Embed Size (px)
Citation preview

Brit. Heart J., 1967, 29, 689.
Application of Multipoint Electrodes to Telemetryin Patient-monitoring and During Physical Exercise
DAVID LEWES AND D. W. HILL
From the Cardiac Unit, Bedford General Hospital, and the Research Department of Anasthetics,The Royal College of Surgeons, London W.C.1
Telemetry (Gk: Te'Ao, end; ,tdirpov, measure)is defined as the making of measurements at a dis-tance from the subject.
Following the successful use of a dry multipointelectrode for routine electrocardiography (Lewes,1965, 1966; Stock, 1966; Turner, 1966; Keen andJohnson, 1966), we have conducted preliminarytrials using a multipoint chest electrode for the moni-toring by radio-telemetry ofpatients with myocardialinfarction and in the assessment of cardiac functionduring physical exercise. Latterly our studies haveembraced the transmission of the electrocardiogramover the General Post Office (G.P.O.). telephonesystem using multipoint electrodes and transistorizedelectrocardiographs.
Resuscitation in the intensive care units in theUnited Kingdom involves monitoring by conven-tional methods which include the wiring of complexapparatus at the bedside directly to the patient.This state of affairs is far from ideal since modernelectronic equipment, especially when incorporatingan oscilloscope and alarm devices, aggravates theemotional tension and anxiety of a seriously ill pat-ient already predisposed by cardiac infarction todangerous dysrhythmias. Indeed, it is likely thatsuch monitoring equipment, designed to anticipateand detect dysrhythmia, occasionally precipitates thedisorder it is meant to prevent, especiaUy in theseriously ill and emotionally disturbed subject.
Current methods of bedside monitoring suffer theadded disadvantage that, in the event of an emer-gency necessitating external cardiac massage, wiresconnecting patient and adjacent apparatus are anencumbrance to resuscitation procedures. From thepatient's point of view, monitoring by telemetry isideal since it overcomes these disadvantages. Radio-telemetry, moreover, is obligatory for the electro-cardiographic assessment of the cardiac state under
Received September 23, 1966.4 689
conditions where conventional electrocardiographyis either impractical or impossible, for example,during a conventional exercise test or while running.
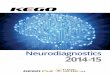
Since a multipoint electrode requires no prepara-tion with jelly or paste and achieves skin contact atnumerous points by penetrating the stratum cor-neum, which is responsible for the greater part ofnatural skin resistance (Robertson, 1937), artefactskin potentials due to electrode-skin movement maybe greatJy diminished (Fig. 1). Movement of a flatmetal electrode, separated from the skin by a fluid-conducting medium, produces electrical potentialsat the electrode/jelly/skin interfaces which arereflected in the radiocardiogram or conventionalelectrocardiogram by artefact potentials, or as awandering baseline (Boter, den Hertog, and Kuiper,1966).
APPARATUS AND METHODSRadio-telemetry Systems. Crystal-controlled trans-
mitters and receivers were used throughout (Fig. 2).The term "crystal-controlled" means that reception bythe receiver is locked to the transmission, thus makingretuning of the receiver unnecessary.The first system employed was the R.K.G. 100 by
Telemedics of Southampton, Pennsylvania. It is a fre-quency-modulated system, having a carrier frequency of80 megacycles per second and a range of 100 yards.The second system was the C & M Radiocardiographproduced by Medical & Industrial Equipment Ltd., ofLondon. It is an amplified and frequency-modulatedsystem operating at 169 Mc/s. AM/FM uses a com-bination of amplitude and frequency modulation: ampli-tude modulation alters the amplitude of the transmittedcarrier wave, and frequency modulation alters the fre-quency of the carrier. Both telemetry systems can beadapted to operate in the 102-2-102-4 Mc/s bandproposed for medical radio-telemetry by the G.P.O. AG.P.O. licensing fee of 20 shillings is necessary for usersof medical radio-telemetry equipment and covers a five-year period.Most of our radio-telemetric recordings were made
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Lewes and Hill
RESTING 1r.
SPRINTING
ON SPOT
ARM~~~~~~~~~~~A
PRESS-UPS 4s_A ~~~~~~~~~Sl
RESTING r_m~~~srr*~
.h A.A%JlS
S~~~
rc
nr§s _ '~~~~~~~~~~~~~M
FIG. 1.-Electrocardiograms recorded in a healthy man of 50, using in (A) two standard Philips suction clothelectrodes, and in (B) two multipoint suction electrodes, applied to the manubrium sterni and xiphisternum.
Note the steady baseline and reduction of artefact potentials during exercise in (B).
.
aS.
_-
5 _|~~/
I14
FIG. 2.-The C&M Radiocardicput connected to the chest electi
with the British telemetry system which has been avail-able in the country for more than five years at a total costless than that of a reliable modem single-channel electro-cardiograph. The transmitter and receiver are eachpowered by a compact standard radio 9-volt battery(Ever Ready PP6 or equivalent) which operates *ithintermittent use for 40-50 hours and continuously forapproximately 10 hours; renewal of batteries is inexpen-sive, simple, and quickly effected.The transmitter and receiver, each with its self-con-
,.,:...:......q.... . 1... :: i':'X~~~~~iS:_:: .. :::':: ... 3MN
°ph (eical: Inutra Eqimn Lt.) soin the:trnsite :::i:::.::n::':.,;jasand receive !:::.':':.8:temia bloc fo the recordin apartu. G. ..3
tained aerial and FM/AM circuits, normally reject allunwanted radio signals, so that only electrical signalsfrom the patient are transmitted and received by thetelemetry equipment. The transmitter and receiver,including batteries, weigh approximately 566 g. and2-26 kg. (20 oz. and 5 lb.), respectively.The recorders used with these systems were: Philips
Cardiopan 1, Elmqvist Junior portable, NewmarkCardette (all single-channel), and the Mingograf-24B(double channel).
690
.t
.....
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Application of Multipoint Electrodes to Telemetry in Patient-monitoringElectrodes. Circular multipoint electrodes of 2-8 cm.
diameter, made from a tin-plated soft iron nutmeg grater(Lewes, 1965), were soldered to a centrally placed press-stud contact. A centrally perforated disc of thick paper2*8 cm. diameter was glued to the back surface of eachelectrode. A disc of coarse linen approximately twicethe diameter of the electrode was lightly attached to theelectrode, which was then steam-sterilized.
Electrode Application. The most suitable electrode-skin areas, in regard to the production of minimalelectromyographic activity, have been found to be overthe manubrium sterni and the fifth or sixth left inter-costal space just anterior to the mid-axillary line. Theselected areas were shaved, if necessary, and thoroughlycleaned with ether. The sterilized electrode was pressedfirmly into position on to the cleaned, stretched skin.The linen disc, previously saturated on one side with anon-irritant waterproof glue*, was then affixed to theelectrode and surrounding skin, which was well stretchedwith the fingers of one hand during application. Firmpressure was maintained for several minutes until theglue had set; this process was hastened by using a hairdryer, as first suggested by a patient. An application ofthe glue to the outer surface of the linen disc ensured awaterproof arrangement which was unaffected by dailybathing. Unless the electrode be firmly applied andsecurely glued in position, a varying skin-contact resis-tance due to electrode movement may mar the radio-cardiogram during physical activity. Skin-contactresistance is also altered by direct pressure on the elec-trode.The Telemedics RKG 100 receiver contains a skin
resistance meter, and with proper electrode applicationthe skin contact resistance for paired electrodes wasusually less than 10 kQ at 20 c.p.s., but readings as low as3 kQ were occasionally observed. An experimental latexgluet is at present being evaluated and has given promis-ing results.The transthoracic lead gives a tall R wave and positive
T wave in normal subjects and proved satisfactory bothfor patient-monitoring and for interpretation of theelectrocardiogram during physical exercise.
MONITORING BY RADIO-TELEMETRY INMYOCARDIAL INFARCTION
Small diameter patient leads were connected tothe studs ofthe electrodes and to the input terminalsof the transmitter which was placed in the patient'spyjama pocket, or secured beneath his pillow. Thereceiver was located in a central monitoring area, itsoutput being fed to a conventional electrocardio-graph and oscilloscope to produce signals identicalwith those normally recorded at the bedside (Fig. 3).
Results. Preliminary studies in four subjects haveshown that satisfactory monitoring by radio-tele-metry using multipoint electrodes can be achieved
* Type Saba-select FH1 by Depex Ltd., Debilt, HoLland.t Manufactured by I.C.I. Pharmaceuticals Ltd.
with a minimum of mental and physical disturbanceto the patient, not only in acute cardiac infarctionwhen a patient might be desperately ill and appre-hensive (Fig. 4), but also for periods of up to twoweeks during convalescence (Fig. 3). There was nocomplaint of discomfort from the electrodes which,in two patients, werewom continuously while under-taking normal convalescent activities. Skin damage,moreover, was negligible, the superficial abrasionrequiring no dressing after removal ofthe electrodes.In no patient has infection or skin reaction due tothe glue or metal been observed following the appli-cation of the sterilized multipoint electrodes.
RADIO-ELECTROCARDIOGRAPHYDURING PHYsIcAL EXERCISE
The use of radio-telemetry techniques to recordelectrocardiograms from exercising subjects is bynow well known (Bellet et al., 1962). It might beexpected, however, that the use of dry multipointelectrodes would reduce motion artefact signals.Employing the technique of electrode applicationdescribed above, radiocardiograms both at rest andduring physical exercise were made during a 16-week period on a man aged 50 years in whom the leftaxillary multipoint electrode remained in its originalposition throughout this time (Fig. 5). After 18days the manubrial electrode stud attachment be-came dislodged, necessitating renewal of the entireelectrode. The resultant skin damage was slightand consisted of punctate areas of epithelial hyper-plasia roughly corresponding to the points of theelectrode, as well as light pigmentation due to chronicirritation (Fig. 6).The original left axillary electrode, in position
more than four months later, required further appli-cation of glue to the cloth disc which eventuallybecame rigid necessitating renewal every few weeks;this change was made without disturbing theattachment of the multipoint electrode to the chestwall.For four months our subject led a full and active
life, took a daily bath, and was undisturbed by thepresence of the electrode. Although physically fithe happened to be liable to attacks of paroxysmalatrial fibrillation customarily suppressed by digoxin0 75 mg. daily. While in sinus rhythm there wereno abnormal cardiac symptoms, even on strenuousexertion, but when the fibrillation set in, effortdyspnea and palpitation were troublesome. Nor-mal rhythm was promptly restored by propranolol20 mg. orally (Fig. 7).
Results. During strenuous physical exercise,such as running up and down stairs, multipoint chest
691
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Lewes and Hill
Day Method
Radio
rest
rest
Radio2 rest ....2Radio $s
rest ~~~~. ...... ...._.
6 Direct 9
Radio
walking
rest
FIG. 3.-Serial radiocardiograms and direct electrocardiograms recorded in a man of 54 over a 2-week periodduring convalescence following postero-lateral cardiac infarction, using multipoint chest electrodes applied
to the manubrium sterni and left axilla (see text).
electrodes, when correctly applied, yielded a radio-cardiogram with a consistently steady baseline andminimal artefact potentials, factors that may beundesirable as they render interpretation difficult orimpossible when using conventional electrodes andabrasive saline jelly (Fig. 7 and 8).Throughout the 16-week period of observation
radiocardiograms have been recorded on 11 differentoccasions at intervals of a week or more during suchactivities as running on the level or upstairs, steptests, or sprinting on the spot. In each of five suchexaminations, controlled by conventional electrodes
and abrasive saline jelly, the continuous tracingsobtained with the dry multipoint electrodes wereunequivocally superior to the control records (Fig.8). The final radiocardiogram was recorded duringa step-test 116 days after the original application ofthe left axillary electrode (Fig. 9). The contactresistance for the paired chest electrodes had nowrisen to 20 kQ (d.c.), and it was not possible to recordan acceptable radiocardiogram during more vigorousexercise.The left axillary electrode, when removed four
days later, was rusted and plugged with epithelial
692
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Application of Multipoint Electrodes to Telemetry in Patient-monitoring 693......
11 2 5 pm Radio w4yNApJ_ % 9. _-
11 30pm Radio
12 50acm Radio_' j VJ s fJ4Jo
12 55am Radio 1 F t ,_, _*00am Radio t-_>;
I 05carrm Radio
08am Rcdic
S am Radio * -'-- >*r r -V A
2 5 am Rodi' r < ' < ' ¾
26 am Radio . V v - --
1 40cm Radio A
I 4 2 am Radio ,,X l>t4tI$tJ A
5 2am Radio - f jr '-- h ^
I 5Sam Radio ir '\-w v \
8O00am Direct .-Jtt4/-0-0 1lO sec. after \ \0- E _ defibrillation I <v Nj u U
-900am Direct -Q) Terminal
FIG. 4.-Serial radiocardiograms recorded during a 9j-hour period in a man of 57 dying within 24 hours ofmassive anterior cardiac infarction, confirmed at necropsy. Multipoint electrodes were applied to the
manubrium sterni and mid-axillary line in the sixth intercostal space.
debris; the underlying skin, however, was smooth (Hill, 1966), with the co-operation of G.P.O. engin-and unbroken, showing only punctate areas of dark eers.pigmentation.
Method and Apparatus. A standard Post Office Datel
Modem equipment was modified to provide an F.M.TRANSMISSION OF ELECTROCARDIOGRAMS system with a carrier frequency of 1700 c.p.s. The
BY G.P.O. TELEPHONE LINES electrocardiogram was recorded with a Cardette tran-The first known demonstration in Great Britain sistorized electrocardiograph by Louis Newmark Ltd.,
of the transmission of an electrocardiogram and which had been fitted with a transistorized single-sidedorther biologicalwaveforms byGanO. telephoane output stage to feed the Datel Modem. The outputother biological waveforms by G.P.O. telephone from the Modem was fed to an ordinary telephone lineJines was given on March 29, 1966, at the Bio- obtained by normal dialling. At the receiving endmedical Exhibition at the New Horticultural Hall, another Modem fed a second Cardette. The patientWestminster, by Professor J. P. Payne and one of us was fitted with a set of multipoint limb electrodes.
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

RESTING (sittinq).S/Recorder. S/Receiver. S/Transmitters~~~~~~- ^| t |ss| -'';
Running up and down stairs (19 steps) for 2 minutes. Continuous recor-d of 54 seconds.
t;>~~~~~~r r/%Aqt V K. rl, e/N JVJA' 2.o/>oo*|||13 :1 1 I~/V i
trecording.,^fysAD or
17inch display cathode ray tube osioscosat ti tAetN
Nl.rt,,,,,f.>tIiI,j5J,t,<tIIiIij 11111u11114m.or*
FIG. 5.-Radiocardiogram at rest and during physical exercise in a man of 50 years. Multipoint chest elec-trodes applied to the xiphisternum and left mid-axillary line 114 hours previously and worn continuouslyduring normal daily activities. Skin contact resistance of paired electrodes 7 kQ2 (a.c.) before and after
recording.
The patient was a 44-year-old man undergoing a were transmitted. There was no significant degree ofurinary bladder operation at St. Paul's Hospital, London. interference present on the tracings (Fig. 10).The electrocardiogram and pnetunotachogram were dis-played onla Cardette electrocardiograph and a pair of DISCUSSION17-inch display cathode ray tube oscilloscopes at the NewHorticultural Hall two miles from the hospital. One Multipoint electrocardiography without skinmillivolt calibration pulses and the standard limb leads preparation is receiving increasing support as a
FIG. 6.---Multipomnt chest electroide and electrode skin area after 18 days of continuous application. Notethe punctate areas of epithehal hyperplasia and darkening of the skin due to local erythema and pigmentation.
Lewes and Hill694
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Multipoint: Rest.
Multipoint: Steptest (18') minute followed by continuous record during 2nd minute.
Multipoint: Running up and down stairs (19 steps). Continuous record.
I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~[II''~~~~~~~~~~~~~~~~~~~~~~~~~~I
6 hours later. Normal rhythmMultipoint: Rest.
/ MuItipoint: Running up and down stairs (19 steps). Continuous record
XuIjI tstEj|ir j1 j "'|I I||Ib-!trmControl: Rest C
tM electrodes and Combride Jelly.
Control: Running up and down stairs (19 steps)-Cambridge Jelly.
FIG. 7.-Continuous radio-telemetric records at rest and during exercise using multipoint chest electrodesin a man of 50, in whom the left axillary electrode had been continuously in position for 36 days. Top records:atrial fibrillation. Middle records: normal rhythm after propranolol. Bottom records: control tracings in
normal rhythm using conventional electrodes and Cambridge jelly.
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

696 Lewes and Hill
MultIpoint Rest.
!-1.. ' 1 . 1 . 1 !!!'*! s. l1.* 1: ! *.1: | . !:::!
Multipoint: Running around OP. waiting area after 2 minute steptest. Continuous record.
.tt!I I I !! !! !!..It1 f ! ! .1!I 1111ll I I I .
Control C & M electrodes & Cambridge Jelly. Rest. Extra Systole
iz ! (if I j l
Continuous record.Control: Running around O.R waiting area after 2 minute steptest. Cambridge Jelly.
{YiP.V.2 i... . .... ..... .. - . , . . ...... . * ^ .i.. . I..
,j,,.............:...... fiji W, Wl. ,_.i...XX.bA~S~>;7..1..!.....|s; ! t !! ii I Ii Ii IL|||}
FIG. 8.-Continuous radio-telemetric records during exercise, using multipoint electrodes and control tracingsemploying conventional electrodes and Cambridge jelly. The left axillary multipoint electrode had been
continuously in position for 25 days.
convenient, clean, and time-saving method of re- For routine electrocardiography and patient moni-cording electrocardiograms from the body surface toring, and for survey work when saving time is(Stock, 1966; Turner, 1966; Wilton-Davies, 1966; important, the method has been found quick andErnsting, 1966; Keen and Johnson, 1966). reliable, yielding records indistinguishable from
JIJL 1 Clll /ntv
FIG. 9.-Radiocardiogram (a) at rest and (b) during a step-test, using multipoint electrodes and recorded 116days after the original application of the left axillary electrode. Contact resistance for paired electrodes
20 k9Q (d.c.).
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Application of Multipoint Electrodes to Telemetry in Patient-monitoring
J N
~~~~~~~~~~- .v+X^*!1~~^^z+tt+A.. II%11...l,, ; e - t 5 ' ''<.<... .... ....
A...
FIG. 10.-Electrocardiogram (I) and pneumotachogram (Pn) of a patient during operation, which were trans-mitted over the G.P.O. telephone system and recorded on two display cathode ray oscilloscopes and by a tran-
sistorized electrocardiograph two miles from the operating theatre. (See text.)
those obtained in the same subjects with conven-tional electrodes and saline jelly (Stock, 1966; Keenand Johnson, 1966).
Satisfactory electrocardiograms using only multi-point electrodes have been obtained at the highHimalaya (Turner, 1966), in the decompressionchamber (Ernsting, 1966), and by telemetry underconditions of increased barometric pressure equiva-lent to 100 feet of sea water (Wilton-Davies, 1966).
Direct electrocardiograms have been recordedwith multipoint electrodes in horses (Lewes, 1965;A. Stevenson, personal communication, 1966).One of us (D. W. H.), working with Professor L. A.Geddes, at the Texas University College of Veterin-ary Medicine, has recently recorded equine electro-cardiograms by radio-telemetry using multipointelectrodes. Coarse stainless steel grater electrodes,of approximately 13 sq. cm. (2 sq. in.), were appliedto the unclipped skin of the legs and thorax. Thetracings recorded both by direct and radio-telemetricmethods were indistinguishable from those obtainedafter subsequent preparation of the multipoint elec-trodes and skin with concentrated saline solution.Finally, Wilton-Davies (1966) has recorded oculo-grams in human subjects with multipoint electrodes,which have proved the equal in performance and thesuperior in convenience of application to suction cupelectrodes and saline jelly.The present study explores the possibilities of the
application of multipoint chest electrodes to radio-telemetry, not only for patient monitoring in cardiacinfarction, but also in assessing cardiac functionduring differing forms ofphysical activity which pre-clude the use of conventional electrocardiography.It has been shown that a relatively crude multipointelectrode, efficiently applied, is capable of yielding ahigh quality radiocardiogram during physical exer-cise days or weeks after its original application to thechest. Lastly, the value of the dry multipoint
electrode in patient-monitoring during surgicaloperation, and the future possibilities in GreatBritain of the transmission of the electrocardiogramand other biological wave forms over the G.P.O.telephone system to distant centres for immediateinterpretation or storage by tape for computeranalysis, have been indicated.
It is the present intention of the G.P.O. to limitthe transmission by radio of physiological signals toa distance of some 600 feet. Patient mobility can bemaintained at greater distances by feeding the out-put of the radio receiver into a Datel Modem andthence to a G.P.O. telephone line, and we havedemonstrated this. It may be desirable, however,to monitor a patient having a transient cardiacdysrhythmia over periods such as a normal workingday. In this situation it is convenient for the patientto wear a miniature tape recorder which will recordthe electrocardiogram (Holter, 1961).
In the field ofpatient-monitoring in cardiac infarc-tion, we consider that telemetry may eventually re-place conventional methods. Both clinical observa-tion and the volunteered statements of patients whohave survived critical cardiac infarction indicate be-yond doubt that frightening electronic equipmentand alarm signals at the bedside destroy equanimity,heighten emotional tension, and militate againstrecovery by rendering a susceptible patient evenmore liable than his disease dictates to the dangerousdysrhythmias which all too frequently determine anearly demise.Apart from aggravating emotional tension in a
seriously ill patient, there are the practical difficultiesin the nursing and emergency treatment of a patientwired to numerous instruments at the bedside.G. E. Godber (personal communication, 1966) hasstated that: "Telemetry in this field is certainly oneof the more important developments.... One ofour troubles in units for acute cardiac infarction is
697
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Lewes and Hill
the ease with which leads become detached ... andso one does look to this sort of development as soonas possible."The superior records that may be obtained by
multipoint electrodes during physical exercise, com-pared with those given by conventional jelly elec-trodes, point the way to the ideal form of multipointelectrode which should be developed in the immedi-ate future. The electrode should be as small aspossible yet capable of a low skin-contact resistanceby embodying the maximum number of points perunit area, each of which can penetrate the insulatingkeratinized skin layer. It should require neitherjelly nor paste and be dry, apart from the accumula-tion of natural sweat and electrolytes beneath itssurface, so that it may be left in position for days orweeks, a necessity, for example, during prolongedobservation in the compression chamber or in astro-nauts.Both for long-term patient-monitoring and during
exercise studies, it is desirable to stick the electrodeto the skin surface with a non-irritant glue. Wehave used the same glue as Boter et al. (1966), butwe have been able to keep a multipoint electrodeglued to a patient for four months, whereas theelectrodes of Boter et al., using the glue plus an elec-trode jelly, often exhibit a skin reaction after 24hours. This suggests that for long-term use thechoice of jelly is important. Kahn (1965) and Boteret al. (1966) have designed ingenious electrodes toovercome the artefacts arising from the relativemotion of the electrode and jelly. This problemdoes not arise with multipoint electrodes since jellyor paste is not used. More recently Fluck andBurgess (1966) have developed press-stud non-irri-tant jelly chest electrodes for continuous monitoringfor periods of a week or more, which they state yielda stable electrocardiogram when the patient ismoving.The present multipoint electrodes are relatively
crude and may exhibit initial contact impedances ofup to 10 kQ at 20 c.p.s. This value of impedance,nevertheless, is satisfactory for use with modemelectrocardiographs having input impedances of1 MQ or more, and central terminal averagingresistors substantially higher than 10 kQ.The National Aeronautics and Space Administra-
tion, Washington D.C. (1966), have now developeda simplified and improved method for recording theelectrocardiogram and other biological data in testpilots, which replaces bulky sensors requiringshaving and messy creams. Roman (1966) andPatten, Ramme, and Roman (1966) have perfectedhigh-impedance electrode techniques in which thebare end of a teflon-covered copper wire four-thousandths of an inch in diameter is captured in a
conductive fast-drying glue rich in metallic silverwhich is sprayed on to the chest wall. The elec-trode area 19 mm. in diameter and 0 5 mm. in thick-ness is covered by a thin coat of an insulating spraywhich dries immediately. Application of one elec-trode, including skin preparation, averages 20seconds. These electrodes have been used success-fully during 700 hours of flight recording and 500hours of records from working subjects on theground.The above reports from The National Aero-
nautics and Space Administration and evidence todate ofthe practical value ofthe multipoint electrodesuggests that a dry electrode requiring no skinpreparation is likely to replace conventional jellymethods both for telemetry and for routine electro-cardiography.
SUMMARYAn experimental dry multipoint chest electrode
requiring no skin preparation with electrode jelly orpaste has been used successfully in a preliminarystudy of patient-monitoring in cardiac infarction byradio-telemetry and for the assessment of cardiacstatus during physical exercise.The equipment used and the methods employed
are described. The battery-operated British tele-metry system, which may be purchased for less thanthe cost of a modem single-channel electrocardio-graph, will permit intermittent monitoring for about50 hours and, when used continuously, for approxi-mately 10 hours. Batteries which are inexpensivemay be quickly replaced.
It is considered that patient-monitoring by tele-metry should replace current methods which mayincrease the emotional tension and anxiety ofseriously ill patients already predisposed by cardiacinfarction to dangerous cardiac dysrhythmias, andat the same time render emergency treatment at thebedside difficult.
Radio-telemetry is obligatory for the electrocardio-graphic assessment of cardiac fimction during physi-cal exercise which precludes the use of conventionalelectrocardiography, and is of value in helping toestablish more valid criteria which will assist theinvestigation of cardiovascular disease.
We wish to thank Mr. E. P. Childerhouse and Mr.R. S. Mark of Medical and Industrial Equipment Ltd.,and Dr. A. Rooker of Aveley Electronics Ltd. for loaningradio-telemetry equipment, and Mr. A. Stevenson ofLouis Newmark Ltd. for providing transistorized elec-trocardiographs for this study. The assistance of theG.P.O. is gratefully acknowledged, and we thankHewlett-Packard Ltd. and Texas Instruments Ltd.,Bedford, who made the electrodes, for their help andco-operation.
698
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from

Application of Multipoint Electrodes to Telemetry in Patient-monitoring
This investigation was supported by research awardsfrom The British Heart Foundation and The North-West Metropolitan Regional Hospital Board to one of us(D. L.), who wishes to thank Dr. William Evans for hisencouragement and advice in carrying out this researchand in the preparation of this paper.The multipoint electrode is subject to U.K. Patent
Applications No. 52253/64 and 44049/65, and in theU.S.A. under the protection of the National ResearchDevelopment Corporation, Victoria Street, London.R. Ward (Turned Parts) Ltd. of Aberystwyth, andHewlett-Packard Ltd. in Edinburgh and Palo Alto,California, U.S.A., are carrying out further developmentof the multipoint electrode which they intend to producecommercially in the near future.
REFERENCESBellet, S., Eliakim, M., Deliyiannis, S., and LaVan, D. (1962).
Radioelectrocardiography during exercise in patientswith angina pectoris. Circulation, 25, 5.
Boter, J., den Hertog, A., and Kuiper, J. (1966). Distur-bance-free skin electrodes for persons during exercise.Med. biol. Engng., 4, 91.
Ernsting, J. (1966). Multipoint electrocardiography.Lancet, 1, 1429.
Fluck, D. C., and Burgess, P. A. (1966). A press-stud elec-
trode for continuous monitoring of the electrocardio-gram. Lancet, 1, 1405.
Hill, D. W. (1966). Transmitting physiological signals bytelephone. World med. Electron., 4, 108.
Holter, N. J. (1961). New method for heart studies.Science, 134, 1214.
Kahn, A. (1965). Motion artefacts and streaming potentialsin relation to biological electrodes. Digest of 6th. Int.Conf. Med. Electron., Biol. Engng, Tokyo, p. 562.
Keen, H., and Johnson, V. (1966). Multipoint electrocardio-graphy. Lancet, 2, 109.
Lewes, D. (1965). Multipoint electrocardiography withoutskin preparation. Lancet, 2, 17.(1966). Multipoint electrocardiography without skinpreparation. World med. Electron., 4, 240.
National Aeronautics and Space Administration, WashingtonD.C. (1966). Release no. 66-116 (May 17).
Patten, C. W., Ramme, F. B., and Roman, J. (1966). Dryelectrodes for physiological monitoring. NASA Tech-nical Note (NASA, TN D-3414).
Robertson, D. (1937). The examination and recording of thehuman electrocardiogram by means of the cathode-rayoscillograph. J. Instn. elect. Engrs., 81, 497.
Roman, J. (1966). High impedance electrode techniques.Aerospace Med., 37, 790.
Stock, P. (1966). Multipoint electrocardiography. Lancet,1, 1042.
Turner, R. W. D. (1966). Multipoint electrocardiography.Lancet, 1, 1158.
Wilton-Davies, C. C. (1966). Multipoint electrocardio-graphy. Lancet, 1, 1209.
699
on March 9, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.29.5.689 on 1 Septem
ber 1967. Dow
nloaded from