Embed Size (px)
Citation preview

Florida International UniversityFIU Digital Commons
FIU Electronic Theses and Dissertations University Graduate School
7-1-2016
Anxiety and Callous-Unemotional Traits:Physiological and Behavioral Responses to Others'DistressKathleen I. CrumFlorida International University, [email protected]
DOI: 10.25148/etd.FIDC000726Follow this and additional works at: https://digitalcommons.fiu.edu/etd
Part of the Child Psychology Commons, and the Clinical Psychology Commons
This work is brought to you for free and open access by the University Graduate School at FIU Digital Commons. It has been accepted for inclusion inFIU Electronic Theses and Dissertations by an authorized administrator of FIU Digital Commons. For more information, please contact [email protected].
Recommended CitationCrum, Kathleen I., "Anxiety and Callous-Unemotional Traits: Physiological and Behavioral Responses to Others' Distress" (2016).FIU Electronic Theses and Dissertations. 2599.https://digitalcommons.fiu.edu/etd/2599
FLORIDA INTERNATIONAL UNIVERSITY
Miami, Florida
ANXIETY AND CALLOUS-UNEMOTIONAL TRAITS: PHYSIOLOGICAL AND
BEHAVIORAL RESPONSES TO OTHERS’ DISTRESS
A dissertation submitted in partial fulfillment of
the requirements for the degree of
DOCTOR OF PHILOSOPHY
in
PSYCHOLOGY
by
Kathleen Isabel Crum
2016
ii
To: Dean Michael R. Heithaus
College of Arts, Sciences and Education
This dissertation, written by Kathleen Isabel Crum, and entitled Anxiety and Callous-
Unemotional Traits: Physiological and Behavioral Responses to Others' Distress, having
been approved in respect to style and intellectual content, is referred to you for judgment.
We have read this dissertation and recommend that it be approved.
_______________________________________
Stacy L. Frazier
_______________________________________
Maureen C. Kenny
_______________________________________
Erica D. Musser
_______________________________________
Jonathan S. Comer, Major Professor
Date of Defense: July 1, 2016
The dissertation of Kathleen Isabel Crum is approved.
_______________________________________
Dean Michael R. Heithaus
College of Arts, Sciences and Education
_______________________________________
Andrés G. Gil
Vice President for Research and Economic Development
and Dean of the University Graduate School
Florida International University, 2016

iii
© Copyright 2016 by Kathleen Isabel Crum
All rights reserved.

iv
DEDICATIONS
To my loving family, a team I would never trade; to my dear friend Tiffany, who
crosses this finish line with me in my heart; and to everyone in the arena, wondering how
much they dare to achieve.

v
ACKNOWLEDGMENTS
I am immensely grateful for the support and guidance provided by mentors,
committee members, colleagues, and friends throughout this process. Without my major
professor, Dr. Jonathan Comer—who helped me realize my potential and taught me to
never give up—and my team of dedicated research assistants, Christina Flores and
Michelle Lorenzo, this project would not have been possible.
This project was generously supported by an Elizabeth Munsterberg Koppitz
Fellowship in Child Psychology, awarded to Kathleen Isabel Crum by the American
Psychological Foundation (APF). Study findings and conclusions are those of the author,
and do not necessarily represent the views of the APF.
vi
ABSTRACT OF THE DISSERTATION
ANXIETY AND CALLOUS-UNEMOTIONAL TRAITS: PHYSIOLOGICAL AND
BEHAVIORAL RESPONSES TO OTHERS’ DISTRESS
by
Kathleen Isabel Crum
Florida International University, 2016
Miami, Florida
Professor Jonathan S. Comer, Major Professor
Research documents considerable anxiety-related heterogeneity in youth with callous-
unemotional traits (CU), a pattern of callousness and shallow emotionality (Frick & Ellis,
1999) associated with lasting impairment (Fontaine et al., 2011). This heterogeneity may
relate to behavioral differences, with the presence of both CU and anxiety associated with
increased questionnaire-based reports of aggression and/or historical documentations of
past aggression (Kahn et al., 2013). Anxiety in CU youth is associated with greater
attention to others’ distress cues (Kimonis et al., 2012) compared to CU-only
counterparts, in contrast to the decreased distress-cue attentiveness thought to contribute
to aggression in CU youth (Dadds et al., 2011). Through its association with
improvements in CU youths’ ability to detect others’ distress, anxiety may heighten
autonomic activity associated with emotional processing, in contrast to the dampened
autonomic activity observed in CU youth (de Wied et al., 2012). It is possible that CU
associations with distress-cue recognition and parasympathetic-based emotion-regulation
vary as a function of anxiety, and in turn are associated with aggression. The present
study, conducted with a sample of youth ages 7-13 (N=45), incorporated laboratory tasks
vii
and self- and caregiver-report questionnaires to assess the extent to which child anxiety,
traumatic stress, CU, and their interactions, predict observed aggressive behavior toward
other children and perceptions of others’ emotions while experimentally manipulating
distress-cue salience. Exploratory analyses considered parasympathetic activity that may
associate with observed relationships. Overall, results align with non-experimental
research suggesting that CU is associated with greater aggression in the presence of
anxiety (Fanti et al., 2013), and clarify that anxiety moderates the effect of CU on
aggression, but only in the absence of distress cues from a potential victim. Results also
hint that relationships between anxiety and parasympathetic responses to others’ distress
may help explain anxiety-related heterogeneity in CU youths’ aggression. Findings
suggest that children with CU and anxiety may benefit from emotional training to
anticipate others’ distress and identify distress cues. In aggressive situations involving
these youth, increasing others’ distress-cue salience may attenuate violence. Future
research must further investigate emotional processing deficits, and their role in the
development of aggression, among CU youth with anxiety.
viii
TABLE OF CONTENTS
CHAPTER PAGE
I. INTRODUCTION .............................................................................................1
CU Traits ............................................................................................................1
Heterogeneity in CU ..........................................................................................2
CU and Anxiety .................................................................................................3
Anxiety and Emotional Processing in CU .........................................................5
Impact of anxiety on attention biases in CU ................................................7
Links between anxiety and physiological response in CU ..........................8
Impact of anxiety on behavioral and physiological responses to others’
distress in CU ...............................................................................................9
Project Aims and Hypotheses ..........................................................................10
II. METHODOLOGY ..........................................................................................15
Participants and Recruitment ...........................................................................15
Procedures and Measures .................................................................................16
Analytic Plan ....................................................................................................22
III. RESULTS ........................................................................................................24
Addressing Aim Ia: Elucidating the interactive effects of CU and anxiety
on aggression ...................................................................................................25
Addressing Aim Ib: Elucidating the interactive effects of CU and traumatic
stress on aggression..........................................................................................25
Addressing Aim IIa: Investigating the interactive effects of CU and anxiety
on aggression in the presence versus absence of distress cues ........................25
Addressing Aim IIb: Investigating the interactive effects of CU and
traumatic stress on aggression in the presence versus absence of distress
cues ..................................................................................................................28
Addressing Aim IIIa: Elucidating the main and interactive effects of CU
and anxiety on perceptions of a potential victim’s emotional state in an
experimental context ........................................................................................28
Addressing Aim IIIb: Investigating the main and interactive effects of CU
and traumatic stress on perceptions of a potential victim’s emotional state
in an experimental context ...............................................................................30
Addressing Aim IVa: Elucidating the main and interactive effects of CU
and anxiety on parasympathetic response to others’ distress...........................31
Addressing Aim IVb: Elucidating the interactive effects of CU and
traumatic stress on parasympathetic-based response to others’ distress ..........33
IV. DISCUSSION ..................................................................................................33
Overview ..........................................................................................................33
Aggression .......................................................................................................34
Perceptions of Peer Emotions ..........................................................................35

ix
Physiological Responses ..................................................................................36
Trauma-related Findings ..................................................................................37
Clinical Implications ........................................................................................38
Limitations .......................................................................................................38
Future Directions .............................................................................................41
Summary and Conclusions ..............................................................................41
REFERENCES ............................................................................................................43
APPENDICES .............................................................................................................54
VITA ............................................................................................................................81

x
LIST OF TABLES
TABLE PAGE
1. Descriptive statistics……………………….…………………………….….58
2. Zero-order correlations between study variables......…………………….….59
3. Coefficients for the SuperBuilder hierarchical regression models predicting
aggression, with anxiety as moderator……………………………………....60
4. Coefficients for the SuperBuilder hierarchical regression models predicting
aggression, with traumatic stress as aa moderator…………………………..61
5. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the absence of a distress cue, with anxiety as a
moderator………………………………………………..…………………..62
6. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the presence of a distress cue, with anxiety as a
moderator……………………………………………………………...…….64
7. Coefficients for the hierarchical regression models predicting changes in
perceptions of simulated opponent’s emotions, with anxiety as a
moderator…………………………………………………………………....66
8. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the absence of a distress cue, with traumatic stress
as a moderator……………...………………………………………………..68
9. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the presence of a distress cue, with traumatic stress
as a moderator……………………………………………………………….70
10. Coefficients for the hierarchical regression models predicting changes in
perceptions of simulated opponent’s emotions, with traumatic stress as a
moderator…………………………………………………………………....72
11. Coefficients for hierarchical regression models predicting parasympathetic
responses, with anxiety as a moderator……………………………………..74
12. Coefficients for HLM predicting RSADistress scores across time, with CU
and anxiety as moderators…………………………….…………………….75
13. Coefficients for hierarchical regression models predicting parasympathetic
responses, with traumatic stress as a moderator…………….…………..….76
xi
14. Coefficients for HLM predicting RSADistress across time, with CU and
traumatic stress as moderators……………………………...………………77

xii
LIST OF FIGURES
FIGURE PAGE
1. Excerpts from the SuperBuilder game play simulation. Participants were
told they were building the red brick skyscraper, while their opponent was
building the yellow skyscraper……………………………………...……….55
2. Explanation of SuperBuilder sound blast levels presented to the child
participant……………………………………………………………………56
3. Neutral and distress messages, respectively, sent from the SuperBuilder
simulated opponent to the child participant………………………..………...57
4. Visual depiction of statistical models………………………………..……....78
5. Graph depicting the interactive relationship between CU and anxiety when
predicting aggression in the absence of a distress cue…………………….....79
6. Graph depicting the relationships between respiratory sinus arrhythmia and
caregiver-reported child anxiety scores on the MASC across the five
distress-condition epochs in the Distress Response task………...…………..80
xiii
LIST OF ACRONYMS AND ABBREVIATIONS
American Psychiatric Association APA
Antisocial behavior AB
Attention Deficit-Hyperactivity Disorder ADHD
Callous-unemotional traits CU
Central nervous system CNS
Child PTSD Symptom Scale CPSS
Conduct problems CP
Electrocardiogram EKG
Full-scale Intelligence Quotient FSIQ2
Hierarchical linear modeling HLM
Hostile attribution bias HAB
Inventory of Callous-Unemotional Traits ICU
Lower limit of 95% confidence interval LLCI
Medium Med
Missing completely at random MCAR
Multidimensional Anxiety Scale for Children, Second Edition MASC
Parasympathetic nervous system PNS
Peer Perception Scale PPS
Posttraumatic Stress Disorder PTSD
Respiratory sinus arrhythmia RSA
Standard deviation SD
Standard error SE
Statistical Package for the Social Sciences SPSS

xiv
Upper limit of 95% confidence interval UCLI
Wechsler Abbreviated Scale of Intelligence, Second Edition WASI-II

1
I. INTRODUCTION
Research documents considerable heterogeneity in youth presenting with callous-
unemotional (CU) traits, a pattern characterized by callousness, shallow emotionality,
and a lack of guilt following transgressions (CU; Frick & Ellis, 1999). Empirical work
suggests that anxiety-related heterogeneity in youth showing CU traits may be related to
meaningful differences in associated aggressive behavior, with the presence of both CU
traits and anxiety associated with a specific pattern of emotional processing deficits and
higher levels of aggression than children with just CU traits (Docherty, Boxer,
Huesmann, O’Brien, & Bushman, 2015; Euler et al., 2015; Fanti, Demetrious, &
Kimonis, 2013; Humayun, Kahn, Frick, & Viding, 2014; Kahn et al., 2013; Kimonis,
Skeem, Cauffman, & Dmitrieva, 2011; Lee, Salekin, & Iselin, 2010; Rosan, Frick,
Gottlieb, & Fasicaru, 2015). However, much of this research has relied exclusively on
questionnaire reports of aggressive behavior rather than observed aggressive behavior
(e.g., Kimonis et al., 2011; Lee et al., 2010), and has not examined how anxiety and CU
traits predict child aggression in the context of experimentally manipulated distress cue
salience from potential victims. Much remains to be learned about the processes
underlying observed associations between anxiety, CU traits, and aggressive behavior
among youth in order to optimally inform taxonomy questions and intervention efforts.
CU Traits
Considerable evidence documents the occurrence of children with serious
behavior problems who exhibit callousness, shallow emotionality, and a lack of guilt
following transgressions (i.e., CU traits; Frick & Ellis, 1999). Such CU traits constitute a
2
profile now recognized in leading psychiatric taxonomies (e.g., American Psychiatric
Association [APA], 2013), affect roughly one-third of youth with behavior problems
(Christian et al., 1997), and are associated with significant social and behavioral
impairment across the lifespan (Fontaine et al., 2011; Lynam et al., 2007; Obradovic,
Pardini, Long, & Loeber, 2007), and although they have been traditionally
conceptualized in the context of conduct disorder, emerging empirical work supports
consideration of CU traits as a transdiagnostic construct (Herpers, Rommelse, Bons,
Buitelaar, & Scheepers, 2012; Herpers, Klip, Rommelse, Greven, & Buitelaar, 2016;
Moran et al., 2009).
There is now strong evidence that children showing CU traits differ in important
ways from children with behavioral problems who do not show CU traits, and from
children without behavioral problems. For example, relative to peers, CU youth exhibit
antisocial behavior (AB) that is more severe, stable, and varied in nature (Frick, Kimonis,
Dandreaux, & Farell., 2003b; Frick & Dantagnan, 2005), show higher levels of reactive
(lashing out in response to perceived provocation) and proactive (calculated, goal-
directed aggression in the absence of anger; Dodge & Coie, 1987) aggression (Fanti,
Frick, & Georgiou, 2009; Lozier, Cardinale, VanMeter, & Marsh, 2014; Marsh et al.,
2013; Waschbusch et al., 2004), and show diminished or varied responsiveness to
traditional behavioral treatments targeting AB (Hawes, Price, & Dadds, 2014b;
McDonald et al., 2011; Waschbusch et al., 2007) relative to children without CU traits.
Heterogeneity in CU
Much remains to be learned about pathways leading to AB among youth showing
CU traits. Given physiological, temperamental, and cognitive differences associated with
3
CU, it has been proposed that the AB of children with CU arises from a separate pathway
relative to the AB of children without CU (Frick et al., 2003a). Moreover, it is unclear
whether the same mechanisms underlie AB development for all children with CU, or
whether multiple distinct pathways systematically eventuate in CU profiles. Through its
relationship with causal pathways to AB, heterogeneity associated with underlying
processes in CU likely contributes to mixed intervention response.
CU and Anxiety
Evidence suggests that children with CU constitute a heterogeneous population, with
some but not all susceptible to anxiety, which in turn is associated with increased
dysfunction and impairment. Importantly, analogous to primary and secondary variants of
psychopathy in adults (Karpman, 1948; Skeem, Poythress, Edens, Lilienfeld, & Cale,
2003), whereas the majority of youth showing CU traits do not show elevated levels of
anxiety, a subset of CU youth do, and elevated anxiety appears to alter the presentation of
CU traits in several key ways. Among children with CU, anxiety has been associated with
greater questionnaire-based reports of impulsivity and externalizing behavior problems,
as well as higher reports of aggression and delinquency (Kahn et al., 2013; Rosan et al.,
2015; Vaughn et al., 2009), especially reactive aggression (Fanti et al., 2013), a more
extensive criminal offense record (Kimonis et al., 2011), and increased reports of
depressive and psychotic symptoms (Docherty et al., 2015; Vaughn et al., 2009) relative
to CU youth without anxiety. These anxiety-related differences hold true despite
comparable levels of CU traits, although some studies have noted increased (Kimonis et
al., 2011; Lee et al., 2010) or decreased (Euler et al., 2015) CU trait severity among youth
who show anxiety symptoms relative to CU youth without anxiety. Anxiety may interact

4
with CU in important ways, but the nature of such interactions and their impact on youth
aggressive behavior remain unclear, impeding the identification of tailored treatment
targets, and hindering efforts to address the unique needs of children at various points on
these continua. Moreover, and importantly, research examining interactions between CU
and anxiety and their effects on AB has relied almost exclusively on questionnaire reports
of child aggressive behavior (e.g., Fanti et al., 2013; Kahn et al., 2013, Rosan et al.,
2015), and the studies that used criminal records did not assess aggression in an
experimental context (e.g., Kimonis et al., 2011; Lee et al., 2010), which limits
interpretations and cannot rule out issues related to reporter biases, shared method
variance, and external circumstances.
Of note, several studies have observed greater trauma exposure among CU youth
experiencing anxiety symptoms relative to their counterparts without anxiety (Euler et al.,
2015; Kahn et al., 2013; Kimonis et al., 2012; Tatar et al., 2012). Trauma is central to
theory underlying origins of primary and secondary variants in psychopathy (e.g., Porter,
1996), and may be a particularly relevant factor in the affective and behavioral
characteristics of children with CU and anxiety, considering research suggesting that
traumatic stress-related emotional numbing symptoms link violence exposure and
delinquency (Allwood, Bell, & Horan, 2011), and often co-occur with
hypervigilance/hyperarousal symptoms (Weems, Saltzman, Reiss, & Carrion, 2003).
Furthermore, trauma-exposed youth show a specific pattern of emotional processing
abnormalities, including an attentional bias towards threat (Dalgleish, Moradi, Taghavi,
Neshat-Doost, & Yule, 2001), enhanced identification of fearful faces (Masten et al.,
2008), and heightened sympathetic nervous system activity (see Teicher, Andersen,

5
Polcari, Anderson, & Navalta, 2002). It is worthwhile to assess the degree to which the
aggressive reactivity and internalizing symptoms (e.g., Docherty et al., 2015; Fanti et al.,
2013) reported by CU youth experiencing anxiety symptoms may actually represent
traumatic stress symptoms. Thus far, trauma exposure and traumatic stress symptoms
have been examined as clinical correlates differentiating variants of CU youth with
respect to anxiety (e.g., Humayun et al., 2013; Kimonis et al., 2012); the potential for
traumatic stress to moderate the link between CU and observed aggression in the context
of experimentally manipulated distress cues has not been explored.
Anxiety and Emotional Processing in CU
Anxiety-related variations in CU presentation may be a result of differences in
emotional processing across affected youth, as deficits in emotional processing are
thought to facilitate the development of AB, including aggression, in CU youth (Blair et
al., 2006). Child CU traits are associated with deficits in distress cue detection and
recognition, as well as emotional responding (e.g., Blair et al., 2005; Muñoz, 2009;
Woodworth & Waschbusch, 2008) that are susceptible to correction via increases in
distress cue salience (Dadds et al., 2006; Dadds, El Masry, Wimalaweera, & Guastella,
2008; van Baardewijk et al., 2009). Child CU traits have also been associated with
deficits in physiological reactions to distress-related cues as indexed by correlates of
parasympathetic and sympathetic activity, an important factor in emotional responding
(e.g., Blair et al., 2005; de Wied, van Boxtel, Matthys, & Meeus, 2012). These deficits in
recognizing and responding to others’ emotions correspond with reported deficiencies in
cognitive and affective empathy (e.g., Dadds et al., 2009)—the ability to identify and
match others’ emotional states, respectively (see Hoffman, 1984).
6
Attention to, and interpretation of, others’ emotions influences affective matching
of emotional states and, ultimately, emotional responding (Eisenberg et al., 2009; 2010).
In addition to deficiencies in cognitive empathy—that is, accurately identifying others’
distress-related emotions (Eisenberg & Fabes, 1990; Hoffman, 1984)—CU youth show a
pattern of hostile social cognition (see Frick, Ray, Thornton, & Kahn, 2014 for a review).
Youth with CU traits downplay the effects of their aggression on victims in hypothetical
conflict situations, reporting less concern for victims’ suffering, and endorsing social
goals focused on dominance and forced respect (Pardini, 2011; Pardini & Byrd, 2012).
When children with CU experience anxiety symptoms, they may be particularly at risk
for difficulties accurately identifying others’ emotions, as anxiety is associated with its
own unique pattern of social-cognitive biases, including biased attention towards threat-
related stimuli (Taghavi, Moradi, & Neshat-Doost, Yule, & Dalgleish, 2000) and a
tendency to interpret neutral stimuli as negative or threatening (Reid, Salmon, &
Lovibond, 2006). Although Kimonis and colleagues (2012) examined attention to distress
cues among children with CU and anxiety using distressing pictures in a dot-probe task,
the extant literature on anxiety in children with CU traits has not investigated perceptions
of peer emotion in experimental tasks approximating social interactions.
Understanding these emotional deficits is essential to prevention of AB among
children with CU traits, and research has shown the importance of potential victims’
distress cue salience in reducing emotion recognition deficits and altering aggressive
behavior in CU youth. Increased salience of others’ emotional cues has been linked to
increased accuracy of emotion recognition among CU youth, perhaps as a function of
attention to distress cues (Dadds et al., 2012). Indeed, when children are specifically
7
instructed to attend to emotional cues indicating others’ distress, and when distress cue
salience itself is increased (Blair, Colledge, Murray, & Mitchell, 2001), discrepancies in
distress-related emotion recognition between youth with and without CU traits are
reduced (Dadds et al., 2008). Increases in others’ distress cue salience have also been
associated with a decrease in the strength of the relationship between CU traits and
aggression (van Baardewijk et al., 2009). However, it remains unclear how anxiety-based
heterogeneity may affect associations between CU, aggression, others’ distress cue
salience, and physiological and behavioral responses to others’ emotions, as well as
perceptions of others’ emotions.
Impact of anxiety on attention biases in CU.
By signaling the potential for a variety of links between emotional processing and
CU traits, anxiety-based differences in attention to others’ distress cues may have
important implications for understanding links between CU and aggressive behavior, and
for developing informed treatment targets. Indeed, evidence suggests that anxiety in CU
youth alters emotional processing, and points to variation in the processes underlying the
cognitive, temperamental, and behavioral styles typical to CU traits. Among youth with
high levels of CU, anxiety is associated with greater attention to others’ distress cues
(Kimonis, Frick, Cauffman, Goldweber, & Skeem, 2012) than CU-only counterparts, in
contrast to the decreased attentiveness to these cues thought to contribute to AB in CU
youth (Dadds et al., 2011). Only one existing study has examined attention to others’
distress cues as a function of CU and anxiety (Kimonis et al., 2012), and while Kimonis
and colleagues’ findings provide preliminary information on patterns of emotional
deficits among CU youth, further research incorporating observational paradigms is
8
needed to examine how such anxiety-CU interaction patterns may influence
corresponding behavioral heterogeneity.
Links between anxiety and physiological response in CU.
Attentional differences accompanying anxiety in children with CU may be
directly associated with corresponding differences in physiological processes, which may
in turn affect clinical presentation and intervention response. Despite the lack of research
in this area, anxiety in CU youth may result in distinct physiological profiles in response
to others’ distress. As anxiety is associated with improvements in the ability of CU youth
to detect others’ distress cues (Kimonis et al., 2012), anxiety may indirectly heighten
related autonomic activity associated with emotional processing, in contrast to the
dampened parasympathetic and sympathetic activity typically observed in CU youth
(e.g., Anastassiou-Hadjicharalambous & Warden, 2008b; Blair, 1999; de Wied et al.,
2012; Muñoz, Frick, Kimonis, & Aucoin, 2008). Further, neural abnormalities in the
form of limited amygdala function (e.g., Blair et al., 2006; Jones, Laurens, Herba, Barker,
& Viding, 2009; Lozier et al., 2014) are associated with the “fearlessness” commonly
ascribed to youth with high levels of CU (e.g., Pardini, 2006). Fearlessness is
contradictory, however, to the worry and fears associated with chronic, trait-like anxiety
in youth with CU (e.g., Fanti et al., 2013). It may be that anxiety lessens these CU-related
abnormalities, reducing the blunted parasympathetic and sympathetic activity observed in
non-anxious children with CU traits. Thus far, no research has explored relationships
between CU, anxiety, and physiological response to others’ distress.
9
Impact of anxiety on behavioral and physiological responses to others’ distress in
CU.
Considering the potential and observed alterations in emotional processing
associated with anxiety in children with CU, it is possible that CU associations with
distress cue recognition and with physiological correlates of emotional response and
regulation vary as a function of anxiety, and in turn are associated with aggressive
behavior in important ways. Emotional processing and physiological correlates appear to
play a central role in driving behavioral responses to fear or distress in other individuals.
Indeed, accurate emotion identification and optimal levels of affective arousal—
facilitated by matching of affective states—are required to elicit prosocial responses to
others’ distress such that a lack of affective arousal—that is, an affective response to
others’ distress, thought to be facilitated by physiological activity—precludes prosocial
behavior (Eisenberg & Fabes, 1990; Eisenberg et al., 2010). On the other hand, overly
high levels of affective arousal are associated with personal distress, which may even
encourage aggressive behavior towards the perceived cause of distress, or withdrawal
from the distressing stimulus (Eisenberg & Eggum, 2009; Eisenberg et al., 2010). If
anxiety enables children with CU to attend to and recognize others’ distress more easily,
or enables children with CU to experience heightened physiological response to others’
distress, differences in behavior should be apparent; however, the manner in which
differences in emotional processing associated with anxiety are linked to aggressive
behavior is thus far unexamined. Importantly, existing research on relationships between
CU, anxiety, and aggression has relied almost exclusively on questionnaire measures,
rather than observed measures of aggression (e.g., Rosan et al., 2015), and no existing
10
research has examined these relationships in an experimental context; thus the complex
interplays between these factors remain unclear.
Improved understanding of the potential pathways by which emotional processing
is linked to aggression among children with CU and anxiety may lie in investigating the
role of distress cue salience (e.g., Kimonis et al., 2012). By intensifying others’ emotional
cues and reducing their ambiguity, increases in the salience of distress cues may
influence the manifestation of aggression among children with CU and anxiety.
Experimental manipulation of distress cues in the context of social interaction is needed
to clarify the role of emotional processing in the heightened aggression documented in
children with CU and anxiety. Given this theoretical and empirical background, it is
possible that anxiety significantly alters the relationship between CU and empathy-related
responding, shaping underlying processes that contribute to behavioral and social
impairment.
Project Aims and Hypotheses
The overall goal of this work is to examine the complex interplays between child
CU and anxiety in predicting aggressive behavior, to examine how the salience of others’
distress cues affects links between CU, anxiety, and aggression, and to consider
physiological processes—specifically, parasympathetic activity associated with emotion
regulation—that may correlate with such associations. The research incorporated an
experimental manipulation in a sample of youth ages 7 to 13 (N=45), incorporating
laboratory tasks and self- and caregiver-report questionnaires to assess the extent to
which child anxiety, traumatic stress symptoms, CU traits, and their interactions, predict
observed aggressive behavior toward other children and perceptions of others’ emotions
11
while experimentally manipulating the salience of distress cues from the other child.
Observations of aggressive behavior were collected in the context of a competitive game
simulation in which, unbeknownst to participating youth, the opponent child against
whom participants could aggress was in fact a programmed computer simulation.
Exploratory analyses further considered parasympathetic functioning and regulation that
may associate with observed relationships. By enhancing the field’s understanding of
anxiety-related heterogeneity and its interaction with CU, and examining the intricate
relationships between underlying attentional and physiological processes and aggression
in children, the current study can meaningfully advance theoretical models of CU and lay
an empirical foundation for targeted treatment development. Further, the current study
can lay the groundwork for future translational investigations of physiological processes
mediating emotional processing abnormalities in CU youth.
•Aim Ia: Elucidate the interactive effects of CU and anxiety on behaviorally
observed aggression in an experimental context. Hypothesis: Given the growing body of
literature documenting a subset of children with CU traits who show significant anxiety
and increased questionnaire-based reports of aggression (e.g., Docherty et al., 2015,
Rosan et al., 2015) and more extensive criminal records (Kimonis et al., 2011), it was
hypothesized that child anxiety will moderate the impact of CU severity on behaviorally
observed aggression (regardless of distress cue salience), such that higher levels of child
anxiety would be associated with a stronger link between CU and observed aggression.
•Aim Ib: Elucidate the interactive effects of CU and traumatic stress symptoms on
behaviorally observed aggression. Hypotheses: Given research documenting more
extensive trauma histories among children with CU and anxiety than their CU-only
12
counterparts (e.g., Euler et al., 2015), along with literature indicating potential overlap
between callousness and posttraumatic emotional numbing symptoms (Allwood et al.,
2011), it was hypothesized that among trauma-exposed youth, traumatic stress symptom
severity will moderate the impact of CU severity on behaviorally observed aggression
(regardless of distress cue salience), such that higher levels of traumatic stress would be
associated with a stronger link between CU and observed aggression.
•Aim IIa: Investigate the extent to which the interactive effects of CU and anxiety
on observed aggression vary relative to the salience of a potential victim’s distress.
Hypotheses: It was expected that CU severity would be strongly associated with observed
aggression when the salience of a potential victim’s distress is manipulated to be absent,
but would not be associated with observed aggression when the potential victim’s distress
was manipulated to be salient (van Baardewijk et al., 2009). It was expected that the
predictive value of the interaction between CU and anxiety would differ in the presence
versus absence of others’ distress cues, given the unique pattern of emotional deficits
observed among youth with CU and anxiety (Kimonis et al., 2012).
•Aim IIb: Investigate the extent to which the interactive effects of CU and
traumatic stress symptoms on observed aggression vary relative to the salience of a
potential victim’s distress. Hypotheses: It was expected that the predictive value of the
interaction between CU and traumatic stress symptoms would differ in the presence
versus absence of others’ distress cues, given the trauma histories reported among youth
with CU and anxiety (e.g., Kahn et al., 2013), and the emotional deficits observed among
youth with posttraumatic stress (e.g., Dalgleish et al., 2001; Masten et al., 2008).

13
•Aim IIIa: Elucidate the main and interactive effects of CU and anxiety on
perceptions of a potential victim’s emotional state in an experimental context.
Hypothesis: Given research documenting reductions in emotion recognition deficits (e.g.,
Dadds et al., 2006) with increased distress cue salience among CU youth, it was expected
that CU severity would not be associated with ratings of the simulated opponent’s affect
ratings in the absence of a distress cue, but that in the presence of a distress cue, CU
severity would be associated with increased ratings of the simulated opponent’s negative
affect, and decreased ratings of the simulated opponent’s neutral and positive affect. It
was further expected that anxiety would moderate the effect of CU severity on ratings of
the simulated opponent’s distress-related emotions. Specifically, it was predicted that
higher levels of child anxiety would be associated with a stronger link between CU and
ratings indicating the simulated opponent’s negative affect, such that greater anxiety was
associated with higher ratings of these emotions, given literature indicating increased
attention to distress cues (Kimonis et al., 2012) among children with CU and anxiety. It
was also expected that CU severity would be associated with changes in ratings of the
opponent’s negative affect, but that anxiety would moderate the effect of CU severity on
such changes. Specifically, it was predicted that higher levels of child anxiety would be
associated with a stronger link between CU and changes in perceptions of opponents’
negative affect, given the increased attention to distress cues (Kimonis et al., 2012)
observed among children with CU and anxiety.
•Aim IIIb: Investigate the main and interactive effects of CU and traumatic stress
on perceptions of a potential victim’s emotional state in an experimental context.
Hypothesis: Given literature documenting enhanced identification of fearful faces among
14
trauma-exposed youth (Masten et al., 2008), it was expected that traumatic stress would
moderate the effect of CU severity on ratings of the simulated opponent’s negative affect.
Specifically, it was predicted that higher levels of child traumatic stress would be
associated with a stronger link between CU and ratings of the simulated opponent’s
negative affect, such that greater traumatic stress was associated with higher ratings of
these emotions. It was also expected that child traumatic stress would moderate the effect
of CU severity on changes in ratings of the opponent’s negative affect, such that higher
levels of traumatic stress would be associated with a stronger link between CU and
changes in perceptions of opponents’ negative affect, given literature linking child
traumatic stress to enhanced identification of others’ fear-related cues (Masten et al.,
2008).
•Aim IVa: Elucidate the interactive effects of CU and anxiety on
parasympathetic-based regulation in response to others’ distress. Hypothesis: It was
expected that CU will be associated with blunted parasympathetic response to others'
distress similar to previous findings (e.g., Anastassiou-Hadjicharalambous & Warden,
2008b; de Wied et al., 2012), but that anxiety would alter this relationship by increasing
parasympathetic response to this stimulus, given that anxiety has been associated with
increased attention to distress cues among CU youth (Kimonis et al., 2012).
•Aim IVb: Elucidate the interactive effects of CU and traumatic stress on
parasympathetic response to others’ distress. Hypothesis: It was expected that traumatic
stress would alter the relationship between CU and blunted parasympathetic regulation by
increasing parasympathetic response to others’ distress, given that traumatic stress has
been associated with both increased attention to distress cues (e.g., Masten et al., 2008)—
15
an emotional processing pattern observed among CU youth (Kimonis et al., 2012)—and
heightened autonomic activity (Teicher et al., 2002).
Gaining a better understanding of the relationships between child anxiety,
traumatic stress, CU, and observed aggressive behavior in the context of experimentally
manipulated distress cue salience is critical to informing individualized treatment
strategies and offsetting future difficulties. As a whole, these efforts can contribute
valuable information to assessment and intervention science, reducing the heavy burden
that CU places on affected individuals, their families, and society at large.
II. METHODOLOGY
Participants and Recruitment
All study activities were approved by the Florida International University
Institutional Research Board. A conduct problems (CP)-enhanced community sample was
recruited, given the relatively low rate of CU in the general community (Rowe et al.,
2010). Specifically, community recruitment of youth included—in addition to broad
school-based and flyer-based recruitment—strategic recruitment outreach at clinics
offering behavioral treatments for child behavior problems. Phone screens were
administered to interested caregivers of potential participants to assess whether children
met the following eligibility criteria: 1) age of seven to thirteen years, inclusive; 2) no
reported history of autism spectrum disorder or severe mental or physical impairments
(e.g., intellectual disability, deafness, blindness); and 3) no current psychotropic
treatment, except for stimulant medications which could be easily discontinued for study
participation. Eligible families were invited to a laboratory visit to complete the
following: 1) informed consent and assent, 2) child laboratory tasks and rating scales, and
16
3) caregiver rating scales. Prior to the visit, families of children taking stimulant
medication were asked to forgo medication administration for a 48-hour washout period.
This period is considered sufficient to preclude stimulant medication effects on tasks
(Greenhill et al., 2001), and has been used in previous research on children’s cognitive
task performance (e.g., Wilson, Mitchell, Musser, Schmitt, & Nigg, 2011).
Participants were 45 children between the ages of seven and thirteen (M=9.89,
SD=1.58; 71.1% boys, 28.9% girls) and their caregivers. Caregivers (90.9% mothers,
6.8% fathers, 2.3% grandmothers) reported on child participants’ emotions and behavior,
as well as demographic information. Regarding race/ethnicity, per caregiver report,
75.6% of child participants were Hispanic, 13.3% were non-Hispanic White, and 11.1%
were non-Hispanic Black. Among families for whom income was reported, 50% of
caregivers reported an annual income of $48,000 or lower, 25% of caregivers reported an
income between $50,000 and $97,000, and 25% of caregivers reported an annual income
of $100,000 or higher. Children recruited from clinics showed no differences from
children recruited from other community sources with regard to gender (χ2(1)=0.65,
p=.42), race/ethnicity (χ2(2)=1.38, p=.50), age (t(43)=-0.33, p=74) and household income
(t(34)=0.13, p=.90).
Procedures and Measures
During the laboratory visit, informed consent and assent was obtained from
caregivers and child participants, respectively. Next, caregivers completed questionnaires
on children’s emotion and behavioral characteristics, while children participated in
several experimental tasks and completed self-report questionnaires. Two laboratory
tasks were used to measure child responses to others' distress, and task order was
17
counterbalanced to control for any potential task sequence effects. The order in which
the laboratory tasks were administered was chosen using a counterbalance sheet, such
that the task order was reversed from the preceding participating, allowing approximately
50% of children to participate in one task first, and 50% of children to participate in the
other task first. Following participation in the laboratory tasks, an intelligence test was
administered to child participants, and then children completed self-report questionnaires.
Lastly, children were de-briefed on the use of deception (as described below) in the
laboratory tasks. Caregivers were compensated with a $25 gift card, and children
received a toy, following completion of all study activities and measures.
Child callous-unemotional traits. Caregiver ratings on the Inventory of Callous
Unemotional Traits (ICU; Essau, Sasagawa, & Frick, 2006) were used to measure child
CU traits. The ICU is a well-established measure of CU traits in this age group, and is
comprised of 24 items rated on a scale from 0 (“Not at all true”) to 3 (“Definitely true”).
Using the original scoring, Kimonis, Fanti, and Singh (2014) found children with a
parent-rated ICU total score of 24 or above would benefit from services tailored towards
CU traits. Numerous studies support the reliability and validity of the ICU, particularly in
distinguishing between CP behaviors and CU (e.g., Fanti et al., 2009; Kimonis et al.,
2008; Kimonis et al., 2014; Roose et al., 2009). Hawes and colleagues (2014a) used
exploratory factor analysis to identify an alternative scoring method that improved the
psychometric properties of the measure. Total scores obtained using Hawes’ et al.’s
alternative scoring method were used in the present analyses. Internal consistency was
acceptable in the current sample (α=.81).
18
Child anxiety. Child anxiety was measured by caregiver ratings on the
Multidimensional Anxiety Scale for Children, Second Edition (MASC; March, Parker,
Sullivan, Stallings, & Conners, 1997; March, 2013). The MASC is comprised of 39 items
on a scale from 0 (“Never true about me”) to 3 (“Often true about me”). The MASC
assesses several domains of anxiety that are summed to yield a total anxiety score. The
test-retest reliability and predictive validity of the MASC have been demonstrated by past
research (e.g., Muris, Merckelbach, Ollendick, King, & Bogie, 2002; Wei et al., 2014).
Internal consistency was very strong in the current sample (α=.92).
Prior child trauma exposure and posttraumatic stress symptoms. In keeping
with previous studies exploring the role of anxiety in CU (e.g., Kimonis et al., 2012),
children completed a self-report measure of trauma exposure and corresponding
posttraumatic stress symptoms. The Child PTSD Symptom Scale (CPSS; Foa et al.,
2001) was used to measure child posttraumatic stress symptoms. First, children were
administered a preliminary trauma exposure questionnaire. A list of the following
potentially traumatic events was provided: a) anything really terrible or upsetting, like
being very sick or badly hurt; b) seen anyone die or badly hurt; c) been in a really bad
accident or fire where you could have died; d) been in anything like a really bad
hurricane, flood, or earthquake or had a tornado near where you lived; e) been robbed or
attacked; f) been touched on parts of your body that you really didn’t want to be touched;
g) been made to touch someone else in places that you didn’t want to; h) been hit over
and over or hurt very badly by someone; i) anything else that someone has done to you,
or made you do, that you didn’t like. Children were asked to select “Yes” or “No” if they
had experienced any of these events (regardless of which, or how many, events they had
19
experienced). If children selected “Yes,” they were asked to complete the CPSS. The
CPSS is composed of 17 symptom-severity items rated from 0 (“Not at all or only at one
time”) to 3 (“5 or more times a week/almost always”), and 7 impairment “Yes” or “No”
items. The symptom severity items comprise several subscales—including re-
experiencing, avoidance, and hyperarousal—that are summed to create a total score. The
test-retest reliability and construct validity of the CPSS have been demonstrated in past
research (Foa et al., 2001; Gillihan, Aderka, Conklin, Capaldi, & Foa, 2013; Nixon et al.,
2013). Internal consistency of the CPSS was very strong in the current sample for the
symptom-severity (α=.92) items.
Child distress-response. The distress-response task was designed to assess
parasympathetic nervous system (PNS) regulation of physiological arousal in response to
the distress of others. Respiratory sinus arrhythmia (RSA; the high-frequency component
of the heart-rate variability spectrum) is an indicator of PNS regulation of physiological
arousal (Hayano et al., 2001; Appelhans & Luecken, 2006). During the task, children
were seated in a comfortable chair and connected to psychophysiological equipment.
Specifically, heart rate was measured using EKG leads applied to the upper right clavicle
and lower left rib, as well as a grounding electrode on the lower right rib. Impedance
cardiography allowed assessment of RSA and respiration using four electrodes. One
electrode was applied over the clavicle close to the neck, and another electrode was
applied to the back of the neck in a corresponding location. Additionally, one electrode
was applied over the xiphoid process, with another electrode applied to a corresponding
location over the spine.

20
Child participants were told they would listen to two recordings, including one
recording of nature sounds, and one recording of another child who was very upset.
Initial recording occurred for five minutes, during which a relaxation soundtrack was
played, to establish a resting baseline. Immediately following the relaxation soundtrack
audio recording, a five-minute audio recording of a distressed child crying was played.
Data collection and analysis occurred through equipment and software from MindWare
Technologies, Ltd. (Gahanna, OH). Respiration and heart rate were used to calculate
heart-rate variability, from which RSA was assessed using spectral analysis. Lower
resting RSA and parasympathetic-based regulation in response to distress cues reflects
reduced parasympathetic activity, a response observed in CU youth in comparison to
youth with behavior problems and healthy controls (Anastassiou-Hadjicharalambous &
Warden, 2008b; de Wied et al., 2012) and ADHD youth with low prosocial behavior, a
proxy for CU traits (Musser, Galloway-Long, Frick, & Nigg, 2013), in comparison to
ADHD youth without low prosocial behavior. Given high correlations across RSAResting
epochs (rs=.68-.90) and RSADistressExposure epochs (r=.78-.90), RSAResting was calculated by
averaging RSA across the five 60-second epochs of data collection during the relaxation
phase, and RSADistressExposure was calculated by averaging RSA across the five 60-second
epochs of data collection during the distress phase. RSAReactivity was calculated by
subtracting RSADistressExposure from RSAResting.
Child aggression. Aggression assessment consisted of a game simulation task
(SuperBuilder) modeled after the FastKid! task developed by Thomaes and colleagues
(2008), and a well-validated protocol used in adults with psychopathy (Giancola &
Zeichner, 1995). The task was designed for the present study to offer a standardized and
21
observational assessment of aggression, as well as changes in aggression with respect to
experimentally manipulated distress cue salience. Participants were told they were going
to play a computer game against another child situated out of sight in a nearby room. In
reality, the experimenter controlled all events, and there was no real child opponent. Prior
to the game, children were told that the goal of the game was to press a specific keyboard
button very quickly to construct buildings at a faster rate than their “opponent”, and that
there are two rounds with several trials each. First- and third-round winners earned the
opportunity to send the opponent a text message. Second- and fourth-round winners
earned the opportunity to “blast” the opponent with white noise. The “opponent” was
rigged to win the first and third round. Figures 1 -3 present several screen shots from the
computer task.
Distress cue salience was manipulated within subjects, with participants receiving
a neutral text message from the competitor following the first round (i.e., “This game is
crazy fast! #JustDoIt” accompanied by a neutral emoticon), and a text message
expressing distress following the third round (i.e., “Super worried about that blast!”
accompanied by a sad emoticon). To ensure that child participants were able to read the
message received from their fictitious opponent, participating youth were asked to read
each message aloud immediately following receipt. Participants were rigged to win the
second and fourth round, were given an example of the noise they could use against their
opponent, with intensities ranging from no noise (level 0) to 100 dB (level 10; intensity
of a smoke alarm), and were told that levels 7 and above are extremely loud. Observed
aggression was measured by noise levels chosen; noise levels from round 2 represent
child aggression in the absence of a distress cue, noise levels from round 4 represent
22
aggression in the presence of a distress cue, and the sum of these noise levels represents
total observed aggression. Participants entered noise levels chosen using the keyboard,
and typed responses were recorded directly into a document. The first response typed was
considered the noise level chosen. Immediately following their entry, children were asked
to confirm the noise level they chosen; each child accurately related his or her typed
choice (r=1.00, p<.001).
Following each round of SuperBuilder, children were administered a peer
perception scale (PPS), in which they rated their perceptions of the intensity of emotions
(i.e., sad, scared, angry, calm, happy) experienced by the fictitious competitor on a scale
from 0 (“Not at all”) to 4 (“Extremely”).
Child intelligence. The Wechsler Abbreviated Scale of Intelligence, Second
Edition (WASI-II; Wechsler, 1999; 2011) was used to measure children’s intelligence.
While the instrument is comprised of four subtests—Block Design, Vocabulary, Matrix
Reasoning, and Similarities, a full-scale IQ (FSIQ2) may be calculated using the Matrix
Reasoning and Vocabulary subtests. The factor structure and validity of the WASI have
been supported (Canivez, Konold, Collins, & Wilson, 2009; Sakolfske, Caravan, &
Schwartz, 2000).
Analytic Plan
Means, SDs, and zero-order correlations among study variables were first
computed. A check was conducted examining the success of tasks’ manipulation of
others’ distress salience. Paired-samples t-tests were conducted examining differences
between the distress and no distress salience conditions with regard to participant reports
on the PPS of how “calm,” “happy,” “angry,” “sad,” and “scared” their opponent was.

23
Regression techniques were used to assess relationships between CU, anxiety, and
physiological, as well as behavioral, responses to others' distress. Prior to conducting the
main analyses, data were checked for normality and other assumptions of regression
models; given the skewed distribution of several study variables and sample size,
bootstrap estimations of population distributions were used to increase confidence in
results (Efron, 1979; Efron & Tibshirani, 1993). Bootstrapping resampling techniques
produce robust standard errors and confidence interval estimates when assumptions of
regression are not met (Bollen & Stine, 1990; Russel & Dean, 2000).
Hierarchical linear regression models were used to assess moderation for study
Aims I-III. Figure 4 depicts the analytical models examined to predict aggression,
changes in child ratings of peer emotions between the neutral and distress messages, and
parasympathetic responses to distress. Moderation analyses were conducted using the
PROCESS macro for SPSS (Hayes, 2012). For each model predicting behavioral or
parasympathetic response outcomes, the main effects of child CU traits and anxiety were
entered, as well as the product term of CU traits and anxiety; parallel models were
created by entering the main effects of child CU traits and traumatic stress, as well as the
product term of CU traits and traumatic stress. Significant moderation is defined by a
significant interaction (product) term of the predictor (CU traits) and proposed moderator
(anxiety or traumatic stress) after accounting for main effects (Baron & Kenny, 1986;
Holmbeck, 1997; Kendall & Comer, 2011). In bootstrapped regression, 95% bias-
corrected confidence intervals, rather than p-values, are used to assess significance;
specifically, the null hypothesis is rejected if zero does not fall within the confidence
interval (Rasmussen, 1987). Variables were mean-centered prior to entry in analyses.

24
Additional moderation analyses predicting parasympathetic responses further
examined whether clinical characteristics differentially predicted participants’
parasympathetic responses to others’ distress unfolding across time. Specifically,
hierarchical linear modeling (HLM) was used to examine whether CU, anxiety, traumatic
stress, and their interactions predicted changes in RSADistress across time during prolonged
exposure to others distress. Separate, parallel models predicting RSADistress across the 5
individual distress-condition epochs (i.e., RSADistress1 through RSADistress5) were created
for anxiety and traumatic stress moderators, such that time, CU, anxiety, and their
interactions were entered as predictors in one model, and time, CU, traumatic stress, and
their interactions were entered as predictors in a second model. RSAResting was entered as
a covariate in both models.
Missing values analyses found no significant differences among participants with
and without missing data on study variables, suggesting that data were missing
completely at random, χ2(168)=190.75, p=.11 (MCAR; Little & Rubin, 1987). Given the
random nature and small overall percentage (1.7%) of missing data, listwise deletion was
used to handle missing observations.
III. RESULTS
Table 1 presents descriptive data for study variables and participant
demographics. Nearly half (45.5%, N=20) of this CP-enhanced community sample
showed significant CU traits according to Kimonis and colleagues’ (2014) criteria (i.e.,
ICU > 24). Roughly 31% (N=14) of the sample showed anxiety in the high-average range
or above (i.e., MASC t score > 55), with approximately 20% (N=9) showing clinically
elevated anxiety (i.e., MASC t score > 60; March, 2013). With regard to trauma, 55.6%
25
(N=25) of the sample experienced a traumatic event; of these children, approximately
31% (N=14) met symptom severity criteria for PTSD (Foa et al., 2001; Hawkins &
Radcliffe, 2006).
Youth were fairly aggressive overall, with only 4.4% (N=2) of children choosing
not to aggress against their opponent at all following receipt of the neutral message, and
only 8.9% (N=4) choosing not to aggress against their opponent at all following receipt
of the distress message. Roughly 71% (N=32) of youth delivered a “blast” at level 7 or
above, which was explained to the participants as “extremely loud” during the game
instructions; this percentage remained the same following receipt of both neutral and
distress messages from the opponent. The number of children selecting the highest
blast—level 10—increased from 23 (approximately 51%) following receipt of a neutral
message to 27 (60%) following receipt of a distress message. Table 2 provides zero-order
correlations for main study variables.
Manipulation checks indicated the task was successful in manipulating the
salience of the opponent distress. A paired-samples t-tests manipulation check revealed
children’s ratings of how “scared” and “sad” they perceived their opponent to be indeed
increased from the no distress/neutral message condition to the distress salience condition
(t(43)=7.75, p<.001, t(43)=5.03, p<.001, respectively). Children’s ratings of how “angry”
they perceived their opponent to be also increased from the no distress/neutral message
condition to the distress salience condition (t(43)=5.90, p<.001). Similarly, children’s
ratings of how “calm” and “happy” they perceived their opponent to be decreased from
the no distress/neutral message condition to the distress salience condition (t(42)=-2.50,
p=.02, t(43)=-7.37, p<.001, respectively).

26
Addressing Aim Ia: Elucidating the interactive effects of CU and anxiety on
aggression
Table 3 presents results from hierarchical regression analyses examining the main
and interactive effects of CU traits and anxiety on total observed child aggression
exhibited during the SuperBuilder game. The overall model was significant in the
prediction of total aggression pooled across the two conditions, F(3, 40)=3.03, p=.04; R2
=0.18. However, neither CU traits nor anxiety significantly predicted total aggression
pooled across the two conditions. Similarly, the product term examining the interactive
effect between CU traits and anxiety did not significantly predict total aggression pooled
across the two conditions.
Addressing Aim Ib: Elucidating the interactive effects of CU and traumatic stress
on aggression
Table 4 presents results from hierarchical regression analyses examining the main
and interactive effects of CU traits and traumatic stress on total observed child aggression
exhibited during the SuperBuilder game. The overall model was not significant in the
prediction of aggression, with F(3, 19)=0.27, p=.85, R2 =0.05.
Addressing Aim IIa: Investigating the interactive effects of CU and anxiety on
aggression in the presence versus absence of distress cues
Table 3 also presents results from hierarchical regression analyses examining the
main and interactive effects of CU traits and anxiety on child aggression exhibited during
the SuperBuilder game, broken down by condition (i.e., presence versus absence of
others’ distress salience).

27
Observed aggression in the absence of a distress cue. The overall model was
significant, F(3, 40)=4.41, p=.01; R2 =0.34. Anxiety and CU traits each significantly
predicted aggression in this condition—explaining 16.2% and 6.5%, respectively, of the
variance in aggression in the absence of a distress cue. As a main effect, CU positively
predicted observed aggression, whereas anxiety as a main effect negatively predicted
observed aggression. In addition, the product term examining the interactive effect
between CU traits and anxiety contributed additional, unique predictive value (F(1,
40)=4.54, p=.04; R2Δ=0.12), indicating that the association between CU traits and
aggression in the absence of a distress cue was not uniform across varying levels of
anxiety.
Follow-up analyses examined simple slopes associated with high, medium, and
low levels of anxiety. High was defined as one standard deviation above the centered
mean anxiety total score, medium was defined as within one standard deviation of the
centered mean anxiety total score, and low was defined as one standard deviation below
the centered mean anxiety total score. Analyses revealed that CU traits were significantly
predictive of increased aggression in the absence of a distress cue among children with
medium and high levels of anxiety (β=0.16, SE=0.06, 95% CI=0.03-0.29 and β=0.37,
SE=0.14, 95% CI=0.10-0.65, respectively). In contrast, CU traits were not predictive of
increased aggression in the absence of a distress cue among children with low levels of
anxiety (β=-0.05, SE=0.09, 95% CI=-0.24-0.14). Figure 5 presents a graphical depiction
of the interactive relationship between CU and anxiety when predicting aggression in the
absence of a distress cue.
28
Observed aggression in the presence of a distress cue. The overall model was
not significant in the prediction of aggression in the presence of a distress cue, F(3,
40)=0.31, p=.82; R2 =0.04. Similarly, neither CU, anxiety, nor their interaction
significantly predicted observed aggression in the presence of a distress cue.
Addressing Aim IIb: Investigating the interactive effects of CU and traumatic stress
on aggression in the presence versus absence of distress cues
Table 4 also presents results from hierarchical regression analyses examining the
main and interactive effects of CU traits and traumatic stress on child aggression
exhibited during the SuperBuilder game, broken down by condition (i.e., presence versus
absence of others’ distress salience).
Aggression in the absence of a distress cue. The overall model was not
significant in the prediction of aggression, with F(3, 19)=0.36, p=.79, R2 =0.05.
Aggression in the presence of a distress cue. The overall model was not
significant in the prediction of aggression, with F(3, 19)=0.25, p=.86, R2 =0.04.
Addressing Aim IIIa: Elucidating the main and interactive effects of CU and anxiety
on perceptions of a potential victim’s emotional state in an experimental context
Tables 5 and 6 present results from hierarchical regression analyses examining the
main and interactive effects of CU traits and anxiety on child ratings of opponent
emotions in neutral and distress cue conditions (respectively) in the SuperBuilder game.
Ratings of opponent emotions in the absence of a distress cue. The overall
models were not significant in predicting child ratings of opponent “calm” (F(3, 38)=0.12
p=.95; R2 =0.01), “happy” (F(3, 39)=1.01, p=.40; R2 =0.06), “angry” (F(3, 39)=1.49,
29
p=.23; R2 =0.11), “sad” (F(3, 39)=0.77, p=.52; R2 =0.04), and “scared” (F(3, 39)=0.20,
p=.90; R2 =0.03) feelings.
Ratings of opponent emotions in the presence of a distress cue. The overall
models were not significant in predicting child ratings of opponent “calm” (F(3,
39)=1.89, p=.15; R2 =0.11), “happy” (F(3, 39)=2.04, p=.12; R2 =0.12), “angry” (F(3,
39)=2.17, p=.11; R2 =0.08), “sad” (F(3, 39)=0.07, p=.97; R2 =0.01), and “scared” (F(3,
39)=1.69, p=.19; R2 =0.09) feelings.
Change in ratings of opponent emotions between neutral- and distress-cue
conditions. Table 7 presents results from hierarchical regression analyses examining the
main and interactive effects of CU traits and anxiety on change in child ratings of
opponent emotions between neutral and distress cue conditions in the SuperBuilder game.
Overall models were not significant in predicting change in ratings of opponent “calm”
(F(3, 38)=1.59, p=.21; R2 =0.09), “scared” (F(3, 39)=0.79, p=.51; R2 =0.07), and “sad”
(F(3, 39)=0.05, p=.98, R2 =0.01) feelings. The overall model was significant in the
prediction of change in ratings of opponent “angry” feelings, F(3, 39)=3.49, p=.02; R2
=0.15. However, neither CU traits nor anxiety significantly predicted change in ratings of
opponent “angry” feelings between the two conditions. Similarly, the product term
examining the interactive effect between CU traits and anxiety did not significantly
predict change in ratings of opponent “angry” feelings between the two conditions. The
overall model was significant in the prediction of change in ratings of opponent “happy”
feelings was significant, F(3, 39)=3.73, p=.02; R2 =0.19. Neither anxiety nor its
interaction with CU traits significantly predicted change in ratings of opponent “happy”
feelings between the two conditions. However, CU traits were a significant negative
30
predictor in this model. Specifically, the greater the child’s CU severity, the less change
in ratings between the neutral- and distress-cue conditions.
Addressing Aim IIIb: Investigating the main and interactive effects of CU and
traumatic stress on perceptions of a potential victim’s emotional state in an
experimental context
Tables 8-9 present results from hierarchical regression analyses examining the
main and interactive effects of CU traits and traumatic stress on child ratings of opponent
emotions in neutral and distress cue conditions in the SuperBuilder game.
Ratings of opponent emotions in the absence of a distress cue. The overall
models were not significant in predicting child ratings of opponent “calm” (F(3,
17)=0.39, p=.76; R2 =0.07), “happy” (F(3, 18)=0.63, p=.61; R2 =0.09), “angry” (F(3,
18)=1.04, p=.40; R2 =0.20), “sad” (F(3, 18)=1.09, p=.38; R2 =0.13), and “scared” (F(3,
18)=0.36, p=.78; R2 =0.12) feelings.
Ratings of opponent emotions in the presence of a distress cue. The overall
models were not significant in predicting child ratings of opponent “happy” (F(3,
18)=1.07, p=.39; R2 =0.12), “angry” (F(3, 18)=0.41, p=.75; R2 =0.10), and “sad” (F(3,
18)=0.37, p=.77; R2 =0.07) feelings. The overall model was significant in the prediction
of ratings of opponent “scared” feelings, F(3, 18)=7.91, p=.001; R2 =0.36. Child CU was
a significant negative predictor, and child traumatic stress was a significant positive
predictor, of ratings of opponent “scared” feelings. Specifically, greater traumatic stress
was associated with higher ratings, and greater CU was associated with lower ratings, of
opponent “scared” feelings. The overall model was also significant in the prediction of
ratings of opponent “calm” feelings, F(3, 18)=4.18, p=.02; R2 =0.46. Child CU was a
31
significant positive predictor of ratings of opponent “calm” feelings. Specifically, greater
CU was associated with higher ratings of opponent “calm” feelings.
Change in ratings of opponent emotions between neutral- and distress-cue
conditions. Table 10 presents results from hierarchical regression analyses examining the
main and interactive effects of CU traits and traumatic stress on change in child ratings of
opponent emotions between neutral and distress cue conditions in the SuperBuilder game.
The overall models were not significant in predicting change in ratings of opponent
“calm” (F(3, 17)=0.87, p=.48; R2 =0.24), “happy” (F(3, 18)=1.95, p=.16; R2 =0.27),
“angry” (F(3, 18)=0.20, p=.90; R2 =0.03), and “sad” (F(3, 18)=0.23, p=.88; R2 =0.08)
feelings. The overall model was significant in the prediction of change in ratings of
opponent “scared” feelings, F(3, 18)=6.97, p=.003; R2 =0.28. However, neither CU traits
nor traumatic stress significantly predicted change in ratings of opponent “scared”
feelings between the two conditions. Similarly, the product term examining the
interactive effect between CU traits and traumatic stress did not significantly predict
change in ratings of opponent “scared” feelings between the two conditions.
Addressing Aim IVa: Elucidating the main and interactive effects of CU and anxiety
on parasympathetic response to others’ distress
Table 11 presents results from hierarchical regression analyses examining the
main and interactive effects of CU traits and anxiety on baseline parasympathetic
functioning (RSAResting) and on parasympathetic response exhibited during the Distress
Task (RSAReactivity). Models were not significant in the prediction of RSAResting, F(3,
39)=0.98, p=.41, R2 =0.09, nor in the prediction of RSAReactivity , F(3, 39)=0.75, p=.53, R2
=.03.

32
Table 12 presents results from HLM analyses examining the main and interactive
effects of CU, anxiety, and their interaction associated with minute-to-minute changes in
RSADistress across time. RSAResting, entered as a covariate, was a significant positive
predictor of RSADistress across time, and the interaction between time and child anxiety
was a significant negative predictor of RSADistress. Time, CU, anxiety, and the interactions
between Time and CU, and Time and the product term of CU and anxiety, were not
significant predictors of in RSADistress.
Follow-up analyses probing the significant AnxietyXTime interaction in the
prediction of RSADistress across time examined RSADistress across time among the
subgroups of youth with high versus low levels of anxiety. High anxiety was defined as
above the mean MASC total score, and low anxiety was defined as below the mean
MASC total score. Among youth with high anxiety, analyses indicated that RSAResting
(the covariate) and Time were significant predictors of RSADistress (B=0.99, SE=0.05,
t(120)=20.45, p<.001 and B=-0.09, SE=0.04, t(120)=-2.16, p=.03, respectively).
Specifically, among youth with higher anxiety, RSADistress declined in a linear fashion
from minute 1 through minute 5 during exposure to others’ distress. In contrast, among
youth with low anxiety, while RSAResting (the covariate) was a significant predictor of
RSADistress (B=0.90, SE=0.05, t(100)=18.83, p<.001), Time was not a significant predictor
(B=-0.004, SE=0.04, t(100)=-0.11, p=.91). That is, among youth with higher anxiety
severity, RSA patterns suggest progressive parasympathetic suppression across time
during exposure to others’ distress, whereas exposure to others distress is not associated
with progressive parasympathetic suppression across time in youth with lower anxiety
severity.
33
Figure 6 presents a graphical depiction of the relationships between anxiety and
RSADistress across time.
Addressing Aim IVb: Elucidating the interactive effects of CU and traumatic stress
on parasympathetic-based response to others’ distress
Table 13 presents results from hierarchical regression analyses examining the
main and interactive effects of CU traits and traumatic stress on baseline parasympathetic
functioning (RSAResting) and on parasympathetic response exhibited during the Distress
Task (RSAReactivity). Models were not significant in the prediction of RSAResting F(3,
19)=0.38, p=.77, R2 =0.03, nor in the prediction of RSAReactivity, F(3, 19)=0.71, p=.56, R2
=.05.
Table 14 presents results from HLM analyses examining the main and interactive
effects of CU, anxiety, and their interaction associated with minute-to-minute changes in
RSADistress across time. Time, CU, traumatic stress, and their interactions were not
significant predictors of RSADistress changes across time.
IV. DISCUSSION
Overview
The present study examined complex relationships between youth CU traits,
observed aggression, anxiety, trauma, perceptions of others’ emotions, and physiological
and behavioral responses to other’s distress. Overall, these results derived from
observational child aggression data are consistent with previous research that has only
utilized questionnaire-based data on child aggression (e.g., Fanti et al., 2013; Humayun et
al., 2013; Rosan et al., 2015) in suggesting that CU traits are associated with greater
aggression in the presence of higher levels of anxiety, and further clarify specific
34
conditions under which this relationship applies. Specifically, the present findings
obtained with an experimental paradigm indicate that anxiety moderates the effect of CU
on child aggression, but only in the absence of salient distress cues from a potential
victim. These findings extend research suggesting that children with CU traits and
anxiety are more aggressive than children with elevated CU but not anxiety, as well as
children low on both CU traits and anxiety (Fanti et al., 2013; Kahn et al., 2012).
Collectively, findings have both theoretical implications for CU traits as a construct, and
clinical relevance in the prevention and situational attenuation of aggression.
Aggression
The present work also adds to an increasing body of research documenting a
strong relationship between CU traits and aggression (e.g., Fanti et al., 2009;
Waschbusch et al., 2004), given that CU traits—and not just their interaction with
anxiety—positively predicted observed aggression towards the opponent when the
opponent’s distress was not apparent. Results further supported the findings of van
Baardewijk and colleagues (2009), who observed in a similar task that the relationship
between CU traits and aggression changes when distress is made salient; however, the
present study was the first to consider the role of anxiety in this relationship.
Theoretical distinctions between children with CU traits and anxiety versus
children with CU traits but no anxiety are supported by the observed interaction. It
appears that anxiety provides useful predictive information on the clinical presentation of
CU traits, particularly in ambiguous social situations during which potential victims’
distress is unclear. Interestingly, although anxiety by itself predicted reduced aggression
under such ambiguous circumstances, anxiety actually sensitized youth with CU to
35
aggress more than seen in CU youth without anxiety. It is possible that the increased
attention to distress cues noted among CU youth experiencing anxiety represents a
sensitivity to negative emotional cues in general, similar to the attentional biases towards
negative- and threat-related cues (Mogg & Bradley, 2005; Reid et al., 2006), and bias
towards interpreting ambiguous information negatively (Taghavi et al., 2000)
documented among anxious children. While CU traits have not previously been
associated with a hostile attribution bias (HAB; Dodge, Price, Bachorowski, & Newman,
1990; Frick et al., 2003a; Helseth, Waschbusch, King, & Willoughby, 2015), perhaps the
combination of cognitive biases associated with anxiety and the callousness of CU traits
yields the impulsive, aggressive reactivity documented in these youth (e.g., Fanti et al.,
2013; Kahn et al., 2013).
Perceptions of Peer Emotions
Indeed, it appears that CU traits are associated with difficulty understanding
others’ emotions, even when distress is made apparent. Youth CU traits were associated
with lower ratings of opponent fear and higher ratings of calm in the presence of a
distress cue from the opponent, as well as less change in participant ratings of perceived
opponent happiness from the neutral to distress message during the SuperBuilder task.
These findings support previous literature documenting that increased distress cue
salience reduces—but does not eliminate—emotion recognition deficits associated with
CU, as well as a tendency for CU youth to minimize victim distress resulting from
aggression (Pardini & Byrd, 2012). Importantly, in the present experimental study,
distress was salient enough to reduce the impact of CU on observed aggressive behavior,
regardless of perceived opponent emotion. The reduced impact of CU on aggression,
36
regardless of perceived emotion of the opponent, suggests the potential for effecting
change on a behavioral level relatively quickly, by increasing the “visibility” of a
potential victim’s distress—while supporting long-term reductions in aggressive behavior
through training to not only recognize, but also anticipate, others’ distress and respond
with prosocial behavior.
Physiological Responses
With regard to physiological responses to others’ distress, findings did not support
the hypothesized interactive relationship between CU and anxiety in predicting resting
RSA and RSA reactivity. The lack of effects was in contrast to the results of previous
studies showing that CU traits are associated with blunted parasympathetic activity at rest
(e.g., de Wied et al., 2012) and in response to threat and distress cues (e.g., Anastassiou-
Hadjicharalambous & Warden, 2008b). Given the relatively small sample size of the
present study, and the relatively small nature of psychohysiological effects in studies
comparing CNS activity of youth with and without CU traits (e.g., Anastassiou-
Hadjicharalambous & Warden, 2008b; de Wied et al., 2012; Musser et al. 2013), power
to detect moderation effects may have been compromised. Interestingly, anxious youth
showed greater parasympathetic suppression across time with extended exposure to
another child’s distress; the same was not true of non-anxious children. Existing literature
indicates that high RSA reactivity in response to distressing stimuli may be a biomarker
of reduced emotion regulation capabilities (Beauchaine, 2015). While sample size may
have precluded detection of effects related to CU and its interaction with anxiety across
time (as suggested by the trending effects noted in Table 9), findings related to anxiety
and RSA reactivity over time hint that the specific parasympathetic response pattern
37
associated with anxiety may explain anxiety-related heterogeneity in aggressive behavior
among CU youth. As research both specific to CU traits and on empathy in general
suggests that blunted parasympathetic and sympathetic activity may be partially
responsible for deficits in empathy-related responding, rather than solely the failure to
detect and understand emotional cues (e.g., Blair et al., 2006; Shirtcliff et al., 2009),
further investigation is needed to identify whether physiological responses contribute to
anxiety-related heterogeneity among CU youth—particularly given the increased
attention to distress cues observed in CU youth experiencing anxiety symptoms (Kimonis
et al., 2012). Future studies would do well to investigate specific profiles of
parasympathetic response to others’ distress across time in larger samples.
Trauma-related Findings
Statistical power may also have interfered with detection of trauma-related
moderation effects, as traumatic stress data were available only for the part of the sample
that experienced a traumatic event (N=25). However, among these youth, traumatic stress
symptom severity still predicted increased ratings of opponent fear in the presence of a
distress cue, in line with literature documenting enhanced identification of fear-related
cues among trauma-exposed youth (e.g., Masten et al., 2008). Child CU traits were also
positively correlated with traumatic stress—but not anxiety—indicating a potential
relationship between CU and traumatic stress that is not accounted for by trauma-related
anxiety. The high rate of trauma exposure in this CP-enhanced community sample sheds
light on the overall need to understand potential trauma responses—particularly given
evidence that traumatic stress influences perceptions of others’ fear—and the observed
38
correlation between CU traits and traumatic stress suggests the need for further
exploration of how these constructs co-occur in trauma-exposed youth.
Clinical Implications
Important clinical and practical implications follow from study findings as a
whole. Children with CU traits may benefit from training to anticipate situations that may
cause others’ distress, to attend to, and accurately identify, distress cues (and cues to the
potential for distress) and to alter behavior accordingly with contingency management
and prosocial behavior training. Given that high anxiety levels increase the likelihood for
aggression in the absence of salient distress cues (and the presence of neutral, ambiguous
cues), identifying children with high levels of CU traits and anxiety for emotional
training-based intervention may be particularly important. In potentially aggressive
situations involving children with CU traits, increasing the salience of others’ distress
cues (and/or potential for distress) may attenuate aggressive outcomes. Interestingly, the
widely encouraged practice of ignoring, or remaining confident/neutral when facing
aggression and provocation may not apply to victims of aggressors with CU—and
especially aggressors with CU and anxiety. In these situations, it may be best for victims
to make their distress salient to the aggressor in order to reduce aggression.
Limitations
Conclusions should be interpreted in light of several study limitations. The first
set of limitations relates to the nature of the study sample. The sample size may have
yielded inadequate statistical power to detect small-to-medium effects, particularly low-
magnitude psychophysiological effects, and trauma-related effects that were, by
necessity, examined in an even smaller participant subset. Sample size precluded

39
investigation of the relationships of interest while controlling for demographic factors
relevant to aggression, such as age and gender (Baillargeon et al., 2007; Costello,
Mustillo, Erklani, & Angold, 2003; Loeber & Hay, 1997). Future research would do well
to investigate physiological responses—including indices of both parasympathetic and
sympathetic activity, given research indicating blunted parasympathetic and sympathetic
responses in CU youth (e.g., Blair et al., 1999; de Wied et al., 2012)—to others’ distress
in larger samples, as well as the potential role of trauma in differences between CU youth
with and without anxiety in a trauma-exposed sample. In addition, the CP-enhanced
sample yielded data that did not conform to normality standards for typical linear
regression analyses. While bootstrapping techniques allowed for correction and increased
confidence in results, future research should investigate relationships in larger clinical
samples, so that statistical techniques geared towards analyzing skewed data (e.g.,
Poisson regression) may be used. Relatedly, as CU traits are typically conceptualized in
the context of child behavior problems, conducting further study in a clinical sample
would allow more in-depth analysis of the CU construct. However, the practice of
blending community recruitment with recruitment of youth with serious behavior
problems in order to yield a CP-enhanced sample is not unprecedented in the CU and
anxiety literature (e.g., Docherty et al., 2015). Third, the sample included mostly
Hispanic youth, with few African American children and few non-Hispanic Caucasian
children. Although this sample is fairly representative of the ethnic demographics of the
city in which data were collected (70% Hispanic, 11.9% White non-Hispanic, 16.3%
Black or African American non-Hispanic; U.S. Census Bureau, 2010), results may not
generalize to other populations and cultures.

40
A second set of limitations relates to the nature of data collected, including
measures in the SuperBuilder task and information on traumatic exposure. Although data
were collected on child perception of peer emotions, data were not collected on child
perception of peer intentions, precluding the assessment of interpretive biases and social
goals during the SuperBuilder task. Given the reactive profile of children with CU and
anxiety (e.g., Fanti et al., 2013), and the potential for interactive social-cognitive biases
associated with both CU (e.g., Pardini, 2011) and anxiety (e.g., Taghavi et al., 2000),
future research would do well to assess the role of cognition more extensively. Moreover,
children displayed relatively high aggression overall during the SuperBuilder task,
reducing the variability of aggression that could be predicted. Perhaps the aggression task
evoked competitive behavior that interfered with the emotional matching theorized to
underlie empathy (Eisenberg & Eggum, 2009), as observed in adult research (e.g.,
Cikara, Bruneau, & Saxe, 2011; Weyers, Mühleberger, Kund, Hess, & Pauli, 2009). With
regard to traumatic exposure, information on exposure to specific trauma types
experienced (e.g., physical abuse, witnessing community violence, natural disaster
exposure) was not collected. As a result, it was not possible to examine how trauma-
related findings may vary across various forms of traumatic exposure. Given previous
investigations indicating more extensive trauma histories among CU youth with anxiety
in comparison to their non-anxious counterparts (e.g., Humayun et al., 2015; Kimonis et
al., 2012), and research suggesting that emotional numbing symptoms link violence
exposure and delinquency (Allwood et al., 2011), it is possible that specific forms of
traumatic exposure (e.g., violence exposure) are more strongly associated with aggression
and aspects of emotional processing among youth with CU traits than other forms of
41
traumatic exposure (e.g., exposure to a natural disaster). Future studies would do well to
collect information on youths' exposure to specific forms of trauma.
A final limitation relates to study time period. Given the short-term nature of the
laboratory-based task, long-term conclusions cannot be drawn. Similarly, long-term
predictions of behavior and outcomes cannot be made, given the absence of longitudinal
follow-up data. While practice effects may preclude the administration of the
SuperBuilder task as-is at regular intervals, perhaps further task development and
sophistication (e.g., randomization of task conditions) would allow for more long-term
comparison. Longitudinal reports and records-based (e.g., school disciplinary records)
data would allow future researchers to examine the long-term predictive value of
observed responses to others’ distress among children with CU and anxiety.
Future Directions
In addition to the specific considerations for future research noted above, further
investigation is needed in general to identify potential mechanisms by which CU and
anxiety symptoms interact to increase aggression in the absence of distress cues. While
study findings suggest that emotional processing plays a role in this relationship, research
may do well to assess whether increases and decreases in aggression under these
conditions are mediated by physiological responses, social cognitive processes (such as a
HAB or perceptions of dominance), or both.
Summary and Conclusions
Despite the limitations noted above, the present study was the first to examine
relationships between CU traits, anxiety, and observed aggression in an experimental task
allowing manipulation of distress cue salience, and the first to examine relationships

42
between CU traits, anxiety, and parasympathetic responses to others’ distress. Findings
extend existing research by highlighting the role of emotional cues in the observed
aggressive responses of children with CU traits, particularly CU youth experiencing
anxiety symptoms. Although previous research has equated CU traits with a lack of
anxiety (see Frick & White, 2008), the present study joins a growing body of work
indicating that these two constructs are not mutually exclusive, but rather may interact to
predict some of the most concerning outcomes. The distinction between subset of
children with CU traits with and without anxiety appears to have significant clinical and
theoretical utility in predicting the heterogeneity of behavior among youth with CU traits,
as well as pointing to potential treatment targets; future research must further investigate
the nature of emotional processing deficits, and their role in the development of AB,
among children with CU traits and anxiety.

43
REFERENCES
Allwood, M.A., Bell, D.J., & Horan, J. (2011). Posttrauma numbing of fear, detachment,
and arousal predict delinquent behaviors in early adolescence. Journal of Clinical
Child & Adolescent Psychology, 40(5), 659-667.
doi:10.1080/15374416.2011.597081.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Anastassiou-Hadjicharalambous, X., & Warden, D. (2008a). Cognitive and affective
perspective-taking in conduct-disordered children high and low on callous-
unemotional traits. Child and Adolescent Psychiatry and Mental Health, 2(16), 1-
11. doi:10.1186/1753-2000-2-16.
Anastassiou-Hadjicharalambous, X., & Warden, D. (2008b). Physiologically-indexed and
self-perceived affective empathy in conduct-disordered children high and low on
callous unemotional traits. Child Psychiatry and Human Development, 39, 503-
517.
Appelhans, B. M., & Luecken, L. J. (2006). Heart rate variability as an index of regulated
emotional responding. Review of General Psychology, 10(3), 229-240.
Baillargeon, R. H., Zoccolillo, M., Keenan, K., Côté, S., Pérusse, D., Wu, H., Boivin, M.,
& Tremblay, R. E. (2007). Gender differences in physical aggression: A
prospective population-based survey of children before and after 2 years of age.
Developmental Psychology, 43(1), 13-26. doi: 10.1037/0012-1649.43.1.13
Baron, R.M., & Kenny, D.A. (1986). The moderator-mediator variable distinction in
social psychological research: Conceptual, strategic, and statistical consideration.
Journal of Personality and Social Psychology, 51, 1173-1182. doi:10.1037/0022-
3514.51.6.1173.
Beauchaine, T. P. (2015). Respiratory sinus arrhythmia: A transdiagnostic biomarker of
emotion dysregulation and psychopathology. Current Opinions in Psychology,
1(3), 43-47.
Blair, R. J. R. (1999). Responsiveness to distress cues in the child with psychopathic
tendencies. Personality and Individual Differences, 27(1), 135-145. doi:
10.1016/S0191-8860(98)00231-1
Blair, R. J. R., Budhani, S., Colledge, E., & Scott, S. (2005). Deafness to fear in boys
with psychopathic tendencies. Journal of Child Psychology and Psychiatry, 46(3),
327-336.
44
Blair, R. J., Colledge, E., Murray, L., & Mitchell, D. G. (2001). A selective impairment
in the processing of sad and fearful expressions in children with psychopathic
tendencies. Journal of Abnormal Child Psychology, 29(6), 491-498.
Blair, R. J. R., Peschardt, K. S., Budhani, S., Mitchell, D. G. V., & Pine, D. S. (2006).
The development of psychopathy. Journal of Child Psychology and Psychiatry,
47(3), 262-275.
Bollen, K. A., & Stine, R. (1990). Direct and indirect effects: Classical and bootstrap
estimates of variability. Sociological Methodology, 20, 115-140.
Canivez, G. L., Konold, T. R., Collins, J. M., & Wilson, G. (2009). Construct validity of
the Wechsler Abbreviated Scale of Intelligence and Wide Range Intelligence
Test: Convergent and structural validity. School Psychology Quarterly, 24(4),
252-265. doi: 10.1037/a0018030
Christian, R.E., Frick, P.J., Hill, N.L., Tyler, L., & Frazer, D.R. (1997). Psychopathy and
conduct problems in children: II. Implications for subtyping children with conduct
problems. Journal of the American Academy of Child & Adolescent Psychiatry,
36, 233–241.
Cikara, M., Bruneau, E. G., & Saxe, R. R. (2011). Us and them: Intergroup failures of
empathy. Current Directions in Psychological Science, 20(3), 149-153. doi:
10.1177/0963721411408713
Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A. (2003). Prevalence and
development of psychiatric disorders in childhood and adolescence. Archives of
General Psychiatry, 60, 837-844. doi:10.1001/archpsyc.60.8.837.
Dadds, M. R.., Cauchi, A. J., Wimalaweera, S., Hawes, D. J., & Brennan, J. (2012).
Outcomes, moderators, and mediators of empathic-emotion recognition training
for complex conduct problems in childhood. Psychiatry Research, 199, 201-207
Dadds, M. R., El Masry, Y., Wimalaweera, S., & Guastella, A. J. (2008). Reduced eye
gaze explains “fear blindness” in childhood psychopathic traits. Journal of the
American Academy of Child and Adolescent Psychiatry, 47(4), 455-463. doi:
10.1097/CHI.0b013e31816407f1
Dadds, M. R., Hawes, D. J., Frost, A. D. J., Vassallo, S., Bunn, P., Hunter, K., & Merz, S.
(2009). Learning to “talk the talk”: The relationship of psychopathic traits to
deficits in empathy across childhood. Journal of Child Psychology and
Psychiatry, 50(5), 599-606.

45
Dadds, M. R., Jambrak, J., Pasalich, D., Hawes, D. J., & Brennan, J. (2011). Impaired
attention to the eyes of attachment figures and the developmental origins of
psychopathy. Journal of Child Psychology and Psychiatry, 52(3), 238-245
Dadds, M. R., Perry, Y., Hawes, D. J., Merz, S., Riddell, A. C., Haines, D. J., Solak, E.,
& Abeygunawardane, A. I. (2006). Attention to the eyes and fear-recognition
deficits. British Journal of Psychopathy, 189, 280-281.
Dalgleish, T., Moradi, A. R., Taghavi, M. R., Neshat-Doost, H. T., & Yule, W. (2001).
An experimental investigation of hypervigilance for threat in children and
adolescents with post-traumatic stress disorder. Psychological Medicine, 31,
541-547.
de Wied, M. van Boxtel, A., Matthys, W., & Meeus, W. (2012). Verbal, facial, and
autonomic responses to empathy-eliciting film clips by disruptive male
adolescents with high versus low callous unemotional traits. Journal of Abnormal
Child Psychology, 40(2), 211-223. doi: 10.1007/s10802-011-9557-8.
Docherty, M., Boxer, P., Huesmann, L. R., O’Brien, M., & Bushman, B. J. (2015).
Exploring primary and secondary variants of psychopathy in adolescents in
detention and in the community. Journal of Clinical Child and Adolescent
Psychology, 1-15. doi: 10.1080/15374416.2014.979934
Dodge, K. A., & Coie, J. D. (1987). Social-Information-Processing factors in reactive and
proactive aggression in children's peer groups. Journal of Personality and Social
Psychology, 53(6), 146-1158.
Dodge, K. A., Price, J. M.., Bachorowski, J., & Newman, J. P. (1990). Hostile
attributional biases in severely aggressive adolescents. Journal of Abnormal
Psychology, 99(4), 385-392. doi: 10.1037/0021-843X.99.4.385
Efron, B. (1979). Computers and the theory of statistics: Thinking the unthinkable.
Society for Industrial and Applied Mathematics Review, 21, 460-480.
Efron, B., & Tibshirani, R. J. (1993). An introduction to the bootstrap. New York, NY:
Chapman & Hall.
Eisenberg, N., & Eggum, N. D. (2009). Empathic responding: Sympathy and personal
distress. In: J. Decety & W. Ickes (Eds), The social neuroscience of empathy (pp.
71-83). Cambridge, MA: MIT Press.
Eisenberg, N., Eggum, N. D., & Di Giunta, L. (2010). Empathy-related responding:
Associations with prosocial behavior, aggression, and intergroup relations. Social
Issues and Policy, 4(1), 143-18. doi:10.1111/j.1751-2409.2010.01020.x.
46
Eisenberg, N., & Fabes, R. A. (1990). Empathy: Conceptualization, measurement, and
relation to prosocial behavior. Motivation and Emotion, 14(2), 131-149.
Essau, C.A., Sasagawa, S., & Frick, P.J. (2006). Callous-unemotional traits in a
community sample of adolescents. Assessment, 13, 454-469.
Euler, F., Jenkel, N., Stadler, C., Schmeck, K., Fegert, J. M., Kolch, M., & Schmit, M.
(2015). Variants of girls and boys with Conduct Disorder: Anxiety symptoms and
callous-unemotional traits. Journal of Abnormal Child Psychology, 43(3), 773-
785.
Fanti, K. A., Demetriou, C. A., & Kimonis, E. R. (2013). Variants of callous unemotional
conduct problems in a community sample of adolescents. Journal of Youth and
Adolescence, 42, 964-979.
Fanti, K.A. Frick, P.J., & Georgiou, S. (2009). Linking callous-unemotional traits to
instrumental and non-instrumental forms of aggression. Journal of
Psychopathology and Behavioral Assessment, 31, 285-298.
Foa, E. B., Johnson, K. M., Feeny, N. C., & Treadwell, K. R. (2001). The child PTSD
Symptom Scale: a preliminary examination of its psychometric properties.
Journal of Clinical Child Psychology, 30(3), 376-384.
Fontaine, N. M., McCrory, E. J. Boivin, M., Moffitt, T. E. & Viding, E. (2011).
Predictors and outcomes of joint trajectories of callous unemotional traits and
conduct problems in childhood. Journal of Abnormal Psychology, 120(3), 730-
742.
Frick P. J., Cornell, A. H., Bodin, S. D., Dane, H. A., Barry, C. T., & Loney, B. R.
(2003a). Callous-unemotional traits and developmental pathways to severe
aggressive and antisocial behavior. Developmental Psychology, 39, 246-260.
Frick, P. J., & Dantagnan, A. L. (2005). Predicting the stability of conduct problems in
children with and without callous-unemotional traits. Journal of Child and Family
Studies, 14(4), 469-485.
Frick, P. J., & Ellis, M. (1999). Callous–unemotional traits and subtypes of conduct
disorder. Clinical Child and Family Psychology Review, 2, 149–168.
Frick, .P. J, Kimonis, E. R., Dandreaux, D. M, & Farell, J. M. (2003b). The 4 year
stability of psychopathic traits in non-referred youth. Behavioral Science & Law,
21, 713–736.

47
Frick, P. J., Ray, J. V., Thornton, L. C., & Kahn, R. E. (2014). Can callous-unemotional
traits enhance the understanding, diagnosis, and treatment of serious conduct
problems in children and adolescents? A comprehensive review. Psychological
Bulletin, 140(1), 1-57. doi: 10.1037/a0033076
Frick, P. J., & White, S. F. (2008). Research review: The importance of callous-
unemotional traits for developmental models of aggressive and antisocial
behavior. Journal of Child Psychology and Psychiatry, 49(4), 359-375. doi:
10.1111/j.1469-7610.2007.01862.x
Giancola, P.R., & Zeichner, A. (1995). Construct validity of a competitive reaction-time
aggression paradigm. Aggressive Behavior, 21, 199–204.
Gillihan, S. J., Aderka, I. M., Conklin, P. H., Capaldi, S., & Foa, E. B. (2013). The Child
PTSD Symptom Scale: Psychometric properties in female adolescent sexual
assault survivors. Psychological Assessment, 25(1), 23-31. doi: 10.1037/a0029553
Greenhill, L. L., Swanson, J. M., Vitiello, B., ... Wigal, T. (2001). Impairment and
deportment responses to different methylphenidate doses in children with ADHD:
The MTA titration trial. Child and Adolescent Psychiatry, 40, 168-179.
Hawes, S. W., Byrd, A. L., Henderson, C. E. Gazda, R. L., Burke, J. D., Loeber, R., &
Pardini, D. A. (2014a). Refining the parent-reported Inventory of Callous-
Unemotional Traits in boys with conduct problems. Psychological Assessment,
26(1), 256-266. doi: 10.1037/a0034718
Hawes, D. J., Price, M. J., & Dadds, M. R. (2014b). Callous-unemotional traits and the
treatment of conduct problems in childhood and adolescence: A comprehensive
review. Clinical Child & Family Psychology Review, 17(3), 248-267. doi:
10.1007/s10567-014-0167-1
Hawkins, S. S., & Radcliffe, J. (2006). Current measures of PTSD for children and
adolescents. Journal of Pediatric Psychology, 31(4), 420-430.
Hayano, J., Sakakibara, Y., Yamada, A., Yamada, M., Mukai, S., Fujinami, T., …
Takata, K. (1991). Accuracy of assessment of cardiac vagal tone by heart rate
variability in normal subjects. The American Journal of Cardiology, 67(2), 199-
204.
Hayes, A. F. (2012). PROCESS: A versatile computational tool for observed variable
mediation, moderation, and conditional process modeling [White paper].
Retrieved from http://www.afhayes.com/public/process2012.pdf
48
Helseth, S. A., Waschbusch, D. A., King, S., & Willoughby, M. T. (2015). Aggression in
children with conduct problems and callous-unemotional traits: Social
information processing and response to peer provocation. Journal of Abnormal
Child Psychology, 43(8), 1503-1514. doi: 10.1007/s10802-015-0027-6
Herpers, P. C., Klip, H., Rommelse, N. N., Greven, C. U., & Buitelaar, J. K. (2016).
Associations between high callous-unemotional traits and quality of life across
youths with non-conduct disorder diagnoses. European Journal of Child and
Adolescent Psychiatry, 25(5), 547-555. doi: 10.1007/s00787-015-0766-5
Herpers, P. C., Rommelse, N. N., Bons, D. M., Buitelaar, J. K., & Scheepers, F. E.
(2012). Callous-unemotional traits as a cross-disorders construct. Social
Psychiatry and Psychiatric Epidemiology, 47(12), 2045-2064. doi:
10.1007/s00127-012-0513-x
Hoffman, M. L. (1984). Interaction of affect and cognition in empathy. In C. E. Izard, J.
Kagan, & R. B. Zajonc (Eds.), Emotions, cognition, and behavior (pp. 103-131).
New York, NY: Cambridge University Press.
Holmbeck, G.N. (1997). Toward terminological, conceptual, and statistical clarity in the
study of mediators and moderators: Examples from the child-clinical and pediatric
psychology literatures. Journal of Consulting and Clinical Psychology, 65, 599-
610. doi:10.1037/0022-006X.65.4.599.
Humayun, S., Kahn, R. E., Frick, P. J., & Viding, E. (2013). Callous unemotional traits
and anxiety in a community sample of 7-year-olds. Journal of Clinical Child &
Adolescent Psychology, 43(1), 36-42. doi: 10.1080/15374416.2013.814539.
Jones, A. P., Laurens, K. R., Herba, C. M., Barker, G. J., & Viding, E. (2009). Amygdala
hypoactivity to fearful faces in boys with conduct problems and callous-
unemotional traits. American Journal of Psychiatry, 166(1), 95-102. doi:
10.1176/appi.ajp.2008.07071050
Karpman, B. (1948). Conscience in the psychopath: Another version. American Journal
of Orthopsychiatry, 18, 455–491.
Kendall, P.C., & Comer, J.S. (2011). Research methods in clinical psychology. In D.H.
Barlow (ed.), The Oxford Handbook of Clinical Psychology (pp. 52-75). NY:
Oxford University Press. doi:10.1093/oxfordhb/9780195366884.013.0004.
Kahn, R. E., Frick, P. J., Youngstrom, E. A., Youngstrom, J. K., Feeny, N. C., &
Findling, R. L. (2013). Distinguishing primary and secondary variants of callous
unemotional traits among adolescents in a clinic-referred sample. Psychological
Assessment, 25(3), 966-978. DOI: 10.1037/a0032880.

49
Kimonis, E. R., Fanti, K. A., & Singh, J. F. (2014). Establishing cut-off scores for the
parent-reported Inventory of Callous-Unemotional Traits. Archives of Forensic
Psychology, 1(1), 27-48.
Kimonis, E. R., Frick, P. J., Cauffman, E., Goldweber, A., & Skeem, J. (2012). Primary
and secondary variants of juvenile psychopathy differ in emotional processing.
Development and Psychopathology, 24, 1091-1103.
Kimonis, E. R., Skeem, J. L., Cauffman, E., Dmitrieva, J. (2011). Are secondary variants
of juvenile psychopathy more reactively violent and less psychosocially mature
than primary variants? Law and Human Behavior, 35(5), 381-391.
Lee, Z., Salekin, R. T., & Iselin, A. R. (2010). Psychopathic traits in youth: Is there
evidence for primary and secondary subtypes? Journal of Abnormal Child
Psychology, 38, 381-393. Doi: 10.1007/s10802-009-9372-7
Little, R. J. A., & Rubin, D. B. (1987). Statistical analysis with missing data. New York,
NY: John Wiley & Sons.
Loeber, R., & Hay, D. (1997). Key issues in the development of aggression and violence
from childhood to early adulthood. Annual Review of Psychology, 48, 371-410.
doi: 10.1146/annurev.psych.48.1.371
Lozier, L. M., Cardinale, E. M., VanMeter, J. W., & Marsh, A. A. (2014). Mediation of
the relationship between callous unemotional traits and proactive aggression by
amygdala response to fear among children with conduct problems. Journal of the
American Medical Association of Psychiatry, 71(6), 627-636.
doi:10.1001/jamapsychiatry.2013.4540
Lynam, D. R., Caspi, A., Moffitt, T. E., Loeber, R., & Stouthamer-Loeber, M. (2007).
Longitudinal evidence that psychopathy scores in early adolescence predict adult
psychopathy. Journal of Abnormal Psychology, 116, 155-165.
March J. S. (2013). Multidimensional Anxiety Scale for Children–2nd edition: Technical
manual. Toronto, Ontario, Canada: Multi-Health Systems.
March, J. S., Parker, J. D., Sullivan, K., Stallings, P., Conners, C. K. (1997). The
Multidimensional Anxiety Scale for Children (MASC): Factor structure,
reliability, and validity. Journal of the American Academy of Child and
Adolescent Psychiatry, 36(4), 554-565.
Marsh, A. A., Finger, E. C., Fowler, K. A., Adalio, C. J., Jurkowitz, I. T. N., Schechter, J.
C., … Blair, R. J. R. (2013). Empathic responsiveness in amygdala and anterior
cingulate cortex in youths with psychopathic traits. Journal of Child Psychology
and Psychiatry, 54(8), 900-910. doi:10.1111/jcpp.12063.
50
McDonald, R., Dodson, M. C., Rosenfield, D., & Jouriles, E. N. (2011). Effects of a
parenting intervention on features in psychopathy in children. Journal of
Abnormal Child Psychology, 39, 1013-1023. DOI: 10.1007/s10802-011-9512-8.
Mills-Koonce, W. R., Wagner, N. J., Willoughby, M. T., Stifter, C., Blair, C., & Granger,
D. A.. (2015). Greater fear reactivity and psychophysiological hyperactivity
among infants with later conduct problems and callous-unemotional traits.
Journal of Child Psychology and Psychiatry, 56(2), 147-154. doi:
10.1111/jcpp.12289
Moran, P., Rowe, .R, Flach, C., Briskman, J., Ford, T., Maughan, B., & Goodman, R.
(2009). Predictive value of callous-unemotional traits in a large community
sample. Journal of the American Academy of Child and Adolescent Psychiatry,
48, 1079–1084. doi:10.1097/CHI.0b013e3181b766ab
Muñoz, L.C. (2009). Callous-unemotional traits are related to combined deficits in
recognizing afraid faces and body poses. Journal of the American Academy of
Child and Adolescent Psychiatry, 48(5), 554-562.
Muñoz, L.C., Frick, P. J., Kimonis, E. R., Aucoin, K. J. (2008). Types of aggression,
responsiveness to provocation, and callous-unemotional traits in detained
adolescents. Journal of Abnormal Child Psychology, 36, 15-28.
Muris, P., Merckelbach, H., Ollendick, T., King, N., & Bogie, N. (2002). Three
traditional and three new childhood anxiety questionnaires: Their reliability and
validity in a normal adolescent sample. Behaviour Research and Therapy, 40,
753-772. doi: 10.1016/S0005-7967(01)00056-0
Musser, E. D., Galloway-Long, H. S., Frick, P. J., & Nigg, J. T. (2013). Emotion
regulation and heterogeneity in Attention-Deficit/Hyperactivity Disorder.
Journal of the American Academy of Child and Adolescent Psychiatry, 52(2),
163-171. doi: 10.1016/j.jaac.2012.11.009
Nixon, R. D. V., Yule, W., Perrin, S., Meiser-Stedman, R., Dalgleish, T., Clark, D. M., &
Smith, P. (2013). The Child PTSD Symptom Scale: An update and replication of
its psychometric properties. Psychological Assessment, 25(3), 1025-1031. doi:
10.1037/a0033324
Obradovic, J., Pardini, D. A., Long J. D., & Loeber, R. (2007). Measuring interpersonal
callousness in boys from childhood to adolescence: An examination of
longitudinal invariance and temporal stability. Journal of Clinical Child and
Adolescent Psychology, 36, 276-292.
51
Pardini, D.A. (2006). The callousness pathway to severe violent delinquency. Aggressive
Behavior, 32, 1–9.
Pardini, D. A., & Byrd, A. L. (2012). Perceptions of aggressive conflicts and others’
distress in children with callous-unemotional traits: ‘I’ll show you who’s boss,
even if you suffer and I get in trouble.’ Journal of Child Psychology and
Psychiatry, 53(3), 283-291. doi:10.1111/j.1469-7610.2011.02487.x
Pardini, D.A. (2011). Perceptions of social conflicts among incarcerated adolescents with
callous-unemotional traits: ‘You’re going to pay. It’s going to hurt, but I don’t
care’. Journal of Child Psychology and Psychiatry, 52, 248–255. doi:
10.1111/j.1469-7610.2010.02336.x
Porter, S. (1996). Without conscience or without active conscience? The etiology of
Psychopathy revisited. Aggression and Violent Behavior, 1, 179–189.
Rasmussen, J. L. (1987). Estimating correlation coefficients: Bootstrap and parametric
approaches. Psychological Bulletin, 101, 136-139.
Reid, S. C.., Salmon, K., & Lovibond, P. F. (2006). Cognitive biases in childhood
anxiety, depression, and aggression: Are they pervasive or specific? Cognitive
Therapy and Research, 30, 531-549. doi: 10.1007/s10608-006-9077-y
Rosan, A., Frick, P. J., Gottlieb, K. A., & Fasicaru, L. (2015). Callous-unemotional traits
and anxiety in a sample of detained adolescents in Romania. Journal of Evidence-
Based Psychotherapies, 15(1), 79-95.
Rowe, R., Maughan, B., Moran, P., Ford, T., Briskman, J., & Goodman, R. (2010). The
role of callous unemotional traits in the diagnosis of conduct disorder. Journal of
Child Psychology and Psychiatry, 51(6), 688-695.
Russell, C. J., & Dean, M. A. (2000). To log or not to log: Bootstrap as an alternative to
the parametric estimation of moderation effects in the presence of skewed
dependent variables. Organizational Research Methods, 3(2), 166-185.
Saklofske, D. H., Caravan, G., & Schwartz, C. (2000). Concurrent validity of the
Wechsler Abbreviated Scale of Intelligence (WASI) with a sample of Canadian
children. Canadian Journal of School Psychology, 16(1), 87-94. doi:
10.1177/082957350001600106
Shirtcliff, E. A., Vitacco, M. J., Graf, A. R., Gostisha, A. J., Merz, J. L., & Zahn-Waxler,
C. (2009). Neurobiology of empathy and callousness: Implications for the
development of antisocial behavior. Behavioral Science and the Law, 27(2), 137-
171. doi: 10.1002/bsl.852
52
Skeem, J. L., Poythress, N., Edens, J. F., Lilienfeld, S. O., & Cale, E. M. (2003).
Psychopathic personality or personalities? Exploring potential variants of
psychopathy and their implications for risk assessment. Aggression and Violent
Behavior, 8, 513–546.
Taghavi, M. R., Moradi, A. R., Neshat-Doost, H. T., Yule, W., & Dalgleish, T. (2000).
Interpretation of ambiguous emotional information in clinically anxious children
and adolescents. Cognition and Emotion, 14(6), 809-822. doi:
10.1080/02699930050156645
Tatar II, J. R., Cauffman, E., Kimonis, E. R., & Skeem, J. L. (2012). Victimization
history and posttraumatic stress: An analysis of psychopathy variants in male
juvenile offenders. Journal of Child & Adolescent Trauma, 5, 102-113. doi:
10.1080/19361521.2012.671794
Teicher, M. H., Andersen, S. L., Polcari, A., Anderson, C. M., & Navalta, C. P. (2002).
Developmental neurobiology of childhood stress and trauma. Psychiatric Clinics
of North America, 25(2), 397-426. doi: 10.1016/S0193-953X(01)00003-X
Thomaes, S., Bushman, B. J., Stegge, H., & Olthof, T. (2008). Trumping shame by blasts
of noise: Narcissism, self-esteem, shame, and aggression in young adolescents.
Child Development, 79(6), 1792-1801.
U.S. Census Bureau. (2010). Data Tables for Florida, Counties, and Incorporated Cities.
Retrieved from:
http://edr.state.fl.us/Content/population-demographics/2010-
census/data/index.cfm
Van Baardewijk, Y., Stegge, H., Bushman, B. J., & Vermeiren, R. (2009). Psychopathic
traits, victim distress and aggression in children. Journal of Child Psychology and
Psychiatry, 50(6), 718-725. doi:10.1111/j.1469-7610.2008.02023.x.
Vaughn, M. G., Edens, J. F., Howard, M. O., & Smith, S. T. (2009). An investigation of
primary and secondary psychopathy in a statewide sample of incarcerated youth.
Youth Violence and Juvenile Justice, 7(3), 172-188. doi:
10.1177/15412040009333792
Waschbusch, D. A., Carrey, N. J., Willoughby, M. T., King, S., & Andrade, B. F. (2007).
Effects of Methylphenidate and behavior modification on the social and academic
behavior of children with Disruptive Behavior Disorders: The moderating role of
callous/unemotional traits. Journal of Clinical Child & Adolescent Psychology,
36(4), 629-644.
53
Waschbusch, D. A., Porter, S., Carrey, N., Kazmi, S. O., Roach, K. A., D’Amico, D. A.
(2004). Investigation of the heterogeneity of disruptive behavior in elementary-
age children. Canadian Journal of Behavioral Science, 36(2), 97-112.
Wechsler, D. (1999). Wechsler Abbreviated Scale of Intelligence. San Antonio, TX: The
Psychological Corporation.
Wechsler, D. (2011). Wechsler Abbreviated Scale of Intelligence (2nd ed.). Bloomington,
MN: Pearson.
Weems, C. F., Saltzman, K. M., Reiss, A. L., & Carrion, V. G. (2003). A prospective test
of the association between hyperarousal and emotional numbing in youth with a
history of traumatic stress. Journal of Clinical Child & Adolescent Psychology,
32(1), 166-171. doi: 10.1207/S15374424JCCP3201_15
Wei, C., Hoff, A., Villabo, M. A., Peterman, J., Kendall, P. C., Piacentini, J., … March, J.
(2014). Assessing anxiety in youth with the Multidimensional Anxiety Scale for
Children (MASC). Journal of Clinical Child and Adolescent Psychology, 43(4),
566-578. doi: 10.1080/15374416.2013.814541
Weyers, P., Mühlberger, A., Kund, A., Hess, U., & Pauli, P. (2009). Modulation of facial
reactions to avatar emotional faces by nonconscious competition priming.
Psychophysiology, 46, 328-335. doi: 10.1111/j.1469-8986.2008.00771.x
Woodworth, M., & Waschbusch, D. (2008). Emotional processing in children with
conduct problems and callous-unemotional traits. Child Care and Healthy
Development, 34(2), 234-244.

54
APPENDICES
55
Figure 1. Excerpts from the SuperBuilder game play simulation. Participants were told
they were building the red brick skyscraper, while their opponent was building the yellow
skyscraper.

56
Figure 2. Explanation of SuperBuilder sound blast levels presented to the child
participant.

57
Figure 3. Neutral and distress messages, respectively, sent from the SuperBuilder
simulated opponent to the child participant.
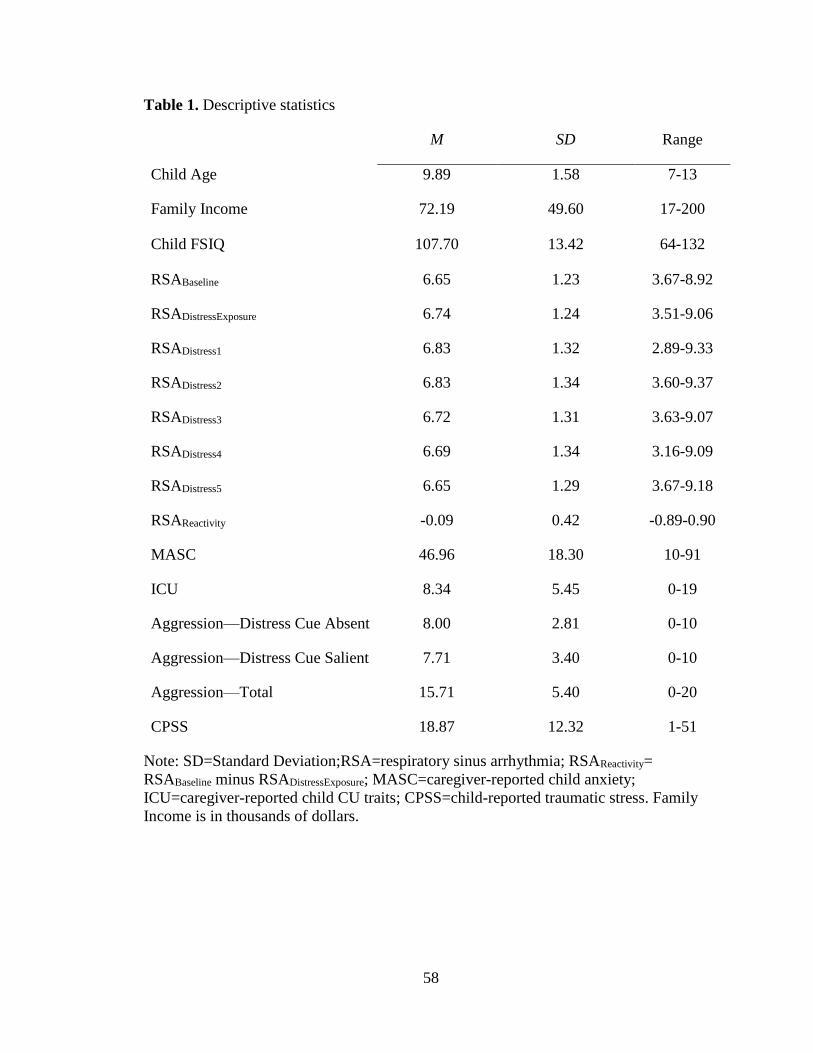
58
Table 1. Descriptive statistics
M SD Range
Child Age 9.89 1.58 7-13
Family Income 72.19 49.60 17-200
Child FSIQ 107.70 13.42 64-132
RSABaseline 6.65 1.23 3.67-8.92
RSADistressExposure 6.74 1.24 3.51-9.06
RSADistress1 6.83 1.32 2.89-9.33
RSADistress2 6.83 1.34 3.60-9.37
RSADistress3 6.72 1.31 3.63-9.07
RSADistress4 6.69 1.34 3.16-9.09
RSADistress5 6.65 1.29 3.67-9.18
RSAReactivity -0.09 0.42 -0.89-0.90
MASC 46.96 18.30 10-91
ICU 8.34 5.45 0-19
Aggression—Distress Cue Absent 8.00 2.81 0-10
Aggression—Distress Cue Salient 7.71 3.40 0-10
Aggression—Total 15.71 5.40 0-20
CPSS 18.87 12.32 1-51
Note: SD=Standard Deviation;RSA=respiratory sinus arrhythmia; RSAReactivity=
RSABaseline minus RSADistressExposure; MASC=caregiver-reported child anxiety;
ICU=caregiver-reported child CU traits; CPSS=child-reported traumatic stress. Family
Income is in thousands of dollars.

59
Table 2. Zero-order correlations between study variables.
1 2 3 4 5 6 7 8 9 10 11 12 13
1. Age -
2. Gender -.01 -
3. Ethnicity .08 .07 -
4. Income -.21 .13 -.33* -
5. RSABaseline -.03 .30 -.01 -.25 -
6. RSADistressExposure .09 .23 .06 -.34* .94** -
7. RSAReactivity .19 .17 -.19 .30 .13 -.21 -
8. MASC .10 -.20 -.17 .21 -.23 -.26 .08 -
9. ICU .15 .05 .20 -.25 .05 .03 .08 -.11 -
10. AggressionNeutral -.31* .04 .05 -.18 .23 .23 -.01 -.37* .32* -
11. AggressionDistress -.39** -.07 .04 .003 -.05 -.07 .05 -.09 .13 .51** -
12. AggressionTotal -.42** -.03 .05 -.10 .09 .08 .03 -.25 .25 .84** .89** -
13. FSIQ -.07 .16 -.24 .39* .01 -.02 .10 .02 -.32* -.25 -.11 -.19
14. CPSS .05 .13 .002 -.18 .04 -.03 .23 -.28 .43* .11 .11 .12 -.32
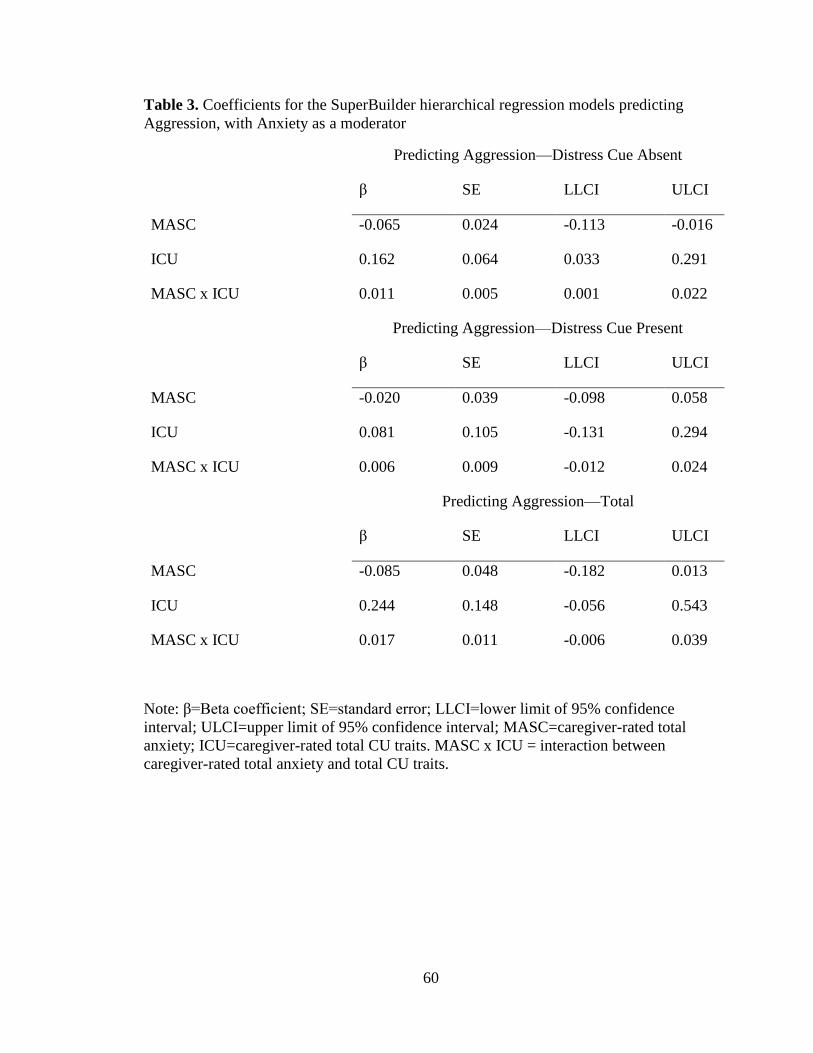
60
Table 3. Coefficients for the SuperBuilder hierarchical regression models predicting
Aggression, with Anxiety as a moderator
Predicting Aggression—Distress Cue Absent
β SE LLCI ULCI
MASC -0.065 0.024 -0.113 -0.016
ICU 0.162 0.064 0.033 0.291
MASC x ICU 0.011 0.005 0.001 0.022
Predicting Aggression—Distress Cue Present
β SE LLCI ULCI
MASC -0.020 0.039 -0.098 0.058
ICU 0.081 0.105 -0.131 0.294
MASC x ICU 0.006 0.009 -0.012 0.024
Predicting Aggression—Total
β SE LLCI ULCI
MASC -0.085 0.048 -0.182 0.013
ICU 0.244 0.148 -0.056 0.543
MASC x ICU 0.017 0.011 -0.006 0.039
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; MASC=caregiver-rated total
anxiety; ICU=caregiver-rated total CU traits. MASC x ICU = interaction between
caregiver-rated total anxiety and total CU traits.

61
Table 4. Coefficients for the SuperBuilder hierarchical regression models predicting
Aggression, with traumatic stress as a moderator
Predicting Aggression—Distress Cue Absent
β SE LLCI ULCI
CPSS 0.0001 0.059 -0.124 0.124
ICU 0.099 0.137 -0.187 0.385
CPSS x ICU 0.001 0.010 -0.020 0.022
Predicting Aggression—Distress Cue Present
β SE LLCI ULCI
CPSS 0.019 0.074 -0.136 0.173
ICU 0.085 0.164 -0.259 0.429
CPSS x ICU -0.005 0.016 -0.039 0.028
Predicting Aggression—Total
β SE LLCI ULCI
CPSS 0.019 0.124 -0.240 0.277
ICU 0.184 0.271 -0.383 0.752
CPSS x ICU -0.004 0.024 -0.054 0.046
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; CPSS=child-rated total traumatic
stress; ICU=caregiver-rated total CU traits. CPSS x ICU = interaction between child-
rated total traumatic stress and total CU traits.
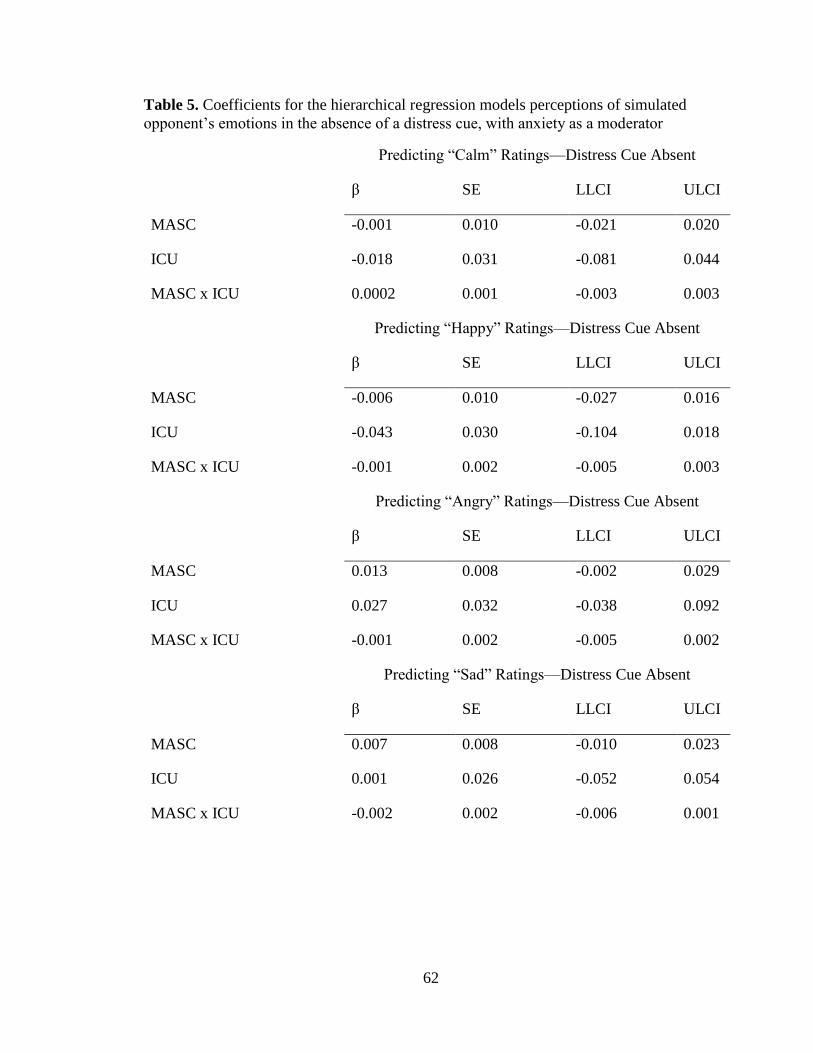
62
Table 5. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the absence of a distress cue, with anxiety as a moderator
Predicting “Calm” Ratings—Distress Cue Absent
β SE LLCI ULCI
MASC -0.001 0.010 -0.021 0.020
ICU -0.018 0.031 -0.081 0.044
MASC x ICU 0.0002 0.001 -0.003 0.003
Predicting “Happy” Ratings—Distress Cue Absent
β SE LLCI ULCI
MASC -0.006 0.010 -0.027 0.016
ICU -0.043 0.030 -0.104 0.018
MASC x ICU -0.001 0.002 -0.005 0.003
Predicting “Angry” Ratings—Distress Cue Absent
β SE LLCI ULCI
MASC 0.013 0.008 -0.002 0.029
ICU 0.027 0.032 -0.038 0.092
MASC x ICU -0.001 0.002 -0.005 0.002
Predicting “Sad” Ratings—Distress Cue Absent
β SE LLCI ULCI
MASC 0.007 0.008 -0.010 0.023
ICU 0.001 0.026 -0.052 0.054
MASC x ICU -0.002 0.002 -0.006 0.001
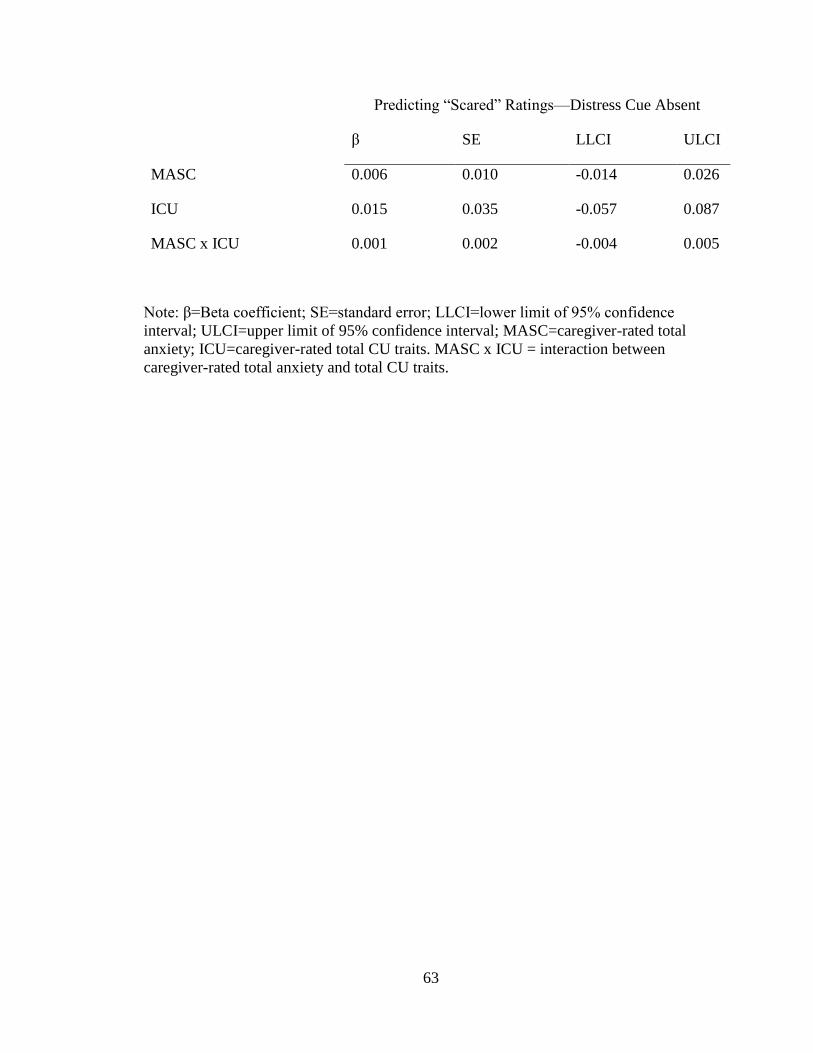
63
Predicting “Scared” Ratings—Distress Cue Absent
β SE LLCI ULCI
MASC 0.006 0.010 -0.014 0.026
ICU 0.015 0.035 -0.057 0.087
MASC x ICU 0.001 0.002 -0.004 0.005
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; MASC=caregiver-rated total
anxiety; ICU=caregiver-rated total CU traits. MASC x ICU = interaction between
caregiver-rated total anxiety and total CU traits.
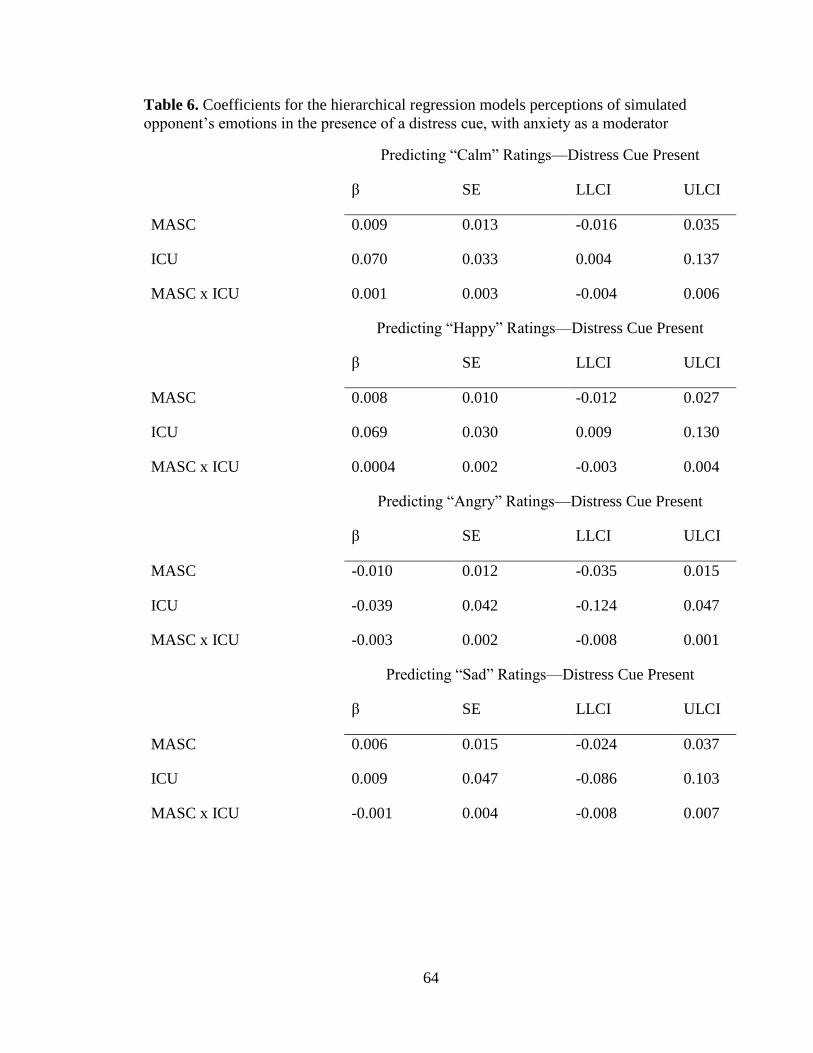
64
Table 6. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the presence of a distress cue, with anxiety as a moderator
Predicting “Calm” Ratings—Distress Cue Present
β SE LLCI ULCI
MASC 0.009 0.013 -0.016 0.035
ICU 0.070 0.033 0.004 0.137
MASC x ICU 0.001 0.003 -0.004 0.006
Predicting “Happy” Ratings—Distress Cue Present
β SE LLCI ULCI
MASC 0.008 0.010 -0.012 0.027
ICU 0.069 0.030 0.009 0.130
MASC x ICU 0.0004 0.002 -0.003 0.004
Predicting “Angry” Ratings—Distress Cue Present
β SE LLCI ULCI
MASC -0.010 0.012 -0.035 0.015
ICU -0.039 0.042 -0.124 0.047
MASC x ICU -0.003 0.002 -0.008 0.001
Predicting “Sad” Ratings—Distress Cue Present
β SE LLCI ULCI
MASC 0.006 0.015 -0.024 0.037
ICU 0.009 0.047 -0.086 0.103
MASC x ICU -0.001 0.004 -0.008 0.007
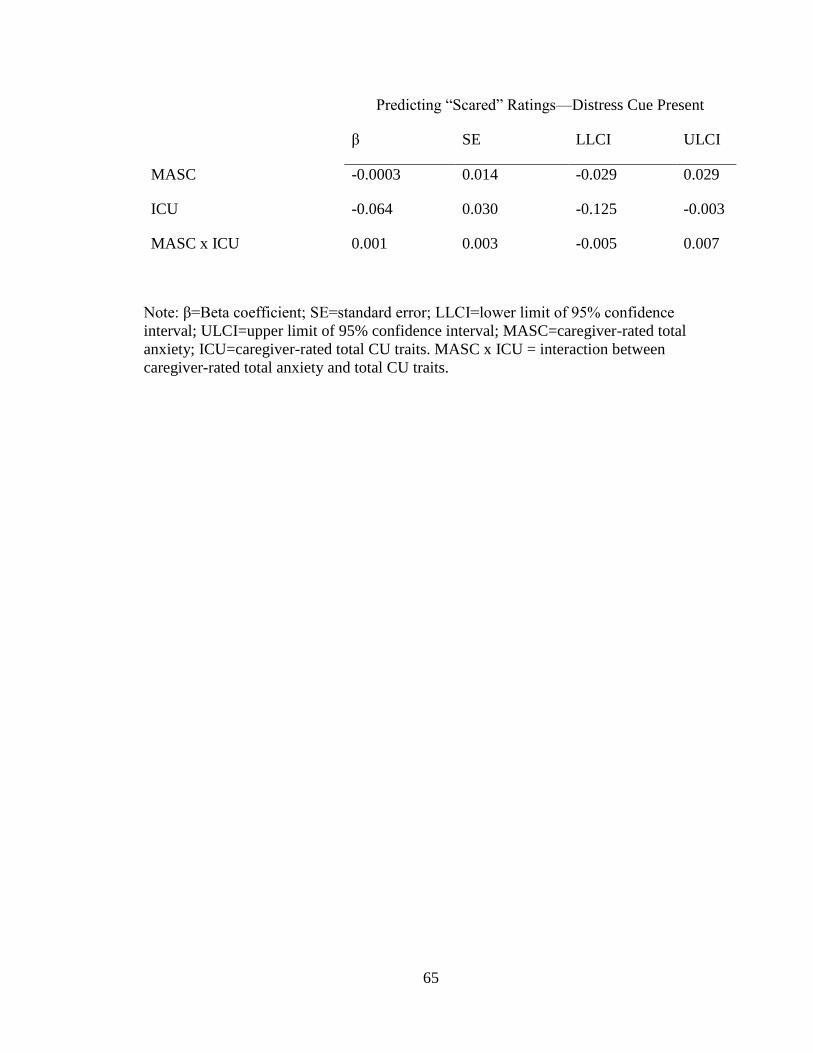
65
Predicting “Scared” Ratings—Distress Cue Present
β SE LLCI ULCI
MASC -0.0003 0.014 -0.029 0.029
ICU -0.064 0.030 -0.125 -0.003
MASC x ICU 0.001 0.003 -0.005 0.007
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; MASC=caregiver-rated total
anxiety; ICU=caregiver-rated total CU traits. MASC x ICU = interaction between
caregiver-rated total anxiety and total CU traits.

66
Table 7. Coefficients for the hierarchical regression models predicting changes in
perceptions of simulated opponent’s emotions, with anxiety as a moderator
Predicting Change in “Calm” Ratings
β SE LLCI ULCI
MASC -0.010 0.016 -0.042 0.022
ICU -0.088 0.052 -0.192 0.017
MASC x ICU -0.001 0.003 -0.007 0.005
Predicting Change in “Happy” Ratings
β SE LLCI ULCI
MASC -0.013 0.012 -0.037 0.011
ICU -0.112 0.037 -0.188 -
0.037
MASC x ICU -0.001 0.002 -0.005 0.003
Predicting Change in “Angry” Ratings
β SE LLCI ULCI
MASC 0.024 0.014 -0.005 0.052
ICU 0.066 0.037 -0.009 0.142
MASC x ICU 0.002 0.002 -0.003 0.007
Predicting Change in “Sad” Ratings
β SE LLCI ULCI
MASC 0.0002 0.018 -0.035 0.036
ICU -0.008 0.052 -0.112 0.097
MASC x ICU -0.001 0.005 -0.011 0.008
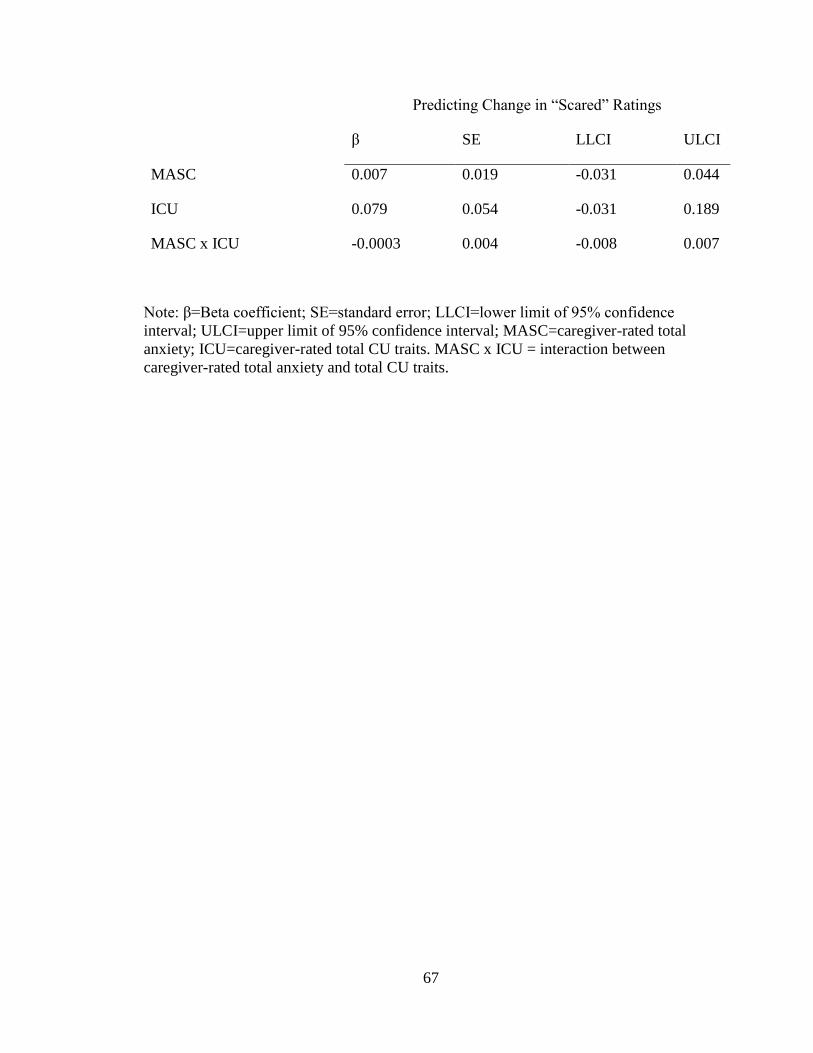
67
Predicting Change in “Scared” Ratings
β SE LLCI ULCI
MASC 0.007 0.019 -0.031 0.044
ICU 0.079 0.054 -0.031 0.189
MASC x ICU -0.0003 0.004 -0.008 0.007
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; MASC=caregiver-rated total
anxiety; ICU=caregiver-rated total CU traits. MASC x ICU = interaction between
caregiver-rated total anxiety and total CU traits.

68
Table 8. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the absence of a distress cue, with traumatic stress as a moderator
Predicting “Calm” Ratings—Distress Cue Absent
β SE LLCI ULCI
CPSS -0.017 0.032 -0.084 0.050
ICU 0.043 0.072 -0.109 0.194
CPSS x ICU -0.001 0.006 -0.014 0.011
Predicting “Happy” Ratings—Distress Cue Absent
β SE LLCI ULCI
CPSS 0.014 0.026 -0.041 0.067
ICU -0.059 0.065 -0.196 0.078
CPSS x ICU 0.002 0.008 -0.015 0.018
Predicting “Angry” Ratings—Distress Cue Absent
β SE LLCI ULCI
CPSS 0.020 0.038 -0.060 0.100
ICU 0.043 0.071 -0.106 0.193
CPSS x ICU 0.002 0.013 -0.026 0.030
Predicting “Sad” Ratings—Distress Cue Absent
β SE LLCI ULCI
CPSS 0.027 .027 0.332 -0.030
ICU -0.005 0.050 0.929 -0.110
CPSS x ICU -0.003 0.008 0.735 -0.019
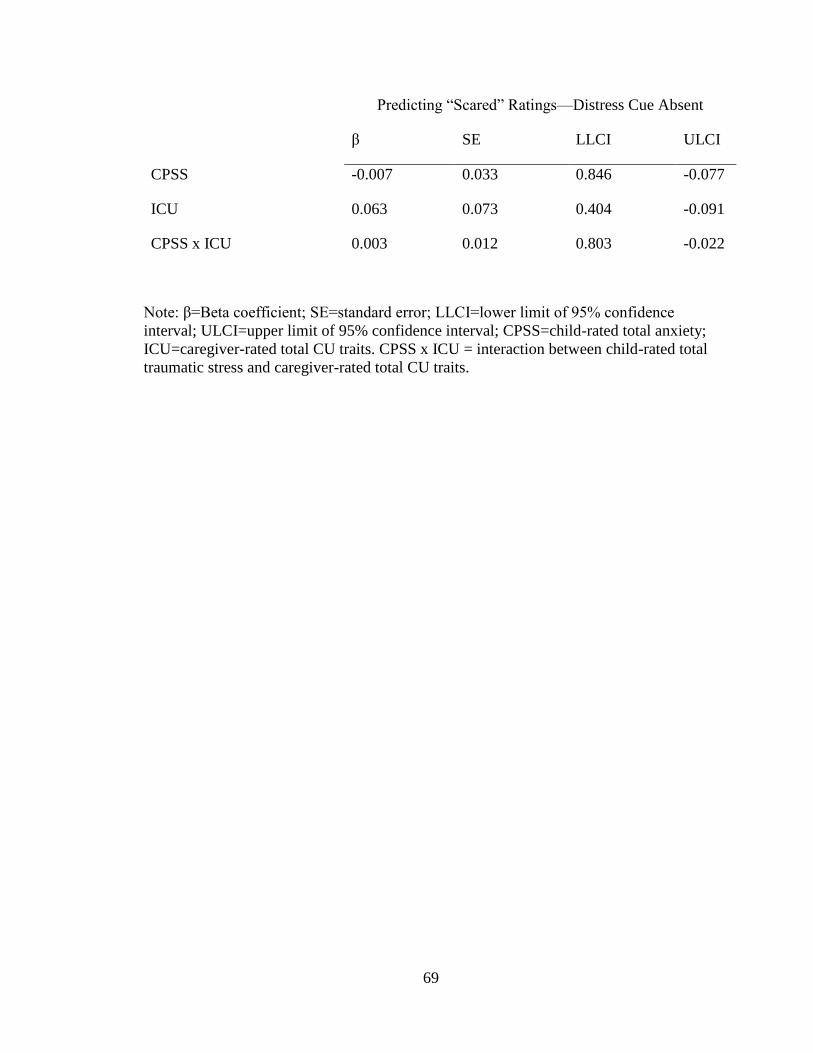
69
Predicting “Scared” Ratings—Distress Cue Absent
β SE LLCI ULCI
CPSS -0.007 0.033 0.846 -0.077
ICU 0.063 0.073 0.404 -0.091
CPSS x ICU 0.003 0.012 0.803 -0.022
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; CPSS=child-rated total anxiety;
ICU=caregiver-rated total CU traits. CPSS x ICU = interaction between child-rated total
traumatic stress and caregiver-rated total CU traits.

70
Table 9. Coefficients for the hierarchical regression models perceptions of simulated
opponent’s emotions in the presence of a distress cue, with traumatic stress as a
moderator
Predicting “Calm” Ratings—Distress Cue Present
β SE LLCI ULCI
CPSS -0.058 0.030 -0.121 0.006
ICU 0.165 0.048 0.064 0.266
CPSS x ICU 0.009 0.005 -0.002 0.019
Predicting “Happy” Ratings—Distress Cue Present
β SE LLCI ULCI
CPSS 0.003 0.028 -0.056 0.062
ICU 0.069 0.057 -0.050 0.189
CPSS x ICU -0.001 0.005 -0.011 0.009
Predicting “Angry” Ratings—Distress Cue Present
β SE LLCI ULCI
CPSS 0.034 0.031 -0.031 0.010
ICU -0.005 0.075 -0.161 0.152
CPSS x ICU 0.002 0.008 -0.016 0.019
Predicting “Sad” Ratings—Distress Cue Present
β SE LLCI ULCI
CPSS 0.012 0.038 -0.067 0.091
ICU 0.023 0.086 -0.158 0.203
CPSS x ICU 0.005 0.0007 -0.010 0.019
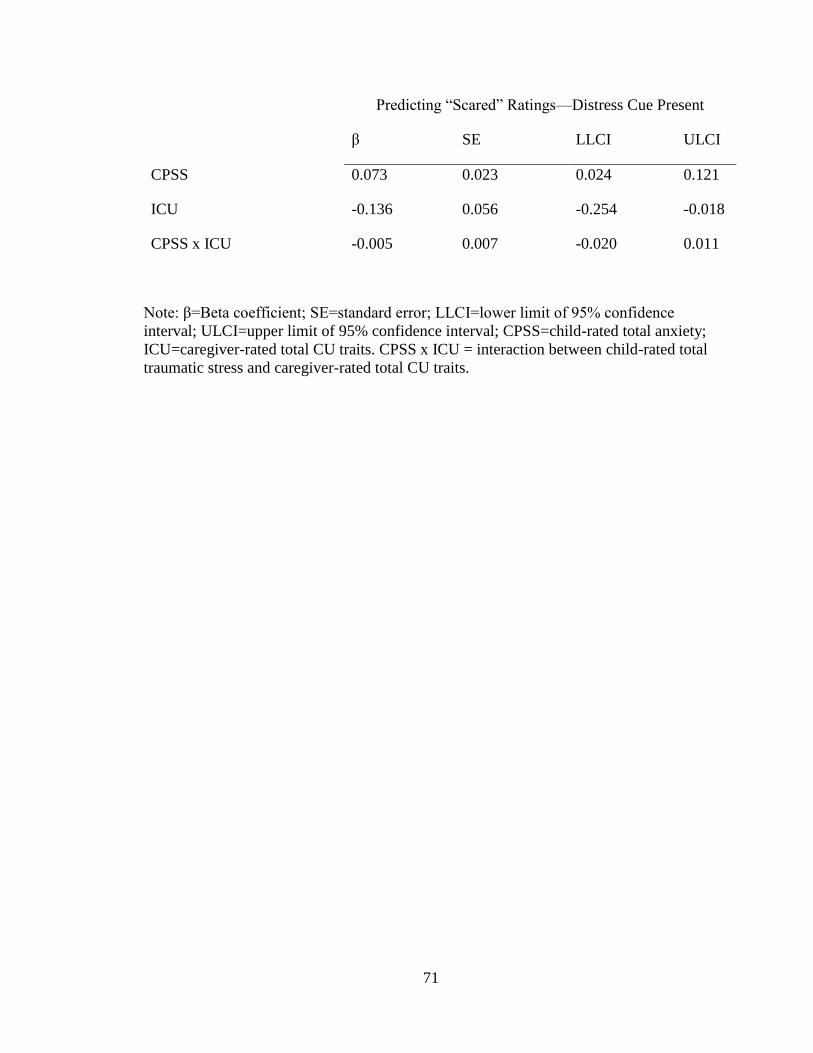
71
Predicting “Scared” Ratings—Distress Cue Present
β SE LLCI ULCI
CPSS 0.073 0.023 0.024 0.121
ICU -0.136 0.056 -0.254 -0.018
CPSS x ICU -0.005 0.007 -0.020 0.011
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; CPSS=child-rated total anxiety;
ICU=caregiver-rated total CU traits. CPSS x ICU = interaction between child-rated total
traumatic stress and caregiver-rated total CU traits.
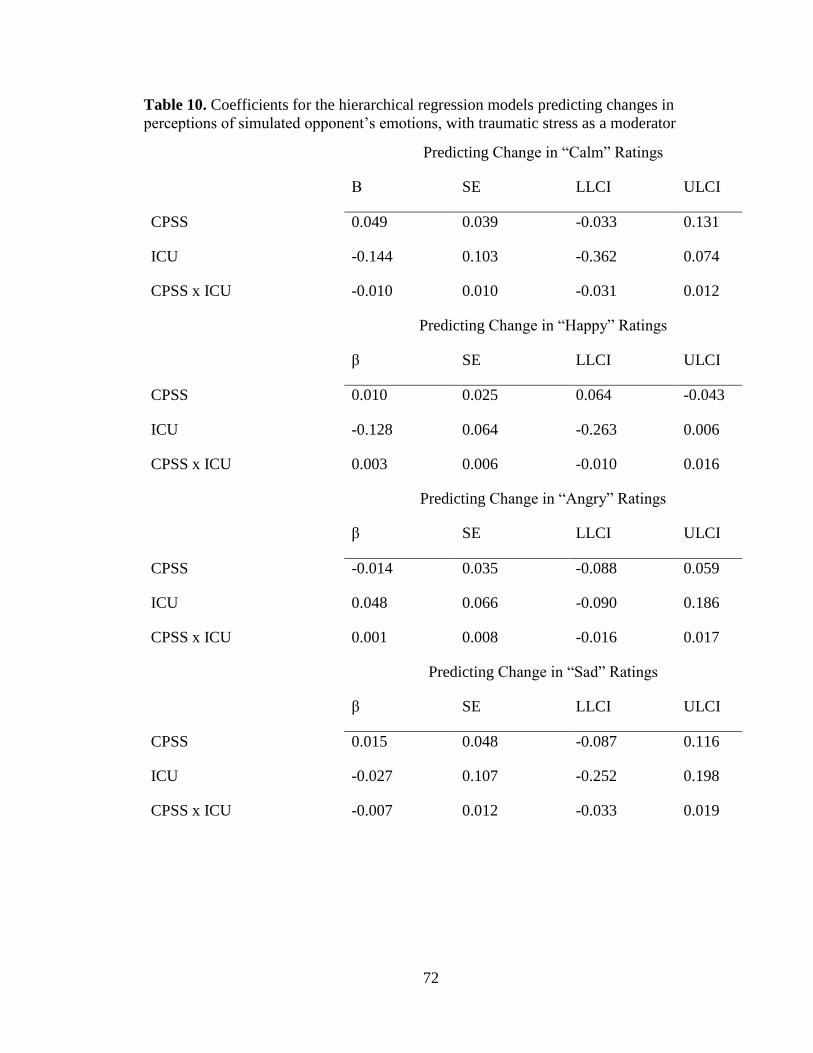
72
Table 10. Coefficients for the hierarchical regression models predicting changes in
perceptions of simulated opponent’s emotions, with traumatic stress as a moderator
Predicting Change in “Calm” Ratings
Β SE LLCI ULCI
CPSS 0.049 0.039 -0.033 0.131
ICU -0.144 0.103 -0.362 0.074
CPSS x ICU -0.010 0.010 -0.031 0.012
Predicting Change in “Happy” Ratings
β SE LLCI ULCI
CPSS 0.010 0.025 0.064 -0.043
ICU -0.128 0.064 -0.263 0.006
CPSS x ICU 0.003 0.006 -0.010 0.016
Predicting Change in “Angry” Ratings
β SE LLCI ULCI
CPSS -0.014 0.035 -0.088 0.059
ICU 0.048 0.066 -0.090 0.186
CPSS x ICU 0.001 0.008 -0.016 0.017
Predicting Change in “Sad” Ratings
β SE LLCI ULCI
CPSS 0.015 0.048 -0.087 0.116
ICU -0.027 0.107 -0.252 0.198
CPSS x ICU -0.007 0.012 -0.033 0.019

73
Predicting Change in “Scared” Ratings
β SE LLCI ULCI
CPSS -0.079 0.052 0.030 -0.189
ICU 0.199 0.116 -0.045 0.442
CPSS x ICU 0.008 0.019 -0.033 0.048
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; CPSS=child-rated traumatic
stress; ICU=caregiver-rated total CU traits; CPSS x ICU= interaction between child-rated
total traumatic stress and caregiver-rated total CU traits.
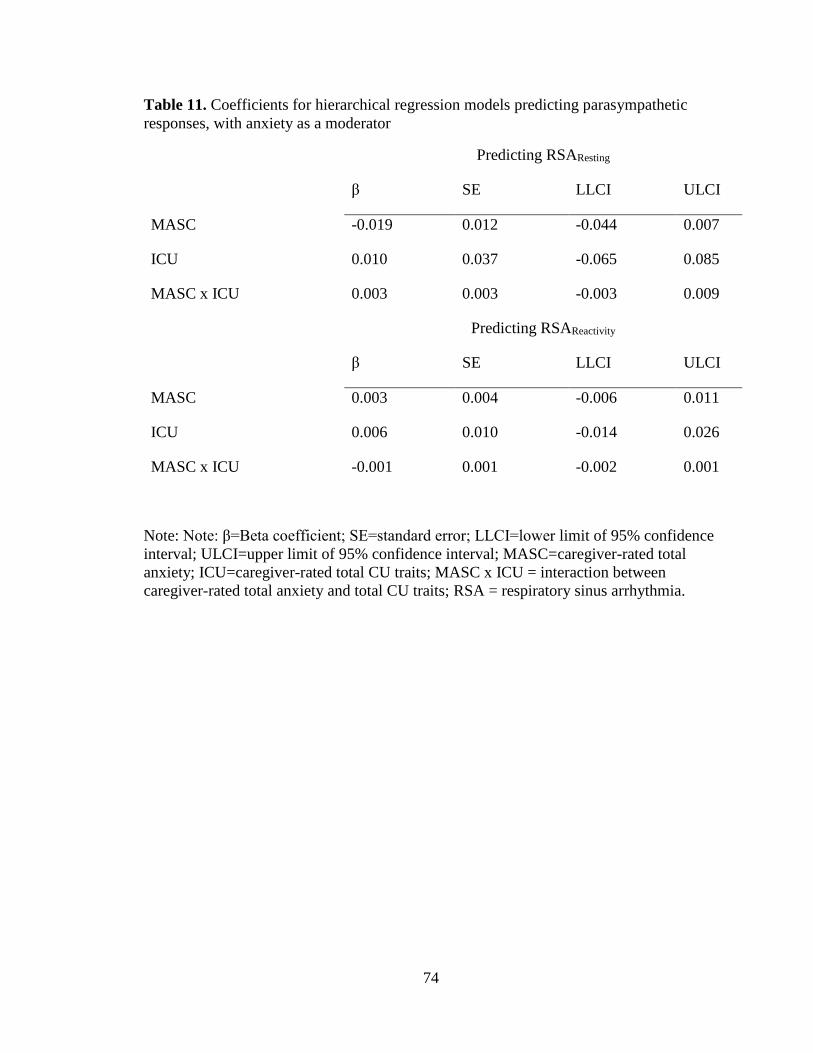
74
Table 11. Coefficients for hierarchical regression models predicting parasympathetic
responses, with anxiety as a moderator
Predicting RSAResting
β SE LLCI ULCI
MASC -0.019 0.012 -0.044 0.007
ICU 0.010 0.037 -0.065 0.085
MASC x ICU 0.003 0.003 -0.003 0.009
Predicting RSAReactivity
β SE LLCI ULCI
MASC 0.003 0.004 -0.006 0.011
ICU 0.006 0.010 -0.014 0.026
MASC x ICU -0.001 0.001 -0.002 0.001
Note: Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; MASC=caregiver-rated total
anxiety; ICU=caregiver-rated total CU traits; MASC x ICU = interaction between
caregiver-rated total anxiety and total CU traits; RSA = respiratory sinus arrhythmia.
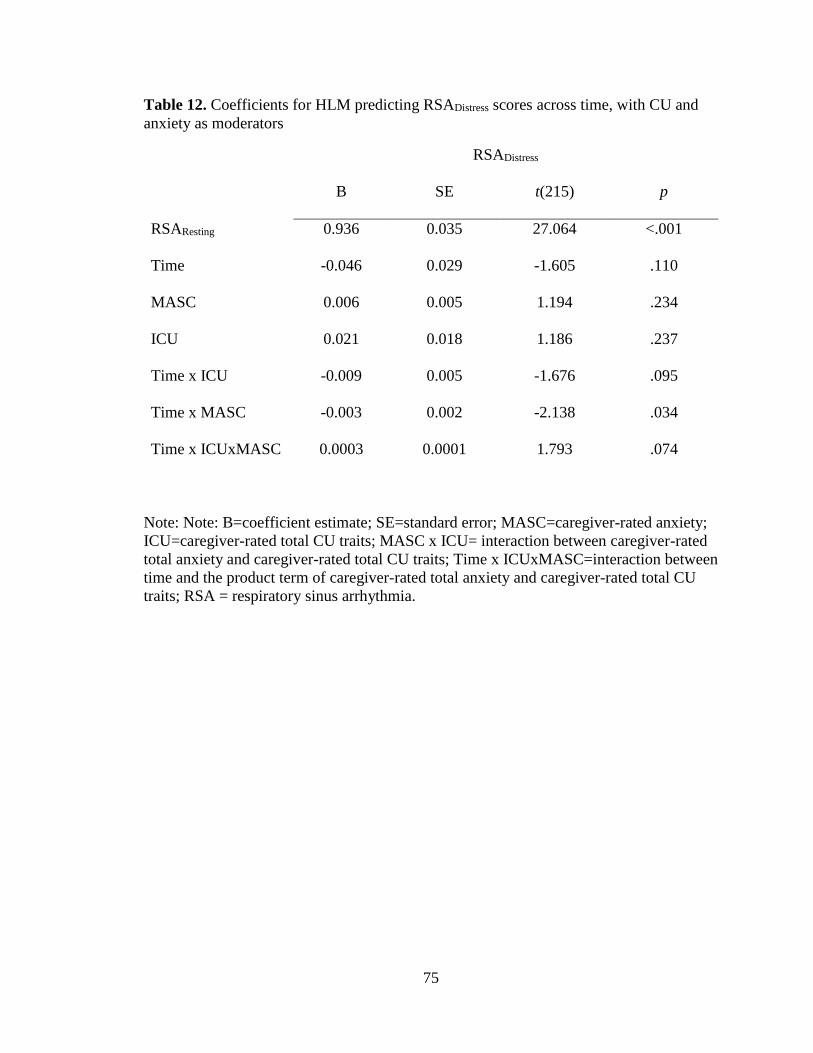
75
Table 12. Coefficients for HLM predicting RSADistress scores across time, with CU and
anxiety as moderators
RSADistress
B SE t(215) p
RSAResting 0.936 0.035 27.064 <.001
Time -0.046 0.029 -1.605 .110
MASC 0.006 0.005 1.194 .234
ICU 0.021 0.018 1.186 .237
Time x ICU -0.009 0.005 -1.676 .095
Time x MASC -0.003 0.002 -2.138 .034
Time x ICUxMASC 0.0003 0.0001 1.793 .074
Note: Note: B=coefficient estimate; SE=standard error; MASC=caregiver-rated anxiety;
ICU=caregiver-rated total CU traits; MASC x ICU= interaction between caregiver-rated
total anxiety and caregiver-rated total CU traits; Time x ICUxMASC=interaction between
time and the product term of caregiver-rated total anxiety and caregiver-rated total CU
traits; RSA = respiratory sinus arrhythmia.
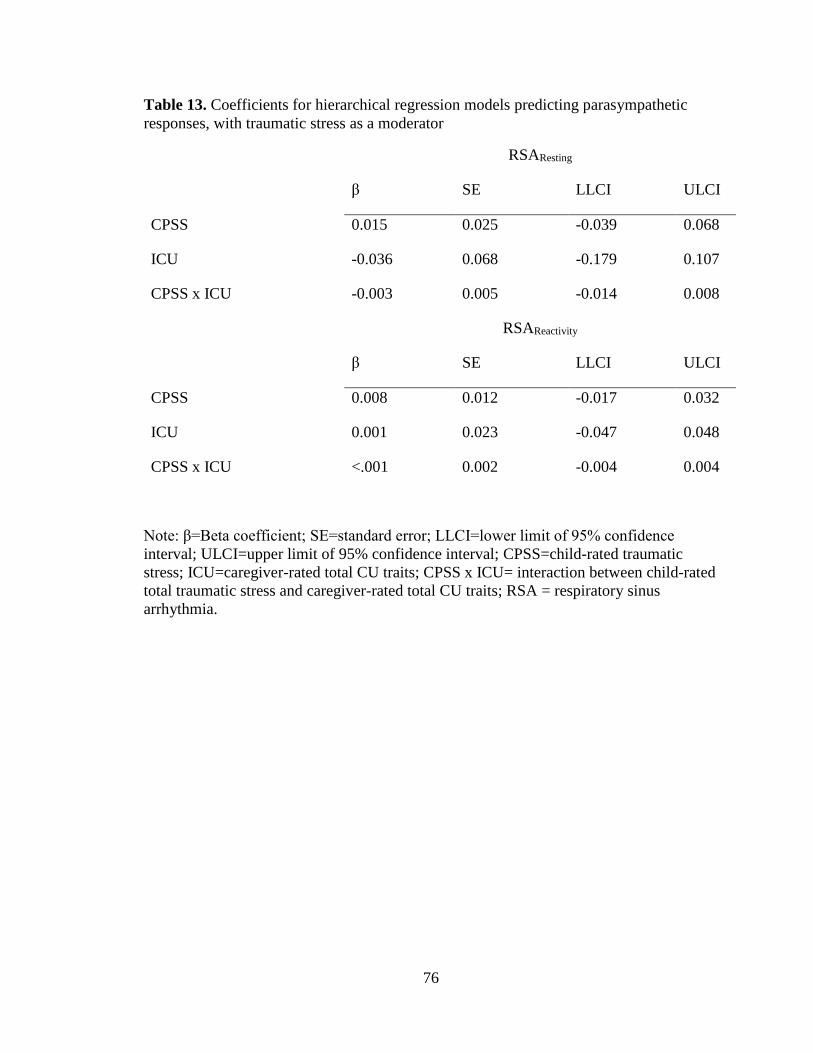
76
Table 13. Coefficients for hierarchical regression models predicting parasympathetic
responses, with traumatic stress as a moderator
RSAResting
β SE LLCI ULCI
CPSS 0.015 0.025 -0.039 0.068
ICU -0.036 0.068 -0.179 0.107
CPSS x ICU -0.003 0.005 -0.014 0.008
RSAReactivity
β SE LLCI ULCI
CPSS 0.008 0.012 -0.017 0.032
ICU 0.001 0.023 -0.047 0.048
CPSS x ICU <.001 0.002 -0.004 0.004
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; CPSS=child-rated traumatic
stress; ICU=caregiver-rated total CU traits; CPSS x ICU= interaction between child-rated
total traumatic stress and caregiver-rated total CU traits; RSA = respiratory sinus
arrhythmia.
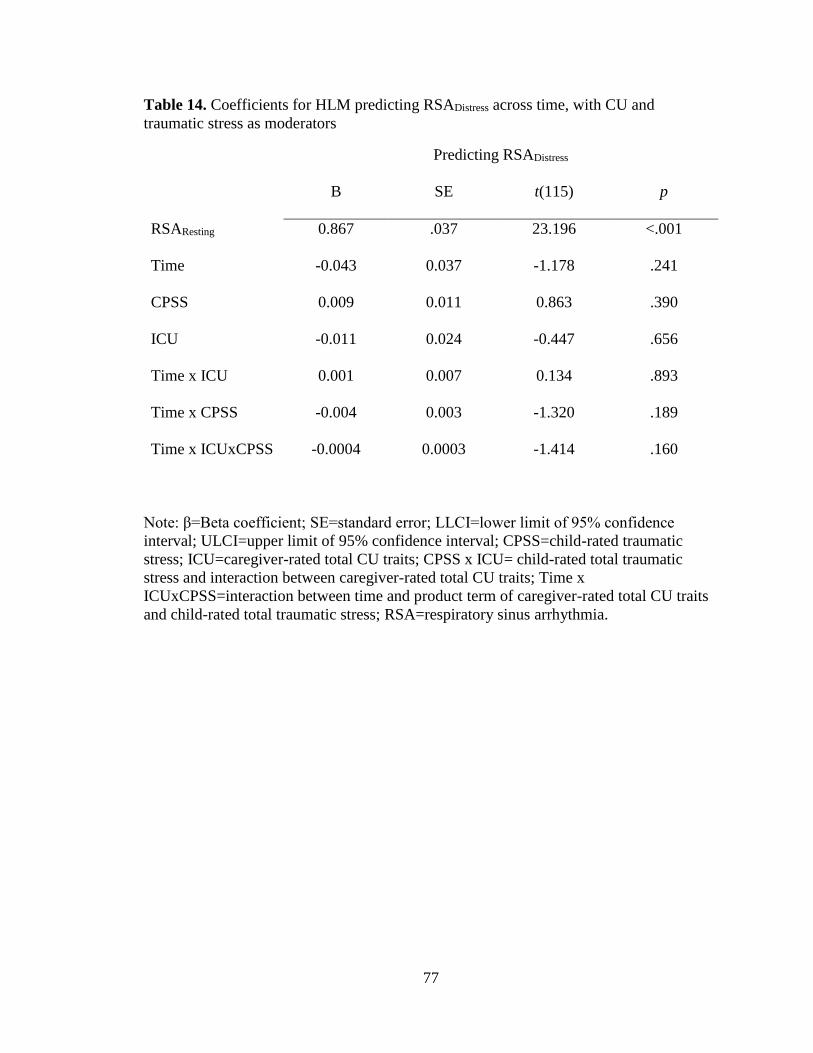
77
Table 14. Coefficients for HLM predicting RSADistress across time, with CU and
traumatic stress as moderators
Predicting RSADistress
B SE t(115) p
RSAResting 0.867 .037 23.196 <.001
Time -0.043 0.037 -1.178 .241
CPSS 0.009 0.011 0.863 .390
ICU -0.011 0.024 -0.447 .656
Time x ICU 0.001 0.007 0.134 .893
Time x CPSS -0.004 0.003 -1.320 .189
Time x ICUxCPSS -0.0004 0.0003 -1.414 .160
Note: β=Beta coefficient; SE=standard error; LLCI=lower limit of 95% confidence
interval; ULCI=upper limit of 95% confidence interval; CPSS=child-rated traumatic
stress; ICU=caregiver-rated total CU traits; CPSS x ICU= child-rated total traumatic
stress and interaction between caregiver-rated total CU traits; Time x
ICUxCPSS=interaction between time and product term of caregiver-rated total CU traits
and child-rated total traumatic stress; RSA=respiratory sinus arrhythmia.

78
Aim I/b.
Aim II/b.
Aim III/b.
Figure 4. Visual depiction of statistical models.
CU Traits Aggression
Anxiety/Traumatic Stress
CU Traits Aggression without Salient Distress Cue/
PPS Ratings/Change in PPS Ratings
Anxiety/Traumatic Stress
CU Traits Aggression with Salient Distress Cue/
PPS Ratings/Change in PPS Ratings
Anxiety/Traumatic Stress
CU Traits Parasympathetic Regulation
Anxiety/Traumatic Stress

79
Figure 5. Graph depicting the interactive relationship between CU and anxiety when
predicting aggression in the absence of a distress cue.
0
2
4
6
8
10
12
ICU Low ICU Med ICU High
MASC Low MASC Med MASC High
Aggre
ssio
n—
Dis
tres
sC
ue
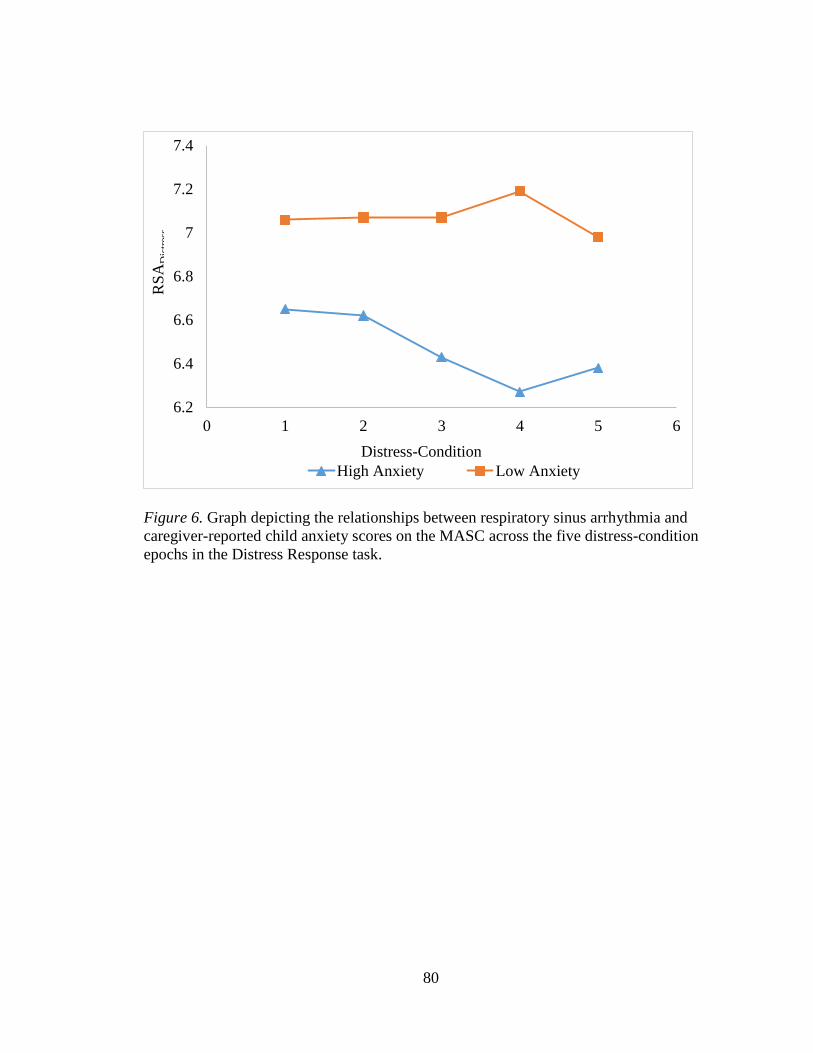
80
Figure 6. Graph depicting the relationships between respiratory sinus arrhythmia and
caregiver-reported child anxiety scores on the MASC across the five distress-condition
epochs in the Distress Response task.
6.2
6.4
6.6
6.8
7
7.2
7.4
0 1 2 3 4 5 6
High Anxiety Low Anxiety
RS
AD
istr
ess
Distress-Condition
81
VITA
KATHLEEN ISABEL CRUM
2005-2009 B.A., Psychology, Honors College, Summa Cum Laude
Florida International University
Miami, Florida
2009 National Institute of Health Travel Award
2010-2014 M.S., Psychology
Florida International University
Miami, Florida
2010-2016 Graduate Assistant
Florida International University
Miami, Florida
2013 & 2014 Award for Distinguished Poster Contribution
2014 Elizabeth Munsterberg Koppitz Graduate Student
Fellowship in Child Psychology
2014-2016 Doctoral Candidate
Florida International University
Miami, Florida
2015 Student Research Award Competition Honorable Mention
2015-2016 Clinical Intern
Medical University of South Carolina
Charleston, South Carolina
SELECTED PUBLICATIONS
Babinski, D.E., Waxmonsky, J.G., Waschbusch, D.A., Humphrey, H., Alfonso, A.,
Crum, K.I.,…Pelham, W.E. (2014). A pilot study of stimulant medication for adults with
ADHD who are parents of adolescents with ADHD: the acute effects of stimulant
medication on observed parent-adolescent interactions. Journal of Child and Adolescent
Psychopharmacology, 24(10), 582-585.
Detweiler, M. F., Comer, J. S., Crum, K. I., & Albano, A. M. (2014). Social anxiety in
children and adolescents: Biological, developmental, and social considerations. In S. G.
Hofmann, & P. M. DiBartolo (Eds.), From social anxiety to social phobia: Multiple
perspectives (3rd ed.). Boston, MA: Allyn and Bacon.
82
Miller, N.V., Haas, S. M., Waschbusch, D. A., Willoughby, M. T., Helseth, S. A., Crum,
K. I., Coles, E. K., & Pelham, W. E., Jr. (2014). Behavior therapy and callous-
unemotional traits: Effects of a pilot study examining modified behavioral contingencies
on child behavior. Behavior Therapy, 45(5), 606-618.
Waxmonsky, J. G., Waschbusch, D. A., Babinski, D. E., Humphrey, H. H., Alfonso, A.,
Crum, K.I., Bernstein, M., Slavec, J., Augustus, J. N., & Pelham, W. E. (2014). Does
pharmacological treatment of ADHD in adults enhance parenting performance? Results
of a double-blind, randomized trial. CNS Drugs, 28(7), 665-677.
Chou, P., Cornacchio, D., Cooper-Vince, C., Crum, K. I., & Comer, J. S. (2015). DSM-5
and the assessment of childhood anxiety disorders: Meaningful progress, new problems,
or persistent diagnostic quagmires? Psychopathology Review, 2(1), 30-51.
Crum, K. I., & Comer, J. S. (2015). Using synchronous videoconferencing to deliver
family-based mental health care. Journal of Child and Adolescent Psychopharmacology,
26(3), 229-234.
Crum, K. I., Cornacchio, D., Greif Green, J., Coxe, S., & Comer, J. S. (2015). Conduct
problems among youth exposed to the Boston Marathon attack: The moderating role of
violent crime exposure. Journal of Clinical Child and Adolescent Psychology. (Online.)
Crum, K. I., Waschbusch, D. A., Bagner, D., & Coxe, S. (2015). Effects of callous-
unemotional traits on the association between parenting and child conduct problems.
Child Psychiatry and Human Development, 46(6), 967-980.
Cornacchio, D., Crum, K. I., Coxe, S., Pincus, D. B., & Comer, J. S. (2016). Irritability
and severity of anxious symptomatology among youth with anxiety disorders. Journal of
the American Academy of Child and Adolescent Psychiatry, 55(1), 54-61.
Crum, K. I., Waschbusch, D. A., & Willoughby, M. T. (2016). Callous-unemotional traits
influence the nature of the student-teacher relationship and its association with long-term
outcomes. Journal of Emotional and Behavioral Disorders, 24, 16-29.
Waschbusch, D. A., Willoughby, M. T., Haas, S. M., Helseth, S. A., Crum, K. I.,
Altszuler, A. R., Ross, J. M., Coles, E. K., & Pelham Jr., W. E. (in press). Effects of
behavioral treatment modified to fit the learning style of children with conduct problems
and callous-unemotional (CU) traits. Journal of Consulting and Clinical Psychology.
Crum, K. I., Cornacchio, D., Coxe, S., Greif Green, J., & Comer, J. S. (accepted). The co-
occurrence of posttraumatic stress and conduct problems following the Boston Marathon
bombing: A latent profile analysis. Journal of Traumatic Stress.