Embed Size (px)
Citation preview

13/06/2018
1
Dr Alan Japp
Edinburgh Heart Centre
Advanced Echo 2018
Aortic Regurgitation
Aortic Regurgitation
• Causes and Consequences of AR
• AR Guidelines
• Assessment of AR severity
• Illustrative cases
AR: Causes, classification & consequences
Primary valve disease Aortic root pathology
Rheumatic Dilatation: Marfan’s bicuspid etc
Congenital (e.g. bicuspid) Aortic dissection*
Degenerative / calcific
Endocarditis*
Traumatic (e.g. leaflet rupture)*
Inflammatory e.g. SLE
*Cause of acute aortic regurgitation
Carpentier Classification Type 1: normal cusps; poor coaptation due to root enlargement
Type 2: cusp prolapse Type 3: poor cusp tissue quality or quantity (retraction, erosion)
Valve morphology
Unicuspid (unicommisural) Quadricuspid
Tricuspid Bicuspid
AR: Causes, classification & consequences
Primary valve disease Aortic root pathology
Rheumatic Dilatation: Marfan’s bicuspid etc
Congenital (e.g. bicuspid) Aortic dissection*
Degenerative / calcific
Endocarditis*
Traumatic (e.g. leaflet rupture)*
Inflammatory e.g. SLE
*Cause of acute aortic regurgitation
Carpentier Classification Type 1: normal cusps; poor coaptation due to root enlargement
Type 2: cusp prolapse Type 3: poor cusp tissue quality or quantity (retraction, erosion)

13/06/2018
2
ESC 2017 algorithm for management
of AR
ESC 2017 guidelines: the role of echo
Aorta
Valve
LV
ESC Guidelines 2017 Assessing AR severity
ESC BSE
ESC 2017 guidelines: the role of echo
Aorta
Valve
LV
TOE, MRI, aortogram
ESC Guidelines 2017

13/06/2018
3
Dujardin et al. Circulation. 1999;99:1851-1857
Post AVR outcomes
Outcomes with conservative therapy
Bonow RO et al. Circulation. 1985;72:1244–56.
ESC 2017 guidelines: the role of echo
Aorta
Valve
LV
TOE, MRI, aortogram
MRI
ESC Guidelines 2017 ESC 2017 guidelines: the role of echo
Aorta
Valve
LV
TOE, MRI, aortogram
MRI
CT, MRI
Case 1: A full house (almost)
• 20 y/o male
• Presents with palpitation. No SOBOE
• Short stature, slight build, previous drug use (?IV)
• Displaced apex++, collapsing pulse, , carotid
pulsations, EDM
• TTE
Case 1: A full house (almost)

13/06/2018
4
Case 1: A full house (almost) Case 1: huge coaptation defect
Case 1: LVOT jet width area
Jet width / LVOT diam = 67%
Case 1: Pressure half time
PHT = 206 ms
Case 1: Descending aorta Case 1: Descending aorta
End-diastolic velocity = 100 cm/s

13/06/2018
5
Case 1: Abdominal aorta Case 1: LV remodelling (1)
BSA = 1.6 cm2
Indexed LVESV = 31 mm/m2
Case 1: LV remodelling (2)
LVEF = 47%
Case 1: LV Recovery
Pre AVR Post AVR
Case 1: LV Recovery
Pre AVR Post AVR
Case 2: Extreme Measures
• 38 y/o man; mild exertional SOB
• Tall, some marfanoid features
• Displaced apex, EDM
• TTE

13/06/2018
6
Case 2: Extreme Measures Case 2: Extreme Measures
Case 2: Central coaptation defect Case 2: colour assessment
Case 2: LVOT jet width
Jet width / LVOT diam = 48%
Case 2: Poor CW signal
PHT approx 350 ms

13/06/2018
7
Case 2: Descending aorta Case 2: Descending aorta
End-diastolic velocity = ?
Case 2: Descending aorta
End-diastolic velocity = ?
Case 2: Advanced LV remodelling
End-diastolic velocity = ?
LVEF = 30%
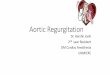
PISA radius 8mmAliasing velocity 45 cm/s
Case 2: TOE - EROA & Regurgitant volume Case 2: EROA & Regurgitant volume

13/06/2018
8
PISA radius 0.8 cmAliasing velocity 45 cm/sAV max 410 cm/sAV VTI 181 cm
EROA = PISA area x aliasing velocity / VmaxEROA = (2 x 3.14 x 0.82 x 45) / 410
EROA = 181 / 410 = 0.45 cm2
Regurgitant vol = EROA x AR VTI
Regurgitant vol = 0.45 x 181 = 81 mL
PISA radius 8mm
Aliasing velocity 45 cm/s
Case 2: EROA & Regurgitant volume Case 2: Outcome
• Successful root and valve replacement (significant leaflet disease at operation)
• Post-op LV still severely dilated and impaired
• Symptomatically well
• Sudden (presumed arrhythmic) death in hospital at day 14 post-op
Case 2: Outcome
Chaliki et al. Circulation . 2002;106:2687-2693
Case 3: A high pressure case
• 23 y/o male IV drug user
• Staph aureus sepsis
• TTE 36 hours ago – no clear evidence of endocarditis
• Haemodynamic deterioration
• Inotropic / pressor support; not ventilated
• Scanned at bedside in ICU by cardio registrar
Case 3: A high pressure case Case 3: A high pressure case

13/06/2018
9
Case 3: A high pressure case Case 3: A high pressure case
Case 3: A high pressure case Case 3: A high pressure case
PHT = 93 ms
Case 4: Severe LV; Severe AR?
• 49 y/o man; palpitation!!
• Ventricular ectopics++
• Moderate alcohol excess; No CVS hx
• No limiting SOB
• Soft EDM; displaced apex; no other physical signs
Case 4: Severe LV; Severe AR?

13/06/2018
10
Case 4: Severe LV; Severe AR? Case 4: Severe LV; Severe AR?
Case 4: Not a short PHT Case 4: No holodiastolic flow reversal
Case 4: Very eccentric! Case 4: Very eccentric!

13/06/2018
11
Case 4: TOE Case 4: TOE
Case 4: Very eccentric!
Vena contracta 0.4 cm
PISA radius 0.6 cm
EROA 0.29cm2 (!!)
Regurgitant vol 47 mL
Case 4: MRI assessment
• LVEF 19%
• Global wall thinning; normal indexed LV mass
• Regurgitant volume 38 mL
• Regurgitant fraction 31%
• No myocardial fibrosis
• No aortic dilatation
Case 4: MRI assessment
• LVEF 19%
• Global wall thinning; normal indexed LV mass
• Regurgitant volume 38 mL
• Regurgitant fraction 31%
• No myocardial fibrosis
• No aortic dilatation
Conclusion: Severe DCM. Moderate aortic regurgitation
Does strain have a role?

13/06/2018
12
Take home messages
• Valve, ventricle, aorta
• Severity challenging; acknowledge uncertainty
• Track the LV carefully (GLS? Biomarkers?)
• Increasing role for multi-modality imaging (esp MRI)
• Acute severe AR a life-threatening emergency