Embed Size (px)
Citation preview

Cardiovascular Medicine and Surgery
Aortopulmonary WVindow with Anomalous Originof the Right Coronary Artery from the Pulmonary Trunk
Juan A. Casillas, M.D., Julio P. de Leon, M.D., Fernando Viliagra, M.D.,Salvador L. Checa, M.D., Pedro A. Sanchez, M.D., Ricardo Gomez, M.D.,
Ramon Fortuny, M.D., and Jose Mil Brito, M.D.
A case of aortopulmonary window associated with an anomalousorigin of the right coronary artery from the pulmonary artery in a
3-month-old boy is reported. Angiographic diagnosis could be difficultbecause of the simultaneous filling of both great arteries that obscurethe origin ofthe anomalous vessel; however, a careful evaluation oftheangiogram may contribute to an accurate diagnosis. The surgicalcorrection of this association of defects requires the connection of theaorta with the anomalous coronary ostium. An intrapulmonarytunneling procedure by means of a baffle is described. (Texas HeartInstitute Journal 1986; 13:325-331)
Key words: aortopulmonary window; intrapulmonary tunneling
AORTOPULMONARY window is a rare
congenital cardiac anomaly that fre-quently masks other congenital heartdefects. 2-19We report the successful operation of
an infant with an aortopulmonary windowand anomalous origin of the right coronaryartery from the anteromedial wall of thepulmonary trunk.
CASE REPORT
A 3-month-old boy was referred to our
surgical unit with a 1-month history of conges-tive heart failure. On examination, he was
dyspneic and acyanotic, with bounding periph-eral pulses, a Grade 3/4 continuous murmur atthe left upper sternal border, and an enlargedliver. His weight was 4.190 kg. The electrocar-diogram showed sinus rhythm and biventricu-lar hypertrophy (Fig. 1). A chest X-ray
film revealed moderate cardiomegalyand increased pulmonary vascular mark-ings. Cardiac catheterization disclosed a largeleft-to-right shunt at arterial level, with ele-vated pressure in the pulmonary artery (TableI). Aortography showed a large aortopulmo-nary defect. The anomalous origin of the rightcoronary artery from the pulmonary trunk wasclearly seen (Fig. 2), but it was overlookedpreoperatively. Surgical repair was donewith the aid of cardiopulmonary bypass,deep hypothermia, and circulatory arrest.A 15-mm wide aortopulmonary window andthe anomalous right coronary artery were
apparent from outside and through a pulmo-nary arteriotomy. Right and left coronary
arteries were otherwise normal in size anddistribution. The anomalous coronary ostium,situated 5 to 7 mm below the aortopulmonarywindow, was connected to the aorta by means
of a 2.5 x 1.5 cm intrapulmonary baffle of
Texas Heart Institute Journal
From the Servicio de Cirugia Cardiaca Pediatrica, HospitalRamon y Cajal, Madrid, Spain.Address for reprints: Juan A. Casillas, M.D., C/ Santiago de Chile 6,60B, Santiago deCompostela, La Corufia, Spain.
Aortopubnonary Wusdow 325

avr
avl
avf
V3r V3
Vi
V2
V4
V5
Mg. 1 Preoperative electrocardiogram.
TABLE 1. Preoperative Cardiac Catheteri-zation Data
Pressure 02 Saturation(mm Hg) (%)
Left ventricle 70/10 93Aorta 70/26 g3Right ventricle 50/8 81Main pulmonary
artery 50/22 89Right pulmonary
artery 40/18 87Right atrium 3Left atrium 8 93
Flg. 2 Aortogram in lateral projection. The area ofthe aortopulmonary window is shown (arrows) withfilling of the right coronary artery as it arises from thepulmonary artery. PA = pulmonary artery; RCA =
Right coronary artery.
expanded polytetrafluorethylene, as was
reported by Hamilton et al20 and Takeuchi etal.21 The pulmonary artery was closed bydirect suture, leaving a wide arterial lumen(Fig. 3). The postoperative course was
uneventful, and the patient was discharged inexcellent condition (Fig. 4).
Vol. 13, No. 3, September, 1986
I I
I I i
V6
V7
-1.
ii
'7.-'
326 Aortopulmonary Mrsdow
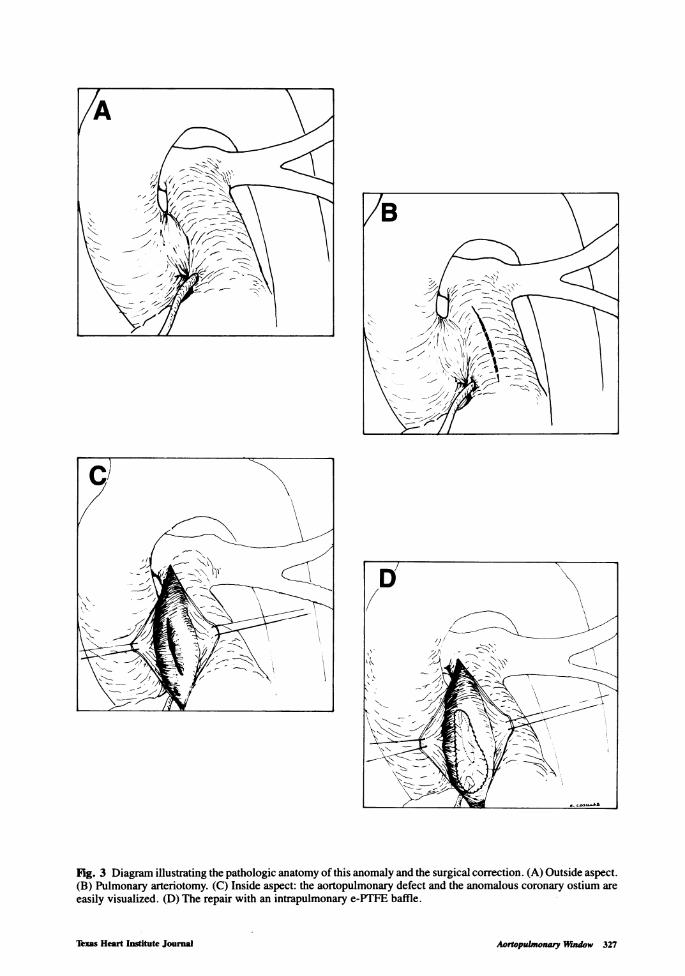
Fig. 3 Diagram illustrating the pathologic anatomy of this anomaly and the surgical correction. (A) Outside aspect.(B) Pulmonary arteriotomy. (C) Inside aspect: the aortopulmonary defect and the anomalous coronary ostium areeasily visualized. (D) The repair with an intrapulmonary e-PTFE baffle.
Jbxas Heart Institute Journal Aortopulmonawy Endow 327

av r
I I
III
avl
avf
V3V3r
VI V4
V2 V5
Fig. 4 Postoperative electrocardiogram without signs of ischemia.
DISCUSSION
To the best of our knowledge, eleven cases
of aortopulmonary window with anomalousorigin of the coronary arteries have beenreported (Table II). The right coronary arterywas involved in eight cases, including our
own patient, and the left coronary artery infour patients.
Alterations in septation of the aorta and thepulmonary artery may happen between the 5thand 6th weeks of embryonic life. The lack ofdevelopment of spiral septum and alterationsin the rotation of troncoconus cause the aor-
topulmonary defects.'6'22In the preoperative diagnosis of this ano-
maly and the existence of associatedanomalies that are frequently seen in thepulmonary arteries or in the subclavianarteries, the difficult part is that the angio-graphic evaluation must be exact. Aortic rootinjection is the best preoperative study todiagnose the aortopulmonary window and todetermine the relationship of the pulmonaryarteries and the coronary arteries with thedefect. The visualization of a coronary artery
after injection in the right ventricle, withelevated pressure in the pulmonary artery incases of aortopulmonary window, suggeststhat the coronary arteries originate in thepulmonary trunk. 11The clinical picture of the patients with
aortopulmonary window is dominated by thesigns and symptoms ofcongestive heart failurecaused by the left-to-right shunt. The patho-physiology of this combination ofanomalies issimilar to the anomalous origin of the leftcoronary artery from the pulmonary artery(Bland-White-Garland Syndrome) with ven-
tricular septal defect. In both cases, the 02
saturation and the pressures in the pulmonaryartery are at systemic level, and the anomalouscoronary artery carries moderately well-oxygenated blood from the pulmonary trunk tothe myocardium.The first surgical intent to correct the
aortopulmonary defect through a ligature inassociation with this coronary anomaly led tointraoperative problems that did not permit theuse of this technique.'3'15 In the same way, theclosure of the aortopulmonary window, leav-ing the coronary ostium in the pulmonary
Vol. 13, No. 3, September, 1986
Vs
V7
328 Aortopubnonary Wuufow

.> co .> s, U Ct0> a V11
<;z a0C.2
0z(Cu C >,> >0) *
a < < <
rC 23 cm 0
0 00u0CD ' 0
co o " 75
Cur Co 0cuo ~ Co CL.
0
0 0 0 0 0.z z z z z c. E,
CD
a.
c'o> CL o
acn
a:Cl)
C'.>
0 0 0 0
z z z z
a-
dCl)
< < < <: < < < < < <: J
a: a: a:a:r a: a: -a -j -aa:r
lgt Om)'(D t V- _
N N CM 0)7t 0 00Le) cD co ND _ C CO N0) 0) 0) 0)) 0) 0) 0)1- 7-v -7 7- 7-
1-0 00C m
E
CD) cD
0) 0)
0) (I) TC
0) 0) 0)O- O- -
0
0 co
"CDCu
co 0
0cin i ...a< a: co in a-
04 cr) "it LO co N a) 0 -CM
CD
C,.50
Cu
C
0
E
75CL
co
0
C,)
Cu)
C
0E0Cu
2-o
01cn*I_
co
CU
0
C
a: a
0
0
a)CI
0
to
CDuC
-
co
*< 1
Cu11 o
0
Dt
CD-
t0n
~JO)
Texas Heart Institute Journal
z
0E0
0
-W
L. U
a0
~01- a
= aa.
_IoC
ac
I-
e0
a-
N.
60
(5Z
0
c:
Ch)
CVI-e
._
co
0
E0
a.0
m
0.
CO
0
2
co
0
0r-
cocn
0
0
CV
C)
0
r.0
J0
Cu0
0.0
0co
Aortopubnonary Wudow 329

artery by oversight, resulted in the patient'sdeath.17 These events are similar to thosedescribed in cases of anomalous origin of theleft coronary artery from the pulmonary arterywith ventricular septal defect, after the ven-tricular septal defect closure, and withoutthe reinsertion of the coronary artery inthe aorta.2325
For these reasons, the surgical technique forthe correction of this anomaly necessarilyincludes the connection of the anomalouscoronary ostium with the aorta to support anadequate myocardial perfusion. Differenttechniques were employed for such purposesas the transfer of the coronary ostium to theaorta, 16 rotation plastic procedure with pulmo-nary tissue patch,'8 and tunneling.9"4 In thispatient, using the aortopulmonary windowwith the help of an e-PTFE baffle (2.5 x 1.5cm), we connected the aorta with the anomal-ous ostium, as described by others 20,21 in theBland-White-Garland Syndrome.
In any case, after careful inspection of thepulmonary arteries and the ostium of thecoronary arteries, extracorporeal circulationmust be done through the aorta or the pulmo-nary artery to carry out an adequate correction.
ACKNOWLEDGMENT
We acknowledge the excellent technicalassistance of Mr. Eugenio M. Casillas for hishelp in preparing the graph.
REFERENCES
1. Putnam TC, Gross RE. Surgical management ofaortopulmonary fenestration. Surgery 1966;59:727.
2. Blondeau PH, Menasche PH, D'Allaines CL,Piwnica A, Dubost CH. Fistules aorto-pulmonaires congenitales: Six cases operas:Resultats tardifs 3 a 20 ans apres 1' intervention.Ann Chir: ChirThorac Cardiovasc 1980; 34:233.
3. Deverall PB, Lincon JCR, Aberdeen E, BonhamCarter RE, Waterston DJ. Aortopulmonarywindow. JThorac Cardiovasc Surg 1969; 57:479.
4. Langlois J, Binet JP, Planche LL, Conso JF. LeTraitment chirurgical des fistules aorto-pul-monaires. A propos de seize cas. Ann Chir: ChirThorac Cardiovasc 1980; 34:216.
5. Marchand M, Lemoine G, Morrille P, RiberollesCD, Lecompte Y, Bex JP, Leca F, Hazan E,Neveaux JY, Mathey J. Fistules aorto-pul-monaires. Experience de quince cas. Ann Chir:Chir Thorac Cardiovasc 1980; 34:224.
6. Cooley DA, McNamara DG, Latson JR. Aor-ticopulmonary septal defect: Diagnosis andsurgical treatment. Surgery 1957; 42: 101.
7. Castafieda AR, Kirklin JW. Tetralogy of Fallotwith aorticopulmonary window. Report of twosurgical cases. J Thorac Cardiovasc Surg 1977;74:467.
8. Crawford FA Jr, Watson DG, Joransen JA.Tetralogy of Fallot with coexisting type IIaortopulmonary window. Ann Thorac Surg 1981;31:78.
9. Shore DF, Yen Ho S, Anderson RH, DeLeval M,Lincoln C. Aortopulmonary septal defect coexist-ing with ventricular septal defect and pulmonaryatresia. Ann Thorac Surg 1983; 35:132.
10. Jacobson JG, Trusler GA, Izukawa T. Repair ofinterrupted aortic arch and aortopulmonarywindow in an infant. Ann Thorac Surg 1979;28:290.
11. Agius PV, Rushworth A, Connolly N. Anomal-ous origin of the left coronary artery from thepulmonary artery associated with an aortopulmo-nary septal defect. Br Heart J 1970; 32:708.
12. Doty DB, Richardson JV, Falkousky GE, Gor-donova MI, Burakovsky VI. Aortopulmonaryseptal defect: Hemodynamics, angiography, andoperation. Ann Thorac Surg 1981; 32:244.
13. Shumacker HB. Discussion of Reference 6.14. Burroughs JT, Schumutzer KJ, Linder F,
Neuhans G. Anomalous origin of the rightcoronary artery with aorticopulmonary windowand ventricular septal defect. J Cardiovasc Surg1962; 3:142.
15. Morrow AG, Greenfield LJ, Braunwald E.Congenital aortopulmonary septal defect: Clini-cal and hemodynamic findings, surgicaltechnique and results of operative correction.Circulation 1962; 25:463.
16. Blieden LL, Moller JH. Aorticopulmonary septaldefect. An experience with 17 patients. Br HeartJ 1974; 36:630.
17. Richardson JV, Doty DB, Rossi NP, Ehrenhaf T.The spectrum of anomalies of aortopulmonaryseptation. JThorac Cardiovasc Surg 1979; 78:21.
18. Luisi SV, Ashraf NH, Gula G, Radley-Smith R,Yacoub M. Anomalous origin of the right coro-nary artery with aortopulmonary window:Functional and surgical considerations. Thorax1980; 35:446.
19. Bourlon F, Kreitmann P, Jourdan J, GrinneiserD,Schmitt R, Dor V. Anomalous origin of the leftcoronary artery with aortopulmonary window. Acase report with surgical correction and delayedcontrol. Thorac Cardiovasc Surg 1981; 29:91.
20. Hamilton DI, Ghosh PK, Donnelly RJ. Anoperation for anomalous origin of the leftcoronary artery. Br Heart J 1979; 41: 121.
21. Takeuchi S, Imamura H, Katsumoto K, HayashiI, Katohgi T, Yozu R, Ohkura M, Inone T. Newsurgical method for repair of anomalous leftcoronary artery from pulmonary artery. J ThoracCardiovasc Surg 1979; 78:7.
Vol. 13, No. 3, September, 1986330 Aortopulmonary Mndow

22. Meisner H, Schmidt-Habelmann P, Sebening F,Klinner W. Surgical correction of aortopulmo-nary septal defects. A review of the literature andreport of eight cases. Chest 1968; 53:750.
23. Rao BNS, Lucas RVJr, Edwards JE. Anomalousorigin of the left coronary artery from the rightpulmonary artery associated with ventricularseptal defect. Chest 1970; 58:616.
24. Monselise MB, Vlodaver Z, Neufeld HN. Singlecoronary artery. Origin from the pulmonaryartery in association with ventricular septaldefect. Chest 1978; 58:613.
25. Wilcox WD, Hagler DJ, Lie TJ, Danielson GK,Smith HC, Fulton RE. Anomalous origin of theleft coronary artery from pulmonary artery inassociation with intacardiac lesions. Report oftwocases. J Thorac Cardiovasc Surg 1979; 78:12.
26. Doty DB. Safe closure of aortopulmonarywindow. Chest 1983; 83:443.
Corrections: Flow Characteristics of Coronary Balloon Catheters (June, 1986; 2:213-215). On the left-hand side of the lowerpicture on page 214, the words should have read Pressure (psi) instead of Pressure (mm Hg).
Left Coronary Artery Spasm Causing Severe Left Ventricular Dysfunction Without Myocardial Infarction (June1986; 2:223-231). The pictures on Fig. 2 and Fig. 3 are reversed.
Jlzxs Heart Institute Journal Aortopubnoar Wdow 331








![Anatomical variation of the origin of the left vertebral ... · [10] Panicker HK, Tarnekar A, Dhawane V, Ghosh SK. Anomalous origin of left vertebral artery – embryological basis](https://img.pdfslide.net/doc/110x75/6061a70263c3fb0e604de723/anatomical-variation-of-the-origin-of-the-left-vertebral-10-panicker-hk-tarnekar.jpg)