that efaA might be an adhesin in the endocarditis. Theproduction of efaA by strains of E. faecalis is common. We have founda high prevalence of this gene (95%), which is in agreement with thefindings of Sedgley et al (13).
The GelE gene was detected in 75% of the E. faecalis strains, thusagreeing with the findings of Zhu et al (21). Gelatinase (gelE) is a hydro-phobic metalloproteinase with the capacity of cleaving insulin, casein,hemoglobin, collagen, gelatin, and fibrin. The expression of gelE washigher in biofilm-positive than in biofilm-negative strains (9, 31).
The asa (60%) and esp (70%) genes also had high prevalence inour study, corroborating other studies in the literature (13, 29).Aggregation substance (asa) is a pheromone-responsive plasmid-encoded bacterial adhesin that mediates efficient contact between donorand recipient bacterium, facilitating plasmid exchange. Asa was alsofound to mediate binding to extracellular matrix proteins, includingtype I collagen. Binding to type I collagen by bacteria may be of particularimportancewith respect to endodontic infections because this is themainorganic component of the dentin (21, 32). Asa373was identified in 15%of the isolates, which disagrees with the findings of Sedgley et al (13),who had not detected this gene. Asa373 differs from the classic asa inits protein structure and was reported to exhibit some moderatelyconserved amino acid motifs when its database sequence was comparedwith those of some other bacterial adhesins (33).
The enterococcal surface protein (esp) is encoded by the esp geneand may be involved in the colonization and persistence of E. faecalisduring infections (34). The enterococcal gene esp, which encodes thehigh–molecular-weight surface protein esp, has been detected in abun-dance among bacteremia and endocarditis isolates but is rare in stoolisolates from healthy individuals (35). It is likely that it mediates theprimary interaction of the pathogen with host surfaces during biofilmformation (31).
Finally, cytolysin (cylA) was not detected, which is in disagreementwith Sedgley et al (13), who identified these genes in 18% of the cases.CylA can induce tissue damage through lysis of erythrocytes anddestruction of host cells. Sedgley et al (13) found that 36% of the E. fae-calis endodontic strains are capable of producing hemolysin. The genesin the cyl operon encode cytolysin, where cylA is the only reading framenecessary for the expression of component A, a serine protease.
The different expression profiles of these virulence factors can beexplained by geographic differences, dietary habits, and infection stage(9, 13). This can be important for understanding the pathogenicity ofvirulence factors and their effects on the host.
It was concluded that E. faecalis isolates from persistent endodon-tic infections showed varied degrees of intermediate/total resistance toseveral antimicrobial agents, with amoxicillin + clavulanate being themost effective. The periodic evaluation of the susceptibility to antibioticsis an important practice for establishing the best drug if their use isnecessary. Moreover, the strains showed different patterns of virulencegenes of E. faecalis, and their monitoring should be encouraged inorder to elucidate changes in their resistance profiles.
AcknowledgmentsWe would like to thank Maicon R.Z. Passini, Augusto R. Lima,
Priscila A. Francisco, and Renata C. Pelegrini for their technicalsupport.
Resistance and Virulence of Enterococcus faecalis 1027

Clinical Research
Supported by grants from Research Support Foundation of theState of S~ao Paulo (FAPESP) (grant no. 2012/23697-4), NationalScientific and Technological Development Council (CNPq) (grantno. 308162/2014-5) and Coordination for Improvement of HigherEducation Personnel (CAPES).
The authors deny any conflicts of interest related to this study.
References1. Pinheiro ET, Gomes BP, Ferraz CC, et al. Evaluation of root canal microorganisms
isolated from teeth with endodontic failure and their antimicrobial susceptibility.Oral Microbiol Immunol 2003;18:100–3.
2. Endo MS, Signoretti FG, Kitayama VS, et al. Culture and molecular detection of frompatients with failure endodontic treatment and antimicrobial susceptibility of clinicalisolates. Enterococcus faecalis. Braz Dent Sci 2014;17:83–91.
3. Medeiros AW, Pereira RI, Oliveira DV, et al. Molecular detection of virulence factorsamong food and clinical Enterococcus faecalis strains in South Brazil. Braz JMicrobiol 2014;45:327–32.
4. Murray BE. The life and times of the Enterococcus. Clin Microbiol Rev 1990;3:46–65.
5. Morrison D, Woodford N, Cookson B. Enterococci as emerging pathogens ofhumans. Soc Appl Bacteriol Symp Ser 1997;83:89S–99.
6. Gomes BP, Jacinto RC, Montagner F, et al. Analysis of the antimicrobial susceptibilityof anaerobic bacteria isolated from endodontic infections in Brazil during a periodof nine years. J Endod 2011;37:1058–62.
7. Sanchez ML, Jones RN. E test, an antimicrobial susceptibility testing methodwith broad clinical and epidemiologic application. Antimicrob News Lett 1992;8:1–7.
8. Sousa EL, Gomes BP, Jacinto RC, et al. Microbiological profile and antimicrobialsusceptibility pattern of infected root canals associated with periapical abscesses.Eur J Clin Microbiol Infect Dis 2013;32:573–80.
9. Wang L, Dong M, Zheng J, et al. Relationship of biofilm formation and gelE geneexpression in Enterococcus faecalis recovered from root canals in patientsrequiring endodontic retreatment. J Endod 2011;37:631–6.
10. Martinho FC, Gomes BP. Quantification of endotoxins and cultivable bacteria in rootcanal infection before and after chemomechanical preparation with 2.5% sodiumhypochlorite. J Endod 2008;34:268–72.
11. M€oller AJ. Microbiological examination of root canals and periapical tissues ofhuman teeth. Methodological studies. Odontol Tidskr 1966;74(suppl):1–380.
12. Ribeiro AC, Matarazzo F, Faveri M, et al. Exploring bacterial diversity of endodonticmicrobiota by cloning and sequencing 16S rRNA. J Endod 2011;37:922–6.
13. Sedgley CM, Molander A, Flannagan SE, et al. Virulence, phenotype and genotypecharacteristics of endodontic Enterococcus spp. Oral Microbiol Immunol 2005;20:10–9.
14. Clinical and Laboratory Standards Institute. Performance Standards for Antimi-crobial Susceptibility Testing; Twenty-Third Informational Supplement. Wayne,PA: Clinical and Laboratory Standards Institute; 2013.
15. Jacinto RC, Montagner F, Signoretti FG, et al. Frequency, microbial interactions,and antimicrobial susceptibility of Fusobacterium nucleatum and Fusobacteriumnecrophorum isolated from primary endodontic infections. J Endod 2008;34:1451–6.
1028 Barbosa-Ribeiro et al.
16. Skucaite N, Peciuliene V, Vitkauskiene A, Machiulskiene V. Susceptibility of end-odontic pathogens to antibiotics in patients with symptomatic apical periodontitis.J Endod 2010;36:1611–6.
17. Lins RX, de Oliveira Andrade A, Hirata Junior R, et al. Antimicrobial resistance andvirulence traits of Enterococcus faecalis from primary endodontic infections.J Dent 2013;41:779–86.
18. Al-Ahmad A, Ameen H, Pelz K, et al. Antibiotic resistance and capacity for biofilmformation of different bacteria isolated from endodontic infections associatedwith root-filled teeth. J Endod 2014;40:223–30.
19. Heintz CE, Deblinger R, Oliet S. Antibiotic sensitivities of enterococci isolated fromtreated root canals. J Endod 1975;1:373–6.
20. Pinheiro ET, Gomes BP, Drucker DB, et al. Antimicrobial susceptibility of Entero-coccus faecalis isolated from canals of root filled teeth with periapical lesions. IntEndod J 2004;37:756–63.
21. Zhu X, Wang Q, Zhang C, et al. Prevalence, phenotype, and genotype of Entero-coccus faecalis isolated from saliva and root canals in patients with persistent apicalperiodontitis. J Endod 2010;36:1950–5.
22. Sun J, Sundsfjord A, Song X. Enterococcus faecalis from patients with chronic peri-odontitis: virulence and antimicrobial resistance traits and determinants. Eur J ClinMicrobiol Infect Dis 2012;31:267–72.
23. Rams TE, Feik D, Mortensen JE, et al. Antibiotic susceptibility of periodontal Entero-coccus faecalis. J Periodontol 2013;84:1026–33.
24. Coleri A, Cokmus C, Ozcan B, et al. Determination of antibiotic resistance and resis-tance plasmids of clinical Enterococcus species. J Gen Appl Microbiol 2004;50:213–9.
25. Sedgley CM, Lennan SL, Clewell DB. Prevalence, phenotype and genotype of oralenterococci. Oral Microbiol Immunol 2004;19:95–101.
26. Schwaiger K, Schmied EM, Bauer J. Comparative analysis on antibiotic resistancecharacteristics of Listeria spp. and Enterococcus spp. isolated from laying hensand eggs in conventional and organic keeping systems in Bavaria, Germany. Zoono-ses Public Health 2010;57:171–80.
27. Rodriguez-N�u~nez A, Cisneros-Cabello R, Velasco-Ortega E, et al. Antibiotic use bymembers of the Spanish Endodontic Society. J Endod 2009;35:1198–203.
28. Agence francaise de s�ecurit�e sanitaire des produits de sant�e AFSSAPS. Prescriptionof antibiotics for oral and dental care. Med Mal Infect 2012;42:193–202.
29. Hubble TS, Hatton JF, Nallapareddy SR, et al. Influence of Enterococcus faecalisproteases and the collagen-binding protein, Ace, on adhesion to dentin. Oral Micro-biol Immunol 2003;18:121–6.
30. Lowe AM, Lambert PA, Smith AW. Cloning of an Enterococcus faecalis endocarditisantigen: homology with adhesins from some oral streptococci. Infect Immun 1995;63:703–6.
31. Tendolkar PM, Baghdayan AS, Gilmore MS, Shankar N. Enterococcal surface pro-tein, Esp, enhances biofilm formation by Enterococcus faecalis. Infect Immun2004;72:6032–9.
32. Linde A, Goldberg M. Dentinogenesis. Crti Rev Oral Biol Med 1993;4:679–728.33. Kayaoglu G, Ørstavik D. Virulence factors of Enterococcus faecalis: relationship to
endodontic disease. Crit Rev Oral Biol Med 2004;15:308–20.34. Shankar N, Lockatell CV, Baghdayan AS, et al. Role of Enterococcus faecalis surface
protein Esp in the pathogenesis of ascending urinary tract infection. Infect Immun2001;69:4366–72.
35. Shankar V, Baghdayan AS, Huycke MM, et al. Infection-derived Enterococcus fae-calis strains are enriched in esp, a gene encoding a novel surface protein. InfectImmun 1999;67:193–200.
JOE — Volume 42, Number 7, July 2016