Embed Size (px)
Citation preview


2
Objectives
Objectives Methodology Results Discussion
How are changes in the prices of drugs (either through the
introduction of generics or subsidization by a third party) will affect
the demand?
⇰ To forecast demand for HCV medication under several
scenarios (over a 10-year period)
⇰ To assess the responsivenness of the demand for HCV
medication to changes in prices of the medicines

3
Outline
⇰ Methodological Approach
o Mathematical Model
⇰ Two Base Cases for Treatment Cascade
o Current Best Regimen vs. Future Best Regimen
⇰ Two Financing Scenarios
o Free-Market vs. Third Party Coverage
⇰ Working Assumptions ⇰ Main Results:
o Low-income, Lower-Middle & Upper-middle income countries
⇰ Sensitivity Analysis
⇰ Discussion & Policy Recommendations
Objectives Methodology Results Discussion

4
Methodological Approach
Objectives Methodology Results Discussion
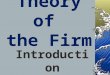
⇰ A Susceptible-Infected-Removed (SIR) Model (e.g. Elbasha 2013):
⟿ New infections are assumed to be of the naïve nature (No re-
infection)
⟿ Population is assumed to mix homogeneously
N
Susceptible S
Acutely infected I
Immune R
Chronically infected Fm

5
Methodological Approach
x
Acute
HCV
I(t)
μ
Recovered
R(t) Mortality Unrelated to HCV
μ
Susceptible
S(t)
ν
μ
F0(t)
μ
ε1 F1(t)
μ
ε2 F2(t)
μ
ε3 F3(t)
μ
ε4 F4(t) ε0
μ
σ
λ
Objectives Methodology Results Discussion

6
Methodological Approach
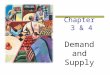
⇛ The chronically infected go through the diagnosis cascade starting with HCV
detection and ending once treatment is accepted.
Objectives Methodology Results Discussion
Outline of the Stages of Detection, Referral to Care and Treatment
Health
System
Absorption
Capacity
Ability-to-
Pay
Price
Elasticity
of Demand
(Among
those with
ATP)
Treatment
Received
α'5
Chronically
Infected
α1
HCV
Detected
α2
Referred
to Care
α3 Fibrosis
Staging
α4
Medically
Eligible
Patients
(based on
scenarios)
α"5
α'"5
α5

7
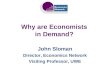
Methodological Approach: Diagnosis Rate (r0 = α1*α2*α3)
⇛ Diagnosis rate reflects the probability that a chronically infected individual would have ⟿ had HCV detected ⟿ been referred to care and ⟿ gone through fibrosis staging. ⇛ For the current best case, this rate (r0) is assumed to be 5% in the year 2013
⇛ For the future best case, this rate (r0) is assumed to be 15% in the year 2013
Objectives Methodology Results Discussion
Stage 2013 to
2014 2014 to
2015 2015 to
2016 2016 to
2017 2017 to
2018 2018 to
2019 2019 to
2020 2020 to
2021 2021 to
2022 2022 to
2023 Acute 0,1% 0,1% 0,1% 0,2% 0,2% 0,2% 0,2% 0,3% 0,3% 0,4%
F0 0,5% 0,6% 0,7% 0,8% 0,9% 1,0% 1,2% 1,3% 1,5% 1,8% F1 1,0% 1,2% 1,3% 1,5% 1,7% 2,0% 2,3% 2,7% 3,1% 3,5% F2 2,5% 2,9% 3,3% 3,8% 4,4% 5,0% 5,8% 6,7% 7,6% 8,8% F3 10,0% 11,5% 13,2% 15,2% 17,5% 20,1% 23,1% 26,6% 30,6% 35,2% F4 15,0% 17,3% 19,8% 22,8% 26,2% 30,2% 34,7% 39,9% 45,9% 52,8%
Stage 2013 to
2014 2014 to
2015 2015 to
2016 2016 to
2017 2017 to
2018 2018 to
2019 2019 to
2020 2020 to
2021 2021 to
2022 2022 to
2023 Acute 5,0% 5,8% 6,6% 7,6% 8,7% 10,1% 11,6% 13,3% 15,3% 17,6% F0 10,0% 11,5% 13,2% 15,2% 17,5% 20,1% 23,1% 26,6% 30,6% 35,2% F1 15,0% 17,3% 19,8% 22,8% 26,2% 30,2% 34,7% 39,9% 45,9% 52,8% F2 20,0% 23,0% 26,5% 30,4% 35,0% 40,2% 46,3% 53,2% 61,2% 70,4% F3 25,0% 28,8% 33,1% 38,0% 43,7% 50,3% 57,8% 66,5% 76,5% 80,0% F4 35,0% 40,3% 46,3% 53,2% 61,2% 70,4% 80,0% 80,0% 80,0% 80,0%

8
Methodological Approach: Eligibility(α4)
⇛ The probability that an individual will be offered treatment is based on their eligibility for treatment.
⇛ All individuals eligible for treatment are offered treatment after fibrosis staging.
⟿ α4 is the probability that the individual will fulfil the eligibility criteria (depending on WHO (2014) guidelines).
⇛ Scope of eligibility for treatment:
⟿ Initial analysis: only fibrosis stage F3 & F4
⟿ Sensitivity analysis: treatment of everyone who is chronically infected
(F0 to F4).
Objectives Methodology Results Discussion

9
Methodological Approach: Treatment Rate (α5)
⇛ Individuals are at liberty to either accept or refuse treatment based on conditions:
⟿ Side effects of the drug (acceptability of treatment)
⟿ Costs involved (Ability-to-Pay (ATP))
⇛ Sensitivity analysis to take into account differential acceptability of treatment &
various thresholds for ATP
Objectives Methodology Results Discussion
In the Two Cases: ⟿ Number of people willing and able to accept treatment depends on
three factors:
oHealth System’s Absorption Capacity (AC) 𝛂’5
o Individuals’ Ability-To-Pay (ATP) 𝛂’’5
oPrice elasticity of demand (𝛏dq) 𝛂’’’5
Treatment rate 𝛂5

1
0
Methodological Approach: Treatment Rate (α5)
Objectives Methodology Results Discussion
⇛ For the current best case, the initial absorbtion capacity of the health system is assumed to be 5% in the year 2013 and increasing (annually) by 5% over time, i.e. AC t = AC t-1+0.05.
⇛ For the future best case, the initial absorbtion capacity of the health system is
assumed to be 5% in the year 2013 and increasing (annually) by 15% over time, i.e. AC t = AC t-1+0.15 (with a maximum 80% capacity at end of period)
⇛ The price elasticity of demand measures the change in demand as a result of a 1
percent decrease in prices. ⟿For the current best case, it is assumed that elasticity is 0.9 for the
highest income quintile and reduces to 0.5 for the lowest income quintile in each country.
⟿For the future best case, it is assumed that elasticity is 0.9 irrespective of the income quintile.
⇛ Individuals are considered as able-to-pay for medication if the cost of the regimen represents at most 40% of their per-capita GDP.

1
1
Methodological Approach: Prices & Cost of Treatment
Objectives Methodology Results Discussion
⇛ For the initial analysis drugs are assumed to cost the same in all countries irrespective of their income levels. ⟿ Current lowest prices are used as the reference prices ⟿ Prices are assumed to fall by an annual rate of 3.4% as in the price of brand ARVs. ⟿The total cost of medication will depend on the genotype.
Genotype Medication Cost (12 Weeks) in
USD Recommended
Duration (Weeks)
1, 4 Sofosbuvir 840
12
Current Best WHO (2014)
Ribavirin 53
Peg-IFN 500
2 Sofosbuvir 840 12
Ribavirin 53
3 Sofosbuvir 840 24
Ribavirin 53
All Genotypes Sofosbuvir 840
12 Future Best Another DAA 420

1
2
⊛ Treatment Module: Two FINANCING Scenarios: (Free Market vs. Subsidised)
Objectives Methodology Results Discussion
⧆ Free Market Prices: ↪ Demand for drugs depends on ATP ⧇ Subsidised:
↪ Third party willing to cover a fraction of the avg. costs (say, e.g., 50%) ↪ Demand for drugs based on ATP after subsidies have been applied.
Major sensitivity analysis
⟿ Changes in Eligibility Criteria
⟿ Changes in third-party subsidies
⟿ Changes in ATP thresholds
⟿ Changes in price reduction rates

1
3
⊛ Countries Used in Analysis
Objectives Methodology Results Discussion
Low Income
Countries
($664)
Lower-Middle Income
Countries
($2751)
Upper Middle Income
Countries
($9025)
Included Benin, Burkina Faso, Gambia, Guinea, Guinea Bissau,
Liberia, Mali, Mauritania, Niger, Sierra Leone, Togo, Central African Republic,
Chad, Democratic Republic of Congo, Burundi, Comoros,
Ethiopia, Kenya, Madagascar, Malawi, Mozambique,
Rwanda, Tanzania, Uganda, Zimbabwe, Haiti, Afghanistan,
Bangladesh, Nepal, Cambodia, Kyrgyz Republic,
Tajikistan
Cape Verde, Côte d’Ivoire, Ghana, Nigeria, Senegal, Cameroon, Congo, São Tomé & Principe, Lesotho, Swaziland, Djibouti, Zambia, Egypt, Morocco, Iraq,
Sudan, Yemen, Bolivia, Paraguay, Belize, El Salvador, Guatemala, Honduras, Nicaragua, Guyana,
Pakistan, India, Bhutan, Sri Lanka, Indonesia, Lao People’s Democratic Republic, Philippines, Vietnam, Fiji,
Papua New Guinea, Armenia, Georgia, Moldova, Ukraine,
Uzbekistan, Albania, Mongolia
Angola, Gabon, Botswana, Namibia, South Africa,
Seychelles, Algeria, Islamic Republic of Iran, Jordan, Tunisia,
Argentina, Brazil, Chile, Colombia, Ecuador, Peru,
Uruguay, Venezuela, Costa Rica, Mexico, Panama, Dominican Republic, Jamaica, Suriname, Maldives, Malaysia, Thailand,
China, Azerbaijan, Belarus, Kazakhstan, Turkmenistan,
Russia, Bosnia & Herzegovina, Serbia, Montenegro, The Former Yugoslav Republic of Macedonia,
Turkey, Bulgaria, Latvia, Lithuania, Romania
Excluded Eritrea, Democratic Republic of Korea, Myanmar, Somalia
Kiribati, Kosovo, Marshall Islands, Federal States of Micronesia,
Samoa, Solomon Islands, South Sudan, Syrian Arab Republic,
Timor-Leste, Tonga, Vanuatu, West Bank & Gaza
Cuba, Dominica, Grenada, Lebanon, Libya, Mauritius, Palau,
St. Lucia, St. Vincent and the Grenadine, Tuvalu

1
4
⊛ Data Sources
Objectives Methodology Results Discussion
Data & Variables Data Sources
⌛ Economic-related Data ⟿ Share of GDP held by each quintile (income per capita (share of GDP /# of i's in each q) ⟿ GDP ⬆ overtime
World Development Indicators (WDI) International Monetary Fund’s World Economic
Outlook Database (April 2014)
⌛ Population related Data: ⟿ size, mortality, growth rate
World Development Indicators (WDI) WB Projection Tables; World Health Statistics (2013)
⌛ Prices of medication ⌛ Recommended therapy per genotype
WHO guidelines (2014), Open Society pharmaceutical companies & other media sources
⌛ Transition probabilities exogenous & given by the natural history of the disease
⌛ Incidence rates exogenous and obtained from literature
⌛ Sensitivity Parameters: ⟿ treatment option, rate & type of third party coverage, & rate of price decrease)
exogenously determined but allowed to vary based on assumptions made
NA: extrapolated using geography, genotypes, GDP

15
⌛Main Results⌛
Some Definitions
•Medication Expenditure: This refers to the total (cumulative) expenditure on drugs at the end
of the period.
•Cost of Regimen: This is the average cost of the drug regimen at the end of the period for end-
user (patient).
Objectives Methodology Results Discussion

16
Results: Base case of Low Income Countries (LICs) [price decrease = 3.4, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Objectives Methodology Results Discussion
Current Best Future Best
LIC LIC Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 32 075 37 798 657 1 166 Free Market
By 2018 137 451 154 849 029 1 097 Free Market
By 2023 382 208 401 162 603 981 By 2023 950 173 948 104 095 923 By 2018 299 055 362 184 232 583 Subsidised
50% By 2018 693 806 798 787 520 549 Subsidised
50% By 2023 1 600 895 1 716 199 586 490 By 2023 2 171 704 2 245 180 280 461
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

⟿ LIC markets are and will remain limited in size - there are fewer and fewer LICs
- HVC prevalence is relatively low
⟿ In the most pessimistic scenario (current best regimen, free market) there will still be
over 380.000 patients treated by 2023, for 400 Million USD over 10 years
⟿ In the most optimistic scenario (future best regimen, 50% subsidy) there would be
almost 2.2 million people treated by 2013, for 2.2 Billion USD over 10 years.
⟿ In none of 4 scenarios we see the number of new patients treated annually decline
over time.
⟿ Alternative actions (steeper price declines, higher levels of subsidy, improved
diagnostic access and health system performance are needed to realize meaningful
impact on the epidemic in LIC.
17
Lessons from LIC Base Case Scenarios
Objectives Methodology Results Discussion

18
Results: Base case of Lower-Middle Income Countries (LMICs) [price decrease = 3.4, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Objectives Methodology Results Discussion
Current Best Future Best
LMIC LMIC Cummulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cummulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 2 996 937 3 815 860 410 1 233 Free Market
By 2018 8 613 412 9 965 213 852 1 097 Free Market
By 2023 13 085 821 14 923 572 220 1 037 By 2023 19 660 396 20 902 839 829 923 By 2018 6 606 014 8 505 262 636 617 Subsidised
50% By 2018 16 193 401 18 830 253 427 549 Subsidised
50% By 2023 24 539 091 28 684 844 550 519 By 2023 30 070 869 32 627 246 899 461
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

⟿ LMIC markets will be massive
⟿ In the most pessimistic scenario (current best regimen, free market) over 13 Million
patients will have been treated by 2023, for a total of almost 15 Billion USD over 10
years.
⟿ In the most optimistic scenario (future best regimen, 50% subsidy) over 30 Million
patients will have been treated, for a total of almost 33 Billion USD over 10 years
⟿ The number of new patients treated decline over time only in the future best regimen
case scenarios with 50% subsidy (most optimistic)
⟿ For public health impact either lower prices than projected, or subsidy for treatment
will be needed, along with improved access to diagnostics and health system
performance.
19
Lessons from LMIC Base Case Scenarios
Objectives Methodology Results Discussion

20
Objectives Methodology Results Discussion
Results: Base case of Upper-Middle Income Countries (UMICs) [price decrease = 3.4, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Current Best Future Best
UMIC UMIC Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 7 930 697 10 095 540 115 1 204 Free Market
By 2018 19 553 810 22 930 786 148 1 097 Free Market
By 2023 23 122 496 26 712 822 039 1 012 By 2023 28 459 792 31 761 059 115 923 By 2018 9 775 460 12 421 029 900 602 Subsidised
50% By 2018 23 552 170 27 660 696 916 549 Subsidised
50% By 2023 25 650 001 29 882 590 436 506 By 2023 29 540 482 33 692 538 796 461
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

⟿ UMIC markets will be massive too and may reach saturation of demand by 2023
⟿ In the most pessimistic scenario (current best regimen, free market) over 23 Million
patients will have been treated by 2023, for a total of over 26 Billion USD over 10
years.
⟿ In the most optimistic scenario (future best regimen, 50% subsidy) over 29 Million
patients will have been treated, for a total of over 33 Billion USD over 10 years
⟿ The number of new patients treated declines over time in all scenarios.
⟿ For impact on the epidemic, better performance in case finding and health system
organization will be needed than in the current best regimen scenario. Subsidy would
improve the impact marginally.
21
Lessons from UMIC Base Case Scenarios
Objectives Methodology Results Discussion

22
Objectives Methodology Results Discussion
Results: Base case of All Countries [price decrease = 3.4, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Current Best Future Best
Low-to-Middle Income Low-to-Middle Income Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
CumUlative Number Treated
Medication Expenditure ($)
Cost of Regimen
($) By 2018 10 959 710 13 949 199 182 1 208 Free
Market By 2018 28 304 673 33 050 849 029 1 107 Free
Market By 2023 36 590 525 42 037 556 862 1 016 By 2023 49 070 361 53 612 003 039 931 By 2018 16 680 529 21 288 476 768 604 Subsidised
50% By 2018 40 439 377 47 289 737 863 553 Subsidised
50% By 2023 51 789 987 60 283 634 573 508 By 2023 61 783 055 68 564 965 975 465
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

⟿LIC markets will be small - additional price decreases, better
diagnostic/health system performance and high levels of subsidy are
needed to have a meaningful public health impact
⟿ LMIC and UMIC markets will be massive
⟿ In LMIC, third party coverage would boost demand (X2.0 to X3.0)
In LMIC, impact on the epidemic will require both greater price decreases
than projected, better access to diagnostics and health system organization;
⟿ In UMIC saturation of demand, high coverage, and impact on the epidemic
may be reached if diagnostics and health system organization can be
improved, and subsidy will impact demand in a limited way.
⟿ Comparison of "current" and "future" best regimen case scenarios suggests
that simplification in drug regimens and access to diagnostics might boost
LIC, LMIC and UMIC markets in the next 5 years (X 2.5 to X4.0) and
increase demand at the 2023 horizon.
23
Summary: Lessons from Base Case Scenarios
Objectives Methodology Results Discussion

24
Sensitivity Analysis:
Expand eligibility for treatment
from F3-F4 to F0-F4
Objectives Methodology Results Discussion
Main Lesson
In all cases, demand would be very sensitive to an extension of current
treatment eligibility guidelines.
If it happened now, there would be, in L+MIC combined, by the end of 2023:
57 million people treated, compared to 36.5 million in the current best regimen
case/free market baseline scenario
198 million people treated, compared to 62 million in the future best regimen
case/50% subsidy baseline scenario

25
Results: Base case of Lower-Middle Income Countries (LMICs) [price decrease = 3.4, subsidy = 50%, Treatment Group = F0 to F4, ATP =40%]
Objectives Methodology Results Discussion
Current Best Future Best
LMIC LMIC Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 4 164 082 5 280 333 248 1 233 Free Market
By 2018 25 093 120 28 829 997 752 1 097 Free Market By 2023 22 677 558 25 448 559 537 1 037 By 2023 79 299 298 82 336 253 704 923
By 2018 9 370 928 11 997 202 592 617 Subsidised 50%
By 2018 51 745 204 59 670 005 575 549 Subsidised 50% By 2023 43 763 614 50 128 875 779 519 By 2023 131 398 116 138 651 692 810 461
Sensitivity F0 to F4
Number of Individuals Treated (Annual) in ‘000s
Base Case F3 to F4
Number of Individuals Treated (Annual) in ‘000s

26
Objectives Methodology Results Discussion
Results: Base case of All Countries [price decrease = 3.4, subsidy = 50%, Treatment Group = F0 to F4, , ATP =40%]
Current Best Future Best
Low-to-Middle Income Low-to-Middle Income Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 14 329 479 18 194 647 956 1 208 Free Market
By 2018 66 775 765 77 468 459 288 1 107 Free Market
By 2023 57 409 964 65 130 922 767 1 016 By 2023 155 415 975 165 042 152 868 931 By 2018 22 256 235 28 317 898 252 604 Subsidised
50% By 2018 105 133 961 122 000 893 547 553 Subsidised
50% By 2023 84 458 350 96 800 688 559 508 By 2023 197 920 762 204 900 065 654 465
Sensitivity F0 to F4
Number of Individuals Treated (Annual) in ‘000s
Base Case F3 to F4
Number of Individuals Treated (Annual) in ‘000s

27
Sensitivity Analysis: Subsidy Rate 0% - 100% (25% Interval)
Objectives Methodology Results Discussion
Main Lesson
Free of charge drugs for end-users at the point of delivery (100% subsidy)
would be required to have a significant impact on the number of annual cases
in need of treatment in LIC.
High-level of third-party coverage (≥ 75% subsidy) would be needed to boost
demand (X2.0 or more) in LMIC.
This is shown in the current best regimen case scenarios in the next 3 slides.

28
Results: Sensitivity Analysis of Low Income Countries (LICs) [price decrease = 3.4, subsidy = 0% - 100%, Treatment Group = F3 to F4, ATP =40%] Current Best
Objectives Methodology Results Discussion
Current Best Current Best
By 2018 LIC By 2023 LIC
Subsidy Cumulative
Number Treated
Medication Expenditure
($)
Cost of Regimen ($)
Subsidy Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
0% 32 609 38 423 765 1 166 0% 397 495 416 914 125 981 25% 102 772 123 913 117 874 25% 775 667 820 740 040 735 50% 299 055 362 184 232 583 50% 1 600 895 1 716 199 586 490 75% 931 776 1 130 756 487 291 75% 4 201 765 4 540 084 705 245 100% 4 122 755 4 978 565 682 0 100% 10 705 603 11 836 440 879 0
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

29
Results: Sensitivity Analysis of Lower-Middle Income Countries (LMICs) [price decrease = 3.4, subsidy = 0% - 100%, Treatment Group = F3 & F4] Current Best
Objectives Methodology Results Discussion
Current Best Current Best
By 2018 LMIC By 2023 LMIC
Subsidy Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
Subsidy Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
0% 3 060 995 3 894 338 396 1 233 0% 13 593 409 15 468 255 426 1 037 25% 4 609 513 5 926 929 458 925 25% 17 594 130 20 272 215 366 778 50% 6 606 014 8 505 262 636 617 50% 24 539 091 28 684 844 550 519 75% 11 070 840 14 581 070 999 308 75% 34 377 849 40 968 808 505 259 100% 14 072 595 18 545 573 989 0 100% 36 955 349 44 499 146 459 0
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

30
Sensitivity Analysis: Rate of Price Reduction 25% (2014-
2016) then 5.2%
Objectives Methodology Results Discussion
Main Lesson
•⟿ In LIC, an initial “price shock” would help create a significant market
The value of the LIC market will reach almost 1billion US$ in the most pessimistic scenario (current best case/free market) compared to 400 Million over 10 years in the base case, without "price shock“
⟿ In LMIC, it will increase access to treatment by a factor of 1.5 to 2.0, while
maintaining total value of market over the next ten years
⟿ In UMIC, it will increase demand by 30% to 50% in the next five years
(without affecting total $ value of market). It will reach similar levels of
coverage at the 2023 horizon (with circa 15% to 25% decrease in total $
market value)
⟿ Prices would still be well above the marginal costs at the 2023 horizon for
DAA-only treatment

31
Results: Base case of Low Income Countries (LICs) [price decrease = 25% (2014-2016) then 5.2%, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Objectives Methodology Results Discussion
Current Best Future Best
LIC LIC Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 227 882 166 402 918 677 Free Market
By 2018 626 556 435 200 510 637 Free Market
By 2023 1 617 499 951 020 996 518 By 2023 2 743 006 1 570 501 423 488 By 2018 913 270 680 810 757 338 Subsidised
50% By 2018 1 859 570 1 350 129 733 318 Subsidised
50% By 2023 4 302 163 2 612 181 020 259 By 2023 5 202 940 3 157 593 207 244
Sensitivity 25% decrease (2014-2016) then 5.2%
price decrease
Number of Individuals Treated (Annual) in ‘000s
Base Case 3.4% price decrease
Number of Individuals Treated (Annual) in ‘000s

32
Results: Base case of Lower-Middle Income Countries (LMICs) [price decrease = 25% (2014-2016) then 5.2%, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Objectives Methodology Results Discussion
Current Best Future Best
LMIC LMIC Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 6 602 310 5 283 687 069 716 Free Market
By 2018 14 943 103 11 281 629 789 637 Free Market
By 2023 24 157 270 16 113 287 505 548 By 2023 30 654 679 19 885 788 946 488 By 2018 12 599 899 10 426 181 482 358 Subsidised
50% By 2018 24 119 479 18 849 357 477 318 Subsidised
50% By 2023 35 089 176 24 503 565 392 274 By 2023 38 503 177 26 776 480 939 244
Sensitivity 25% decrease (2014-2016) then 5.2%
price decrease
Number of Individuals Treated (Annual) in ‘000s
Base Case 3.4% price decrease
Number of Individuals Treated (Annual) in ‘000s

33
Objectives Methodology Results Discussion
Results: Base case of Upper-Middle Income Countries (UMICs) [price decrease = 25% (2014-2016) then 5.2%, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Current Best Future Best
UMIC UMIC Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 11 777 910 9 553 864 619 699 Free Market
By 2018 23 494 442 19 227 713 680 637 Free Market
By 2023 26 398 485 18 461 980 178 535 By 2023 29 563 287 22 622 144 642 488 By 2018 12 933 821 10 602 263 121 349 Subsidised
50% By 2018 23 756 967 20 081 649 149 318 Subsidised
50% By 2023 26 418 170 18 844 086 380 268 By 2023 29 467 175 23 268 590 605 244
Sensitivity 25% decrease (2014-2016) then 5.2%
price decrease
Number of Individuals Treated (Annual) in ‘000s
Base Case 3.4% price decrease
Number of Individuals Treated (Annual) in ‘000s

34
Objectives Methodology Results Discussion
Results: Base case of All Countries [price decrease = 25% (2014-2016) then 5.2%, subsidy = 50%, Treatment Group = F3 & F4, ATP =40%]
Current Best Future Best
Low-to-Middle Income Low-to-Middle Income Cumulative
Number Treated
Medication Expenditure ($)
Cost of Regimen
($)
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
By 2018 18 608 102 15 003 954 605 701 Free Market
By 2018 39 064 101 30 944 543 980 642 Free Market
By 2023 52 173 254 35 526 288 679 537 By 2023 62 960 972 44 078 435 011 492 By 2018 26 446 989 21 709 255 361 351 Subsidised
50% By 2018 49 736 015 40 281 136 359 321 Subsidised
50% By 2023 65 809 509 45 959 832 793 268 By 2023 73 173 292 53 202 664 751 246
Sensitivity 25% decrease (2014-2016) then 5.2%
price decrease
Number of Individuals Treated (Annual) in ‘000s
Base Case 3.4% price decrease
Number of Individuals Treated (Annual) in ‘000s

35
Sensitivity Analysis: Ability-to-Pay 10% - 50% (10% Interval)
Objectives Methodology Results Discussion
Main Lesson
⟿ Results are quite robust to economic uncertainties on the demand-side :
they are only moderately sensitive to assumptions about elasticity of demand
to price under households’ budgetary constraints (ability-to-pay).
⟿ However, monitoring of patients’ actual preferences and behaviors will
remain key for scaling up access to treatment.

36
Results: Base case of Lower-Middle Income Countries (LMICs) [price decrease = 3.4, Treatment Group = F3 & F4, ATP = 10% - 50%] Free Market Current Best
Objectives Methodology Results Discussion
Current Best Current Best
By 2018 LMIC By 2023 LMIC
ATP Cumulative Number
Treated Medication Expenditure
($) Cost of
Regimen ($) ATP
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
10% 102 412 129 393 235 1 233 10% 1 600 011 1 726 601 121 1 037 20% 878 543 1 106 010 591 1 233 20% 5 112 034 5 690 018 998 1 037 30% 1 601 150 2 007 741 934 1 233 30% 9 667 006 10 861 429 547 1 037 40% 2 996 937 3 815 860 410 1 233 40% 13 085 821 14 923 572 220 1 037 50% 4 154 053 5 326 640 212 1 233 50% 16 246 509 18 686 068 921 1 037
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

37
Results: Base case of Lower-Middle Income Countries (LMICs) [price decrease = 3.4, Treatment Group = F3 & F4, ATP = 10% - 50%] Free Market Future Best
Objectives Methodology Results Discussion
Future Best Future Best
By 2018 LMIC By 2023 LMIC
ATP Cumulative
Number Treated Medication Expenditure
($) Cost of
Regimen ($) ATP
Cumulative Number Treated
Medication Expenditure ($)
Cost of Regimen ($)
10% 141 202 160 422 457 1 097 10% 3 640 066 3 591 103 257 923 20% 2 492 557 2 890 841 608 1 097 20% 9 952 737 10 158 847 036 923 30% 5 299 542 6 072 426 421 1 097 30% 15 790 197 16 455 983 462 923 40% 8 613 412 9 965 213 852 1 097 40% 19 660 396 20 902 839 829 923 50% 11 013 613 12 800 267 111 1 097 50% 23 318 367 24 966 796 915 923
Number of Individuals Treated (Annual) in ‘000s Cumulative Number of Individuals Treated in ‘000s

⟿ Model does not take into account potential re-infections and is limited to initial
treatment initiation.
⟿ Model does not fully take into account the impact of treatment on rates of
transmission (incidence remains exogenous).
⟿ There is an intrinsic difficulty in predicting ex-ante human behaviours and market
dynamics
⟿ Heterogeneity and uncertainty on epidemiological data used ?
⟿ Some assumptions on price dynamics derived from the experience of HIV/AIDS
drugs ?
38
Some limitations of the forecasting exercise
Objectives Methodology Results Discussion

⟿There is a significant opportunity for a massive scale up of access to HCV treatment
↪ ↑ in health system absorption capacity will be required.
↪ ↑ in treatment eligibility from F3-F4 to F0-F4 would greatly increase demand.
↪ a significant ↓ in initial drug prices is needed for LIC and LMIC, and should be
possible because it would increase the total value of the LIC and LMIC markets
over a 10 year horizon.
↪ significant subsidy will be needed in LIC markets and some subsidy in LMIC to
decrease the number of new cases needing treatment. The willingness to
subsidize will be greater if the drugs are more affordable – and would increase the
value of the market.
⟿ There is a rationale for adapting policies for HCV treatment access according to
countries’ level of development.
39
Some major lessons of the forecasting exercise
Objectives Methodology Results Discussion