Embed Size (px)
Citation preview
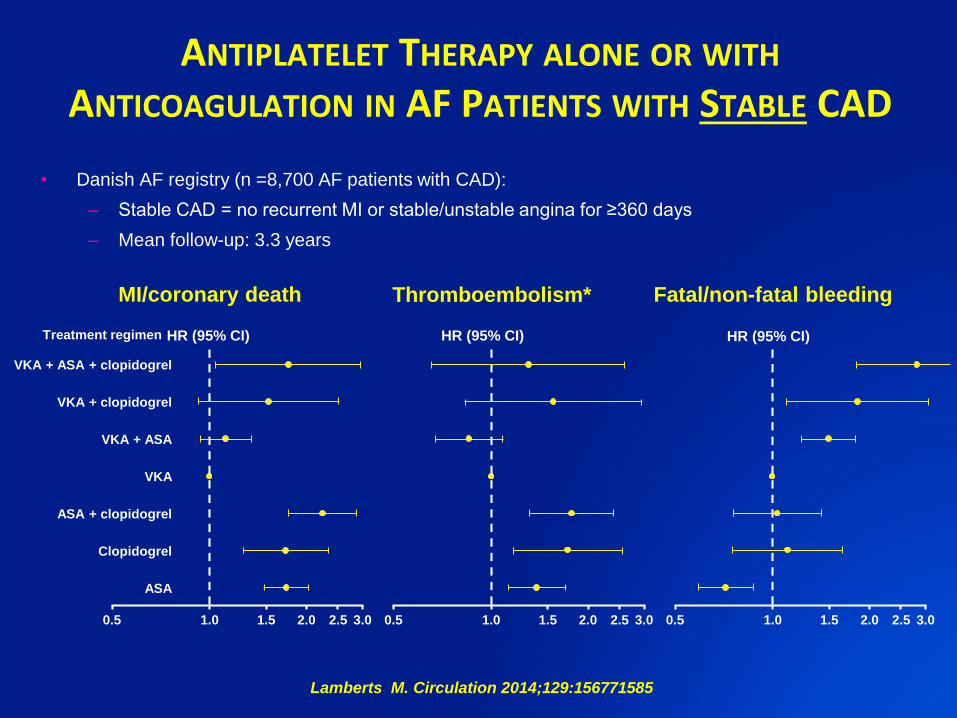
ANTIPLATELET THERAPY ALONE OR WITH
ANTICOAGULATION IN AF PATIENTS WITH STABLE CAD
• Danish AF registry (n =8,700 AF patients with CAD):
– Stable CAD = no recurrent MI or stable/unstable angina for ≥360 days
– Mean follow-up: 3.3 years
MI/coronary death Thromboembolism* Fatal/non-fatal bleeding
HR (95% CI) HR (95% CI) HR (95% CI)
0.5 1.0 1.5 2.0 2.5 3.0 0.5 1.0 1.5 2.0 2.5 3.00.5 1.0 1.5 2.0 2.5 3.0
VKA + ASA + clopidogrel
VKA + clopidogrel
VKA + ASA
VKA
ASA + clopidogrel
Clopidogrel
ASA
Treatment regimen
Lamberts M. Circulation 2014;129:156771585
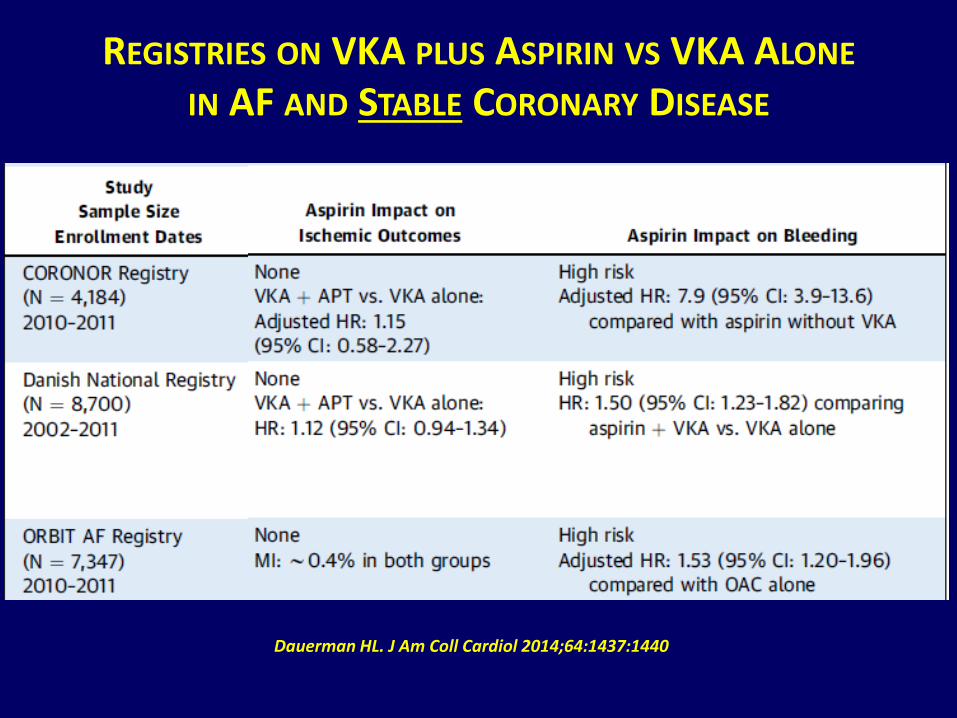
REGISTRIES ON VKA PLUS ASPIRIN VS VKA ALONE
IN AF AND STABLE CORONARY DISEASE
Dauerman HL. J Am Coll Cardiol 2014;64:1437:1440
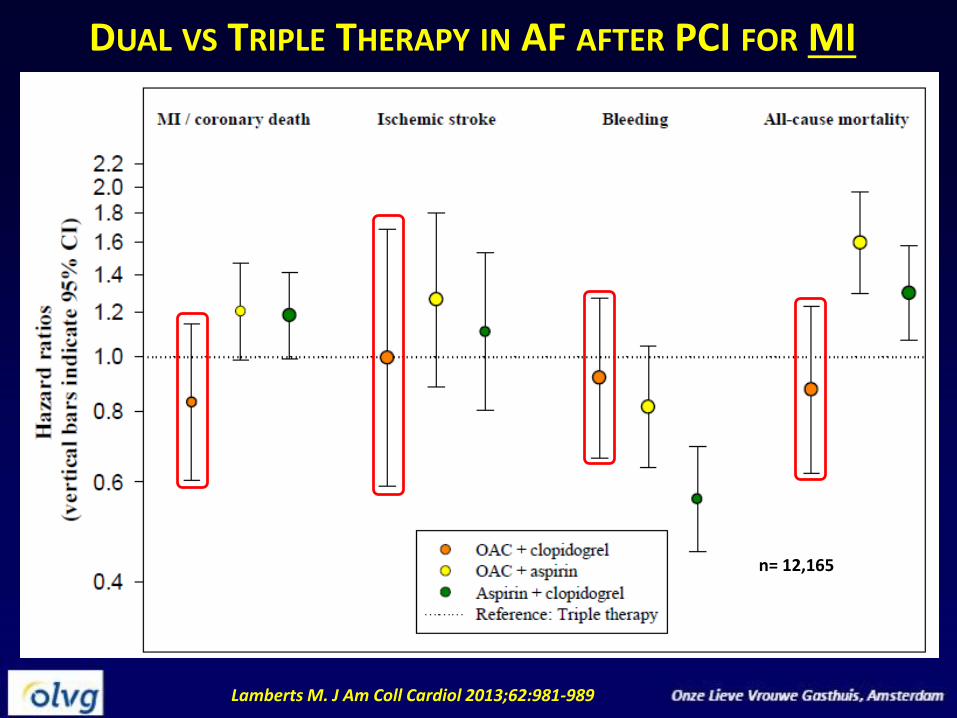
DUAL VS TRIPLE THERAPY IN AF AFTER PCI FOR MI
Lamberts M. J Am Coll Cardiol 2013;62:981-989
n= 12,165
|
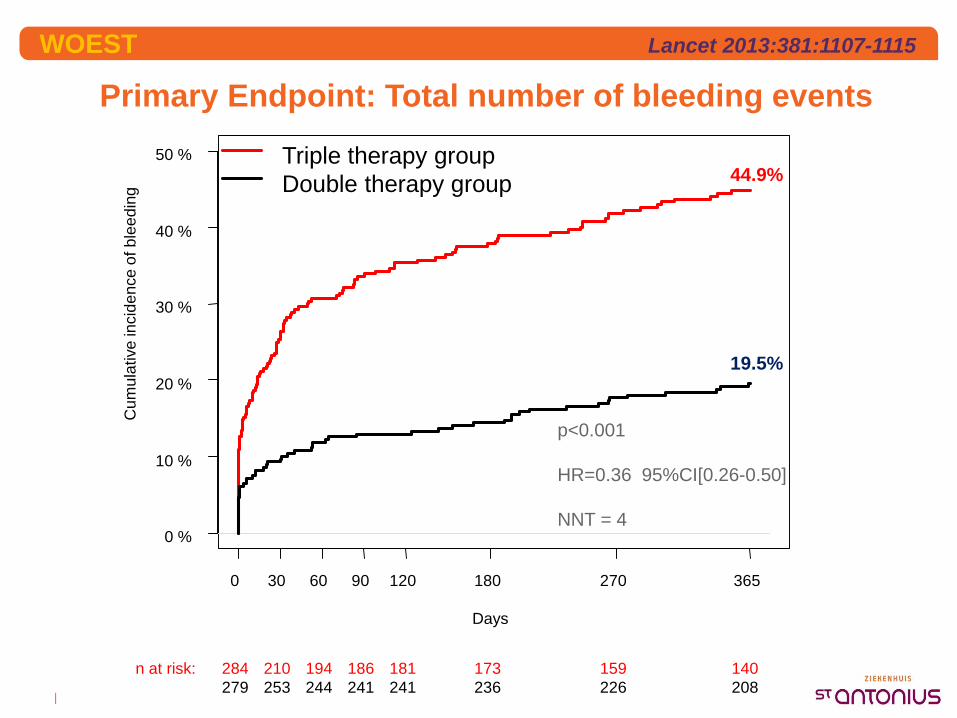
Primary Endpoint: Total number of bleeding events
WOEST
Days
Cum
ula
tive
incid
en
ce o
f b
lee
din
g
0 30 60 90 120 180 270 365
0 %
10 %
20 %
30 %
40 %
50 %
284 210 194 186 181 173 159 140n at risk:
279 253 244 241 241 236 226 208
Triple therapy group
Double therapy group 44.9%
19.5%
p<0.001
HR=0.36 95%CI[0.26-0.50]
NNT = 4
Lancet 2013:381:1107-1115
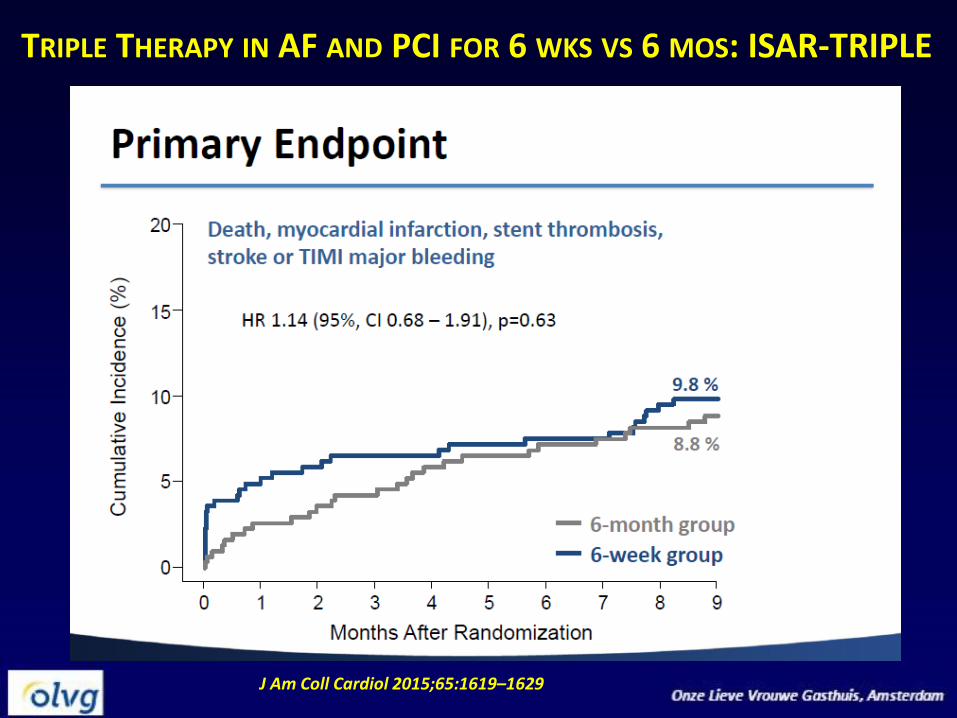
J Am Coll Cardiol 2015;65:1619–1629
TRIPLE THERAPY IN AF AND PCI FOR 6 WKS VS 6 MOS: ISAR-TRIPLE
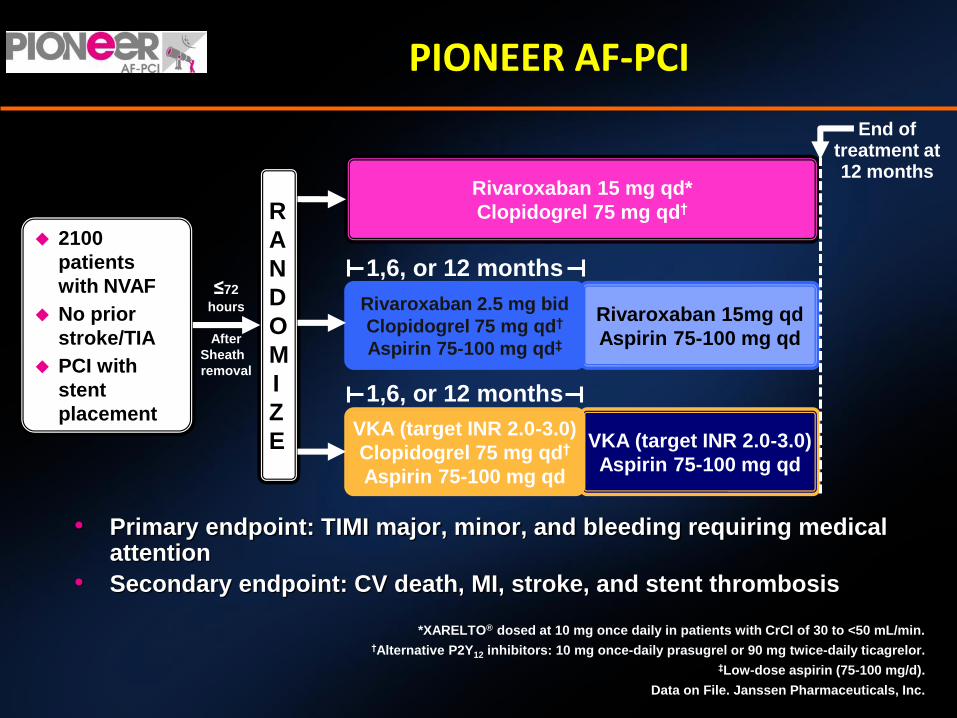
PIONEER AF-PCI
• Primary endpoint: TIMI major, minor, and bleeding requiring medical attention
• Secondary endpoint: CV death, MI, stroke, and stent thrombosis
*XARELTO® dosed at 10 mg once daily in patients with CrCl of 30 to <50 mL/min.
†Alternative P2Y12 inhibitors: 10 mg once-daily prasugrel or 90 mg twice-daily ticagrelor.
‡Low-dose aspirin (75-100 mg/d).
Data on File. Janssen Pharmaceuticals, Inc.
2100
patients
with NVAF
No prior
stroke/TIA
PCI with
stent
placement
R
A
N
D
O
M
I
Z
E
1,6, or 12 months
Rivaroxaban 15 mg qd*
Clopidogrel 75 mg qd†
Rivaroxaban 15mg qd
Aspirin 75-100 mg qd
Rivaroxaban 2.5 mg bid
Clopidogrel 75 mg qd†
Aspirin 75-100 mg qd‡
VKA (target INR 2.0-3.0)
Aspirin 75-100 mg qd
VKA (target INR 2.0-3.0)
Clopidogrel 75 mg qd†
Aspirin 75-100 mg qd
≤72
hours
After
Sheath
removal
1,6, or 12 months
End oftreatment at12 months
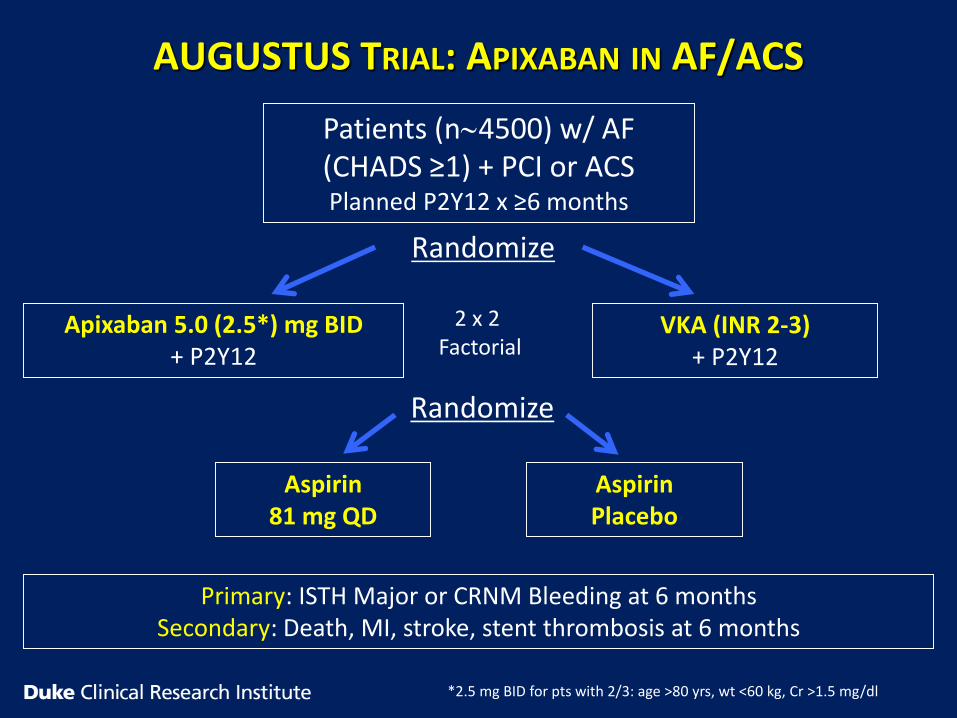
AUGUSTUS TRIAL: APIXABAN IN AF/ACS
Patients (n4500) w/ AF (CHADS ≥1) + PCI or ACSPlanned P2Y12 x ≥6 months
Apixaban 5.0 (2.5*) mg BID+ P2Y12
VKA (INR 2-3)+ P2Y12
Randomize
Randomize
Aspirin81 mg QD
AspirinPlacebo
Primary: ISTH Major or CRNM Bleeding at 6 monthsSecondary: Death, MI, stroke, stent thrombosis at 6 months
2 x 2 Factorial
*2.5 mg BID for pts with 2/3: age >80 yrs, wt <60 kg, Cr >1.5 mg/dl