Embed Size (px)
Citation preview

ANTIPSYCHOTIC PRESCRIBING GUIDELINES DECEMBER 2018
This policy supersedes all previous versions of guidelines for antipsychotic prescribing

1 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Policy title The Trust Antipsychotic Prescribing Guidelines
Policy reference
PHA35
Policy category
Clinical
Relevant to All clinical staff who deal with medication in the Trust.
Date published
January 2019
Implementation date
January 2019
Date last reviewed
December 2018
Next review date
December 2021
Policy lead Lucy Reeves, Chief Pharmacist
Contact details Email: [email protected]
Accountable director
Vincent Kirchner, Medical Director
Approved by: Drugs and Therapeutic Committee December 2018
Ratified by: Quality Committee January 2019
Document history
Date Version Summary of amendments
March 2012 1 New Guidelines
January 2014 2 Revision
May 2016 3 Further guidance and clarifications
January 2019 4 HDAT and valproate guidance updated
Membership of the policy development/ review team
Audrey Coker, Lead Pharmacist for Clinical Services.
Consultation Dr Antonio Metastasio, Consultant Psychiatrist, Dr Sujata Soni, Consultant Psychiatrist, Dr Stella Kingett, Consultant Psychiatrist, Dr Laurine Hanna, Consultant Psychiatrist, David Rogalski, Lead Pharmacist, Krishna Amin, Lead Pharmacist, Lucy Reeves, Chief Pharmacist, Members of the Drugs and Therapeutics Committee
DO NOT AMEND THIS DOCUMENT
Further copies of this document can be found on the Foundation Trust intranet.

2 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Contents Page
1 Introduction 4
2 Aims and objectives 4
3 Scope of the policy 4
4 Key points 4
5 Patients at risk of developing psychosis 7
6 Schizophrenia / Psychosis 7
7 Depot antipsychotic medication 14
8 Management of treatment-resistant schizophrenia 16
9 Co-morbid physical conditions 24
10 Cardiovascular disease 24
11 Co-morbid diabetes 25
12 Weight gain 25
13 Dyslipidaemia 25
14 Extrapyramidal side effects 26
15 Neuroleptic malignant syndrome 27
16 Hyperprolatinaemia 27
17 Venous thromboembolism 28
18 Pregnancy and breastfeeding 29
19 Antipsychotics in bipolar affective disorder 29
20 Treatment resistant depression or psychotic depression 30
21 Catatonia 33
22 Older adults (>65years) 33
23 Learning disabilities 34
24 Substance misuse 37
25 Smoking cessation 37
26 Associated documents 37
27 Dissemination and implementation arrangements 37
28 Training requirements 38
29 Monitoring and audit arrangements 38

3 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
30 Review of the policy 39
31 References 39
32 Appendices 43
Appendix 1: Suggestions for switching antipsychotic because of poor tolerability Appendix 2: Antipsychotic depot injections – suggested doses and frequencies Appendix 3: High dose antipsychotic therapy form Appendix 4: Choice of medication in specific medical condition Appendix 5: Risk factors for QT prolongation Appendix 6: Medicines interactions Appendix 7: Positive cardiometabolic health resource. Lester UK adaptation 2014.

4 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
1 Introduction
These guidelines have been developed to provide clinical staff with clear guidance on
prescribing antipsychotics to ensure safe effective care of patients in line with current NICE
and national good practice guidance and trust formulary. These guidelines apply to the
treatment of patients under the care of the Trust. When prescribing is transferred to primary
care, the GP should take responsibility for monitoring relevant physical health parameters
associated with antipsychotic prescribing. Good communication between the specialist and
GP in such cases is essential for the safe and effective management of patients.
2 Aims and objectives
To ensure quality and cost-effective prescribing of all antipsychotics in order to provide
optimal antipsychotic therapy.
3 Scope of the policy
This policy relates to antipsychotic prescribing in patients with a diagnosis of schizophrenia,
bipolar affective disorder or depression, patients with learning disabilities or with the
substance misuse service.
4 Key points
Table 1: Antipsychotic of choice
The Drugs and Therapeutics Committee of Camden and Islington NHS Foundation Trust
recommends that the oral antipsychotic risperidone be considered as the first-line antipsychotic in all
patients diagnosed with schizophrenia, bipolar disorder and as an adjunct in treatment resistant
depression. It is a widely used, well-established medicine that is known to be equally effective to
other antipsychotics and is relatively low priced.
First choice for treatment with depot medication should be a first-generation antipsychotic depot
injection such as zuclopenthixol decanoate or flupentixol decanoate.
For patients with learning disabilities, see the appropriate section or contact the pharmacy for advice.
4.1.1 In patients with schizophrenia, studies have shown that there is no clear advantage of second-generation antipsychotics over first-generation antipsychotics in effectiveness, safety or cost1,2. Second-generation antipsychotics may have a lower propensity for extrapyramidal side-effects, but this is offset by a higher propensity for metabolic side effects3.
4.1.2 In patients with treatment-resistant schizophrenia, clozapine is significantly more effective than other second-generation antipsychotics in reducing symptoms4.
4.1.3 It is recommended that the choice of antipsychotic is based on5,6.
Patient preference for a particular antipsychotic medication.
Patient’s clinical presentation.
General medical/physical health disorders.

5 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Concurrent medicines.
Antipsychotic side effect profile.
Patient’s past experience of the individual antipsychotic medicines in terms of clinical
response and side-effects.
Level of medication adherence.
Cost-effectiveness.
Long-term treatment plan.
4.1.4 For patients with a diagnosis of psychosis, treatment with antipsychotic medication should be considered an explicit individual therapeutic trial. A trial of the medication at optimum dosage should be for 4–6 weeks5.
4.1.5 Patients must be given information on treatment options and medication at the point of prescribing. Patient information leaflets (PILs) are accessible on the ‘Choice and Medication’ website via the trust intranet or website. The provision of information should be recorded in electronic patient records.
4.1.6 The choice of antipsychotic medication should be made by the patient and healthcare professional together, taking into account the views of the carer if the patient agrees. The indications and expected benefits and risks of oral antipsychotic medication, and the expected time for a change in symptoms and appearance of side effects should be discussed5. The possible side effects of each medicine should be discussed, including:
o metabolic (including weight gain and diabetes). o extrapyramidal (including akathisia, dyskinesia and dystonia). o cardiovascular (including prolonging the QT interval). o hormonal (including increasing plasma prolactin). o other (including unpleasant subjective experiences5.
The side effects that the person is most willing to tolerate should be recorded5.
4.1.7 Before starting antipsychotic medication, the following baseline investigations should be recorded (see appendix 7)5.
4.1.8 Before starting antipsychotic medication, patients with psychosis or schizophrenia should be offered an electrocardiogram (ECG) if:
o specified in the summary of product characteristics (SPC). o a physical examination has identified specific cardiovascular risk (such as
diagnosis of high blood pressure). Patients should be offered a physical examination and baseline investigations before initiating an antipsychotic. Inability to carry this out e.g. patient refusal should be documented in the notes. On-going physical health monitoring should be carried out and abnormal results responded to appropriately, communicated to the GP and documented in the notes.
o there is a personal history of cardiovascular disease or o an inpatient5.

6 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
4.1.9 Use the intervention framework (Lester UK adaptation) for monitoring physical health (appendix 7).
4.1.10 It is recognised it is not always possible to conduct an ECG before starting an antipsychotic. Inability to conduct an ECG e.g. patient refusal should be documented in the notes.
4.1.11 At the start of treatment, a dose at the lower end of the licensed range should be prescribed and slowly titrated within the licensed dose range. Reasons for dosages outside the licensed dose range should be recorded. The rationale for continuing, changing or stopping antipsychotics and effects should be recorded5.
4.1.12 The justification for dosages outside the range given in the BNF should be documented in the clinical records. Refer to the trust policy for the use of high dose antipsychotic medication for further details and specifications7.
4.1.13 The secondary care team should maintain responsibility for monitoring patients' physical health and the effects of antipsychotic medication until the person's condition has stabilised and prescribing is transferred to primary care. In practice-based teams, this should be done in collaboration with the GP.
4.1.14 Non-prescribed therapies the patient wishes to use (including complementary therapies), alcohol, tobacco, prescription and non-prescription medicines should be discussed with the patient, and carer if appropriate, including the safety and efficacy of the therapies, and possible interference with the therapeutic effects of prescribed medication and psychological treatments5.
4.1.15 If 'as required' (p.r.n.) prescriptions of antipsychotic medication is prescribed the following should be carried out- review of clinical indications, frequency of administration, therapeutic benefits and side effects each week or as appropriate. Check whether 'p.r.n.' prescriptions have led to a cumulative dosage above the maximum specified in the BNF or SPC5.
4.1.16 Initial loading doses (rapid neuroleptisation) should not be used5. For the management of acutely disturbed behaviour, refer to the trust policy for rapid tranquillisation7.
4.1.17 Regular combined antipsychotic medication should not be prescribed routinely except for short periods when switching from one antipsychotic to another5.
4.1.18 Anticholinergic agents should not be routinely prescribed prophylactically with antipsychotic medication. Their use for emergent extrapyramidal problems responsive to such medication (e.g. parkinsonism and acute dystonia) should be determined on an individual basis taking into account factors such as the patient’s history of extrapyramidal side effects and the risk of anticholinergic side-effects. Anticholinergic medicines cause side effects e.g. dry mouth constipation, urinary disturbances and cause central adverse effects (e.g. cognitive impairment, worsening of tardive dyskinesia and delirum8.
4.1.19 Regular review of the medication regime should address the following and be documented in the patient records:
Therapeutic efficacy.
Side-effects.

7 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Medication adherence.
Physical health.
Need to continue, change, or stop the medication and the implications of the
decision taken.
4.1.20 When adherence with oral antipsychotic medication is unreliable, liquids or orodispersible tablets facilitate monitoring of ingestion. However, liquids and orodispersible tablets should not be routinely used and must be stopped when patients are discharged from hospital or teams providing supervised administration (e.g. crisis teams/assertive outreach teams/early intervention service). They are only useful as treatment interventions if effectively supervised on a daily basis. Alternatively these formulations may be appropriate for use in patients with swallowing difficulties.
4.1.21 First choice for treatment with depot medication should be a first-generation antipsychotic depot injection such as zuclopenthixol decanoate or flupentixol decanoate.
5 Patients at risk of developing psychosis
5.1.1 People considered to be at increased risk of developing psychosis should not be offered antipsychotic medication (as described or with the aim of decreasing the risk of or preventing psychosis)5.
5.1.2 A first presentation of sustained psychotic symptoms in primary care should not be initiated with antipsychotic medication unless it is done in consultation with a consultant psychiatrist5.
6 Schizophrenia / Psychosis
6.1 First episode psychosis (FEP)
6.1.1 NICE5 recommends that the choice of first-line antipsychotic should be made by the patient and healthcare professional together. This decision should take into account the evidence for relative liability for side-effects particularly considering common and serious side-effects such as extrapyramidal motor symptoms and metabolic problems, individual patient risk factors for side-effects, relevant medical history and individual patient preference6. Patient information leaflets (PILs) comparing medication treatment options can be accessed via the Choice and Medication link on the trust intranet.
6.1.2 The Drugs and Therapeutics Committee of Camden and Islington NHS Foundation Trust approved risperidone as the first-line oral antipsychotic choice in all patients diagnosed with schizophrenia.
6.1.3 The choice of antipsychotic must also take into account factors listed under ‘key points’.
6.1.4 There is evidence that first-episode psychosis responds to lower doses of antipsychotic medication than those required for the treatment of established schizophrenia6,9,10,11 (refer to the Maudsley Guidelines). First episode patients are more likely to experience problematic side effects than patients with a history of receiving antipsychotics6. The results of subsequent symptom and side-effect

8 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
reviews should be documented in the clinical records with the rationale for continuation or any change in medication.
6.1.5 The dose should be slowly titrated upwards, if indicated, to the optimal range for that medicine, and not exceeding the maximum licensed BNF dose5.
6.1.6 An individual trial of the antipsychotic of choice should be conducted. The aim is to achieve an adequate trial, optimum dosage with good adherence for four to six weeks5,6.
6.1.7 If the first line antipsychotic is poorly tolerated or ineffective, at an appropriate dose for an appropriate duration:
Review the diagnosis5.
Assess medicine adherence (including adequate dose and duration) and the reasons
for non-adherence e.g. adverse effects5.
Consider confounding factors (e.g. substance misuse, co-morbid conditions, other
prescribed medicines). A urine drug screen can be carried out to test for recent
substance use. An accurate history of substance and alcohol misuse should be
elucidated wherever possible5.
Underlying organic illness.
Current psychosocial stresses perpetuating the illness
6.1.8 Treatment options include:
Increase the antipsychotic dose (within licensed dose range).
Change to another antipsychotic (if the first antipsychotic was a typical, consider
changing to an atypical) following a discussion with the patient and/or carer.
Suggestions for switching antipsychotics because of poor tolerability are listed in
appendix 1.
6.1.9 For patients with psychosis, the following should be recorded regularly and systematically throughout treatment, but especially during titration: response to treatment, including changes in symptoms and behaviour side effects of treatment, taking into account overlap between certain side effects and clinical features of schizophrenia (for example, the overlap between akathisia and agitation or anxiety) and impact on functioning the emergence of movement disorders weight (the GASS tools in the electronic patient records)5.

9 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
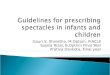
6.1.10 Figure 1: First-episode psychosis: treatment algorithm3,5
Agree choice of antipsychotic with patient and/or carer. If not possible start second-generation antipsychotic. Consider risperidone as first-line
in patients newly-diagnosed with schizophrenia.
Titrate if necessary to minimum-effective dose (see Maudsley Guidelines)
Adjust dose according to response and tolerability (ensuring adherence)
Assess over 4-6 weeks
Poor adherence related to poor tolerability -
discuss with patient and change medication. If
poor adherence related to other factors,
consider early use of
depot
Continue at dose established as
effective
Change medicine and follow the
above process. Consider use of either a second generation or
first generation antipsychotic
Clozapine
Effective
ective
Not effective Not tolerated/
poor adherence
Not effective
Period of assessment - 4-6 weeks as per NICE guidelines. Early use
of clozapine much more likely than anything else to be successful.

10 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
6.2 Figure 2: Relapse or acute exacerbation of schizophrenia: treatment algorithim
6.2.1 Patients where treatment adherence is doubtful or known to be poor:3
Investigate reasons for poor adherence
If lack of insight consider:
undertaking a medication attitude questionnaire and discussing the patient’s beliefs and the provision of PILs.
the use of a depot
If due to disorganisation:
simplify medication regime
reduce anticholinergic load
consider use of adherence aids - see trust medicines policy.
consider a depot
If due to poor tolerability, discuss with patient and carer
and consider switching to a more acceptable
antipsychotic.

11 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
6.2.2 Figure 3: Patients who are adherent to treatment3:
Identify any social or psychosocial precipitants.
Provide appropriate support/therapy.
Continue usual antipsychotic treatment at optimal
dose (and adequate duration).
If acute treatment required: Add a short-term sedative or
Review medication history.
Switch to alternative acceptable antipsychotic if appropriate.
Discuss choice with patient and/or carer.
Assess over at least 6 weeks.
If ineffective, switch to clozapine.
If clozapine monotherapy is ineffective, consider augmentation strategies.
If clozapine is not an option, consider alternative options listed in current Maudsley prescribing
guidelines.

12 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
6.3 Maintaining response and relapse-prevention in schizophrenia: pharmacotherapy3,5,6,12,13
6.3.1 Antipsychotics should be continued for one to two years following a first episode of psychosis5,6. Patients should be informed there is a high risk of relapse if they stop medication over the next one to two years5. There should be at least five years of maintenance treatment for chronic patients with multiple episodes of illness3.
6.3.2 Review antipsychotic medication annually, including observed benefits and any side effects5.
6.3.3 Doses that are acutely effective should be continued as prophylaxis. However after a first episode, careful dose reduction is supportable3.
6.3.4 Patients need to be informed of the recognised risks of discontinuing medicines early and they (and their carers) should be educated to understand the early warning signs if there is a relapse in the psychosis.
6.3.5 Clinical features which may be associated with a lower risk of relapse or which suggest that relapse may be easier to manage if it does occur:
Prodormal brief or absent.
Short duration of untreated psychosis (e.g. only a few weeks).
Severe psychosocial stressors precipitating the first episode psychosis.
Absence of first rank symptoms of schizophrenia.
High level of functioning before illness.
Late onset e.g. after 25 years.
Good insight and awareness of warning signs.
Has been willing to accept treatment voluntarily when acutely ill.
Stable social circumstances.

13 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
6.3.6 When deciding on a switch of antipsychotic medication, account should be taken of the risk of destabilisation of the illness and provocation of adverse effects. The care plan should address reversible risk factors for relapse such as comorbid substance misuse, poor adherence and critical environment.
6.3.7 Any reduction in dosage should be cautious and closely monitored given the increased risk of relapse. The method of switching e.g. cross-tapering or stopping the original antipsychotic first may vary depending on individual circumstance13. Contact the pharmacy for advice.
6.3.8 The risk of relapse may result in patients continuing on antipsychotics indefinitely.
6.3.9 An intermittent targeted treatment approach should not be used routinely as an alternative to continuous antipsychotic maintenance. NICE recommends that this be considered only for patients (with schizophrenia or psychosis) who will not accept continuous maintenance treatment or if it is contraindicated e.g. side effect sensitivity5.
6.3.10 Depot antipsychotics should be considered if patients prefer this after an acute episode or if avoiding covert non-adherence to medication is a clinical priority5.
6.4 Withdrawal of treatment
6.4.1 If the patient has remained symptom free and a withdrawal of the antipsychotic is considered the following factors should be considered:
Is the patient is symptom-free and if so for how long? Long-standing, non-distressing symptoms which have not previously been responsive to medication be excluded3.
What is the severity of adverse effects3?
What was the previous pattern of illness (including speed of onset, duration and severity of episodes and danger posed to self and others3.
Has dosage reduction been attempted before and if so what was the outcome3?
What are the patient’s current social circumstances? Is it a period of relative stability or are stressful life events anticipate3.
What is the social cost of relapse3.
Is the patient/carer able to monitor symptoms and if so will they seek helpful3.
If withdrawing antipsychotic medication, this should be undertaken gradually and the patients regularly monitored for signs and symptoms of relapse5.
6.4.2 After withdrawal from antipsychotic medication, continue monitoring for signs and symptoms of relapse for at least 2 years5.
6.4.3 Patients, carers and key workers should be aware of the early signs of relapse and how to access help. Targeted treatment would be much less effective than continuous prophylaxis. Those with a history of aggressive behaviour or serious suicide attempts and those with residual psychotic symptoms should be considered for life-long treatment3.

14 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
6.5 Management of relapses
6.5.1For people with an acute exacerbation or recurrence of psychosis or schizophrenia oral
antipsychotic medication should be offered or existing medication reviewed5. 6.5.2 The choice of medicine should be influenced by the same criteria recommended for
starting treatment. Take into account the clinical response and side effects of the service user's current and previous medication5.
6.6 Behaviour that challenges 6.6.1 See the Trust rapid tranquillisation guidelines.
7 Depot antipsychotic medication
TABLE 2: DEPOT ANTIPSYCHOTIC OF CHOICE:
First choice for treatment with depot medication should be a first-generation long-acting antipsychotic depot injection such as zuclopenthixol decanoate or flupentixol decanoate.
Risperidone long-acting injection should only be used in patients with intolerable side-
effects to first-generation depot injections.
Paliperidone monthly depot is reserved for the treatment of adults with schizophrenia and patients with documented tolerability to risperidone. It requires a non-formulary form signed by the consultant and approval for use by a Lead Pharmacist.
Paliperidone 3 monthly depot is reserved for the treatment of adults with schizophrenia and patients with documented tolerability to risperidone and who have received paliperidone monthly depot for four months. It requires a non-formulary form signed by the consultant and approval for use by the Chief Pharmacist or Medical Director.
Aripiprazole depot is reserved for the treatment of adults with schizophrenia and patients with a documented tolerability and response to aripiprazole. It requires a non-formulary form signed by the consultant and approval for use by a Lead Pharmacist.
Olanzapine depot is not approved for use due to clinical safety issues and post-administration monitoring requirements making it impractical to use. It requires a non-formulary form signed by the inpatient and community consultants and approval for use by the Chief Pharmacist or Medical Director.
7.1 When initiating depot antipsychotic medication:
7.1.1 The service user's preferences and attitudes towards the mode of administration (regular intramuscular injections) and organisational procedures (for example, home visits and location of clinics) should be taken into account. To assess the risks and benefits of the medicine regimen a small test dose as set out in the BNF or SPC should initially be used5.
7.1.2 Consider offering depot antipsychotic medication to people with psychosis or schizophrenia:
who would prefer such treatment after an acute episode.
where avoiding covert non-adherence (either intentional or unintentional) to antipsychotic medication is a clinical priority within the treatment plan5.
7.1.3 Administration of depot formulations has been demonstrated to prevent relapse in patients in whom adherence to medication is suboptimal. However, depot injections of first-generation antipsychotics may give rise to a higher incidence of extrapyramidal reactions than oral preparations; extrapyramidal side-effects

15 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
(EPSEs) occur less frequently with second-generation antipsychotic depot preparations. Risperidone, aripiprazole (restricted use only) and paliperidone (restricted use only) depot injections are currently the only available atypical depots approved for use in the trust and are considerably more expensive than typical antipsychotic depot (see appendix 2).
7.1.4 Depot antipsychotics are administered by deep intramuscular injection at intervals of 1 to 4 weeks. When initiating therapy with sustained-release preparations of first-generation antipsychotics, patients should first be given a small test-dose to assess sensitivity to EPSEs and to reveal any sensitivity to the base oil (see appendix 2)3. In general, not more than 2–3 ml of oily injection should be administered at any one site; correct injection technique (including the use of z-track technique) and rotation of injection sites are essential (refer to the trust Depot antipsychotic medication: guidelines for prescribing and administering on the intranet). If the dose needs to be reduced to alleviate side-effects, it is important to recognise that the plasma concentration may not fall for some time after reducing the dose, therefore it may be a month or longer before side-effects subside14.
7.1.5 There is no evidence to suggest that shortening the dose interval improves efficacy. Moreover, injections are painful, so less frequent administration is desirable3.
7.1.6 There is a delay in achieving the peak plasma level, therapeutic effect and steady-state plasma level with depot injections. Doses may be reduced if adverse effects occur, but should only be increased after careful assessment over at least 1 month. The use of adjunctive oral medication to assess depot requirements may be helpful, but it too is complicated by the slow emergence of antipsychotic effects. At the start of therapy, plasma levels of antipsychotic released from a depot increase over several weeks to months without increasing the given dose. Dose increases during this time to steady-state plasma levels are thus unnecessary3.
7.1.7 There is no clear-cut division in the use of the typical antipsychotics, but zuclopenthixol may be suitable for the treatment of agitated or aggressive patients whereas flupentixol can cause over-excitement in such patients. Zuclopenthixol decanoate may be more effective in preventing relapses than other conventional antipsychotic depot preparations5, 14. Although the incidence of extrapyramidal reactions is similar for the conventional antipsychotics3,14, fluphenazine has relatively more EPSEs, but perhaps less weight gain3.
7.1.8 Only patients who suffer intolerable side-effects (extrapyramidal side effects, tardive dyskinesia) with first-generation depot injections, and are unlikely to be adherent with oral atypical medication, should be considered for risperidone long-acting injection.
7.1.9 Patients who are responding well and are not experiencing any intolerable side-effects from first-generation depot injections should not be transferred to long-acting atypical antipsychotic injections.
7.1.10 Risperidone long-acting injection is administered every two weeks into the gluteal or deltoid site. It should not be given at different time intervals. Oral risperidone should be given prior to starting the injection to assess tolerability and response. Patients stabilised on 4mg per day or less of oral risperidone should start on 25mg of the long acting injection. A starting dose of 37.5mg may be considered in patients maintained on higher oral doses. Oral antipsychotic therapy should be continued for at least three weeks after the first injection of risperidone. Oral antipsychotic is sometimes required for longer (6-8 weeks)15. Part vials of risperidone long-acting injection cannot be used (as it is a suspension).

16 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
7.1.11 Paliperidone palmitate is the prolonged-release suspension for injection for the maintenance treatment of schizophrenia in patients that have a documented response and tolerability to risperidone. It is restricted in the formulary. Compared to risperidone long-acting injection, paliperidone depot does not need refrigerating, is given monthly rather than fortnightly, into either gluteal or deltoid muscles. It may be used without prior stabilisation with oral treatment16. There is no evidence to suggest paliperidone palmitate offers any clinical advantage compared to risperidone injection in terms of efficacy or safety17.
7.1.12 Patients on risperidone injection should not routinely be switched to paliperidone palmitate. This may be appropriate in individual cases where there is a response to risperidone, but significant adherence issues affecting the frequency of administration. Paliperidone palmitate is potentially useful in a limited group of patients who have responded to risperidone but are unable to continue with risperidone treatment. As paliperidone is renally excreted, it is an option for patients with hepatic impairment who have previously responded to risperidone18 and for patients requiring risperidone injection of greater than 50mg every two weeks (unlicensed dosage)3.
7.1.13 Paliperidone three monthly depot is indicated for the maintenance treatment of schizophrenia in adult patients who are clinically stable on 1-monthly paliperidone palmitate injectable product, preferably for four months or more. It is restricted in the formulary48.
7.1.14 Aripipazole depot is a second generation antipsychotic depot indicated for maintenance treatment of schizophrenia in adult patients stabilised with oral aripiprazole19.
7.1.15 Olanzapine embonate is another second-generation antipsychotic depot indicated for maintenance-treatment in schizophrenia. It is non-formulary within the trust. Olanzapine depot injection has the disadvantage that patients need to be observed in a healthcare facility by appropriately qualified personnel for at least three hours after each dose to check for 'post-injection syndrome’ which has signs and symptoms consistent with olanzapine overdose (sedation and/or delirium)20. For this reason, the clinical suitability for this medicine in the community is likely to be severely limited. As with oral olanzapine, weight gain and metabolic effects (raised serum cholesterol, triglyceride and glucose levels) are common.
7.1.16 Refer to appendix 2 for suggested doses and frequencies of antipsychotic depot injections.
8 Management of treatment-resistant schizophrenia (TRS)
Table 3: Antipsychotic of choice in treatment resistant schizophrenia
Clozapine is considered the first-line antipsychotic in patients diagnosed with treatment resistant schizophrenia.
8.1 Treatment resistant schizophrenia
8.1.1 Treatment-resistant schizophrenia is defined as a lack of satisfactory clinical improvement despite the use of adequate doses of at least two different antipsychotic agents, including an atypical antipsychotic agent prescribed for adequate duration (4-6 weeks).1 There is evidence that long-term treatment resistance may develop within

17 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
the first two years of illness if psychosis remains untreated. Treatment should be initiated as soon as possible after a diagnosis of psychosis has been made12.
8.1.2 For people who do not respond adequately to pharmacological or psychological intervention:
Review the diagnosis.
Establish that there has been adherence to antipsychotic medication, prescribed at
an adequate dose and for an adequate duration.
Review engagement with and use of psychological treatments and ensure that these
have been offered.
Consider other causes of non-response e.g. co-morbid substance misuse, concurrent
prescribed medication or physical illness5.
8.1.3 A distinction should be made between treatment resistance and treatment intolerance. For treatment resistant patients, they should be offered a trial of clozapine at the earliest opportunity. Treatment intolerance could be described as experiencing adverse effects to such a degree that continuation with treatment is unwarranted. However this does not mean the patient is treatment resistant. Side effect burden can be assessed using the Clozapine GASS tool located under the ‘Medication’ tab in the electronic patient record. In such circumstances, an alternative antipsychotic other than clozapine can be offered22.
8.1.4 Clozapine should be introduced at the earliest opportunity in patients with evidence of treatment resistant schizophrenia. Clozapine is restricted due to its adverse side effect profile. It is licensed for use in treatment resistant schizophrenia and for psychotic disorders occurring during Parkinson’s disease where standard treatment has failed14. It is also licensed for patients with a diagnosis of schizophrenia who have severe, untreatable neurological adverse reactions to other antipsychotic agents, including atypical antipsychotics23.
8.1.5 Clozapine should be offered to people with schizophrenia whose illness has not responded adequately to treatment despite the sequential use of adequate doses of at least 2 different antipsychotic medicines. At least 1 of the medicines should be a non-clozapine second-generation antipsychotic5.
8.1.6 Prior to initiating clozapine, the patient, consultant and pharmacist must be registered with the clozapine patient monitoring service. A baseline full blood count (FBC), is required prior to registration of the patient and prescribing clozapine. Baseline Us & Es, LFTs, lipids, glucose and an ECG are also recommended. Regular FBC (white blood cells, neutrophils and platelets) monitoring is mandatory while taking clozapine. Blood samples are rated in a traffic light system (green, amber, red) and are at a defined frequency (weekly, fortnightly, monthly) depending on the length of treatment (refer to the specification of product characteristics)23.
8.1.7 For an adequate trial, clozapine monotherapy should be prescribed for 3-6 months6. Clozapine serum levels may guide dosage and check adherence where there is suboptimal response or side effects are problematic6.
8.1.8 For people with schizophrenia whose illness has not responded adequately to clozapine at an optimised dose, healthcare professionals should consider point 8.1.2

18 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
(including measuring therapeutic serum levels) before adding a second antipsychotic to augment treatment with clozapine5.
8.2 Augmentation
8.2.1 Augmentation strategies should only be considered after optimised clozapine treatment has been administered for a period of at least than 3 to 6 months. An adequate trial of augmentation may need up to 8 -10 weeks5,6. Below is a table (Table 4) of augmentation options including non-antipsychotics from the Maudsley Prescribing Guidelines3. A medicine that does not compound the common side effects of clozapine should be chosen5.
8.2.2
Table 4: Suggested options for augmenting clozapine3.
Amisulpride 400-800mg/day
Some evidence and experience suggests it may be worthwhile (two small RCTs, one of which found an increased adverse‐effect burden). May allow clozapine dose reduction.
Aripiprazole 15-30mg/day
A meta‐analysis suggests some effect. Improves metabolic parameters.
Haloperidol 2mg/day Modest evidence of benefit.
Lamotrigine 25-300mg May be useful in partial and non-responders. A meta-analysis suggests moderate effect size.
Risperidone 2-6mg/day Supported by a randomised controlled trial, but there are two negative RCTs each with miniscule response rates. Small number of reports of increases in clozapine plasma levels.
Sulpiride 400mg/day May be beneficial in partial and non-responders. Supported by a randomised controlled trial (RCT).
8.2.2 An adequate trial of augmentation may require 8-10 weeks. Various other adjunctive treatments have been tried in treatment resistant schizophrenia. There is lack of persuasive evidence for efficacy from RCTs which share several limitations. These include lithium, valproate and lamotrigine6. The British Association of Psychopharmacology (BAP) guidelines conclusions are in Table 5.
Table 5: BAP conclusions on the efficacy of augmentation treatment.6
Adjunctive Treatment Conclusion
Lithium Lithium as an adjunctive treatment to antipsychotic may only be worth considering for patients with schizophrenia who exhibit affective symptoms.
Sodium Valproate Valproate has a role in the prophylaxis of clozapine induced seizures.
Lamotrigine A systemic review of five studies including clozapine treated patients concluded there was an advantage for lamotrigine augmentation of clozapine over placebo for both positive and negative symptoms.
8.2.3 Also see the trust clozapine treatment guidelines on the trust intranet.

19 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
8.3 Alternatives to clozapine in the treatment of treatment resistant schizophrenia
8.3.1 Where clozapine cannot be used because of adverse events or patient refusal, other medicines or medicine combinations may be tried, but outcomes are generally poorer. Options are listed in a current copy of the Maudsley prescribing guidelines. Some of these options, if not included in the Trust formulary will require a non-formulary approval. Further advice can be obtained from the Pharmacy department.
8.4 High dose antipsychotic therapy (HDAT)
8.4.1 High dose antipsychotic therapy is defined as a total daily dose of a single antipsychotic which exceeds the upper limit stated in the specification of product characteristics or BNF with respect to the age of the patient and the indication being treated or a total daily dose of two or more antipsychotics which exceeds the SPC or BNF maximum using the percentage method. The percentage method requires converting the dose of each medicine into a percentage of the BNF maximum recommended dose for that medicine and adding these together. A cumulative dose of more than 100% is a high dose24.
8.4.2 There is no evidence that high-dose antipsychotic use is beneficial for patients with first-episode psychosis and such use should be avoided. Antipsychotic polypharmacy should be avoided. ‘Top-up’ oral antipsychotic doses for patients on depot/long-acting injections should be used only as a short-term measure. Where antipsychotic response is poor, switching medication should be the preferred course of action, rather than increasing doses above BNF limits. A short-term benzodiazepine prescription could be preferable for the sedation of patients with aggression at this early stage of the illness24.
8.4.3 There is no justification in the published literature for high-dose antipsychotics in the treatment of persistent aggression. Regular and frequent review of treatment plans in relevant clinical settings might allow for the safe and appropriate use of antipsychotic medication without any increase in violence. When prescribing medication to target the medium or long term risk of violence, the clinician should bear in mind the limited evidence and only prescribe medication after a thorough multidisciplinary assessment, risk-benefit evaluation and careful review of effects and side effects. Continuing adherence of prescribed medication is important in the long-term reduction of aggressive behaviour. Of the available antipsychotic medication, clozapine has the best evidence base for reducing the risk of violence in people with schizophrenia in the long-term24.
8.4.4 In treatment resistant schizophrenia, before resorting to a high dose evidence based strategies should be exhausted, including optimised use of clozapine. If a high dose antipsychotic treatment regimen is initiated, this should be as a limited therapeutic trial, with the dosage returned to conventional levels after a three month period unless the clinical benefits evidently outweighing risks24.
8.4.5 Clinicians should be aware prescribing high doses of antipsychotics might worsen already compromised cognitive function in their patients (particularly older people). High dose antipsychotics have a greater liability for extrapyramidal side effects for which anticholinergic/anti-Parkinsonism medicines might be required which may worsen cognitive function24.
8.4.6 Resistance by the clinical team to a reduction in dose might be due to concerns regarding the risk of the patient causing harm to self or others. These concerns need

20 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
to be balanced against the risk of harm to the patient’s health by adverse effects of high doses and lack of clinical benefits. In the absence of evidence, a gradual stepwise dose reduction to the maximum licensed dose over a period of time with monitoring for emergent adverse effects would seem a sensible strategy. A subsequent reduction to the minimum effective dose should also be considered. Ideally other prescribing changes that were scheduled to occur at the same time should be minimised in order to assist identification of the casual agent for emergent adverse effects or clinical benefits24.
8.4.7 Doses of antipsychotics prescribed above the maximum licensed dosages are off-label. Refer to the ‘Unlicensed Medicines and Unlicensed Use of Licensed Medicines (Off-Label) policy.
8.4.8 Dose-related side effects include extrapyramidal side effects, tachycardia, postural hypotension, sedation, seizures and hyperprolactinamia24. For the management of cardiac side effects, see section 10. For management of extrapyramidal side effects, see section 14. For management of neuroleptic malignant syndrome, see section 15. For management of hyperprolactinaemia, see section 16.
8.4.9 The use of antipsychotic medicines with more pronounced effects on cardiac repolarisation can only be justified if the medicine has specific advantages for the patient in comparison with antipsychotic medicines with less marked cardiac risks. High doses and medicine combinations should only be used when there is a clinical justification, particularly if the combination might result in a medicine interaction or additive ECG effects24.
8.4.10 Before using high doses, ensure that:
Sufficient time has been allowed for response.
At least two different antipsychotics have been tried sequentially.
Clozapine has failed or not tolerated due to agranulocytosis or other serious adverse effect. Most other side effects can be managed. Some patients may refuse clozapine outright.
Adherence is not in doubt (use of blood tests, liquids, dispersible tablets, depot preparations).
Adjunctive medicines such as antidepressants or mood stabilisers are not indicated.
Psychological approaches have been tried or are not appropriate3.
The decision to use high doses should:
Be made by a senior psychiatrist.
Involve the multidisciplinary team.
Be done if possible with the patient’s informed consent3.
Process
Rule out contraindications (ECG abnormalities, hepatic impairment). Undertake a physical examination.
Assess for cardiovascular disease.
Enquiry into the family history of sudden death.
Consider and minimise any risks posed by concomitant medication e.g. potential to cause QTc prolongation, electrolyte disturbance or pharmacokinetic interactions.
Document the decision to prescribe high doses in the clinical notes along with a description of target symptoms. The use of an appropriate rating scale is advised.

21 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Adequate time for response should be allowed after each dosage increment before a further increase is made3,24.
Monitoring
Physical monitoring should be carried out as outlined in appendices 8 and 9.
All patients on high doses should have regular ECGs (baseline, when steady state serum levels have been reached after each dosage increment and then every 6 to 12 months). Additional biochemical/ECG monitoring is advised if medicines that are known to cause electrolyte disturbances or QTc prolongation are subsequently co-prescribed.
Target symptoms should be assessed after six weeks to three months. If insufficient improvement in these symptoms has occurred, the dose should be decreased to the normal range3.
8.4.11 The following tables are the monitoring high dose antipsychotic monitoring guidelines for three different circumstances. The HDAT form under the ‘Medication’ tab in electronic patient records must be completed. Also see appendix 3.
Table 6: Regular long-term high dose antipsychotic therapy:
Parameters Pre-treatment Dose change Long-term
ECG and QTc interval
Baseline Repeat a week after escalation
Repeat once every 3 months or more frequently if clinically indicated.
U & Es and LFTs
Baseline Monitor regularly if abnormal results, according to clinical need.
Repeat once at 3 months or more frequently if clinically indicated.
Vital signs (BP, pulse and temperature
Baseline Repeat Recheck every 3 months or more frequently if clinically indicated.
Care plan On commencement
Review at MDT Review every 3 months or more frequently if clinically indicated.
As per trust high dose antipsychotic therapy form, physical observations should be documented in the NEWs chart. HDAT should be reduced if there is no clear observable effect.
If possible the patient and/or carers should be informed about the high dose treatment. A patient information leaflet (Choice and Medication link, handy factsheet: high doses of antipsychotics) should be offered from the trust intranet. Patients should be asked to report side effects they think they may experience.

22 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Table 7: High dose antipsychotic therapy during cross-titration
Parameters Pre-treatment Dose change
ECG and QTc interval Baseline Repeat a week after a dose increase.
U & Es and LFTs Baseline Monitor regularly if abnormal results, according to clinical need.
Vital signs (BP, pulse and temperature
Baseline Repeat at review of ECG results (after dose increase) and after completing HDAT.
Care plan On commencement Review at MDT.
Adapted from the trust high dose antipsychotic therapy form. Physical observations should be documented in the NEWs chart.
If possible the patient and/or carers should be informed about the high dose treatment. A patient information leaflet (Choice and Medication link, handy factsheet: high doses of antipsychotics) should be offered from the trust intranet. Patients should be asked to report side effects they think they may experience.
Table 8: High dose antipsychotic therapy as a result of as required or rapid
tranquillisation medication
Parameters Pre-treatment Post administration of as required or rapid tranquillisation medication
ECG and QTc interval Baseline Repeat a few days after dose increase
U & Es and LFTs Baseline Monitor regularly if abnormal results, according to clinical need.
Vital signs (BP, pulse and temperature
Monitor as rapid tranquillisation guidance when the medication was given by the oral or the IM route.
RT: follow the rapid tranquillisation monitoring guidance
Care plan On commencement Review
Physical observations should be documented in the NEWs chart.
If possible the patient and/or carers should be informed about the high dose treatment. A patient information leaflet (Choice and Medication link, handy factsheet: high doses of antipsychotics) should be offered from the trust intranet. Patients should be asked to report side effects they think they may experience.
8.4.12 If a patient is discharged from an inpatient unit on HDAT, then the patient’s GP and other relevant community mental health personnel must be informed by the discharging doctor of the HDAT status and the required monitoring/review arrangements.

23 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
9 Co-morbid physical conditions
If a person has rapid or excessive weight gain, abnormal lipid levels or problems with blood glucose management, offer interventions in line with relevant NICE guidelines5. Use the intervention framework (Lester UK adaptation) for monitoring physical health (appendix 7). A quick reference guide to choice of medication in specific medical conditions is listed in appendix 4 and should be read in conjunction with NICE guidance5 and the Maudsley prescribing guidelines3. It is not an exhaustive list. With complex cases it is advisable to refer to, or consult with, relevant specialists and/or obtain the most up-to-date advice. The information should be interpreted in light of the patient’s clinical presentation, previous response to treatment(s), risk of relapse, patient preference medical co-morbidities and potential medicines interactions. For additional guidance on physical health monitoring refer to appendix 7. In each condition, discuss with the patient the risks and benefits of treatment and document clearly in notes the reasons for choice of antipsychotic. Avoid polypharmacy, start with a low dose, monitor closely and increase dose slowly only after careful assessment.
10 Cardiovascular disease
Some antipsychotics are linked to prolongation of the cardiac QT interval, a risk
factor for the ventricular arrhythmia torsade de pointes, which is often fatal. ECG
monitoring is essential for all patients prescribed antipsychotics3. Overall risk is
probably dose-related3. Medicine interactions (involving enzyme inhibition) are
important. Commonly used metabolic inhibitors include fluvoxamine, fluoxetine,
paroxetine and valproate. Guidance on risk factors and the effect of antipsychotics on
the QT interval is outlined in the Maudsley prescribing guidelines3. Also refer to the
specifications of product characteristics for further information and contact the
pharmacy department if further advice is required.
It is good practice to get an ECG prior to initiating an antipsychotic. There may be
occasions an ECG cannot be done prior to initiating an antipsychotic and will be done
at a later date. Patients can be sent to the ECG clinic at the acute trust. An ECG prior
to and ECG monitoring during antipsychotic therapy is important in the following
situations3:
High risk antipsychotic medicines are contemplated e.g. haloperidol or pimozide or
combined antipsychotics (within a week of reaching therapeutic dose3,24.
High dose or short-acting parenteral antipsychotic medicine therapy is to be used in
an elderly patient or a patient with a history of cardiovascular disease. Urea and
electrolytes should also be checked (particularly plasma potassium) especially in
patients at higher risk of electrolyte abnormalities (e.g. patients with anorexia
nervosa, liver disease, diuretic use or dehydration). ECGs should be perfomed every
few days following initiation of high dose treatment or during a period of dose
escalation until it is judged that steady state concentrations have been reached.
Thereafter ECG and electrolyte assessment is recommended every few months, at
times of acute illness, when potentially interacting medicines are introduced or the
patient experiences symptoms that could be due to arrhythmia, for example syncope
or fits24.

24 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
High doses of antipsychotics should be avoided in rapid tranquillisation (particularly
parenterally)24
Table 9: Management of QT prolongation in patients receiving antipsychotic medicines3.
QTc Action Refer to cardiologist
<440msec (men) or <470msec (women)
None unless abnormal T-wave morphology
Consider if in doubt
>440msec (men) or > 470msec (women), but < 50msec
Consider reducing dose or switching to a medicine of lower effect; repeat ECG
Consider
>500msec Repeat ECG. Stop suspected causative medicine(s) and switch to a medicine of lower effect
Immediately
Abnormal T-wave morphology
Review treatment. Consider reducing dose or switching to a medicine of lower effect.
Immediately
Correct electrolyte disturbances (potassium and magnesium) if present
See appendix 5 for the effect and quantifying risks of different antipsychotics on QTc
interval (low effect, moderate effect, high effect, unknown effect, no known effect).
In the absence of conclusive data, assume all antipsychotics are linked to sudden cardiac death. The lowest dose possible should be prescribed and polypharmacy/metabolic interactions avoided3. An ECG should be undertaken on admission and if there is previous abnormality or additional risk factor at yearly check-up. Moderate/high risk antipsychotic:- consider an ECG a week after reaching a therapeutic dose3.
11 Co-morbid diabetes
Olanzapine and clozapine has a high risk of causing impaired glucose tolerance and diabetes, quetiapine, risperidone and phenothiazines a moderate risk, and haloperidol low risk. Antipsychotics with minimal effects are aripiprazole, amisulpride, asenapine and lurasidone3. See appendix 1.
12 Weight gain
Olanzapine has the greater propensity to cause weight gain and to a more significant extent. Quetiapine and risperidone have a moderate risk of causing weight gain and to a more moderate extent3. Aripiprazole or lurasidone may reverse weight gain. Haloperidol and amisulpride have a low risk of causing weight gain and to a low extent. In relation to valproate, weight gain can be significant3. See appendix 1.
13 Dyslipidaemia
13.1 Olanzapine, clozapine appears to have the greatest propensity to increase lipids,
quetiapine and risperidone moderate propensity3. Aripiprazole may be treatment of choice for antipsychotic induced dyslipidaemia3. See appendix 1.

25 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
14 Extrapyramidal side effects
14.1 Haloperidol appears to have the greatest propensity to cause extrapyramidal side effects, risperidone a mild propensity, olanzapine mild to no propensity, quetiapine, none and aripiprazole. Clozapine is an alternative3. See appendix 1.
14.2 Dystonia (uncontrolled muscular spasm)3
Anticholinergic medicines (procyclidine, orphenadrine, trihexyphenidyl) can be given orally, intramuscularly or intravenously depending on the severity of symptoms. Patients may not be able to swallow. Response to the intramuscular route takes around 20 minutes. Consider switching to an antipsychotic medicine with a lower propensity for extrapyramidal side effects3.
14.3 Pseudo-parkinsonism (tremor etc)3
Options include:- Consider reducing the dose of the antipsychotic or Change to an antipsychotic medicine with lower propensity for pseudo-parkinsonism (see appendix 1). Anticholinergics: The majority of patients do not require long-term anticholinergics. The prescriptions should be reviewed every three months. Anticholinergic medicines should not be prescribed at night as symptoms are usually absent3.
14.4 Akathisia (restlessness)3
Options include:- Consider reducing the dose of the antipsychotic or Change to an antipsychotic medicine with lower propensity for akathisia (see appendix 1). A reduction in symptoms may be seen with propranolol 30-80mg/day (evidence – poor). Anticholinergic medicines are generally unhelpful3.
14.5 Tardive dyskinesia (abnormal movements)3
Options include:- Consider reducing the dose of the antipsychotic or Change to an antipsychotic medicine with lower propensity for tardive dyskinesia (data is conflicting) (see appendix 1 for options). Clozapine is the antipsychotic most likely to be associated with resolution of symptoms. Quetiapine, olanzapine or aripiprazole may also be useful in this regard. Tetrabenazine has some efficacy as add-on treatment. For other treatment options, see the Maudsley prescribing guidelines. For the management of side effects due to clozapine, see the clozapine treatment guidelines on the intranet.

26 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
15 Neuroleptic malignant syndrome
15.1 Neuroleptic malignant syndrome is a rare, but potentially serious or even fatal adverse effect of all antipsychotics3.
15.2 Risk factors include high potency typical medicines, recent or rapid dose increase, rapid dose reduction, abrupt withdrawal of anticholinergics, antipsychotic polypharmacy3.
15.3 Initially all antipsychotics should be withdrawn and temperature, pulse, blood pressure monitored. Benzodiazepines (e.g. IM lorazepam) if not already prescribed should be considered3. Liaise with medical staff at the acute trust as a medical admission may be required3.
15.4 Re-starting antipsychotic treatment would be required in most cases. Antipsychotics should be stopped for at least five days, preferably longer. All symptoms of neuroleptic malignant syndrome should have resolved completely first. An antipsychotic structurally unrelated to that previously associated with NMS or an antipsychotic with low dopamine affinity (quetiapine or clozapine) should be considered. Whilst aripiprazole may be considered, it has a long half-life and is linked to an increased risk of NMS. Avoid depots of any kind and high potency conventional antipsychotics3. See appendix 1.
16 Hyperprolactinaemia
16.1.1 The following antipsychotics are usually not associated with hyperprolactinaemia – aripiprazole, asenapine, clozapine and quetiapine. Lurasidone and olanzapine are low risk. Aripiprazole usually decreases plasma prolactin. Prolactin-elevating antipsychotics are amisulpride, sulpiride, risperidone, paliperidone and first generation antipsychotics3.
16.1.2 Prolactin-elevating antipsychotic should if possible be avoided in the following patient groups:
Patient under 25 years of age i.e. before peak bone mass.
Patient with osteoporosis.
Patients with history of hormone-dependent breast cancer.
Young women3.

27 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
16.1.3 All patients should have a prolactin level measured before starting any antipsychotic known to be associated with raised prolactin3 if possible. At three months, all patients should be asked about prolactin-related symptoms. If hyperprolactinaemia is suspected or a prolactin elevating antipsychotic is prescribed, another prolactin level should be obtained. Where prolactin is high and the patient is symptomatic, consider switching to an antipsychotic that is less likely to raise prolactin. An alternative is to add aripiprazole (3-6mg/day) to existing treatment. Higher doses of aripiprazole appear unnecessary. Symptoms tend to resolve slowly and symptoms severity does not reflect prolactin changes. Where aripiprazole augmentation is successful, consideration should be given to reducing the dose of the antipsychotic responsible for raising prolactin with the aim of aripiprazole monotherapy. Only if this strategy fails should combined antipsychotic treatment be considered3.
16.1.4 If the prolactin level is high, but the patient is asymptomatic, the clinical implications should be discussed with the patient and a joint decision taken on whether to continue current treatment with annual monitoring or switch to another antipsychotic3.
16.1.5 If the patient needs to remain on a prolactin elevating antipsychotic, but cannot tolerate aripiprazole, then a dopamine agonist e.g. amantadine, bromocriptine and cabergoline should be considered, but each has a potential to worsen psychosis (although not reported in trials). For this indication, a non-formulary form should be completed3.
16.1.6 Long-term use of prolactin-elevating medicines should be avoided in young women, given the possible increased risk of breast cancer and the known risk of decreased bone mineral density3.
16.1.7
Table 10: Prolactin concentration interpretation3
Normal Women 0-25ng/ml 0-530mIU/L
Men 0-20ng/ml 0-424mIU/L
Consider a systematic assessment of prolactin-related side effects and discussion of clinical consequences.
530 -2500mIU/l
Need referral for tests to rule out prolactinoma. >2500mIU/l
Take blood sample at least 1 hour after waking or eating.
Minimise stress during venupuncture (stress elevates plasma prolactin).
16.1.8 See appendix 1.
17 Venous thromboembolism
17.1 Antipsychotics are associated with a small but important risk of venous thromboembolism, resulting in an elevated incidence of pulmonary embolism, stroke and myocardial infarction, particularly in the early part of treatment.
Risk factors include younger people, early part of treatment and dosage. Signs of venous thromboembolism:
calf pain or swelling
breathing difficulties
signs of myocardial infarction or stroke

28 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
17.2 To minimise the risk, the lowest therapeutic dose should be prescribed and hydration and physical mobility should be encouraged.
18 Pregnancy and breastfeeding
When initiating an antipsychotic in a woman planning pregnancy, previous response must be taken into account. Quetiapine has a relatively low rate of placental passage3. When assessing the risks and benefits of antipsychotic medication for a pregnant woman, the risk of gestational diabetes and excessive weight gain and the limited data of safety for antipsychotics in pregnancy and postnatal period should be taken into account. Pregnant women taking antipsychotic medication should be advised about diet and weight gain should be monitored, in line with the guideline on weight management before, during and after pregnancy. Monitor for gestational diabetes in pregnant women taking antipsychotic medication in line with the guideline on diabetes in pregnancy and offer an oral glucose tolerance test. Prolactin levels should be monitored in women who are taking prolactin-raising antipsychotic medication and planning a pregnancy, because raised prolactin levels reduce the chances of conception. A prolactin-sparing antipsychotic should be considered if prolactin levels are raised25. An antipsychotic should be offered as prophylactic medication if a woman with bipolar disorder becomes pregnant and is stopping lithium, or plans to breastfeed26. Also see appendix 4 for further information. For patients’ prescribed adjunctive valproate, refer to the trust bipolar affective disorder guidelines for details of the pregnancy prevention programme.
19 Antipsychotics in bipolar affective disorder
Table 11: Antipsychotic of choice in bipolar affective disorder
The Drugs and Therapeutics Committee recommend that the oral antipsychotic risperidone be
considered as the first-line antipsychotic in all patients diagnosed bipolar disorder. For the full
management of BPAD, refer to Trust prescribing guidelines for the management of bipolar
affective disorder, NICE guidance and Maudsley prescribing guidelines.
Antipsychotics are used in the pharmacological management of bipolar affective disorder not
only for their antipsychotic properties, but also for their sedative, anxiolytic, antimanic and
antidepressive properties3.

29 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
19.1 Management of mania, hypomania or mixed affective state.
Table 12: Medicine choice in the management of bipolar affective disorder26
Options Medicine choice Comments
Management of mania or hypomania or mixed affective state and not taking an antipsychotic or mood stabiliser
First line An antipsychotic Options listed in NICE – haloperidol, olanzapine, quetiapine or risperidone. Second line Another antipsychotic
Third line Antipsychotic and lithium
Fourth line Antipsychotic and valproate Consider if lithium is ineffective or not suitable.
Management of mania or hypomania or mixed affective state and already prescribed lithium
First line Check lithium levels. If inadequate, maximise levels.
Second line Consider adding an antipsychotic to lithium
Options listed in NICE – haloperidol, olanzapine, quetiapine or risperidone depending on any advance directive, the patient’s preference and previous response to treatment, co-morbidity and side effects.
Management of mania or hypomania or mixed affective state and already prescribed valproate
First line Maximise dose of valproate (off-label) within BNF limits.
Sodium valproate – off-label. This is the preparation of choice in the trust formulary.
Second line Consider adding an antipsychotic to valproate
Options listed in NICE – haloperidol, olanzapine, quetiapine or risperidone depending on any advance directive, the patient’s preference and previous response to treatment, co-morbidity and side effects.
If a person develops mania or hypomania or mixed affective state and is taking an antidepressant as monotherapy, consider stopping the antidepressant and offer an antipsychotic (see table9)26.
19.2 Management of moderate to severe bipolar depression:-
Table 13: Management of moderate to severe bipolar depression (no medicine prescribed)26
Options Medicine choice Comments
First line 1a Fluoxetine and olanzapine (off-label) These are first line alternative options depending on the person’s preference and previous response to treatment.
First line 1b Quetiapine
First line 1c Olanzapine (off-label)
First line 1d Lamotrigine (off-label)
Second line Lamotrigine (off-label) If treatment failure with (fluoxetine and olanzapine) or quetiapine.
Management of moderate to severe bipolar depression and already prescribed lithium
First-line Check lithium levels. If inadequate, maximise levels.
Second line If lithium levels are maximum, undertake the addition of one of 1a - 1d above to it.
These are first line alternative options depending on the person’s preference and previous response to treatment.
Third-line Lamotrigine and lithium If treatment failure with (fluoxetine and olanzapine) or quetiapine, stop this additional treatment and consider adding lamotrigine to lithium.
Management of moderate to severe bipolar depression and already prescribed valproate
First-line Consider increasing the dose within the therapeutic range.
Off-label
Second line
If at the maximum tolerated dose or at the top of the therapeutic range & there is a limited response, undertake the addition of 1a-1d above to valproate.
These are first line alternative options depending on the person’s preference and previous response to treatment.
Third-line Lamotrigine and valproate (off-label) If treatment failure with (fluoxetine and olanzapine) or quetiapine, stop this treatment and consider adding lamotrigine to valproate.

30 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
19.3 Reviewing treatment for bipolar depression
Within 4 weeks of resolution of symptoms, discuss with the person, and their carers if appropriate, whether to continue pharmacological treatment for bipolar depression or start long-term treatment. The potential benefits of long-term treatment and the risks, including side effects of medication used for long-term treatment should be explained. If the person decides to continue pharmacological treatment for bipolar depression, it should be offered for a further 3–6 months, and then reviewed26.
19.4 Long-term pharmacological management of bipolar disorder
Table 14: Long-term pharmacological treatment of bipolar disorder26
First line Lithium
Second-line Lithium and valproate (off-label) Consider combination therapy if lithium monotherapy is ineffective.
Third-line 3a Valproate (off-label) or olanzapine Consider these options if lithium is poorly tolerated or not suitable e.g. blood tests are declined.
Third-line 3b Quetiapine If it has been effective in an episode of mania or bipolar depression.
19.5 When planning long-term pharmacological treatment to prevent relapse, medicines
that have been effective during episodes of mania or bipolar depression should be taken into account. Discuss with the person whether they prefer to continue this treatment or switch to lithium, and explain that lithium is the most effective long-term treatment for bipolar disorder26. The possible benefits and risks of each medicine for them should be discussed with the person. If stopping long-term pharmacological treatment: recognising early signs of relapse and what to do if symptoms recur should be discussed. Treatment should be stopped gradually and the person monitored for signs of relapse. Continue monitoring symptoms, mood and mental state for 2 years after medication has stopped entirely. This may be undertaken in primary care26.
19.6 Limited data suggests that continuation of the antipsychotic medicine beyond 24 weeks is unproductive3.
19.7 Treatment resistant bipolar disorder
Clozapine added to usual treatment principally lithium or anticonvulsants was superior to usual treatment alone over one year in treatment resistant bipolar patients including those with rapid cycling and mixed states. It however lacks formal proof of efficacy, but is mentioned in the Maudsley prescribing guidelines. Treatment with clozapine is monitored by the Clozapine Patient Monitoring Service, but is an unlicensed indication27,28,29. The use of clozapine in the management of bipolar disorder would require a non-formulary approval (refer to the trust formulary policy).
19.8 Guidelines on the use of antipsychotic medicines:-
Treatment with antipsychotic medication should be considered an explicit individual therapeutic trial. The side effects should be discussed with the person and acceptable side effects should be recorded. The indications, benefits and risks should be recorded. The expected time of onset of benefit and side effects should be recorded26. At the start of treatment, a dose that is appropriate for the phase and severity of the illness should be prescribed. Dose above the maximum recommended in the BNF or SPC should not be routinely prescribed. If high dose antipsychotic therapy (HDAT) is prescribed, the reasons should be recorded and justified. The person should be

31 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
informed that HDAT is unlicensed. The rationale for continuing, changing or stopping medication, and the effects of such changes should be recorded26. The Trust high dose antipsychotic therapy guidelines should be implemented.
19.20 Monitoring antipsychotic medication
The following should be monitored and recorded during dose titration and then regularly and systematically throughout treatment:
response to treatment, including changes in symptoms and behaviour
side effects and their impact on physical health and functioning
the emergence of movement disorders
adherence26. If out-of-range test results are reported at any stage of treatment, the person should be offered further investigations and treatment as needed26.
19.21 'As required' (p.r.n.) prescriptions of antipsychotic medication
Clinical indications, frequency of administration, therapeutic benefits and side effects should be reviewed each week or more often if needed. ‘As required’ (prn) prescriptions should not unintentionally lead to a total antipsychotic dosage above the maximum specified in the BNF or SPC. Regular combined antipsychotic medication should not be started except for short periods (for example, when changing medication)26.
19.22 Stopping antipsychotic medicines
When stopping an antipsychotic medicine, the dose should gradually be reduced over at least 4 weeks to minimise the risk of relapse26.
19.23 Further information
For further information, refer to the trust Bipolar Affective Disorder Prescribing Guidelines on the intranet. GPs can be referred to the antipsychotic factsheet:- https://www.ncl-mon.nhs.uk/wp-content/uploads/Interface_prescribing/FS_Antipsychotic_Monitoring.pdf
20 Treatment resistant depression or psychotic depression
The NICE (depression) and the BAP (2008) guidelines recommend the combination
of aripiprazole, olanzapine, quetiapine, or risperidone and an antidepressant when
standard doses of the latter have failed.30,31 If a patient does not respond to initial
pharmacological treatment, NICE guidance provides a number of options including
augmentation treatment with an atypical antipsychotic. Based on its lower acquisition
costs risperidone should be used first line as an adjunctive therapy in a major
depressive episode if an atypical antipsychotic is to be selected. Quetiapine,
olanzapine or aripiprazole may be considered if it is thought risperidone would not be
tolerated. However, there is some evidence quetiapine may be less well tolerated30.
Therefore olanzapine or aripiprazole are preferred second-line options, whilst
quetiapine may be a third-line atypical antipsychotic. The choice of antipsychotic will
also be influenced by the patient’s medical history and history of side effects32.

32 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
21 Catatonia
21.1 The treatment of stupor is dependent on it’s cause.
Stupor Benzodiazepines are the medicines of choice for stupor occurring in the context of affective and conversion disorders. There is most clinical experience with lorazepam Many patients will respond to standard dose of (up to 4mg per day), but repeated and higher doses (between 8-24mg per day) may be needed. Doses on the first day can be given orally or sublingually. Doses thereafter should be given intramuscularly.
21.2 Catatonia
Catatonia in schizophrenia is less likely to respond to benzodiazepines with a response in the range of 40–50%. In stupor associated with schizophrenia, ECT and benzodiazepines are the treatments of choice. The use of antipsychotic medication should be carefully considered, but some authors recommend antipsychotics should be avoided. There is probably most evidence supporting clozapine and olanzapine.
Factors to consider if antipsychotic medication is considered:-
previous diagnosis and response to antipsychotic treatment
likelihood of non‐adherence precipitated stupor.
21.2 Antipsychotic medication should be avoided where there are clear signs of NMS. If NMS is be ruled out and stupor occurs in the context of non‐adherence to
antipsychotic treatment, early re‐establishment of antipsychotic medication is recommended. This is particularly important where stupor represents a withdrawal syndrome.
22 Older Adults (>65 years)
22.1 Older people are more sensitive to side effects, more likely to have physical co-morbidity and be taking many other medicines. So consider:
Medicine interactions with other medication.
Dosage.
Avoiding medicines that block alpha-adrenoceptors, have anticholinergic side effects
and are very sedative, have a long half-life and are potent inhibitors of hepatic
metabolizing enzymes.
Cardiac risk factors - QT prolongation.
Risk of extrapyramidal side effects, sedation and falls3, 33.
22.2 Patients over 65 years generally require lower antipsychotic doses due to increased age-related sensitivity to the therapeutic and adverse effects of medication12.
Pre – treatment assessment repeated every 3 – 6 months to detect common side
effects e.g. postural hypotension, antimuscarinic effects, and Parkinsonism22.
Doses should be reviewed regularly and a periodic reduction in dose (for some

33 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
patients) may be indicated22.
Medicines for side effects should be avoided and a better tolerated alternative
found22.
Therapy should be kept as once a day administration whenever possible3.
22.3 For the use of antipsychotics in the management of behavioural disturbances in dementia, refer to current Maudsley prescribing guidelines. Atypical and typical antipsychotics were associated with similar increased risk for all-cause mortality and cerebrovascular events. Patients treated with typical antipsychotics have an increased risk of cardiac arrhythmias and extrapyramidal symptoms relative to patients prescribed atypical antipsychotics. Patients prescribed atypical antipsychotics are exposed to an increased risk of venous thromboembolism and aspiration pneumonia. There is an increased risk of mortality (all causes) in patients with dementia3. Both typical and atypical antipsychotics may hasten cognitive decline in dementia, although there is some evidence to refute this3.
22.4 Risperidone is licensed for short-term use (up to six weeks) in persistent aggression in moderate to severe Alzheimer’s dementia unresponsive to non-pharmacological approaches and where there is risk of harm to the patients or others3,12. If used for a longer period, this must be regularly monitored and trial reduction/withdrawal attempted after three months. Continued use (> 6 weeks) is outside the marketing authorisation and becomes off-label use. Justification for continuation of the prescription should be recorded in the electronic patient records. Risperidone is licensed up to 1mg twice a day, although the optimal dose is dementia has been found to be 500micrograms twice a day (1mg daily)3. Review of the antipsychotic needs to be done at 4-6 weeks (may be earlier in inpatients), then 3 months and then every 6 months if physically stable and there are no adverse effects3. For monitoring recommendations see the Positive cardiometabolic health resource. Lester UK adaptation. 2014. Further monitoring recommendations can also be obtained from the Maudsley prescribing guidelines.
22.5 Alternative antipsychotic medicines may be used (off-licence) if risperidone is contraindicated or not tolerated. Olanzapine has some positive efficacy data for reducing aggression in dementia. Quetiapine (although not as effective as risperidone and olanzapine) may be considered in patients with Parkinson’s disease or Lewy body dementia (at very small doses) because of it’s low propensity for causing movement disorders3.
23 Learning Disabilities34
23.1 Psychotropic medication treatment should be based on:
A psychiatric diagnosis or
Managing behaviour disorders following assessment and formulation with input from
a multidisciplinary team, family and carers34.
23.2 Diagnostic and functional assessments should address the following:
Medical pathology
Psychosocial and environmental conditions
Health status
Current medication

34 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Presence of psychiatric condition
History, previous interventions and results
Functional analysis of behaviour34
23.3 General principles for dosing: Start low and go slow - use lower initial doses and increase more slowly than in the
general population. Consider starting with half the usual adult dose of antipsychotic
and increase twice as slowly12.
Use the same or lower maintenance maximum doses as in the general population.
Periodically consider gradual dose reduction.
Reduce doses at the same or slower rates than in the general population34.
23.4 Antipsychotics are used across a broad range of behavioural disturbances, most consistently useful for aggression and irritability. Before the advent of atypicals, the best evidence was for haloperidol in the context of autism and zuclopenthixol for behavioural disturbances3.
23.5 The best evidence is for risperidone at low (500micrograms – 2mg) for aggression and mood stability (now licensed for short-term use), particularly with associated autism, though in non-autistic cases. Aripiprazole has an FDA licence for behavioural disturbance in young people with autism. There is some evidence to support olanzapine and case reports of clozapine for severe cases of aggression, though not widely used (mainly highly specialist inpatient) settings3.
23.6 Results for quetiapine are modest at best3.
23.7 Notable side effects include worsening of seizures, sedation, extrapyramidal reactions (including with risperidone at normal doses, especially in individuals who already have mobility problems), problems with swallowing (with clozapine and other antipsychotics) and worsening of cognitive function with anticholinergic medicines3.
23.8 Consent should be obtained from the person before beginning treatment. For adults who lack capacity, decisions regarding treatments are taken using the best interest principle. The option chosen should be the least harmful for the person35.
23.9 Medicines interactions
Co-morbidity is common in people with learning disabilities such as physical illness or epilepsy resulting in multiple medicine regimes. This increases the risk of medicine interactions. Some important medicine interactions are given in the BNF or contact the pharmacy team. Also see appendix 6.
23.10 Challenging behaviour35
Antipsychotic medication to manage behaviour that challenges should be considered only if: psychological or other interventions alone do not produce change within an agreed time or treatment for any coexisting mental or physical health problem has not led to a reduction in the behaviour or the risk to the person or others is very severe (for example, because of violence, aggression or self-injury). Antipsychotic medication should only be offered in combination with psychological or other interventions35.

35 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Take into account the person's preference (or that of their family member or carer, if appropriate), side effects, response to previous antipsychotic medication and interactions with other medication when offering and antipsychotic medication35.
Antipsychotic medication should initially be prescribed and monitored by a specialist (an adult psychiatrist) who should: identify the target behaviour decide on a measure to monitor effectiveness (for example, direct observations, the Aberrant Behaviour Checklist or the Adaptive Behaviour Scale), including frequency and severity of the behaviour and impact on functioning. A low dose should be started and the minimum effective dose should be prescribed. A single medicine should be prescribed, whilst monitoring side effects. The effectiveness and any side effects of the medication should be reviewed after 3–4 weeks. The medication should be stopped if there is no indication of a response at 6 weeks. The behaviour that challenges should be re-assessed. As-needed medication should be prescribed for as short a time as possible and it’s use recorded and reviewed. The medication should be reviewed if there are changes to the person's environment (e.g. staff change, new care setting) or their physical or mental health35.
The following should be documented: rationale for medication (explained to the person with a learning disability and everyone involved in their care, including their family members and carers) how long the medication should be taken for a strategy for reviewing the prescription and stopping the medication. If there is a positive response to antipsychotic medication the extent of the response should be recorded, the change in behaviour and any side effects or adverse events. A full multidisciplinary review should be undertaken after 3 months and then at least every 6 months covering all prescribed medication (including effectiveness, side effects and plans for stopping) continuing to prescribe only medication that has proven benefit35.
When prescribing is transferred to primary or community care, or between services, the psychiatrist should give clear guidance to the practitioner responsible for continued prescribing about: which behaviours to target monitoring of beneficial and side effects taking the lowest effective dose how long the medication should be taken for plans for stopping the medication.
For the use of rapid tranquillisation, see the Trust rapid tranquillisation guidelines.
23.11 Autistic spectrum disorder36
Antipsychotic medication should not be used for the management of core symptoms of autism. Antipsychotics can be considered for any coexisting mental disorders as per NICE guidance36.
Antipsychotic medication can be considered in conjunction with a psychosocial intervention for challenging behaviour when there has been no or limited response to psychosocial or other interventions (such as environmental adaptations). Antipsychotic medication should be prescribed by a specialist and quality of life outcomes monitored carefully. The effects of the medication should be reviewed after 3–4 weeks and discontinued at 6 weeks if there is no indication of a clinically important response. Antipsychotic medication can be considered on it’s own for challenging behaviour when psychosocial or other interventions could not be delivered and monitored as above.

36 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
23.12 Monitoring:
The physical health monitoring requirements for antipsychotic treatment, as listed in
appendix 7, should be followed. More frequently or additional monitoring may be
considered, if clinically appropriate.
24.0 Substance Misuse
24.1 Substance misuse in fully antipsychotic treatment adherent individuals increases relapse rates to the levels seen in non-adherent individuals with schizophrenia. Where there are suspicions of illicit drug induced psychosis, urine drug tests should be undertaken. As outlined previously, a physical examination should be done if possible, including blood pressure, temperature, pulse, respiration and an ECG3. A blood test to check liver function tests should be obtained if possible. The duration of detection of drugs in the urine varies and the table highlighting common illicit drugs is available in the ‘Drug misuse and dependence: UK guidelines on clinical management’37.
24.2 A summary of interactions between ‘street drugs’ and medicines prescribed for mental illness is available in the Maudsley Prescribing Guidelines3. The risks of a prolonged QTc interval appears to be higher with methadone, although this risk seems to be mainly associated with doses greater than 100mg per day. The addition of an antipsychotic may have an additive effect38. Patients should be warned about potential interactions between psychotropic medicines and illicit drugs. The problems and potential dangers of using non-prescribed substances and alcohol to counteract the effects or side effects of prescribed medicines should be discussed39.
24.3 Further information refer to Trust Guidance for Prescribing in Substance Misuse Services for guidance on opiate substitute prescribing.
25.0 Smoking cessation 25.1 People with psychosis or schizophrenia who smoke should be offered help to stop
smoking, even if previous attempts have been unsuccessful. Be aware of the potential significant impact of reducing cigarette smoking on the metabolism of other medicines, particularly clozapine and olanzapine5.
25.2 Refer to trust Prescribing Guidelines for Smoking Cessation on the trust intranet for
more detailed information
26. Associated documents
Clozapine treatment guidelines.
Depot antipsychotic medication. Guidelines for prescribing and administering.
Guidance for the use of zuclopenthixol acetate (clopixol acuphase) in adults.
Prescribing guidelines for the management of bipolar affective disorder.
Rapid tranquillisation guidance.
27.0 Dissemination and implementation arrangements
This document will be circulated to all managers who will be required to cascade the
information to members of their teams. It will be available to all staff via the Foundation Trust
intranet.

37 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
28.0 Training requirements
Staff will be provided training in how to use this policy in line with the Trust’s Mandatory
Training Policy and the Learning and Development Guide. For training requirements please
refer to the Trust’s Mandatory Training Policy and Learning and Development Guide.
29.0 Monitoring and audit arrangements
See table below

38 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
30.0 Review of the policy
These guidelines shall be reviewed in 3 years or earlier should a new guidance or change of
practice came to light.
31.0 References
1. Lieberman J., Stroup T.S, McEvoy J., et al. Clinical antipsychotics trials of
`intervention effectiveness [CATIE] Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med; 353(12): 1209-23 (2005).
2. Jones P.B, et al. Randomised-controlled trial of the effect on quality of life of second-vs. first-generation antipsychotic drugs in schizophrenia. Cost-utility of the latest antipsychotic drugs in schizophrenia study (CUtLASS-1). Arch Gen Psychiatry; 63:1079-87 (2006).
3. Taylor D. Paton C., Barnes T.R. and Young A.H. Editors. The South London and
Maudsley NHS Foundation Trust. Prescribing Guidelines. 13th Edition. London. Wiley Blackwell (2018).
4. Lewis SW, Barnes TRE, Davies L, et al. Randomised-controlled trial of effect of
prescription of clozapine versus other second-generation antipsychotic drugs in resistant schizophrenia. Schizophr Bull ;32:715–23 (2006).
5. Psychosis and schizophrenia in adults: prevention and management. Clinical guidelines. National Institute for Clinical Excellence (NICE) (2014). (online). Available: https://www.nice.org.uk/guidance/cg178/resources/psychosis-and-schizophrenia-in-adults-prevention-and-management-35109758952133 (accessed 5th January 2016).
6. Evidence - based guidelines for the pharmacological treatment of schizophrenia:
Recommendations from the British Association for Psychopharmacology. Thomas
Element to be monitored
Lead How Trust will monitor compliance
Frequency Reporting arrangements
Acting on recommendations and Lead(s)
Which committee or group will act on recommendations?
Change in practice and lessons to be shared
Antipsychotic prescribing
Chief Pharmacist
Medication charts are clinically screened by a pharmacist.
On going Drugs and Therapeutics Committee
Drugs and Therapeutics Committee
Review of policy; implementation practices and procedures. Re- audit Give feedback to prescribers.

39 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
RE Barnes and the schizophrenia consensus group of the British Association for Psychopharmacology. Journal of Psychopharmacology 0(0) 1-54 (2011).
7. Camden and Islington NHS Foundation Trust. Rapid Tranquillisation Guidance. 11th Edition. (2018).
8. Ogino S. et al. Benefits and limits of anticholinergic use in schizophrenia: focussing on it’s effect on cognition function. Psychiatry and Clinical Neurosciences 2014; 68: 37-49.
9. Crespo-Facorro et al: A practical clinical trial comparing haloperidol, risperidone and olanzapine for the acute treatment of first-episode non-affective psychosis. J Cl Psychiatry 67:1511-1521 (2006).
10. Robinson D et al :Predictors of relapse following response from a first-episode of
schizophrenia or schizoaffective Disorder. Arch Gen Psychiatry 56:241-247 (1999).
11. Schooler N et al : Risperidone and haloperidol in first-episode psychosis : a long-term randomised trial. Am J Psychiatry 162:947-953 (2005).
12. Central North West London NHS Foundation Trust. Guidelines for use of
antipsychotics in people with schizophrenia and first episode psychosis. April 2012.
13. Bazire S. Psychotropic drug directory 2016. .
14. https://www.evidence.nhs.uk/formulary/bnf/current/4-central-nervous-system/42-drugs-used-in-psychoses-and-related-disorders/422-antipsychotic-depot-injections.
15. Risperidone injection (online). Available: https://www.medicines.org.uk/emc/medicine/30449 (accessed 28th January 2016).
16. Paliperidone long-acting injection for schizophrenia. National Prescribing Centre. 2010 (online). Available: http://www.npc.nhs.uk/new_medicines/cns/schiz/oth_paliperidone.php (accessed 27th January 2012).
17. Dong-Jing Fu et al. Paliperidone palmitate versus risperidone long-acting injection in
markedly to severely ill schizophrenia subjects: onset of efficacy with recommended initiation regimens. Clinical schizophrenia and related psychoses. Summer 2014, p101 -109A.
18. Enc 3 Appx 3 clinical expert summary paliperidone palmitate (Xeplion). All Wales Medicines Strategy Group. November 2011 (online). Available: http://www.wales.nhs.uk/sites3/docmetadata.cfm?orgid=371&id=181234&pid=50967 (accessed 27th January 2012).
19. Aripripazole depot (online). Available: https://www.medicines.org.uk/emc/medicine/28494 (accessed 28th January 2016).
20. Eli Lilly and Company. Olanzapine Pamoate (OP) Depot, Psychopharmacologic Drugs Advisory Committee Briefing Document. 2008 (online). Available: http://www.fda.gov/ohrms/dockets/ac/08/briefing/2008-4338b1-03-Lilly.pdf (accessed 27th January 2012).
21. The Specification of Product Characteristics: Zypadhera 210mg, 300mg, 405mg powder and solvent for prolong release suspension for injection (1st of September

40 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
2015) (online). Available: http://www.medicines.org.uk/EMC/medicine/21361/SPC/ZYPADHERA+210+mg%2c+300+mg%2c+and+405+mg%2c+powder+and+solvent+for+prolonged+release+suspension+for+injection/ (accessed 5th January 2016).
22. The Sussex Partnership NHS Foundation Trust. Guidance on the Use of Antipsychotics. 3rd Edition. 2015.
23. Novartis. The Specification of Product Characteristics: Clozaril 25mg and 100mg Tablets (11th September 2014) (online). Available: http://www.medicines.org.uk/EMC/medicine/1277/SPC/Clozaril+25mg+and+100mg+Tablets/ (accessed 5th January 2016).
24. Royal College of Psychiatrists. College Report CR190. Consensus statement on high dose antipsychotic medication. November 2014.
25. NICE clinical guideline 192. Antenatal and postnatal mental health: clinical management and service guidance. December 2014.
26. NICE clinical guideline 185. Bipolar disorder The assessment and management of bipolar disorder in adults, young people and children in primary and secondary care. January 2015.
27. Jones P.B, et al. Randomised-controlled trial of the effect on quality of life of second-vs. first-generation antipsychotic drugs in schizophrenia. Cost-utility of the latest antipsychotic drugs in schizophrenia study (CUtLASS-1). Arch Gen Psychiatry; 63:1079-87 (2006).
28. Coker A. Camden and Islington NHS Foundation Trust. Audit of the Trust High Dose Antipsychotic Therapy Guidelines on Inpatient Wards at Highgate Mental Health Centre. August 2011.
29. Goodwin GM, Consensus Group of the British Association for Psychopharmacology. Evidence Based Guidelines for Treating Bipolar Disorder: revised second edition – recommendations for the British Association for Psychopharmacology. J. Psychopharmacol.online first published March 27, 2009.
30. National Institute for Health and Clinical Excellence. Depression. The treatment and management of depression in adults. This is a partial update of NICE Clinical Guideline 23. NICE Clinical Guidance 90. London. 2009.
31. Anderson I.M. et al. Evidence-based guidelines for treating depressive disorders with
antidepressants: A revision of the 2000 British Association for Psychopharmacology Guidelines. Journal of Psychopharmacology (2008) 22(4); p 343 – 396.
32. Coker A. Medicines evaluation, antipsychotic adjuncts
33. Bazire S. The Psychotropic Drug Directory. The Professionals’ Pocket Handbook and Aide Memoire. Aberdeen. HealthComm UK Ltd. 2014.
34. The Frith Prescribing Guidelines for Adults with Intellectual Disability edited by S.
Bhaumik and D. Branford.
35. Challenging behaviour and learning disabilities: prevention and interventions for people with learning disabilities whose behaviour challenges. https://www.nice.org.uk/guidance/ng11/resources/challenging-behaviour-and-

41 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
learning-disabilities-prevention-and-interventions-for-people-with-learning-disabilities-whose-behaviour-challenges-1837266392005 (accessed 25th Janaury 2016).
36. Autism in adults: diagnosis and management. https://www.nice.org.uk/guidance/cg142/resources/autism-in-adults-diagnosis-and-management-35109567475909 (accessed in 25th January 2016).
37. Drug misuse and dependence: UK guidelines on clinical management. http://www.nta.nhs.uk/uploads/clinical_guidelines_2007.pd
38. Lingford-Hughes A.R. et al. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance misuse, harmful use, addiction and comorbidity: recommendations from BAP. Journal of psychopharmacology, 0(0), 1-54. 2012.
39. NICE. Psychosis with co-existing substance misuse. Assessment and management of adults and young people. NICE clinical guideline 120. March 2011.
40. Drug Safety Update. Citalopram and escitalopram: QT interval prolongation—new maximum daily dose restrictions (including in elderly patients), contraindications, and warnings (December 2011). (online) Available: http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON137769 (accessed 3rd of February 2012).
41. Foisy M. et al . Predicted interactions between psychotropics and protease inhibitors/non nucleoside reverse transcriptase inhibitors (June 2011) (online). Available: http://www.hivclinic.ca/main/drugs_interact_files/psych-int.pdf (accessed 27th October 2011).
42. Database of antiretroviral drug interactions. Interactions between antipsychotics and antiretrovirals. (undated) (online) Available: http://hivinsite.ucsf.edu/insite?page=ar-00-02&post=10¶m=9 (accessed 27th October 2011).
43. HAART may affect chemotherapy treatment in HIV positive cancer patients (June
2011) (online). Available: http://www.aidsbeacon.com/news/2011/06/07/haart-may-affect-chemotherapy-treatment-in-hiv-aids-positive-cancer-patients/ (accessed 27th of October 2011).
44. Cheung S. Clozapine Patient Monitoring Service. Personal Communication. 30 th
August 2011. 45. Clozapine Therapy. Role of Therapeutic Drug Monitoring (TDM) Factsheet
(November 20101) (online). Available: https://www.clozaril.co.uk/scrMain.htm (accessed 27th October 2011).
46. BNF https://bnf.nice.org.uk/. June 2018.
47. National Institute for Clinical Excellence. Obesity. December 2006. NICE Clinical Guidance 4 http://www.rcpsych.ac.uk/pdf/e-version%20NICE%20Endorsed%20Lester%20UK%20adaptation2%20.pdf
48. https://www.medicines.org.uk/emc/product/7230/smpc

1 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 1: Suggestions for switching antipsychotics because of poor tolerability The table below lists potential side-effects of antipsychotics with suggested alternatives if a switch is considered appropriate. It is not exhaustive and should be consulted in conjunction with NICE guidance5 and the Maudsley prescribing guidelines3. Note the risk of some treatment-emergent effects may be more likely in patients with a history of relevant risk factors (e.g. age, gender, ethnicity, past medical history, concomitant medication, family history, presence of organic disease) or in certain patient-groups, e.g. risk of EPS with young, neuroleptic-naïve males. Factors to consider before switching include: current mental state; severity of side-effects; previous pattern of illness (including severity of episodes and danger posed to self and others); the need for close monitoring during changeover period; patient adherence/preference; consideration of dose-reduction before switching; and potential adjunctive pharmacological/non-pharmacological measures. The following antipsychotics are non-formulary: asenapine, ilioperidone, lurasidone, ziprasidone. Non-formulary applications would be required.
Appendix 2: Suggestions for switching antipsychotics because of poor tolerability3,5,46
Adverse Effect Suggested antipsychotic Alternative Avoid if possible Comments
Acute extrapyramidal side-effects (EPS)
Aripiprazole Olanzapine Quetiapine
Clozapine Lurasidone
Typical antipsychotics EPS are dose-related, more likely with high- dose typicals and uncommon with atypicals. Aripiprazole – akathisia can be problematic.
Akathisia Olanzapine Quetiapine
Clozapine
Dyslipidaemia Amisulpride Aripiprazole Lurasidone
Asenapine *Olanzapine *Clozapine *Quetiapine *Phenothiazines
*If no option but to prescribe any of these, perform 3-monthly fasting blood lipids for first year then yearly
Impaired glucose tolerance
Amisulpride Aripiprazole Lurasidone
Haloperidol *Olanzapine *Clozapine
* If no option but to prescribe either of these, then test fasting blood glucose at baseline, then at one month, then 4-6 monthly
Hyperprolactinaemia Aripiprazole
Lurasidone Quetiapine Clozapine
Clozapine Olanzapine
Risperidone Amisulpride Paliperidone Sulpiride Typical antipsychotics
Sexual dysfunction Aripiprazole Quetiapine Lurasidone
Clozapine
Risperidone Amisulpride Typical antipsychotics

2 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 1 contd: Suggestions for switching antipsychotics because of poor tolerability
Adverse Effect Suggested antipsychotic Alternative Avoid if possible Comments
Sedation Amisulpride Aripiprazole Risperidone Sulpiride
Haloperidol Trifluoperazine
Chlorpromazine Clozapine Olanzapine
Neuroleptic Malignant Syndrome (NMS)
Antipsychotic structurally unrelated to that associated with NMS or with low DA affinity (quetiapine or clozapine)
Aripiprazole High potency typicals Depot antipsychotics
Close monitoring of physical and biochemical parameters required.
Postural hypotension
Amisulpride Aripiprazole
Lurasidone
Haloperidol Sulpiride Trifluoperazine
Caution with: Clozapine Chlorpromazine Quetiapine Risperidone
Hypertension No specific recommendations
No antipsychotic contraindicated in essential hypertension, but extreme care needed with clozapine
Attention to risk factors including antipsychotic-induced weight gain and IGT; smoking. Unpredictable sharp rise in BP on starting new medicine/increasing dose suggests direct pharmacological mechanism of the antipsychotic.
Weight gain Amisulpiride Aripiprazole Haloperidol Lurasidone
Asenapine Trifluoperazine
Olanzapine Clozapine
Psychotropic-related QTc prolongation
Lurasidone Paliperidone (with ECG monitoring)
Low dose monotherapy of any medicine not formally contra-indicated in QT prolongation (with ECG monitoring)
Any intravenous antipsychotic, pimozide, sertindole. A medicine or a combination of medicines exceeding the 100% BNF limits.
Beware other medicine interactions and physiological risk factors, e.g. cardiac, metabolic (see appendices 5 and 6) Measure QTc in all patients prescribed antipsychotics on admission, before discharge and at yearly check-up.

3 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 1 contd: Suggestions for switching antipsychotics because of poor tolerability
Adverse Effect Suggested antipsychotic Alternative Avoid if possible Comments
Tardive dyskinesia Clozapine Aripiprazole Olanzapine Quetiapine
Typical antipsychotics Stop anticholinergic if prescribed
Anticholinergic side-effects
Sulpiride Amisulpride Aripiprazole Asenapine Iloperidone Lurasidone
Clozapine Beware danger of potentially life-threatening constipation with clozapine
Contact sensitisation
Other antipsychotics in the trust formulary.
Chlorpromazine, promazine (non-formulary), levomepromazine (non-formulary)
Patients should be warned to avoid direct contact with chlorpromazine and to use sunscreen if necessary. Handle with care. Do not crush tablets.

1 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 2: Antipsychotic depot injections – suggested doses and frequencies3, 16, 18, 19, 22
Medicine Trade name Test dose(mg) Dose range (mg/week) Dosing interval (weeks) Comments Flupentixol Depixol 20 12.5–400 2–4 Maximum licensed dose is very high relative to
decanoate other depots. Oily injection.
Fluphenazine Modecate 12.5 6.25–50 2–5 High EPS. Oily injection. Contains sesame oil.
Decanoate
Haloperidol Haldol 25* 12.5–75 4 High EPS. Oily injection. Contains sesame oil.
Decanoate Haloperidol short-acting injection is also
available.
Zuclopenthixol Clopixol 100 100–600 2–4 ? Slightly better efficacy. Oily injection.
Decanoate Contains sesame oil.
Intermediate-acting injection
is also available (zuclopenthixol acetate:
Acuphase) lasting for 3 days.
Atypical Antipsychotic depot injections1,2,3,4
Risperidone Risperidal consta Not required 12.5–25 mg 2 Medicine release delayed for 2–3 weeks. Store in
microspheres the fridge. Aqueous suspension: prefilled syringe
Aripiprazole depot Abilify depot Not required 400mg once a month (300mg once a 4 The dose may be reduced to 300mg every month if
month if side effects are present. side effects occur.
Olanzapine ZypAdhera
embonate
Paliperidone Xeplion Not required
palmitate
Switching from oral risperidone or paliperidone By deep intramuscular injection into the deltoid muscle, 150 mg on day 1, then 100 mg on day 8, then adjusted at intervals of 4
weeks according to response; recommended maintenance dose 75 mg (range 25–150 mg) every 4 weeks1.
Note: Following the second dose, monthly maintenance doses can be administered into either the deltoid or gluteal muscle.
Switching from risperidone long-acting injection (RLAI)
When switching from risperidone injection, paliperidone palmitate should be initiated in place of the next scheduled dose. The one
week initiation dosing regimen on day 1 and 8 respectively is not required. The following doses are commended:-
Previous RLAI dose (every 2 weeks) Paliperidone palmitate dose (monthly) 25mg 50mg 37.5mg 75mg 50mg 100mg If other switches are considered, advice should be obtained from the Pharmacy.
Recommended dosing and titration scheme when switching between oral olanzapine and olanzapine depot injection
Daily oral olanzapine dose Recommended starting dose of olanzapine depot injection Maintenance dose after 2 months of treatment
10 mg/day 210 mg / 2 weeks or
405 mg/ 4 weeks
150 mg / 2 weeks or
300 mg / 4 weeks†
15 mg/day 300 mg / 2 weeks 210 mg / 2 weeks or 405 mg/ 4 weeks
20 mg/day 300 mg / 2 weeks 300 mg / 2 weeks

2 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Paliperidone Trevicta Not required Palmitate 3 monthly
Dose equivalences
Paliperidone palmiate (monthly) Paliperidone palmitate (3 monthly)
50mg 175mg
75mg 263mg
100mg 350mg
150mg 525mg

1 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
APPENDIX 3: HIGH DOSE ANTIPSYCHOTIC THERAPY MONITORING FORM (HDAT)
7
Name: DOB: Ward:
Consultant: Date high dose therapy began:
Name of Doctor: Grade: Junior Doctors SPR Consultant Other Date:
Antipsychotic Medication (regular)2,3
Medicine Dose %BNF Max
Please, specify reason(s) for high dose antipsychotic therapy (HDAT)4,5
Other Medication:
CAUTION INCREASED RISK IN FOLLOWING CATEGORIES OF PATIENTS
7:
Old age:
Hepatic/renal impairment:
Obesity: Weight: …………………..
Heavy user of tobacco or alcohol:
History of arrhythmia:
History of myocardial infarction or IHD:
Medicine interactions (inc. medicines with additive ECG effects)
Other
Baseline Dose change
Dose change
Month 6 Month 12
ECG8
QT interval
QTc
Interval
LFTs9
Alk Phos
ALT
Total
Bilirubin
U & Es9
Na
K
Urea
Creatinine
BP, Pulse
Temp10
Please, record daily for one week - on initiation of HDAT, and after each increase in dose of antipsychotic.
Review Date(s)
11
Has patient/carers been informed of the high dose nature of therapy Yes/No12
Is high dose therapy covered on the consent form (where applicable) Yes/No
The HDAT form is located under the ’Medication’ tab in electronic patient records.
Royal College of Psychiatrists. College Report CR190. Consensus statement on high dose antipsychotic medication. November 2014 should be consulted for further advice. The report may be obtained via the Royal College of Psychiatrists website.

2 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
1. The consensus working group agreed to take the following as a definition of a high dose: ‘A total daily dose of a single antipsychotic which exceeds the upper limit stated in the summary of product characteristics or BNF and a total daily dose of two or more antipsychotics which exceeds the SPC or BNF maximum using the percentage method’.
2. To evaluate if a patient is on high dose antipsychotic therapy: express the dose of each antipsychotic as a percentage of its BNF maximum and add (including crosstapering regimens or as result of additional prn medication). If the total exceeds 100% - then patient is on “high dose antipsychotic therapy” (HDAT). For example: a patient on olanzapine 20 mg nocte and clopixol 400 mg i.m each week is on 100% of maximum Olanzapine dose and 66% of maximum clopixol dose: a total of 166% - thus, this Rx does constitute “high dose”. Such therapy CAN be given but it must be documented as such in the patient’s notes. The Royal College of Psychiatric Guidelines (RCPsych) must then be followed. Any further increases in dose/dosages of antipsychotic(s). Should be done slowly – waiting at least two weeks, before each subsequent dose increase. (Please note: both Consensus Statement on “The use of high dose Antipsychotic Medication” and Council Report CR57 “The Association between antipsychotic drugs and sudden death” do not recommend use of more than one antipsychotic at a time. Additionally, NICE guidance on use of atypicals does not recommend combining the latter with typical antipsychotics.
3. If the use of prn antipsychotic medication (whether p.o or i.m) pushes patient’s therapy into HDAT, please record use of such medication in notes. If this occurs for one day or more then: review therapy, and the rapid tranquillisation monitoring guidance must be implemented for both the oral or intramuscular routes.
4. Before high dose therapy is commenced – the possibilities of substance misuse, personality disorder, inadequate time to respond, poor adherence, misdiagnosis of psychosis, akathisia and “response to Clozapine” should be eliminated.
5. Other management techniques should be considered e.g. de-escalation or psychological techniques.
6. Decision to initiate high dose therapy should ONLY be made by a consultant, or registrar with MRCPsych following an individual risk benefit assessment on consultation with the clinical team. Obtaining a second medical opinion should be considered. The decision, risks & benefits, aims and how the outcomes will be assessed must be documented in the case notes/Care Notes.
7. RCPsych guidelines emphasise the importance of CAUTION to high dose antipsychotic therapy. These include:
Old Age History of myocardial infarction Medicine Interactions
Hepatic/Renal impairment History of arrhythmia Medicines with additive ECG effects
Obesity History of ischaemic heart disease Heavy users of tobacco/alcohol
These patients need to be monitored more closely as some patients may be contraindicated to HDAT. Patients should be
assessed for cardiovascular disease prior to antipsychotic treatment regardless of dose. Modifiable risk factors for ischaemic
heart disease inc. smoking, hypertension, hyperlipidaemia, sedentary lifestyle and obesity) should be identified and managed
appropriately. Under the circumstances of rapid tranquillisation where an assessment is difficult and ECGs impossible, it is
prudent to avoid high doses.
8. For patients prescribed regular high dose antipsychotic therapy, the monitoring guidance in the antipsychotic prescribing guidelines must be followed.
9. For patients prescribed a crosstapering antipsychotic regimen, see the monitoring guidance in the antipsychotic prescribing guidance must be followed.
10. For patients prescribed antipsychotic therapy within BNF limits and is also given additional PRN medication resulting in an above BNF dosage, the monitoring guidance in the antipsychotic prescribing guidance or the rapid tranquillisation guidance must be followed.
11. Where possible – discuss the decision to commence high dose antipsychotic therapy with the patient and/or patient’s carers.

3 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 4: Choice of medication in specific medical conditions3
Medical condition
Suggested antipsychotic Avoid if possible Comments
Epilepsy Trifluoperazine Haloperidol, flupenthixol, sulpiride, amisulpride, aripiprazole, risperidone
Clozapine Chlorpromazine (avoid completely) Depot antipsychotics Loxapine (not available in the UK) Lurasidone (experience limited) asenapine (experience limited) Zotepine (avoid completely) (not available in the UK) Olanzapine Quetiapine
The majority of antipsychotics decrease the seizure threshold. Clozapine – very epileptogenic. Approximately 5% who receive more than 600mg/day develop seizures. Sodium valproate or lamotrigine are the anticonvulsants of choice as they have a lower incidence of leucopenia than carbamazepine. None of the depot preparations currently available are thought to be epileptogenic. The kinetics of depots are complex (seizures may be delayed). If seizures do occur, the offending medicines may not be easily withdrawn. Depots should be used with extreme care. Beware pharmacokinetic interactions with anticonvulsants (see appendix 6).
Pregnancy There is no clear evidence that any antipsychotic is a major teratogen. Consider using/ continuing the medicine the mother has previously responded to rather than switching prior to/during pregnancy When initiating an antipsychotic in a woman planning pregnancy, previous response must be taken into account. Quetiapine has a relatively low rate of placental passage
Depot antipsychotics (Anticholinergics)
Discuss with the patient the absolute and relative risks associated with treating and not treating the mental disorder during pregnancy and the postnatal period. If patient established on another antipsychotic, the most up-to-date advice should always be obtained. A change in treatment may not be necessary or wise. The pharmacy department must be contacted for advice. Consider referral to specialist perinatal services.
Breastfeeding It is usually advisable to continue the medicine that was used in pregnancy except clozapine. In this case clozapine should be continued and advised not to breastfeed. Olanzapine or quetiapine. The pharmacy can be contacted for advice on alternative antipsychotics.
Clozapine (Women taking clozapine should be advised against breastfeeding and clozapine should be continued)
The benefits of breastfeeding to the mother and infant must be weighed against risk of medicine exposure in the infant. Infant exposure can be decreased by timing feeds to avoid peak medicine levels. The pharmacy department must be contacted for advice for advice on alternative antipsychotics. Consider referral to specialist perinatal services.

4 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Renal impairment
No agent clearly preferred to another. However for typical antipsychotic, suggest haloperidol 2-6mg/day; for atypical agent, suggest olanzapine 5mg/day
Sulpiride Amisulpride Depot antipsychotics Medicines known to prolong QTc interval Highly anticholinergic agents (risk of urinary retention)
Olanzapine and clozapine may cause and aggravate diabetes, a common cause of renal disease. Avoid medicines known to prolong QTc interval. In established renal failure, electrolyte changes are common so it may be best to avoid antipsychotics with the greatest risk of QTc prolongation. Weight gain (a risk with antipsychotics) may predispose to diabetes which can cause rhabdomyolysis and renal failure. Be vigilant for dystonias and NMS (as the resulting rhabdomyolysis can cause or worsen renal failure). Rhabdomyolysis can occur without symptoms of NMS.
Hepatic impairment
Sulpiride (no dosage reduction required if renal function is normal) Amisulpride (no dosage reduction required if renal function is normal) Paliperidone : if a depot is required.
Sedative or constipating medicines, e.g. chlorpromazine, clozapine (risk of hepatic encephalopathy). Avoid antipsychotic hepatotoxic in their own right e.g. MAOIs, chlorpromazine, clozapine. Avoid medicines with a long-half life or those that need to be metabolised to render them active. Depot antipsychotics.
Monitor LFTs weekly, at least initially. If LFTs deteriorate after a new medicine is introduced, consider switching to another medicine. One third of patients who are prescribed antipsychotics have at least one abnormal LFT and 4% of at least one LFT is elevated three times above the upper limit of normal. Transaminases are mostly affected and this generally occurs within 1-6 weeks of treatment initiation. Only rarely does clinically significant hepatic damage result.
Atrial fibrillation
Aripiprazole Lurasidone
Clozapine Olanzapine Paliperidone Avoid QT-prolonging medicines in ischaemic heart disease, and those which increase heart rate.
In permanent AF with rate control medicine choice is less crucial, but probably best to avoid medicines with potent effects on the ECG (ziprasidone, pimozide, sertindole) and those which increase the heart rate. Avoid QT-prolonging medicines in ischaemic heart disease. Beware arrhythmogenicity of psychotropics, their effect on ventricular rate (some induce reflex tachycardia via postural hypotension, others e.g. clozapine, quetiapine directly increase heart rate. Risk of interaction between co-prescribed antiarrhymics or rate-controlling medicines.

5 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
HIV Quetiapine, risperidone and aripipraole have been suggested as first-line antipsychotics.
Clozapine may be helpful in the treatment of individuals with HIV associated psychosis with medicine-induced parkinsonism. Clozapine, certain HIV medicine and the virus may have overlapping suppressive effects on bone marrow so extreme close monitoring of the white cell is recommended. Treatment of clozapine should only be initiated in patients who are medically well and stable on retroviral treatment. Clozapine not routinely recommended but may be helpful in low doses in patients with higher CD4 counts who are otherwise medically stable. May be helpful in HIV-associated psychosis with medicine-induced parkinsonism. It is not known whether patients with HIV have a greater risk of agranulocytosis, extremely close monitoring of the white cell count is recommended.
Liaise closely with HIV specialists and MDT team. Beware interaction between antipsychotics and antiretrovirals (see appendix 6). Idiosyncratic interactions between risperidone and ritonavir have been reported. Patients may be more susceptible to extrapyramidal side-effects, NMS and tardive dyskinesia.

6 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 5: Risk factors for QT prolongation3,40
Effects of antipsychotics on QTc interval Effect of QTc interval
High effect
Any intravenous antipsychotic Pimozide, Sertindole A medicine/combination of medicines > 100% BNF limits
Extensive average QTc prolongation (usually > 20msec at normal clinical doses).
Moderate effect
Amisulpride Chlorpromazine Haloperidol Levomepromazine Quetiapine
Observed to prolong QTc by > 10msec on average when given at normal doses or where ECG monitoring is officially recommended.
Low effect
Aripiprazole Asenapine Clozapine Flupentixol Fluphenazine Loxapine Prochlorperazine Olanzapine Paliperidone Risperidone Sulpiride
Severe QTc prolongation has been reported only following overdose or where only small average increases (<10msec) has been observed at clinical doses.
No effect
Lurasidone
QT prolongation has not been reported either at therapeutic doses or in overdose.
Unknown effect Pipothiazine Trifluoperazine Zuclopenthixol
Non-psychotropics associated with QT prolongation
Antibiotics Erythromycin, clarithromycin, ampicillin, co-trimoxazole, pentamidine, some 4-quinolones
Antimalarials Chloroquine, mefloquine, quinine
Antiarrthythmics Quinidine, disopyramide, procainamide, sotolol, amiodarone, bretylium
Others Amantadine, cyclosporin, diphenhydramine, hydroxyzine, methadone, nicardipine, tamoxifen
Physiological risk factors
Cardiac Long QT syndrome Bradycardia Ischaemic heart disease, Myocardial infarction Myocarditis Left ventricular hypertrophy
Metabolic Hypokaleamia Hypomagnesaemia Hypocalcaemia
Others Extreme physical exertion Stress or shock Anorexia nervosa Extremes of age Female gender
Hypokalaemia-related QTc prolongation is more commonly observed in acute psychotic admissions. There are a number of physical and genetic factors which may not be discovered in routine examination, but which probably predispose patients to arrhythmia3.

7 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 6: Medicine interactions3, 15, 16,23,22, 24, 34, 41,42, 43, 44,45
Medicine Combination Common Interactions
Antipsychotics and angiotensin converting enzyme (ACE) inhibitors, angiotensin-II receptor antagonists or calcium channel blockers.
Risk of postural hypotension.
Antipsychotics and antiarrhythmic medicines
Increased risk of ventricular arrhythmia with anti-arrhythmic medicines that prolong the QT interval such as amiodarone, bretylium, quinidine, sotalol, procainamide, quinidine, disopyramide.
Antipsychotics and antibacterials.
Erythromicin possibly increases plasma concentration of clozapine. Ciprofloxacin increases the plasma levels of clozapine and possibly olanzapine. Increased serum levels may result in an increase in seizures. Plasma concentrations of quetiapine are possibly increased by macrolides e.g. erythromycin. The following antibacterials have been associated with QT prolongation and so could have synergistic effect- erythromycin, clarithromicin, ampicillin, co-trimoxazole, pentamidine and some 4-quinolones.
Antipsychotics and antidepressants
Increased risk of arrhythmia with tricyclic antidepressants. Selective serotonin re-uptake inhibitors and venlafaxine increase the plasma concentration of clozapine. Fluoxetine and venlafaxine increase the plasma concentration of haloperidol. Severe EPSEs have been reported with fluoxetine and haloperidol. There is an important and significant interaction between clozapine and fluvoxamine. Fluvoxamine inhibition results in a significant increase in clozapine serum levels. Fluvoxamine inhibits clozapine metabolism dramatically (e.g. clozapine 100 mg/d + 25 mg/d fluvoxamine equivalent to 600-700 mg/d clozapine in some patients – very rarely deaths have occurred after such an interaction).
Antipsychotics and antiepileptics
The threshold for convulsions is lowered. Carbamazepine is contraindicated with clozapine due to the increased risk of neutropenia. Carbamazepine lowers the plasma concentration of aripiprazole, chlorpromazine, clozapine, fluphenazine, haloperidol, olanzapine, paliperidone, quetiapine, risperidone. Phenytoin lowers the plasma concentration of aripiprazole, clozapine, haloperidol, phenothiazines, quetiapine and risperidone, Phenytoin serum levels are increased by phenothizapines. The risk of neutropenia is increased if clozapine or olanzapine is given with valproate. Valproate increases plasma concentration of clozapine and possibly quetiapine. Valproate plasma concentration are increased by risperidone. Phenobarbital decreases the plasma concentration of aripiprazole, chlorpromazine, clozapine, haloperidol, promethazine and quetiapine.
Antipsychotics and antimalarials
The following antimalarials have been associated with QT prolongation and so could have a synergistic effect – chloroquine, mefloquine, quinine.

8 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 6 contd: Medicine interactions
Medicine Combination Common Interactions
Antipsychotics and antivirals
The effect of anti-retrovirals on antipsychotics is unpredictable. The plasma concentration of clozapine is possibly increased by ritonavir (avoid concomitant use) and possibly by amprenavir1. Conversely, decreased plasma concentrations of clozapine have been reported with the concomitant use of ritonavir. A decreased effect of olanzapine has also been reported. Amprenavir increases the effect of clozapine. Plasma concentration of olanzapine reduced by ritonavir (may need to increase dose). Plasma concentration of aripiprazole possibly reduced by efavirenz and nevirapine. Metabolism of aripiprazole possibly inhibited by amprenavir, atazanavir, fosamprenavir, indinavir, lopinavir, nelfinavir, ritonavir, saquinavir (reduce dose of aripiprazole). Plasma concentrations of antipsychotics possibly increased by ritonavir. There is an increased risk of coma when ritonavir is prescribed concomitantly with risperidone. Lopinavir + ritonavir decrease levels of clozapine and olanzapine. Use of risperidone decreases the effect of these two antiretrovirals, can lead to reversible coma and increases propensity for extrapyramidal side effects. Increased risk of ventricular arrhythmias when clozapine, haloperidol or phenothiazines are given with saquinavir – avoid concomitant use. Specialist advice should be obtained when clozapine and antiretrovirals are concurrently prescribed as some combinations may be contraindicated (agranulocytosis, QT prolongation) and therefore prescribed off-label. Differing antiretrovirals may increase or decrease clozapine serum levels.
Antipsychotics and atomoxetine
Increased risk of ventricular arrhythmias when antipsychotics that prolong the QT interval are given with atomoxetine.
Antipsychotics and beta-blockers
Increased risk of ventricular arrhythmias particularly when sotalol is given with zuclopenthixol, haloperidol, amisulpride, phenothiazines and risperidone.
Antipsychotics and medicines with Immunosuppressant activity.
Clozapine is contraindicated with some medicines with immunosuppressant activity e.g. carbamazepine, chloramphenicol, carbimazole, penicillamine, phenylbutazone, sulphonamides, cytotoxic agents and depot antipsychotic medicines.
Antipsychotics and lithium.
Increasing lithium levels has a direct neurotoxic effect, including increased risk of neuroleptic malignant syndrome (NMS), particularly with clozapine, haloperidol and phenothiazines, flupenthixol, zuclopenthixol. Possible risk of toxicity when given with olanzapine or sulpiride. Lithium increases both neutrophil and WCC and has been used to maintain clozapine treatment in patients who have developed neutropenia. Lithium does not seem to protect against true-induced agranulocytosis. See the trust clozapine treatment guidelines.
Antipsychotics and other medicines.
The following medicines have been associated with QT prolongation and so could have synergistic effect- amantadine, ciclosporin, diphenhydramine, hydroxyzine, nicardipine, tamoxifen.
Antipsychotics and smoking.
Patients diagnosed with schizophrenia who smoke tend to require higher doses of antipsychotics than non smokers. It can be dangerous for patients prescribed clozapine to stop smoking3. On average, starting and stopping smoking doubles or halves the clozapine dose requirements. On smoking cessation, consider reducing the dose by 25% over one week. The plasma level should be repeated after stopping. Anticipate further dose reductions. The use of nicotine replacement therapy does not compensate for this interaction. See the trust clozapine treatment guidelines.
NB: This list is not exhaustive. Further information may be obtained by consulting the BNF or contacting the Pharmacy Department.

9 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
Appendix 7: Positive cardiometabolic health resource. Lester UK adaptation. 2014.

10 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019

11 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019

12 ANTIPSYCHOTIC PRESCRIBING GUIDELINES_PHA35_JANUARY 2019
https://www.rcpsych.ac.uk/pdf/e-version%20NICE%20Endorsed%20Lester%20UK%20adaptation2%20.pdf. It can be accessed via the Royal College of Psychiatrists: https://www.rcpsych.ac.uk/quality/nationalclinicalaudits/schizophrenia/nationalschizophreniaaudit/nasresources.aspx#CMH