Embed Size (px)
Citation preview

Journal of Medical Virology 79:1017–1024 (2007)
Application of Molecular and SerologicalAssays to Case Based Investigations of Rubellaand Congenital Rubella Syndrome
Li Jin* and Brenda Thomas
Virus Reference Department, Centre for Infections, Health Protection Agency, London, UK
Rubella and congenital rubella syndrome con-tinue to be important health problems world-wide. The detection of rubella RNA directly inclinical specimens is a critical factor in earlylaboratory diagnosis of recent or congenital in-fection, in addition todetectionof rubella-specificIgM. In order to comply with recent WHO recom-mendations for establishing uniform geneticanalysis protocols for rubella virus we havedeveloped a new block based PCR assay (PCR-E317), which extends the sequence generated bythe block based PCR-E592 currently in use, tocover the minimum acceptable 739 nucleotides(nt) window at the E1 gene. In addition, a real-time PCR assay has been developed to allowrapid detection of the virus in the laboratory.The assays were applied to a number of clinicalspecimens collected from patients includingrecent rubella incidences in the UK, Ethiopiaand Turkey, two prenatal and two congenitalrubella syndrome cases. Rubella RNA wasdetected in specimens from two patients thatwere collected too early for IgM detection, in twoamniotic fluids for prenatal diagnosis and in thefollow up specimens from the two infant withcongenital rubella syndrome tested for viralsecretion. At least four genotypeswere identifiedamong these patients. The results showed thatmolecular assays are important tools in the earlydiagnosis of rubella and congenital rubellasyndrome, in the provision of molecular epide-miological information for tracking transmissionpathways and in adding to the knowledge ofrubella strain distribution worldwide. J. Med.Virol. 79:1017–1024, 2007.� 2007 Wiley-Liss, Inc.
KEY WORDS: rubella; congenital rubellasyndrome; case based inves-tigations; real time and PCR
INTRODUCTION
Rubella (German measles) is a mild, asymptomaticand self-limiting illness caused by the rubella virus.
Man is the only host and the incubation period fromexposure to the appearance of the rash, is usually 14–21 days. The illness is usually mild in children, and oftenthe first manifestation is the fine, pink rash spreadingfrom the forehead and face downwards, which may lastfor 1–5 days. Adults often feel unwell before the rashappears, and may have pains in the joints resemblingarthritis. The major reason for the attention devoted tothe eradication of rubella is that infection during earlypregnancy often leads to severe birth defects known ascongenital rubella syndrome.
As a result of immunisation programs, rubella hasbeen almost eliminated in some developed countries. Inthe UK, single rubella vaccination was offered to allteenage girls in 1969 and antenatal screening and anational congenital rubella syndrome register wasestablished in 1971. Combined measles, mumps andrubella (MMR) vaccination was introduced for allchildren at fifteen months of age in 1988, and in 1994 anational vaccination campaign for measles and rubellaaimed at all 5–16 years, resulted in 92% uptake. Tosupport the MR campaign, enhanced epidemiologicalsurveillance of rubella using IgM antibody testing inoral fluid to confirm notified cases was introduced andlaboratory reports by age, status e.g. pregnancy andvaccine coverage have been monitored since 1994. Thelast outbreak of rubella in the UK occurred in 1996 withmost cases occurring in young adult males, who were notvaccinated routinely with MMR prior to 1988 and weretoo old (�16years) for the MMR campaign in 1994.Rubella infection is now rare and congenital rubellasyndrome is exceedingly rare in the UK, although therewas a small increase in congenital rubella syndromeassociated with an outbreak in1996 [Stevenson et al.,1998]. However, a small number of antenatal women arestill at risk, increasingly those who enter the UK from
*Correspondence to: Li Jin, WHO Specialised Laboratory forMeasles and Rubella, Centre for Infections, Health ProtectionAgency, 61 Colindale Avenue, London NW9 5QE, UK.E-mail: [email protected]
Accepted 16 February 2007
DOI 10.1002/jmv.20847
Published online in Wiley InterScience(www.interscience.wiley.com)
� 2007 WILEY-LISS, INC.

overseas unvaccinated, and a susceptible populationmay build up in those born in the UK before 1990.
Rubella virus is the only member of the genusRubivirus in the Togaviridae family, and is an envelopedvirus with a positive sense, single stranded RNAgenome. Laboratory diagnosis based on detection ofanti-rubella IgM and viral RNA by PCR, mainly in oralfluid specimens, has been established at the WHOGlobal Specialised Laboratory for Measles and Rubellaat the Health Protection Agency, UK. It is used routinelyfor diagnosis of rubella infection [Perry et al., 1993; Vyseand Jin, 2003; Cooray et al., 2005]. A positive prenataldiagnosis by PCR could constitute a criterion forconsidering termination of pregnancy and PCR is alsoa suitable assay for monitoring long-term rubella virussecretion in children with congenital rubella syndrome.
WHO and the WHO European Regional Office haverecently proposed the goal of elimination of congenitalrubella syndrome (<1/1,000,000) in Europe by 2010. Inaddition, they made a recommendation to standardizethe nomenclature for the genetic characteristics ofwild-type rubella viruses with the aims of enhancingmolecular epidemiological tracking of viral transmis-sion pathways, monitoring geographical and chrono-logical viral genomic changes and documentinginterruption of viral transmission. Genetically distinctgroups of rubella viruses currently circulating in theworld will be reassigned into genotypes according to aminimum acceptable sequence window of 739 nucleo-tides (nt) of the E1 gene proposed at a meeting at WHOheadquarters in September 2004 [WHO, 2005]. To meetthe WHO goals, a block-based nested PCR assay for a317 nt sequence of the E1 gene has been developed, withthe product that extends from the E1-592 nt regiondeveloped previously for national rubella/CRS surveil-lance [Cooray et al., 2005] to the 739 nt as required. Thestudy has shown that this newly developed PCR-E317 ntassay is more sensitive than that based on 592 nt andthat the sequence data derived from it alone can beapplied for genotyping. In addition, a real-time PCRassay has been developed to meet the requirement ofearly diagnosis of rubella and congenital rubellasyndrome.
MATERIALS AND METHODS
Clinical Specimens Applied to RubellaSerological Diagnosis and Surveillance
Laboratory confirmation of primary rubella infectionis based mainly on detection of rubella specific anti-IgMantibody, and prenatal antibody screening on detectionof rubella anti-IgG in serum or oral fluid. In 2005, 1314specimens in total were received. The majority (972 oralfluids and 94 sera) were tested for rubella IgM and248 were for IgG antenatal screening. IgM and IgGantibodies were detected in serum and oral fluid speci-mens with the rubella MACRIA assay [Perry et al.,1993] and the GACELISA assay [Vyse et al., 1999]respectively. The Dade Behring ELISA assay (Dade
Behring, Germany) for IgG detection was also appliedto sera.
Clinical Specimens Applied toRV RNA Detection
Forty-one specimens from 21 patients were used inthis study for the comparison of the three block basedPCRs. These include 13 samples collected in the UKbetween January 2004 and June 2006, comprising twoamniotic fluids, nine sera, one urine and one throat swabfrom five adult patients (Table I) and 18 specimens fromtwo suspected congenital rubella syndrome babies(Table II). In addition, there were 12 specimens fromoutside the UK comprising six oral fluids from Turkeycollected between 2001 and 2003 and six sera fromEthiopia collected during measles outbreaks in 2004.
Eighteen samples comprising the six sera frompatients in Ethiopia and 12 samples collected and testedin the UK between 2003 and 2005 were used forcomparison of the three block based PCR assays whichgenerate genomic products with different sizes, PCR-E835 (nt8711–9545), PCR-E592 [nt8711–9302, Coorayet al., 2005] and PCR-E317 (nt9221–9545). Newaliquots of these samples were extracted for the purposeof this comparison.
RNA Extraction and Reverse Transcription
Total nucleic acid was extracted from 100 ml ofclinical specimen using the MagnaPure system (Roche,Switzerland) and the RNA in 40 ml was reverse trans-cribed into cDNA using random primers as describedpreviously [Jin et al., 1996; Cooray et al., 2005].
Block Based PCR Assays for Rubella VirusGenome Amplification
PCR-E317. The primers (Table III) were designedusing Oligo6 software, and yield a 317 nt fragment ofrubella E1 gene, covering the 30 end of the 739 nt window(E1 nt8731–9469) required by WHO for genotyping. Theassay was named as PCR-E317 and the accountablesequence is 280 nt in length excluding the primers. Theprimers E1.5 and E1.6R were used for the first roundPCR and E1.7 and E1.8R for the nested PCR andsequencing.
PCR-E835. The published forward primers E1.1and E1.3 [Cooray et al., 2005] and the newly selectedreverse primers E1.6R and E1.8R were combined in anested PCR to generate an 835 nt PCR product (794 ntaccountable), which contains the minimum acceptablewindow proposed by WHO [WHO, 2005]. As in an earlierpublished PCR-E592 assay, 20 ml of cDNA was used forboth PCR amplifications, PCR-E317 and PCR-E835,using the same running conditions [Cooray et al., 2005].
Real-Time PCR for RubellaVirus Genome Detection
The assay was designed by Applied Biosystems, UK.Based on our specification, the primers NS9F and NS9R
J. Med. Virol. DOI 10.1002/jmv
1018 Jin and Thomas

J. Med. Virol. DOI 10.1002/jmv
TA
BL
EI.
Ru
bel
laC
ase
Inves
tigati
on
Pati
ent
(age)
-case
no.
Sam
ple
days
aft
eron
set
Sam
ple
IgM
/IgG
PC
RG
enot
yp
e(l
ink
)S
train
nam
eG
enB
an
kacc
essi
onn
o.
H044220607
(29
yea
rs)
-14-2
6/4
0*
Am
nio
tic
flu
idN
KP
os-5
92
1D
(Ph
ilip
pin
es)
RV
s/L
ond
on.G
BR
/42.0
4[1
D]
EF
210053
H052720511
(39
yea
rs)-
25
–6/4
0*
Am
nio
tic
flu
idP
os/P
os$
Pos
-592
Pos
-317
1g
(Ru
ssia
)R
Vs/
Lon
don
.GB
R/2
7.0
5[1
g]
EF
210052
H060940131
(27
yea
rs)-
31{
Ser
um
Pos
/Neg
Pos
-317
2B
RV
s/L
ond
on.G
BR
/08.0
6[2
B]
EF
210054
8S
eru
mP
os/P
osN
otd
one
—H
06076-1
41
(36
yea
rs)-
41{
Ser
um
Neg
/Neg
Not
don
e—
RV
s/L
ond
on.G
BR
/07.0
6[2
B]
EF
210055
14
Ser
um
Pos
/Pos
Pos
-317
2B
H061760277
(23
yea
rs)-
51
Uri
ne
—P
os-3
17
2B
RV
s/L
ond
on.G
BR
/17.0
6[2
B]
EF
210056
2S
eru
mN
eg/N
egP
os-3
17
—35
Ser
um
Neg
/Pos
Not
don
e—
H062020005
(38
y)-
6N
KS
eru
mE
qv/N
egP
os-3
17
2B
RV
s/L
ond
on.G
BR
/19.0
6[2
B]
EF
210057
H062280002
(48
y)-
72
Th
roat
swab
—P
os-3
17
2B
RV
s/L
ond
on.G
BR
/22.0
6[2
B]
EF
210058
2S
eru
mN
eg/N
egN
otd
one
—8
Ser
um
Pos
/Pos
Not
don
e—
#E
TH
559
(4y)-
813
Ser
um
Pos
Pos
-592
Pos
-317
1g
RV
s/Jig
iga.E
TH
/09.0
4[1
g]
EF
210043
ET
H564
(9m
)-9
5S
eru
mP
osP
os-5
92
Pos
-317
1g
RV
s/E
Hra
regie
.ET
H/1
2.0
4[1
g]
EF
210044
ET
H572
(2y)-
10
2S
eru
mP
osP
os-5
92
Pos
-317
1g
RV
s/G
ura
gie
.ET
H/1
4.0
4/1
[1g]
EF
210045
ET
H576
(6y)-
11
3S
eru
mP
osP
os-5
92
Pos
-317
1g
RV
s/G
ura
gie
.ET
H/1
4.0
4/2
[1g]
EF
210046
ET
H605
(10y)-
12
6S
eru
mP
osP
os-5
92
1g
RV
s/S
idam
o.E
TH
/23.0
4[1
g]
EF
210059
ET
H612
(3y)-
13
7S
eru
mP
osP
os-5
92
1D
RV
s/T
igra
y.E
TH
/24.0
4[1
D]
EF
210060
#T
UR
1431
(7y)-
14
NK
Ora
lfl
uid
Pos
**P
os-5
92
Pos
-317
1g?
RV
s/Is
tan
bu
l.T
UR
/01/1
EF
210047
TU
R1476
(8y)-
15
NK
Ora
lfl
uid
Pos
**P
os-5
92
Pos
-317
1g?
RV
s/Is
tan
bu
l.T
UR
/01/2
EF
210048
TU
R1497
(7y)-
16
NK
Ora
lfl
uid
Pos
**P
os-5
92
Pos
-317
1g?
RV
s/Is
tan
bu
l.T
UR
/01/3
EF
210049
TU
R1446
(NK
)-17
NK
Ora
lfl
uid
Pos
**P
os-5
92
1g?
RV
s/ID
iyarb
ak
ir.T
UR
/03/1
EF
210061
TU
R1453
(NK
)-18
NK
Ora
lfl
uid
Pos
**P
os-5
92
1g?
RV
s/ID
iyarb
ak
ir.T
UR
/03/2
EF
210062
TU
R1501
(NK
)-19
NK
Ora
lfl
uid
Neg
**P
os-5
92
1g?
RV
s/ID
iyarb
ak
ir.T
UR
/03/3
EF
210063
*Ges
tati
onw
eek
s.**
Tes
ted
inse
rum
sam
ple
s.$T
este
dby
oth
erla
b.
#E
TH
:E
thio
pia
&T
UR
:T
urk
ey;N
K:n
otk
now
n;–
not
ap
pli
cable
.{ E
stim
ate
dd
ay
ofon
set.
Case Investigation of Rubella and CRS 1019

and probe NS9M (Table III) were selected within thenon-structural gene and the DNA probe (Table III) wasconjugated with minor groove binder (MGB), named asTaqMan-MGB probe. The assay was performed initiallyas recommended (ABI, UK) in a 50 ml reaction contain-ing 25 ml of universal master mix, 0.833 ml of primer/probe mix and 24.2 ml of cDNA as template. The cDNAwas generated using random primers as for the PCRassay of measles virus described previously [Jin et al.,1996]. The final concentrations used for the primers andprobe were 0.9 mM and 0.25 mM, respectively. A reactionmixture of 25 ml was also tested for comparison with the50 ml reaction. The assay was carried out using the ABIPRISM 7000 Taqman (ABI) as recommended at tem-peratures of 508C for 2 min, 958C for 10 min and 40 cyclesof 958C for 15 sec, 608C for 30 sec, 728C for 30 sec andfinal extension of 608C for 10 min.
Evaluation of the Sensitivity ofthe Developed Assays
The cDNA of the positive control, a virus isolate(Thomas strain) which was also used as the positivecontrol of block based PCR assays was amplified by realtime PCR and the product (56 nt) was directly clonedinto the TOP-TA PCR 2.1 vector and transformed intoE.coli according to the manufacturer’s instructions (Invi-
trogen, UK). The copy number of cloned rubella virusplasmid DNA containing the 56 nt target for the realtime PCR assay was calculated based on the OD value at260 nm. Serial dilutions were used in both 25 ml and 50mlreaction mixes to plot a standard curve of DNA copynumber. The sensitivities of the PCR-E592, PCR-E317and the real time PCR assays were then evaluated using10�1 to 10�5 dilutions of cell culture fluid of rubellaThomas strain, calculated from the standard curve to beequivalent to 5321 (10�1) to 2 (10�4) copies. Thereproducibility of the RT PCR was evaluated byrepeated duplicate or triplicate testing of the standards.
In addition, the sensitivity of the three block basedPCR assays for clinical samples was compared by re-testing by PCR-E317 and PCR-E835 the cDNA of 18clinical samples that had been tested previously by PCR-E592.
Sequencing and Genotyping the DetectedRubella Virus Genomes
Block based PCR products were purified andsequenced as previously described [Vyse and Jin,2002]. Genotyping was performed by sequence dataanalysis and compared with the reference strainsproposed by WHO [WHO, 2005] using DNAStar (Clustal& Megalign) software.
J. Med. Virol. DOI 10.1002/jmv
TABLE II. Investigations of Two Infants with Congenital Rubella Syndromes
PatientAge
month Sample IgM/IgG BB-PCR GenotypeStrain nameGenBank no.
Case 20 H040240385 DOB 4/8/2003with chronic pneumonia & motherfrom Africa
4 Urine — Neg — RVs/London.GBR/52.04[1g]CRSEF210050
4 Oral fluid Pos/Pos Neg —16 NPA* — Pos-835 1g-79417 NPA — Pos —24 Blood Pos/Pos Pos —26 Skin-Bio — Pos-592 1g-55126 Skin-Bio — Pos —28 Serum Pos/Pos Neg —28 Blood — Neg —
Case 21 H050840127 DOB 2/9/2004with very poor lung function;mother 15 year, European Egyptianfrom France
5 Urine — Neg — RVs/London.GBR/08.05[1E]CRSEF210051
5 NPA — Pos-835 1E-7945 Serum Pos/- Neg —6 Blood Pos/Pos Pos —
6.5 Serum Pos/- Pos —8 Blood Pos/- Pos —
12 NPA — Pos-592 1E-55112 Blood Pos/- Pos-592 1E-55112 NPA — Pos-317 1E-280
NPA: nasal pharyngeal aspirates;–not applicable or not done.
TABLE III. Sequences and Locations of the Primers and Probe
Dsignedname Sense Position Sequence 50–30
PCR productsize (nt)
E1.5 þ 9221–9240 TTGGGGCTGAAGTTCAAGAC 325E1.6R � 9529–9545 TGGTGTGTGTGCCATACE1.7 þ 9226–9245 GCTGAAGTTCAAGACAGTTC 317E1.8R � 9526–9542 TGTGTGTGCCATACACCNS9F þ 4803–4818 GGCTCAGCGCGTTCCT 56NS9R � 4841–4858 GGCGGGAACCTCCTTGAGNS9M � 4820–4834 FAM-GACGCCGGGGCACTG-MGB
1020 Jin and Thomas

RESULTS AND DISCUSSION
Serological Diagnosis andSurveillance of Rubella
Of the 1066 specimens received for rubella IgM testingat our laboratory in 2005, only 28 cases were IgMpositive and serologically confirmed (http://www.hpa.org.uk/infections/topics_az/rubella/data_rub_not.htm).Similar low levels of detection had also been observed inprevious years, 17 laboratory confirmed cases in 2003and 14 in 2004, suggesting that rubella incidence is lowand rubella infection still under control in the UK.
Sensitivity of the Newly Developed PCRs
Both the real time PCR and the PCR-E317 detectedrubella cDNA at 10�4 (two copies) of serially diluted cellculture fluid of rubella Thomas strain, whereas PCR-E592 was one 10-fold dilution less sensitive (12 copies,Table IV). However, it was noticed that freeze–thawcycles and long-term storage at 48C reduced the titres ofthe diluted DNA standards. It has also been found thatthe sensitivity of PCR assays for detection of rubellaRNA can be affected by freeze–thawing of the clinicalspecimens, extracted viral RNA, cDNA and first roundPCR products kept at either �70 or �208C, suggestingthat rubella virus genome may be labile and that greaterattention should be paid to specimen collection, trans-port and storage. In addition, the random primedreverse transcription reactions could be more efficientfor one region, e.g. the H gene by the real time assay thanfor another, the E1 gene by the block based PCRs, whichrequires further studies.
Specificity of the selected primers and probe wasconfirmed by checking the statistical significance ofmatches and searching for similarity between sequencesusing the Basic Local Alignment Search Tool (BLAST) athttp://www.ncbi.nlm.nih.gov/BLAST.
Evaluation of the PCR Assays by Detection ofRubella RNA in Clinical Samples
In the 18 clinical specimens that were tested bythree block based PCR assays in parallel, rubella RNAwas detected in 16 samples by PCR-E317 whereas only13 were positive by PCR-E592 and 12 by PCR-E835(Table V). The results suggest an association betweenthe sensitivity of rubella PCR assays and the size of PCRproduct. PCR assays that target an area of the E1 gene
that is >500 nt in size may result in failure to detect thevirus in 16–22% of clinical specimens.
Due to the scarcity of rubella cases in the UK, thereproducibility and sensitivity of the real time PCRassay in clinical specimens was not able to be evaluated.However, it has been adopted by a laboratory in Indiaand the results of its application to a large number ofclinical specimens will be available in the near future(publication in preparation).
Detection of Rubella Virus in ClinicalSpecimens by PCR Assays
The five sporadic rubella infections reported inpatients in London since the week 7 of 2006 (Table I,cases 3–7) were all initially suspected to be measlesinfection. Neither measles nor rubella IgM was detectedin four of five of their early sera, whereas rubella virusgenome was found by the PCR-E317 in all four earlyspecimens and one specimen taken at possible day 14after onset. Rubella IgM and/or IgG were detected infollow up sera from all the cases and confirmed thediagnosis of rubella.
In samples collected during a measles outbreak inEthiopia in 2004 rubella IgM and RNA were detected inall six sera from six patients (cases 8–13) taken between2 and 13 days after onset (Table I). Rubella genome wasdetected initially in all six samples by PCR-E592 but inonly four of the six tested eight months later by PCR-E317 after several freeze–thaw cycles. In contrast to theUK patients who were aged between 23 and 48 years, theEthiopian patients were aged between 9 months and10 years, reflecting the immunisation status in thesetwo countries.
In samples collected from six patients (cases 14–19) inTurkey in 2001 and 2003 (Table I), five of six sera wererubella IgM positive and all six oral fluids collected
J. Med. Virol. DOI 10.1002/jmv
TABLE IV. Sensitivity of the Real Time and Block BasedPCR Assays
Positive cDNAdilutions
Real time-PCRct value/copy no. PCR-E317 PCR-E592
10�1 27.85/5341 þ þ10�2 32.46/192 þ þ10�3 36.30/12 þ þ10�4 38.50/2 þ �10�5 — � �
TABLE V. Comparison of the PCR Assays Applied to RubellaRNA Detection in Clinical Specimens
Samples PCR-E835 PCR-E592 PCR-E317
1. Serum � � þ2. Serum þ þ þ3. Serum � þ þ4. Serum � � �5. Serum þ þ þ6. Serum þ þ þ7. Nasal pharyngeal � � þ8. Throat swab þ þ þ9. Oral fluid þ þ þ
10. Oral fluid þ þ þ11. Oral fluid þ þ þ12. Oral fluid þ þ þ13. Oral fluid þ þ þ14. Nasal pharyngeal � � þ15. Serum � � �16. Amniotic fluid þ þ þ17. Amniotic fluid þ þ þ18. Amniotic fluid þ þ þTotal Pos/tested 12/18 13/18 16/18
Case Investigation of Rubella and CRS 1021

simultaneously were rubella RNA positive by PCR-E592initially, whereas only three were positive by PCR-E317when the specimens were retested after freeze–thaw.The three patients from 2001 were 7 or 8 years old andages of those three patients in 2003 were unknown.Prenatal diagnosis. Two amionic fluid specimens
(cases 1 and 2) were tested for diagnosis and confirma-tion of prenatal rubella (Table I). Patient 1 was from thePhilippines and was known to be infected at 4/40 weeksgestation, with fetal death occurring at 26 weeks.Patient 2 had primary rubella at 5–6/40 weeks gesta-tion, acquired in Russia, and the rubella diagnosis wasconfirmed at another laboratory by sero-conversion, lowavidity IgG and IgM in three other samples. Rubellagenome was detected in a sample from patient 1 by PCR-E592 initially (negative by PCR-E317 after freeze–thaw, when the test became available) and in a samplefrom patient 2 by both PCR-E592 and PCR-E317.Genotypes 1D and 1g were identified and these mayrepresent the domestic or predominant rubella strainsin the Philippines and Russia, respectively. Althoughdetection of the rubella genome by PCR providesadditional evidence of infection, there were too fewamionic fluid samples to evaluate its use alone forprenatal diagnosis. The correlation of rubella RNAdetection in amionic fluid and fetal infection requiresfurther study.Postnatal diagnosis. The investigation of two
infants (cases 20 and 21) with congenital rubellasyndrome is summarised in Table II. Nine specimenscollected from each of the two patients, including theinitial and follow up specimens, were tested. Althoughrubella IgG was detected at the age of four months incase 20 and at six months in case 21, rubella IgM and/orrubella genome were continually detectable up to theages of 24 and 12 months in these two infants. Rubellagenome was not detected in the specimens collected atthe age 28 months in case 20, while the rubella IgM wasstill detectable suggesting there is a possible associationbetween viremia and humoral immune reaction. Bothinfants were born with very poor lung function orchronic pneumonia. Rubella genome was detected inoral fluid, nasal pharyngeal aspirates and blood sam-ples, but not in urine, suggesting that the route of viralsecretion may relate to the affected organs, and couldlast as long as 2 years postnatally. Genotyping ofsequential positive samples was repeated to check itsconsistency and to exclude any possibility of contamina-tion during PCR processing. The sequences generatedfrom samples from the same individual were allidentical suggesting that no further mutation occurredin the E1 region detected during the long-term incuba-tion. The genotypes 1g and 1E detected may representdomestic or predominant RV strains in Africa andEurope, respectively, the areas of origin of the mothers,who were not vaccinated. These results indicate thatcongenital rubella syndromes could re-emerge in the UKdue to importations, despite the success of the rubellaimmunisation program. According to a recent report,60% of the mothers of CRS infants in the UK were born
abroad, most had come to the UK as adults and rubellavaccination had not been offered [Tookey, 2002].Identification of population groups with high suscept-ibility rates, such as Asian women in South and EastLondon [Devi et al., 2002] for targeted immunisation,requires urgent attention.
Genotyping and phylogenetic analysis. Rubellavirus RNA is very labile compared to measles andmumps RNA [Jin et al., 2002; Cooray et al., 2005] and itsintegrity may not be well preserved in samples collectedduring field investigations and in sporadic specimenscollected by clinicians. Inadequate storage and trans-portation makes impossible the successful amplificationof the minimum acceptable region (the E1-739 nt)required by WHO. However, the smaller fragmentgenerated by the PCR-E317 assay, which comprises apart of the minimum requirement of 739 nt (C-terminal224 nt) plus an additional 56 nt, was successfullyamplified from some clinical specimens in this study.Samples from the five UK rubella patients wereconfirmed to be genotype 2B based on the accountable280 nt only. Amplification of this region is also shown toresult in a more sensitive assay than PCR-E592(Table I).
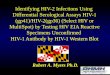
Figure 1 shows the phylogenetic analysis of thesamples used in this study based on lengths of the E1gene between 280 nt and 794 nt. All the reference strains[WHO, 2005] one of the prenatal strains (Table I, case 2),two postnatal strains (Table II), four of the six ETHstrains from sera and three of the six TUR strains fromoral fluids (Table I) were analysed based on 794 nt. FiveUK strains (3 sera, urine and TS) were based on 280 nt.The remaining six samples (two from ETH, three fromTUR and one prenatal (Table I, case 1) were analysedbased on the 552 nt. The full length of 794 nt rather thanthe 739 nt WHO required of reference strains wasapplied to data analysis, which helped to connect thosesequences of the 50 part of the 551 nt and 30 part of 280 ntin some cases (Fig. 1). Similar phylogenetic trees weredrawn based on either the 280 or 551 nt region for thoseavailable data (results not shown). Bootstrap value wasnot measured due to the different lengths of sequences,and these 21 strains were however, clearly assigned toone of the current proposed genotypes when comparedwith the reference strains [WHO, 2005].
At least four genotypes were identified. (Fig. 1,Tables I & II). The five UK strains (cases 3–7) identifiedin 2006 belonged to genotype 2B although two had one ortwo point mutations. All these patients were adults (27–48 years) living in London and were infected withrubella during the period between February and June2006. No connection, recent travel history or foreigncontacts were found to indicate importation. By con-trast, the multiple genotypes found in the UK inprenatal amniotic fluid specimens from women fromthe Philippines and Russia (1D and 1g) and from infantswith CRS whose mothers were of African and Frenchorigin (1g and 1E) were most likely to be importations.
Five of the six Ethiopian strains were conducted into acluster of genotype 1g and were closely related to the
J. Med. Virol. DOI 10.1002/jmv
1022 Jin and Thomas

reference Uganda strain (u588-ug 01, data provide byCDC, USA). The sixth which was the only one from thegeographic area of Southern Tigray (Case 13) belongedto genotype 1D. This suggests that at least twogenotypes may be circulating in Ethiopia.
All the specimens from Turkey were conducted into asolo cluster closely related to 1g but obviously different
from the cluster of ETH strains. Compared with allgenotype reference strains, the three Turkish strainsbased on 794 nt showed over 4% divergence from all thereference strains, suggesting that this may represent anew genotype. However, no cell culture isolate isavailable to allow sequencing of the entire structuralprotein as recommended [WHO, 2005].
J. Med. Virol. DOI 10.1002/jmv
Fig. 1. Phylogenetic tree for genotyping newly detected rubella strains. The phylogenetic analysis wasbased on a 794 nt of the E1 gene, which contained the minimal required 739 nt. Reference strains [WHO,2005] were used as the basic dataset and the genotype is indicated at the end of GenBank accessionnumbers. Provisional genotypes 2c and 1g (sequences provided by CDC, USA), as well as the positivecontrol Thomas strain were also included. The 21 strains investigated in this study were compared with thereferences and the sequence lengths are indicated at the end of strain names.
Case Investigation of Rubella and CRS 1023

All the 21 strains in this study were clearly conductedinto clusters along with reference strains regardless ofthe lengths of the sequence, suggesting that the smallerE1 fragments which are more easily detected can beused as an option to screen rubella virus genotypes inclinical samples. Two rubella strains, Ed29-UNK03 andKent12-UNK03 published in our previous article[Cooray et al., 2006], and included in the analysis wererenamed as RVs/Edinburgh.GBR/25.03[1E] and RVs/KentGBR/21.03[2B]CRS, and reassigned to genotypes1E and 2B, respectively (GenBank accession numbersEF210065 and EF210066), according to the WHOnomenclature for genetic characterisation of rubellaviruses. Sequence data for these 21 strains have beensubmitted to GenBank (accession numbers EF210043–EF210063).
The newly developed PCR assays in this study provideadditional laboratory tools for molecular diagnosis andepidemiological surveillance of rubella and the dataadd to the literature on the discrimination as well asgeographical distributions of rubella strains in theworld. In addition, the findings highlight the need forcountries to establish laboratory surveillance, to iden-tify trends in incidence of congenital rubella syndromeand susceptibility to rubella and to introduce rubellavaccination among women of child-bearing age.
ACKNOWLEDGMENTS
The authors are very grateful to Dr Wondatir Nigatu(Ethiopia), Dr Gulay Korukluoglu (Turkey), Dr. MikeShortland at St. Georges Hospital, London, Dr. CarolynAdcock at Plymouth Hospital NHS Trust, doctors atDerriford Hospital, Plymouth, and all other generalpractioners and hospital clinicians in the UK and
Consultants in Communicable Disease Control whocollected specimens and sent them to our laboratory forconfirmation. We also thank Dr. David Brown for hiskind support, and all colleagues in the Immunisationand Diagnosis Unit, Virus Reference Department,Centre for Infections, Health Protection AgencyColindale, for their support in testing the specimens.
REFERENCES
Cooray S, Warrener L, Jin L. 2005. Improved RT-PCR for diagnosis andepidemiological surveillance of rubella. J Clin Virol 35:73–80.
Devi R, Muir D, Rice P. 2002. Congenital rubella: down but not out.Lancet 7:360.
Jin L, Richards A, Brown DWG. 1996. Development of a dual target-PCR for detection and characterisation of measles virus in clinicalspecimens. Mol Cell Prob 10:191–200.
Jin L, Vyse AJ, Brown DWG. 2002. The detection of measles, mumpsand rubella by RT-PCR on oral fluid: its role in diagnosis andsurveillance. Bullet WHO 80:76–77.
Perry KR, Brown DW, Parry JV, Panday S, Pipkin C, Richards A. 1993.Detection of measles, mumps, and rubella antibodies in saliva usingantibody capture radioimmunoassay. J Med Virol 40:235–240.
Stevenson J, Murdoch G, Riley A, Duncan B, McWhirter M, Christie P.1998. Implementation and evaluation of a measles/rubella vaccina-tion campaign in a campus university in the UK following anoutbreak of rubella. Epidemiol Infect 121:157–164.
Tookey P. 2002. Congenital rubella: down but not out. Lancet 360:803.
Vynnycky E, Gay NJ, Cutts FT. 2003. The predicted impact of privatesector MMR vaccination on the burden of congenital rubellasyndrome. Vaccine 21:2708–2719.
Vyse AJ, Jin L. 2002. An RT-PCR assay using oral fluid samples todetect rubella virus genome for epidemiological surveillance. MolCell Prob 16:93–97.
Vyse AJ, Brown DWG, Cohen BJ, Samuel R, Nokes DJ. 1999. Detectionof rubella virus-specific immunoglobulin G in saliva by anamplification-based enzyme-linked immunosorbent assay usingmonoclonal antibody to fluorescein isothiocyanate. J Clin Microbiol37:391–395.
WHO. 2005. Standardization of the nomenclature for genetic char-acterisation of wild-type rubella viruses. Weekly Epidemiol Rec.80:126–132.
J. Med. Virol. DOI 10.1002/jmv
1024 Jin and Thomas