Embed Size (px)
Citation preview
Journal of Traumatic Stress, Vol. 19, No. 4, August 2006, pp. 471–479 ( C© 2006)
Anxiety Sensitivity and Depression: Mechanismsfor Understanding Somatic Complaints in VeteransWith Posttraumatic Stress Disorder
Matthew JakupcakSeattle Division, Puget Sound Health Care System, Seattle, WA and Department of Psychiatryand Behavioral Sciences, University of Washington School of Medicine, Seattle, WA
Travis OsborneEvidence-Based Treatment Centers of Seattle, Seattle, WA and Department of RehabilitationMedicine, University of Washington School of Medicine, Seattle, WA
Scott Michael and Jessica CookSeattle Division, Puget Sound Health Care System, Seattle, WA and Department of Psychiatryand Behavioral Sciences, University of Washington School of Medicine, Seattle, WA
Peg AlbrizioSeattle Division, Puget Sound Health Care System, Seattle, WA
Miles McFallSeattle Division, Puget Sound Health Care System, Seattle, WA and Department of Psychiatryand Behavioral Sciences, University of Washington School of Medicine, Seattle, WA
A study was conducted among 45 male veterans seeking inpatient treatment for posttraumatic stressdisorder (PTSD) to test whether the relationship between PTSD and somatic complaints was accountedfor by depression and anxiety sensitivity. Posttraumatic stress disorder symptom severity, depressionsymptom severity, and anxiety sensitivity were each positively and significantly related to veterans’self-reported severity of somatic complaints. Results of hierarchical regression analyses indicated thatanxiety sensitivity and depression severity account for the relationship between PTSD and veterans’somatic complaints, suggesting PTSD influences somatic complaints by virtue of underlying symptomsof depression and anxiety sensitivity.
A line of research has emerged with regard to the re-
lationship between PTSD and somatic complaints (e.g.,
Beckham et al., 1998; Shalev, Bleich, & Ursano, 1990).
Among people with both PTSD and somatic symp-
toms (i.e., physical pain, cardiovascular, neurological, gas-
trointestinal, and audiological difficulties), pain symptoms
are the most commonly reported complaint (McFarlane,
Atchison, Rafolowicz, & Papay, 1994; Shalev et al., 1990;
Correspondence concerning this article should be addressed to: Matthew Jakupcak, VAPSHCS Psychiatry, 1660 S. Columbian Way, Seattle, WA 98108. E-mail:[email protected].
C© 2006 International Society for Traumatic Stress Studies. This article is a US Government work and, as such, is in the public domain in the United States of America. Published onlinein Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/jts.20145
White & Faustman, 1989). White and Faustman (1989)
examined the medical records of male veterans seeking in-
patient treatment for PTSD and found that 42% of the
sample had evidence of multiple medical problems, with
25% of the veterans suffering from musculoskeletal or pain
problems. However, there is evidence that self-reports of
pain are higher in individuals with PTSD compared to in-
dividuals without PTSD, even in the absence of objective
471

472 Jakupcak et al.
assessments of physical injury (Asmundson & Norton,
1995; McFarlane et al., 1994; Shalev et al., 1990), per-
haps indicating that somatization may be more common
among people with PTSD (see also, Engel, 2004).
Beckham and colleagues (1997) investigated rates of
chronic pain and somatization in veterans seeking outpa-
tient PTSD treatment using self-reports of PTSD symptom
severity, depression, pain, pain-related disability, and mea-
sures of somatization. The authors report over 80% of the
sample suffered chronic pain symptoms, with 49% of the
sample reporting pain in at least three areas. Furthermore,
PTSD symptom severity was positively and strongly asso-
ciated with self-reported pain levels, pain-related disabil-
ity, and somatization whereas veterans’ depressive symp-
toms were only significantly related to overall percentage
of bodily pain. The evidence of high rates of pain in the
sample prompted Beckham et al. (1997) to conclude that
“. . .veterans with PTSD may experience actual physical
symptoms, but how interpretation of physical symptoms,
chronic pain, and PTSD relate will require further empir-
ical investigation” (p. 385).
A number of psychological mechanisms have been pro-
posed to explain the relationships that PTSD has with
somatic complaints such as pain (see Asmundson, Coons,
Taylor, & Katz, 2002; Sharpe & Harvey, 2001). In gen-
eral, theoretical models acknowledge the co-occurrence and
potentially interactive relationships of physical–medical
mechanisms (e.g., musculoskeletal damage incurred during
psychological trauma events) and cognitive mechanisms,
such as fear and avoidance styles of coping, depressive at-
tributions, and catastrophic interpretations of bodily sen-
sations (Otis, Keane, & Kerns, 2003). Two potential psy-
chological mechanisms that may explain the relationship
between PTSD and somatic complaints have gained in-
creasing empirical support: comorbid depression and anx-
iety sensitivity.
D E P R E S S I O N A N D S O M A T I C C O M P L A I N T S
Depression is often accompanied by somatic com-
plaints (Kroenke, 2003; Simon, VonKorff, Piccinelli,
Fullerton, & Ormel, 1999); there is a well-established as-
sociation between depression and reports of chronic pain
(Fishbain, Cutler, Rosomoff, & Rosomoff, 1997; Romano
& Turner, 1985). Several psychological theories have been
proposed to explain the relationship between depression
and somatic complaints. Physical symptoms may be an
early indicator of later problems with mood (Terre, Poston,
Foreyt, & St. Jeor, 2003). More specifically, the onset of
somatic complaints, such as pain symptoms, may interfere
with access to positive reinforcers (i.e., enjoyable activities),
lead to increased feelings of helplessness, and activate neg-
ative cognitive schemas or distortions (e.g., catastrophiz-
ing) that contribute to depression (Banks & Kerns, 1996;
Campbell, Clauw, & Keefe, 2003; Pincus & Williams,
1999). Alternatively, depressed persons may misinterpret
typical physical sensations as being indicative of an under-
lying illness (Miranda, Meyerson, Marx, & Tucker, 2002).
In both civilian and veteran populations, depression is
highly comorbid with PTSD (Kessler, Sonnega, Bromet,
Hughes, & Nelson, 1995; Orsillo et al., 1996). As such,
the association between PTSD and pain and somatic
complaints may be spurious in nature and better ex-
plained by the presence of comorbid depression. There
is evidence that, among civilians, PTSD is related to so-
matic complaints by virtue of comorbid depressive symp-
toms (Miranda et al., 2002; Roy-Byrne, Smith, Goldberg,
Afari, & Buchwald, 2004). Yet, studies of veterans seek-
ing mental health services indicate that PTSD symp-
tom severity is related to the severity ratings of somatic
complaints, whereas depression severity is not (Beckham
et al., 1997, 1998). Even if depression partly accounts for
the association between PTSD and somatic complaints,
PTSD may be related to somatic complaints via other
mechanisms.
A N X I E T Y S E N S I T I V I T Y A N D S O M A T I CC O M P L A I N T S
Sometimes referred to as a “fear of fear,” anxiety sensitivity
describes an individual’s hypersensitivity and catastrophic
reaction to physical signs of autonomic arousal associated
with anxiety (Taylor, 1999). Anxiety sensitivity has been
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

Somatic Complaints in Veterans With PTSD 473
implicated in the etiology of anxiety disorders, such as ago-
raphobia and panic disorder (see Taylor, 1999), and found
to predict patterns of emotional-avoidance and vigilance
to interoceptive bodily sensations (Zvolensky & Forsyth,
2002). Researchers have observed high levels of anxiety sen-
sitivity in persons with PTSD (Taylor, Koch, & McNally,
1992) and there is evidence that anxiety sensitivity predicts
the onset and maintenance of PTSD symptoms (Fedoroff,
Taylor, Asmundson, & Koch, 2000; Keogh, Ayers, &
Francis, 2002). Furthermore, anxiety sensitivity has been
found to positively predict severity ratings of chronic pain
symptoms (Asmundson & Norton, 1995; Asmundson
& Taylor, 1996), perhaps because increased awareness
of autonomic arousal exacerbates the awareness or ex-
perience of somatic symptoms (Norton & Asmundson,
2003).
S T U D Y O B J E C T I V E S
The current study utilized an existing data set to examine
depression and anxiety sensitivity as psychological mech-
anisms that might account for the relationship between
PTSD and somatic complaints. It was hypothesized that
PTSD would emerge as a proxy risk variable, predicting
somatic complaints by virtue of its association with symp-
toms of depression and anxiety sensitivity. A proxy risk
factor model describes relationships in which one variable
(i.e., the proxy risk factor) is found to be highly associ-
ated with an outcome through its relationship to one or
more variables strongly associated with that outcome (see
Kraemer, Stice, Kazdin, Offord, & Kupfer, 2001).
M E T H O D
Participants
Participants were recruited from the population of pa-
tients admitted to the inpatient PTSD Evaluation and
Brief Treatment Unit at the VA Puget Sound Health
Care System in Seattle, Washington. All participants were
given a diagnosis of PTSD based on the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition
(DSM-IV; American Psychiatric Association, 1994) cri-
teria generated from information gathered in standard
psychiatric interviews conducted during admission to the
unit. Fifty-three men consented to participate in a study
described as examining fear and avoidance behaviors associ-
ated with PTSD. Nine participants who were approached
for the study declined to participate. Eight participants
were excluded from the current analyses due to missing
data. Of the remaining 45 participants, 39 were White
(86.7%), two were African American (4.4%), and one
was Latino (2.4%); three participants did not report their
race. The mean age of the sample was 55.4 years (SD =5.3).
A medical chart review was conducted to determine if
the rates of chronic pain in this sample were comparable to
those previously found in veterans seeking PTSD treatment
(i.e., Beckham et al., 1997; White & Faustman, 1989).
Chronic pain was defined as the presence of nonacute,
nontransient pain lasting at least 3 months (see Interna-
tional Association for the Study of Pain, 1986). Participants
were identified as having chronic pain based (a) a previ-
ous diagnosis–treatment of chronic pain syndromes (e.g.,
a diagnosis of degenerative disc disease or a documented
narcotic plan for ongoing treatment of chronic pain); or
(b) pain symptoms assessed during medical examinations
conducted by psychiatric nurses, physician assistants, or
psychiatrists on the inpatient PTSD treatment team. This
review of medical records indicated that 37(70%) of the
veterans enrolled in the study had evidence of chronic
pain.
Procedure
Participants were asked to complete a questionnaire packet
including measures of fear and avoidance symptoms spe-
cific to the domains of physical–somatic functioning and
emotional functioning. Additionally, participants were
asked for permission to access pertinent psychiatric and
medication information that they provided upon admis-
sion to the inpatient PTSD unit, including medical pro-
fessionals’ intake examinations and diagnoses.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

474 Jakupcak et al.
Measures
Anxiety sensitivity. Anxiety sensitivity was assessed using
the Bodily Sensations Questionnaire (BSQ; Chambless,
Caputo, Bright, & Gallagher, 1984). The BSQ is an 18-
item self-report measure of the fear of physical sensations
associated with autonomic arousal and anxiety. Respon-
dents rate the degree of fear they experience in response to
symptoms associated with anxiety (e.g., heart palpitations,
feeling short of breath, and sweating) on a 5-point scale
(1 = not frightened or worried by this sensation; 5 = extremely
frightened by this sensation). The BSQ has demonstrated
strong psychometric properties (Chambless et al., 1984)
and there is strong support for the construct validity of
the scale (Berg, Shapiro, Chambless, & Aherns, 1998;
Chambless et al., 1984).
PTSD symptom severity. The Mississippi Scale for
Combat-Related PTSD (M-PTSD; Keane, Caddell, &
Taylor, 1988) is a commonly used self-report measure that
assesses PTSD symptom severity. The scale is comprised of
35 items assessing PTSD symptoms and experiences asso-
ciated with trauma exposure (e.g., feelings of guilt/shame).
Respondents are asked to endorse the degree to which they
experience each of the symptoms described on a 5-point
Likert-type scale (1 = not at all true, 5 = extremely true).
Item ratings are summed to provide a continuous measure
of PTSD symptom severity. The measure has demonstrated
good psychometric properties and there is strong evidence
for the scale’s ability to assess PTSD symptoms accurately
in veterans (Keane et al., 1988; McFall, Smith, Roszell,
Tarver, & Malas, 1990).
Depression and somatic complaint symptoms. The Pa-
tient History Questionnaire (PHQ; Spitzer, Kroenke, &
Williams, 1999) is a self-report measure based on the
clinician-administered Primary Care Evaluation of Mental
Disorders (PRIME-MD; Spitzer et al., 1994). The PHQ
assesses a variety of psychiatric symptoms, including symp-
toms of depression, anxiety, and eating disorders, as well
as somatic complaints and current or recent alcohol abuse.
Prior research suggests that the PHQ has good psycho-
metric properties and is an effective screening measure for
common psychiatric conditions such as depression (e.g.,
Kumar, Kim, Krefetz, & Steer, 2001; Spitzer et al., 1999).
The 9-item depression subscale of the PHQ was used to
assess depressive symptom severity. The subscale asks indi-
viduals, “Over the last 2 weeks, how often have you been
bothered by any of the following problems?” Participants
then indicate how often they experienced each of the nine
DSM-IV symptoms for a major depressive episode during
the past 2 weeks (not at all, several days, more than half the
days, nearly every day). Scores were summed to provide a
continuous measure of depression symptom severity, with
higher scores indicating more severe depressive symptoms.
The 13-item somatic subscale of the PHQ was used
to assess somatic complaint symptoms. The subscale asks
participants, “During the last 4 weeks, how much have
you been bothered by any of the following problems?” The
subscale assesses somatic complaints, including stomach
and back pain, pain in the legs, arms, or joints, menstrual
cramps,1 pain during sex, headaches, gut-pain (constipa-
tion, nausea, gas, and indigestion), chest pain, dizziness,
fainting spells, racing heart, and shortness of breath. Re-
sponses were assigned numerical values (0 = not bothered
at all, 1 = bothered a little, and 2 = bothered a lot) and the
scores were summed to provide a continuous measure of
somatic complaint symptoms, with higher scores indicat-
ing more severe and greater number of complaints (see
Kroenke, Spitzer, & Williams, 2002).
R E S U L T S
Analytic Plan
Hierarchical multiple regression analyses tested (a) whether
PTSD (proxy risk factor) predicted somatic complaints,
and (b) whether the relationship between PTSD and so-
matic complaints was explained by anxiety sensitivity or
depression symptom severity. Although strategies used to
test a proxy risk factor model are consistent with those
1 This item was not included in the total score somatic complaint score, asthe sample was entirely comprised of men.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.
Somatic Complaints in Veterans With PTSD 475
used to test mediation, unlike tests of mediation, a proxy
risk factor model does not require the establishment of
the order of onset for each factor (Kraemer et al., 2001).
Based on the criteria of proxy risk factor models (Kraemer
et al., 2001), we predicted that (a) PTSD symptom severity
would positively predict the severity of veterans’ somatic
complaints; (b) PTSD symptom severity would positively
predict both anxiety sensitivity and depression symptom
severity; and (c) when separately entered into the same
model with PTSD symptom severity, depression and anx-
iety sensitivity would each predict somatic complaints and
the relationship between PTSD symptom severity and so-
matic complaints would no longer be significant.
Preliminary Analyses
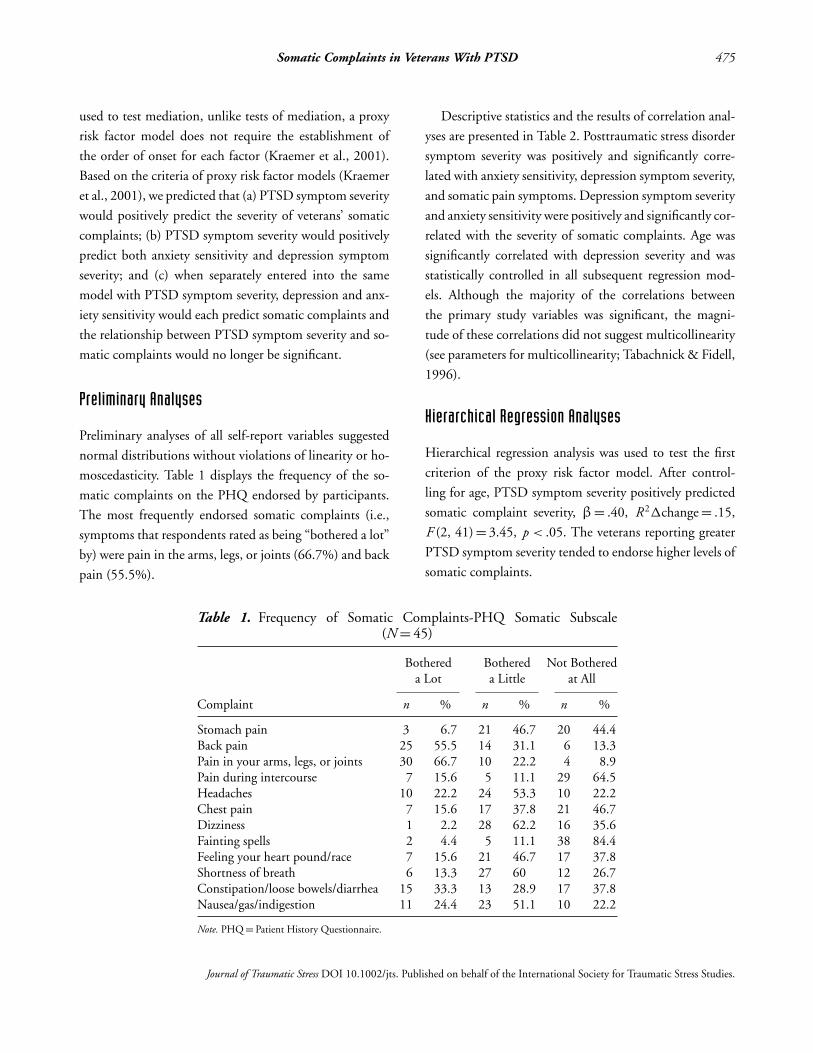
Preliminary analyses of all self-report variables suggested
normal distributions without violations of linearity or ho-
moscedasticity. Table 1 displays the frequency of the so-
matic complaints on the PHQ endorsed by participants.
The most frequently endorsed somatic complaints (i.e.,
symptoms that respondents rated as being “bothered a lot”
by) were pain in the arms, legs, or joints (66.7%) and back
pain (55.5%).
Table 1. Frequency of Somatic Complaints-PHQ Somatic Subscale(N = 45)
Bothered Bothered Not Bothereda Lot a Little at All
Complaint n % n % n %
Stomach pain 3 6.7 21 46.7 20 44.4Back pain 25 55.5 14 31.1 6 13.3Pain in your arms, legs, or joints 30 66.7 10 22.2 4 8.9Pain during intercourse 7 15.6 5 11.1 29 64.5Headaches 10 22.2 24 53.3 10 22.2Chest pain 7 15.6 17 37.8 21 46.7Dizziness 1 2.2 28 62.2 16 35.6Fainting spells 2 4.4 5 11.1 38 84.4Feeling your heart pound/race 7 15.6 21 46.7 17 37.8Shortness of breath 6 13.3 27 60 12 26.7Constipation/loose bowels/diarrhea 15 33.3 13 28.9 17 37.8Nausea/gas/indigestion 11 24.4 23 51.1 10 22.2
Note. PHQ = Patient History Questionnaire.
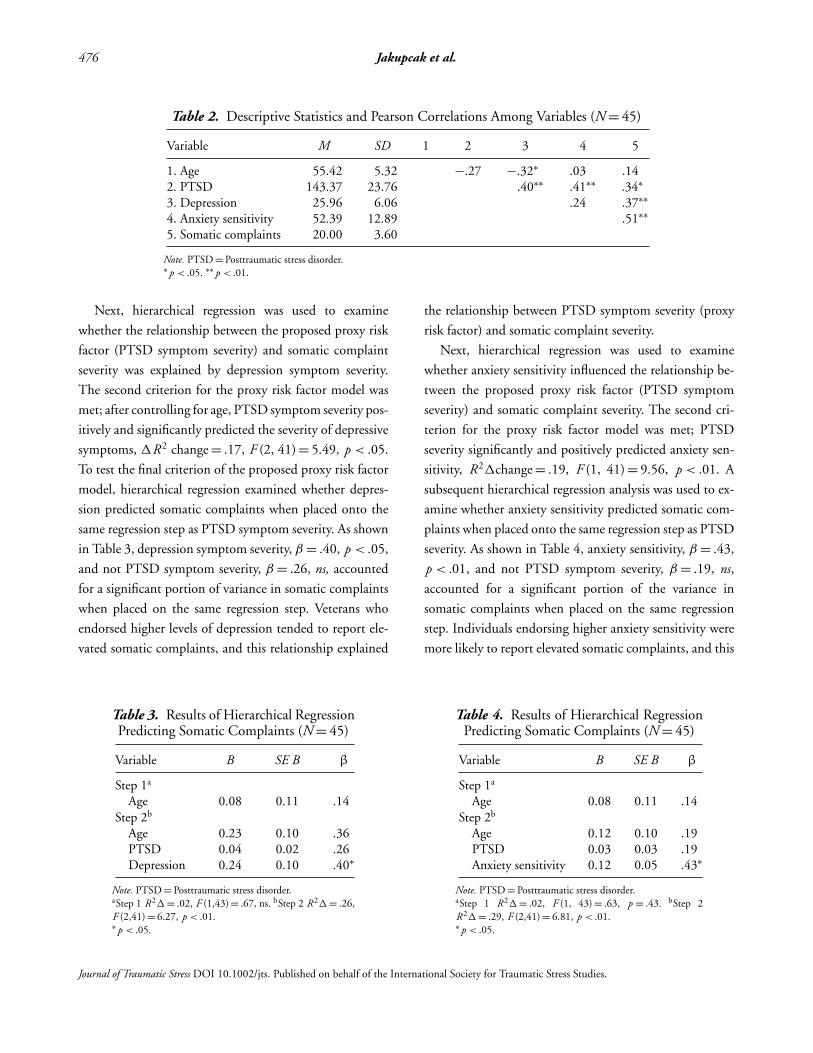
Descriptive statistics and the results of correlation anal-
yses are presented in Table 2. Posttraumatic stress disorder
symptom severity was positively and significantly corre-
lated with anxiety sensitivity, depression symptom severity,
and somatic pain symptoms. Depression symptom severity
and anxiety sensitivity were positively and significantly cor-
related with the severity of somatic complaints. Age was
significantly correlated with depression severity and was
statistically controlled in all subsequent regression mod-
els. Although the majority of the correlations between
the primary study variables was significant, the magni-
tude of these correlations did not suggest multicollinearity
(see parameters for multicollinearity; Tabachnick & Fidell,
1996).
Hierarchical Regression Analyses
Hierarchical regression analysis was used to test the first
criterion of the proxy risk factor model. After control-
ling for age, PTSD symptom severity positively predicted
somatic complaint severity, β= .40, R2�change = .15,
F (2, 41) = 3.45, p < .05. The veterans reporting greater
PTSD symptom severity tended to endorse higher levels of
somatic complaints.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.
476 Jakupcak et al.
Table 2. Descriptive Statistics and Pearson Correlations Among Variables (N = 45)
Variable M SD 1 2 3 4 5
1. Age 55.42 5.32 −.27 −.32∗ .03 .142. PTSD 143.37 23.76 .40∗∗ .41∗∗ .34∗
3. Depression 25.96 6.06 .24 .37∗∗
4. Anxiety sensitivity 52.39 12.89 .51∗∗
5. Somatic complaints 20.00 3.60
Note. PTSD = Posttraumatic stress disorder.∗ p < .05. ∗∗ p < .01.
Next, hierarchical regression was used to examine
whether the relationship between the proposed proxy risk
factor (PTSD symptom severity) and somatic complaint
severity was explained by depression symptom severity.
The second criterion for the proxy risk factor model was
met; after controlling for age, PTSD symptom severity pos-
itively and significantly predicted the severity of depressive
symptoms, �R2 change = .17, F (2, 41) = 5.49, p < .05.
To test the final criterion of the proposed proxy risk factor
model, hierarchical regression examined whether depres-
sion predicted somatic complaints when placed onto the
same regression step as PTSD symptom severity. As shown
in Table 3, depression symptom severity, β = .40, p < .05,
and not PTSD symptom severity, β = .26, ns, accounted
for a significant portion of variance in somatic complaints
when placed on the same regression step. Veterans who
endorsed higher levels of depression tended to report ele-
vated somatic complaints, and this relationship explained
Table 3. Results of Hierarchical RegressionPredicting Somatic Complaints (N = 45)
Variable B SE B β
Step 1a
Age 0.08 0.11 .14Step 2b
Age 0.23 0.10 .36PTSD 0.04 0.02 .26Depression 0.24 0.10 .40∗
Note. PTSD = Posttraumatic stress disorder.aStep 1 R2�= .02, F (1,43) = .67, ns. bStep 2 R2� = .26,F (2,41) = 6.27, p < .01.∗ p < .05.
the relationship between PTSD symptom severity (proxy
risk factor) and somatic complaint severity.
Next, hierarchical regression was used to examine
whether anxiety sensitivity influenced the relationship be-
tween the proposed proxy risk factor (PTSD symptom
severity) and somatic complaint severity. The second cri-
terion for the proxy risk factor model was met; PTSD
severity significantly and positively predicted anxiety sen-
sitivity, R2�change = .19, F (1, 41) = 9.56, p < .01. A
subsequent hierarchical regression analysis was used to ex-
amine whether anxiety sensitivity predicted somatic com-
plaints when placed onto the same regression step as PTSD
severity. As shown in Table 4, anxiety sensitivity, β = .43,
p < .01, and not PTSD symptom severity, β = .19, ns,
accounted for a significant portion of the variance in
somatic complaints when placed on the same regression
step. Individuals endorsing higher anxiety sensitivity were
more likely to report elevated somatic complaints, and this
Table 4. Results of Hierarchical RegressionPredicting Somatic Complaints (N = 45)
Variable B SE B β
Step 1a
Age 0.08 0.11 .14Step 2b
Age 0.12 0.10 .19PTSD 0.03 0.03 .19Anxiety sensitivity 0.12 0.05 .43∗
Note. PTSD = Posttraumatic stress disorder.aStep 1 R2�= .02, F (1, 43) = .63, p = .43. bStep 2R2�= .29, F (2,41) = 6.81, p < .01.∗ p < .05.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

Somatic Complaints in Veterans With PTSD 477
relationship explained the association between PTSD
symptom severity and somatic complaints.
D I S C U S S I O N
The review of veterans’ medical records indicated that
the majority of the veterans in this sample suffered from
chronic pain. These rates of chronic pain were higher than
those previously found among veterans seeking inpatient
PTSD treatment (White & Faustman, 1989) and compa-
rable to rates reported by Beckham et al. (1997). Consis-
tent with previous findings (Shalev et al., 1990; White &
Faustman, 1989), pain symptoms were found to be the
most common type of somatic complaint.
Posttraumatic stress disorder symptom severity was pos-
itively and significantly related to veterans’ somatic com-
plaints. In addition, PTSD symptom severity significantly
and positively predicted both depression symptom sever-
ity and anxiety sensitivity. Yet when depression symptom
severity and anxiety sensitivity were entered into separate
regression analyses, PTSD symptom severity no longer ac-
counted for a significant portion of the variance associated
with somatic complaints. This would suggest that, among
veterans with PTSD, the relationship between PTSD sever-
ity and somatic complaints can be accounted for by co-
morbid depression and anxiety sensitivity. As noted pre-
viously, the relationship between depression and somatic
complaints is well established (e.g., Romano & Turner,
1985), and there is evidence that depression may account
for the relationship between PTSD and somatic complaints
in civilians (Miranda et al., 2002). The current findings in-
dicate this is also the case for veterans with PTSD and that,
in addition to depression, anxiety sensitivity may be an
important factor for understanding the nature of somatic
complaints in persons with PTSD.
Perhaps anxiety sensitivity and the attention to signs
of physiological arousal exacerbate awareness and the
experience of pain symptoms for persons with PTSD
(Asmundson et al., 2002). As previously noted, anxiety
sensitivity is associated with an increased awareness of in-
teroceptive bodily sensations (Zvolensky & Forsyth, 2002),
potentially increasing one’s awareness of somatic symptoms
that might be present. In this sample, medical records in-
dicated that 70% of the veterans suffered from chronic
pain. Repeatedly scanning the body for signs of anxiety
might lead these veterans to have an increased awareness of
their pain symptoms. Another potential explanation lies in
the interpretation of pain signals. Pain sensations may be
perceived to indicate that one’s health is worsening, which
could trigger anxiety and increased vigilance for signs of
potential danger in the body.
This was a preliminary study that utilized an exis-
tent data set. As such, a number of limitations suggest
a need for caution in interpreting the results. The sam-
ple was homogenous (White male veterans, mostly of
the Vietnam era) and drawn from an inpatient psychi-
atric setting, so the findings may not generalize to fe-
male, outpatient, or civilian populations of persons with
PTSD, or to populations more diverse in race or ethnicity.
Although staff members of a PTSD-specialty unit diag-
nosed participants, measurements of PTSD and depression
symptom severity were based on self-report instruments,
rather than clinician-administered structured interviews
(e.g., Clinician-Administered PTSD Scale [Blake et al.,
1990]). Thus, the assessment of these factors may be sub-
ject to self-report biases. Because the sample was comprised
of veterans who met diagnosis for PTSD, the range of
PTSD symptom severity was restricted at the lower end.
Restriction in the range of PTSD symptom severity and
limited statistical power associated with a small sample size
may have obscured a PTSD specific effect. In addition,
because the study is a cross-sectional design and temporal
precedence cannot be established, we cannot infer causality
from these relationships.
Nonetheless, the results of this study suggest that anx-
iety sensitivity and depression may represent psychologi-
cal mechanisms that account for the relationship between
PTSD and somatic complaints. In addition to addressing
depression, therapies that target anxiety sensitivity asso-
ciated with PTSD (see Taylor, 2003) might be particu-
larly useful for veterans with PTSD and comorbid somatic
complaints. Further research is needed to replicate these
findings in larger samples and more diverse populations
of persons with PTSD. Future studies should use designs
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

478 Jakupcak et al.
that include comprehensive assessment measures of PTSD,
depressive disorders, onset of physical pain, and current
functional impairment.
R E F E R E N C E S
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders (4th ed.). Washington, DC: Author.
Asmundson, G. J., Coons, M. J., Taylor, S., & Katz, J. (2002). PTSDand the experience of pain: Research and clinical implications ofshared vulnerability and mutual maintenance models. CanadianJournal of Psychiatry, 47, 930–937.
Asmundson, G. J., & Norton, G. R. (1995). Anxiety sensitivityin patients with physically unexplained chronic back pain: Apreliminary report. Behaviour Research and Therapy, 33, 771–777.
Asmundson, G. J., & Taylor, S. (1996). Role of anxiety sensitivity inpain-related fear and avoidance. Journal of Behavioral Medicine,19, 577–586.
Banks, S. M., & Kerns, R. D. (1996). Explaining high rates of depres-sion in chronic pain: A diathesis stress framework. PsychologicalBulletin, 119, 95–110.
Beckham, J. C., Crawford, A. L., Feldman, M. E., Kirby, A. C.,Hertzberg, J. R., Davidoson, T., et al. (1997). Chronic post-traumatic stress disorder and chronic pain in Vietnam combatveterans. Journal of Psychosomatic Research, 43, 379–389.
Beckham, J. C., Moore, S. D., Feldman, M. E., Hertzberg, J. R.,Kirby, A. C., & Fairbank, J. A. (1998). Health status, soma-tiziation, and symptom severity of posttraumatic stress disorderin combat veterans with posttraumatic stress disorder. AmericanJournal of Psychiatry, 155, 1565–1569.
Berg, C. Z., Shapiro, N., Chambless, D. L., & Ahrens, A. H. (1998).Are emotions frightening? II: An analogue study of fear of emo-tion, interpersonal conflict, and panic onset. Behavior Researchand Therapy, 36, 3–15.
Blake, D., Weathers, F., Nagy, L., Kaloupek, D., Klauminizer, G.,Charney, D., et al. (1990). Clinician-Administered PTSD Scale(CAPS). A clinician’s rating scale for assessing current and lifetimePTSD: The CAPS-1. Behavior Therapist, 13, 187–188.
Campbell, L. C., Clauw, D. J., & Keefe, F. J. (2003). Persistentpain and depression: A biopsychosocial perspective. BiologicalPsychiatry, 54, 399–409.
Chambless, D. L., Caputo, G. C., Bright, P., & Gallagher, R. (1984).Assessment of fear of fear in agoraphobics: The Body SensationsQuestionnaire and the Agoraphobic Cognitions Questionnaire.Journal of Consulting and Clinical Psychology, 52, 1090–1097.
Engel, C. C., Jr. (2004). Somatization and multiple idiopathic phys-ical symptoms: Relationship to traumatic events and posttrau-matic stress disorder. In P. P. Schnurr & B. L. Green (Eds.),Trauma and health: Physical health consequences of exposure toextreme stress (pp. 191–216). Washington DC: American Psy-chological Association.
Fedoroff, I. C., Taylor, S., Asmundson, J. G., & Koch, W. J. (2000).Cognitive factors in traumatic stress reactions: Predicting PTSDsymptoms from anxiety sensitivity and beliefs about harmfulevents. Behavioral and Cognitive Psychotherapy, 28, 5–15.
Fishbain, D. A., Cutler, R., Rosomoff, H. L., & Rosomoff, R. S.(1997). Chronic pain associated depression: Antecedent of con-sequence of chronic pain? A review. Clinical Journal of Pain, 13,116–137.
International Association for the Study of Pain (1986). Classificationof chronic pain. Pain, 24 (suppl. 1), S1–S226.
Keane, T. M., Caddell, J. M., & Taylor, K. L. (1988). Mississippi scalefor combat-related posttraumatic stress disorder: Three studiesin reliability and validity. Journal of Consulting and ClinicalPsychology, 56, 85–90.
Keogh, E., Ayers, S., & Francis, H. (2002). Does anxiety sensitiv-ity predict post-traumatic stress symptoms following childbirth?A preliminary report. Cognitive Behavior Therapy, 31, 145–155.
Kessler, R. C., Sonnega, E., Bromet, M., Hughes, M., & Nelson, C.B. (1995). Posttraumatic stress disorder in the National Comor-bidity Survey. Archives of General Psychiatry, 52, 1048–1060.
Kraemer, H. C., Stice, E., Kazdin, A., Offord, D., & Kupfer, D.(2001). How do risk factors work together? Mediators, mod-erators, and independent, overlapping, and proxy risk factors.American Journal of Psychiatry, 158, 848–856.
Kroenke, K. (2003). Patients presenting with somatic complaints:Epidemiology, psychiatric co-morbidity and management. Inter-national Journal of Methods in Psychiatric Research, 12, 34–43.
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2002). The PHQ-15:Validity of a new measure for evaluating the severity of somaticsymptoms. Psychosomatic Medicine, 64, 258–266.
Kumar, G., Kim, A. H., Krefetz, D., & Steer, R. A. (2001). Screen-ing for major depressive disorders in adolescent psychiatric inpa-tients with the mood modules from the Primary Care Evaluationof Mental Health Disorders and Patient Health Questionnaire.Psychological Reports, 2, 274–278.
McFall, M. E., Smith, D. E., Roszell, D. K., Tarver, D. T., & Malas,K. L. (1990). Convergent validity of measures of PTSD in Viet-nam combat veterans. American Journal of Psychiatry, 147, 645–648.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

Somatic Complaints in Veterans With PTSD 479
McFarlane, A. C., Atchison, M., Rafolowicz, E., & Papay, P. (1994).Physical symptoms in posttraumatic stress disorder. Journal ofPsychosomatic Research, 42, 607–617.
Miranda, R., Jr., Meyerson, L. A., Marx, B. P., & Tucker, P. M.(2002). Civilian-based posttraumatic stress disorder and physicalcomplaints: Evaluation of depression as a mediator. Journal ofTraumatic Stress, 15, 297–301.
Norton, P. J., & Asmundson, G. J. (2003). Amending the fear-avoidance model of chronic pain: What is the role of physiologicalarousal? Behavior Therapy, 34, 17–30.
Orsillo, S. M., Weathers, F. W., Litz, B. T., Steinberg, H. R., Huska,J. A., & Keane, T. M. (1996). Current and lifetime psychiatricdisorders among veterans with war zone-related posttraumaticstress disorder. Journal of Nervous and Mental Disease, 184,307–313.
Otis, J. D., Keane, T. K., & Kerns, R. D. (2003). An examination ofthe relationship between chronic pain and post-traumatic stressdisorder. Journal of Rehabilitation Research and Development,40, 397–406.
Pincus, T., & Williams, A. (1999). Models and measurement ofdepression in chronic pain. Journal of Psychosomatic Research,47, 211–219.
Romano, J. M., & Turner, J. A. (1985). Chronic pain and depression:Does the evidence support a relationship? Psychological Bulletin,97, 18–34.
Roy-Byrne, P., Smith, W. R., Goldberg, J., Afari, N., & Buchwald,D. (2004). Post-traumatic stress disorder among patients withchronic pain and fatigue. Psychological Medicine, 34, 363–368.
Shalev, A., Bleich, A., & Ursano, R. J. (1990). Posttraumatic stressdisorder: Somatic comorbidity and effort tolerance. Psychoso-matics: Journal of Consultation Liaison Psychiatry, 31, 197–203.
Sharp, T. J., & Harvey, A. G. (2001). Chronic pain and posttraumaticstress disorder: Mutual maintenance? Clinical Psychology Review,21, 857–877.
Simon, G. E., VonKorff, M., Piccinelli, M., Fullerton, C., & Ormel,J. (1999). An international study of the relation between somaticsymptoms and depression. New England Journal of Medicine,341, 1329–1335.
Spitzer, R. L., Kroenke, K., & Williams, J. B. (1999). Validation andutility of a self-report version of the PRIME-MD: The PHQ-primary care study. Journal of the American Medical Association,282, 1737–1744.
Spitzer, R. L., Williams, J. B., Kroenke, K., Linzer, M., deGruy, F.V., Hahn, S. R., et al. (1994). Utility of a new procedure fordiagnosing mental disorders in primary care: The PRIME-MD1000 study. The Journal of the American Medical Society, 272,1749–1756.
Tabachnick, B. G., & Fidell, L. S. (1996). Using Multivariate Statis-tics (3rd ed.). New York: Harpercollins.
Taylor, S. (1999). Anxiety sensitivity: Theory, research, and treat-ment of the fear of anxiety. Hillsdale, NJ: Erlbaum.
Taylor, S. (2003). Anxiety sensitivity and its implications for under-standing and treating PTSD. Journal of Cognitive Psychotherapy,17, 179–186.
Taylor, S., Koch, W. J., & McNally, R. J. (1992). How does anxietysensitivity vary across the anxiety disorders? Journal of AnxietyDisorders, 6, 249–259.
Terre, L., Poston, W. S., Foreyt, J., & St. Jeor, S. T. (2003). Dosomatic complaints predict subsequent symptoms of depression?Psychotherapy & Psychosomatics, 72, 261–267.
White, P., & Faustman, W. (1989). Coexisting physical conditionsamong inpatients with post-traumatic stress disorder. MilitaryMedicine, 154, 66–71.
Zvolensky, M. J., & Forsyth, J. P. (2002). Anxiety sensitivitydimensions in the prediction of body vigilance and emo-tional avoidance. Cognitive Therapy and Research, 26, 449–460.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.





























