Embed Size (px)
Citation preview

American Epilepsy Society | Annual Meeting
“Paraneoplastic and autoimmune
encephalitis resulting in refractory
status epilepticus”
Josep Dalmau, MD, PhD
ICREA Research Professor at IDIBAPS/Hospital Clinic,
University of Barcelona
Adjunct Professor of Neurology, University of Pennsylvania.

Disclosure
Dr. Dalmau has received license fee payments from
Euroimmun. He receives royalties from Athena Diagnostics
and Euroimmun for patents related to Ma2 and NMDA
receptor antibody testing

Lancaster and Dalmau, Nat Review Neurol 2012;8:380-390
Intracellular
HuD; Ma2, CRMP5
• Encephalomyelitis
• Limbic encephalitis
Synaptic
intracellular
Amphiphysin;
GAD65
• Limbic
encephalitis,
• Refractory seizures
Cell surface/
synaptic
receptors
NMDAR; AMPAR;
GABA(B); LGI1;
Caspr2; other
• Psychosis
• Limbic encephalitis
• Dyskinesias
• Seizures
• Level of
consciousness,
• Sleep dysfunction

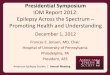
Anti-Ma2 encephalitis: pathological features
Dalmau et al., Brain 2004;127:1831-1844

Syndrome Clinical
significance
Response to
immunotherapy
GluR3
(AMPA
receptor)
Rasmussen’s
encephalitis (?) Low
Infrequent/
moderate
TPO Hashimoto’s
encephalitis Low Frequent
NR2A, NR2B
(NMDAR)
Non-specific,
lupus, stroke,
Rasmussen’s
None Unclear
Other antibodies associated to epilepsy
(usually non-paraneoplastic)

Lancaster et al.
Neurology, 2011;
77:179-89.

Prodrome
Agitation, psychosis,
catatonia, memory
deficit, speech reduction,
abnormal movements
+/- seizures
coma,
hypoventilation,
+/- dysautonomia
Clinical Worsening
Clinical Improvement
Anti-NMDAR encephalitis
Dalmau et al., . Lancet Neurol 2011;10:63-74

Slide Unavailable

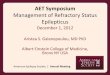
Anti-NMDAR encephalitis in 577 patients:
First symptom
Seizures
Movement disorder
Level of consciousness
Speech disturbances
Behavior
Cognition
Memory loss
Other
Age < 12 years Age 12-17 years Age ≥ 18 years
Titulaer et al., Lancet Neurol, in press

EEG in Anti-NMDAR encephalitis
Florance et al., Ann Neurol 2009;66:11-18

Extreme Delta Brush: a unique EEG pattern of
anti-NMDAR encephalitis
Schmitt S et al. Neurology 2012;79:1094-1100

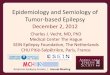
Anti-NMDAR encephalitis in 501 patients:
Improvement (median follow-up 24 months)
Patients 501 450 382 307 252
0%
20%
40%
60%
80%
100%
4 8 12 18 24
6
5
4
3
2
1
0
months
Modified
Rankin Scale
Titulaer et al., Lancet Neurol, in press

Patient’s antibodies decrease the clusters of NMDAR
Dalmau et al.
Lancet Neurol
2008;7:1091

Patients’ antibodies decrease synaptic NMDAR currents
Hughes et al., J Neurosci 2010;30:5866-5875

Patients’ antibodies decrease NMDAR
cluster density in vivo
Hughes et al., J Neurosci 2010;30:5866-5875

Disorders of synaptic/cell surface autoimmunity
Antigen Syndrome and main features
NMDA-R Anti-NMDAR encephalitis
GABA-B Limbic encephalitis with prominent seizures, status
AMPA Limbic encephalitis, psychosis
LGI1 Limbic encephalitis, myoclonus, hyponatremia
Caspr2 Encephalitis and/or neuromyotonia
GlyR Stiff-person syndrome, hyperekplexia, PERM
mGluR5 Ophelia syndrome
DPPX (Kv4.2) Agitation, myoclonus, tremor, seizures, diarrhea

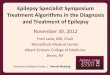
20 mV
5 sec
Control CSF (1%), 24 hours
Patients’ antibodies block GABABR function
100 µM
Baclofen
Patient CSF (1%), 24 hours
100 µM
Baclofen
Lancaster et al., not reported
Slide Unavailable

LGI1
“VGKC-
complex
antibodies”
Encephalitis,
neuromyotonia
Morvan’s syndrome,
painful neuropathy
CASPR2
Limbic encephalitis,
hyponatremia,
myoclonic-like
movements (tonic
seizures, facio-brachial
dystonic seizures)
Multiple disorders Unknown
antigens
Rosenfeld M et al., Neurology: Clin Practice 2012; 1(September):215-222

LGI1
•Secreted synaptic protein
•Associates with VGKCs and AMPA
receptors via the ADAM proteins
•LGI1-null mice have seizures,
early death
•Human mutations associate with
“autosomal dominant lateral
temporal lobe epilepsy”
Post-synaptic
Pre-synaptic
LGI1
ADAM23
ADAM22 AMPA-R
VGKC
LGI1
LGI1

Tonic seizures
in anti-LGI1
encephalitis
Andrade et al., Neurology
2011;76:1355-1357
Irani et al., Ann Neurol 2010, Oct 28.
doi: 10.1002/ana.22307

Clinical, neuroimaging,
serum and CSF evaluation
Exclusion of other
disorders
Tumor surveillance,
chronic mmunosuppression
Response
Rituximab,
cyclophosphamide
No response
Antibodies to intraneuronal
proteins
Onconeuronal antigens
Hu, Ma2, CRMP5, amphiphysin
Oncologic treatment +
T-cell suppression
Antibodies to cell surface or
synaptic proteins
NMDAR,, GABA(B)R, AMPAR, LGI1,
Caspr2, GlyR, unknown antigens
Corticosteroids, IVIg, plasma exchange +
tumor removal if present
Autoimmune Encephalitis: Diagnosis and Treatment
Lancaster et al., Neurology 2011;77:179-189

























![Indistinguishable synaptic pharmacodynamics of the NMDAR ...molpharm.aspetjournals.org/content/molpharm/early/...nitro-7-sulfonyl-benzo[f]quinoxaline, OGD: oxygen glucose deprivation,](https://img.pdfslide.net/doc/110x75/5f0545397e708231d412218a/indistinguishable-synaptic-pharmacodynamics-of-the-nmdar-nitro-7-sulfonyl-benzofquinoxaline.jpg)