Embed Size (px)
Citation preview

Antiphospholipid syndrome associated with progressive fibrosing alveolitis 233
Antiphospholipid syndrome in a patient withrapidly progressive fibrosing alveolitis
Andrew D Kelion, John R Cockcroft, James M Ritter
Department ofClinicalPharmacology,UMDS, Guy'sHospital, London SEl9RT, UKAD KelionJR CockcroftJM Ritter
Correspondence toProfessor JM Ritter,Department of ClinicalPharmacology, UMDS,Medical School Building,Guy's Hospital, London SEI9RT, UK
Accepted 27 October 1994
SummaryThe antiphospholipid syndrome is athrombotic disorder which can occur in aprimary form or more classically insystemic lupus erythematosus. Anassociation between cryptogenic fibros-ing alveolitis and the antiphospholipidsyndrome has not previously beenreported. We describe a patient withsevere cryptogenic fibrosing alveolitiswho developed pulmonary embolism andmyocardial infarction in the presence ofantiphospholipid antibody. The case alsoillustrates that worsening respiratoryfunction may represent superimpositionof one lung pathology on another, andmay not simply be a deterioration of thepre-existing disease.
Keywords: antiphospholipid syndrome, fibrosingalveolitis
Introduction
The antiphospholipid syndrome is a disorderinvolving both arterial and venous thrombosisin association with antibodies directed againstphospholipids. It was first described in patientswith systemic lupus erythematosus (SLE),'subsequently in lupus variants such as discoidlupus and Sjogren's syndrome, and more rarelyin rheumatoid arthritis and primary vasculitis.2It has not, however, been described in associa-tion with cryptogenic fibrosing alveolitis. Thefollowing case demonstrates such an associa-tion in a patient whose worsening dyspnoea wasdue to one life-threatening aetiology superim-posed on another.
Case report
A 58-year-old woman was admitted to hospitalwith a six-week history ofprogressive dyspnoeaand a non-productive cough for two weeks. Shehad been fit and well in the past, except forpossible tuberculosis in childhood. There wasno history of skin or joint problems, or recur-rent abortions. She was a lifelong nonsmokerand was the landlady of a pub. She kept twodogs and a cat, but no birds.She had pronounced flushing ofthe face with
no other skin changes. There was finger club-bing. She was apyrexial with a heart rate of 90beats/min and a blood pressure of 160/
80 mmHg. The jugular venous pressure wasnot elevated. She had a right ventricular heave,a loud pulmonary component of the secondheart sound, and an ejection systolic murmur atthe lower left sternal edge, findings consistentwith pulmonary hypertension. There were fineinspiratory crackles over both lower tubes.The chest radiograph showed severe inters-
titial shadowing over most of the left lung field,with lesser basal shadowing on the right.Arterial blood gases with the patient breathingair were P02 9.2 kPa, pCO2 5.2 kPa, pH 7.45. Aventilation-perfusion lung scintigram did notsuggest pulmonary embolism (figure).Serology revealed the presence of antinuclearantibody in both IgG and IgM forms at a titreof 1/160; this gave a diffuse homogeneousstaining pattern. Anti-double-stranded DNAantibody and other immunological markers forSLE and other connective tissue diseases werenot detected. Antiphospholipid antibody wasalso present in the IgG form at a titre of26 units(moderately positive; Lupus ResearchLaboratory, St Thomas's Hospital, London);lupus anticoagulant was not detected. Bron-choscopy was unremarkable, as was the resultof broncheoalveolar lavage. Lung functiontests revealed a restrictive defect: FEVy 1.0-1.1(predicted 1.9-2.7), FVC 1.1 (2.3-3.1), FEVy1.0/FVC 100% KCO 1.2 (1.5-2.5).A diagnosis of cryptogenic fibrosing
alveolitis was made. She was commenced onprednisolone 60 mg and improved dramaticallywithin 48 hours. She was discharged on areducing course of prednisolone. Six weekslater she was readmitted to hospital with atwo-day history of worsening dyspnoea. Shewas by now taking 10 mg prednisolone daily.On examination she was very distressed andcyanosed. She was apyrexial, with a heart rateof 120 beats/min, a blood pressure of 160/80 mmHg, and a respiratory rate of 60 breaths/min.The chest radiograph on admission showed
dense reticular shadowing in both lower zones.The arterial blood gases with the patientbreathing 100% oxygen were P02 6.2 kPa,PCO2 5.7 kPa, pH 7.26, bicarbonate 19 mmol/l,oxygen saturation 76%. The electrocardio-graph (ECG) was unremarkable. Renal func-tion was normal. Routine haematology was asfollows: haemoglobin 15.0 g/dl, white cellcount 19.0 x 109/1 (neutrophil leucocytosis),platelet count 157 x 109/1. Clotting times wereall within the normal range, as were levels of
on Decem
ber 26, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.71.834.233 on 1 A
pril 1995. Dow
nloaded from

Kelion, Cockcroft, Ritter
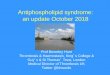
Figure Ventilation perfusion lung scans. At initial presentation, ventilation (a) and perfusion (b) scans werematched whereas subsequently there were un-matched defects in the perfusion scan (d) compared with theventilation scan (c). All views were right posterior oblique.
antithrombin 3, protein C, and protein S. Theerythrocyte sedimentation rate was 32 mm/h,and the C-reactive protein titre was 2.9 mg/dl(normal range < 1 mg/dl).The pulse oximeter reading on high-flow
oxygen remained 75-80% at rest, but droppeddramatically on the slightest exertion. In-creased doses of steroid were administeredintravenously (methylprednisolone 500 mgdaily), and intravenous cefotaxime and oralerythromycin were given for a possiblecommunity-acquired pneumonia. A ventila-tion-perfusion lung scintigram was per-formed. This showed widespread segmentaland subsegmental perfusion defects in bothlung fields, with a normal ventilation scan:these appearances were strongly suggestive ofpulmonary embolism (figure). She was treatedwith intravenous heparin.
She became progressively more exhausted,and by the 5th hospital day had a temperatureof 380C and an oxygen saturation of 68%. Theplatelet count had fallen to 64 x 109/1. TheECG now showed changes characteristic of anacute inferior myocardial infarction. She wasintubated and ventilated in the intensive careunit. The next day an open lung biopsy wasperformed to obtain an histological diagnosis as
her lung function was too poor to allow bron-choscopic biopsy (PO2 13 kPa, pCO2 14 kPaand pH 6.90 on pressure control ventilationwith an inspired oxygen concentration of70%). Anticoagulation with heparin proveddifficult to control, and postoperativelybleeding occurred from the chest drain. Theactivated partial thromboplastin time wasfound to be 148 s (normal range 29-39 s), andintravenous epoprostenol was substituted forheparin. Histology of the lung biopsy showedextensive interstitial fibrosis, consistent withfibrosing alveolitis, with superimposedpneumonic changes. Blood cultures wererepeatedly negative, as was serology foratypical organisms. Intravenous cyclophos-phamide was added to the methylprednisolone.
She remained in deep coma despite thewithdrawal of sedation. CT scan of the brainshowed a massive intracerebral haemorrhageinto the right parietal lobe with severe midlineshift and herniation of the cerebellar tonsilsthrough the foramen magnum. Shedeteriorated rapidly and died.Post-mortem examination confirmed mas-
sive right intracerebral haemorrhage that wasfelt to be the immediate cause of death. Thelungs were both firm and solid with confluent
234 on D
ecember 26, 2021 by guest. P
rotected by copyright.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.71.834.233 on 1 April 1995. D
ownloaded from

Antiphospholipid syndrome associated with progressive fibrosing alveolitis 235
Table Diseases associated with antiphospholipid antibodies
Rheumatological Haematological Other
Systemic lupus erythematosus Autoimmune haemolytic anaemia and Liver diseaseDiscoid lupus thrombocytopaenic purpura Endocrine disorders -Rheumatoid arthritis Lymphomas and leukaemias hypothyroidism & Addison's diseaseVasculitis Waldenstrom's macroglobulinaemia Drugs - oral contraceptives, drug-inducedSystemic sclerosis, polymyositis, lupus
'overlap syndromes' Ulcerative colitisJuvenile chronic arthritisSjogren's syndromePsoriatic arthropathyRaynaud's phenomenaBehqet's diseaseAcute rheumatic fever
whitish nodules. Histology showed interstitialfibrosis with a superimposed acute purulentbronchopneumonia; no organisms were seenwith several special stains. There wasperipheral segmental thromboembolism in theright lung, with bilateral deep vein thrombosisin the calves and thighs. There was a recentposterolateral subendocardial myocardialinfarction, with minimal coronaryatheromatous disease. No vasculitic processwas evident in any of the tissues studied. Thesefindings confirmed the diagnosis of rapidlyprogressive cryptogenic fibrosing alveolitisassociated with thromboembolic disease, in thepresence of the antiphospholid antibody. Cur-rent criteria for the classification of theantiphospholipid syndrome require positivityfor antiphospholipid antibodies to beconfirmed on two occasions, six to eight weeksapart.3 However, in this case the patient diedbefore a second estimation of antiphospholipidantibodies could be made and unfortunately nostored serum was available to allow for post-mortem determination.
Discussion
The antiphospholipid syndrome can present ina variety of ways depending on the artery orvein affected by thrombosis. Deep venousthrombosis, recurrent pulmonary embolism,and myocardial infarction, all of which occur-red in the patient described above, are commonmodes of presentation.There was no evidence of pulmonary
embolism at the original presentation, and thedevelopment of multiple pulmonary emboliprobably led to the rapid clinical deterioration
and the final admission. Although the his-tological findings suggested a pneumonic pro-cess superimposed on the fibrosing alveolitis,special stains failed to reveal any causativemicroorganism and repeated cultures werenegative. The myocardial infarction may haveprecipitated admission to the intensive careunit. Even without these thrombotic insults,our patient's long-term prognosis would havebeen very poor given the severity of her under-lying lung pathology.The ultimate cause of death was a massive
intracerebral bleed. Interestingly, the lupusanticoagulant in association with false positivesyphilis serology (the original marker forantiphospholipid antibody) was first describedin two SLE patients with a bleeding disorderand a prolonged prothrombin time.4 Subse-quently it has become clear that thrombosis andnot haemorrhage is by far the more importanteffect of the antiphospholipid antibody.'The antiphospholipid syndrome is classical-
ly associated with SLE and lupus variants, andhas rarely been described in rheumatoidarthritis and vasculitis (table). Our patient hadhistologically proven fibrosing alveolitis, butno features of SLE. Antinuclear antibody is anon-specific serological marker, and itspresence is well described in cryptogenicfibrosing alveolitis, occurring in 21-42% ofcases.5'6 To our knowledge, this is the firstreport of an association between cryptogenicfibrosing alveolitis and the antiphospholipidsyndrome.
We gratefully acknowledge the help of Dr SuRamachandra, Senior Registrar in Histopathology.
1 Bowie EJW, Thompson JH Jr, Pascuzzi CA, Owen CA Jr.Thrombosis in systemic lupus erythematosus despite cir-culating anticoagulants. J Lab Clin Med 1963; 62: 416-30.
2 Hughes GRV. The antiphospholipid syndrome: ten yearson. Lancet 1993; 342: 341-4.
3 Harris EN. Syndrome of the black swan. Br J Rheumatol1987; 26: 324-5.
4 Conley CL, Hartmann RC. A haemorrhagic disorder causedby circulating anticoagulant in patients with disseminatedlupus erythematosus. J Clin Invest 1952; 31: 621-2.
5 Chapman JR, Charles PJ, Venables PJ, et al. Definition andclinical relevance of antibodies to nuclear ribonucleoproteinand other nuclear antigens in patients with cryptogenicfibrosing alveolitis. Am Rev Respir Dis 1984; 130: 439-43.
6 Holgate ST, Haslam P, Turner-Warwick M. Thesignificance of antinuclear and anti-DNA antibodies incryptogenic fibrosing alveolitis. Thorax 1983; 38: 67-70.
on Decem
ber 26, 2021 by guest. Protected by copyright.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.71.834.233 on 1 A
pril 1995. Dow
nloaded from