Embed Size (px)
Citation preview

Appendix 1
NHS South West and the Association of the British Pharmaceutical Industry Medicines Safety Partnership
Medicine Allergy Matters
Appendix 1: members of the group
Membership
NHS Chair Dr Carole Buckley GP & Prescribing Lead NHS Bristol Industry Chair
Lesley Beer Regional Business Director, Astrazeneca
Dr Jill Loader Associate Director Medicines Management
NHS South West Mike Wilcock Head of Prescribing Support Unit, Truro
Mary Monnington Director of Nursing & Patient Safety Somerset
Primary Care Trust
Sally Tomlin Chief Pharmacist, Salisbury NHS Foundation
Trust
Mark Stone Project Pharmacist, Devon Local
Pharmaceutical Committee Jo Atkinson Medical Advisor, Pfizer
Lisa Rosewarne Strategic Healthcare Development Manager,
Organon (Schering Plough)
Barnaby Poulton / Navin Joshi
Customer Marketing, MSD
Helen Morrison ABPI Outreach Facilitator
Dr Edward Kaminski Consultant Immunologist, Plymouth Hospitals
NHS Trust

Appendix 2
Focus group
Salisbury NHS Foundation Trust Salisbury District Hospital
Salisbury Wiltshire SP2 8BJ
11th June 2008 Dear , As a member of Salisbury NHS Foundation Trust you have indicated that you would be willing to get involved in certain events. I am writing to invite you to take part in a discussion group to talk about drug allergies. Salisbury NHS Foundation Trust is committed to developing services that meet the needs of the patient, the family, carer or a friend. This includes listening to what they say and giving them a chance to share their experiences or views and ideas. Holding a discussion with a number of patients, carers, professional healthcare workers and a professional facilitator has shown to be an effective way of identifying views. A leaflet has been included with this letter explaining in detail what a discussion group is. The pharmacy department is very keen to understand what people mean when they say they have an ‘allergy’ or are ‘allergic’ to something. Often patients tell us that they are allergic to a medicine because it gave them a tummy upset or a headache. This is a side effect and not an allergy and this might mean that they are not then given the best type of medicine for their condition. Sometimes too the allergies are not recorded properly in the patients’ health record and this might mean that they are then given a medicine that might put them at risk. The pharmacy department want to know how they can improve the understanding of the public about
• Exactly what an allergy is • The difference between a true allergy and a side effect • How we could develop an awareness campaign
Our plan is to hold a discussion group to discuss these things on: -
• 30th June
• 5pm
• Rooms D & E Level 5 Salisbury NHS Foundation Trust
• A light supper and refreshments will be served

Appendix 2
Please return completed forms by 23rd June 2008 A Freepost addressed envelope has been included. Should you require help with travel expenses, this includes any parking fees, please let me know, either by adding it to the return form, or phoning me. Your request for help will be held in complete confidence. Unfortunately we are unable to provide transport due to the pressure on the system for in patients and outpatient attendance. Enclosed is a map of the hospital to help you find the venue. If you have any doubts about where you are going, then please either phone me, or ask at the main reception area when you arrive. If you would like to know more about the discussion group please contact: - PALS, 0800 374208 or ext 2960, [email protected] We do hope that you will be able to join us. Yours sincerely Sally Tomlin Chief Pharmacist
Name Address 2. Telephone Number
I am able to attend the allergies group Please specify any dietary requirements for those attending I am unable to attend I will / will not need help with travel expenses. My estimated mileage will be:-
Please return completed form to: 3. PALS
Freepost (SCE14405) note no stamp required 4. Salisbury District Hospital
Salisbury SP2 8BR
Appendix 2
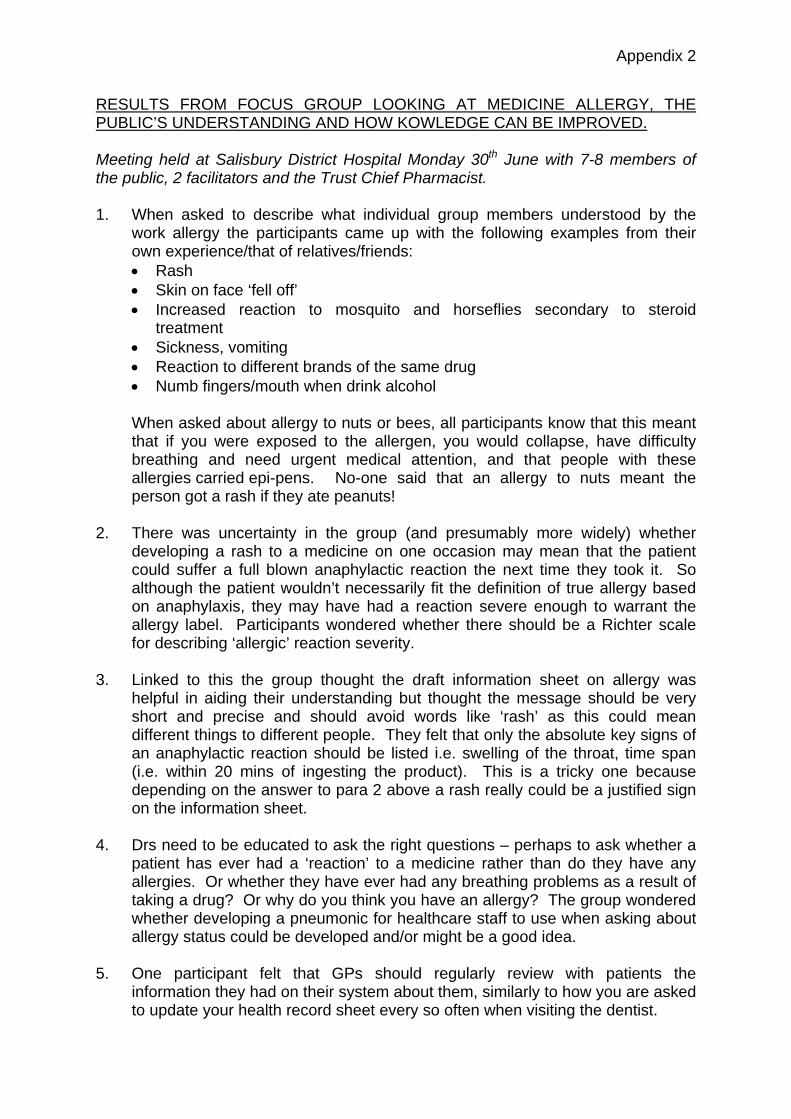
RESULTS FROM FOCUS GROUP LOOKING AT MEDICINE ALLERGY, THE PUBLIC’S UNDERSTANDING AND HOW KOWLEDGE CAN BE IMPROVED. Meeting held at Salisbury District Hospital Monday 30th June with 7-8 members of the public, 2 facilitators and the Trust Chief Pharmacist. 1. When asked to describe what individual group members understood by the
work allergy the participants came up with the following examples from their own experience/that of relatives/friends: • Rash • Skin on face ‘fell off’ • Increased reaction to mosquito and horseflies secondary to steroid
treatment • Sickness, vomiting • Reaction to different brands of the same drug • Numb fingers/mouth when drink alcohol
When asked about allergy to nuts or bees, all participants know that this meant
that if you were exposed to the allergen, you would collapse, have difficulty breathing and need urgent medical attention, and that people with these allergies carried epi-pens. No-one said that an allergy to nuts meant the person got a rash if they ate peanuts!
2. There was uncertainty in the group (and presumably more widely) whether developing a rash to a medicine on one occasion may mean that the patient could suffer a full blown anaphylactic reaction the next time they took it. So although the patient wouldn’t necessarily fit the definition of true allergy based on anaphylaxis, they may have had a reaction severe enough to warrant the allergy label. Participants wondered whether there should be a Richter scale for describing ‘allergic’ reaction severity.
3. Linked to this the group thought the draft information sheet on allergy was helpful in aiding their understanding but thought the message should be very short and precise and should avoid words like ‘rash’ as this could mean different things to different people. They felt that only the absolute key signs of an anaphylactic reaction should be listed i.e. swelling of the throat, time span (i.e. within 20 mins of ingesting the product). This is a tricky one because depending on the answer to para 2 above a rash really could be a justified sign on the information sheet.
4. Drs need to be educated to ask the right questions – perhaps to ask whether a
patient has ever had a ‘reaction’ to a medicine rather than do they have any allergies. Or whether they have ever had any breathing problems as a result of taking a drug? Or why do you think you have an allergy? The group wondered whether developing a pneumonic for healthcare staff to use when asking about allergy status could be developed and/or might be a good idea.
5. One participant felt that GPs should regularly review with patients the information they had on their system about them, similarly to how you are asked to update your health record sheet every so often when visiting the dentist.

Appendix 2
This could either be done face to face at a routine consultation or by questionnaire/email….
6. There was unanimous agreement that pharmacists should be asking patients about allergy status when the patient collects their medicines and that the pharmacist should then feed this info back to the GP.
7. Participants also wanted practice nurses, health visitors and district nurses to
be responsible for checking allergy status when interacting with patients and making sure that accurate, up to date information was held on GP systems. These staff could also promote the bracelet initiative, and perhaps carry some with them in case they find a true allergy patient who hasn’t got one.
8. Participants in the focus group liked the idea of having something like a credit
card or allergy card to show details of true allergies and what medicines this meant that the person shouldn’t be given, but had concerns about its limitation if the patient became separated from where they kept their information card.
9. They also thought the bracelets should be much better publicised, more readily available and more widely used. Apparently ‘Medic Alert’ do a whole range, including necklaces etc. The participants felt these should be issued free to patients identified as having a true allergy, by the professional identifying the allergy, i.e. the GP or hospital. So if, whilst in hospital it was discovered that you had a true allergy to penicillin, on discharge you would be given a bracelet/necklace or what ever of your choosing to take home with your take home medicines.
10. The group really liked the idea of a very simple but graphic poster aimed at the public and healthcare staff drawing on the public’s good knowledge of allergy to bees, nuts etc. The idea was something like a picture of a bee, some nuts, some shellfish and some tablets down the left hand side with arrows to a dead body! (Perhaps we were getting a bit carried away at this stage but I think with the right graphics, this type of image could get the message across).
11. In the education campaign they also thought it was important to stress the positive and negative messages of making sure you know your allergy status. Positive that it could save your life, reduce unnecessary NHS expenditure by having to revive you in ITU etc and support this with the negative message that if you have an incorrect allergy status identified you could be denied really important medicines for your condition.
12. The group suggested using national/local media to encourage the public to stop using the word ‘allergy’ so much and to use it in a more precise way and to get a better understanding of side effects vs. intolerance vs. allergy.
13. Examples of media outlets to publicise the message included local radio stations, local TV news programmes, local press plus national publications like Woman’s Weekly etc. Posters in hospitals, GP surgeries and dentists were good but the group felt that people only go there when they are ill and to spread the message to a wider public the posters should also be displayed in libraries
Appendix 2
and similar venues.
14. Village newsletters, WI speakers circuit, Boots/Tesco’s newsletters could also be useful sources to disseminate the message. The group also liked the idea of having the allergy status printed on the repeat prescription side of the prescription form.
15. All participants said that they would like to have feedback on what ever actions came out of the work being done on this by the SW/ABPI group and had been pleased to be part of the discussion if it meant that our work could save someone’s life.
Sally Tomlin Chief Pharmacist 8.7.08 With thanks to Maggie Cherry and Katrina Brockbank for their help in organising and facilitating this meeting.

Appendix 3
ABPI/SW SHA Medicines Allergy Project – Review of Technology use in Allergic Status Recording in Primary Care Settings.
Introduction A joint working initiative between the Association of the British Pharmaceutical Industry (ABPI) and the South West Strategic Health Authority identified a number of projects where the combined inputs of both parties could have significant impact on patient care. One work stream has been to design, implement and evaluate a joint working project that specifically addresses the documentation of patients’ medicines allergy status and delivers against the following recommendations, that healthcare organisations should:
1. Audit the frequency of incidents involving medicine allergy and the extent to which allergy status is documented;
2. Ensure all electronic prescribing and dispensing systems include a record of the patient’s medicine allergy status;
3. Consider the use of an allergy wristband to alert healthcare staff to the allergy status of the patient;
4. Develop local systems to alert staff to products containing penicillin.
5. To utilise the learning from this project and ensure implementation across all health care settings and disciplines in the South West and shared nationally to improve practice and raise awareness with regard to a boarder range of drug allergies.
6. To demonstrate the benefits of joint working between the NHS and the pharmaceutical industry to all stake holders involved in this project and communicate its success to appropriate parties.
As a review of the recording of drug allergy (as opposed to adverse reactions) in medical records in the South West, a number of routes of investigation were pursued including with GPs and with PRIMIS+ (part of Connecting For Health) to understand the role of the IT systems in the recording and display of information about allergic status. Allergies recording in the South West Data on Allergies is audited by Practices and PCTs to fulfil the IM and T DES requirements if signed up to. The data (for payment to be triggered) must then be uploaded to the PRIMIS+ CHART tool. Data are then available to Practice and PCT on allergy recording. These data are available by disease area drug allergy recording (eg musculoskeletal, CVD) as well as specifically penicillin. Reviewing at Penicillin recording, it is easy to see significant variation within and between PCTs in the South West in the quality of data recorded. There are also contrasting amounts of variation, Cornwall PCT for example showed a larger variation of GP practice allergy recording than other PCTs. Variation in Allergy recording appears to be due to the following:

Appendix 3
1. GP Systems methodologies for recording allergy data Each system has a unique way of recording allergic status to drugs. This varies in terms of screens used, clicks needed, windows based systems vs DOS etc. There is often confusion and errors in mixing allergy data recording with other ADRs or contraindications for a given drug. There is also the option to record 'Moderate' or 'Severe' allergy in eg Vision systems.
2. GP systems data structures Each GP clinical systems has different database structures which record allergy information in different ways. This can be as tags to individual prescriptions; the option to tag entire classes of drugs (eg in EMIS); linking of allergy Read codes to Prescriptions or recording allergies using proprietary codes. The Read code dictionary does not provide the option for 'Allergy to drug X…' Read codes except for a very few specific examples eg penicillin. It is for this reason that it is very difficult to interrogate GP system data for allergies using anything other than the systems suppliers own audit tools.
3. How the individual clinical systems utilise allergic status information in decision support.
Allergic Status to a given drug in GP systems provides users with prompts should the drug in question be prescribed again. Some users however utilise the 'allergic status' alert to prompt on a previous adverse (but maybe non-allergic) event. This is evident in at least one GP clinical system meaning that false positives may be commonplace.
4. Accuracy data-transfer from GP to other healthcare providers Transfer of clinical data from one system to another is problematic when the data is not a simple Read code. The linking of drug Read code to allergic status or other flag mechanism for allergy is thus output as simple text. It is then the responsibility of the receiving healthcare provider to re-enter the data into the new system utilising their own mechanism for allergy data recording. This of course is also dependant on the quality of the data from the originating practice (see 1-3 above) as well as the skills of the data recorder. This also will apply to migration of data from prior versions of Coding systems to SNOMED within practice or from practice to other provider. PRIMIS+ offers training for primary care facilitators covering these areas and as part of our recommendations for the SW SHA project we are intending to make fuller usage of this service. Not all PCTs have data quality/similar facilitators. They have until recently perhaps been regarded as 'nice to have'. These facilitators often end up not utilising their PRIMIS+ trained expertise, ie undertaking clinically focussed change management in data recording. Instead they spend time supporting practices with hardware/software issues.

Appendix 3
The Summary Care and Healthspace Record Readiness policy document (launched April 08) has driven increased interest in PCTs employing these individuals. There is a need there-in to record the presence of a data quality facilitator. Recommendations to take forward in the South West SHA
1. Ensure all PCTs Information officers are aware of the PRIMIS+ resource available to them – both the information available from CHART and the training.
2. Local IT facilitators (job titles vary) to receive briefing on the project to ensure they understand it's objectives and how they can impact on its success.
3. SHA to flag project to PCTs to cascade to facilitators' line managers the importance of this project and to allow time within facilitators objectives
4. Facilitators to highlight project in every practice contact, leaving briefing materials and ensuring practices are aware of the resource they provide (remembering that as part of the IM and T DES they must have processes in place for allergy recording) as well as awareness of the overall project
5. Briefing to go to Senior partner and Practice Manager re project and awareness of resource (on agreement with local PCT?)
6. Chris Brown – regional PRIMIS coordinator is happy to meet/brief SHA/PCTs on resource and how this could be used
7. PRIMIS+ happy to be involved in any events related to the project where they can provide support
8. Engage with GP system user groups to highlight the Allergy project and ensure the subject is on the agenda to cover at all user group meetings (Target EMIS, Vision, Microtest in the South West as the predominant suppliers).

Appendix 4
Patient education (provide allergy leaflet) +/- GP communication if believe that GP record is incorrect
yes no
What symptoms did you experience?
Does not include symptoms
associated with true allergy
Issue allergy pack - card and leafletDear Dr letterUpdate PMR
Query immediately with prescriber if appropriate eg suspect penicillin allergy yet patient has “penicillin”
prescription
Nettle rash, hives or any other rash, swelling of the mouth, tongue or throat difficulty breathing, swallowing or speaking, wheezing or asthma attack.
Every prescription for an antibiotic OR patient asks
opportunistically
Have you ever had a problem with penicillin?
Counsel patient re effective medicine taking eg finish course, empty stomach
Community Pharmacist Flowchart for Pilot of Community Pharmacist Flowchart for Pilot of Medicine Allergy Matters ProjectMedicine Allergy Matters Project

Appendix 5
Allergy Project Evaluating the impact of community pharmacists on patient knowledge about allergy Interim report The community pharmacist at OSS Bristol agreed to talk to patients about drug allergies when they presented to the pharmacy to collect dispensed medication. Between 2-4 weeks after completion of the forms the clinical pharmacist in OSS contacted the patients to review the initial consultations. See the attached encounter sheet for details. The study was started on 4th August 2008 and this interim evaluation took place 4 weeks later. Results Forms completed – 9 Follow up phone call – 7 (there had not been 2 weeks between the completion of the CP form and the evaluation for the last two phone calls)
1. Female 23/02/40. Reported allergy to penicillin. Confirmed by CP, not on pharmacy clinical system. Patient had full recall of conversation and the allergy was recorded on the practice system. Allergy status added to pharmacy records
2. Female 29/08/78. Reported allergy to cream. CP identified NOT allergy. No allergy recorded on practice system and patient confirmed recall of conversation. Patient reassured not allergic to Trimovate
3. Male 19/11/78. Patient identified allergy to Ibuprofen (as trade name), not confirmed by CP and patient has had Ibuprofen since. Patient described an allergic reaction but CP unable to identify drug. No allergies identified on practice system
4. Female 17/12/52. Patient and CP identified no allergies but practice system identified allergies to Fluoxetine, Erythromycin and codeine phosphate. Telephone number unavailable. Alert on practice system to discuss with patient at next appointment.
5. Female 28/05/80. No allergies identified by patient, CP or practice. 6. Female 18/07/78. Patient reported an allergy to an antibiotic in childhood. CP confirmed has
had common antibiotics since and allergy unlikely. No recorded allergy on practice system 7. Female 11/10/80. Patient identified allergy to Diclofenac, CP felt this was an ADR. No
recorded allergies on practice system. Number unobtainable. Note on clinical system to discuss at next appointment and get an up to date phone number.
Discussion The CP reports that it is time consuming to have a discussion with the patient about allergy, hence the small numbers. The CP involved is not doing MUR’s. However there was significant information in four out of seven completed cases. It is also clear that there is confusion about allergy to medicines among patients.

Appendix 5
Conclusion The impression of the staff taking part is that community pharmacy is ideally placed to offer advice about allergy to medicines and to disseminate that information to the patients and practice. However it is a time consuming exercise and the impact on pharmacy needs more evaluation. The issue of finance also needs to be addressed in a commercial organisation CB 7/09/08
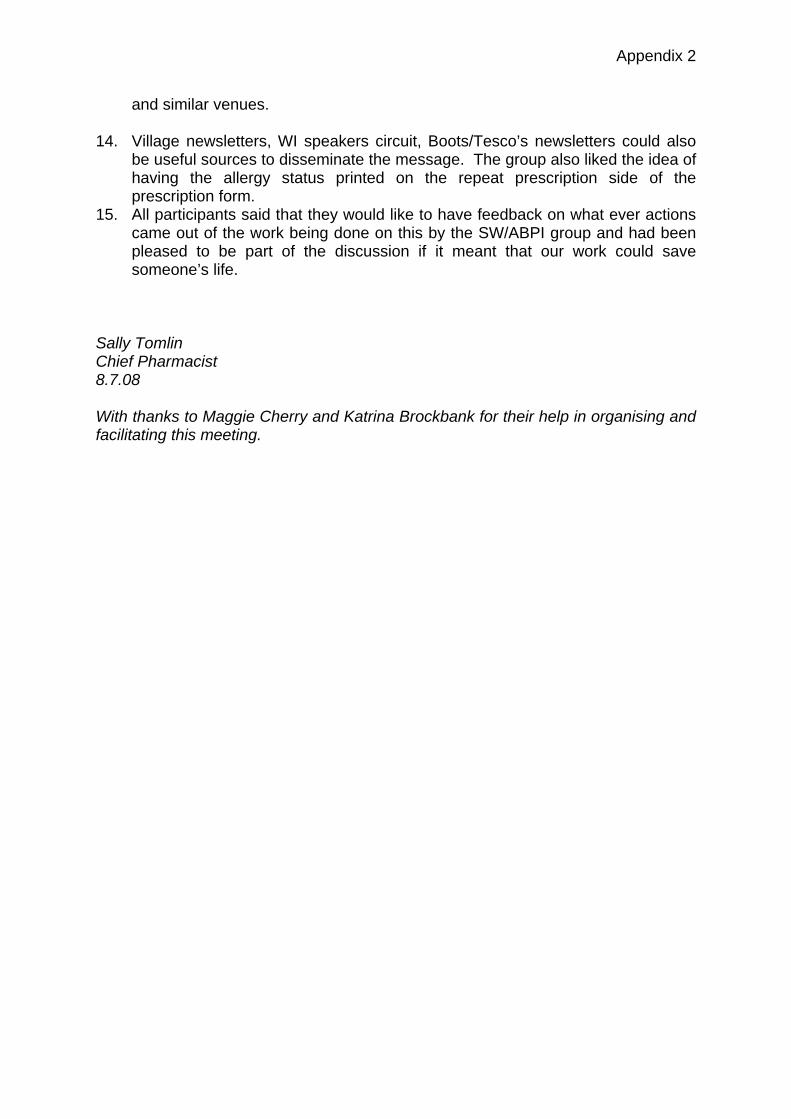
Appendix 5
THE OLD SCHOOL SURGERY ALLERGY PROJECT
DATA COLLECTION SHEET
Patient Name: ……………………………………………. Dob: ……………………………………………. Date: ..................................................................... 1. Does the patient report a drug allergy: Yes/No Medicine…………… 2. Community Pharmacist confirmed allergy: Yes/No Medicine…………… 3. Community Pharmacy clinical system has allergy alert: Yes/No Medicine…………… 4. Community Pharmacist identified
discrepancy: Yes/No Medicine…………… Comments: Follow-up Phone Call: Date: ……………………………………… 1. Do you remember talking to the Community Pharmacist
about your drug allergy? Yes/No
2. Did you identify any medicines that you were allergic to? Yes/No If yes, please state Medicine ……………….. ………………… ……………… 3. Were there any medicines that you thought you were allergic to that the CP thinks are not allergies? Yes/No If yes, please state Medicine ……………….. ………………… ……………… CB/sjj July 2008

Appendix 6
SOUTH WEST MEDICINES SAFETY PARTNERSHIP
ABPI and SW Health Authority
Allergy Project
Community Pharmacy Pilot
The project aim was to raise the profile of medicine allergies in the general public. The project team saw community pharmacy as a key communication point to inform members of the public. It was decided that pharmacists would actively consult members of the public who presented antibiotic prescriptions to be dispensed and consult any patients asking for ad hoc advice on antibiotics.
The consultation included a number of questions which tried to elicit whether the patient’s allergy was likely to be a ‘true allergy’ and provided general information on medicines allergies supported by the written information pack.
The Plymouth Pilot
The community pharmacy pilot of the medicines allergy matters campaign took place in Devonport Pharmacy, Plymouth and in “a” community pharmacy in Cornwall. The Plymouth pilot took place over a two week time period.
Plymouth Pharmacy Results
Number of Patients
Encountered
Number of patients with suspected true medicines allergy
Allergy Information
Material Issued
Verbal Advice Given on
Medicines Allergy
Patients Allergy Status Confirmed With Doctors PMR
19 2 18 18 2
The results indicated that there are a significant number of people who visit a pharmacy who have suspected medicines allergy. This high proportion of allergic patients probably occurred because of the prior selection that was taking place, as we were only targeting patients who were dispensed antibiotics in a pharmacy. Another factor to note was that these patients were only suspected of having an allergy and their status was not tested.
Patients gave positive feedback about the verbal advice and about the allergy information pack which was provided. The patients’ with a suspected allergy felt the allergy status card which was given was very useful and indicated they would carry on their person.

Appendix 6
Lessons Learned From Pilot
The pilot uncovered a few shortcomings of the community pharmacy campaign. Firstly the encounter sheet used by the pharmacist had some irrelevant information when fully considering the aims of the project, the columns ‘Drug allergy material issued’ and ‘verbal advice given’ could have been merged. The column patient encounter initiated by was probably unnecessary.
Secondly we recorded whether the advice and information pack was issued to the patient but not whether the patient felt that the advice provided was helpfully in improving their understanding of medicine allergies, this being the aim of the project.
Lastly the pharmacist was required to send a letter to the patients G.P. to confirm the allergy status, this letter was not required to be followed up by contacting the G.P. However in the Plymouth pilot the pharmacist contacted the G.P. directly by telephone to confirm the allergy status stated on the patient’s record. On the two occasions where a suspected allergy patient was encountered the G.P.s records were confirmed as being correct for both patients. A recommendation would be that for future campaigns the pharmacist would be required to contact the G.P. by telephone and there would be a column in the encounter sheet to state whether the patient records were correct.

Appendix 7
Pharmacy Intervention Record: Penicillin Allergic Patient Encounter Data Collation Sheet
Background: Penicillin hypersensitivity occurs in approximately 0.18% of patients. A true allergic reaction is rare but can be fatal, about 1-5 per 10,000 of courses administered
cause such a reaction. Instructions: 1) Check all patients presenting with a prescription for an antibiotic. ALSO use if patient opportunistically asks you about antibiotic allergy 2) Fill in the
data collection sheet below 3) Send Dear Doctor letter if necessary If yes, what
symptoms did you
experience: Patient No./ PMR
I.D. /
Initials
Patient encounte
r initiated
by: Pharmac
ist or other (e.g.
poster, word of mouth)
Are symptoms a
true indication of an allergy?
Drug allergy
material issued?
If true allergy, ALSO
complete next column
Verbal advice given from
support leaflet?
Patient's
verbal conse
nt requested to
share information with G.P.
Dear Doctor
letter sent to G.P. to confirm details?
Pharmacy's PMR
details updated
for patient?
Answer/Tick
Pharmaci
st Other Y N
Unsure Y N Y N Y / N Y N Y
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21

Appendix 7
Appendix 7

Appendix 7

Appendix 7

Appendix 7

Appendix 7
Appendix 7