Embed Size (px)
Citation preview
1
ANXIETY DISORDERS AND CHRONIC PAIN: AN UPDATE FOR NON PAIN SPECIALISTS
Ricks Warren, Ph.D., ABPPDan DeSena, LMSW, DMAAnxiety Disorders Program
Dept. of Psychiatry University of MichiganADAA, March 5, 2010
Baltimore, MD
Overview of Workshop
• Relationship between anxiety disorders and chronic pain
• Interventions for anxiety and fear in chronic pain
• Depression, anger, and perceive injustice as risk factors
• Psychosocial treatments for chronic pain
2
Prevalence and Cost of Chronic Pain
• Approximately 10% of the general population report having experienced chronic idiopathic (noncancer related) pain in the past 12 months
• Direct cost: About $100 billion annually
• Adding indirect costs due to absenteeism and lost productivity: $200 billion
• Asmundson & Katz (2009)
Definitions of Pain—The Fifth Vital Sign
• The International Association for the Study of Pain (IASP) defines pain as
• “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or as described by the patient in terms of such damage”
• “The IASP defines chronic pain as ‘pain which has persisted beyond normal tissue healing time’, taken, in absence of other criteria, to be 3 months.” (Smith et al, 1999).
3
Definitions of Pain
• Pain• Acute Pain• Chronic Pain• Chronic vs. Acute Pain• Recurrent Pain• Pain Behaviors• Disability• Thorne (2004)
A BiopsychosocialConceptual Model of Pain
PAIN BEHAVIOR
SUFFERING
PAIN
NOCICEPTION
Clinical Essentials of Pain Management, Robert J Gatchel, 2005
4
Psychosocial Risk Factors
“There is increasing acceptance that psychosocial factors play a crucial role in the transition from an acute episode of low back pain (LBP) or a sequence of such episodes, to a chronic back disorder, and that they may also be etiological factors.” Pincus, et al. (2002)
“Psychosocial factors and emotional distress should be assessed because they are stronger predictors of low back pain outcomes than either physical examination findings or severity and duration of pain”
(Chou et al., 2007)
Passive coping (worrying, fear avoidance, anger and frustration)predicted poorer outcome, and optimism, active coping strategies, and greater social support predicted better outcome in neck pain.
(Carroll et al. 2008)
Psychological Risk Factors
• Depression• Anxiety/Fear• Anger• Perceived Injustice
5
Depression
• Research suggests that 40% to 50% of chronic pain patients suffer from depressive disorders.
• Chronic pain often leads to depression.• A prospective study (Jarvik et al., 2005) demonstrated
that levels of depression predicted the development of low back pain 3 years following the initial assessment. Patients with depression were 2.3 times more likely to report back pain compared to those who did not report back pain.
• Rates of suicidal ideation and attempts are 2-3 times higher with chronic pain than in gen. pop. (Edwards et al. 2006).
Why aren’t All Chronic Pain Patients Depressed?
Two factors appear to mediate the pain-depression relationship:
1. Patient’s appraisals of the effects of the pain on their lives and,
2. Appraisals of their ability to exert any control over their pain and lives.
Rudy et al., 1988; Turk, Okifuji, & Scharff, 1995; Gatchel et al., 2007)
6
Anxiety Disorders and Chronic Pain
• “Among studies that have examined the co-occurrence of anxiety disorders and depressive disorders with chronic pain conditions, it is noteworthy that the associations between anxiety disorders and chronic pain have been found to be stronger than the associations between depression and chronic pain” (Sareen et al.,2005).
Anxiety Disorders and Pain• Panic Disorder
– 71% reported current pain symptoms– 40% reported chronic pain (Kuch et al.,1991)
• Social Anxiety Disorder– Similar findings (Admundson et al., 2000)
• PTSD– 30% of patients seeking outpatient tx for PTSD report
chronic pain.– 50 to 80% of military veterans and volunteer
firefighters with PTSD report chronic pain– Asmundson & Katz (2009).
7
Pain and Anxiety Disorders
• “Findings from community –dwelling adults (n=85,088) from 17 countries indicate that those with back or neck pain are two to three times more likely to have had past 12-month panic disorder, agoraphobia, or social anxiety disorder, and almost three times more likely to have had GAD or PTSD.”– Asmundson & Katz (2009.
Which Comes First?
• Anxiety Disorders may be as likely to precede as to follow the onset of the pain condition.
Asmundson & Katz (2009).
8
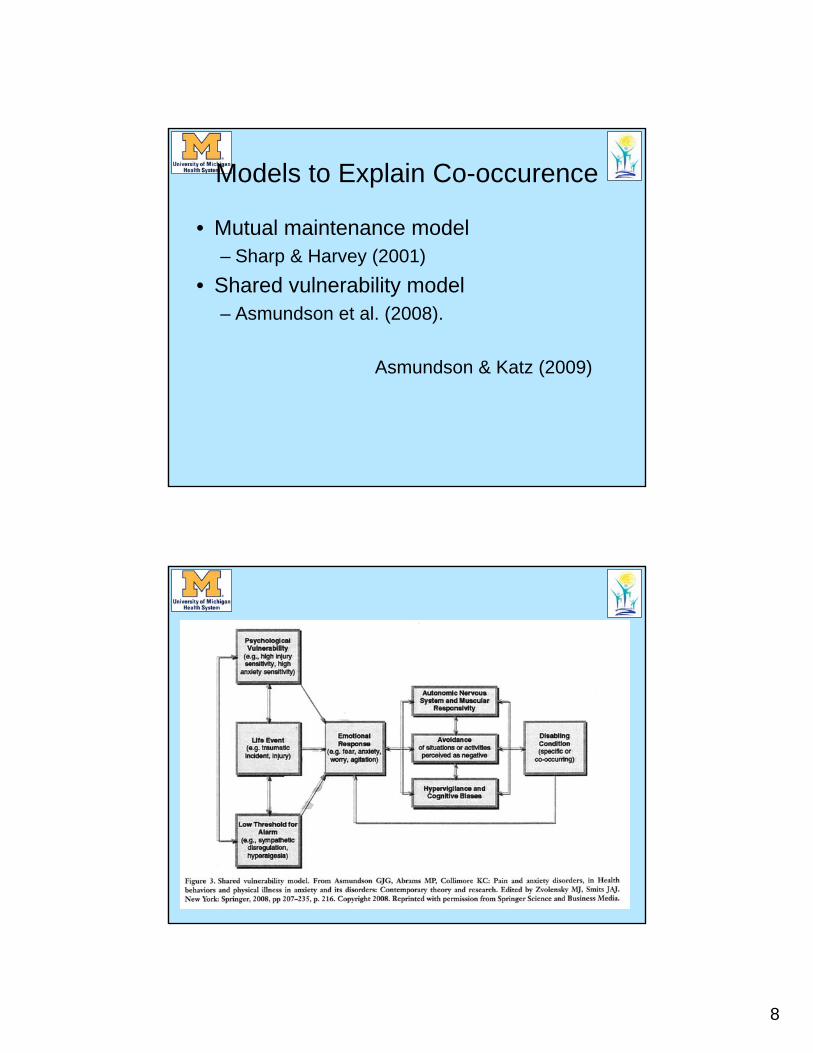
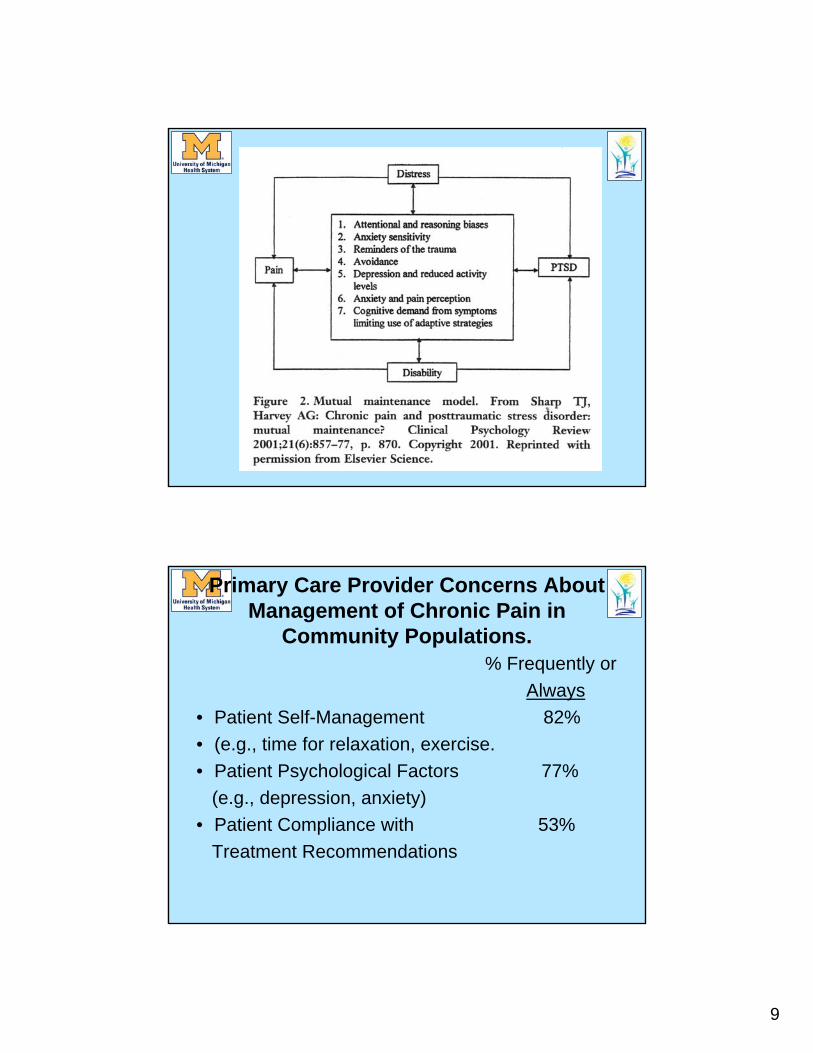
Models to Explain Co-occurence
• Mutual maintenance model– Sharp & Harvey (2001)
• Shared vulnerability model– Asmundson et al. (2008).
Asmundson & Katz (2009)
9
Primary Care Provider Concerns About Management of Chronic Pain in
Community Populations.% Frequently or
Always• Patient Self-Management 82%• (e.g., time for relaxation, exercise.• Patient Psychological Factors 77%
(e.g., depression, anxiety)• Patient Compliance with 53%
Treatment Recommendations
10
Assessment Tools
• Brief Pain Inventory (Cleeland, 1991).• Pain Disability Index (Pollard, 1984)• Beck Depression Inventory II (Beck et al., 1996)• Patient Health Questionnaire (PHQ; also a
measure of depression)• Fear Avoidance and Belief Questionnaire
(Waddell et al., 1993) • Pain Catastrophizing Scale (Sullivan et al.,
1995)• Pain Anxiety Symptom Scale-20 (PASS-20).
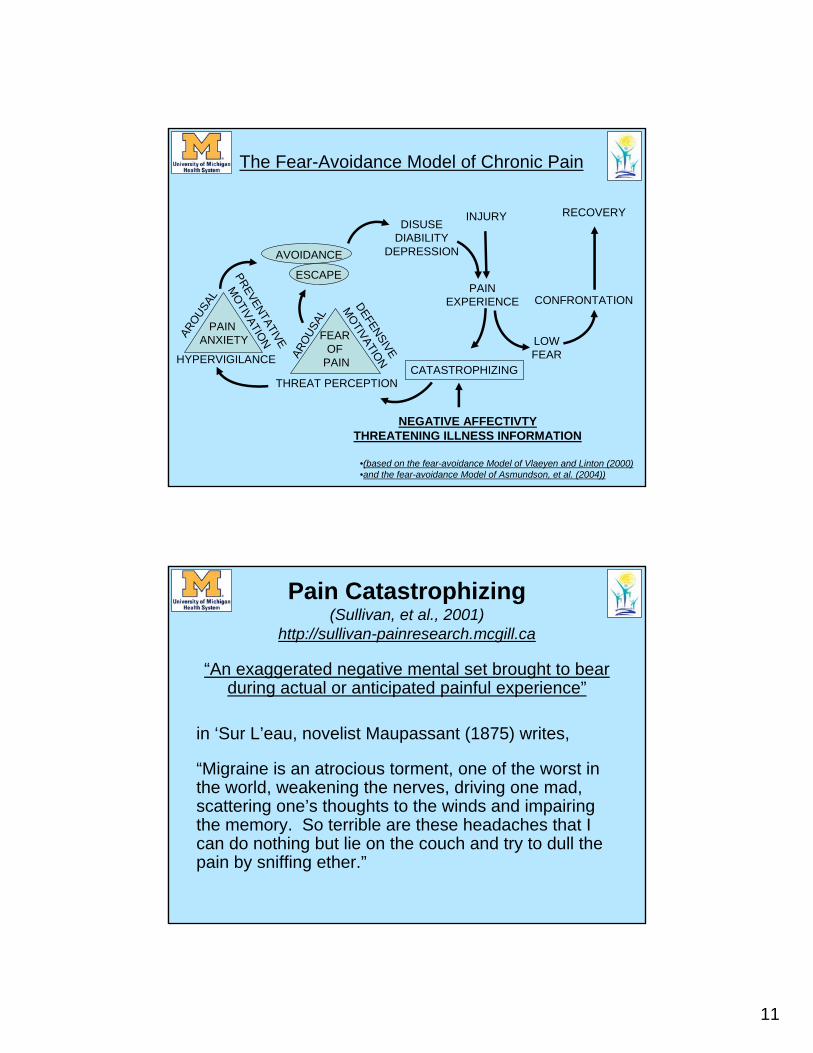
The Fear-Avoidance Model of Musculoskeletal Pain
(Waddell et al.,1993, Leeuw et al., 2007, Gatchel et al., 2007)
• Fear-avoidance beliefs in patients seeking care for acute pain may be predictive of pain persistence, disability, and long-term sick leave.
• These beliefs are also related to the future inception of back pain in the general population.
• Fear-avoidance beliefs of health care providers were found to be related to their treatment behavior and their recommendations for engaging in physical activities.
11
AVOIDANCE
DISUSEDIABILITY
DEPRESSION
ESCAPE
FEAR OF
PAINAROU
SAL
THREAT PERCEPTION
DEFENSIVE
MOTIVATION
PAIN ANXIETY
HYPERVIGILANCE
AROUSA
L
PREVENTATIVE
MOTIVATION
CATASTROPHIZING
NEGATIVE AFFECTIVTYTHREATENING ILLNESS INFORMATION
INJURY
LOWFEAR
CONFRONTATION
RECOVERY
PAINEXPERIENCE
The Fear-Avoidance Model of Chronic Pain
•(based on the fear-avoidance Model of Vlaeyen and Linton (2000) •and the fear-avoidance Model of Asmundson, et al. (2004))
Pain Catastrophizing (Sullivan, et al., 2001)
http://sullivan-painresearch.mcgill.ca
“An exaggerated negative mental set brought to bear during actual or anticipated painful experience”
in ‘Sur L’eau, novelist Maupassant (1875) writes,
“Migraine is an atrocious torment, one of the worst in the world, weakening the nerves, driving one mad, scattering one’s thoughts to the winds and impairing the memory. So terrible are these headaches that I can do nothing but lie on the couch and try to dull the pain by sniffing ether.”
12
Pain Castastrophizing (Cont’d)
Sullivan (2009) comments that, “Maupassant’s words describe the torment of his pain, his emotional distress, and the disability that pain brings to his life. He feels overwhelmed by his pain, and helpless to deal with it. He surrenders to the pain, and seeks chemical means of dulling it”.
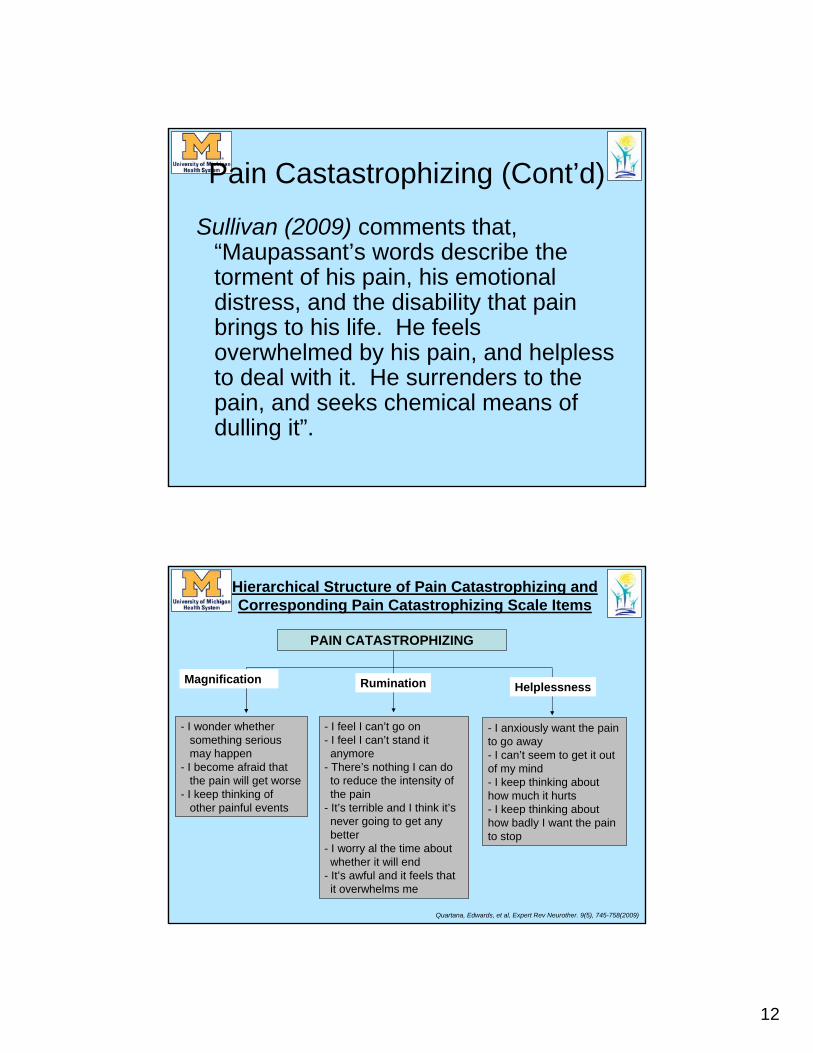
Hierarchical Structure of Pain Catastrophizing and Corresponding Pain Catastrophizing Scale Items
Rumination
- I wonder whether something serious may happen
- I become afraid that the pain will get worse
- I keep thinking of other painful events
- I feel I can’t go on- I feel I can’t stand it anymore
- There’s nothing I can do to reduce the intensity of the pain
- It’s terrible and I think it’s never going to get any better
- I worry al the time about whether it will end
- It’s awful and it feels that it overwhelms me
- I anxiously want the pain to go away- I can’t seem to get it out of my mind- I keep thinking about how much it hurts- I keep thinking about how badly I want the pain to stop
Magnification
PAIN CATASTROPHIZING
Helplessness
Quartana, Edwards, et al, Expert Rev Neurother. 9(5), 745-758(2009)
13
Pain Catastrophizing (cont.)
Pain Catastrophizing is associated with:
•Heightened pain experience, acute and chronic pain severity
•Illness behaviors, including, the frequency and duration of hospital stay, use of staff-administered analgesics after breast cancer surgery, more frequent visits to health-care professionals, and use of over-the-counter medication.
Pain Catastrohizing (Cont’d)
• Heightened disability, even when controlling for depression, anxiety, neuroticism, disease severity, and pain severity.
• Postsurgical pain outcomes and disability, and pain-related activity interference.
• Deleterious effects on patients’ social support networks.
14
Pain Catastrophizing (cont.)
• Is independent of other pain related distress variables, such as anxiety, fear of pain, and neuroticism.
• May be predictive of the inception on chronic musculoskeletal pain in the general population.
• May predict depression and suicide ideation
Pain Catastrophizing (cont.)
• Is reduced with CBT and/or physical therapy interventions and may mediate reductions in disability and pain intensity.
15
Anger and Pain
• Higher level of anger is associated with higher level of pain.
• Possible reasons include:Anger increases muscle reactivity in specific sites where there is pain.Endogeneous opiod dysfunctionAlterations in immune system functioningAnger may lead to aversive interpersonal reactionsAnger may increase depressed mood
Perceived Injustice
Perceptions of injustice are also associated with the persistence of post-traumatic stress symptoms consequent to injury.” (Sullivan, 2008, p.4.)
16
Perceived Injustice
Injured individuals who report high levels of perceived injustice also experience more intense pain, more severe depression and are less likely to return to work….. display more pain behavior and rate themselves as being more severely disabled.
Perceived Injustice
“Recent research suggests that perceived injustice consequent to injury might represent one of the strongest predictors of problematic outcomes.
Injured individuals who report high levels of perceived injustice also experience more intense pain, more severe depression and are less likely to return to work….. display more pain behavior and rate themselves as being more severely disabled (User Manual for the Injustice Experience Questionnaiare, p. 4, Sullivan, 2008
http://sullivan-painresearch.mcgill.ca
17
Anger Targets and Intensity
• 69% of patients angry at someone• Targets Intensity• 74% Self 4.46%• 62% Health Care Providers 3.50%• 59% Person Who Caused Injury .53%• 38% Whole World 1.97%
• (96 chronic low back and leg pain pts. (Okifuji et al., 1999)
Anger Targets and Intensity
• “The intensity of anger directed toward oneself was significantly related to pain severity and depression” (p. 9).
18
Anger Constructs
• Trait vs state anger• Anger management style
Anger in vs. Anger out• Hostility• Aggression
Anger Interventions
• Constructive verbal expression (assertiveness training
• Cognitive reappraisal• Relaxation training• Overcoming Situational and General
Anger (Deffenbacher & Mckay, 2000)• Hostility reduction programs (Gidron et
al.,1999).
19
Anger Assessment
• Injustice Experience Questionnaire (Sullivan, 2002)
• Targets of Anger Scale (Okifuji et al., 1999)
CBT for Pain Management
• Disclosure• Cognitive Restructuring• Activity Scheduling• Relaxation and Biofeedback• Hypnosis• Exposure Interventions
• Main et al. (2008)
20
More CBT for Chronic Pain
• Cognitive-Coping Strategies• Expressive Writing Exercises• Assertiveness Training• Education- About pain and the stress-pain
conncection
• Thorne (2004)
Cognitive-Coping Strategies for Chronic Pain Management
• Focused Attention• Distancing• Positive Self-Statements• Ignoring Pain• Praying/Hoping/Wishing• Imagery Distraction• Mental Distraction• Catastrophizing Thorne (2004)
21
Focused Attention
• Description: Attending to the sensory qualities of the pain
• Example: “I think of myself as being interested in pain and wanting to describe it to myself in detail”
• Potential Utility: Some support
Distancing
• Descritption: Reinterpreting pain sensations in a emotionally detached way
• Example: “I try not to think of it as my body, but rather as something separate from me.”
• Potential Utility: Some support
22
Positive Self-Statements
• Description: Telling oneself that one can manage the pain.
• Example: “I ‘psych’ myself up to deal with the pain, perhaps telling myself that it won’t last much longer.”
• Potential Utility: Good
Ignoring the Pain
• Description: Disregarding or overlooking the pain
• Example: “I don’t pay any attention to it.• ”• Potential Utility: Equivocal
23
Praying/Hoping/Wishing
• Description: “Calling upon God or luck to cure and end the pain.”
• Example: “I pray for the pain to stop.”
• Potential Utility: Not helpful
Imagery Distraction
• Description: Imagining a scene incompatible with pain
• Example: “I use my imagination to develop pictures that help distract me.”
• Potential Utility: Not helpful
24
Mental Distraction
• Description: Distraction through mental activity.
• Example: I describe objects in the room to myself.”
• Potential Utility: Not helpful
Catastrophizing
• Description: Focusing on the Negative Emotional Component of the Pain.
• Example: “I find myself expecting the worst.”
• Potential Utility: Anticopingn
25
Are There Protective Factors for Chronic Pain and Disability?
(Gatchel et al., 2007).
Optimism—“the tendency to believe that one will generally experience good vs. bad outcomes in life” (Scheir & Carver, 1985)
• Related to less catastrophizing and more use of active coping strategies in chronic pain patients.
Optimism
• Predicted pleasant daily mood in fibromyalgia.
• In rheumatoid arthritis, optimism associated with less depression, higher life satisfaction and to less pain for patients in the early and intermediate stages of disease.
26
Optimism
• Associated with better general health, adaptation to chronic disease and recovery after various surgical procedures.
• Predicted ischemic pain tolerance and unpleasantness in patients with TMJ.
Stages of Change Model• Pain Stages of Change Questionnaire• Multidimensional Pain Readiness to Change
Questionnaire
– Precontemplation
– Contemplation
– Action
– Maintenance
27
Motivational Interviewing in Musculoskeletal Care
• Shannon & Hillsdon, 2007
Acceptance and Chronic Pain (McCracken & Vowles, 2006)
• “There is increasing supportive evidence for acceptance of chronic pain, with a general finding that greater acceptance is associated with less disability, distress, and utilization of healthcare resources (see Vowles et al., 2008).
• Acceptance and Commitment Therapy for Chronic Pain (Dahl et al., 2005).
• Living Beyond Your Pain (Dahl & Lundgren, 2006).
28
Mindfulness Based Stress Reduction (MBSR)
• Full Catastrophe Living: Using the Wisdom of your body and mind to face stress, pain, and illness (Kabat-Zinn, 1990; Morone et al., 2008)
Loving-Kindness Meditation for Chronic Low Back Pain
• Patients with chronic low back pain who participated in an 8-week loving-kindness program, compared with usual care, demonstrated significant reductions in pain, anger, and psychological distress.
• Carson et al.,2005.





























