Embed Size (px)
Citation preview

1
AP112 Pathologic Diagnosis of Infectious
Diseases: New Strategies and Challenges
Course DirectorSherif R. Zaki, M.D., Ph.D.

2
Course Objectives
• Differentiate between infectious and non-infectious processes
• Design syndromic approach to diagnosis of infectious diseases
• Compare histopathologic, special stains, immunohistochemical testing and molecular methods and make a rational decision on which methods to use in your practice

3
Course Objectives• Decide which criteria/tests
(histopathology, special stains, IHC, etc) are applicable to achieve specific diagnoses
• Determine if testing can be performed in your laboratory vs. specialty laboratory
• Discuss clinical history, pathologic examination and epidemiologic analysis that might prompt consideration of a bioterrorism event or of an emerging disease

4
Agenda
• Sherif Zaki, M.D., Ph.D. 1:35-2:15Chief, Infectious Disease Pathology Centers for Disease Control and PreventionRole of Pathology in Studies of Emerging Infectious Diseases and Other Health Threats
• Margie A. Scott, M.D. 2:15-3:00Chief, Pathology & Laboratory Medicine ServiceCentral Arkansas Veterans Healthcare SystemMicrobiology and Molecular Applications for the Modern Laboratory

5
Agenda
• A. Brian West MD, FRCPath . 3:30-4:15Department of PathologyNew York University Medical CenterGastrointestinal Infections: a systematic approach to diagnosis
• Wun-Ju Shieh, M.D., M.P.H., Ph.D. 4:15-5:00Staff Pathologist, Infectious Disease Pathology Centers for Disease Control and PreventionPathologic Diagnosis of Encephalitis

6
Role of Pathology in Studies of
Emerging Infectious Diseases and Other Public Health Threats
Sherif R. Zaki, M.D., Ph.D.Chief, Infectious Disease Pathology Activity
National Center for Infectious DiseasesCenters for Disease Control and Prevention
© College of American Pathologists 2004. Materials are used with the permission of
Sherif R. Zaki, MD, PhD.

7

8
Factors in the Emergence of Infectious Diseases• Human demographics and behavior• Technology and Industry• Economic development and land use• International travel and commerce• Microbial adaptation and change• Breakdown of public health measures• Deliberate disseminationFrom Institute of Medicine, 1992

9
Infectious Disease Pathology and Public Health• Pathologists among first health care workers
to encounter infectious disease outbreaks• Pathologists are in excellent position to
discover emerging infectious diseases• Collaborative research
– Epidemiologists– Clinicians– Veterinarians– Microbiologists

10
Infectious Disease Pathology and Public Health• Many examples of recent emerging
infectious diseases diagnosed through autopsies
• Autopsy is increasingly being viewed as an effective surveillance tool– Pathologic specimens can serve as
sentinel indicators of emerging pathogens

11
Recent Global Challenges to Public Health (CDC)
• 93 - Hantavirus Pulmonary Syndrome – U.S.• 94 - Plague/leptospirosis – India• 95 - Leptospirosis – Nicaragua• 95-01 -VHFs (Ebola, Lassa, RVF) – Africa, Asia• 96 - Typhus – Burundi• 97 - H5N1 Influenza – Hong Kong• 98-99 - Enterovirus 71 - Malaysia, Taiwan• 98 - Plague – Ecuador• 99 - Nipah virus – Malaysia, Singapore• 99-04 -West Nile virus – U.S.• 00 - Rift Valley – Kenya, Saudi Arabia, Yemen• 01 - Anthrax – U.S.• 03 - SARS – Global• 03 - Monkeypox – U.S.• 03-04 - Pediatric Influenza Deaths – U.S.• 02-04 – Emerging viral infections in transplant recipients – U.S.

12
Syndromic Approach to Diagnosis of Emerging Infectious Diseases
• Hemorrhagic Fevers – Hantavirus, Lassa, Malaria,Anthrax
• Cutaneous Rash – Monkeypox, Rickettsialpox• Pneumonia – SARS, influenza• Encephalitis – WNV, Nipah• Transplant (Immunosuppressed) – WNV, LCM,
Rabies

13
Syndromic Approach to Diagnosis of Emerging Infectious Diseases
• Histopathologic pattern• Laboratory approach
– Culture– Serology– EM– IHC– Molecular

14

15
Tissues
VascularBone
Musculo-Skeletal
Eyes, SkinEyesSkin
Donor
Organs
HeartLungsLiver
PancreasKidney
Organ and Tissue Recovery
Screening and Testing

16Iwamoto M, et al. Transmission of West Nile Virus from an organ donor to four transplant recipients. NEJM, 2003; 348(22):2196-2203.Cushing MM, et al. Fatal West Nile virus encephalitis in a renal transplant recipient. AJCP, 2004; 121:26-31.

17

18
Investigation of Rabies Infections in Organ Donor and Transplant Recipients –
Alabama, Arkansas, Oklahoma, and Texas, 2004. MMWR, 2004; 53(26):586-589.

19
Investigation of Rabies Infections in Organ Donor and Transplant Recipients –
Alabama, Arkansas, Oklahoma, and Texas, 2004. MMWR, 2004; 53(26):586-589.

20
Investigation of Rabies Infections in Organ Donor and Transplant
Recipients – Alabama, Arkansas, Oklahoma, and Texas, 2004.
MMWR, 2004; 53(26):586-589.

21
Investigation of Rabies Infections in Organ Donor and Transplant Recipients –
Alabama, Arkansas, Oklahoma, and Texas, 2004. MMWR, 2004; 53(26):586-589.

22
Case Histories• On Dec 8, 2003, CDC contacted by WI
DOH– Two organ transplant recipients died– Another organ transplant recipient with
seizure– All from same donor
• Organ procurement organization contacted, all stored tissues quarantined

23
EM of Cytopathic Agentin Vero E6 Cells
Mouse Brain
LCM IHC

24Kidney recipient #1

25Kidney recipient #2: skin

26
Liver recipient

27
LCMV- liver transplant Lassa fever- liver
Imported Lassa fever – New Jersey. MMWR, 2004; In Press.

28
Clinical History
• 38 yo male from NJ• Traveled to West Africa frequently• 08/21/04 – high fever, chills, severe
sore throat, diarrhea, and back pain• 08/23/04 – boarded flight from Sierra
Leone to Newark, connecting at Gatwick Airport
• 08/24/04 – arrived in Newark, was hospitalized, and died

Geographic Distribution
of Arenaviruses

30
Airplane Seating PlanRow 19 A B C D E F J K L Row 19
Row 20 A B C D E F J K L Row 20
Row 21 A B C D E F J K L Row 21
Row 22 A B C D E F J K L Row 22
Row 23 A B C D E F J K L Row 23
Red – Index case
Green – contacted and healthy
Blue – not contacted
Imported Lassa fever – New Jersey. MMWR, 2004; In Press.

31
•36 yo male 3rd mate on MS Overseas Marilyn
•Made port in West Africa (Sierra Leone, and Nigeria)
•08/23/04 – high fever, chills, severe sore throat, and myalgia
•08/31/04 – died onboard, body frozen in meat locker, and ship quarantined off of Texas coast

32

33

34
Dengue
Imported Dengue – United States, 1997 and 1998. MMWR, 2000; 49:248-53.

35
Yellow Fever
Fatal Yellow Fever in a traveler returning from Venezuela, 1999. MMWR, 2000; 49:303-05.

36
May 1993
On presentation
3 days later3 days later

37

38

39

40

41

42
122
3
7
23
12
3
1
5
21
3
1 11 11112
3
12
1112
1122
12
32
12
4
1
3
112
12
1 112
6
43 3
111
32
4
6
4
223
1 1
33
8
6
3
6
23
11 122
12
32
1 11 1
1
34
7
5
1
2
3
1
4
1
1
23
1 111
121 11
1
1111
1
11
1
21
2
1 3
2
242
2
1 1
22
1
1
1
2
1
12
1
112
12
1
1
21
0
2
4
6
8
10
12
14
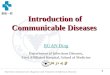
J M S J M S J M S J M S J M S J M S J M S J M S J M S J M S J
Month and Year of Onset
Num
ber o
f Cas
es
Alive Dead
Hantavirus Pulmonary Syndrome Cases by OutcomeUnited States, as of January 15, 2003
*Thirty-two additional cases (nineteen deceased) with onset before 1993 not shown.
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
N=333*

43

44Zaki SR, et al. Leptospirosis associated with an outbreak of acute febrile illness and pulmonary hemorrhage, Nicaragua 1995: Lancet, 1996; 347:535-36.
test

45
Zaki SR, et al. Leptospirosis associated with an outbreak of acute febrile illness and pulmonary hemorrhage, Nicaragua 1995: Lancet, 1996; 347:535-36.

46

47
Rainfall Data 1994 - 1998, Springfield, IL
Jan Feb Mar Apr May Jun Jul0
2
4
6
8
10
12
Month
Prec
ipita
tion
(inch
es) 1998 Precipitation (inches) 1994-1997 Mean Precip. (inches)
Illinois triathlon

48
Springfield Triathlon Participants (n=875)
nvestigation - telephone survey, case control study,it i ti ti i t l i ti ti l b t

49Guarner J, et al. Leptospirosis mimicking acute cholecystitis among athletes participating in a triathalon. Human Path., 2001; 32(7):750-52.

50
Recognition: Palm Beach County, Florida• 63 yo male photo editor
employed by American Media, Inc.
• Onset 9/30/01: fever, fatigue, sweats, altered mental status
• Admitted to hospital 10/2
• CDC notification 10/3
Sa
sS
Alachua
BakerBay
Bradford
Brevard
Broward
Calhoun
Charlotte
Citrus
Clay
Collier
Columbia
Dade
De Soto
Dixie
Duval
Flagler
Franklin
Gadsden
Gilchrist
Glades
Gulf
Hamilton
Hardee
Hendry
Hernando
Highlands
Hillsborough
Hol mes
Indian River
Jackson
Jefferson
Lafayette
Lake
Lee
Leon
Levy
Liberty
Madison
Manatee
Marion
Martin
Monroe
NassauOkaloosa
Okeechobee
Orange
Osceola
PalmBeach
Pasco
Polk
Putnam
St Johns
St Lucie
nta Rosa
Sarasota
SeminoleSumter
SuwanneeTaylor
Union
Volusia
Wakulla
WaltonWashington
Alachua
BakerBay
Bradford
Brevard
Broward
Calhoun
Charlotte
Citrus
Clay
Collier
Columbia
Dade
De Soto
Dixie
Duval
Flagler
Franklin
Gadsden
Gilchrist
Glades
Gulf
Hamilton
Hardee
Hendry
Hernando
Highlands
Hillsborough
Hol mes
Indian River
Jackson
Jefferson
Lafayette
Lake
Lee
Leon
Levy
Liberty
Madison
Manatee
Marion
Martin
Monroe
NassauOkaloosa
Okeechobee
Orange
Osceola
Pal mBeach
Pasco
Polk
Putnam
St Johns
St Lucie
Sarasota
SeminoleSumter
SuwanneeTaylor
Union
Volusia
Wakulla
WaltonWashington
Santa RosaEscambia

51
InhalationalAnthrax
CSF Gram Stain
Chest CT

52
Guarner J, et al. Pathology and pathogenesis of bioterrorism-related inhalational anthrax. AJP, 2003;163(2):701-9.

53
Inhalational Anthrax: Florida 2001
Guarner J, et al. Pathology and pathogenesis of bioterrorism-related inhalational anthrax. AJP, 2003;163(2):701-9.

54
Guarner J, et al. Pathology and pathogenesis of bioterrorism-related inhalational anthrax. AJP, 2003;163(2):701-9.

55Guarner J, et al. Pathology and pathogenesis of bioterrorism-related inhalational anthrax. AJP, 2003;163(2):701-9.

56
Shieh W-J, et al. The critical role of pathology in the investigation of bioterrorism-related cutaneous anthrax. AJP, 2003;121:26-31.

57
Index Case in New York City
• Oct 1st: Seen by Infectious Disease MD and reports handling “threat” letter at work
• Oct 3rd: Bacterial cultures of wound and Sept 25th letter test (-) for B.
anthracis• Oct 8th: Patient re-contacts DOH after
hearing of Florida anthrax case• Oct 9-11:Developed contingency plans with
NBC

58
Friday, October 12, 2001
• 12 AM: CDC reports (-) PCR on biopsy• 3 AM: CDC reports IHC + on biopsy• 6 AM: NYCDOH’s EOC activated• 9 AM: NBC informed. Start epi
investigation• 12 PM: Press conference at NBC• 3 PM: Open antibiotic distribution clinic
Index Case in New York City

59
Shieh W-J, et al. The critical role of pathology in the investigation of bioterrorism-related cutaneous anthrax. AJP, 2003;121:26-31.

60

61
When it rainsit pours….
• By the evening of October 12th, 3 additional highly suspect cutaneous cases were reported (all associated with major media outlets)
• As each case confirmed by IHC, multidisciplinary teams mobilized for on-site investigations and response

62
1. Palm Beach County – 10/3
3. Washington, DC – 10/15
2. New York City – 10/124. Trenton, NJ – 10/17
Epidemiologic Investigations of Cases
5. Oxford, CT – 11/20

63
Hamilton, NJPostal Facility
Morgan, NYCPostal Facility
West Palm, FLPostal Facility
Oct. 9 Envelopes
Sept. 18Envelopes
AMI
NBC
ABC
NY Post
CBS
State Dept, VA Mail Processing
Facility
Brentwood, DCPostal Facility
Daschle Office
Leahy Office
Hospital Worker, NYC
Elderly Woman, CT
Bookkeeper, NJ?
?
?
Cases of anthrax associated with paths of mailed envelopes and intended target sites.
Cutaneous case
Inhalational case
Intended target
Known path of mailed envelopes
Recovery site of implicated envelope
? *
Presumed or intendedpath of mailed envelopes
Mail Carrier, NJ
?
? Uncertain path of contaminated mail
Blue = Sept 18 envelopesGreen = Oct 9 envelopesOrange = Undetermined exposure to envelopes
**

64
Spider Bite
(brown recluse)

65

66

67

68

69

70

71

72
Prarie Dog (tongue)
Guarner J, et al. Pathology of monkeypox in prarie dogs: clues into transmission and pathogenesis. EID, 2004; 10(3):426-31.

73

74
Guangdong Province,
China
A
A
Hotel MHong Kong
B
J
H
Hospital 2Hong Kong
A
H
J
B
4 other Hong Kong Hospitals
C DE
Hospital 3 Hong Kong
Hospital 1 HK
Hospital 4 Hong Kong
2 family members
C D E
34 HCWs
HCW
B Germany
Bangkok
Singapore
United States
I
IL§
M§
Vietnam
K † IrelandK †
37 HCWs
HCW
0 HCWs
28 HCWs
156 close contacts of HCWs
and patients
FG †
Canada
G †F
4 family members 10 HCWs
37 close contacts
99 HCWs (includes 17 medical students)
4 HCWs*
3 HCWs
HCW
HCW
2 family members
Unknown number
close contacts
2 close contacts
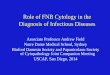
* Health-care workers; † All guests except G and K stayed on the 9th floor of the hotel. Guest G stayed on the 14th floor, and Guest K stayed on the 11th floor; § Guests L and M (spouses) were not at Hotel M during the same time as index Guest A but were at thehotel during the same times as Guests G, H, and I, who were ill during this period.
Chain of transmission among guests at Hotel M—Hong Kong, 2003
Data as of 3/28/03

75
Ksiazek TG, et al. A novel coronavirus
associated with Severe Acute Respiratory Syndrome.
NEJM, 2003; 348(20):1953-66.

76
Zaki SR, et al. Measles. In: Pathology of Infectious Diseases. Eds.
Appleton and Lange, Stamford, CT, 1997;125-136.

77

78

79

80
Ksiazek TG, et al. A novel coronavirus associated with Severe Acute Respiratory Syndrome.
NEJM, 2003; 348(20):1953-66.
SARS Coronavirus Isolate

81
Coronavirus-infected cell in
Bronchial Alveolar Lavage (BAL) of SARS
Patient
Ksiazek TG, et al. A novel coronavirus associated with Severe Acute Respiratory Syndrome.
NEJM, 2003; 348(20):1953-66.

82
Shieh W-J, et al. Immunohistochemical, in situ hybridization, and ultrastructurallocalization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan. Hum Path, 2004; (submitted).

83
Shieh W-J, et al. Immunohistochemical, in situ hybridization, and ultrastructurallocalization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan. Hum Path, 2004; (submitted).

84
SARS-CoV in Intraalveolar Fibrin
Shieh W-J, et al. Immunohistochemical, in situ hybridization, and ultrastructural localization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan. Hum Path, 2004; (submitted).

85
Hamster SARS Model
Anjeannette R, et al. SARS Coronavirus infection of Golden Syrian hamsters. J Virol, 2004; (in press).

86
2003-04 Influenza Season• Early onset
– Early reports of pediatric deaths• Increased media attention• H3N2 predominant strain• Mismatch of vaccine and circulating
strain• CDC requested reporting of influenza-
associated deaths

87
Domestic Influenza Activity – Pediatric Impact
0
1
2
3
4
5
6
7
8
9
10/11
/2003
10/18
/2003
10/25
/2003
11/1/
2003
11/8/
2003
11/15
/2003
11/22
/2003
11/29
/2003
12/6/
2003
12/13
/2003
12/20
/2003
12/27
/2003
1/3/20
041/1
0/200
41/1
7/200
41/2
4/200
41/3
1/200
42/7
/2004
Date of Death
Num
ber o
f Dea
ths
Influenza A (H3N2) Fujian-like
N = 135 deaths from 38 states

88
Signs and Symptoms (n=135)
11%14%30%37%48%59%77%Percentage
Vomiting40 Seizures19 Diarrhea15
Runny nose/congestion50 Difficulty breathing65
Sign/symptom# children
Cough80 Fever/ feverishness104
Children experienced > one symptomChildren experienced > one symptom

89

90

91
Influenza
Guarner J, et al. Immunohistochemical and in situ hybridization studiesof influenza A virus infection in human lungs. AJCP, 2000; 114:227-33.

92
Laboratory confirmation*(n=135)
• 41 (30%) Viral culture• 82 (61%) Rapid tests
– 35 (43%) were confirmed by a second method • 23 (17%) Direct Fluorescent antibody• 18 (13%) IHC staining**• 4 (3%) PCR
* Some children were tested by > 1 method* Some children were tested by > 1 method** 6 diagnosed by IHC alone** 6 diagnosed by IHC alone

93
Pandemic Influenza: The Ever Present Threat

94
Direct Interspecies Transmission of Avian Viruses to Humans Exposed to Infected Poultry
• 1997: 18 cases of human respiratory illness caused by HP avian H5N1; 6 deaths – Hong Kong
• 1998/9: 8 cases of human respiratory illness caused by H9N2; no deaths –China, HK
• 2003: 2 additional HP H5N1 cases in humans; 1 death – China, HK
• 2003: >80 cases of infection by HP H7N7 avian viruses; 1 death - ND
• 2004: 28 cases of human respiratory illness by HP H5N1 avian viruses; 20 deaths – Vietnam and Thailand

95
Summary
• Era of increased awareness of emerging and reemerging diseases
• Fundamental principle is recognition of these diseases
• Importance of multidisciplinary approach• Importance of syndromic approach• Importance of traditional laboratory and
contemporary methods• Frontline role of pathology
– Recognition of emerging infectious diseases– Guiding epidemiologic investigations– BT investigations