Embed Size (px)
Citation preview

August 2019
Approach to glomerular diseases
Abdallah S. Geara, MD
Assistant Professor of Clinical Medicine
Renal, Electrolyte and Hypertension
University of Pennsylvania

2
Approach to proteinuria:
• Dipstick, quantification
Isolated glomerular hematuria:
• Collagen IV nephropathies
Nephrotic syndromes
Rapidly progressive glomerulonephritis
Nephritic syndromes
Acute/inpatient management of nephrotic and nephritic syndromes

3
Proteinuria

4
Different types of proteinuria
Glomerular:
• Mainly albuminuria
• Can be heavy
Tubular:
• Less than 3 g/d, the dipstick can be negative
• LMW (<25 KDa) proteinuria (α1-microglobulin, retinol-binding protein and in the β2-microglobulin
region)
Overflow:
• Albumin infusion
• Immunoglobulin (MM), Myoglobin (rhabdo), hemoglobin (intravascular hemolysis), Lysozyme
(AML)
Post-renal:
• Less than 1g
• UTIs, stones, tumors
Others:
• Transient: Acute illness, heavy exercise (mild <1g/d)
• Orthostatic: 2-5% of adolescents, (1-2 g/d), split urine collection, benign

5
Proteinuria
Normal protein excretion is 80 mg/day (up to 150mg/d is considered normal)J Clin Invest, 1969, vol. 48 (pg. 1189 -1198
Isolated proteinuria:
• NO AKI, NO hematuria, NORMAL sediment
Direct measurement of albuminuria with traditional immunology-based laboratory methods,
such as immunonephelometry, immunoturbidimetry, and radioimmunoassay, can produce
results that vary considerably
Estimated albumin excretion rate (or eAER) can be calculated by multiplying the
spot UACR by the expected 24-hour creatinine generation

6
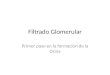
The value of simultaneous measurements of urinary
albumin and total protein in proteinuric patients
Nephrol Dial Transplant. 2012 Apr;27(4):1534-41.
a) ROC curves for uAPR, uACR and uPCR
demonstrating the superiority of uAPR over
uACR in discriminating between tubular
pattern and non-tubular proteinuria pattern
on uPEI (n =1011).
b) (b) ROC curves for uAPR and the specific
tubular markers uNCR and
uβ<sub>2</sub>CR demonstrating non-
inferiority of the uAPR for detecting tubular
proteinuria patterns on uPEI in the renal
outpatient subgroup (n = 248)
UAPR < 0.4 in tubular or overflow proteinuria
UAPR > 0.4 in glomerular proteinuria.

7
Measurement of proteinuria
Urine dipstick:
• Detects albumin (sulfosalicylic acid test for tubular)
• False positive:
– IV contrast (iodinated)
– Alkaline urine (pH>8)
– Gross hematuria
– Antiseptics (chlorhexidine)
24h-urine protein:
• Limited by the amount of daily creatinine excretion
UPCR (first or second morning urine) correlated well with 24 hours); it assume 1g/d
of creat excretion
• UPCR depends on the muscle mass
• underestimate 24-hour proteinuria in blacks, in Hispanics, and in men,
• overestimate proteinuria in whites and in women.

8
Glomerular structure

9

10
Spectrum of Glomerular diseases

11
Isolated hematuria

12
Isolated hematuria
Transient hematuria is a relatively common finding over time in adults
Etiologies:
• IgA nephropathy: episodic gross hematuria
• hereditary nephritis (Alport’s syndrome): + family history
• Thin basement membrane nephropathy: + family history
Renal biopsy does not lead to a change in management (1 of 36 patients)
• 24/28 (86%) of cases of nephrotic range proteinuria
• 22/31 (71%) of cases of acute renal failure
• 58/128 (45%) of cases of chronic renal failure
• 9/28 (32%) of cases with hematuria and proteinuria
• 3/25 (12%) of cases with non-nephrotic proteinuria alone
• 1/36 (3%) of cases with hematuria alone.
Nephrol Dial Transplant. 1994;9(9):1255.

13
Type IV collagen associated nephropathies
3 triple helical protomers:
• alpha-1-1-2
• alpha-3-4-5 (GBM)
• alpha-5-5-6
GBM is a meshwork of laminins, type IV
collagen and others.
GBM measures 300 to 350nm

14
Thin basement membrane disease
(benign familial hematuria) or (AD Alport’s syndrome)
Epidemiology:
• Family history in 30-50%
• 5-9% of the general population
heterozygous mutations in either COL4A3 (α3) or COL4A4 (α4)
Biopsy:
• EM: diffuse thinning of the glomerular basement membranes (GBM)
• Immunostaining for alpha 3,4 and 5 is normal
• Some patients can have an FSGS lesion
Some of the patients develops proteinuria
No ocular or hearing loss
Prognosis is good:
CKD preventive approach

15
Alport’s Syndrome
(hereditary nephritis)
often associated with sensorineural hearing loss and ocular abnormalities
Mutations in the α3 (ch 2), α4 (ch 2) and α5 (ch X) chains of type IV collagen
80% are X-lined, 15% AR, 5% AD
Clinically (genetic abnormality influence the phenotype):• Glomerular hematuria• Ocular abnormalities and progressive
sensorineural hearing loss • X linked: Male ➔ ESRD; female ➔ CKD
and proteinuria• 3% have post transplant anti-GBM disease
Biopsy:
Lamellated GBM or
abnormal deposition
of α3α4α5(IV) on
immunostaining

16
Thin basement membrane
Patients with thin GBMs may have episodic macroscopic hematuria throughout life and
are at risk of developing proteinuria and progressive CKD.

17
Nephrotic syndromes

18

19
Definition of nephrotic syndrome
Nephrotic syndrome (clinical + lab features)
Proteinuria > 3.5g/24h Alb< 3.0 Edema

20
Etiologies of nephrotic syndromes
Renal Sd: Systemic diseases
Minimal change disease (MCD)
(some are genetic: nephrin, podocin, alpha-
actinin-4)
SLE
Focal Segmental GlomeruloSclerosis (FSGS) DM
Membranous Nephropathy (MN) Amyloidosis (AL, AA, familial, senile, others)
Sec FSGS
Sec MCD
(NSAIDs, Hodgkin)
Sec MN
HepB, autoimmune diseases, thyroiditis,
carcinoma, meds (NSAIDs, penicillamine, gold,
and captopril).
Postinfectious and infection-associated glomerulonephritis, membranoproliferative
glomerulonephritis, and IgA nephropathy

21
Associated findings with nephrotic syndrome
Nephrotic range proteinuria without nephrotic syndrome
Hypoalbuminemia:
• Urinary loss (?other factors)
Hyperlipidemia:
• Hyperchol, hypertrig
• Low oncotic pressure => ↑ lipoprotein secretion
Edema:
• Hypoalbuminemia => ↓ oncotic pressure
• Primary renal sodium retention

22
Minimal Change Disease
90% of Nephrotic syndromes in children < 10yo
Biopsy:
• EM: diffuse effacement of the epithelial cell foot processes
Pt can show signs of hypovolemia (Low BP)

23
Focal Segmental GlomeruloSclerosis (FSGS)
Most common primary etiology for nephrotic
syndrome (35%; up to 50% in blacks)
Secondary FSGS:
HIV Reflux nephropathy Previous
glomerular injury (hyperfiltration) Obesity
Meds (bisphosphonate; pamidronate; IFN therapy)
Histology:
• Focal vs diffuse to all the glomeruli
• Segmental vs global to the glomeruli
Primary podocytopathy:
• More acute onset, lower albumin, higher proteinuria, full
nephrotic syndrome
Collapsing FSGS: HIV and bisphosphonate

24
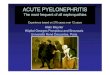
Membranous nephropathy
Thickening of the BM with ED deposits without a proliferative lesion
Primary: Anti-Phospholipase A2 receptor (anti-PLA2R Ab)
Secondary: Hep B, autoimmune diseases, thyroiditis, carcinoma, and drugs (gold,
penicillamine, captopril, and NSAIDs)

25
Amyloidosis
AA, AL, hereditary/familial or age-related
Localized vs systemic
Amyloid fibrils are insoluble polymers comprised of
low molecular weight subunit proteins
Co-deposition of other non-fibrillar substances:
GAGs, serum amyloid P-component (SAP, a
member) and specific apolipoproteins (E and J)

26
Proteinuria
Hypoalbuminemia: due to loss in the urine
• ?hypoalb is out of proportion to the loss
• ?albumin level can be different for the same degree of proteinuria
• Hypoalbuminemia is more severe than PD patients with similar protein loss
Edema:
• Underfilling: decrease oncotic pressure
• Overfilling: primary salt/water retention in the collecting tubules (ANP)
• Less responsive to loops diuretics

27
Hyperlipidemia
1. The low oncotic pressure ➔ it increases hepatic lipoprotein synthesis ➔
hyperlipidemia.
2. Decrease clearance ➔ hyperTrig
hyperChol and hyperTrig and lipiduria

28
Thromboembolism
Pathogenesis:
• Urinary loss of antithrombin and plasminogen
• Increase plts activation
• Hyperfibrinogenemia
Usually Renal vein thrombosis are chronic (acute RVT causes infarction)
• It was never shown that chronic RVT increases the proteinuria or causes AKI
Therapy:
• No guidelines

29
Main clinical consequences
AKI: less in children
Thromboembolism:
• venous, mainly membranous (>10g), renal venous thrombosis (asymptomatic, flank pain + AKI)
• Membranous: Occurs early in the disease, alb ≤ 2.8 increases the risk by 2.5x, doubles for every 1g/dL decrease.
• Other disease: alb <2g/dL; the risk doubles for every 1g/dL decrease of albumin
• ? decreased levels of antithrombin and plasminogen (due to urinary losses)
Infections: low IgG levels (due to urinary loss)
Proximal tubular dysfunction
• glycosuria, aminoaciduria, phosphaturia, bicarbonaturia, and vitamin D deficiency
Anemia

30
Therapy
The approach is histology driven (steroids, CNI, anti-CD20, Cytoxan…)
Proteinuria:
• ACEI/ARBs (caution if the BP is low e.g. MCD)
Edema: low salt diet, diuretics (less delivery due to hypoalbuminemia , urinary prot
binding due to albuminuria)
Hyperlipidemia: reversible, statin
Hypercoag: prophylactic anticoagulation
• 2-3 => aspirin
• <2 => LMWH, warfarin
Most nephrotic syndromes are not an imminent risk of ESRD and the initial therapy
should address the symptoms and prevention of complications

31
Nephritic disease

32
Definition of nephritic syndrome
Rapidly progressive glomerulonephritis (RPGN):
• clinical syndrome
• + urine sediments + AKI (days, weeks or months).
Crescentic GNItis:
• Extensive crescent formation
Crescents:
• Cellular/fibrocellular/fibrous

33
Mild nephritic: nephritic sediment, mild proteinuria (usually less than 1.5 g/day).
(No heavy proteinuria, edema, hypertension, and renal insufficiency)
Severe nephritic (RPGN) diffuse glomerulonephritis, heavy proteinuria (may be in the nephrotic range),
edema, hypertension, and/or renal insufficiency. Diffuse glomerulonephritis affects most or all of the glomeruli.

34

35

36
Pathogenic classification
Immune complex:
• IgA nephropathy: mesangial IgA
• Post-infectious: subepithelial humps
• Lupus: Full house (IgG, IgA, IgM, C3 and C1q), mesangial+ subendothelial
• Cryoglobulin: pseudothrombi (intraluminal)
Pauci-Immune:
• Necrotising GN
• No immune deposits
• ANCA +; GPA or MPA
• ANCA – (5-10%); lysosome-associated membrane protein 2 (LAMP-2)
• Medication induced:
– Propylthiouracil, hydralazine, allopurinol, penicillamine, minocycline.
– MPO-ANCA positive, but some are both high-titer MPO and PR3 (hydralazine).
Anti-GBM

37
Anti-GBM (Goodpasture’s disease)
Ab ((IgG 1 and 3) against an antigen intrinsic (GBM)
anti-GBM antibodies (which are typically immunoglobulin G but sometimes IgA or IgM) is
the NC1 domain of the alpha-3 chain of type IV collagen (alpha-3(IV) chain)
No systemic complaints
Biopsy:
• Linear deposits of IgG or IgA (no clonality)
• (diabetic nephropathy and fibrillary can cause linear deposits)
The Ab is short lived and relapses are rare

38
Lupus nephritis

39
IgA nephropathy

40
Poststreptococcal or infection-related GNitis
The IC formation is likely in situ process
Antigen is a Nephritis-associated plasmin receptor (NAPlr)
Pathology:
• Diffuse proliferative, endocapillary proliferation, subepithelial humps
• Crescent is uncommon
• IF: C3 and IgG
• EM: subepithelial and subendothelial deposits
C3 and CH50 are depressed (C4 usually normal)
Infective endocarditis/Shunt nephritis:
• C3 can be depressed, ANCA can be positive, Crescentic GN is more frequent
• Some patients have a pauci-immune biopsy
Staph-associated GNitis:
• Middle-aged to older adults with concurrent infection, some have cutaneous vasculitis
• Low C3, kidney biopsy is similar to post-infectious

41
Cryoglobulinemic
Cryoglobulins are Igs or a mixture of Igs + Complement components.
Clinical:
• Arthralgia, purpura, skin ulcers, glomerulonephritis, and peripheral neuropathy
Classification:
• Type I: Monoclonal Ig (IgG or IgM)
– Ischemic symptoms (skin, kidney…); thrombotic changes in the kidney
• Mixed cryoglobulin: (MPGN kidney changes)
– type II: monoclonal IgM (RF) + polyclonal IgG (HepC/B, HIV, autoimmune,
lymphoproliferative))
– type III: Polyclonal Igg and IgM
Lab:
• Normal C’ in type I; -RF
• Low C4 in type II; +RF

42

43
General therapy
Pulse methylprednisolone (500 to 1000 mg/day) for 3 days
Consider plasmapheresis (especially with pulmonary involvement)
Prepare for kidney biopsy
Anticipate long term immunosuppression with infection prevention:
• Tb, hepatitis screening
• Immunization (influenza, pneumonia, Varicella)

44
ANCA-associated Vasculitis
Testing for ANCA:
• ELISA
• Indirect IF
Drug-induced ANCA-associated vasculitis:
• (Mostly MPO), including hydralazine,
propylthiouracil, methimazole, carbimazole, and
minocycline.

45
Plasma-cell associated disorder
Blood. 2012 Nov 22;120(22):4292-5

46
Thank you