Embed Size (px)
Citation preview

Approach to Bleeding
ยิง่ยง ชินธรรมมิตร์
คณะแพทยศาสตร์ศิริราชพยาบาล
วนัศุกร์ท่ี ๑๐ กมุภาพนัธ์ พ.ศ.๒๕๕๕
หมอ้หอ้มไมส้ัก ถ่ินรักพระลอ ช่อแฮศรีเมือง ลือเล่ืองแพะเมืองผ ีคนแพร่น้ีใจงาม

หวัขอ้
• Diagnostic approach

Diagnostic Approach to Bleeding
ตอบ 3 ค ำถำม

1. Local or Systemic Bleed ตอบ 3 ค ำถำม
Detail of Bleed
ทั้งปัจจุบันและอดีต,
ประจ ำเดือน
ค ำถำม เลือดออก... Local Systemic
ที่ใดบำ้ง Single site Multiple sites
มีกำรกระแทกหรือไม่
รุนแรงแคไ่หน
มีแผลที่จุดเลือดออก
อยู่แล้วหรือไม ่
Local injury /
pathology,
appropriate
bleeding to injury
Spontaneous or
inappropriate
bleeding to
injury
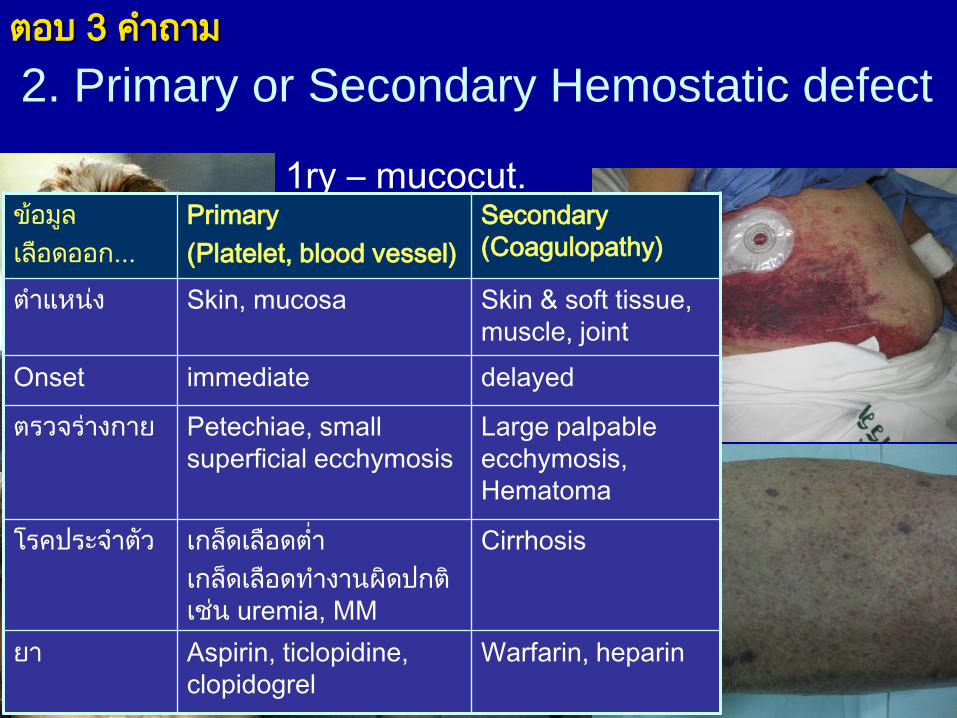
2. Primary or Secondary Hemostatic defect ตอบ 3 ค ำถำม
1ry – mucocut.
2ry – hematoma,
Large ecchymosis
ข้อมูล
เลือดออก...
Primary
(Platelet, blood vessel)
Secondary
(Coagulopathy)
ต ำแหนง่ Skin, mucosa Skin & soft tissue,
muscle, joint
Onset immediate delayed
ตรวจรำ่งกำย Petechiae, small
superficial ecchymosis
Large palpable
ecchymosis,
Hematoma
โรคประจ ำตวั เกล็ดเลือดต่ ำ
เกล็ดเลือดท ำงำนผิดปกติ
เช่น uremia, MM
Cirrhosis
ยำ Aspirin, ticlopidine,
clopidogrel
Warfarin, heparin

3. Inherited or Acquired Bleed ตอบ 3 ค ำถำม
Onset; Hx ถอนฟัน
ผ่ำตัด; family Hx;
โรคประจ ำตัว; ยำ

Local Bleeding
• Local Management
– Pressure
– Packing
– Cauterization
– Suture
– Ligation
– Embolization

Systemic Bleeding
Hemostatic
defect
Inherited Acquired
Primary
Secondary

Systemic Bleeding
Hemostatic
defect
Inherited Acquired
Primary PLT.dysfunction
(eg, vWD); etc.
PLT.ต่ ำ (eg, ITP, AA,
AL, TTP); uremia;
ASA,clopidogrel, etc.
Secondary

Systemic Bleeding
Hemostatic
defect
Inherited Acquired
Primary PLT.dysfunction
(eg, vWD); etc.
PLT.ต่ ำ (eg, ITP, AA,
AL, TTP); uremia;
ASA,clopidogrel, etc.
Secondary Hemophilia, etc. Cirrhosis, warfarin,
heparin, DIC, F.VIII
inhibitor, etc.

Lab
• Lab เบื้องต้น
–CBC
– Blood smear
–Coagulogram
• Lab เพิ่มเติม
– Bone marrow
study
–Mixing test
– Factor assay
– Platelet
aggregation test
– vWF panel

Thrombocytopenia R/O PLT. clumping
Clinical data Obvious causes:
- Inf.: Dengue, malaria, sepsis
- Autoimm.: SLE, Graves’
- Malig.: AL, NHL, AdenoCA
- Drug: CMT; XRT
- Cirrhosis: hypersplenism

Thrombocytopenia R/O PLT. clumping
CBC data
Hb WBC PLT Causes
N N Drug,ITP,chr.DIC (aortic aneurysm)
N
N
-
Clinical data
Heparin, antibiotics
(Betalactam, vancomycin,
rifampicin, bactrim), valproate, quinine, etc.

Thrombocytopenia R/O PLT. clumping
CBC data
Hb WBC PLT Causes
N N Drug,ITP,chr.DIC (aortic aneurysm)
N BM dis.(AL, MDS, Myelophthisis), TTP, Evans, SLE, DIC, PNH, ITP+bleed
N Dengue, drug, MDS, SLE
BM dis., SLE, hypersplenism, MA
- Sepsis, AL, CLL(+2oITP)
Clinical data
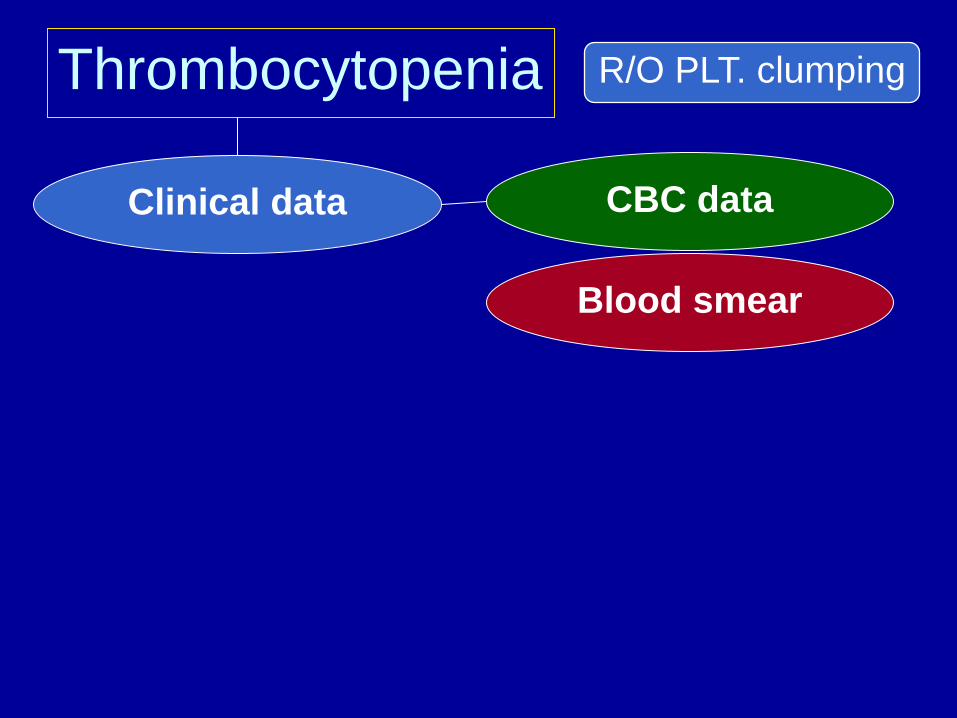
Thrombocytopenia R/O PLT. clumping
CBC data Clinical data
Blood smear

Spherocyte : Evans, SLE
Schistocyte
Fragmented red cell
:TTP, DIC, vasculitis, HELLP/preeclampsia

NRBC
Metamyelocyte
Leukoerythroblastic blood picture Myelophthisis Bone marrow study
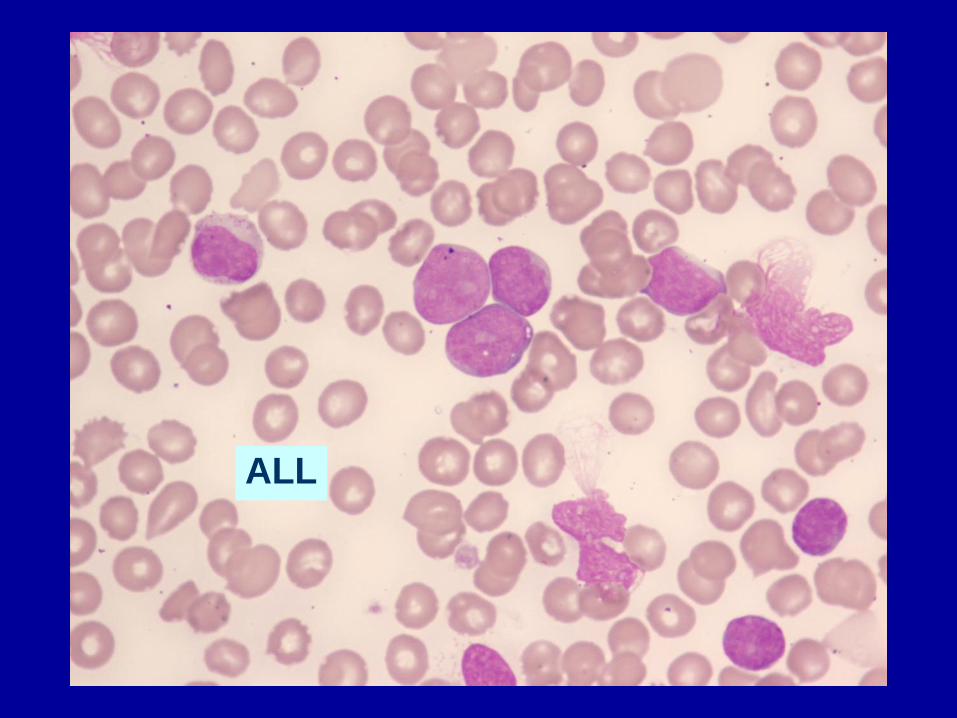
ALL

APL

CLL
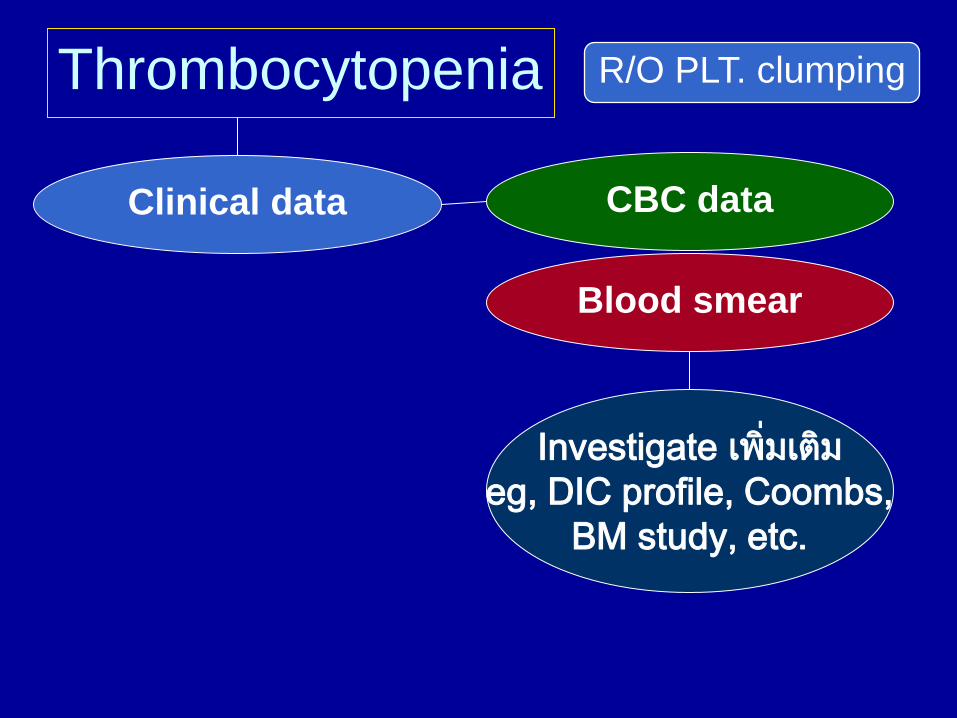
Thrombocytopenia R/O PLT. clumping
CBC data Clinical data
Blood smear
Investigate เพิ่มเตมิ
eg, DIC profile, Coombs,
BM study, etc.

Thrombocytopenia R/O PLT. clumping
CBC data Clinical data
Blood smear
Investigate เพิ่มเตมิ
eg, DIC profile, Coombs,
BM study, etc. Specific Rx
Supportive Rx
PLT transfusion 10 kg/bag contraindication: TTP, HIT
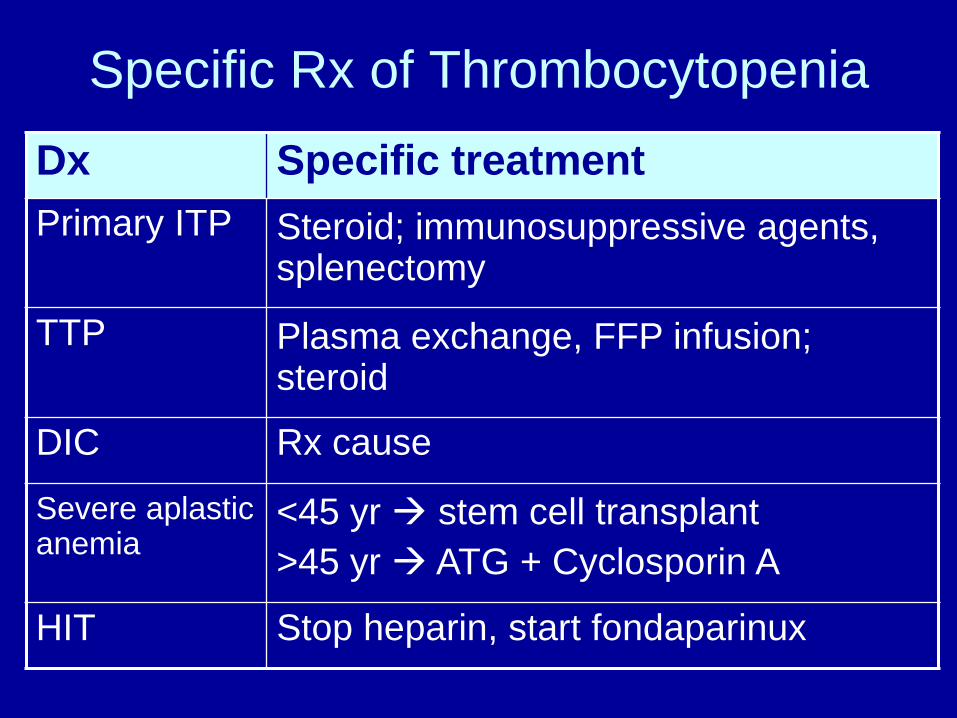
Specific Rx of Thrombocytopenia
Dx Specific treatment
Primary ITP Steroid; immunosuppressive agents, splenectomy
TTP Plasma exchange, FFP infusion; steroid
DIC Rx cause
Severe aplastic anemia
<45 yr stem cell transplant
>45 yr ATG + Cyclosporin A
HIT Stop heparin, start fondaparinux

Coagulopathy

F12a
F11a
F9a
F10a
F2a
Fibrin monomer / polymer
F7a
F8a F5a
TF
in vitro Coagulation
APTT PT
Thrombin time
Intrinsic pathway
Extrinsic pathway
Common pathway
HMWK PK

Prolonged PT, normal APTT Congenital
• F7 def
Acquired
• Liver dis
• Warfarin
• Vit. K def
F12a
F11a
F9a
F10a
F2a
Fibrin monomer / polymer
F7aF7a
F8a
F5a
TFTF
in vitro
Coagulation
APTT PPTT
Thrombin timeThrombin time
Intrinsic
pathwayExtrinsic pathwayExtrinsic pathway
Common pathwayCommon pathway
HMWK
PK F7 assay
Clinical Dx Try Rx + F/U
• DIC – clinical, d-dimer,
fibrinogen
• Def. of fibrinogen • F7 inhibitor – mixing test
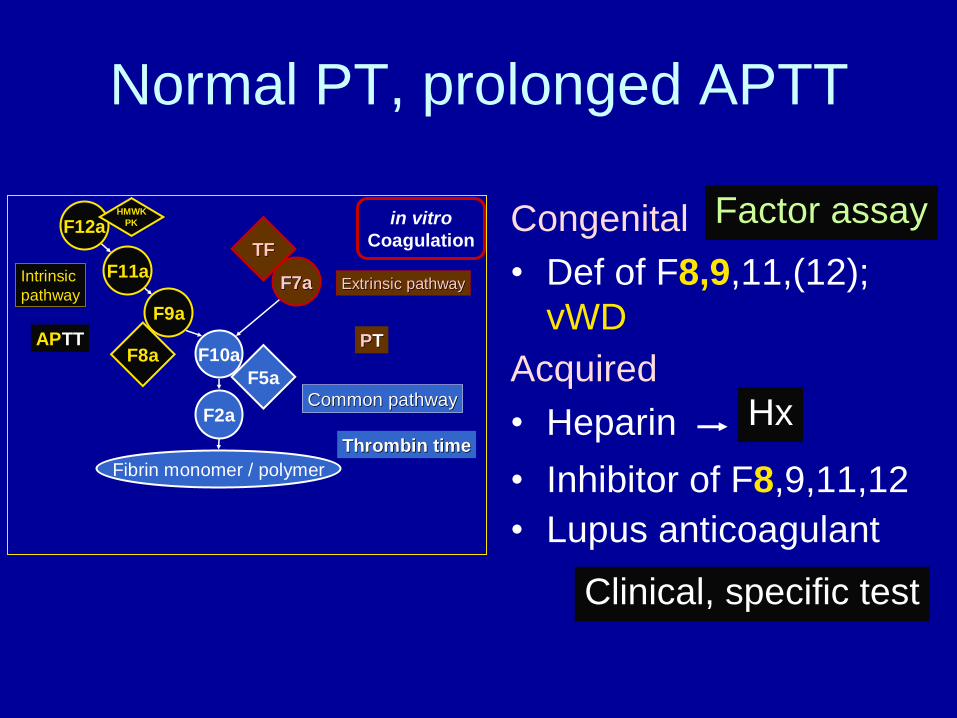
Normal PT, prolonged APTT
Congenital
• Def of F8,9,11,(12);
vWD
F12a
F11a
F9a
F10a
F2a
Fibrin monomer / polymer
F7aF7a
F8a
F5a
TFTF
in vitro
Coagulation
APTT PPTT
Thrombin timeThrombin time
Intrinsic
pathwayExtrinsic pathwayExtrinsic pathway
Common pathwayCommon pathway
HMWK
PK
Acquired • Heparin
• Inhibitor of F8,9,11,12
• Lupus anticoagulant
Factor assay
Hx
Clinical, specific test

Prolonged APTT, Normal PT
Bleeding No bleeding
Mixing test Mixing test
Correctable? Correctable?
Yes
• Def of
F8,9,11 • vWD
No
• F8 inhibitor
• Inhibitor of F9,11
Yes
• F12 def
• Def of HMWK,PK
No
• lupus anti- coagulant
R/O heparin

Prolonged PT, prolonged APTT Congenital
• Def of F10,5,2,1,5+8 Acquired • DIC
• Liver dis
• Warfarin
• Vit. K def
• Heparin high dose
• Snake venom
F12a
F11a
F9a
F10a
F2a
Fibrin monomer / polymer
F7aF7a
F8a
F5a
TFTF
in vitro
Coagulation
APTT PPTT
Thrombin timeThrombin time
Intrinsic
pathwayExtrinsic pathwayExtrinsic pathway
Common pathwayCommon pathway
HMWK
PK
Factor assay
• Inhibitor of F10,5,2,1
• Amyloidosis (F10 def)
Lab: Thrombin time or fibrinogen
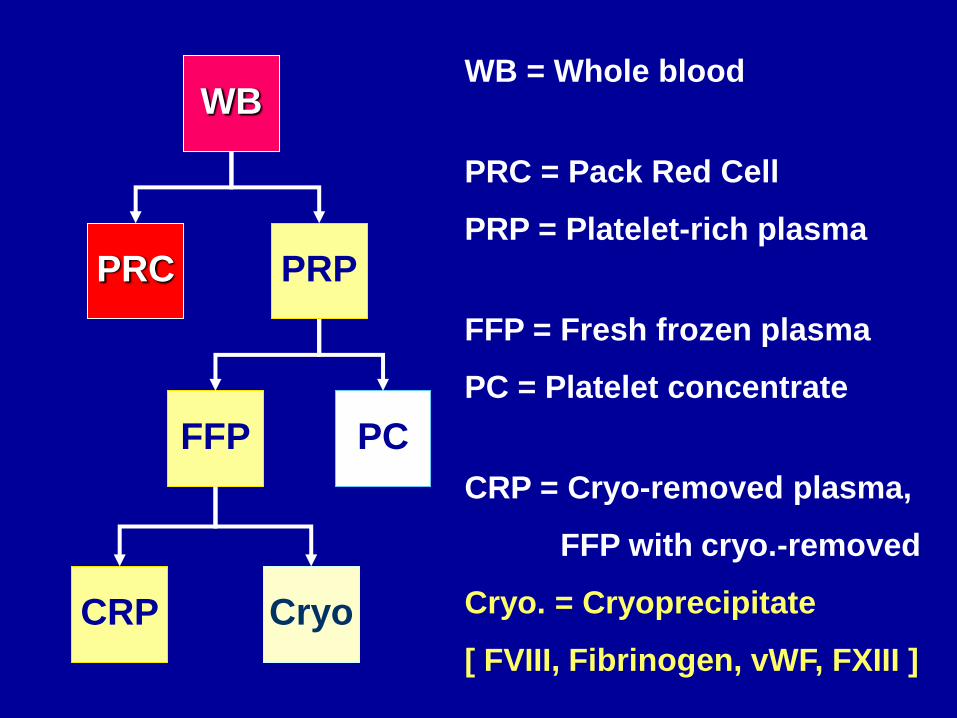
WB
PRC PRP
FFP PC
CRP Cryo
WB = Whole blood
PRC = Pack Red Cell
PRP = Platelet-rich plasma
FFP = Fresh frozen plasma
PC = Platelet concentrate
CRP = Cryo-removed plasma,
FFP with cryo.-removed
Cryo. = Cryoprecipitate
[ FVIII, Fibrinogen, vWF, FXIII ]

Cryoprecipitate: Indications
• Hypofibrinogenemia (congenital/acquired)
• Massive transfusion with bleeding
• Reversal of thrombolytic therapy with bleeding
• Hemophilia A
• von Willebrand disease
• Uremic bleeding
• A component of fibrin glue
• F XIII deficiency

Case Study 1 M 77 yr, large palpable ecchymoses
• PT 82.5 sec (9.9 – 12.7); INR = 8.64
• aPTT 84.7 sec (22.4 – 31.6)
• Platelet adequate
• Never bleed
Most likely Dx?
1. Warfarin
2. DIC
3. Cirrhosis
4. Amyloidosis
5. Pit viper
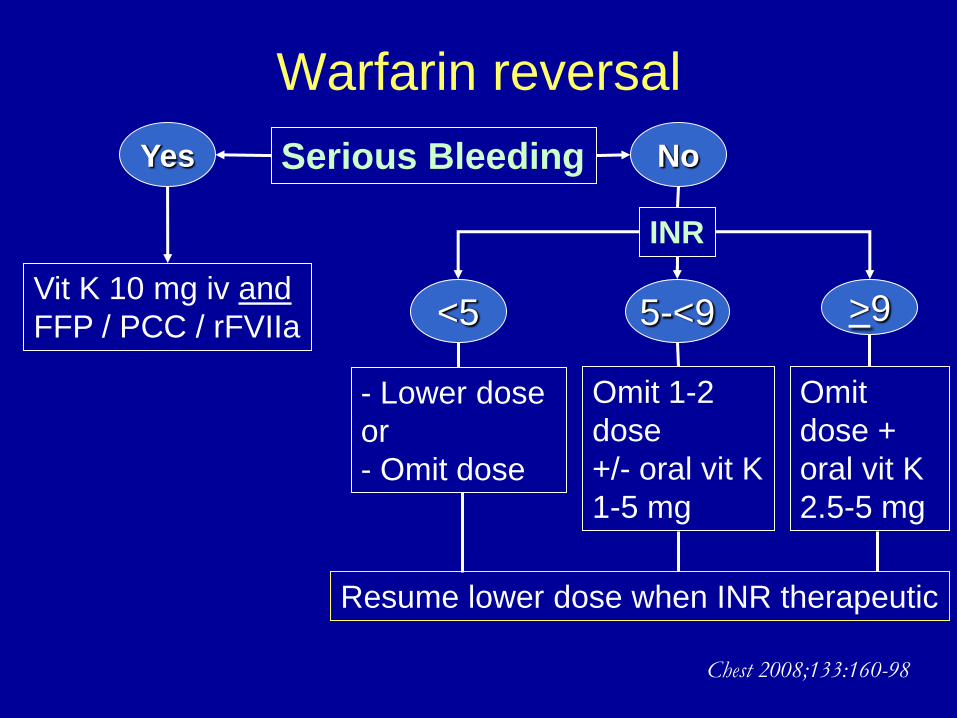
Warfarin reversal
Serious Bleeding Yes No
Vit K 10 mg iv and
FFP / PCC / rFVIIa
INR
<5 5-<9 >9
- Lower dose
or
- Omit dose
Omit 1-2
dose
+/- oral vit K
1-5 mg
Omit
dose +
oral vit K
2.5-5 mg
Resume lower dose when INR therapeutic
Chest 2008;133:160-98
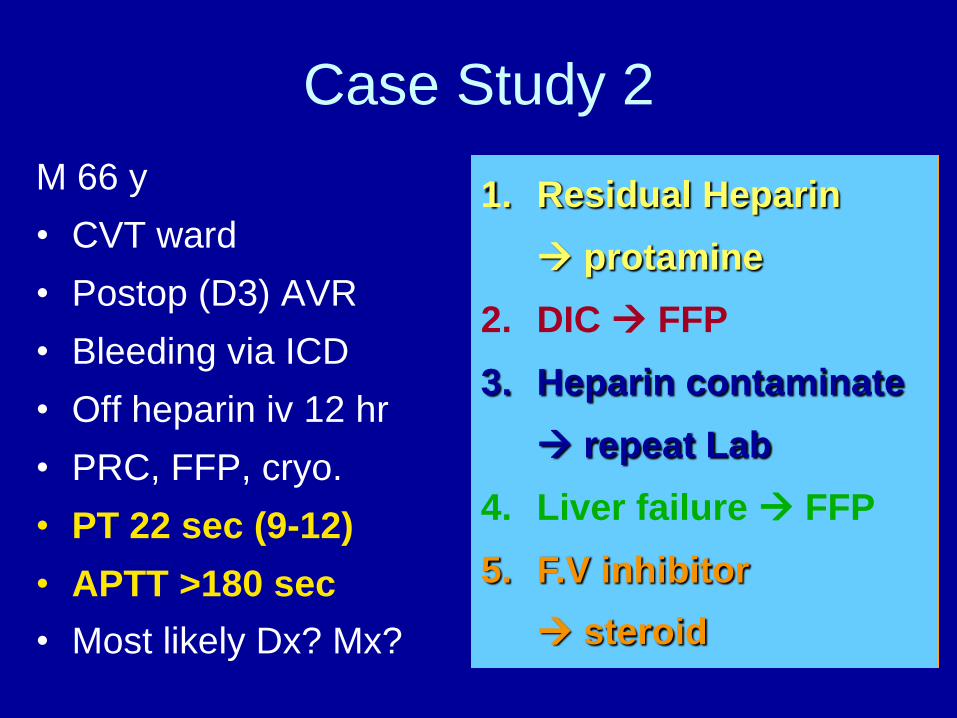
Case Study 2 M 66 y
• CVT ward
• Postop (D3) AVR
• Bleeding via ICD
• Off heparin iv 12 hr
• PRC, FFP, cryo.
• PT 22 sec (9-12)
• APTT >180 sec
• Most likely Dx? Mx?
1. Residual Heparin
protamine
2. DIC FFP
3. Heparin contaminate
repeat Lab
4. Liver failure FFP
5. F.V inhibitor
steroid

Case Study 2
Heparin contamination
Repeat lab via cubital v.
- PT 14 sec (9-12)
- APTT 30 sec (22-30)
Local arterial bleed
Local control
M 66 y
• CVT ward
• Postop (D3) AVR
• Bleeding via ICD
• Off heparin iv 12 hr
• PRC, FFP, cryo.
• PT 22 sec (9-12)
• APTT >180 sec
• Most likely Dx? Mx?

Case 3
M 40 yr , cirrhosis , UGIH, BP 90/60
• platelet 80,000/mm3, PT 15 sec. (N, 9-12) , aPTT 37 sec. (N, 25-35)
• แพทยใ์ห ้PRC 1 u, PLT conc 5 u, FFP 2 u ยังมเีลอืดออกอยู ่ Rx?
A. More FFP
B. More Platelet concentrate
C. Cryoprecipitate
D. Tranexamic acid
E. Endoscopy
Local bleeding with
thrombocytopenia or
coagulopathy
• Management
– local Rx
– systemic Rx
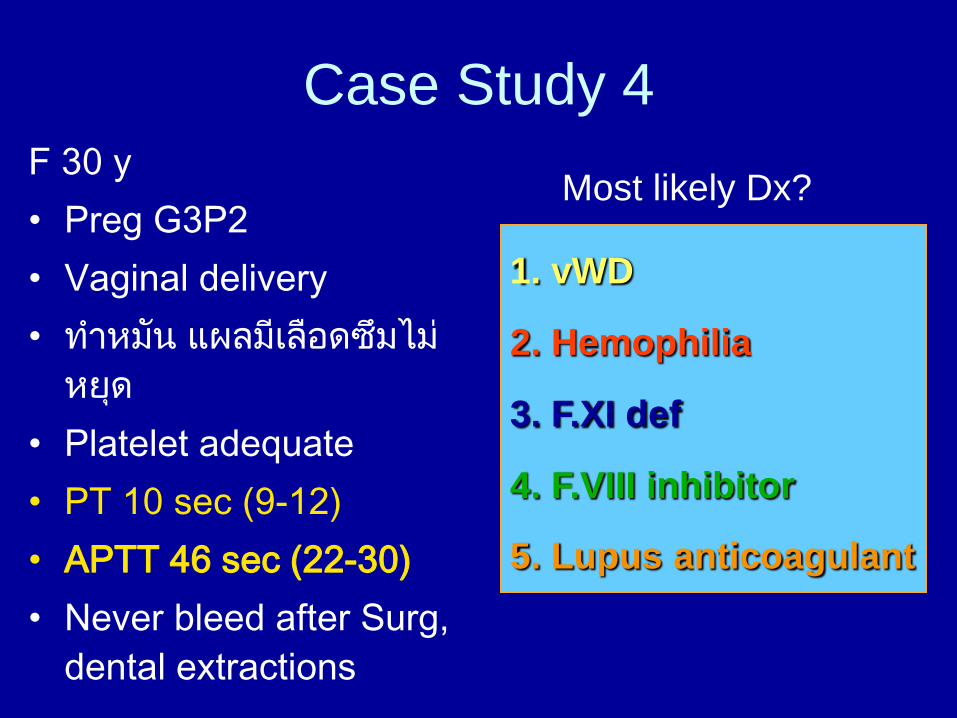
Case Study 4 F 30 y
• Preg G3P2
• Vaginal delivery
• ท ำหมัน แผลมีเลือดซึมไม่
หยุด
• Platelet adequate
• PT 10 sec (9-12)
• APTT 46 sec (22-30)
• Never bleed after Surg,
dental extractions
Most likely Dx?
1. vWD
2. Hemophilia
3. F.XI def
4. F.VIII inhibitor
5. Lupus anticoagulant

Prolonged APTT, Normal PT
Bleeding No bleeding
Mixing test Mixing test
Correctable? Correctable?
Yes
• Def of
F8,9,11 • vWD
No
• F8 inhibitor
• Inhibitor of F9,11
Yes
• F12 def
• Def of HMWK,PK
No
• lupus anti- coagulant
R/O heparin

Case Study 4
F 30 y
• Preg G3P2
• Vaginal delivery
• ท ำหมัน แผลมีเลือดซึมไม่
หยุด
• Platelet adequate
• PT 10 sec (9-12)
• APTT 46 sec (22-30)
• Never bleed
Most likely Dx? Rx?
• Mixing APTT (1:1) 1 hr
= 47 sec (control 33 sec)
• FVIII = 3%
FVIII inhibitor =4 Bethesda Unit
Acquired FVIII inhibitor
associated with postpartum
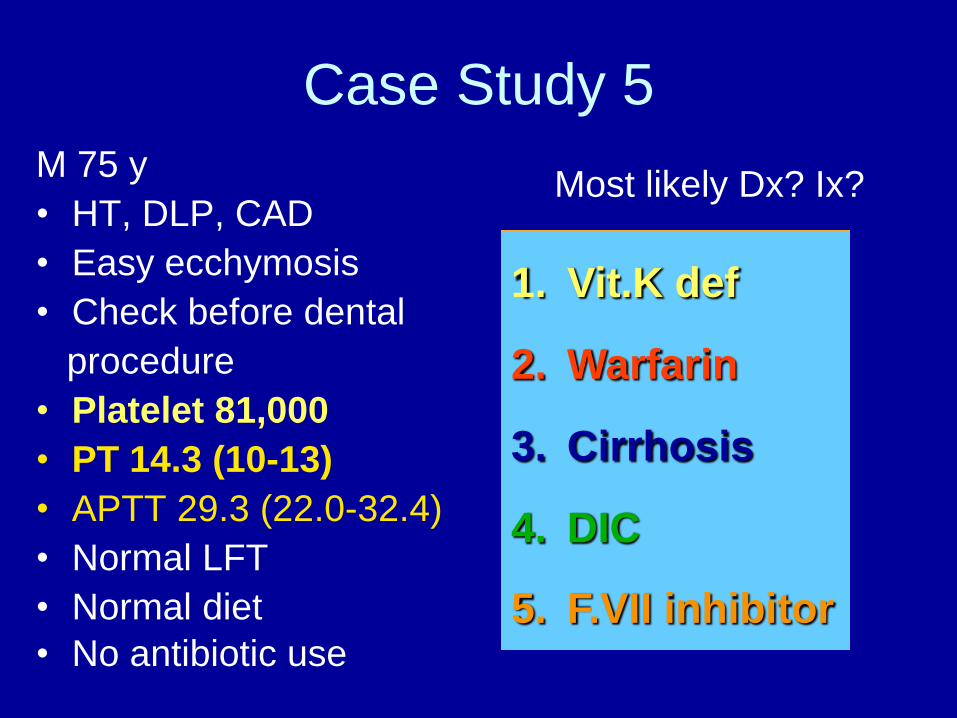
Case Study 5 M 75 y
• HT, DLP, CAD
• Easy ecchymosis
• Check before dental
procedure
• Platelet 81,000
• PT 14.3 (10-13)
• APTT 29.3 (22.0-32.4)
• Normal LFT
• Normal diet
• No antibiotic use
Most likely Dx? Ix?
1. Vit.K def
2. Warfarin
3. Cirrhosis
4. DIC
5. F.VII inhibitor

Prolonged PT, normal APTT Congenital
• F7 def
Acquired
• Liver dis
• Warfarin
• Vit. K def
F12a
F11a
F9a
F10a
F2a
Fibrin monomer / polymer
F7aF7a
F8a
F5a
TFTF
in vitro
Coagulation
APTT PPTT
Thrombin timeThrombin time
Intrinsic
pathwayExtrinsic pathwayExtrinsic pathway
Common pathwayCommon pathway
HMWK
PK F7 assay
Clinical Dx Try Rx + F/U
• DIC – clinical, d-dimer,
fibrinogen
• Def. of fibrinogen • F7 inhibitor – mixing test
Case Study 5 M 75 y
• HT, DLP, CAD
• Easy ecchymosis
• Check before dental
procedure
• Platelet 81,000
• PT 14.3 (10-13)
• APTT 29.3 (22.0-32.4)
• Normal LFT
• Normal diet
• No antibiotic use
Most likely Dx? Ix?
• D-dimer 3200 ug/L
• Fibrinogen 176 mg/dL
• CXR- aortic arch
aneurysm
Chronic DIC
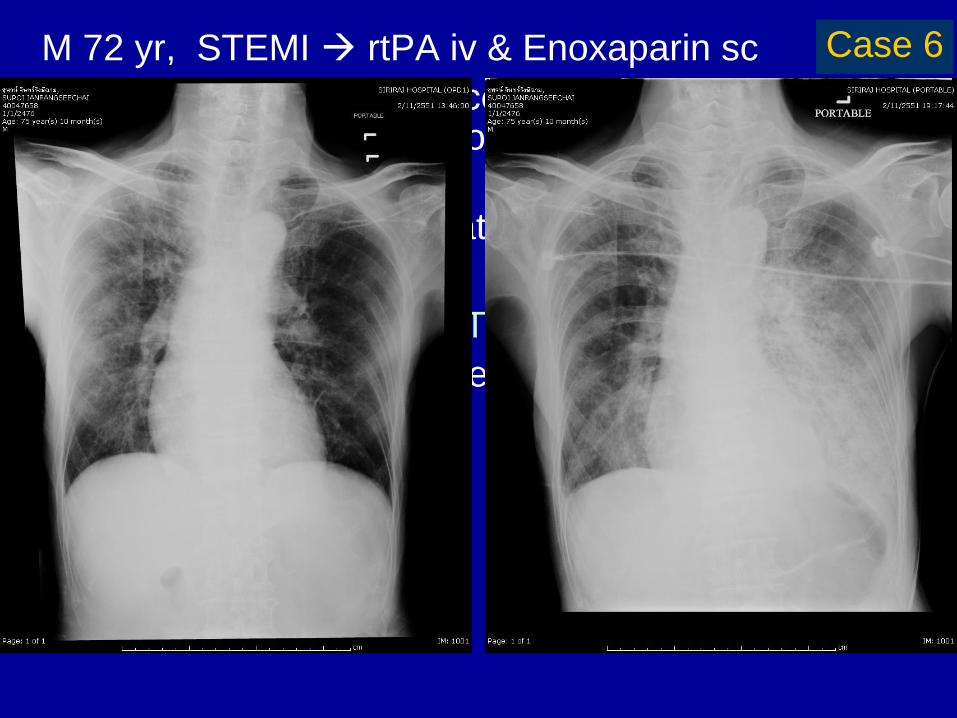
M 72 yr, STEMI rtPA iv & Enoxaparin sc
5-6 hr later – hemoptysis continuously with progressive respiratory distress on respirator
• CXR – new LLL infiltration;
• CBC – normal,
• PT 18.5 (10-12.7), aPTT 59.8 (25-32)
What is your initial management?
A. FFP
B. Protamine
C. Cryoprecipitate
D. rFVIIa
E. APCC
Case 6

M 72 yr, STEMI rtPA iv & Enoxaparin sc
5-6 hr later – hemoptysis continuously with progressive respiratory distress on respirator
• CXR – new LLL infiltration;
• CBC – normal,
• PT 18.5 (10-12.7), aPTT 59.8 (25-32)
What is your initial management?
A. FFP
B. Protamine
C. Cryoprecipitate
D. rFVIIa
E. APCC
Case 6

Thrombolytic agent & Heparin
• SK (Hf. 18-23 min), rtPA (Hf. 3-8 min) ⇩fibrinogen
• Heparin neutralization
– Unfractionated Heparin • protamine 1 mg : residual UFH 100 u
– LMWH (enoxaparin) [60% neutralizable] • <8 hr – protamine 1 mg : LMWH 1 mg
• >8-12 hr – protamine 0.5 mg : LMWH 1 mg
• F/U aPTT 2-4 hr if prolonged repeat protamine 0.5 mg/ LMWH 1 mg
• rFVIIa for uncontrolled bleeding

M 57 yr, DM/HT/CKD
Car accident Bleeding wounds suture continuing bleeding
• Hct 21%, platelet 200,000/mm3
• BUN 92, Cr 12; Coagulogram – normal
• CT brain – acute epidural hematoma
PRC was given as tolerated.
What is the management before operation? A. Platelet transfusion
B. Hemodialysis
C. DDAVP
D. Cryoprecipitate
E. Conjugated estrogen intravenously
Case 7

Uremic bleeding
Treatment Regimen Onset Duration
*PRC /LPB Hct ~30% 1 h While Hct at this level
*EPO 40-150 U/kg Hct 30% Same
x3/wk (7D- ~6 wk)
*Cryoppt. 10 units 1 h 24–36 h[Effective ~ 50%]
*DDAVP 0.3-0.4 mcg/kg 1 h 4 – 8 h
IV or SC
*Conjugated 0.6 mkd iv 5d 6 h 14-21 d (IV)
estrogen 50 mkd po 2 d 5 d (PO)
x 7 days
*Dialysis PD > HD

พระ 24 ปี กำญจนบุรี
• Spontaneous bruises at legs, abdomen, arms for a week
• No underlying dis., no drug use, never bleed
ตรวจที่โรงพยำบำลเอกชนที่กำญจนบุรี
• CBC: Hct 40%, Wbc 9000 (N 42, L 20, M 10, E 28), PLT
150,000
• PT 10 sec (control 10), APTT 35 sec (control 29)
• PE : normal all except ecchymoses
ส่งตรวจอะไรอันดับแรก เพื่อช่วยในกำรวนิิจฉัย
1. Blood smear
2. Repeat coagulogram
3. Mixing test of APTT
4. vWF panel
5. F VIII level
Case 8

Platelets: pale staining
Eosinophils
APDE Acquired platelet dysfunction with eosinophilia

Pseudo gray platelet syndrome
EDTA blood Fingerstick blood
Eur J Haematol 1988;41:326 Int J Hematol 2002;76:376
Clin Lab Haematol 2005;27:336

Thank you for your attention










![Cardiac Surgery PostOp ICU [1862] - it.houstonmethodist.org](https://img.pdfslide.net/doc/110x75/61bd422561276e740b10f7fd/cardiac-surgery-postop-icu-1862-it-.jpg)

















