Embed Size (px)
Citation preview

APPENDIXAPPENDIXJames Taclin C. Banez, MD, James Taclin C. Banez, MD,
FPSGS,FPCSFPSGS,FPCS

Anatomy / Anatomy / FunctionFunction
Location, positionLocation, position Function:Function:
Immunologic Immunologic organorgan
Secrets IgA, Secrets IgA, component of the component of the GUT associated GUT associated lymphoid tissue lymphoid tissue (GALT)(GALT)
Not essential; it’s Not essential; it’s removal ----> (-) removal ----> (-) sepsissepsis

Appendiceal Conditions of Appendiceal Conditions of Surgical ImportanceSurgical Importance
Appendicitis:Appendicitis: Inflammation of the appendixInflammation of the appendix 1500 – perityphlitis – inflammation of the 1500 – perityphlitis – inflammation of the
cecal regioncecal region Most common acute surgical disease of the Most common acute surgical disease of the
abdomenabdomen Peak ----> puberty / early adulthoodPeak ----> puberty / early adulthood Male > female (1.3 : 1)Male > female (1.3 : 1)

AppendicitisAppendicitisPathogenesis:Pathogenesis:
Obstruction Obstruction (dominant causal factor)(dominant causal factor)
1.1. Fecalith – usual causeFecalith – usual cause
2.2. Hypertrophy of the lymphoid tissueHypertrophy of the lymphoid tissue
3.3. Inspissated bariumInspissated barium
4.4. Vegetable and fruit seedsVegetable and fruit seeds
5.5. Intestinal worms (Ascaris)Intestinal worms (Ascaris)
6.6. TumorTumor

AppendicitisAppendicitisPathogenesis:Pathogenesis:
Sequence of events in Sequence of events in Luminal Luminal ObstructionObstruction
Proximal occlusion ---> Closed loop Obst. Proximal occlusion ---> Closed loop Obst. -------- ---> rapid distention due to:---> rapid distention due to:
a.a. Continuing secretion of the mucosaContinuing secretion of the mucosa
b.b. Rapid multiplication of normal floraRapid multiplication of normal flora
---> elevate pressure ---> capillary/venous ---> elevate pressure ---> capillary/venous occlusion (occlusion (CONGESTION CONGESTION 11stst stage): stage):S/Sx: (+) visceral afferent pain fibers (vague, dull, S/Sx: (+) visceral afferent pain fibers (vague, dull, diffuse pain in mid-abdomen or lower epigastrium. diffuse pain in mid-abdomen or lower epigastrium. Increase peristalsis (crampy pain); N/V and Increase peristalsis (crampy pain); N/V and anorexia anorexia

AppendicitisAppendicitisPathogenesisPathogenesis
Inflammatory process involves the serosa of Inflammatory process involves the serosa of appendix and in turns parietal peritoneum in appendix and in turns parietal peritoneum in the region.the region.
Infiltration of PMN (Infiltration of PMN (SUPPURATIVESUPPURATIVE 2 2ndnd stage) stage) Damage of the lining epithelium ---> entrance of Damage of the lining epithelium ---> entrance of
bacteria to the wall.bacteria to the wall. Impairment of blood supply (inc. pressure Impairment of blood supply (inc. pressure
than arterial pressure)---> ellipsoidal infarct than arterial pressure)---> ellipsoidal infarct at antimesenteric border near the tip. at antimesenteric border near the tip. ((GANGRENOUSGANGRENOUS 3 3rdrd stage) ---> stage) ---> ((PERFORATIONPERFORATION 4 4thth stage) stage)
This process is not inevitable. Some subside This process is not inevitable. Some subside spontaneouslyspontaneously

AppendicitisAppendicitis
Pathogens:Pathogens: Anaerobes, aerobesAnaerobes, aerobes Bacteroides fragilis, Bacteroides fragilis,
Escherichia coli, Escherichia coli, Peptostreptococcus, Peptostreptococcus, Pseudomonas, Bacteroides Pseudomonas, Bacteroides splanchnicus, Lactobacillussplanchnicus, Lactobacillus

AppendicitisAppendicitisClinical Manifestation:Clinical Manifestation:
1.1. Abdominal pain:Abdominal pain: Classic pain sequence ……….Classic pain sequence ………. Right lower quadrant painRight lower quadrant pain Others:Others:
Left lower quadrant pain (long appendix)Left lower quadrant pain (long appendix) Flank or back pain (retro-cecal)Flank or back pain (retro-cecal) Supra-pubic (pelvic)Supra-pubic (pelvic) Testicular pain (retro-ileal ----> irritates the Testicular pain (retro-ileal ----> irritates the
spermatic artery and ureterspermatic artery and ureter
2.2. Anorexia: nearly always presentAnorexia: nearly always present
3.3. Vomiting 75%Vomiting 75%
4.4. Obstipation / diarrheaObstipation / diarrhea Usual sequence (95%) : Usual sequence (95%) : ANOREXIA ---> ABD. ANOREXIA ---> ABD.
PAIN ---> VOMITINGPAIN ---> VOMITING

AppendicitisAppendicitisSigns: Signs: PE depends on the location of the PE depends on the location of the
appendix and presence of rupture appendix and presence of rupture
1.1. Direct and rebound tenderness at Mc Direct and rebound tenderness at Mc Burney’s point. ROVSING sign ---> Burney’s point. ROVSING sign ---> indicate muscles peritoneal irritation.indicate muscles peritoneal irritation.
2.2. Involuntary muscle guarding (true reflex Involuntary muscle guarding (true reflex rigidity).rigidity).
3.3. Psoas / Obturator signs ---> retrocecal Psoas / Obturator signs ---> retrocecal appendixappendix
4.4. Para-rectal tendernessPara-rectal tendernessStages I & II – uncomplicated Stages I & II – uncomplicated
Stages III & IV – complicatedStages III & IV – complicated

AppendicitisAppendicitisLaboratory Findings:Laboratory Findings:
1.1. WBC: leucocytosis WBC: leucocytosis
simple = 10,000 to simple = 10,000 to 18,000/mm318,000/mm3
perforated = >18,000/mm3perforated = >18,000/mm3
2.2. Urinalysis :Urinalysis : Hematuria and pyuria due to irritation of Hematuria and pyuria due to irritation of
the ureter and urinary bladderthe ureter and urinary bladder w/o bacteriuriaw/o bacteriuria
3.3. FPA: rarely helpful; (+) fecalith – rare, FPA: rarely helpful; (+) fecalith – rare,
highly suggestive of the dx.highly suggestive of the dx.

AppendicitisAppendicitis4.4. Graded Compression Graded Compression
sonogram:sonogram: 78–96% sensitivity; 78–96% sensitivity;
85–98% specificity85–98% specificity (+) non-compressible (+) non-compressible
appendix, 6mm or > appendix, 6mm or > at AP viewat AP view
(-) easily compressible (-) easily compressible 5mm; not visualized a 5mm; not visualized a & (-) pericecal fluid or & (-) pericecal fluid or massmass
False (-):False (-):
a.a. Appendicitis Appendicitis confined at the tipconfined at the tip
b.b. Retrocecal positionRetrocecal position
c.c. Perforated Perforated appendixappendix
False (+):False (+):
a.a. Periappendicitis from Periappendicitis from surrounding inflammationsurrounding inflammation
b.b. Dilated fallopian tubeDilated fallopian tube
c.c. Inspissated stool can Inspissated stool can mimic an appendicitismimic an appendicitis
d.d. Obese pt., appendix not Obese pt., appendix not compressedcompressed

AppendicitisAppendicitis
5.5. CT scan:CT scan: Shd. not delay or Shd. not delay or
substitute for substitute for prompt operative prompt operative intervention when intervention when clinically indicatedclinically indicated
Used primarily for Used primarily for percutaneous percutaneous drainagedrainage
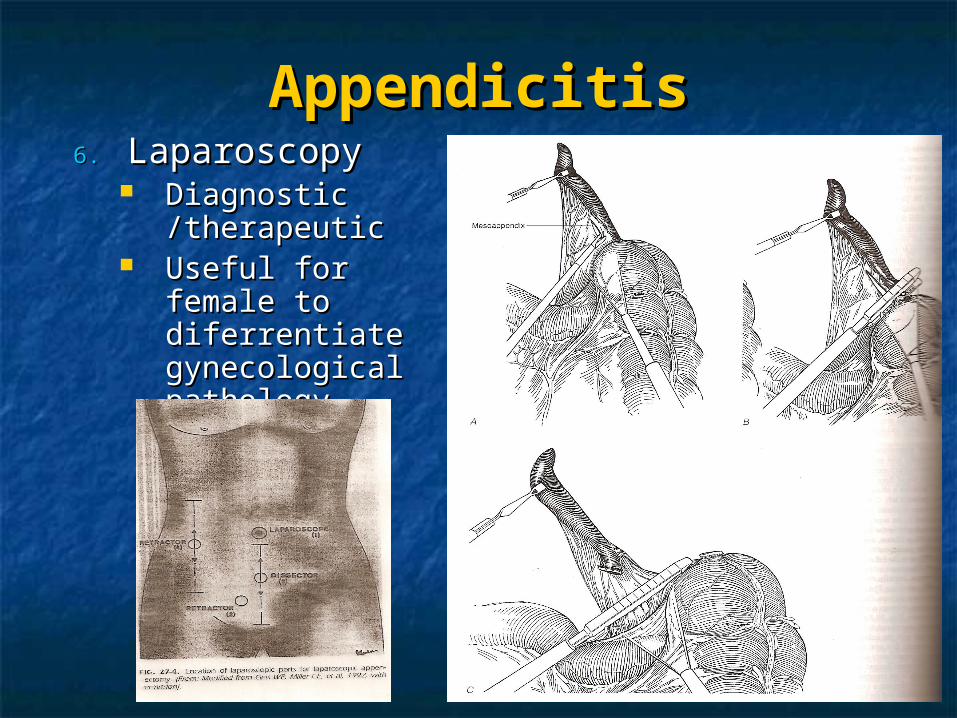
AppendicitisAppendicitis6.6. Laparoscopy Laparoscopy
Diagnostic Diagnostic /therapeutic/therapeutic
Useful for female Useful for female to diferrentiate to diferrentiate gynecological gynecological pathologypathology

Appendiceal Rupture:Appendiceal Rupture: Increase morbidity / mortalityIncrease morbidity / mortality No accurate way to determine the occurrence No accurate way to determine the occurrence
of ruptureof rupture Suspected:Suspected:
1.1. Fever > 39 CFever > 39 C
2.2. WBC of > 18,000/mm3WBC of > 18,000/mm3
3.3. Localized rebound, involuntary muscle Localized rebound, involuntary muscle guardingguarding
4.4. Signs of genralized peritonitisSigns of genralized peritonitis
5.5. Ill defined mass (PHLEGMON – motted loops Ill defined mass (PHLEGMON – motted loops of bowel adherent to the inflamed appendix)of bowel adherent to the inflamed appendix)

Differential Diagnosis:Differential Diagnosis: Most common erroneous pre-op diagnosis:Most common erroneous pre-op diagnosis:
Acute mesenteric lymphaditisAcute mesenteric lymphaditis No organic pathologic conditionNo organic pathologic condition Acute pelvic pathologic conditionAcute pelvic pathologic condition Twisted ovarian cyst / ruptured graafian Twisted ovarian cyst / ruptured graafian
folliclefollicle Acute gastroenteritisAcute gastroenteritis
1.1. Acute mesenteric adenitis:Acute mesenteric adenitis: w/ present or recent URTIw/ present or recent URTI Diffuse pain, tenderness not sharp, (-) rigidityDiffuse pain, tenderness not sharp, (-) rigidity Self limited -----> observeSelf limited -----> observe

Differential Diagnosis:Differential Diagnosis:2.2. Acute gastroenteritis:Acute gastroenteritis:
Childhood, viral gastroenteritisChildhood, viral gastroenteritis Chills, fever, profuse watery diarrhea, N/VChills, fever, profuse watery diarrhea, N/V Hyper-peristaltic abdominal cramps w/o localizing Hyper-peristaltic abdominal cramps w/o localizing
signsign
3.3. Disease of the male:Disease of the male: Torsion of the testes and acute epididymitisTorsion of the testes and acute epididymitis Diagnosed by palpating the enlarged tender Diagnosed by palpating the enlarged tender
seminal vesicleseminal vesicle
4.4. Meckel’s diverticulitis:Meckel’s diverticulitis: Same clinical picture w/ APSame clinical picture w/ AP Associated w/ same complication of AP, hence Associated w/ same complication of AP, hence
needs prompt surgical intervention.needs prompt surgical intervention.

Differential Diagnosis:Differential Diagnosis:5.5. Intussusceptions:Intussusceptions:
Shd. Be differentiated pre-operatively due to Shd. Be differentiated pre-operatively due to different management.different management.
Char:Char:
a.a. Common under 2 y/oCommon under 2 y/o
b.b. Occur in well nourished infant who Occur in well nourished infant who suddenly doubled up due to colicky pain. suddenly doubled up due to colicky pain. Hrs. later pass out bloody mucoid stoolHrs. later pass out bloody mucoid stool
c.c. Sausage shape mass in the RLQSausage shape mass in the RLQ
6.6. Regional enteritis (Crohn’s dse):Regional enteritis (Crohn’s dse): s/sx is almost the same w/ AP this is dx. in s/sx is almost the same w/ AP this is dx. in
celiotomyceliotomy

Differential Diagnosis:Differential Diagnosis:7.7. UTI / Ureteral stone:UTI / Ureteral stone:
Referred pain to the labia, scroyum or penisReferred pain to the labia, scroyum or penis Chills, fever (+) R costo-vertebral angle Chills, fever (+) R costo-vertebral angle
tenderness, hematuria, leucocytosistenderness, hematuria, leucocytosis Dx: -----> pyelographyDx: -----> pyelography
8.8. Gynecological disorders:Gynecological disorders: Rate of erroneous diagnosis of AP is highest Rate of erroneous diagnosis of AP is highest
in young adult femalein young adult female Order of frequency:Order of frequency:
PID -----> ruptured grafian follicle ----> twistd PID -----> ruptured grafian follicle ----> twistd ovarian cyst or tumor -----> endometriosis -----> ovarian cyst or tumor -----> endometriosis -----> ruptured ectopic pregnancyruptured ectopic pregnancy
TREATMENTTREATMENT Adequate hydration, correct electrolyte Adequate hydration, correct electrolyte
imbalanceimbalance Manage other medical problemsManage other medical problems Pre-operative antibiotics:Pre-operative antibiotics:
Simple AP - hrs antibioticSimple AP - hrs antibiotic Ruptured AP - antibiotic until feverRuptured AP - antibiotic until fever Peritonitis - 10 days antibioticsPeritonitis - 10 days antibiotics
Surgery:Surgery:1.1. Open appendectomy:Open appendectomy:
McBurney (oblique); Rocky Davis McBurney (oblique); Rocky Davis (transverse);(transverse);right paramedian; midline incision right paramedian; midline incision

Open Appendectomy:Open Appendectomy:

TREATMENTTREATMENT2.2. Laparoscopy:Laparoscopy:

TREATMENTTREATMENT Phlegmon and small abscesses can be Phlegmon and small abscesses can be
treated conservatively w/ IV antibiotictreated conservatively w/ IV antibiotic Well localized abscess ---> percutaneous Well localized abscess ---> percutaneous
drainagedrainage Complex abscess ---> surgical drainageComplex abscess ---> surgical drainage Interval appendectomy – 6 wks. Interval appendectomy – 6 wks.
Following an acute event treated either Following an acute event treated either non-operatively or w/ simple drainage of non-operatively or w/ simple drainage of an abscess. an abscess.
0-37% recurrent appendicitis0-37% recurrent appendicitis

PROGNOSISPROGNOSISMortality:Mortality:
9.9% -------> 0.2%9.9% -------> 0.2% Factors:Factors:
1.1. Ruptured prior to surgeryRuptured prior to surgery Simple - 0.06% Simple - 0.06% Ruptured - 3%Ruptured - 3%
2.2. Age of pt.:Age of pt.: Ruptured - 15%Ruptured - 15%
Death due to:Death due to:1.1. Uncontrolled sepsis (peritonitis, intra-Uncontrolled sepsis (peritonitis, intra-
abdominal abscess, gm (-) septicemia.abdominal abscess, gm (-) septicemia.2.2. Cardiac / pulmonary insufficiency (elderly)Cardiac / pulmonary insufficiency (elderly)3.3. Pulmonary embolismPulmonary embolism4.4. aspirationaspiration

PROGNOSISPROGNOSISMorbidity:Morbidity:
Simple - 3%Simple - 3% Ruptured - 47%Ruptured - 47% Early:Early:
1.1. Septic :Septic :
a.a. Wound infection / abscessWound infection / abscess
b.b. Intra-abdominal abscess (appendiceal Intra-abdominal abscess (appendiceal fossa, pouch of Douglas, sub-hepatic fossa, pouch of Douglas, sub-hepatic space, multiple intestinal loops.space, multiple intestinal loops.
2.2. Fecal fistula:Fecal fistula:
3.3. Wound dehiscenceWound dehiscence
4.4. Intestinal obstruction: due to locculated Intestinal obstruction: due to locculated abscess & exuberant adhesive formationabscess & exuberant adhesive formation

PROGNOSISPROGNOSIS
Morbidity:Morbidity: Late:Late:
1.1. Adhesived bandsAdhesived bands
2.2. Inguinal hernia (3x greater in pt. who had Inguinal hernia (3x greater in pt. who had appendectomy)appendectomy)
3.3. Incisional hernia (paramedian / midline Incisional hernia (paramedian / midline incision) incision)

Appendicitis in the Appendicitis in the YoungYoung
Difficult to establish diagnosis:Difficult to establish diagnosis:1.1. Inability of a child to give accurate historyInability of a child to give accurate history
2.2. Diagnostic delays by both parents & Diagnostic delays by both parents & physiciansphysicians
Rapid progression to rupture:Rapid progression to rupture: Underdeveloped greater omentum ----> Underdeveloped greater omentum ---->
higher morbidityhigher morbidity < 8y/o had a twofold increase rate of < 8y/o had a twofold increase rate of
perforation as compared to older childrenperforation as compared to older children

Appendicitis during Appendicitis during PregnancyPregnancy
AP is the most frequent extra-uterine dse. AP is the most frequent extra-uterine dse. requiring surgical Tx during pregnancyrequiring surgical Tx during pregnancy
Most frequent during the 1Most frequent during the 1stst & 2 & 2ndnd trimesterstrimesters
S/Sx:S/Sx: Abdominal pain, tendernessAbdominal pain, tenderness Rebound tenderness and guarding less due to Rebound tenderness and guarding less due to
laxity of abdominal walllaxity of abdominal wall Increase WBC; abdominal ultrasoundIncrease WBC; abdominal ultrasound Dx is difficult due to displacement of the Dx is difficult due to displacement of the
appendixappendix

Appendicitis during Appendicitis during PregnancyPregnancy
Dx is difficult due to displacement of the Dx is difficult due to displacement of the appendixappendix

Appendicitis during Appendicitis during PregnancyPregnancy
Risk of surgery:Risk of surgery: Premature labor - 10-15% both for negative Premature labor - 10-15% both for negative
laparotomy and appendectomy for laparotomy and appendectomy for uncomplicated APuncomplicated AP
Appendiceal perforation is significant factor Appendiceal perforation is significant factor associated w/ fetal and maternal death.associated w/ fetal and maternal death.
Fetal mortality - 3-5% w/ early Fetal mortality - 3-5% w/ early appendicitisappendicitis
20% perforation20% perforation Suspicion of appendicitis during Suspicion of appendicitis during
pregnancy shd prompt rapid diagnosis pregnancy shd prompt rapid diagnosis and surgical interventionand surgical intervention

Tumors of the AppendixTumors of the Appendix Appendiceal malignancy is rareAppendiceal malignancy is rare Discovered during laparotomy or in association Discovered during laparotomy or in association
w/ acute inflammation of the appendixw/ acute inflammation of the appendix
1.1. CARCINOID:CARCINOID: Firm, yellow, bulbar mass in the appendixFirm, yellow, bulbar mass in the appendix Located: appendix ---> small bowel ----> rectumLocated: appendix ---> small bowel ----> rectum Carcinoid syndrome is rare in appendiceal carcinoid Carcinoid syndrome is rare in appendiceal carcinoid
unless widespread metastases are presentunless widespread metastases are present Malignant potential related to it’s SIZE ---> > 2cmMalignant potential related to it’s SIZE ---> > 2cm Treatment:Treatment: < 2cm appendectomy< 2cm appendectomy
> 2cm right hemicolectomy> 2cm right hemicolectomy

Tumors of the AppendixTumors of the Appendix2.2. ADENOCARCINOMA:ADENOCARCINOMA:
RareRare Histologic type:Histologic type:
a.a. Mucinous adenocarcinomaMucinous adenocarcinoma
b.b. Colonic adenocarcinomaColonic adenocarcinoma
c.c. AdenocarcinoidAdenocarcinoid Manifestation:Manifestation:
a.a. Acute appendicitisAcute appendicitis
b.b. RLQ massRLQ mass Treatment: right hemicolectomyTreatment: right hemicolectomy Prognosis:Prognosis:
55% ----> 5yr. survival55% ----> 5yr. survival

Tumors of the AppendixTumors of the Appendix3.3. MUCOCELE:MUCOCELE:
Progressive enlargement of the appendix from Progressive enlargement of the appendix from the intraluminal accumulation of a mucoid the intraluminal accumulation of a mucoid substancesubstance
Histologic type:Histologic type:
a.a. Retention cystRetention cyst
b.b. Mucosal hyperplasiaMucosal hyperplasia
c.c. CystadenomasCystadenomas
d.d. CystadenocarcinomaCystadenocarcinoma Rarely occurs w/ gelatinous ascites Rarely occurs w/ gelatinous ascites
(Pseudomyxoma Peritonei) usually associated (Pseudomyxoma Peritonei) usually associated w/ malignant ovarian or appendiceal mucinous w/ malignant ovarian or appendiceal mucinous CA. if present survival is decreasedCA. if present survival is decreased

Tumors of the AppendixTumors of the Appendix3.3. MUCOCELE:MUCOCELE:
Treatment:Treatment: Benign - appendectomyBenign - appendectomy Malignant - right hemicolectomy for Malignant - right hemicolectomy for
cystadenoCA of the appendix; THABSO and cystadenoCA of the appendix; THABSO and appendectomy for ovarian cystadenoCAappendectomy for ovarian cystadenoCA Adjuvant Tx:Adjuvant Tx:
Radiation, intraperitoneal and systemic Radiation, intraperitoneal and systemic chemotherapy recommended but it’s role chemotherapy recommended but it’s role is unclearis unclear
57% local recurrence at appendiceal 57% local recurrence at appendiceal primary siteprimary site
Death ensues due to progresive Death ensues due to progresive obstruction and renal failureobstruction and renal failure

THANK THANK YOUYOU