Embed Size (px)
Citation preview
Aortic Stenosis – Decision Paper 1
Aortic Stenosis
Decision Paper

Aortic Stenosis – Decision Paper 2
National Health Committee (NHC)
The National Health Committee (NHC) is an independent statutory body charged with prioritising new and existing health technologies and making recommendations to the Minister of Health.
It was re-formed in 2011 to establish evaluation systems that would provide the New Zealand people and the health sector with greater value for money invested in health.
The NHC executive is the secretariat that supports the committee. The NHC executive’s primary objective is to provide the committee with sufficient information for it to make decisions regarding prioritisation and reprioritisation of interventions and services. They do this through a range of evidence-based products chosen according to the nature of the decision required and timeframe within which decisions need to be made.
The New Zealand Government has asked that all new diagnostic and treatment (non-pharmaceutical) services, and significant expansions of existing services, are to be referred to the NHC.
In August 2011 the NHC was appointed with new terms of reference and a mandate to establish the capacity to assess new and existing health technologies. Its objectives (under Section 4.2 of its terms of reference – www.nhc.health.govt.nz) include contributing to improved value for money and fiscal sustainability in the health and disability sector by:
• providing timely advice and recommendations about relative cost-effectiveness based on the best available evidence;
• providing advice and recommendations which influence the behaviour of decision-makers, including clinicians and other health professionals;
• providing advice and recommendations which are reflected in resource allocation at national, regional and local levels; and
• contributing to tangible reductions in the use of ineffective interventions and improved targeting to those most likely to benefit.
In order to achieve its objectives under Section 4.2 and to achieve ‘value for money’, the NHC has adopted a framework of four assessment domains – clinical safety and effectiveness; economic; societal and ethical; and feasibility of adoption – in order that assessments cover the range of potential considerations and that the recommendations made are reasonable.
It is intended that the research questions asked will fall across these domains to ensure that when the committee comes to apply its decision-making criteria, it has a balanced range of information available to it. When the NHC is setting those questions, they will have the decision-making criteria in mind.
The 11 decision-making criteria will assist in the determination of the NHC work programme and in the appraisal and prioritisation of assessments.

Aortic Stenosis – Decision Paper 3
Executive summary
1. The suite of severe aortic stenosis assessment documents is part of the extensive cardiovascular programme being undertaken by the National Health Committee. These assessment documents are now at the stage where they can be considered by the committee for sharing with the sector as part of a formal consultation process.
2. The Tier 2 aortic stenosis assessment identifies transcatheter aortic valve implantation (TAVI) and sutureless aortic valve replacement (sutureless AVR) for further assessment to ensure their appropriate use, given limited public funding and cardiothoracic surgical service capacity and capability.
3. Conventional surgical aortic valve replacement remains the gold standard treatment for at least 80% of patients requiring aortic valve replacement. Internationally, sutureless aortic valve replacement and TAVI have been indicated in high-risk patients, comprising about 5% of patients, or no more than 30 patients per annum. TAVI has also been indicated for inoperable patients, comprising a much larger potential patient pool. But for most inoperable patients, medical management or palliative care remain the standard of care.
4. The Tier 3 sutureless aortic valve replacement assessment found available evidence suggesting sutureless AVR is a safe and effective alternative to conventional surgical AVR in high-risk patients. Although limited economic data is available, the procedure may be cost-effective using the Sorin valve, which has reduced significantly in price since the NHC began its assessment of the procedure. There may also be future potential, not yet proven, in relation to reduced length of stay and facilitating minimally invasive cardiac surgery, which could result in productivity and efficiency gains for district health boards (DHBs).
5. The Tier 3 transcatheter aortic valve implantation assessment found that neither the clinical nor the economic evidence suggested a significant expansion in TAVI volumes. The proposed target population with severe aortic stenosis for TAVI is recommended to be limited to those patients with high surgical risk (STS score >8) or those patients identified as technically inoperable (eg with calcific aorta or hostile chest) for surgical AVR. Any expansion into the technically inoperable patient population should come from within current service volumes. Though no expansion in volumes beyond population growth is suggested, reprioritisation of TAVI towards high-risk and technically inoperable patients would modestly increase overall aortic valve replacement volumes. The expected national cost impact would be $1 million, increasing to $1.7 million over five years.
6. For patient safety, it is imperative that TAVI is undertaken in centres with sufficient volume and experience. As volumes are not expected to expand significantly in the foreseeable future, TAVI centres should be limited to the current three centres: Auckland, Waikato and Canterbury.
7. The recommendation is for sutureless AVR and TAVI to be ‘absorbed’ within the current cardiac surgical services budget and resources. These interventions are a further example of general expansion of cardiac services on a procedure-by-procedure basis. This type of incremental approach to new technologies is unsustainable and there is a real need to establish a strategic plan for cardiac services in NZ that sets a five to ten-year view of where the services should be.

Aortic Stenosis – Decision Paper 4
8. The vast majority of severe aortic stenosis patients fall into the business as usual surgical AVR pathway. The potential health and independence gains from investing in new technologies for high-risk aortic stenosis are at this time relatively small.
9. The assessments of AS, sutureless AVR, and TAVI have identified some patient and sector value in the use of the sutureless AVR and TAVI, but there may be more value from implementing improvements to the overall model of care for severe AS.
10. While draft recommendations, contained below, indicates opportunities for improvements in the model of care, it is important to emphasise that the current model of care works reasonably well for most patients with severe AS.
11. A draft revised model of care, worked up in collaboration with key stakeholders, proposes a process to identify patients unlikely to survive for reasons other than their primary cardiac condition, which would make aortic valve replacement clinically futile and cost-ineffective. The revised model of care incorporates:
• a standardised national patient selection criteria for severe aortic stenosis interventions.
• an operative risk tool, preferably STS-PROM rather than EuroSCORE I.
• a frailty and cognitive assessment as part of the clinical decision process.
• patient selection to be undertaken by a specified multidisciplinary team, including a geriatrician.
• mandatory entry of clinical and business data into a national registry for interventions for severe aortic stenosis.
• quality of life measurement from a patient perspective, using a tool such as EQ5D, captured at referral and year 1 and 2 follow-ups.
12. Input from key stakeholders is required on the proposed draft recommendations. This is required to fully understand the implications of the proposed advice and the associated system costs of the non-procedure related aspects of the revised model of care. These costs will include the costs of the national registry, change to surgical risk tool, implementation of frailty tool, potential additional two-year follow-ups, quality of life measurement tool, data collection, entry and reporting, and any further costs associated with the multidisciplinary team, eg costs of geriatrician time.

Aortic Stenosis – Decision Paper 5
Contents
Executive summary 3
Purpose 7
Background 8
Severe aortic stenosis and its treatment 9
Risk stratification of patients 12
Transcatheter aortic valve Implantation (TAVI) 14
Sutureless aortic valve replacement (Sutureless AVR) 20
Medical management/palliative care 21
Proposed model of care for severe aortic stenosis 22
Financial implications of aortic stenosis model of care 26
Implementation 26

Aortic Stenosis – Decision Paper 6
Draft Recommendations A revised model of care for severe aortic stenosis is proposed for implementation including:
1. Standardised national patient selection criteria for severe aortic stenosis interventions where:
1.1. Conventional surgical aortic valve replacement is the gold standard of care for severe symptomatic aortic stenosis for patients with moderate or low risk, ie patients with acceptable surgical risk (STS score less than 8), and less than two of the following – significant physical frailty, cognitive impairment, or multiple significant comorbidities and no issues related to technical inoperability.
1.2. Only patients with an STS score greater than 8 or those patients identified as technically inoperable (eg with calcific aorta or hostile chest) for surgical aortic valve replacement can be prioritised to receive TAVI. Patients with two or more of the following – significant physical frailty, cognitive impairment or multiple significant comorbidities will not be prioritised for TAVI.
1.3. Sutureless valve replacement is only for high-risk patients based on clinician preference and providing the sutureless valve is a similar price to conventional bioprosthetic valves.
1.4. Patients should receive medical management/palliative care if their life expectancy is less than two years following aortic valve replacement. In the absence of a significant improvement in patient survival (with an acceptable quality of life); medical management should be the preferred option if patients cannot expect to benefit from an improved quality of life following valve replacement. This is broadly consistent with the current New Zealand policy setting for TAVI, where candidates should have a life expectancy greater than two years.
2. Decision-making should be informed by diagnostic investigations and the following risk management tools to ensure patients receive the most appropriate intervention:
2.1. Operative mortality risk predicted by STS-PROM (the preferred tool based on current evidence) or EuroSCORE II; not EuroSCORE I.
2.2. Frailty score which measures physical frailty and cognitive function. Patients with high frailty indices are unlikely to survive for reasons other than their primary cardiac condition and this can make invasive and expensive interventions like aortic valve replacement clinically futile and cost-ineffective.
2.3. Quality of life measurement from a patient perspective, using a tool where values can be converted to utilities such as EQ5D. For meaningful results data should be captured at referral and year 1 and 2 follow-ups. Quality of life data provides invaluable feedback to clinicians looking to avoid unnecessary and harmful intervention. Anticipated life expectancy of one year or less, or no expectation of improved quality of life, are considered contraindications for aortic valve replacement.
3. Patient selection to be undertaken by a multidisciplinary team, including appropriate specialist interventional cardiologists, cardiac surgeons, geriatricians and other clinicians. Existing joint cardiac surgery/cardiology conferences to be utilised where possible.
4. Mandatory entry of clinical and business data into a national registry for interventions for severe aortic stenosis. Fields to include:
4.1. Patient information based on and linked to the national NHI system.

Aortic Stenosis – Decision Paper 7
4.2. Surgical risk score (STS-PROM).
4.3. Frailty score which measures physical frailty and cognitive function.
4.4. Quality of life measures from the patient’s perspective using EQ5D, or similar, captured at referral and one and two years post-intervention.
4.5. Technical reasons for inoperability ie calcific aorta, hostile chest.
4.6. Multidisciplinary team treatment decision.
4.7. Treatment undertaken, ie surgical aortic valve replacement, balloon valvuloplasty, transcatheter aortic valve replacement, sutureless aortic valve replacement, medical management or palliative care.
4.8. Valve and delivery system device information to enable tracking.
4.9. Valve Academic Research Consortium-2 (VARC-2) endpoints ie device success, stroke, paravalvular leak, major vascular complications etc.
4.10. Business data including resource utilisation to supplement data collected by DHB patient management and clinical systems to support management of the national AVR waiting list, national AS targets, time to access diagnostics and treatment, and real time budget management.
5. TAVI will be provided through three cardiac centres: Auckland (for the northern region), Waikato (for the remainder of the North Island) and Canterbury (for the South Island).
6. The number of TAVI procedures will equate to a level of 10.7 per 100,000 population 65 years or older across New Zealand, a total of at least 70 procedures.
7. TAVI are currently provided at varying rates across New Zealand. For those DHBs with greater than 10.7 per 100,000, close monitoring is required to ensure the referrals meet the patient criteria and patients are prioritised appropriately for TAVI.
8. The intervention rate is subject to future revision consequent to significant new evidence indicating a material change in the relative value of TAVI within the model of care.
9. The multidisciplinary team for each cardiac centre is expected to manage the schedule and workload to ensure that the appropriate number of surgical aortic valve replacements, TAVI and sutureless valve replacements are delivered for each DHB. The volume of patients receiving these interventions each year is expected to align with the national intervention rate targets and elective surgical targets. Patients will need to be prioritised to meet this requirement.
Purpose
13. This paper provides the background, and context of the draft assessments undertaken for aortic stenosis. These include a Tier 2 aortic stenosis (AS) assessment, a Tier 3 transcatheter aortic valve implantation (TAVI) assessment and a Tier 3 sutureless aortic valve replacement (sutureless AVR) assessment.
14. This paper positions these assessments within the overall ongoing cardiovascular work stream undertaken by the National Health Committee (NHC) since 2011, and outlines the next steps in the process to finalise these assessments, including consultation with the sector.

Aortic Stenosis – Decision Paper 8
Background 15. At the request of the health sector, the NHC has undertaken multiple cardiovascular assessments
since its reconfiguration in 2011. These assessments have tended to focus on very high cost leading edge interventions for elderly patients with established and advanced disease, often with multiple comorbidities. Assessments have included:
1. The cardiac cluster consultation, published March 2014, ISBN: 978-0-478-42791-2; Recommendations approved by the Minister of Health 30/05/2014. The cluster was a synthesis of recommendations from the assessments of renal denervation, percutaneous left atrial appendage occlusion, percutaneous interventions for the treatment of mitral regurgitation, and cardiac catheter ablation for the treatment of atrial fibrillation.
2. Percutaneous left atrial appendage occlusion for stroke prevention in patients with atrial fibrillation. An assessment was published in July 2013 and updated May 2015, with updated recommendations approved by the Minister of Health 10/09/2015, ISBN: 978-0-478-44892-4.
3. Sutureless aortic valve replacement for the treatment of aortic stenosis (Technology Note published May 2012, ISBN: 978-0-478-44894-8).
4. Transcatheter aortic valve implantation (TAVI) for the treatment of aortic stenosis (Briefing Report published September 2012, ISBN: 978-0-478-44898-6).
5. Catheter ablation for the treatment of atrial fibrillation (Technology Note published November 2012 and updated July 2013, ISBN: 978-0-478-44897-9).
6. Percutaneous interventions for the treatment of mitral regurgitation (Technology Note published July 2013, ISBN: 978-0-947491-00-0).
7. Renal artery denervation for the treatment of refractory hypertension (Technology Note published July 2013, ISBN: 978-0-947491-02-4).
8. A strategic overview of cardiovascular disease in New Zealand (Tier 1 assessment published December 2013, ISBN: 978-0-947491-03-1).
9. An overview of ischaemic heart disease (Tier 2 assessment published March 2014, ISBN: 978-0-9922623-1-0).
10. Five ischaemic heart disease Tier 3 assessments, in the process of development, were derived from the IHD overview. Screening for abdominal aortic aneurysm (AAA); reconfigured Tier 2 assessment of the AAA model of care (in progress).
16. Cardiovascular assessments have been undertaken using the NHC's previously documented tiered business case for change methodology.1 The assessment work has developed a detailed understanding of the clinical safety and effectiveness of the respective technologies, including the patient sub-groups (if any) most likely to benefit, and the potential health, economic and societal/ethical impact of the technology. The assessments have sought to understand the feasibility of adopting the new interventions, particularly the impact of introducing additional interventions into a fixed capital and operational service delivery model.
1 http://nhc.health.govt.nz/our-work/models-care-and-tiered-business-case-approach
Aortic Stenosis – Decision Paper 9
17. The NHC has also funded cardiovascular research through a partnership fund with the Health Research Council, the Health Innovation Partnership, including the evaluation of:
1. a frailty tool for patients with ischaemic heart disease;
2. the cost-effectiveness of fractional flow reserve in myocardial infarction; and
3. a process for improving care processes for patients with possible acute coronary syndrome.
18. The NHC has maintained an ongoing interest in TAVI and sutureless AVR as the evidence for the technologies has evolved. Both technologies are used for the treatment of severe aortic stenosis. Our current work presents up-to-date (Tier 3) assessments of the technologies alongside a Tier 2 overview document of aortic stenosis. Although the technologies affect a relatively small group of patients, our discussions with the health sector have indicated the opportunity for material change to the overall model of care for severe aortic stenosis.
Severe aortic stenosis and its treatment 19. Aortic stenosis (AS) is a condition where the main outflow valve of the heart becomes narrowed.
AS is a disease largely of the elderly, and is expected to increase in prevalence due to population ageing. Technically, severe symptomatic AS has been defined as a peak aortic valve velocity of >4 m per second, corresponding to a mean aortic valve gradient >40 mm Hg, and an aortic valve area of < 0.8 cm2. There is also a small group of patients that may benefit from aortic valve replacement who have asymptomatic AS, but have left ventricular dysfunction, with a left ventricular ejection fraction of less than 50%.
20. Without aortic valve replacement, the prognosis for severe symptomatic AS is poor. Patients face a poor prognosis once the disease becomes clinically evident, either with the onset of symptoms or with deterioration in left ventricular function. The life expectancy of patients with clinically evident AS without intervention is two to three years, with sudden death occurring in up to a third of these patients. AS is responsible for the deaths of about 300 New Zealanders a year.
21. The majority (85%) of patients with severe AS in 2012/13 were suffering from at least one of nine comorbid conditions, and over a quarter (27%) had at least three of these conditions (Figure 1). These patients are a lot more likely to have ischaemic heart disease (IHD) and heart failure than a similarly aged group of people. People with IHD have insufficient blood and oxygen flow to the heart muscle. This means not only are these patients suffering from severe AS, but for two-thirds their heart function is additionally compromised due to IHD, warranting best practice treatment. For these patients major interventions may be less appropriate.

Aortic Stenosis – Decision Paper 10
Figure 1: Percentage of people with selected long-term conditions, patients with severe aortic stenosis and a comparator group – 2012/13
Source: 2015 NHC Executive analysis of 2012/13 NZ Health Tracker data
22. There are few preventative measures for AS and no proven medical therapy to prevent its progression. Medical therapy is instead focused on symptom relief. Patients with asymptomatic AS mostly do not require treatment. For patients with severe symptomatic aortic stenosis, or severe AS with significant left ventricular dysfunction, surgical AVR is the standard of care. There are two types of prosthetic valve: mechanical valves that may last up to 25 years but require the recipient to take anticoagulants to prevent stroke; and bioprosthetic (‘tissue’) valves that last ten to 15 years but do not require anticoagulation. AVR can restore a patient’s quality of life and life expectancy to close to that seen in the absence of AS. Standard surgical AVR involves open heart surgery, requiring cardiopulmonary bypass to replace the diseased aortic valve with a prosthetic valve. Transcatheter aortic valve implantation and sutureless aortic valve replacements (discussed below) are alternative to conventional surgical AVR.
23. Not all patients with aortic valve disease are candidates for surgical AVR; operations are complex and durability is limited. Other treatment options for AS, including surgical valve repair and balloon aortic valvuloplasty, have a very limited role in adults with aortic stenosis. Balloon aortic valvuloplasty may occasionally be used as a bridge to surgical AVR, to test if AVR is likely to be beneficial, or for palliative care.
24. A large proportion of patients with AS are elderly and while some elderly patients have good outcomes, others have complications and poor outcomes irrespective of the treatment received, due to frailty, cognitive impairment or poor general health. The majority of patients that do receive surgical valve replacement are over the age of 70.
0
10
20
30
40
50
60
70
80
Ischaemicheart disease
Diabetes Chronicobstructivepulmonary
disease
Gout Stroke Heart failure Mood oranxietydisorder
Dementia Any cancer
Percent
Condition
Severe AS patients
People without Severe AS whoare 65+ years

Aortic Stenosis – Decision Paper 11
Rates of aortic valve replacement were low 10-15 years ago, but now appear comparable with other developed countries 25. Ten to 15 years ago, intervention rates for cardiac surgery including aortic valve replacement
were low in New Zealand compared with other developed countries. Consequently, a service development process for cardiac surgery services in New Zealand was requested by the Minister of Health and initiated in May 2008 by the Ministry of Health with the New Zealand Branch of the Cardiac Society of Australia and New Zealand. A Cardiac Surgery Service Development Working Group was established to lead the development process. In 2008, the working group released a report that recommended increasing cardiac surgery intervention rates, including for aortic valve replacement, by a third between 2007/08 and 2012/13. In 2009, the National Cardiac Surgery Network was established to lead the implementation of the working group’s recommendations. National cardiac surgical targets were introduced in 2009, and in conjunction with increased funding for elective surgery from 2006/07, have led to a substantial growth in the number of AVR operations undertaken.
26. The number of publicly-funded aortic valve replacements for aortic stenosis roughly doubled between 2006/07 and 2013/14 from about 300 to about 600 aortic valve replacements per annum (Figure 2). While volumes of aortic valve replacement have increased, mortality from AS has declined significantly, from about four deaths per 100,000 New Zealanders in 2000 to about three deaths per 100,000 New Zealanders in 2011.
Figure 2: Publicly funded AVR for any diagnosis of aortic stenosis in New Zealand from 2002/03 to 2013/14
Source: NHC analysis of NMDS
27. It is not possible to precisely define the optimal rate of intervention for aortic valve replacement. However, New Zealand’s rate of aortic valve replacement appears to be in line with other developed countries. A 2013 meta analysis of European and US data found about 59% of elderly patients with severe symptomatic AS were receiving valve replacement, whereas the remaining 41% were considered inoperable. In New Zealand, a Waikato hospital study (2005-2009) found about half of patients with symptomatic severe AS in its region did not receive aortic valve replacement. With the approximate doubling of aortic valve replacements in New Zealand between 2006/07 and 2013/14, our expectation is that a significantly greater proportion of patients
0
100
200
300
400
500
600
700
Sutureless valve
TAVI
Other Valves
Mechanical valve
Bioprosthetic valve

Aortic Stenosis – Decision Paper 12
with severe AS now receive valve replacement. Indeed, using national records, it appears a similar proportion of elderly patients with severe AS receive AVR in New Zealand compared with the aforementioned meta analysis.
Risk stratification of patients
28. Patients with severe AS may be broadly categorised into operable or inoperable patients. Inoperable patients are patients who are considered too high-risk for surgery, who without aortic valve replacement would receive limited intervention for symptomatic relief (palliative care and medical management). High-risk patients are eligible for surgery but carry a high risk of mortality.
29. Operable patients may be further stratified by their preoperative risk of mortality from surgical (or transcatheter) aortic valve replacement. There are standard preoperative algorithms for stratifying patients into low, moderate or high risk of operative mortality. The best of these algorithms in cardiac surgery, the Society of Thoracic Surgeons Predicted Risk of Mortality Score (STS-PROM), stratifies patients risk using about 30 variables (including among other factors presence of significant comorbidities, age, ethnicity, and prior cardiac surgery). Low risk is defined as an operative risk of death of less than 4% (STS-PROM <4%). Moderate or intermediate risk and high risk are defined as STS 4%≤ 8%, and STS>8%, respectively. The algorithm has shown a high degree of accuracy in international and New Zealand specific studies. Analysis of the STS database, comprising several hundred thousands of patients, has shown about 5% of AVR patients may be classified as high-risk, 15% as moderate-risk, and 80% as low-risk (see National Health Committee Transcatheter Aortic Valve Implantation Tier 3 report).
30. Further detail is provided on TAVI, sutureless AVR, medical management and palliative care below. Figure 3 presents a schematic estimating the number of patients with aortic stenosis for each treatment pathway. The number of patients with a primary hospital diagnosis of AS in 2012/13, 860, is used as a starting point and then the evidence gathered through the development of the Tier 2 and Tier 3 assessment process is used to calculate the number of patients at each decision-making or risk stratification point. A sensitivity analysis for the schematic is provided in the Tier 2 AS assessment. Note:
• The high-risk patient pool is very small, with less than 30 patients per annum. TAVI, sutureless AVR and conventional surgical AVR are alternative options for high-risk patients.
• Conventional surgical AVR remains the gold standard for moderate-risk patients, though emerging evidence is accruing for TAVI and sutureless AVR in this relatively small population.
• Conventional AVR is the gold standard treatment for low-risk patients, comprising about 80% of patients eligible for valve replacement.
• About a third to two-fifths of patients with severe symptomatic AS may be ineligible for surgical AVR. Most of these patients are ineligible due to significant comorbidities, meaning invasive intervention is likely to be futile.
• In less than a third of inoperable patients TAVI may be feasible, and of these patients most will have significant comorbidities, meaning intervention may be futile. A small group of patients, less than 30 patients per annum, who are inoperable for technical reasons may benefit from TAVI with a reasonable prognosis. These patients have anatomical features that make them poor candidates for surgery but have fewer comorbidities. The evidence for this patient population is limited to a non-pre-specified secondary analysis of a randomised controlled trial and a Canadian TAVI registry.

Aortic Stenosis – Decision Paper 13
• Balloon valvuloplasty is not specifically identified in Figure 3. The procedure is very infrequently used in New Zealand. It may be used for palliation, as a bridge to TAVI or surgical AVR, or as a preoperative test for TAVI.
Figure 3: Estimation of operable and inoperable population and their possible treatment – 2012/13
Source: NHC analysis, adapted from Osnabrugge et al 2013 (19) and Makkar 2014. (53) 95% confidence intervals are in
brackets. Confidence intervals are approximated for the technically inoperable group.

Aortic Stenosis – Decision Paper 14
Transcatheter aortic valve Implantation (TAVI)
31. TAVI is a novel technology that is changing treatment choices for aortic stenosis internationally. It allows for the replacement of the aortic valve, without the need for a median sternotomy (incision that separates the sternum to open the chest cavity) or cardiopulmonary bypass (a machine that takes over the role of the heart and lungs) that accompanies conventional surgical valve replacement. The introduction of TAVI has caused much controversy amongst policy makers and medical practitioners, due to the high cost of the valve and the difficulty in defining its precise role within current models of care for aortic stenosis. The large volume of published research is such that it has been difficult for governing agencies to position the technology in the sector without recommendations becoming obsolete.
32. In 2010/11, at the request of the National Health Board, Auckland DHB’s Clinical Practice Committee (Auckland CPC) provided an independent evaluation of TAVI. At that time, the National Service and Technology Review Advisory Committee (NSTR) had been discontinued and a reconfigured NHC not yet established. Based on the evidence available at the time, Auckland CPC recommended interim approval for high-risk surgical candidates, although it felt cost utility was heavily dependent on complication rates. Auckland CPC did not recommend TAVI for non-surgical candidates because of unfavourable cost utility, although it considered there was a high level of evidence of both safety and efficacy for inoperable patients. The Auckland CPC also indicated that it would be necessary to further review TAVI in 12 to 18 months' time, as more evidence became available.
33. TAVI was added to the NHC's reactive work programme in August 2012, following discussions between the NHC, the manager of electives within the National Health Board and the chairs of the New Zealand Cardiac Network (NZCN) and the National Cardiac Surgery Clinical Network. The NHC published a briefing report on TAVI in September 2012. A literature review was then undertaken and a draft review presented to NHC in May 2013, alongside a proposed engagement process with key stakeholders. This report highlighted the need for a stakeholder workshop to address issues around TAVI's cost-effectiveness and financial sustainability.
34. Stakeholder workshops were undertaken in 2014 (discussed below) concurrent to and informing the NHCs aortic stenosis assessment work.
Current Government policy for funding TAVI
35. Ministerial approval for public funding for TAVI was provided in April 2011, with approval granted for high-risk surgical candidates, subject to nationally consistent criteria and patient prioritisation, including regional multidisciplinary patient review committees. Approval was not granted for inoperable patients, moderate-risk patients or low-risk patients and has not subsequently been granted. High-risk surgical cases were to be identified by having one or more of the following high-risk features:
• Advanced age
• Previous coronary artery bypass graft (CABG)
• Heavily calcified aorta
• High risk Logistic EuroSCORE or STS score
• Previous chest irradiation
• Previous coronary artery bypass graft (CABG)
• Sum of comorbidities (such as renal, pulmonary, hepatic and cerebrovascular), severe pulmonary hypertension, previous chest radiation.
Aortic Stenosis – Decision Paper 15
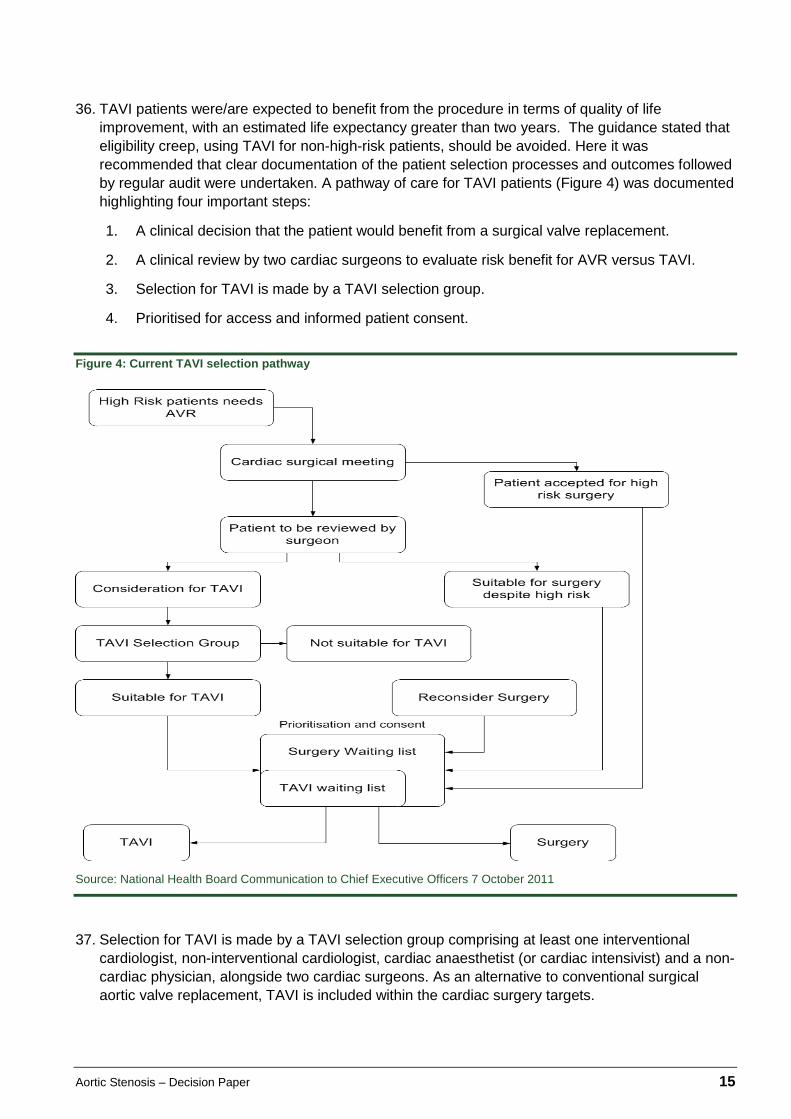
36. TAVI patients were/are expected to benefit from the procedure in terms of quality of life improvement, with an estimated life expectancy greater than two years. The guidance stated that eligibility creep, using TAVI for non-high-risk patients, should be avoided. Here it was recommended that clear documentation of the patient selection processes and outcomes followed by regular audit were undertaken. A pathway of care for TAVI patients (Figure 4) was documented highlighting four important steps:
1. A clinical decision that the patient would benefit from a surgical valve replacement.
2. A clinical review by two cardiac surgeons to evaluate risk benefit for AVR versus TAVI.
3. Selection for TAVI is made by a TAVI selection group.
4. Prioritised for access and informed patient consent.
Figure 4: Current TAVI selection pathway
Source: National Health Board Communication to Chief Executive Officers 7 October 2011
37. Selection for TAVI is made by a TAVI selection group comprising at least one interventional cardiologist, non-interventional cardiologist, cardiac anaesthetist (or cardiac intensivist) and a non-cardiac physician, alongside two cardiac surgeons. As an alternative to conventional surgical aortic valve replacement, TAVI is included within the cardiac surgery targets.

Aortic Stenosis – Decision Paper 16
NHC assessment of TAVI
38. The Tier 2 assessment of AS recognises that TAVI needs to be considered as one intervention in the overall model of care for AS (refer next section). TAVI has a role for high-risk patients provided this population can be clearly and transparently defined and the application of TAVI carefully monitored. There is also potential benefit for technically inoperable patients, who are not currently eligible for public funding.
39. The Tier 3 assessment of TAVI synthesises current evidence relating to the NHC's four assessment domains: clinical safety and effectiveness, economic, societal and ethical, and feasibility of adoption.
40. Internationally, there are many different TAVI devices available and in development. The two most commonly used valves are the Medtronic CoreValve and Edwards Lifesciences Sapien valve. TAVI can be delivered via percutaneous access (transfemoral delivery), or via minimally invasive surgical access (transapical, transaortic/direct aortic or subclavian delivery).(2) Different access routes may be appropriate for different patients, but the two main access routes are the transfemoral (TF) retrograde (against normal blood flow) approach and the transapical (TA) antegrade (in the direction of normal blood flow) approach. The transfemoral approach is the dominant approach used in New Zealand.
41. Internationally, TAVI is supported by health technology assessment agencies and professional bodies for inoperable patients or patients at high risk of mortality from surgical AVR – where surgical AVR remains the gold standard treatment for low and moderate-risk patients. That includes current professional guidance from the American College of Cardiology/American Heart Association (2014), and the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) (2012). In practice, however, it appears that TAVI is already being performed in moderate and low-risk populations in some countries, particularly Germany.
Clinical safety and effectiveness
42. Compared with surgical AVR in high-risk patients, TAVI appears to have similar survival and lower rates of major bleeding events; but is associated with higher rates of aortic regurgitation and major vascular complications. TAVI is also associated with higher rates of pacemaker implantation with the CoreValve but not the Edwards Sapien Valve. Permanent pacemaker insertion is three to four times greater using the CoreValve than the Edwards valve. Renal complications appear to be similar between TAVI and surgical AVR, but elevated using the transapical approach.
43. For inoperable patients, compared with medical management, TAVI is associated with superior survival and reduced hospital readmissions, but higher rates of aortic regurgitation, vascular complications, stroke, and major bleeding events. All-cause mortality for surgically inoperable TAVI patients is still very high in randomised evidence, where it was 43% at two years in the PARTNER randomised controlled trial.
Economic
44. Aortic valve replacement is a high-cost procedure, whether undertaken with conventional surgical AVR or TAVI. The lifetime cost of TAVI ranges from $84,000 to $98,000, for high-risk and technically inoperable patients respectively. The lifetime cost of surgery ranges from $90,000 to $101,000, while medical management is relatively inexpensive, costing about $15,000 per patient over their remaining lifetime.
45. TAVI appear to be highly cost-effective but only in a very small group of patients, namely those patients who are at high risk from surgery. The high-risk AVR patient population in New Zealand (STS>8%) is relatively small, probably less than 30 patients per annum based on current AVR

Aortic Stenosis – Decision Paper 17
volumes. For these patients, TAVI appears to be cost-saving compared with surgery, largely due to the reduced length of stay associated with percutaneous intervention.
46. Our cost-saving finding in high-risk patients is consistent with a recent UK analysis sponsored by the British Heart Foundation which found TAVI had an incremental saving of $3,000 (£1,300) per patient compared with surgical AVR in high-risk patients. A 2013 economic assessment by the Ontario Health Technology Assessment Committee (OHTAC) also found TAVI had an incremental cost saving of $5,000 (C$4,600) per procedure compared with surgery in high-risk patients.
47. For the inoperable patient population, TAVI does not appear to be cost-effective, where the cost per quality adjusted life years is about $74,000. In the subgroup of ‘technically inoperable’ patients, patients who have fewer comorbidities and tend to be younger, the cost per QALY is $40,000, due to vastly better life expectancy. The evidence for this patient population is, however, limited to a secondary analysis of a single randomised controlled trial and registry. Sensitivity analysis shows that cost-effectiveness is most sensitive to the relative efficacy of TAVI compared with surgical AVR and medical management.
Budgetary impact
48. The projected potential budgetary impact of TAVI depends on the population for whom TAVI is funded. On the basis of population growth of people over 65 years of age, TAVI volumes are expected to expand from 66 procedures in 2012/13 to about 84 procedures in 2019/20. For this base case scenario we project a cost profile of about $4.4 million (Confidence interval: $3.5m, $5.3m) in 2015/16, increasing to $6.7 million ($5.3m, $8.0m) in 2019/20, accounting for both the index admission cost and attributable follow-up costs.
49. If TAVI is expanded to inoperable patients, including patients with significant comorbidities, intervention rates could grow to 210 procedures in 2019/20. For this scenario the additional cost (beyond the base case) would be $6.2 million ($5.0m, $7.5m) in 2015/16 increasing to $7.5 million ($6.2m, $9.3m) in 2019/20. That is, the total cost of TAVI would be approximately $14.2 million in 2019/20 if expanded to inoperable patients.
50. If TAVI is expanded to ‘technically inoperable’ patients only, the intervention rate could grow to 113 procedures by 2019/20. Under this scenario, the additional cost (compared with our base case) would be about $1.5 million ($1.2m, $1.8m) increasing to $2.0 million ($1.6m,$2.4m) over the same time period.
51. These scenarios assume an expansion of TAVI volumes. There is, however, little doubt that current volumes are well in excess of what would be expected if only high-risk patients were receiving TAVI in New Zealand. Sixty-six TAVI procedures were undertaken in 2012/13, whereas, on the basis of current AVR volumes, high-risk volumes should account for no more than 20 to 30 patients annually in New Zealand. This finding is corroborated by a recent retrospective study of all TAVI undertaken in New Zealand between 2008 and 2014 that found TAVI had been performed in moderate and high-risk patients. Two substitution scenarios are thus suggested: either TAVI should be limited to high-risk patients only, with moderate-risk patients converting to surgical AVR; or TAVI should be limited to high-risk patients with moderate-risk patients converted to AVR, and remaining TAVI volumes taken up by technically inoperable patients.
52. Under the first scenario, TAVI volumes would be reduced to 20 to 30 patients per annum. With a proficiency requirement of at least 20 TAVI operations per annum, the scenario implicitly assumes a reduction of three TAVI centres to one. As surgical AVR does not appear to be significantly less costly compared with TAVI in moderate-risk patients, we do not project any savings through this scenario. The second substitution scenario assumes maintenance of current TAVI volumes (and allowance for population growth) with any shift to technically inoperable cases consequent to moderate-risk TAVI volumes being converted to surgical AVR. Under this scenario, we project an additional cost of $1 million ($0.8m, $1.2m) increasing to $1.7 million ($1.4m, $2.1m) over five years. This is less than the prior scenario, where technically inoperable volumes were in addition

Aortic Stenosis – Decision Paper 18
to base volumes, but not significantly less due to the implied conversion of moderate risk TAVI patients to surgical AVR.
53. This represents our favoured scenario as it maintains capability across centres whilst avoiding further indication creep into lower-risk population groups. Base case volumes are still one-third in excess of forecast demand from high-risk and technically inoperable patients. Pragmatically, we are not suggesting a reduction in base case volumes, as the apparent excess volume provides some allowance for uncertainty in the estimation of demand. As volumes are not expected to expand significantly in the foreseeable future, TAVI centres should be limited to the current three: Auckland, Waikato and Canterbury.
54. Under our preferred scenario, national TAVI volumes correspond to a rate of 10.7 patients per 100,000 population aged 65 years or older. This assumes a base population of 615,000 people aged 65 years or older in 2012/13, with a national publicly funded intervention rate of 66 TAVI in the same year. The budgetary impact from the preceding scenarios is presented in Table 1.

Aortic Stenosis – Decision Paper 19
Table 1 Future cost of TAVI under various expansion and substitution scenarios
Scenario 2015/16 2016/17 2017/18 2018/19 2019/20 Base case Volume 71 74 77 80 84 Total Cost $4.4m
($3.5m,$5.3m) $5.0m ($4.0m,$6.0m)
$5.6m ($4.5m,$6.7m)
$6.1m ($4.9m, $7.4m)
$6.7m ($5.3m,$8.0m)
Expansion Inoperable 108 (86,131) 113 (90,136) 117, (93,142) 122 (97,147) 127 (101,153) Additional
cost $6.2m ($5.0m, $7.5m)
$6.5m ($5.2m,$7.8m)
$6.9m ($5.5m,$8.3m)
$7.2m ($5.8m,$8.8m)
$7.5m ($6.2m,$9.3m)
Technically inoperable
25 (12,37) 26 (13,39) 27 (13,40) 28 (14,42) 29 (15,44)
Additional cost
$1.5m ($1.2m,$1.8m)
$1.6m ($1.3m,$1.9m)
$1.7m ($1.4m,$2.1m) $1.9m ($1.5m,$2.2m)
$2.0m ($1.6m,$2.4m)
Substitution High-risk only
Volume 23 (22,24) 24 (23,25) 25 (23,26) 26 (24,27) 27 (25,28)
Additional cost
$0.0m $0.0m $0.0m $0.0m $0.0m
High-risk and technically inoperable
Volume 71 74 77 80 84
Additional cost
$1.0m ($0.8m,$1.2m)
$1.2m ($1.0m,$1.5m)
$1.4m ($1.1m,$1.7m)
$1.6m ($1.3m,$1.9m)
$1.7m ($1.4m, $2.1m)
Note: Additional cost is additional to the base case, more detail on the estimated budgetary impact is contained in the Tier 3 TAVI assessment.
Aortic Stenosis – Decision Paper 20
Societal and ethical
55. The Midland region appears to have a higher TAVI intervention rate than other regions (by DHB of domicile), most likely owing to the high volume of TAVI undertaken in Waikato DHB. Patients with severe aortic stenosis tend to be elderly and can have significant morbidities. Mid-term outcomes, even with a successful procedure, can be very poor for these patients. Hence, appropriate patient selection is imperative to avoid futile outcomes. In technically inoperable patients, TAVI is a substitution for medical management rather than surgical AVR and thus raises issues of equity of access that would need to be worked through with the sector.
56. Feasibility of adoption issues are covered in the model of care section below.
Sutureless aortic valve replacement (Sutureless AVR) 57. Sutureless AVR is a relatively new procedure which employs a bioprosthetic (‘tissue’) valve
requiring no (or very few) sutures to stay in place. Sutureless valves stay in place using either a self-expanding or balloon-expandable frame. By removing the need for sutures, operative and cardiopulmonary bypass times may be reduced compared with conventional AVR. Reduced operative time is particularly advantageous for patients requiring multiple procedures including concomitant coronary artery grafting for the treatment of ischaemic heart disease. Sutureless AVR may be undertaken using conventional open heart surgery or minimally invasive techniques. In New Zealand, about 80 sutureless AVR procedures have been undertaken since 2011, all of which have used open heart surgery. Sutureless valves have now been approved for use in Australia and Europe, but not yet in the United States outside clinical trials.
58. The NHC prepared a brief Technology Note on sutureless AVR in May 2012, in response to a request from Waikato District Health Board that year to assess the technology. At the time, it was concluded that insufficient evidence was available for a full assessment to be made, and that sutureless AVR should be conducted only under clinical trial conditions. In March 2013, representatives from ANZSCTS and the Waikato Cardiothoracic and Vascular Surgery Unit, requested that the NHC carry out further assessment of sutureless AVR. It was decided that further assessment of sutureless AVR would be appropriate, given that in the time since the previous NHC report, additional clinical data had been published, NICE (National Institute for Health and Care Excellence) had issued guidance and HealthPACT had assessed the procedure.
Clinical safety and effectiveness
59. The current evidence base is limited for sutureless AVR. Randomised controlled trials with short follow-up time suggest that sutureless AVR is safe, with low incidence of complications and comparable mortality compared with conventional surgical AVR. This is supported by non-randomised controlled trials. Compared with TAVI, sutureless AVR may have lower rates of paravalvular leak. Evidence is limited to observational studies, but sutureless AVR appears to have similar short-term survival compared with surgical AVR in moderate to high-risk patients.
Economic
60. Current evidence suggests sutureless AVR may have similar cost-effectiveness to conventional surgical AVR, with sutureless AVR having comparable outcomes and the possibility of lower costs. The NZ data available from 2012/13, though limited to just 12 sutureless AVR records, show a modest cost differential of $2,000 with similar length of stay compared with conventional bioprosthetic surgical AVR (Table 2). The price differential between sutureless valves and conventional bioprosthetic valves is small and declining. There is currently no evidence of additional procedural or downstream costs associated with sutureless AVR compared with conventional surgical AVR, but there is some evidence of potential savings from reduced hospital and ICU length of stay. Sutureless AVR is a substitute procedure for conventional surgical AVR in

Aortic Stenosis – Decision Paper 21
high-risk patients; as such it is not expected to significantly expand the population pool receiving surgical AVR.
Table 2: Cost of sutureless AVR compared with conventional bioprosthetic AVR
Sutureless AVR All bioprosthetic valves Average cost $48,000 $46,000 Average length of stay (days) 13 12 Valve cost $6,500 $5,700 Number of records 12 331
Source: NHC analysis of NCCP data accessed in 2015, using cost schedule seven.
61. Sutureless valves have declined significantly in price over the past four years as a result of competition. When the NHC first assessed sutureless AVR in 2012, the valve was nearly twice the price it is today. A sutureless valve purchased by Auckland DHB is now roughly the same cost as a regular tissue valve purchased by Canterbury DHB. However, whilst the Sorin Perceval S valve and Medtronic 3f Enable model 6000 valve have become price competitive, the Edwards Lifesciences Intuity valve is reportedly about twice the price of its competitors; with no head-to-head trials available to justify the premium. (32)
62. Medtronic announced its intention to discontinue production of the Medtronic 3f Enable valve in May 2015. There remains variation in price of sutureless valves across the country, which indicates there could be savings. The savings could be obtained from all the DHBs receiving the lowest cost; the lowest costs could be obtained through DHB sharing pricing information or from national collective purchasing.
Societal and ethical
63. Given that the safety and efficacy of sutureless AVR seems comparable, varying access to sutureless valves does not give cause for concern. However, this view may change as the evidence for sutureless AVR evolves.
Feasibility of adoption
64. There may be between five and ten percent of AVR patients that could benefit from sutureless AVR. Potential beneficiaries of the procedure include patients with anatomical features that make suturing difficult or risky, such as a heavily calcified aortic annulus or a very small aortic root. There are no workforce or infrastructure considerations identified that would impede the increase use of sutureless AVR; although, like with all new treatments, appropriate training and oversight would need to be put in place if the use of sutureless AVR increased. Similarly the impact on theatre and staff scheduling and bed days required for sutureless AVR compared with surgical AVR would need to be factored into production planning.
Medical management/palliative care 65. We did not undertake specific assessments on medically managed, including palliative care,
patients. However, in the course of our assessments on aortic stenosis, TAVI and sutureless AVR, it became apparent that there was limited national data on this patient group.
66. New Zealand and international evidence suggest about a third to two-fifths of patients with severe AS may be inoperable (see National Health Committee's Aortic Stenosis Overview Tier 2). That corresponds to a prevalence of about 810 patients, and an incidence of about 300-350 patients per annum. Prevalence is contained by the relatively short life expectancy of these patients.

Aortic Stenosis – Decision Paper 22
67. We estimated a lifetime cost of medically managed severe symptomatic AS of $15,000 per patient (see National Health Committee's Transcatheter Aortic Valve Implantation: Tier 3 Assessment Report).
68. Medical management, with its focus on symptomatic relief, is essentially palliative care. In New Zealand, palliative care has been defined as care for people of all ages with a life-limiting illness which aims to:
1. optimise an individual’s quality of life until death by addressing the person’s physical, psychosocial, spiritual and cultural needs.
2. support the individual’s family, whanau, and other caregivers where needed, through the illness and after death.
69. Palliative care is delivered in a variety of settings, with palliative care generally available where the patient is – be that home, hospital, residential care or hospice. Patients receiving aortic valve replacement (TAVI, surgical AVR or sutureless AVR) and medical management may receive palliative care at the end of their lives. Very limited data was available on end-stage (hospice) palliative care, where we were unable to isolate specific palliative care costs associated with severe AS. To give some indication on the relative materiality of palliative care costs, however, work undertaken by the Ministry of Health indicates that the five-year average palliative care cost for a cancer patient in 2008/09 (understood to receive more palliative care than cardiac patients) was $923.
70. Palliative care is a priority for the Government with the Minister of Health, Jonathan Coleman, recently announcing a review of palliative care services. The review is not about changing the fundamental arrangements of palliative care, but building on progress already made and optimising services to meet future needs. The review follows the Government’s $76.1 million investment into hospice community palliative care services in Budget 2015. The review will be undertaken by the Ministry of Health with support from a Palliative Care Advisory Panel. It will focus on improving services over the next three to five years, while considering the likely demand for those services over the next 10 to 20 years. It will cover primary and specialist services, and all care settings, including the home, hospital, hospice and aged residential care facilities.
71. Medical management is relatively low-cost compared with other treatment options, in part because life expectancy is very limited. The proceeding estimates of the lifetime cost of surgical AVR and TAVI in high-risk and inoperable patients ranged from $84,000 to $101,000, depending on the patient group. In 2012/13, the average cost of AVR was about $45,000 per patient for AS patients across all risk classes. Hence, although we have not specifically calculated the lifetime costs of the much larger moderate and low-risk patient groups, we can be fairly certain that average attributable lifetime cost (post-intervention) for low and moderate-risk surgical AVR patients is in excess of $50,000 per patient. What this means is that medically managed patients comprise a relatively small proportion of the total expenditure on severe AS, probably less than 15%.
Proposed model of care for severe aortic stenosis 72. The assessments of AS, sutureless AVR and TAVI have identified that the balance and level of
investment in severe AS is about right. The challenge for the sector is how new ‘disruptive’ technologies, which have only marginal benefit to patients and the overall model of care, are introduced. The assessments have identified there is marginal patient and sector benefit specific to the use of the sutureless AVR and TAVI (as per the relevant recommendations), however there may be more value from implementing improvements to the overall model of care for severe AS.
73. Aortic valve replacement is an invasive, risky and costly procedure however it is undertaken. The lifetime cost of TAVI ranges from $84,000 to $98,000, for high-risk and technically inoperable patients, respectively. The lifetime cost of surgery ranges from $90,000 to $101,000, while
Aortic Stenosis – Decision Paper 23
medical management is relatively inexpensive, costing about $15,000 per patient over their remaining lifetime. Approximately half all patients on medical management are expected to be dead within a year; with nearly all patients deceased within five years. By comparison, just under half of all high-risk surgical AVR and TAVI patients would be expected to live five years. While patients may survive the procedure, mortality and major adverse events can be significant in some patient groups. To avoid harmful and costly intervention, evidence-based decision-making including surgical and frailty risk assessment, is required.
74. In 2014, the NHC met with sector representatives to discuss potential improvements to the model of care for serve AS. The NHC held its first stakeholder workshop on 28 February 2014 and involved the following groups: the Cardiac Society of Australia and New Zealand (CSANZ), the Australian and New Zealand Society of Cardiothoracic Surgeons (ANZSCTS), the New Zealand Cardiac Network, the College of Intensive Care Medicine of Australia and New Zealand (CICMANZ), Australian and New Zealand Society of Geriatric Medicine (ANZSGM). A second meeting was held on 15 August 2014 which also included representatives from DHB funding and planning, the national Health IT Cluster, and DHB clinical services directors.
75. From these meetings, a proposed revised model of care was drafted. The revised model of care, (subject to sector feedback) indicates four key decision-making points:
1) Severe AS confirmed, initial clinical management decision ‘suitable for intervention’ or ‘not suitable for intervention’.
2) The second decision point is the frailty and comorbidity decision. High frailty scores indicate ‘not for intervention’.
3) The third decision relates to surgical risk. A multidisciplinary team is presented with the results of previous investigations, the surgical risk score (STS or EuroSCORE II) and the frailty score. High-risk patients (STS score >8) are referred to the TAVI pathway, low or medium-risk are referred to the surgical waiting list. Inoperable patients are referred to the medical management or palliative care pathway, with the exception of technically inoperable patients who are referred for TAVI.
4) The final decision relates to the patient’s suitability for the TAVI procedure, and again is made by a multidisciplinary team. Patients may be referred to the surgical waiting list or to the medical management or palliative care pathway if they are not deemed suitable for TAVI.
76. The main points of difference from the current model of care are discussed below.
Standardised national patient selection criteria for severe aortic stenosis interventions • Current New Zealand patient selection guidelines are not consistent with the stated policy
that TAVI be used for high-risk patients only.
• The target population for TAVI procedures is recommended to be limited to those with an STS score greater than 8 or those patients identified as technically inoperable (eg with calcific aorta or hostile chest) for surgical aortic valve replacement. TAVI may be considered for lower risk populations subject to future evidence of its relative safety, effectiveness and cost-effectiveness in these populations.
• The threshold for patients receiving TAVI is a DHB-level prioritisation decision. However, the evidence at this time does not support TAVI for low and moderate-risk patients.
• Monitoring at a national level through the DHB accountability framework, including the potential to establish specific TAVI targets, is proposed to ensure the national prioritisation criteria are implemented and maintained.

Aortic Stenosis – Decision Paper 24
Operative risk tool preferably STS-PROM rather than EuroSCORE I
• New Zealand and international evidence indicates STS-PROM is an accurate predicator of operative mortality while EuroSCORE II may be an improvement on EuroSCORE I.
Frailty and cognitive assessment as part of the clinical decision process • Patients with high frailty indices are unlikely to survive for reasons other than their primary
cardiac condition and this can make invasive and expensive interventions like aortic valve replacement clinically futile and cost-ineffective.
• A formal scoring tool developed by the Ministry of Health, the Cardiac Surgical Appropriateness tool, is now under evaluation and includes measures of patient frailty, comorbidities, cognitive function, and surgical complexity. The NHC has also contributed to the evaluation of the scoring tool through the provision of Health Innovation Partnership funding for the ‘Evaluation of Frailty and Comorbidity in Patients with Ischaemic Heart Disease’ by Professor Ralph Stewart at Auckland DHB. The fields for this tool have been included in the national cardiology registry for the patients included in the trial. It is expected that the tool may be used more broadly than IHD, but this will not be known until the research is completed.
• A tool needs to be developed/adopted and implemented which measures physical frailty and cognitive function and is applicable to aortic stenosis.
Patient selection to be undertaken by a specified multidisciplinary team
• A TAVI programme can only be offered by a hospital with a full cardiac surgery service. It is not clear that all three TAVI centres in New Zealand are employing a comprehensive multidisciplinary team approach. To the extent that this is the case, it is recommended that practice is bought back into line with New Zealand, European and United States professional guidelines.
• With the acknowledged importance of cognitive and frailty testing prior to surgery, the role of the geriatrician in the multidisciplinary team might be considered less optional in the team due to their skills and experience in this field.
• Cardiac surgery/cardiology conferences are long-standing joint multidisciplinary decision-making bodies in New Zealand. For the centres providing TAVI, these are suitable decision making mechanisms (ie multidisciplinary heart teams) for the final TAVI decision. However, for those cardiac centres referring potential TAVI patients to other cardiac centres, it would be appropriate for the referral to come through the existing cardiac surgery/cardiology conference or directly from the referring cardiologist. This is to ensure consistent, timely, cost-effective decision-making for patients and providers, and to enable alignment with professional guidelines and consistent patient selection and management for these patients.
Mandatory entry of clinical and business data into a national registry for all interventions for severe aortic stenosis
• A national registry is recommended which captures the following information:
o Patient information based on and linked to the national NHI system.
o Surgical risk score (STS-PROM).
o Frailty score which measures physical frailty and cognitive function.
o Quality of life measures from the patient’s perspective using the NZ version of EQ5D, or similar, captured at referral and one and two years post-intervention.

Aortic Stenosis – Decision Paper 25
o Technical reasons for inoperability ie calcific aorta, hostile chest.
o Multidisciplinary team treatment decision.
o Treatment undertaken, ie surgical aortic valve replacement, balloon valvuloplasty, transcatheter aortic valve implantation, sutureless aortic valve replacement, medical management or palliative care.
o Valve and delivery system device information to enable tracking.
o Valve Academic Research Consortium-2 (VARC-2) endpoints ie device success, stroke, paravalvular leak, major vascular complications etc.
o Business data including resource utilisation to supplement data collected by DHB patient management and clinical systems to support management of the national AVR waiting list, national AS targets, time to access diagnostics and treatment, and real-time budget management.
• A quality registry requires good governance, to operate within the accountability for reasonableness framework and potentially form part of continuing professional development and accreditation.
• Recently, the Ministry of Health has established two registries: one for cardiac surgery (National Cardiac Surgery Registry, Dendrite Clinical Systems) and the other for cardiology (Acute Predict, Enigma solutions), which includes data on acute coronary syndromes and interventional cardiology procedures. Both registries are operational and neither registry is capturing any data on the overall AS model of care at the current time. DHBs are collecting information on TAVI in local databases. There are advantages and disadvantages of collecting AS model of care information in either registry. Either registry could be modified to include the national AS registry. The New Zealand Cardiac Network and Cardiac Society have indicated a preference for the cardiology registry. The focus needs to be on the outcomes to be achieved and which registry is the most sustainable solution for the sector.
• There will be a cost of establishing and maintaining a national registry for AS including software, reporting, data collection and entry costs which should be factored into the implementation plan.
Quality of life measurement from a patient perspective using a tool such as EQ5D captured at referral and year 1 and 2 follow-ups
• Quality of life data provides invaluable feedback to clinicians looking to avoid unnecessary and harmful intervention. It can also provide the health sector with the evidence required for cost-effective diffusion of emerging technologies.
• European and United States guidelines for valvular disease note the need for clinicians to consider the likely quality of life of patients post-intervention – where an anticipated life expectancy of one year or less, or no expectation of improved quality of life, are considered contraindications for AVR.
• There is a New Zealand precedent, the New Zealand Joint Registry routinely collects quality of life data at baseline and five years using the Oxford 12 Questionnaire.
• World leading registries, including the United States national Society of Thoracic Surgeons (STS) and the American College of Cardiology (ACC) TVT Registry, the French national FRANCE-2 registry, and the German national GARY registry, all include measurement of patient quality of life. In the GARY registry, patient quality of life is measured through a simple and well-established tool, known as the EQ5D. Quality of life is recorded at baseline and at one, three, and five years post-intervention for TAVI and surgical AVR patients.

Aortic Stenosis – Decision Paper 26
• The collection of data at year 1 and 2 follow-ups should be factored into the implementation planning, as not all AS interventions routinely include one and two year follow-ups. DHBs are also implementing strategies to reduce unnecessary follow-ups where possible. There will be costs associated with the measurement tool which need to be considered, including tool licensing, data collection and entry.
Financial implications of aortic stenosis model of care
77. The recommendation is that TAVI and sutureless AVR procedures are provided within the existing cardiac surgical budget. The expected additional cost to DHBs of providing TAVI to technically inoperable patients is about $1 million per annum, increasing to $1.7 million by 2019/20. Sutureless AVR costs are estimated to be only slightly ($2,000) more expensive than surgical AVR, with this gap reducing over time as the cost of the valve reduces.
78. The economic assessments for sutureless AVR and TAVI have been based on international evidence and the New Zealand data that is available through the national costing programme. These costs have also been checked with Auckland DHB. It is recognised that there are limitations with small datasets and applying the assumptions locally from international studies, however, we believe the costs presented in the Tier 3 assessments for the delivery of both TAVI and sutureless AVR impartially represent available information.
79. Further input from stakeholders relating to implementation is required to fully understand the system-wide costs of the other aspects of the revised model of care. These costs include the costs of the national registry, change to surgical risk assessment, implementation of a frailty tool, the potential addition of two years of follow-up, the addition of a quality of life measurement tool, data collection, entry and reporting, and any further costs associated with the multidisciplinary team, eg costs of geriatrician time.
80. Further analysis is also required to cost the benefit of the new model of care, ie what is the overall saving from introducing the four decision-making points and national registry? While there may be a willingness to reprioritise within the cardiac surgery budget to accommodate sutureless AVR and TAVI, the sector will want to understand the financial and other benefits of investing in better data collection (national registry) and the inclusion of geriatricians in the multidisciplinary clinical teams.
Implementation
81. There remain a number of complex issues and challenges to consider for implementation. Feedback from the sector is required to better understand how these may be managed. Some of these challenges include:
• Refocusing TAVI delivery on high-risk and technically inoperable patients.
• Applying an appropriate intervention rate for each DHB’s population for AS interventions (surgical AVR, sutureless AVR, TAVI, medical management).
• Managing the diffusion of TAVI in the longer term. TAVI is likely to become more widely used as evidence of its relative safety, effectiveness and cost-effectiveness in lower risk populations becomes available.
• Management of unmet need identified through improved referral pathways from primary care through to cardiology.
• Access to diagnostics in a timely way to inform each decision point in the model of care.

Aortic Stenosis – Decision Paper 27
• Managing existing workforce issues within these services while implementing a revised model of care. There are existing workforce vacancies for perfusionists and sonographers. A significant medium-term workforce issue relating to the replacement of cardiothoracic surgeons as the current group retires and an issue relating to the scope of practice and facilities available to encourage cardiologists to be based in provincial centres.
• The scope of practice between cardiologists and cardiac surgeons is blurring as TAVI procedures are provided by both specialties in NZ, the implications of which need to be carefully managed.
• Establishing a fair and transparent national price for TAVI and for other AS interventions which reflect the costs of delivering AS interventions for both the DHB of domicile and the DHB of service. Recognising that in 2013/14 the DRGs related to AVR showed a shortfall. While this can create an incentive to prioritise these interventions locally and only fund the procedure when it makes sense – ie not in low-risk patients, this may be challenging in reality.
• Establishing a national registry for the AS model of care when there are two established registries in the sector which could be used to house the AS registry.
• Establishing a nationally consistent approach to clinical decision-making when regional cardiac centres and TAVI centres have developed based on what works locally/regionally.
• Maximising the opportunity of national purchasing and procurement for aortic valves. For example, one type of sutureless valve may be twice the price of its competitor, with no head-to-head trial evidence justifying the price differential.
• Managing facility capacity as individual DHBs seek to establish additional catheterisation laboratories and hybrid catheterisation laboratories/operating theatres.
The recommendation for sutureless AVR and TAVI to be ‘absorbed’ within the current cardiac services budget and resources is a further example of general expansion of cardiac services on a procedure-by-procedure basis. This type of incremental approach to new technologies is unsustainable and there is a real need to establish a strategic plan for cardiac services in NZ that sets a five to ten-year view of where the services should be.

Aortic Stenosis – Decision Paper 28
National Health Committee (NHC) and Executive
The National Health Committee (NHC) is an independent statutory body which provides advice to the New Zealand Minister of Health. It was re-formed in 2011 to establish evaluation systems that would provide the New Zealand people and health sector with greater value for the money invested in health. The NHC executive are the secretariat that supports the committee. The NHC executive’s primary objective is to provide the committee with sufficient information for them to make recommendations regarding prioritisation and reprioritisation of interventions. They do this through a range of evidence-based reports tailored to the nature of the decision required and timeframe within which decisions need to be made.
Citation: National Health Committee. 2015. Aortic Stenosis: Decision Paper. Wellington: National Health Committee
Published in October 2015 by the National Health Committee
PO Box 5013, Wellington, New Zealand
ISBN (to be confirmed for final version)
(HP TBC)
This document is available on the National Health Committee’s website:
http://www.nhc.health.govt.nz/
Disclaimer
The information provided in this report is intended to provide general information to clinicians, health and disability service providers and the public, and is not intended to address specific circumstances of any particular individual or entity. All reasonable measures have been taken to ensure the quality and accuracy of the information provided. If you find any information that you believe may be inaccurate, please email to [email protected].
The National Health Committee is an independent committee established by the Minister of Health. The information in this report is the work of the National Health Committee and does not necessarily represent the views of the Ministry of Health.
The National Health Committee makes no warranty, expressed or implied, nor assumes any legal liability or responsibility for the accuracy, correctness, completeness or use of any information provided. Nothing contained in this report shall be relied on as a promise or representation by the New Zealand Government or the National Health Committee.
The contents of this report should not be construed as legal or professional advice and specific advice from qualified professional people should be sought before undertaking any action following information in this report.
Any reference to any specific commercial product, process, or service by trade name, trademark, manufacturer, or otherwise does not constitute an endorsement or recommendation by the New Zealand Government or the National Health Committee.